examining stress outcomes among depressed mothers treated with ipt jill m. cyranowski, ph.d....
TRANSCRIPT

Examining Stress OutcomesAmong Depressed Mothers
Treated with IPT
Jill M. Cyranowski, Ph.D.Assistant Professor of Psychiatry and Psychology
Western Psychiatric Institute and ClinicUniversity of Pittsburgh Medical Center

PMBC-related research goals Aims of pilot study Feasibility outcomes: recruitment, retention and compliance Pilot study results Acute physiological and emotional
reactivity to child-focused interpersonalstressor
Examining correlates of the cortisolresponse to waking among depressed andnever-depressed moms
Overview
DepressionAnd Interpersonal Life Stress
Major depression associated with perturbations in neuroendocrine and autonomic stress response Importance of understanding depression-
related HPA/SAM dysreguation within asocial/interpersonal context
Evidence of interactions between depression and recent life stress or early childhood trauma

If you improve interpersonal function… alleviating interpersonal problems increasing social support
… decrease depressive symptoms
Role of stress Interpersonal problems engender stress Social support buffers one from the negative
effects of life stress
IPT as a Research Platform
MOOD
Interpersonal Events

Stress Outcomes Study (SOS):Study Goals
Use of non-invasive physiologic procedures that could be implemented in outpatient depression clinic Salivary cortisol Cardiovascular reactivity Continuous EKG for Heart Period Variability (HPV) Obtain dynamic assessment of stress system that examined stress reactivity within a social context Examine the feasibility of study procedures Would mothers be willing and able to participate? Incorporation into clinic procedures

