expert system for offline clinical guidelines and treatment · expert system for offline clinical...
TRANSCRIPT

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2639
Expert System for Offline Clinical Guidelines and Treatment
Tanzila Saba1, Saleh Al-Zahrani
2 and Amjad Rehman
1
1Faculty of Computing, Universiti Teknologi Malaysia (UTM), 81310 Skudai Johor Malaysia
2Faculty of Computer and Information Sciences, Al-Imam Muhammad bin Saud Islamic University Riyadh KSA
Abstract: Offline clinical guidelines are normally designed to coordinate a clinical knowledge base, patient
information and an inference engine to create case based guidance. In this regard, offline clinical guidelines are still
popular among the healthcare professionals for updating and support of clinical guidelines. Although their current
format and development process have several limitations, these could be improved with artificial intelligence
approaches such as expert systems/decision support systems. This paper first, presents up to date critical review of
existing clinical expert systems namely AAPHelpm, MYCIN, EMYCIN, PIP, GLIF and PROforma. Additionally,
an analysis is performed to evaluate all these fundamental clinical expert systems. Finally, this paper presents the
proposed clinical expert system design and development to help healthcare professionals for individual treatment.
[Saba T, Al-Zaharani S, Rehman A. Expert System for Offline Clinical Guidelines and Treatment Life Sci J
2012;9(4):2639-2658] (ISSN:1097-8135). http://www.lifesciencesite.com 393.
Keywords: Expert system, Quality of Information (QoI), Clinical guidelines, Diagnosis, Treatment.
1. Introduction
The developments of Expert Systems (ESs) have
drawn much attention of the research community in the
last few decades. The possibility of expert's systems
has additionally been generally acknowledged in
clinical environment, beginning from a straightforward
database inquiry to complex treatment proposal [1].
The logical writing gives the significant wellspring of
learning joined by nearby and rehearsed based proof.
The information of expert's systems exists as rules.
There are four zones during the time spent building up
a rule based experts system [2,4].
The main issue in the process of expert system
development is rule design and representation. This
territory concentrates on the representation of a rule,
such as type of expression, information sort, upkeep,
nearby adjustment, and so forth. The second territory is
rule securing, which is a procedure that encourages the
information obtaining process specifically from a space
experts. Thirdly, range is rule check & testing.
This procedure plans to guarantee the machine-
interpretable rule is unambiguous and grammatically
and also semantically right. Furthermore, we have to
test rules utilizing existing patient information. The last
procedure is rule execution, which concentrates on the
execution time and guarantees the rule motor can keep
running in different clinical spaces and in different
modes. Expert's systems appear to be extremely useful
in supporting clinical options; be that as it may, it is
hard to get wellbeing experts to really utilize them, so
Abbod et al. [3] abridges ten tenets for effective
execution of expert's systems in clinical environment.
These tenets are:
i. Speed of giving proposal
ii. Anticipate needs and convey progressively.
iii. Recognize that human services experts will
firmly oppose ceasing (recommendations) (need to
give elective choices to stay away from resistance)
iv. Changing bearing is simpler than ceasing.
v. Simple mediations work best a rule on a
solitary screen.
vi. Acquire extra data just when wanted.
vii. Monitor affect, get input and react.
viii. Oversee and keep up learning based systems.
Expert's systems are likewise utilized as a part of
different spaces of human services. For instance,
Chawla and Gunderman [5] compress reconnaissance
systems for early identification of bioterrorism-related
maladies. Coordination of Geographic Information
Systems (GIS) and human services permits depicting
and comprehension the changing spatial association of
social insurance, looking at the relationship between
wellbeing results and get to, and investigating how
conveyance of medicinal services could be enhanced
[6,7].The rest of the paper is organized further into

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2640
three main sections. Section 2, importance of AI in
clinical guidelines, section 3 presents in detail
background of computer interpretable guidelines,
section 4 describes clinical expert systems and their
merits/demerits; section 5 describes existing expert
systems for clinical guidelines along with their
shortcomings. Section 6 presents proposed expert
system. Finally, section 7 covers conclusion.
2. Artificial Intelligence and Clinical Guidelines
The history relation of A.I and clinical guidelines
is very old. The first practice started in early 80s.
Clinical guidelines are supposed to represent the best
clinical suggestions, records and practices.
Subsequently, are presently standouts amongst the
most focal ranges of research in Artificial Intelligence
(AI) in pharmaceutical and in medicinal basic
leadership. Clinical rules assume distinctive parts in the
clinical procedure: for instance, they can be utilized to
bolster doctors in the treatment of illnesses, or for
scrutinizing, for assessment, and for training purposes.
2.1. Collaborative decision making
Cooperative decision making is a circumstance
confronted when people all things considered settle on
a decision from the available options. This choice is no
more extended inferable from any single person who is
an individual from the gathering. This is on the
grounds that every one of the people and social
gathering procedures, for example, social impact adds
to the result. The choices made by gatherings are
frequently unique in relation to those made by people.
Bunch polarization is one clear illustration: bunches
tend to settle on choices that are more extraordinary
than those of its individual individuals, toward the
individual slants [11,12]. However, during the
application of clinical guidelines, there are moments
when this type of decision is required. The selection
among scientifically valid options during the medical
process must be done based on the opinions of the parts
involved (healthcare professionals and patients).
Technology-assisted decision making may help the
generation of ideas and actions, the choice of
alternatives and the negotiation of solutions. The
existence of CIGs and a tool for execution of medical
guidelines enables the implementation of automated
group decision making [13,14].
A group decision environment with a decision
model will help healthcare professionals and patients
clarify their position in the decision making process
and assure that their perspectives and preferences are
heard.
2.2. Expert Systems
A program that does a task that would some way
or another be performed by a human. For instance,
there are some expert systems that can analyze human
diseases, make money related gauges, and timetable
courses for conveyance vehicles. Some expert systems
are intended to replace human specialists, while others
are intended to help them [15,16].
Expert systems are a piece of a general class of
PC applications known as computerized reasoning. To
outline a specialist framework, one needs a learning
designer, a person who concentrates how human
specialists settle on choices and makes an interpretation
of the tenets into terms that a PC can get it [17].
