exhibit d. sample letter to parents about
TRANSCRIPT
Exhibit D. Sample Letter to Parents about Neuropsychological Assessment
{Insert Letterhead}
LETTER TO PARENTS REGARDING NEUROPSYCHOLOGICAL ASSESSMENT
Dear {insert parent or guardian name} ,
Following our recent telephone conversation, this is to confirm {insert child’s name} ’s
neuropsychological assessment on {insert date and time} , at the request of {insert
attorney or other retaining party} . Please plan to be at our office for approximately 7 hours
on your appointment day. As we discussed, we may need to see {insert child’s name} for an
additional session if further testing is required.
{insert child’s name} may be curious about the assessment. Please let your child know that this
is not a typical doctor’s visit (e.g. there are no needles or medical examinations). Your child will
be asked to participate in activities that help us understand more about thinking, learning, and
remembering abilities. Your child may be asked to assemble puzzles, draw pictures, solve
problems, and similar activities.
We are located at {insert address} . Parking is located at {insert parking details}
. See attached map for office location.
On the day of your appointment, please bring copies of the following that we may keep:
1. Your child’s most recent school report card and year-end report cards for previous years.
2. Your child’s Individualized Education Plan (IEP) or other relevant school documents, if
your child has these.
3. Glasses or hearing aids if your child needs them.
4. A lunch and/or snack for yourself and your child.
Enclosed are questionnaires to be completed by {insert child’s name} ’s classroom teacher.
Please sign and complete the enclosed Consent Form for Release of School Information (see
Exhibit F, this volume) and give it and the questionnaires to the teacher along with the self-
addressed stamped envelope.
We look forward to meeting with you and {insert child’s name} . Please contact us or your
attorney should you have any further questions regarding this assessment.
Sincerely,
Exhibit E. Sample Letter to Teacher about Neuropsychological Assessment
{Insert Letterhead}
LETTER TO TEACHER REGARDING NEUROPSYCHOLOGICAL ASSESSMENT
Re: {insert child’s name}
Dear Teacher,
We have scheduled a neuropsychological assessment with your student {insert child’s name}
, as part of a neuropsychological evaluation for legal purposes requested by {insert