Stress Outcomes Study (SOS):Study Goals
Incorporate thorough psychosocial assessment Perceived stress, early life trauma Social support, social function Could we incorporate a proxy evaluation of
levels of expressed emotion (EE) displayed bymothers when talking about their children
Study Participants
Depressed mothers recruited from parent treatment trial (MH64518, Holly Swartz, PI) Age 18-60, mother of child aged 6-18 being
treated in a WPIC child psychiatric clinic Met SCID MDD criteria, HRSD > 15 Randomly assigned to receive either
IPT-MOMS or TAU (treatment as usual) Control mothers matched on age and ethnicity Timing of baseline (“early treatment”) assessment Goal: within 4 weeks of entry into parent study IPT mothers had received an average of 4
sessions prior to baseline assessment
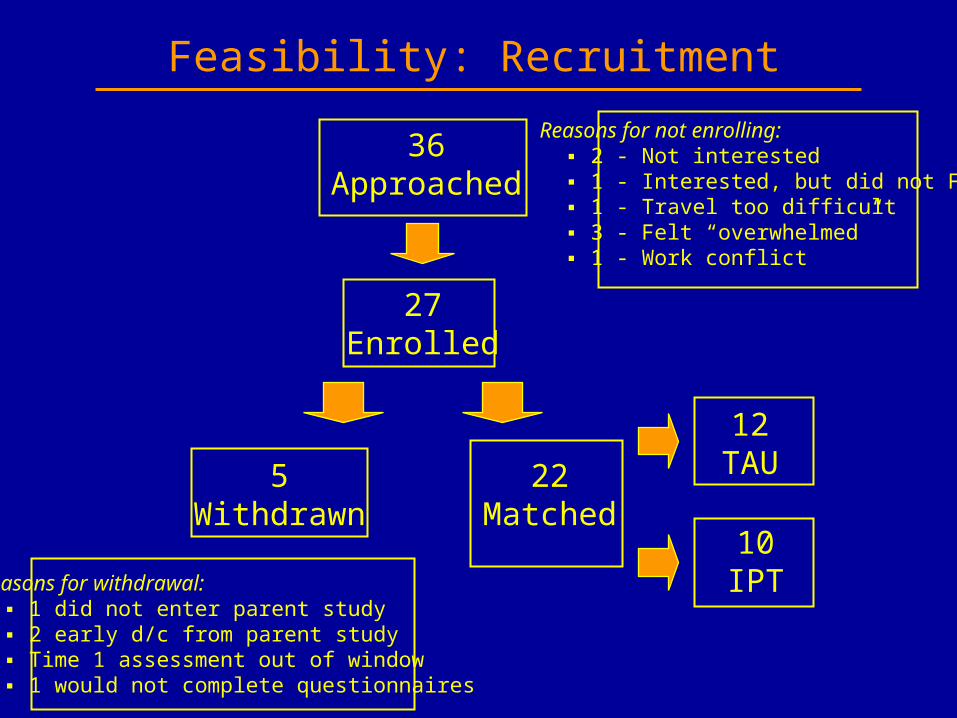
Feasibility: Recruitment
36Approached
27Enrolled
Reasons for not enrolling: ▪ 2 - Not interested ▪ 1 - Interested, but did not FU ▪ 1 - Travel too difficult ▪ 3 - Felt “overwhelmed” ▪ 1 - Work conflict
5Withdrawn
22Matched
12TAU
10IPTReasons for withdrawal:
▪ 1 did not enter parent study ▪ 2 early d/c from parent study ▪ Time 1 assessment out of window ▪ 1 would not complete questionnaires
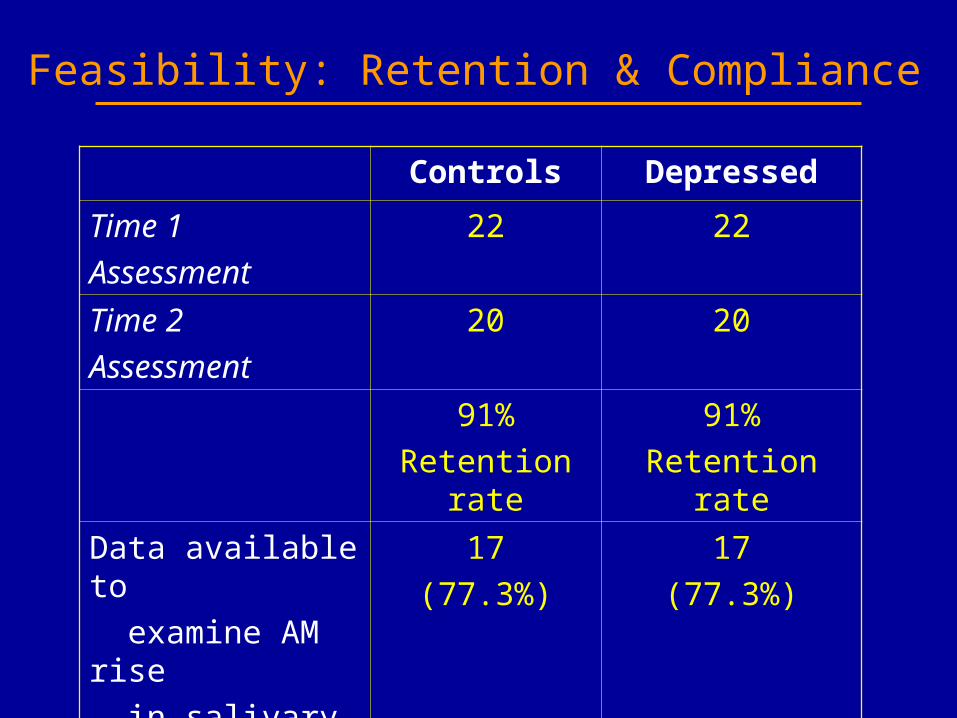
Feasibility: Retention & Compliance
Controls Depressed
Time 1
Assessment
22 22
Time 2
Assessment
20 20
91%
Retention rate
91%
Retention rate
Data available to
examine AM rise
in salivary cortisol
17
(77.3%)
17
(77.3%)

In-Clinic Stress Reactivity Task: Examining Acute Physiological
and Emotional Reactivity to a Child-Focused
Interpersonal Stressor

Give speech about “an interpersonal situation with your [son/daughter] that made you feel angry or stressed.” ■ Describe the situation ■ How did you deal with the situation? ■ How did you feel about the situation and the people involved? ■ How well do you think you handled the situation? How
satisfied are you with the way it all turned out?
■ Told that speech would be video taped and that their performance would be rated at a later time
Speech Stress


In-Clinic Reactivity Task
10 minHabituation 10 min
Resting Baseline
Recovery 1(20 min)
5 minFree
Speech
4 minSpeechStress
Recovery 2(20 min)
Series of 2-3 BP assessments
POMS assessment
2 minSpeech
Prep