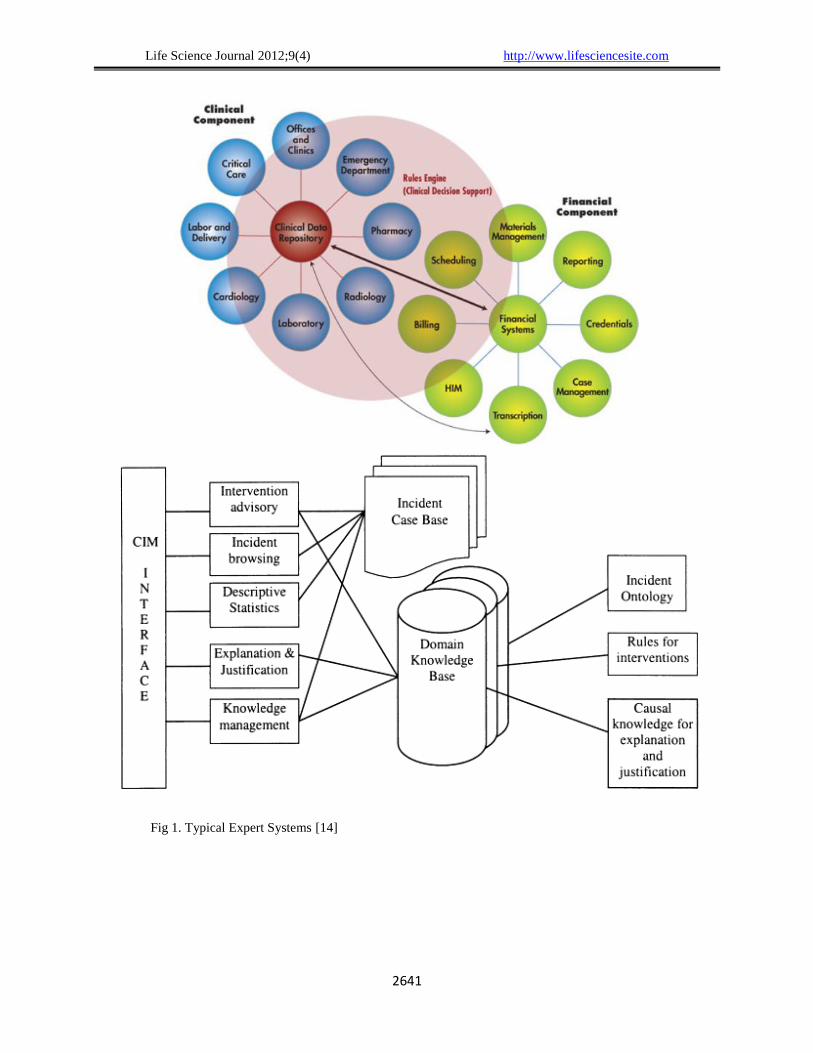
Typical examples of clinical expert systems are
exhibited in Figure 1.
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2641
Fig 1. Typical Expert Systems [14]

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2642
2.3. Case-Based Reasoning (CBR)
Case-based reasoning (CBR), comprehensively
understood, is the way toward taking care of new
issues in light of the arrangements of comparative past
issues. An auto technician who settles a motor by
reviewing another auto that showed comparable side
effects is utilizing case-based thinking. A legal advisor
who advocates a specific result in a trial in view of
lawful points of reference or a judge who makes case
law is utilizing case-based thinking. In this, too, a
designer replicating working components of nature
(honing bio-mimicry), is regarding nature as a database
of answers for issues. Case-based thinking is an
unmistakable sort of similarity making [18,19].
It has been contended that case-based thinking is
an intense strategy for PC thinking, as well as an
unavoidable conduct in regular human critical thinking;
or, all the more drastically, that all thinking depends on
past cases by and by experienced. This view is
identified with model hypothesis, which is most
profoundly investigated in psychological science [20-
22].
Case-based thinking has been formalized for
motivations behind PC thinking as a four-stage
process[23]:
Recover: Given an objective issue, recover from
memory cases pertinent to settling it. A case comprises
of an issue, its answer, and, normally, comments about
how the arrangement was inferred. For instance,
assume Fred needs to get ready blueberry flapjacks.
Being a beginner cook, the most important experience
he can review is one in which he effectively made plain
hotcakes. The strategy he took after for making the
plain hotcakes, together with supports for choices made
en route [24].
Reuse: Map arrangement from past case to
objective issues. This might include adjusting
arrangement as expected to fit the new circumstance. In
the flapjack illustration, Fred must adjust his recovered
answer for incorporate the expansion of blueberries.
Reconsider: Having mapped the past answer for
the objective circumstance, test the new arrangement in
this present reality (or a reproduction) and, if essential,
change. Assume Fred adjusted his flapjack
arrangement by adding blueberries to the player. In the
wake of blending, he finds that the player has turned
blue, an undesired impact. This recommends the
accompanying amendment: defer the expansion of
blueberries until after the player has been scooped into
the container [25].
Hold: After arrangement has been effectively
adjusted to objective issue, store subsequent experience
as another case in memory. Fred, as needs be, records
his recently discovered strategy for making blueberry
flapjacks, in this manner improving his arrangement of
put away encounters, and better setting him up for
future hotcake making requests. The average Case
Base Reasoning is shown in Figure 2.
3.Computer-Interpretable Guidelines
Clinical rules are suggestions on the fitting
treatment and care of individuals with particular
maladies and conditions. Clinical rules depend on the
best accessible confirmation. There is an arrangement
of components that rule scientists might want to see
rules get [26]. The goal of scientists is to change the
static and uninvolved nature of rules. Clinical rules
assume diverse parts in the clinical procedure: for
instance, they can be utilized to bolster doctors in the
treatment of sicknesses, or for scrutinizing, for
assessment, and for training purposes. A wide range of
systems and activities have been produced as of late
with a specific end goal to acknowledge PC helped
administration of clinical rules [27,28].

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2643
Fig 2. Typical Case Based Reasoning system [31]
4. Clinical Expert Systems
4.1. What are Clinical Expert Systems?
Clinical expert systems help human experts in
their work; be that as it may, they don't supplant their
insight and abilities. Basic components of these
systems that are intended to give quiet particular
direction incorporate the learning base (e.g., ordered
clinical data on analyses, sedate associations, and
rules), a program for joining that learning with patient-
particular data, and a correspondence instrument—at
the end of the day, a method for entering tolerant
information into the application and giving significant
data (e.g., arrangements of conceivable judgments,
tranquilize connection alarms, or preventive care
updates) back to the clinician [29,30].
Expert systems could be actualized utilizing an
assortment of stages (e.g. web based, neighbourhood
PC, organized EMR, or a handheld gadget).
Additionally, an assortment of figuring methodologies
can be utilized. These methodologies may rely on upon
whether the expert's systems is incorporated with the
neighbourhood EMR, whether current information is
accessible from focal archive or whether whole
framework is housed outside neighbourhood site and is
gotten to, yet not fused into neighbourhood EMR. On a
fundamental level, any sort of expert's systems could
use any of these basic computational models,
techniques for get to, or gadgets. The decisions among
these components may depend more on the kind of
clinical systems as of now set up, merchant offerings,
work process, security, and monetary limitations than
on the sort or reason for the experts systems [31-33].
4.2. Significance of Clinical Expert Systems
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2644
Clinical expert's systems are methodically created
articulations to help medicinal services experts and
patients about clinical conditions [34]. At first, rules
are just in light of the agreement of gatherings of
specialists; however with the development of
confirmation based clinical practice, different methods
are incorporated into rule improvement. The Delphi
and Ostensible gathering strategies are a portion of the
procedures that are later incorporated into the
improvement procedure are still utilized today.
Presently, clinical expert systems advancement is
focused on around a broad research of the writing and
exhaustive examination of experimental proof. The
procedure typically begins with the decision of the rule
theme or subject, in light of the issues that persuade the
advancement. Clinical rules can be created to an
extensive variety of subjects and clinical territories,
including wellbeing conditions bound to illnesses and
efficient expenses. To pick the subject, it is important
to do a preparatory check of the accessible
confirmation keeping in mind the end goal to find out
the legitimacy of the topic [35-38].
