extern conference 4 oct 2007. history a 4-month-old boy chief complaint: high-grade fever 1 day ...
TRANSCRIPT

Extern conferenceExtern conference
4 OCT 20074 OCT 2007

History
A 4-month-old boy Chief complaint: high-grade fever 1 day Present illness:
3 d PTA he had low grade fever with no other symptoms.
1 d PTA he had high grade fever with chill without URI symptoms, N/V, or diarrhea.
He exhibited lethargy and food refusal. The bulging of his anterior fontanelle was observed. He had no seizure.
History
Present illness: He took only acetaminophen every 4 hours but
his symptoms did not relieved. On the day of admission, he sought for a doctor
and was diagnosed as brain edema. He was suggested to go to a hospital.
He had no history of trauma. Nobody in his family had symptoms like him.

History
Pertinent underlying disease: none Significant medical history: none (healthy) Significant neonatal history: none Developmental history: normal
Smile, hold head up, crawl, localize sounds, glare Dietary history: absolute breast feeding

History
Immunization: BCG, 1OPV, 1DPT, 2HBV Current medication: none Significant family history:
Father - HBV carrier Mother - Euthyroid goiter

Physical examination
T 38.5oC, RR 50/min, HR 180/min, BP91/62mmHg
BW 8.1 kg , Ht 50 cm GA: look sick, drowsiness, not pale, no
jaundice, no edema, dry lips, slightly sunken eye ball, anterior fontanelle-bulging, 2x3 cm
HEENT: pharynx-not injected, normal TM both ears

Physical examination
RS: normal breath sound, no adventitious sound
CVS: normal S1&S2, no murmur Abd: soft, not tender, liver and spleen-not
palpable Genitalia: WNL

Physical examination
CNS: pupil 3 mm BRTL, no facial palsy motor power grade IV+ all DTR 3+ all Stiff neck : positive Brudzinski’s sign : positive Kernig sign : positive


Brudzinski sign

Problem list Fever for 3 days Drowsiness for 1 day Bulging ant.fontanelle and presence of
meningeal signs Mild dehydration

Differential diagnosis Meningitis Sepsis

Approach to Acute Febrile Illness

Definition of fever temperature -Rectal >38ºc
-Oral >37.6
-Axillary >37.3 Acute fever - fever with source
- fever without source
History taking Fever : character, pattern, duration Associate organ/systemic symptom
- RS : cough, rhinorrhea, dyspnea
- GI : nausea, vomiting, diarrhea,
- GU : abnormal urine
- NS : alteration of consciousness, seizure, severe headache

History taking Behavior activity e.g. drowsy, food/milk
intolerance Sick contact Previous treatment, past medication Underlying disease, recent immunization

Physical Examination Vital signs : GA : irritability, sign of dehydration, pale,
jaundice HEENT : TM, nasal discharge, tonsils &
pharynx Skin rash , sign of soft tissue infection CVS : new onset of murmur, embolic
phenomenon

Physical Examination RS : breath sound, adventitious sound,
percussion Abdomen : BS, hepatosplenomegaly NS : level of consciousness, fontanelle, motor
system, meningeal irritation sign Bone and joint system

Investigation CBC ,UA Indication for LP in children with fever
- alteration of consciousness
- age<18 months with first episode of febrile seizure or complex febrile seizure
- age<3 months with sepsis
- suspected meningitis
Meningitis with sepsis

Clinical presentation Depend on the patient’s age
- newborn: nonspecific
- infancy: fever, vomiting, irritability, convulsion, tense& bulging fontanelle
- children: fever, chills, vomiting, severe headache
Meningococcemia : purpura fulminans

purpura fulminans

Clinical presentation Meningeal irritation sign
- significantly less frequent in neonates
- Brudzinski sign, stiff neck, Kernig sign

Kernig’s signSevere stiffness of the hamstrings causes an inability to straighten the leg when the hip is flexed to 90 degrees.

Brudzinski’s sign
Severe neck stiffness causes a patient's hips and knees to flex when the neck is flexed.

AGE COMMON ORGANISM EMPIRICAL ANTIBIOTIC
Newborn infants GBS
E.coli and other gram negative enteric bacteria enterococci
Ampicillin + Gentamicin
Or Cefotaxime
Infants & children < 5 yo H.influenzae type b
S.pneumoniae
Salmonella
N.meningitidis
Cefotaxime
Children older than 5 yo S.pneumoniae
N.meningitidis
Cefotaxime