Controls(N=22)
IPT(N=10)
TAU(N=12)
Age mean(SD)
44.30(7.41)
42.22(7.82)
45.58(8.53)
Education mean(SD)
15.50(2.44)
14.40(2.95)
15.50(2.43)
BMI mean(SD)
27.59(5.85)
28.35(6.09)
31.34(6.16)
% Married or living with partner
% 86% 60% 58%
Study Participants: Demographics

Controls(N=22)
IPT(N=10)
TAU(N=12)
BDI Beck Depression
mean(SD)
2.05(1.81)
16.20*(5.47)
21.18*(8.09)
MASQGD Depression
mean(SD)
15.27(2.71)
23.60**(3.89)
31.36**(7.72)
PSSPerceived Stress
mean(SD)
17.77(5.35)
33.20(5.71)
36.73(5.71)
PSWQ Worry Questionaire
mean(SD)
39.41(10.59)
51.38*(8.52)
63.00*(13.62)
Study Participants: Clinical Variables
IPT vs TAU group comparison: ** p < .01, * p = .06

Mood Reactivity:POMS Depression Scale
POMS Depression
0
1
2
3
4
5
6
7
8
9
10
Baseline Post Speech Recovery 1
Assessment
Controls (N=22)
Dep TAU (N=12)

Mood Reactivity:POMS Depression Scale
POMS Depression
0
1
2
3
4
5
6
7
8
9
10
Baseline Post Speech Recovery 1
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)

Mood Reactivity:POMS Depression Reactivity Scores
Visit 2: Raw Change in POMS DepressionBaseline to Speech Stress
1.09
5.92
3.4
0
1
2
3
4
5
6
7
Base to Speech Stress
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)
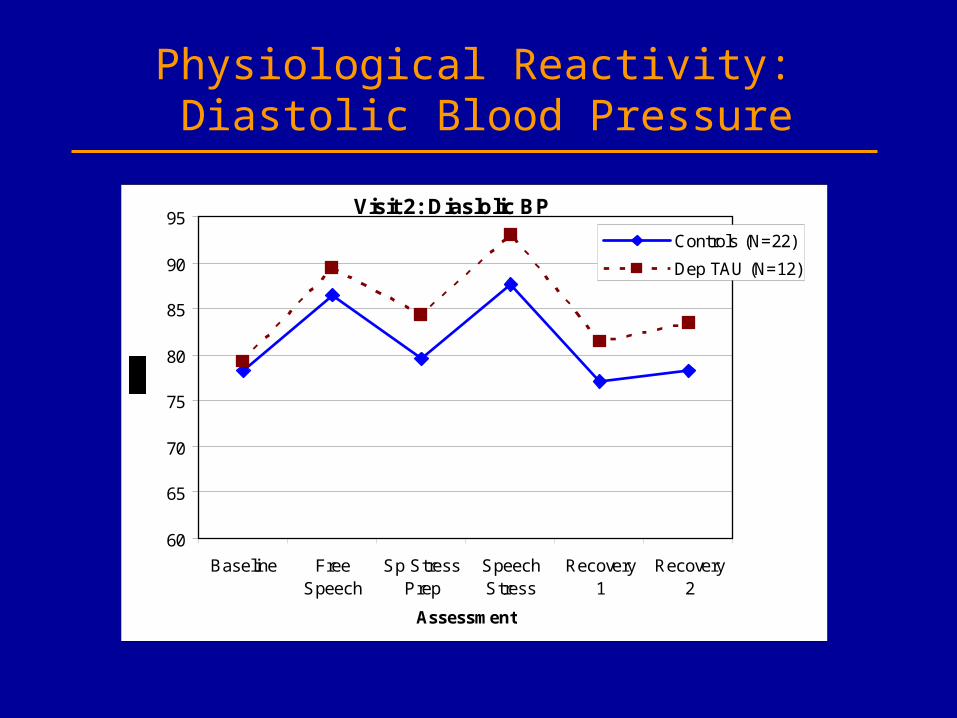
Physiological Reactivity: Diastolic Blood Pressure
Visit 2: Diaslolic BP
60
65
70
75
80
85
90
95
Baseline FreeSpeech
Sp StressPrep
SpeechStress
Recovery1
Recovery2
Assessment
Controls (N=22)
Dep TAU (N=12)
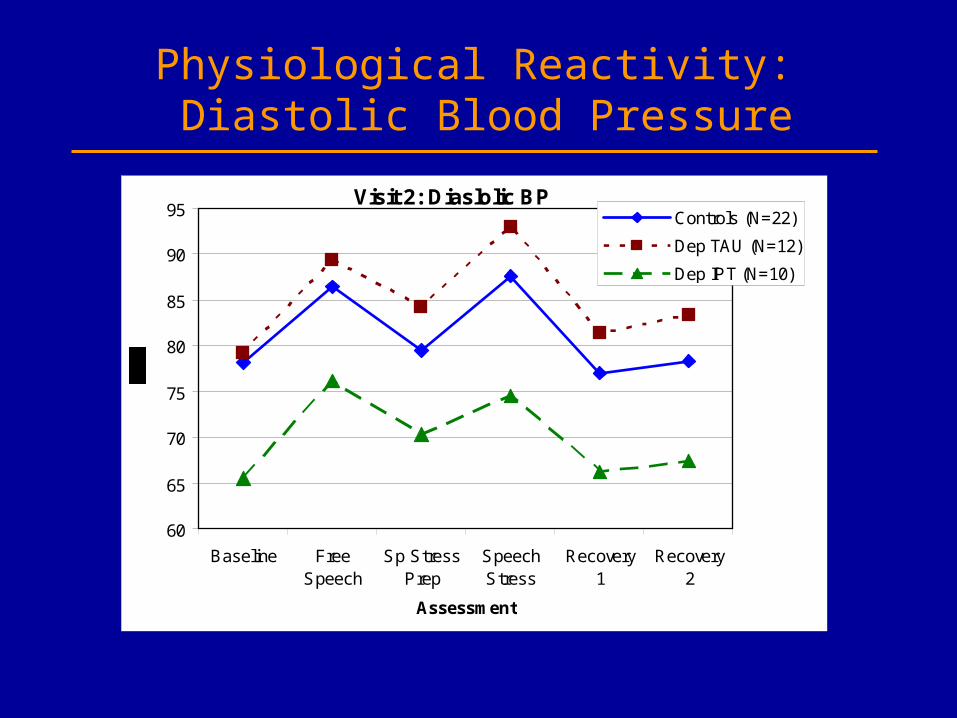
Physiological Reactivity: Diastolic Blood Pressure
Visit 2: Diaslolic BP
60
65
70
75
80
85
90
95
Baseline FreeSpeech
Sp StressPrep
SpeechStress
Recovery1
Recovery2
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)