A large number of the innovation contrasts
depicted in the past few decades. The accompanying
elements might be more pertinent to clinician client /
helping in execution:
(1) Essential needs or issue and objective territory
of look after which experts is being considered (e.g.,
enhance general productivity, distinguish ailment early,
guide in precise analysis or convention based
treatment, or avoid hazardous antagonistic occasions
influencing the patient);
(2) Main choice is whether experts could consider
need or issue distinguished patient from others [40-43].
Experts can give support to clinicians at different
stages in the care procedure, from preventive care
through determination and treatment to checking and
development. Experts as actualized today could
incorporate, for instance, arrange sets custom-made for
specific conditions or sorts of patients (preferably in
light of confirmation based rules and tweaked to reflect
individual clinicians' inclinations), access to rules and
other outside databases that can give data applicable to
specific patients, updates for preventive care, and
alarms about conceivably perilous circumstances that
should be addressed[44,45].
The most well-known utilization of experts is for
tending to clinical needs, for example, guaranteeing
exact findings, and screening in a convenient way for
preventable sicknesses, or turning away unfriendly
medication occasions. In any case, experts can likewise
conceivably bring down expenses, enhance
productivity, and decrease understanding burden. Truth
be told, experts can now and then address each of the
three of these ranges at the same time. For instance, by
alarming clinicians to possibly duplicative testing. For
more mind boggling intellectual assignments, for
example, demonstrative basic leadership, the point of
experts is to help, as opposed to supplant, the clinician
though for different errands, the experts may calm
clinician of the weight of remaking requests for every
experience. The experts may offer proposals, yet
clinician must channel data, survey recommendations,
& choose whether make a move / what move to make?
[46,47].
4.3 Expert's Impact
Current area concentrates on assessments of the
effect of experts on human services quality, utilizing
Donabedian's great meaning of value including
structure, process, and results of medicinal services.
Donabedian upheld that authoritative results, for
example, cost and productivity, and in addition
singular patient wellbeing results, be assessed.
Donabedian's model is extended via Carayon and her
associates' plan of structure, which incorporates
individuals, association, innovations, assignments, and
environment. This extended meaning of structure is
utilized here with the goal that experts affect on cost
and productivity are tended to and included as a major
aspect of effect on structure [48,49]. As delineated
underneath, assessment of effect incorporates mind
process and patient wellbeing results. Basic results are
likewise tended to beneath.
Most distributed assessments of the effect of
experts on medicinal services quality have been
directed in inpatient as opposed to mobile settings, and
most have been in huge scholarly therapeutic focuses,
frequently utilizing "homegrown" systems, where there
is a culture that is acclimated to their utilization and
satisfactory assets (counting ability, time, and
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2645
foundation) to fabricate and look after them. Albeit
numerous business EMRs have expert's capacities,
there has been minimal orderly research on the results
or even on the execution procedures of business
experts in group settings. These oversights, and the
restricted concentration in charge of them, are
especially risky since most doctors' facilities will send
business systems later on, and their way of life and
assets are probably going to vary from those of
expansive scholastic therapeutic focuses. Moreover, the
effect of experts in mobile settings needs more
consideration. A portion of the undertakings inside the
AHRQ Ambulatory Safety and Quality Program are
starting to address this need [50-52].
The exploration on experts has other critical
confinements. To start with, in spite of the fact that
various experts' suggestions have been distributed,
similarly, most research has inspected impacts of
experts on the procedure of care (as opposed to the
results or structure) and has concentrated principally on
clinician basic leadership. Finally, indicative projects
have had restricted use by and by settings. At last, after
effects of examination to date are blended as far as
viability of experts for specific conditions or specific
sorts of experts. These impediments indicate holes in
the writing. In spite of the fact that RCTs are viewed as
the best quality level for research concentrates on,
subjective studies might be better ready to decide why
experts mediation succeeds or comes up short [53].
The accompanying area audits the after effects of
RCT studies and different investigations of experts.
Since the greater part of studies manage process and
patient wellbeing results, these viewpoints is talked
about initially, trailed by an exchange of structure [54].
4.4 Impact on Care Process and Patient Health
Outcomes
The meta-investigations of alarms and updates for
choice support have been genuinely reliable in
demonstrating that they can change clinician basic
leadership and activities, diminish drug blunders, and
advance preventive screening and utilization of proof
based proposals for pharmaceutical solutions. The
information on how those choices influence tolerant
results are more restricted, in spite of the fact that
various studies have demonstrated beneficial outcomes.
By and large, the outcomes demonstrate the capability
of experts to enhance the nature of care [55,56].
In spite of the fact that the studies demonstrating
the capacity of experts to anticipate prescription
mistakes (off base choices) have been reliably positive,
the consequences of research studies on the capacity of
experts to turn away unfavourable medication
occasions (mischief to the patient) have had a tendency
to be blended. Few of the studies looking at the effect
on wellbeing results are RCTs, many studies are
ineffectively outlined, and not all studies indicated
factually critical impacts. Expert's concentrates on that
concentrate on giving analytic choice support have
likewise demonstrated blended results, and less of
these systems have been assessed practically speaking
settings. In any case, contemplates contrasting experts
demonstrative proposals and experts clinicians'
examinations of testing clinical cases have
demonstrated that the symptomatic experts can help
even experts doctors to remember conceivably
imperative analyses they didn't at first consider [57,58].
A portion of the blended results have come about
because of methodological issues, for example, roof
impacts (execution is as of now great preceding
actualizing experts) or low factual energy to recognize
measurably.