attorney or retaining party} , and with the consent of your student’s parents or guardian. To
help us with our assessment, could you kindly complete the enclosed forms and return them to us
as soon as possible. Your observations of {insert child’s name} will form an important part of
this assessment and we appreciate the time and effort you spend on completing these
questionnaires. Please find enclosed a Consent for Release of Information which has been signed
by the parent or guardian, and which is intended for your school’s records. The following items
are enclosed:
Consent Form for Release of School Information (see Exhibit F, this volume), signed by
the parent or guardian and to be retained by the school for your records
{insert list of questionnaires enclosed}
Thank you for your assistance in our assessment. Please do not hesitate to contact me at {insert
contact information} should you have any questions.
Sincerely,
Exhibit F. Sample Consent Form for Release of Information from School
{Insert Letterhead}
CONSENT FORM FOR RELEASE OF SCHOOL INFORMATION
I hereby authorize {insert name of school and school board}
to release any or all educational data, including information labelled “confidential” (e.g.,
achievement test results, psychoeducational assessments, speech and language reports, including
raw test data) to Dr. Smith regarding:
________________________________
Name of Child/Adolescent
___________________________________
Date
___________________________________
Signature of Parent/Guardian
___________________________________
Signature of Child (when appropriate)
___________________________________
Signature of Witness
NOTE:
This form is to be signed by the parent and
retained by the school
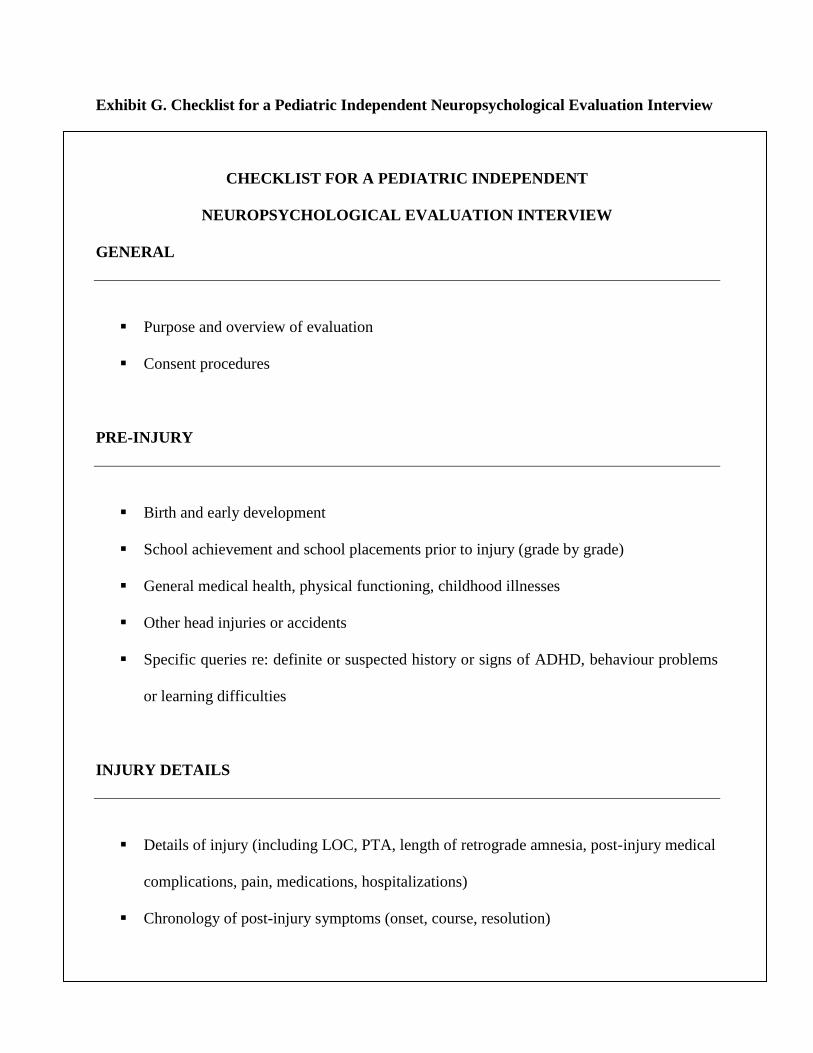
Exhibit G. Checklist for a Pediatric Independent Neuropsychological Evaluation Interview
CHECKLIST FOR A PEDIATRIC INDEPENDENT
NEUROPSYCHOLOGICAL EVALUATION INTERVIEW
GENERAL
Purpose and overview of evaluation
Consent procedures
PRE-INJURY
Birth and early development
School achievement and school placements prior to injury (grade by grade)
General medical health, physical functioning, childhood illnesses
Other head injuries or accidents
Specific queries re: definite or suspected history or signs of ADHD, behaviour problems
or learning difficulties
INJURY DETAILS
Details of injury (including LOC, PTA, length of retrograde amnesia, post-injury medical
complications, pain, medications, hospitalizations)
Chronology of post-injury symptoms (onset, course, resolution)