Physiological Reactivity: Diastolic Blood Pressure Reactivity Scores
Visit 2: Raw Change in DBPBaseline to Speech Stress
9.46
13.73
9.08
8
9
10
11
12
13
14
15
Base to Speech Stress
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)

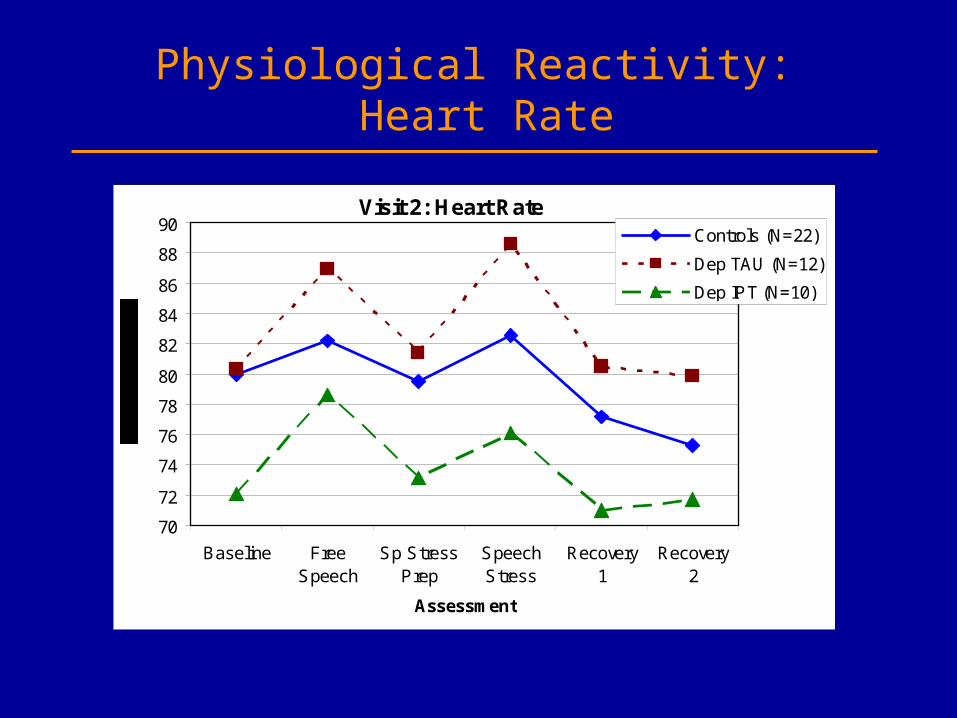
Physiological Reactivity: Heart Rate
Visit 2: Heart Rate
70
72
74
76
78
80
82
84
86
88
90
Baseline FreeSpeech
Sp StressPrep
SpeechStress
Recovery1
Recovery2
Assessment
Controls (N=22)
Dep TAU (N=12)
Physiological Reactivity: Heart Rate
Visit 2: Heart Rate
70
72
74
76
78
80
82
84
86
88
90
Baseline FreeSpeech
Sp StressPrep
SpeechStress
Recovery1
Recovery2
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)