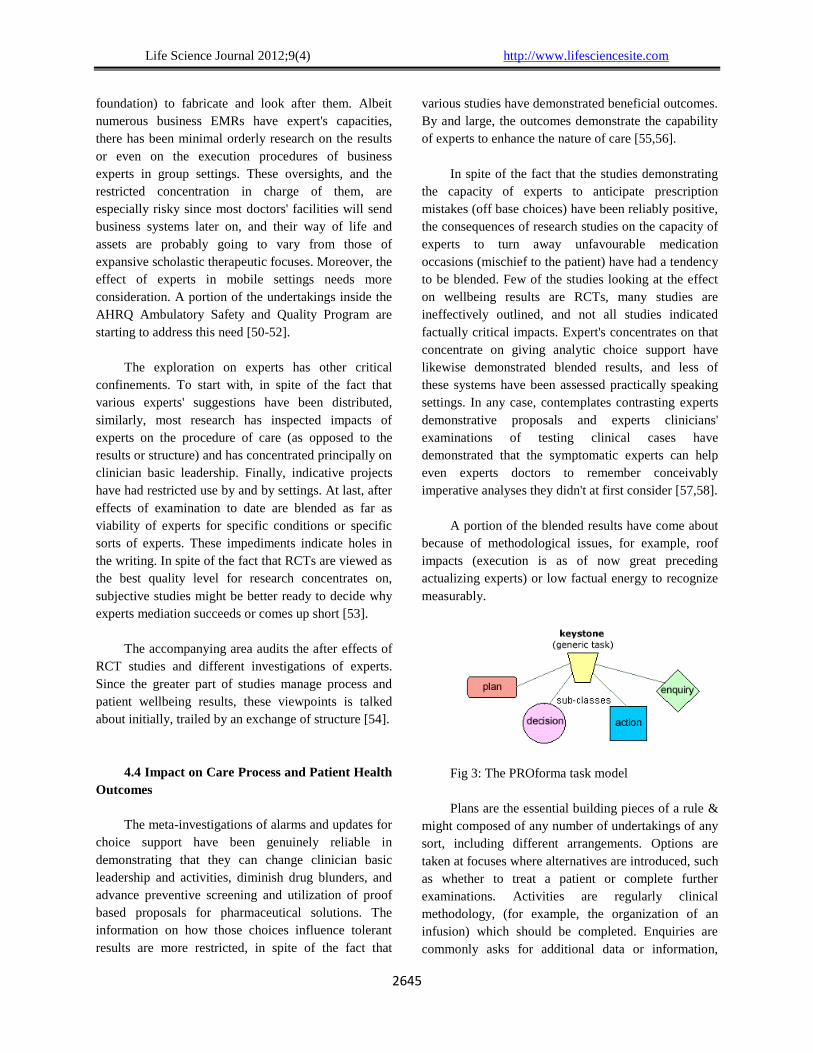
Fig 3: The PROforma task model
Plans are the essential building pieces of a rule &
might composed of any number of undertakings of any
sort, including different arrangements. Options are
taken at focuses where alternatives are introduced, such
as whether to treat a patient or complete further
examinations. Activities are regularly clinical
methodology, (for example, the organization of an
infusion) which should be completed. Enquiries are
commonly asks for additional data or information,

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2646
required before the rule can continue. PROforma
programming comprises of a graphical editorial
manager to bolster the creating procedure, and a motor
to execute the rule particular. The motor can likewise
be utilized as an analyzer amid the application
improvement stage. A PROforma editorial manager
bolsters the development of a rule as far as the four
undertaking sorts. Utilizing the symbols appeared as a
part of the outline, systems of errands can be created
that speak to arrangements or strategies did after some
time. In the manager, legitimate and worldly
connections between assignments are caught normally
by connecting them as required with bolts. Any
procedural and restorative learning required by the rule
all in all or by an individual assignment is entered
utilizing formats connected to every errand. The
subsequent populated graphical structure is naturally
changed over into a database prepared for execution
[85-86].
4. 5. GLARE
GLARE stands for Guide Line Acquisition,
Representation and Execution. Following an analysis
of some of the existing expert systems, it is observed
that this area of research is still fresh. Due to these
various shortcomings, none of the models is largely
adopted by the health informatics community. The
level of complexity is another issue to be addressed
[87]. Table 1 presents an up-to-date review of the
existing expert systems.
The maintenance and library partitions possess
administrative information about the guideline, namely
authoring and version number. The constructs of the
maintenance partition are title, (file) name, author,
version, institution, date of last modification and
validation status. The validation status contains
information about the approval of the guideline in a
local institution and it may have three possible values:
testing, research, production and expired. The
transition from testing to production means a shift of
responsibility from the institution that developed the
MLM to the local institution where the guideline will
be applied. The library compartment contains
constructs used for a detailed description of the
guideline and among them the attribute purpose
enables the expression of the medical objective of the
MLM [88].
The main constructs of the knowledge
compartment are data, evoke, logic and action. The
data construct is used to obtain the values of the
concepts referred in the MLM from the information
system of the healthcare institution. The evoke
construct contains the events that execute MLM and
such events are related with the medical parameters in
data. The decision criteria are expressed in the logic
construct through if-then-else rules and sets of logical,
mathematical and temporal operators. When a rule is
assessed to the value true, a given procedure of the
construct action is proposed. These procedures may
include messages/alerts or the execution of other
MLMs. This approach reveals great modularity and
gives transparency to the decision making process, but
given its simplicity, the ability to capture the full
content of a medical guideline is compromised. Arden
Syntax is mainly used in alert and monitoring systems,
like the ones provided by the Regenstrief Institute. It is
defined in Backus-Naur Form (BNF), a notation
technique used to describe the syntax of computation
languages. Currently the development of Arden Syntax
by HL7 is based on XML [89,90].

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2650
Table 1 Existing Expert Systems for clinical guideline development
5. Proposed Clinical Expert System
An expert system is a program that prevails upon
information of some experts with a view to taking care
of issues or giving exhortation. The way toward
building expert system is frequently called information
designing. The learning designer is included with all
parts of a specialist framework. Building expert system
is for the most part an iterative procedure. The parts
and their association will be refined through the span of
various gatherings of the information build with the
experts and clients system. A general structure of the
proposed expert system is exhibited in Figure 4.
Fig 4. Proposed Expert System’s Structure
5.1 Knowledge
Hence, we established the following knowledge
acquisition procedure with the assistance of our expert
(a physician).
Examine all guidelines to be implemented and create
variable nodes. Most of the time an inclusion,
exclusion criterion would generate a node itself.
Complex criteria could be broken down to simpler
random variables. Superficial variables can also be
created that will act as intermediate nodes to combine
related variables. Find all the common nodes to
Expert Systems Features Decision
Model
Standards adopted
AAPHelp
MYCIN
Rule based
Decision support system
(DSS)
Bayesian
approach
Rule based
No
XML
EMYCIN
DSS
Rule-based
PUFF
GLIF
Decision based on
patient condition
Event-based
and rule-based
RDF,HL7
PIP
Query, plan, decision,
Rule-based
UMLS
PROforma Context based decision Event based XML,
GLARE
Query based decision
Rule-based
XML,
ICD-9
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2652
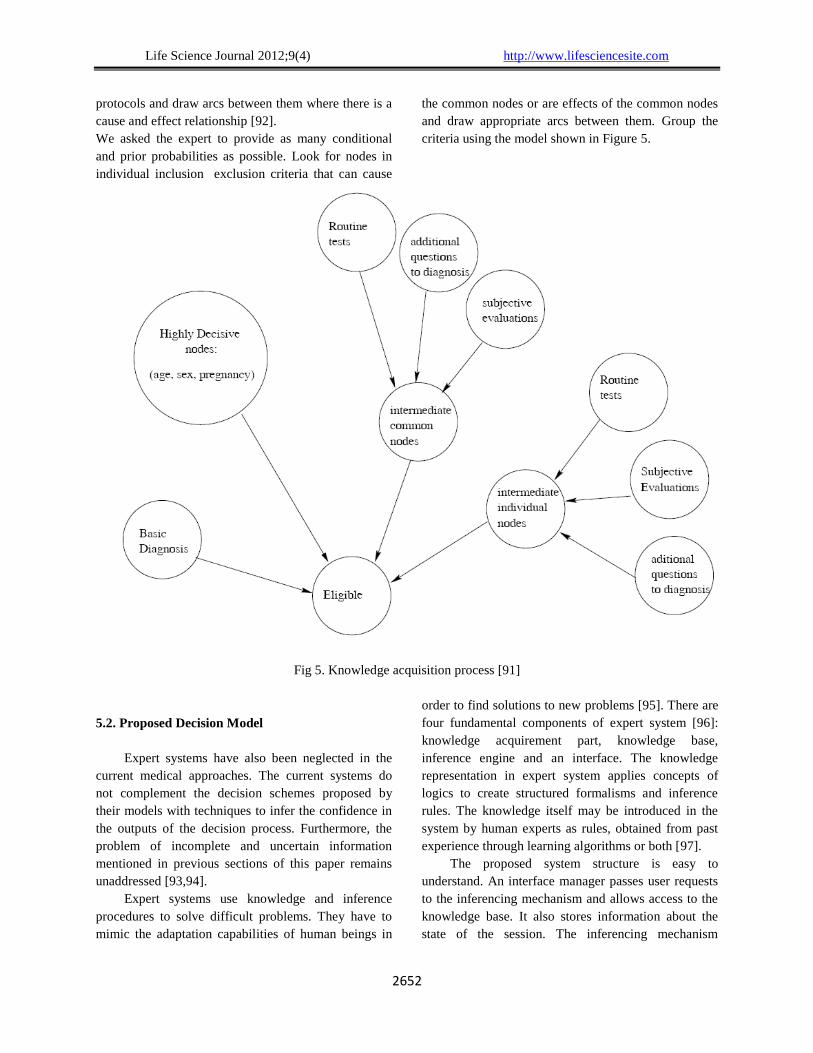
protocols and draw arcs between them where there is a
cause and effect relationship [92].