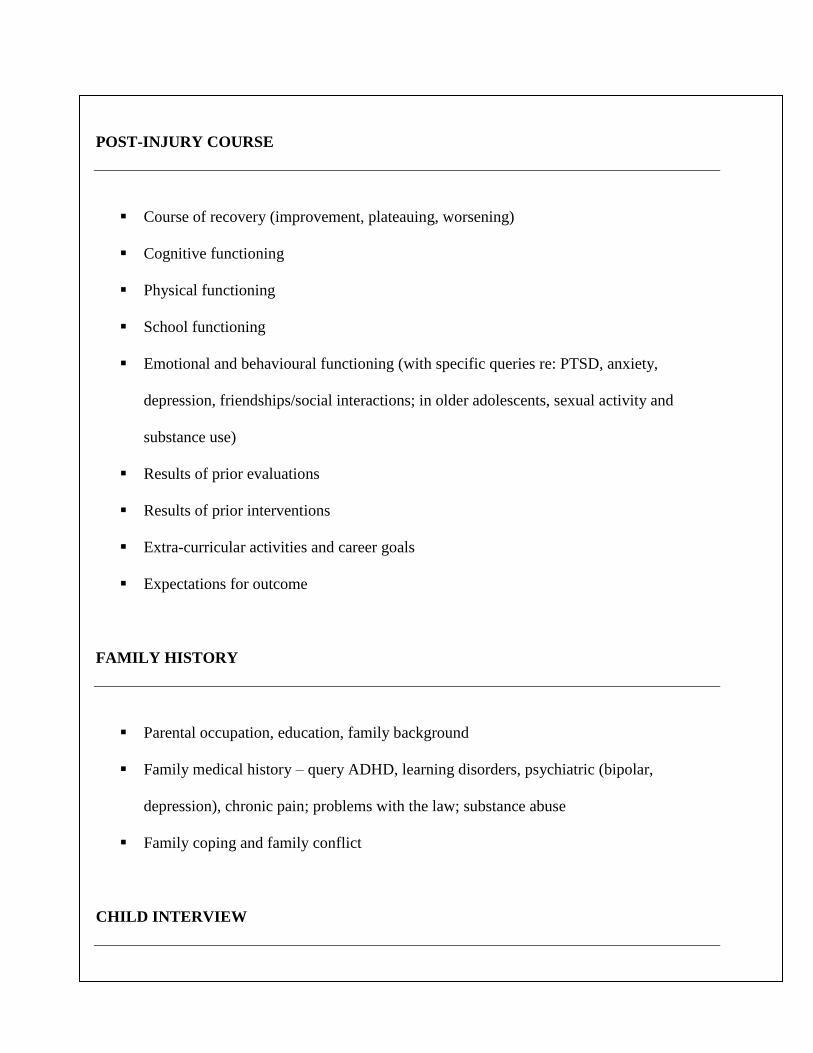
POST-INJURY COURSE
Course of recovery (improvement, plateauing, worsening)
Cognitive functioning
Physical functioning
School functioning
Emotional and behavioural functioning (with specific queries re: PTSD, anxiety,
depression, friendships/social interactions; in older adolescents, sexual activity and
substance use)
Results of prior evaluations
Results of prior interventions
Extra-curricular activities and career goals
Expectations for outcome
FAMILY HISTORY
Parental occupation, education, family background
Family medical history – query ADHD, learning disorders, psychiatric (bipolar,
depression), chronic pain; problems with the law; substance abuse
Family coping and family conflict
CHILD INTERVIEW
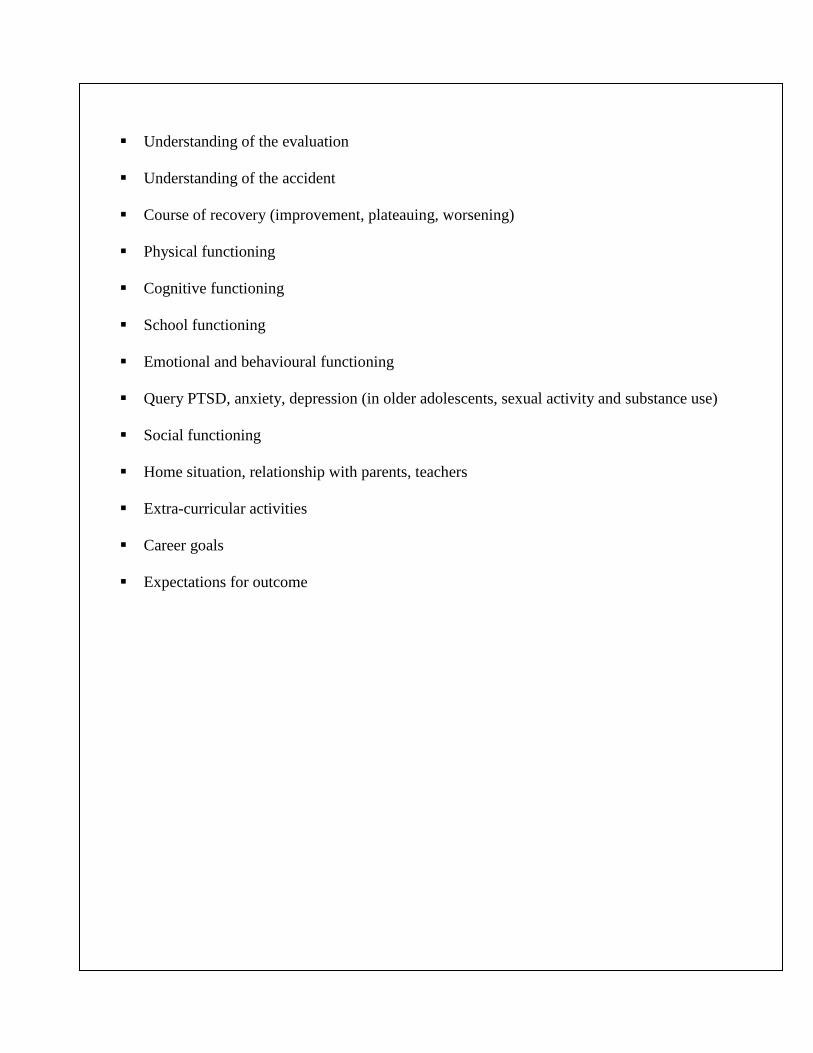
Understanding of the evaluation
Understanding of the accident
Course of recovery (improvement, plateauing, worsening)
Physical functioning
Cognitive functioning
School functioning
Emotional and behavioural functioning
Query PTSD, anxiety, depression (in older adolescents, sexual activity and substance use)
Social functioning
Home situation, relationship with parents, teachers
Extra-curricular activities
Career goals
Expectations for outcome
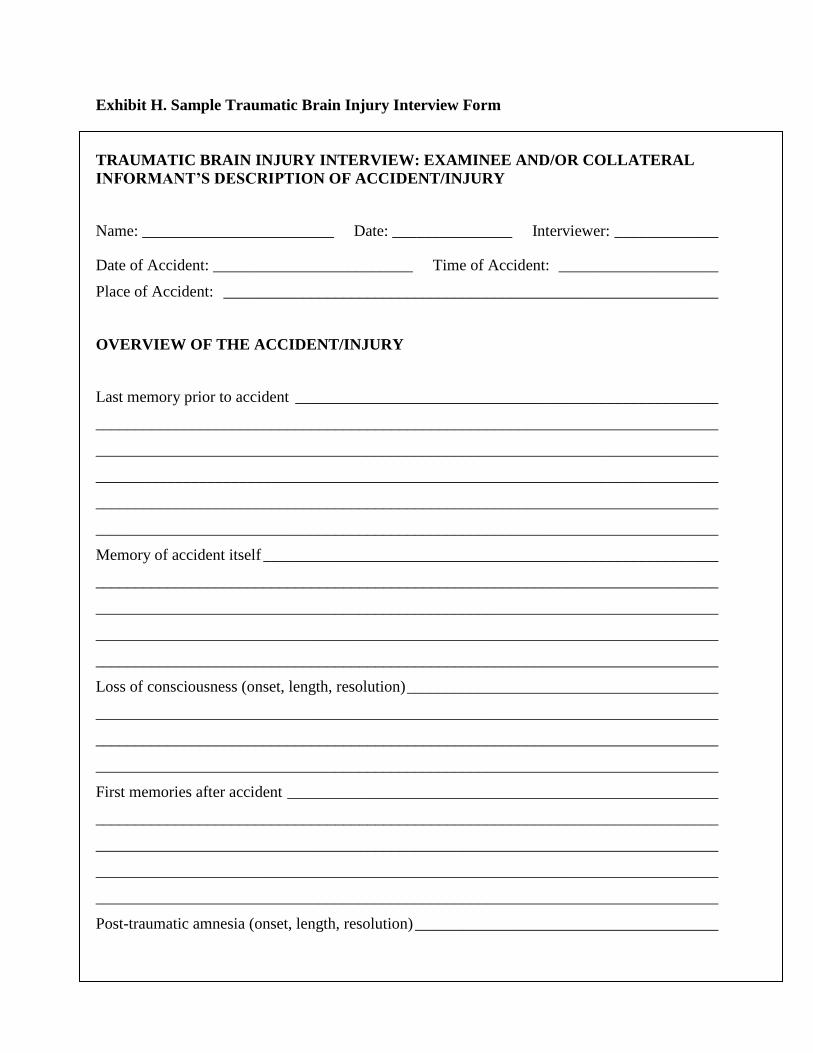
Exhibit H. Sample Traumatic Brain Injury Interview Form
TRAUMATIC BRAIN INJURY INTERVIEW: EXAMINEE AND/OR COLLATERAL
INFORMANT’S DESCRIPTION OF ACCIDENT/INJURY
Name: ________________________ Date: _______________ Interviewer: _____________
Date of Accident: _________________________ Time of Accident: ____________________
Place of Accident: ______________________________________________________________
OVERVIEW OF THE ACCIDENT/INJURY
Last memory prior to accident _____________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Memory of accident itself _________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Loss of consciousness (onset, length, resolution) _______________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
First memories after accident ______________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Post-traumatic amnesia (onset, length, resolution) ______________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
SYMPTOMS AND COURSE OVER TIME
Dizziness ______________________________________________________________________
______________________________________________________________________________
Vertigo _______________________________________________________________________