Physiological Reactivity: Heart Rate Reactivity Scores
Group effect, controlling for: marital status, smoking status, menopausal status, psychotropic med use, and cardiovascular med use, F (2,41) = 4.74, p = .01
Visit 2: Raw Change in HRBaseline to Speech Stress
2.57
8.26
4
0
1
2
3
4
5
6
7
8
9
10
Base to Speech Stress
Assessment
Controls (N=22)
Dep TAU (N=12)
Dep IPT (N=10)
Examining Correlates of the CortisolResponse to Waking Among Depressed
And Never-Depressed Moms

Ambulatory Cortisol Assessment Protocol
Focus on feasibility of implementation Asked to obtain samples for 2 day period 5 samples per day 1 - First wake
2 - 30-mins post-wake3 - 11:00 AM4 - 3:00 PM5 - 8:00 PM
Patients given pre-programmed timers, watches, and diary/instruction cards (“spit kit”)
Used MEMSCAPS for electronic verification


Determining Cortisol Data Integrity
Examined reliability of sample timing using MEMSCAP data and diary cards 2 waking samples – within 10 minutes 11 PM, 3:00 PM, 8:00 PM – within 60 minutes Eliminated any subjects/samples where
Wake time > 11:00 am Subject taking corticosteriod (Advair) Subject indicated problem in comment section Sample outside of temporal assessment window
Used Day 1 samples if: Day 1 was weekday, and First two morning samples were good Otherwise, used Day 2 samples