We asked the expert to provide as many conditional
and prior probabilities as possible. Look for nodes in
individual inclusion�exclusion criteria that can cause
the common nodes or are effects of the common nodes
and draw appropriate arcs between them. Group the
criteria using the model shown in Figure 5.
Fig 5. Knowledge acquisition process [91]
5.2. Proposed Decision Model
Expert systems have also been neglected in the
current medical approaches. The current systems do
not complement the decision schemes proposed by
their models with techniques to infer the confidence in
the outputs of the decision process. Furthermore, the
problem of incomplete and uncertain information
mentioned in previous sections of this paper remains
unaddressed [93,94].
Expert systems use knowledge and inference
procedures to solve difficult problems. They have to
mimic the adaptation capabilities of human beings in
order to find solutions to new problems [95]. There are
four fundamental components of expert system [96]:
knowledge acquirement part, knowledge base,
inference engine and an interface. The knowledge
representation in expert system applies concepts of
logics to create structured formalisms and inference
rules. The knowledge itself may be introduced in the
system by human experts as rules, obtained from past
experience through learning algorithms or both [97].
The proposed system structure is easy to
understand. An interface manager passes user requests
to the inferencing mechanism and allows access to the
knowledge base. It also stores information about the
state of the session. The inferencing mechanism

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2652
requests the hypergraph manager, which builds the
hypergraphs it needs. The classes that make up these
subsystems are all constructed from a number of basic
classes, such as linked lists, hash tables and matrices.
The proposed expert system is not composed
purely and simply of classes, but of collections of
classes that form sub-systems. The separate subsystems
could be altered internally without affecting the others,
as long as their interface to those others is unchanged.
The interfaces evolve quickly as the user demands new
features. However, if the interfaces are kept small the
efforts of change management is localized [98].
The system is not hierarchical in the sense that a
structured program is. Although the interface manager
could be described as a top level function, it performs
many functions and these may be changed. Hence, the
proposed expert system is exhibited in Figure 3.
This loose and simple organization would not
have resulted from a top-down procedure-oriented
methodology. It is therefore, possible to remove any
subsystem and replace it. For example, the Hypergraph
Manager and Inferencing Mechanism could be
removed and replaced with an ordinary backtracking
mechanism [99].
A new Interface Manager could be designed and
fitted onto the rest of the system, without changing
other subsystems. It has made the production of
successive versions easy. Strength of the system is that
it produced classes which could be reused in other
applications, almost as a side effect. Knowledge base
and interface classes might be reusable in other
applications. These properties mean that successive
versions of the system could be developed without
having to start from scratch. This is important because
new demands from users continually arise from their
experience with the system. Additionally, object-
oriented programming languages prefer to procedural
languages because they have inheritance mechanisms.
Inheritance allows one class to include another as part
of its definition. Unwanted plans could be over fitted
and new parameters could be added. The inheriting
class is known as the subclass and the parent class the
super class. A super class may be virtual i.e. it cannot
be used to create objects, as it does not fully defined
one. It serves only as a repository for definitions and
codes that subclasses share.
This decision model leaves the door open for
further research on the complementarily that other
techniques that manage uncertainty, namely Bayesian
Networks, Dempster-Shafer Theory and fuzzy Logic,
may offer to the QoI, since they manage uncertainty in
different ways. The implementation of such a decision
model is essential in order to capture context of the
execution of guidelines and provide measures of
confidence in the outputs [100].
The development of such a decision model is but
a step in the construction of a wider decision platform,
represented in Fig. 6, where healthcare professionals,
members of the same medical team, possibly dispersed
across different locations, can discuss de case of a
patient in the context of an intelligent environment.
Through the use of AI techniques it is possible to
perceive information about the state of stakeholders,
namely their attitudes and emotions and thus determine
the type of interaction they are developing. If one
throws into the equation relevant knowledge, from
exterior sources, concerning the health condition (that
is the object of the discussion) and guideline
recommendations, a group decision environment is
established for healthcare professionals to discuss if a
guideline is suitable for the situation at hand and
mediate/negotiate solutions. Having all this
information enables the medical team, in cases of non-
compliance of guidelines, to build new strategies and
adapt their content to maximize the probability of a
successful treatment.

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2653
Fig 6. Decision model for the execution of clinical guidelines in proposed Expert System.
The development of such a decision model is but a
step in the construction of a wider decision platform,
represented in Fig. 3, where healthcare professionals,
members of the same clinical team, possibly
dispersed across different locations, can discuss de
case of a patient in the context of an intelligent
environment [101].
Through the use of AI techniques it is possible
to perceive information about the state of
stakeholders, namely their attitudes and emotions and
thus determine the type of interaction they are
develop knowledge, from exterior sources,
concerning the health condition (that is the object of
the discussion) and guideline recommendations, a
group decision environment is established for
healthcare professionals to discuss if a guideline is
suitable for the situation at hand and
mediate/negotiate solutions. Having all this
information enables the clinical team, in cases of
non-compliance of guidelines, to build new strategies
and adapt their content to maximize the probability of
a successful treatment [102-103].
6. Conclusion
There are several benefits of using expert
systems to assist healthcare professionals in order to
cure patients. Initially, systems knowledge is
autonomic. Thus, healthcare professionals do not
need to put enough efforts, labour in constructing and
knowledge base updating. When constructing or
maintaining the knowledge source, the only desired
action is to train the model with data. Secondly, the
extracted knowledge is the real world better. Hence,
this paper has presented decision support system to
help healthcare professionals for efficient clinical
treatment. This is an ongoing research line with
several experts working on the implementation of
useful expert systems and the development of
execution engines.