______________________________________________________________________________
Diplopia_______________________________________________________________________
______________________________________________________________________________
Headache ______________________________________________________________________
______________________________________________________________________________
Nausea ________________________________________________________________________
______________________________________________________________________________
Tinnitus _______________________________________________________________________
______________________________________________________________________________
Other _________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
POST-TRAUMATIC STRESS SYMPTOMS
Flashbacks _____________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Nightmares ____________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________

Fear/anxiety/avoidance ___________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
FUNCTIONAL IMPACT OF ACCIDENT/INJURY
Perceived impact on school functioning ______________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Perceived impact on emotional and behavioral functioning _______________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Perceived impact on activities of daily living and functional independence __________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Perceived impact on social and recreational activities ___________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Perceived impact on activities of daily living __________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Exhibit I. Sample Background and History Questionnaire
Dear Parents/Guardian: The following is a detailed questionnaire on your child’s development, medical
history, and current functioning at home and at school. This information will be integrated with the
testing results in order to provide a better picture of your child’s abilities as well as any problem areas.
Please fill out this questionnaire as completely as you can.
CHILD’S FAMILY
Child’s Name: _______________________________________________ Today’s Date: ______________
Birthdate: ____________ Age: _____ Grade: _____ Name of School: _________________________
Birth Country: ______________________________ Age on arrival in Canada if born elsewhere: _______