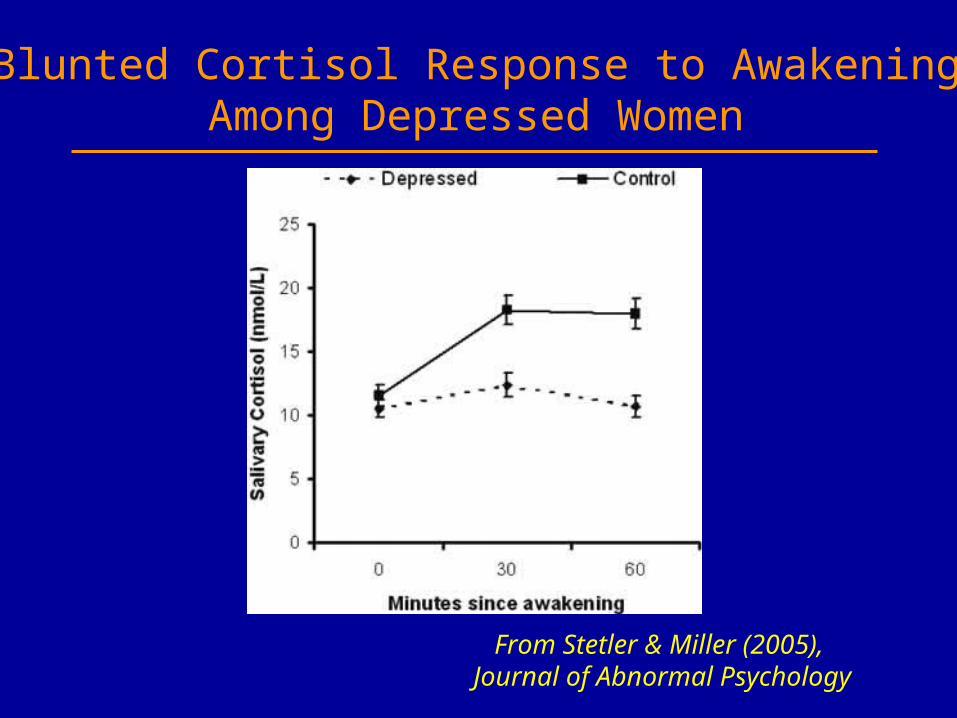
Blunted Cortisol Response to AwakeningAmong Depressed Women
From Stetler & Miller (2005), Journal of Abnormal Psychology
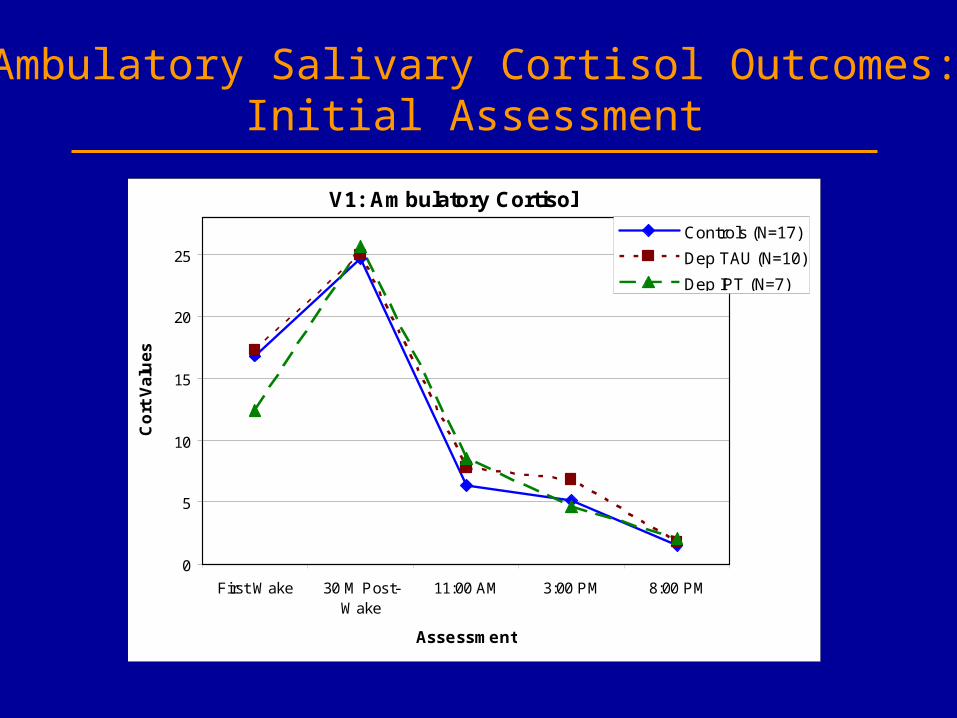
Ambulatory Salivary Cortisol Outcomes:Initial Assessment
V1: Ambulatory Cortisol
0
5
10
15
20
25
First Wake 30 M Post-Wake
11:00 AM 3:00 PM 8:00 PM
Assessment
Co
rt V
alu
es
Controls (N=17)
Dep TAU (N=10)
Dep IPT (N=7)

Self-Reported Early TraumaIn Depressed and Never-Depressed Women
Controls(N=22)
Depressed(N=22)
Total(N=44)
ETI – Total Severity Md 52 * 165 * 88
ETI – Emotional Abuse Md 14 * 128 * 48
ETI – General Trauma Md 6 26 19
ETI – Physical Abuse Md 3 12 8
ETI – Sexual Abuse Md 0 .5 0
27% of Controls scored above group Md73% of Depressed scored above group Md

LES Life Events Reported in Past YearIn Depressed and Never-Depressed Women
Controls(N=18)
Depressed(N=18)
Total number of eventsendorsed
M(SD)
3.17(1.76)
9.50**(5.43)
Cumulative positivity ratings of impact
M(SD)
3.00(3.85)
2.44(1.95)
Cumulative negativity ratings of impact
M(SD)
-3.00(3.53)
-17.33**(13.33)
** p < .01

Stability of AM Rise Indicator over16 Week Study Period
Controls r
p
N
.683**
.007
14
Depressed r
p
N
.398
.159
14