It is also observed that there is a need for a
decision model that addresses the aspects of the
contextualization of guideline execution and the
handling of incomplete and uncertain information.
However, opinions of healthcare professionals have
their own worth and should be included in the whole
process of development of knowledge base of the
expert system. Additionally, one of the current issues
of the guidelines is that they are too rigid and do not
give space for innovation and change. This decision
model of the expert systems should be flexible to
incorporate up-to-date changes.
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2654
References
1. Gardner R, Pryor T, Warner H (1999). The HELP
hospital information system: update 1998. Int J of Med
Inform, 54(3), 169-182.
2. Gruber T (1993). A translation approach to portable
ontologies. Knowl Acquis 5(2):199-220.
3. Abbod M, von Keyserlingk D, Linkens D, Mahfoul M
(2001) Survey of utilization of fuzzy technology in
Medicine and Healthcare. Fuzzy Sets Syst 120:331-349
4. Haron, H. Rehman, A. Wulandhari, L.A. and Saba, T.
(2011) Improved Vertex Chain Code Algorithm for
Curve Length Estimation‖ Journal of Computer Science,
vol. 7(5): 736-743. doi: 10.3844/jcssp.2011.736.743
5. Chawla A, Gunderman R (2008) Defensive medicine:
prevalence, implications, and recommendations. Acad
Rad 15 (7): 948-9
6. Househ M, Kushniruk A, Maclure M, Carleton B,
Cloutier-Fisher D (2011) The use of conferencing
technologies to support drug policy group knowledge
exchange processes: An action case approach. Inter J
Med Inform 80: 251-261
7. Hripcsak G (1994) Writing Arden Syntax clinical logic
modules. Comput Biol Med 24(5): 331-363.
8. Kurniawan, F. Rahim,MSM, Daman, D. Rehman, A.
Mohamad, D. and Mariyam, S. (2011). Region-based
Touched Character Segmentation in Handwritten Words.
International Journal of Innovative Computing,
Information and Control vol. 7(6), 3107-3120.
9. Kurniawan, F. Rehman, A. Mohamad, D. (2009a). From
Contours to Characters Segmentation of Cursive
Handwritten Words with Neural Assistance. IEEE
International Conference on Instrumentation,
Communications, Information Technology and
Bioclinical Engineering (ICICI-BME), 12-18.
10. Karacapilidis N, Pappis C (1997) A framework for
group Expert systems: Combining AI tools and OR
techniques. Eur J Oper Res 103: 373-388.
11. Bichindarits I, Marling C (2006) Case-based reasoning
in health sciences: What’s next? Artif Intell Med 36:
127-135
12. Bodenreider O (2006) The Unified Clinical Language
System (UMLS): integrating bioclinical terminology.
Nucleic Acids Res 32: 267-270
13. Bottrighi A, Terenziani P, Montani S, Torchio M,
Molino G (2006) Clinical guidelines contextualization in
GLARE. AMIA Annu Sympos Proc: p 860
14. Novais P, Carneiro D, Gomes M, Neves J (2012). Non-
invasive Estimation of Stress in Conflict Resolution
Environments. In Demazeau Y, Müller J, Corchado J,
Bajo J (eds.) Advances on Practical Applications of
Agents and Multi-Agent Systems - 10th International
Conference on Practical Applications of Agents and
Multi-Agent Systems (PAAMS 2012) Springer - Series
Advances in Intelligent and Soft Computing, vol 155, pp
153-160
15. Boxwala A, Peleg M, Tu S, Ogunyemi O, Zeng Q,
Wang D, Patel V, Greenes R, Shortliffe E (2004) GLIF3:
a representation format for sharable computer-
interpretable clinical practice guidelines. J Biomed
Inform 37: 147-161
16. Fox J, Black R, Chronakis I, Dunlop R, Patkar V, South
M, Thomson R (2008) From Guidelines to Careflows:
Modelling and Supporting Complex Clinical Processes.
In: Teije A, Miksch S, Lucas P (eds) Computer-based
Clinical Guidelines and Protocols: A Primer and Current
Trends. IOS Press, Amsterdam, pp 44-62
17. Melle W (1978) MYCIN: a knowledge-based
consultation program for infectious disease diagnosis.
Int J Man-Mach Stud 10(3): 313-322.
18. Cheater F, Closs S (1997). The effectiveness of methods
of dissemination and implementation of clinical
guidelines: a selective review. Clin Eff Nurs 1: 4-15
19. Seto E, Leonard K, Cafazzo J, Barnsley J, Masino C,
Ross H (2012) Developing healthcare rule based expert
systems: Case study of a heart failure telemonitoring
system. Inter J Med Inform.
doi:10.1016/j.ijmedinf.2012.03.001.
20. Saba, T. and Rehman, A.(2012). Effects of Artificially
Intelligent Tools on Pattern Recognition, International
Journal of Machine Learning and Cybernetics. DOI:
10.1007/s13042-012-0082-z.
21. Bradburn C, Zeleznikow J (1994) The application of
case-based reasoning to the tasks of health care
planning. In: Wess S, Althoff K, Richter M (eds) Topics
in case-based reasoning: first European Workshop,
EWCBR-93. Springer-Verlag, Berlin pp 365-78
Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2655
22. Bekhti, S. Rehman, A. Al-Harbi, M., Saba, T. (2011).
AQuASys An Arabic Question-Answering System based
on Extensive Question Analysis and Answer Relevance
Scoring. Information and Computation International
Journal of Academic Research, 3(4): 45-54.
23. Schalkoff R (1990) Artificial Intelligence: an
engineering approach. McGraw-Hill, New York.
24. Bratko I, Mozetiec I, Lavraec N (1989) KARDIO: A
study in deep and qualitative knowledge for ESs. MIT
Press, Cambridge
25. Elkin P, Peleg M, Lacson R, Bernstam E, Tu S, Boxwala
A (2000) Toward standardization of electronic guideline
representation. MD Comput 17(6): 39-44
26. Fox J, Alabassi A, Patkar V, Rose T, Black E (2006) An
ontological approach to modelling tasks and goals.
Comput Biol Med 36: 837–856
27. Isern D, Sánchez D, Moreno A (2011) Ontology-driven
execution of clinical guidelines. Comput Methods Prog
Biomed. doi: 10.1016/j.cmpb.2011.06.006
28. Jackson P (1990) Introduction to ESs. Addison-Wesley
Longman Publishing, Boston
29. Kaiser K, Miksch S (2009) Versioning computer-
interpretable guidelines: Semi-automatic modelling of
„Living Guidelines‟ using an information extraction
method. Artif Intell Med 46(1): 55-66.
30. Kalra J (2004) Clinical errors: an introduction to
concepts. Clinical biochemistry 37 (12): 1043-51.
31. Kavanagh B (2009) The GRADE System for Rating
Clinical Guidelines. PLoS Med 6 (9): 5.
32. Konglingren L (2009) HL7: Health Level Seven.
Interface:1-23
33. Koton P (1988) Reasoning about evidence in causal
explanations. In: Mitchell T, Smith R (eds). Proc AAAI-
88. AAAI Press, Menlo Park, 256-61.
34. Clark D (1990) Numerical and symbolic approaches to
uncertainty in AI. Artif Intell Rev 4: 109- 146.