Person filing out this ___________
City of residence: _________________ Home phone #: ______________ Work phone #: ____________
Biological Mother’s Name: ________________________ Age: _____ Highest Grade Completed: _____
Number of Years of Education: ________ Degree/Diploma (if applicable): _________________________
Occupation: _____________________________________________________________________________
Biological Father’s Name: ________________________ Age: _____ Highest Grade Completed: ______
Number of Years of Education: _______ Degree/Diploma (if applicable): __________________________
Occupation: _____________________________________________________________________________
Marital status of biological parents: ___
If biological parents are separated or divorced:
How old was this child when the separation occurred? __________
_____________________________________________________________________________________
Stepparent’s Name: ______________________ Age: _____ Occupation: ______________________
If this child is not living with either biological parent:
Reason: ______________________________________________________________________________
______
Name(s) of legal guardian(s): ____________________________________________________________
List all people currently living in your child’s household:
Name Relationship to Child Age
_______________________________________________________________________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
_______________________________________________________________________________________
If any brothers or sisters are living outside the home, list their names and ages:
_______________________________________________________________________________________
_______________________________________________________________________________________
Primary language spoken in the home: ________________________________________________________
Other languages spoken in the home: _________________________________________________________
If your child’s first language is not English, please complete the following:
Child’s first language: ___________________________________ Age at which your child learned
English: ______________________________________________________________________________
BEHAVIOUR CHECKLIST (CURRENT)
Place a check mark () next to behaviours that you believe your child currently exhibits to an excessive
or exaggerated degree when compared to other children his or her age.