Associations With AM Cortisol Rise:Early Life Trauma
Controls Depressed
Time 1 Time 2 Time 1 Time 2
ETI Total Severity RhopN
-.362.15417
-.200.47515
-.350.16817
-.658**.00815
ETI Emotional Abuse RhopN
-.100.70317
.007.9815
-.270.29517
-.537*.03915
ETI General Trauma RhopN
-.025.92317
-.198.47815
-.302.23817
-.763**.00115
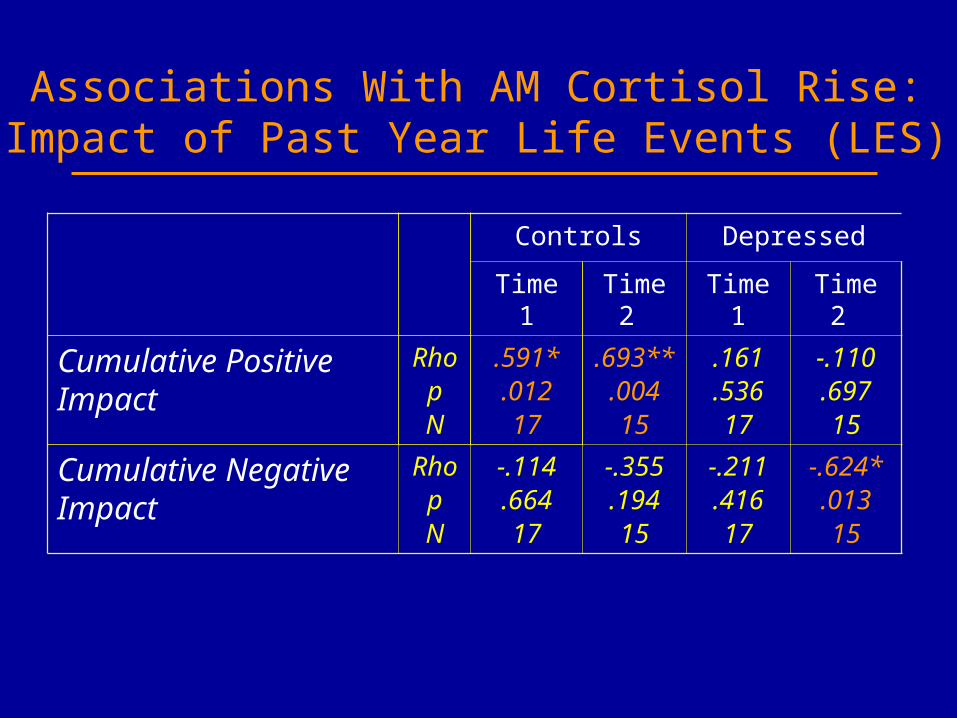
Associations With AM Cortisol Rise:Impact of Past Year Life Events (LES)
Controls Depressed
Time 1 Time 2 Time 1 Time 2
Cumulative Positive Impact
RhopN
.591*.01217
.693**.00415
.161
.53617
-.110.69715
Cumulative Negative Impact
RhopN
-.114.66417
-.355.19415
-.211.41617
-.624*.01315

Depressed Group:Early Trauma (ETI) x Recent Life Events (LES)
-2
0
2
4
6
8
10
12
14
16
Low Negative Life Events High Negative Life Events
AM
co
rtis
ol r
ise
Low Early Trauma
High Early Trauma
Main effect for LES, F(1,14) = 5.80, p < .05
Pilot work supports the feasibility of incorporating
assessment of physiologic stress reactivity and diurnal regulation within outpatient treatment trials Importance of examining stress outcomes within an social/interpersonal context Current social function and social stress Early life traumaIPT trials represent an ideal platform for
examiningrelationship among stress, depression andinterpersonal function over time IPT conceptual model provides ideal fit IPT provides non-pharmacologic probe to
examine relationships over time
Conclusions
Acknowledgements
Holly Swartz Tara HofkensEllen Frank Heather SpielvogleJanet Amico Kristen FreyAnna Marsland
Lynda RoseKathy Light Patty HouckPete Gianaros John Scott DMDPP staff Deb Stapf
Grant Support:National Institute of Mental Health grants
MH64144 (Cyranowski) and MH64518 (Swartz)
Pittsburgh Mind-Body CenterWPIC Mental Health Intervention Research
Center