35. Codish, S, Shiffman R (2005) A Model of Ambiguity
and Vagueness in Clinical Practice Guideline
Recommendations. AMIA Annu Symp Proc: pp 146-150
36. Johnson C, Turley J (2006) The significance of cognitive
modeling in building healthcare interfaces. Int J Med
Inform 75: 163-172.
37. de Clercq P, Blom J, Korsten H, Hasman A (2004)
Approaches for creating computer-interpretable
guidelines that facilitate decision support. Artif Intell
Med 31(1): 1-27
38. Haron, H. Rehman, A. Adi, DIS, Lim, S.P. and Saba,
T.(2012). Parameterization Method on B-Spline Curve.
Mathematical Problems in Engineering, 2012,
doi:10.1155/2012/640472.
39. Dennis S, Edwards S, Partridge M, Pinnock H, Qureshi
S (2004) The dissemination of the British guideline on
the management of Asthma. Respir Med 98: 832-837.
40. Elarbi-Boudihir, M. Rehman, A.(2011), T.Saba. Video
Motion Perception Using Operation Gabor Filter‖.
International Journal of Physical Sciences,6(12): 2799-
2806.
41. Saba, T. Rehman, A. and Elarbi-Boudihir, M. (2011b).
Methods and Strategies on off-line Cursive Touched
Characters Segmentation: A Directional Review.
Artificial Intelligence Review DOI 10.1007/s10462-011-
9271-5.
42. Samwald M, Fehre K, Bruin J, Adlassnig K-P (2012)
The Arden Syntax standard for clinical decision support:
Experiences and directions. J Biomed Inform.
doi:10.1016/j.jbi.2012.02.001
43. Schadow G, Mead C, Walker D (2006) The HL7
reference information model under scrutiny. Stud Health
Technol Inform 124: 151-156.
44. Schalkoff R (1990) Artificial Intelligence: an
engineering approach. McGraw-Hill, New York.
45. Shenoy P, Shafer G (1986) Propagating belief functions
with local computations. IEEE Expert 1(3): 43-52.
46. Shiffman R, Karras B, Agrawal A, Chen R, Marenco L,
Nath S (2000) GEM: a proposal for a more
comprehensive guideline document model using XML. J
Am Med Inform Assoc (5):488-498.
47. Aamodt A, Plaza E (1994) Case-Based Reasoning:
Foundational Issues, Methodological Variations, and
SystemApproaches. AI Commun 7(1): 39-59
48. Antoniou G, Harmelen F (2009) Web Ontology
Language: OWL. In: Staab S, Studer R (eds) Handbook
on Ontologies. Springer Heidelberg, Berlin, pp 91-110
49. Novais P, Salazar M, Ribeiro J, Analide C, Neves J
(2010) Decision Making and Quality-of- Information.
In: Corchado E, Novais P, Analide C, Sedano J (eds)
Soft Computing Models in Industrial and Environmental
Applications, 5th International Workshop (SOCO 2010).

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2656
50. Springer - Series Advances in Intelligent and Soft
Computing vol. 73, pp 187-195
51. Oliveira T, Costa Â, Novais P, Neves J (2012) An
Interpretable Guideline Model to Handle Incomplete
Information. In: Omatu S, Paz Santana J, González S,
Jose M, Bernardos A, Corchado J (eds) Distributed
Computing and Artificial Intelligence, 9th International
52. Conference (DCAI 2012), Springer - Series Advances in
Intelligent and Soft Computing, pp: 437-444.
53. Ohno-Machado L, Gennari J, Murphy S, Jain N, Tu S,
Oliver D et al. (1998) The guideline interchange format.
J Am Med Inform Assoc: 5(4): 357-372.
54. Pearl J (1986) Fusion, propagation, and structuring in
belief networks. Artif Intell 29(3): 241-288.
55. Peleg M, Tu S, Bury J, Ciccarese P, Fox J, Greenes RA,
Hall R, Johnson PD, Jones N, Kumar A, Miksch S,
Quaglini S, Seyfang A, Shortliffe EH, Stefanelli M
(2003) Comparing computer interpretable guideline
models: a case-study approach. J Am Med Inform Assoc
10(1):52-68.
56. Bareiss R (1989) Exemplar-based knowledge
acquisition: a unified approach to concept
representation, classification, and learning. Academic
Press, San Diego.
57. Berger J (1994) Roentgen: radiation therapy and case-
based reasoning. In: O‟Leary D, Selfridge P (eds) Proc
10th Conf Artif Intell Appl. IEEE Computer Society
Press, Los Alamitos, pp 171-177.
58. Berners-Lee T, Hendler J, Lassila O (2001) The
Semantic Web. Sci Am 284(5): 34-43
59. Kurniawan, F. Rehman, A. Mohamed, D (2009b).
Contour Vs Non-Contour based Word Segmentation
from Handwritten Text Lines. An Experimental
Analysis. International Journal of Digital Content
Technology and its Applications, vol. 3(2), 127-131.
60. Logan R, Scott P (1996) Uncertainty in clinical practice:
implications for quality and costs of health care. The
Lancet 347: 595-98.
61. Mead, P. (2000) Clinical guidelines: promoting clinical
effectiveness or a professional minefield? J Adv Nurs 31
(1): 110-116.
62. Miller M, Kearney N (2004) Guidelines for clinical
practice: development, dissemination and
implementation. Int J Nurs Stud 41 (7): 813-821
63. Mohamad, I. Rahim, MSM, Bade, A. Rehman, A. and
Saba, T.(2012). Enhancement of the Refinement Process
for Surface of 3D Object. Journal of American Science.
8(4):358-365.
64. Neves J, Ribeiro J, Pereira P, Alves V, Machado J,
Abelha A, Novais P, Analide C, Santos M, Fernndez-
Delgado M (2012) Evolutionary intelligence in asphalt
pavement modeling and quality-of-information. Prog
Artif Intell 1(1): 119-135.
65. Lucas P (2004) Bayesian networks in biomedicine and
health-care. Artif Intell Med 30(3): 201-214.
66. Nikolopoulos (1997) Expert systems: Introduction to
First and Second Generation and Hybrid Knowledge
Based Systems. CRC Press, New York.
67. Dempster A (1967) Upper and lower probability
inferences based on a sample from a finite univariate
population. Biometrika 54(3-4): 515.
68. Peleg M, Wang D (2006) The Guideline Interchange
Format. Open Clinical.
http://www.openclinical.org/gmm_glif.html. Accessed
23 May 2012.
69. Perner P (1999) An architecture for a CBR image
segmentation system. Intern J Med Inform 12(6): 749-
59.
70. Quaglini S, Stefanelli M, Cavallini A, Micieli G, Facino
C, Mossa C (2000) Guideline-based careflow systems.
Artif Intell Med. 20(1): 5-22.
71. Rahim, MSM. Rehman, A. Faizal-Ab-Jabal, M., Saba, T.
(2011). Close Spanning Tree Approach for Error
Detection and Correction for 2D CAD Drawing.
International Journal of Academic Research, 3(4):
pp.525-535.