Sleeping and Eating
Nightmares
Sleepwalking
Trouble sleeping (describe):
_______________________________________
_______________________________________
_______________________________________
Eats poorly
Picky eater
Eats excessively
Social Development
Prefers to be alone
Shy or timid
More interested in objects than in people
Difficulty making friends
Plays or socialises with younger children
Teased by other children
Bullies other children
Does not seek friendships with peers
Not sought our for friendship by peers
Does not play or socialise with other children
outside of school
Difficulty seeing another person’s point of view
Doesn’t empathise with others
Overly trusting of others
Easily taken advantage of
Overly familiar with people
Doesn’t appreciate humour
Overly attached to certain people
Behaviour
Stubborn
Irritable
Frequent tantrums
Strikes out at others
Throws things at others
Destroys things
Angry or resentful
Oppositional
Negativistic
Lying
Argues with adults
Low frustration threshold
Blames others for own mistakes
Daredevil behaviour
Runs away
Needs a lot of supervision
Impulsive (does things without thinking)
Talks excessively
Skips school
Interrupts frequently
Purposely harms or injures self
Dangerous to self or others (e.g., running into
street) describe:
_______________________________________
_______________________________________
_______________________________________
Talks about killing self (describe):
_______________________________________
_______________________________________
_______________________________________
Unusual fears, habits or mannerisms (describe):
_______________________________________
_______________________________________
_______________________________________
Steals
Depressed
Cries frequently
Excessively worried and anxious
Overly preoccupied with details
Overly attached to certain objects
Not affected by praise
Not affected by negative consequences
Drug abuse
Alcohol abuse
Sexually active
Other Problems
Wets bed
Wets self during the day
Poor bowel control (soils self)
Motor/Vocal tics
Overreacts to noises
Overreacts to touch
Fails to react to loud noise
Poor sense of danger
Has blank spells
Sloppy table manners
Bangs head
Bites nails
Picks nose
Sucks thumb
Masturbation in public places
Excessive daydreaming and fantasy life
Motor Skills
Poor fine motor coordination
Poor gross motor coordination
Clumsy
Cannot tie shoes
Cannot dress self
Difficulty walking
Difficulty running
Cannot throw or catch
BEHAVIOUR CHECKLIST (IF YOUR CHILD IS BEING ASSESSED DUE TO AN INJURY OR ACCIDENT, PLEASE
COMPLETE WITH REGARD TO PRE-INJURY FUNCTIONING)
Place a check mark () next to behaviours that you believe your child exhibited to an excessive or
exaggerated degree, prior to his or her injury, when compared to other children his or her age.
Sleeping and Eating
Nightmares
Sleepwalking
Trouble sleeping (describe):
_______________________________________
_______________________________________
_______________________________________
Eats poorly
Picky eater
Eats excessively
Social Development
Prefers to be alone
Shy or timid
More interested in objects than in people
Difficulty making friends
Plays or socialises with younger children
Teased by other children
Bullies other children
Does not seek friendships with peers
Not sought our for friendship by peers
Does not play or socialise with other children
outside of school
Difficulty seeing another person’s point of view
Doesn’t empathise with others
Overly trusting of others
Easily taken advantage of
Overly familiar with people
Doesn’t appreciate humour
Overly attached to certain people
Behaviour
Stubborn
Irritable
Frequent tantrums
Strikes out at others
Throws things at others
Destroys things
Angry or resentful
Oppositional
Negativistic
Lying
Argues with adults
Low frustration threshold
Blames others for own mistakes
Daredevil behaviour
Runs away
Needs a lot of supervision
Impulsive (does things without thinking)
Talks excessively
Skips school
Interrupts frequently
Purposely harms or injures self
Dangerous to self or others (e.g., running into
street) describe:
_______________________________________
_______________________________________
_______________________________________
Talks about killing self (describe):
_______________________________________
_______________________________________
_______________________________________
Unusual fears, habits or mannerisms (describe):
_______________________________________
_______________________________________
_______________________________________
Steals
Depressed
Cries frequently
Excessively worried and anxious
Overly preoccupied with details
Overly attached to certain objects
Not affected by praise
Not affected by negative consequences
Drug abuse
Alcohol abuse
Sexually active
Other Problems
Wets bed
Wets self during the day
Poor bowel control (soils self)
Motor/Vocal tics
Overreacts to noises
Overreacts to touch
Fails to react to loud noise
Poor sense of danger
Has blank spells
Sloppy table manners
Bangs head