Treatment Dexamethasone in Hib meningitis with in min
after first dose of ATB can reduce risk for hearing and neurologic complication
- 0.15 mg/kg q 6hr for 4 days or
0.4 mg/kg q 12 hr for 2 days
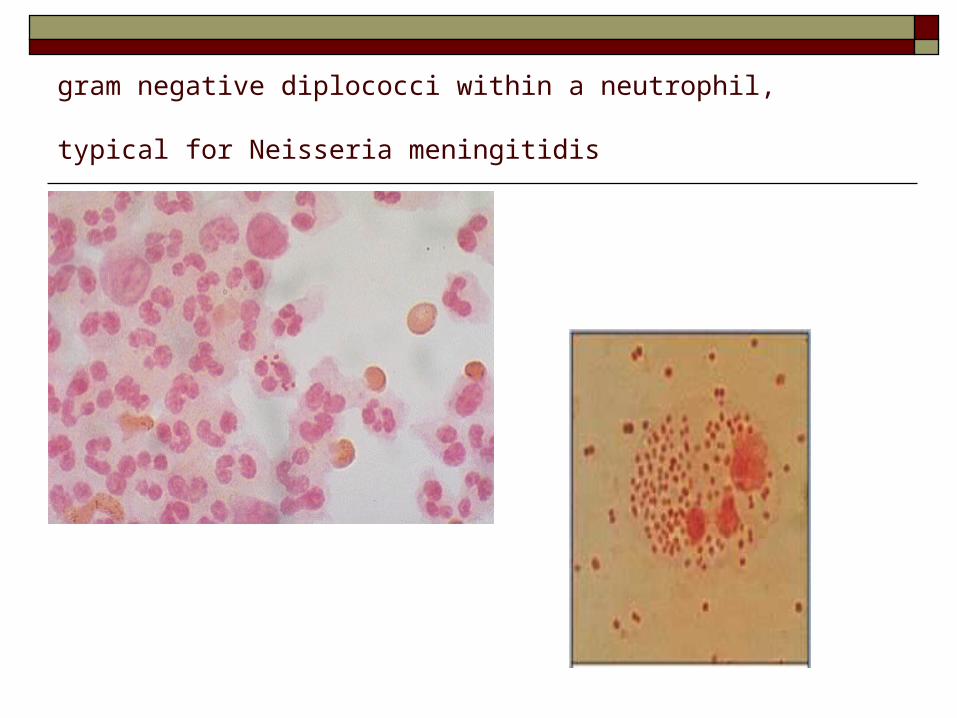
gram negative diplococci within a neutrophil, typical for Neisseria
meningitidis

GBS

S.pneumoniae

H.Infuenzae type B

E.coli

Salmonella sp.
Diagnosis definite diagnosis: CSF examination and C/S CSF gram stain Rapid antigen testing:
GBS, E.coli K1, S.pneumoniae, Hib, N.meningitidis
Hemoculture

Investigation :admission D1 Blood for H/C , CBC , BUN , Cr ,
Electrolyte , BS LP and CSF analysis, CSF culture, gram stain UA ,MUC

Lab : Admission day1 CBC : Hct 35.4, WBC 21160, N72.7, L 15.3,M11.9,
Plt 371,000, MCV79.2 BUN7, Cr0.3 , Na133, K 4.3, Cl 97, HCO3
16,AG20, BS 137 U/A : pH 6.0 ,sp.gr1.015, WBC0-4, Glu3+, Protein -,
Ketone - CSF : Glu 56, TP 100, RBC 10,000, WBC 1,960
(correct WBC : 1,946) CSF G/S : no bacteria was seen, few PMN

Lab : Admission Day2 Bacterial Ag profile: Hib, N. Meningitidis A,
B/Ecoli, C, Y/W, Strep. Agalactiae, Strep. Pneumo : All Negative

CSF profileCondition Normal CSF Normal CSF
(newborn)
Bacterial meningitis
Color
Pressure (mm.H2O)
WBC (mm3)
Protein (mg/dl)
Glucose (mg/dl)
Comments
Clear
50-80
<5, 75% lymphocyte
20-30
>50, 75% BS
Clear
0-30,
2-3% PMN
19-149
32-121
Cloudy
Usually elevated
> 1000
PMNs > 50%
Usually 100-500
Depressed
Organism may be seen by gram stain/
culture

CSF profileCondition Viral
meningitis
TB
meningitis
Pressure (mm.H2O)
WBC (mm3)
Protein (mg/dl)
Glucose (mg/dl)
Comments
Normal or slightly elevated
100-500
PMN<40%
50-100>30
Usually elevated
10-500, PMN early but lymphocyte predominated
100-3,000<50
AFB almost negativeM.TB may be detected by
PCR/C/S
Nelson Textbook of Pediatrics 16th ed.

Diagnosis
Bacterial
meningitis

Treatment1 1.Empirical antibiotics Cefotaxime (300mg/kg/day) 300mg iv q 6hr Gentamicin (5mg/kg/day) 15mg iv q 8hr 2.supportive treatments Paracetamol(120mg/5ml)4ml oral prn for fever
q4-6 hr IV fluid

Treatment2 3.monitoring Record v/s q 4hr Record neuro sign q4hr HC,BW OD Record I/O

Lab : Admission Day2 H/C : gram –ve rod MUC : no growth Bacterial Ag profile: Hib, N. MeningitidisA,
B/Ecoli, C, Y/W, Strep. Agalactiae, Strep. Pneumo : All Negative

Treatment3 Ciprofloxacin <40 MKD>
sig 110 mg iv q 8 hr

TreatmentCausal organism Duration(days)
GBS,L.monocytogenase 14-21
H.influenzae,S.pneumoniae
N.meningitidis
Salmonella
Gram negative bacilli
10-14
7-10
28
21
-Add ciprofloxacin in Salmonella meningitis to prevent relapse
-Change ATB to PGS in mennigococcal meningitis if sensitive

Lab : Admission Day3 CSF culture : Salmonella groupD H/C :Salmonella groupD Drug sensitivity : Cefotaxime, Ciprofloxacin

Repeated LP For diagnosis : in questionable case repeated
LP in 24 hrs For evaluate response of treatment(48-
72hrs after treatment)- cases with poor response- resistant organism- neonatal meningitis
-those received steroid

Complication Seizure Subdural effusion 20-30%,subdural empyema
1% SIADH Hearing loss (require hearing evaluation at the
end of treatment) Hydrocephalus brain abscess

Progress note

Progress note

Plan Continue ATB 28 days

Special thanks
A. Kulkanya Chokephaibulkit, A. Jeeranda Santiprapob A. Panjama