72. Rahim, MSM, Rehman, A. Sholihah, N. Kurniawan, F.
and Mohamad, D. (2012) Region-based Features
Extraction in Ear Biometrics, International Journal of
Academic Research,4(1): 37-42.
73. Ram P, Berg D, Tu S, Mansfield G, Ye Q, Abarbanel R,
et al. (2004) Executing clinical practice guidelines using
the SAGE execution engine. Medinfo 11(1):251-255.
74. Rehman, A. (2012). Machine Learning based Air Traffic
Control Strategy, International Journal of Machine
Learning and Cybernatics DOI: 10.1007/s13042-012-
0096-6.

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2657
75. Rehman, A. and Mohamad, D. (2008). A Simple
Segmentation Approach for Unconstrained Cursive
Handwritten Words in Conjunction of Neural Network.
International Journal of Image Processing, 2(3): 29-35.
76. Rehman, A. and Saba, T. (2011a). Performance Analysis
of Segmentation Approach for Cursive Handwritten
Word Recognition on Benchmark Database. Digital
Signal Processing, 21:486-490.
77. Rehman, A. and Saba, T. (2011b). Document Skew
Estimation and Correction: Analysis of Techniques,
Common problems and Possible Solutions. Applied
Artificial Intelligence, 25(9): 769-787.
78. Rehman, A. and Saba, T (2012c).Analysis of advanced
image processing to clinical and preclinical decision
making with prospectus of quantitative imaging
biomarkers, Artificial intelligence Review, pp. 1-19,
doi:10.1007/s10462-012-9335-1.
79. Rehman, A. and Saba, T (2012d) ―Neural Network for
Document Image Preprocessing‖ Artificial Intelligence
Review, DOI: 10.1007/s10462-012-9337-z.
80. Rehman, A. and Saba, T. (2012e). Features extraction
for soccer video semantic analysis: current achievements
and remaining issues Artificial Intelligence Review,
DOI: 10.1007/s10462-012-9319-1.
81. Rosenbrand K, Croonenborg J, Wittenberg J (2008)
Guideline Development. In: Teije A, Miksch S, Lucas P
(eds) Computer-based Clinical Guidelines and Protocols:
A Primer and Current Trends. IOS Press, Amsterdam: 3-
21.
82. Rosenfeld R, Shiffman R (2006) Clinical practice
guidelines: a manual for developing evidence based
guidelines to facilitate performance measurement and
quality improvement. Otolaryngol. Head Neck Surg Off
J 135:1-28
83. Ruzicka M, Svatek V (2004) Mark-up based analysis of
narrative guidelines with the Stepper tool.
84. In: Kaiser K, Miksch S, Tu SW (eds) Computer-based
support for clinical guidelines and protocols: Proc Symp
Comput Guidel Protoc. IOS Press, pp 132-136.
85. Saba, T. Sulong, G. and Rehman, A. (2011a). Document
Image Analysis: Issues, Comparison of Methods and
Remaining Problems. Artificial Intelligence Review,
35(2):101-118, DOI: 10.1007/s10462-010-9186-6.
86. Seto E, Leonard K, Cafazzo J, Barnsley J, Masino C,
Ross H (2012) Developing healthcare rule based expert
systems: Case study of a heart failure telemonitoring
system. Inter J Med Inform.
doi:10.1016/j.ijmedinf.2012.03.001
87. Seyfang A, Martinez-Salvador B, Serban R, Wittenberg
J, Miksch S, Marcos M (2007)
88. Maintaining formal models of living guidelines
efficiently. In: Bellazzi R, Abu-Hanna A, Hunter J (eds)
AIME '07 Proc 11th Conf Artif Intell Med. Springer-
Verlag, Berlin, pp 441-445.
89. Shahar Y, Miksch S, Johnson P (1998) The Asgaard
project: a task-specific framework for the application
and critiquing of time-oriented clinical guidelines. Artif
Intell Med 14(1-2): 29-51.
90. Shahar, Y, Young O, Shalom E, Mayaffit A, Galperin,
M, Moskovitch R, Hessing A (2004) A framework for a
distributed, hybrid, multiple-ontology clinical-guideline
library, and automated guideline-support tools. J Med
Inform 37: 325-344.
91. Shortliffe E (1984) The adolescence of AI in medicine:
will the field come of age in the '90s? Artif Intell Med
5(2): 93-106
92. Sonnenberg F, Hagerty C (2006) Computer-Interpretable
Clinical Practice Guidelines. Methods Inf Med 45(1):
145-158.
93. Sordo M, Ogunyemi O, Boxwala A, Greenes R (2003)
Descriprion Status Update on GELLO: a Proposed
Standardized Object-Oriented Expression Language for
Clinical Decision Support. Stud Health Technol Inform
107: 164-168
94. Sutton D, Fox J (2003) The syntax and semantics of the
PROforma guideline modeling language. J Am Med
Inform Assoc 10: 433–443.
95. Straszecka E (2004) Clinical Knowledge Representation
in Terms of IF-THEN Rules and the Dempster-Shafer
Theory. In: Rutwoski L, Siekmann J, Tadeusiewicz R,
Zadeh L (eds) Artificial Intelligence and Soft Computing
- ICAISC 2004. Springer, Berlin, pp 1056- 1061.
96. Susskind R (1987) Expert Systems in Law: A
Jurisprudential Inquiry. Clarendon Press, Oxford.
Thomson P (2000) Implementing evidence-based health
care: the nurse teachers‟ role in supporting the

Life Science Journal 2012;9(4) http://www.lifesciencesite.com
2658
dissemination and implementation of SIGN clinical
guidelines. Nurs Educ Today 20 (3): 207-217.
97. Thomson R, Lavender M, Madhok R (1995) How to
ensure that guidelines are effective. BMJ 311:237-242.
98. Tu S, Campbell J, Glasgow J, Nyman M, McClure R,
McClay J, et al. (2007) The SAGE Guideline Model:
Achievements and Overview. J Am Med Inform Assoc
14(5): 589–598.
99. van Gerven M, Taal B, Lucas P (2008) Dynamic
Bayesian networks as prognostic models for clinical
patient management. J Biomed Inform 41: 515-529.
100. Vetternlein T, Mandl H, Adlassnig K-P (2010) Fuzzy
Arden Syntax: A fuzzy programming language for
medicine. Artif Intell Med 49: 1-19.
101. Votruba P, Miksch S, Kosara R (2004) Facilitating
knowledge maintenance of clinical guidelines and
protocols. In: Fieschi M, Coiera E, Li Y-CC (eds) Proc
Medinfo 2004 World Congr Med Inform, AMIA. IOS
Press, San Francisco, p. 5761.
102. Wang D, Peleg M, Tu S, Boxwala A, Ogunyemi O,
Zeng Q, et al. (2004) Design and implementation of the
GLIF3 guideline execution engine. J Biomed Inform
37(5): 305-318.
103. Weidjen T, Boivin A, Burgers J, Schuneman H, Elwyn
G (2011) Clinical practice guidelines and patient
decision aids: An inevitable relationship. J Clin
Epidemiol: 1-6
11/3/2012