Bites nails
Picks nose
Sucks thumb
Masturbation in public places
Excessive daydreaming and fantasy life
Motor Skills
Poor fine motor coordination
Poor gross motor coordination
Clumsy
Cannot tie shoes
Cannot dress self
Difficulty walking
Difficulty running
Cannot throw or catch
EDUCATION PROGRAM
Does your child have an individual education plan (IE
If yes, when was the IEP created? ____________________
If not satisfied, please explain: __________________________________________________________________
__________________________________________________________________________________________
If yes, what grade(s) and why? _________________________________________________________________
__________________________________________________________________________________________
Is your child’s curricu
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
Has your chi
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
Rate your child’s academic performance relative to other children of the same age. Please estimate the grade level
your child is functioning at in the given area if he or she is above or below average.
Above Average Average Below Average Impaired Grade Level
Handwriting _____
Spelling _____
Punctuation _____
Vocabulary _____
Grammar _____
Reading speed _____
Reading comprehension _____
Math skills _____
Check any problems reported from school:
Difficulty sustaining attention
Easily distracted
Daydreaming
Fidgeting / restless
Frequently gets out of seat
Difficulty working quietly
Difficulty working independently
Doesn’t want to be called on
Blurts out answers
Difficulty following instructions
Doesn’t cooperate well in group activities
Doesn’t respect the rights of others
Shifts from one activity to another
Does better in a one-to-one relationship
Won’t wait his/her turn
Teased by other children
Talking back
Refusing to do work
Bullies other children
Fighting
Messy / disorganised
Does not like school
Truant
Excessively tired or sleepy
Describe briefly other classroom or school problems if applicable:

COGNITIVE SKILLS
Rate your child’s cognitive skills relative to other children of the same age.
Above Average Average Below Average Impaired
Speech
Comprehension of speech
Problem solving
Attention span
Memory for events
Organisational skills
Memory for facts
Learning from experience
Conceptual thinking
Overall Intelligence
Check any specific problems:
Poor articulation
Difficulty finding words to express self
Disorganised speech
Ungrammatical speech
Talks like a younger child
Slow learner
Forgets to do things
Easily distracted
Frequently forgets instructions
Frequently loses belongings
Difficulty planning tasks
Doesn’t foresee consequences of actions
Slow thinking
Describe briefly any other cognitive problems that your child may have: _________________________
___________________________________________________________________________________
___________________________________________________________________________________
Describe any special skills or abilities that your child may have: ________________________________
___________________________________________________________________________________
___________________________________________________________________________________
DEVELOPMENTAL HISTORY
If your child is adopted, please fill in as much of the following information as you are aware of.
During pregnancy, did the mother of this child:
If yes, what kind? ____________________________________________________________________________
If yes, how many cigarettes each day? ____________________________________________________________
If yes, what kind? ____________________________________________________________________________
Approximately how much alcohol was consumed each day? __________________________________________
Use dr
If yes, what kind? ____________________________________________________________________________
How often were drugs used? ___________________________________________________________________
List any complications during pregnancy (excessive vomiting, excessive staining/blood loss, threatened
miscarriage, infections, toxemia, fainting, dizziness, etc.): ____________________________________________
__________________________________________________________________________________________
Duration of pregnancy (weeks): __________ Duration of labour (hours): __________ Apgars: _____ / _____
If yes on any of other above, for what reason? _____________________________________________________
__________________________________________________________________________________________
If yes on any of other above, for what reason? _____________________________________________________
__________________________________________________________________________________________
What was your child’s birth weight? _____
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
Were there
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
Was there any maternal depression during the immediate post-natal period?
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
If yes, please describe: ________________________________________________________________________
__________________________________________________________________________________________
Were any of the following present (to a significant degree) during infancy or the first few years of life?
Unusually quiet or inactive
Did not like to be held or
cuddled
Not alert
Difficult to soothe
Colic
Excessive restlessness
Excessive sleep
Diminished sleep
Headbanging
Constantly into everything
Excessive number of accidents
compared to other children
Please indicate the approximate age in months or years at which your child showed the following behaviours. If
you feel that you child was early or late in showing a listed behaviour, please indicate by checking the appropriate
box. Check never if your child has never shown the listed behaviour.
Age Early Late Never Age Early Late Never
Smiled ________ Tied shoelaces ________
Rolled over ________ Dressed self ________
Sat alone ________ Fed self ________
Crawled ________ Bladder trained, day ________
Walked ________ Bladder trained, night ________
Ran ________ Bowel trained ________
Babbled ________ Rode tricycle ________
First word ________ Rode bicycle ________
Sentences ________
CURRENT MEDICATIONS
List all medications that your child is currently taking:
Medication Reason Taken Dosage (If known) Start Date
MEDICAL HISTORY
Date of last physical examination:
Date of last vision examination:
Date of last hearing examination:
Place a check next to any illness or condition that your child has had. When you check an item, also note
the approximate date of the illness (if you prefer, you can simply indicate the child’s age at illness).
Illness or condition Date(s)/age(s) Illness or condition Date(s)/age(s)
s
FAMILY MEDICAL HISTORY
Place a check next to any illness or condition that any member of the immediate family (i.e., brothers,
sisters, aunts, uncles, cousins, grandparents) has had. Please note the family member’s relationship to the
child.
Condition Relationship to
child
Condition Relationship to
child
Seizures or Epilepsy _____________ Neurological illness or disease _____________
Attention deficit _____________ Mental illness _____________
Hyperactivity _____________ Depression or anxiety _____________
Learning disabilities _____________ Tics or Tourette’s syndrome _____________
Mental retardation _____________ Alcohol or drug abuse _____________
Childhood behaviour problems _____________ Suicide attempt _____________
If yes, please list prescription or describe (e.g., nearsighted): _____________________________________
If yes, please describe): ___________________________________________________________________
Does your
List had any previous assessments that your child has had:
Dates of Testing Name of Examiner
Psychiatric
Psychological
Neuropsychological
Educational
Speech Pathology
Have there been any recent stressors that you think may be contributing to your child’s difficulties (e.g.,
illness, deaths, operations, accidents, separations, divorce of parents, parent changed job, changed schools,
family moved, family financial problems, remarriage, sexual trauma, other losses)? __________________
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
List any form of psychological/psychiatric treatment that your child has had (e.g., psychotherapy, family
therapy, inpatient or residential treatment):
Type of Treatment Dates Name of Therapist
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
OTHER INFORMATION
What are your child’s favourite activities? __________________________________________________
____________________________________________________________________________________
List any special interests that your child has: ________________________________________________
____________________________________________________________________________________
List any sports your child plays: __________________________________________________________
If yes, please describe briefly: ____________________________________________________________
____________________________________________________________________________________
____________________________________________________________________________________
What disciplinary techniques do you usually use when your child behaves inappropriately? Place a check
next to each technique that you usually use.
Ignore problem behaviour
Scold child
Take away some activity or food
Threaten child
Reason with child
Redirect child’s interest
Don’t use any technique
Tell child to sit on chair
Send child to his/her room
Spank child
Which disciplinary techniques are usually effective, and with what types of problem(s)? _____________
Which disciplinary techniques are usually ineffective, and with what types of problems? _____________
___________________________________________________________________________________
On the average, what percentage of the time does your child comply with requests or commands? _____
___________________________________________________________________________________
What have you found to be the most satisfactory ways of helping your child? ______________________
___________________________________________________________________________________
What are your child’s assets or strengths? __________________________________________________
___________________________________________________________________________________
Is there any other information that you think that may help me in assessing your child?
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________
___________________________________________________________________________________