examination of the joints and extremities evelyn o. salido, md, fpcp, fpra internal medicine and...
TRANSCRIPT

Examination of the Joints and Extremities
Evelyn O. Salido, MD, FPCP, FPRA
Internal Medicine and RheumatologyJanuary 2009

Objectives in doing MSS PE
To screen for MSS problems among asymptomatic and symptomatic individuals
To determine if complaint in the back or limb is due to a MSS problem
To localize the MSS problem- intra or periarticular
To diagnose

Who should be examined?
Musculoskeletal complaints
Pain
Deformity
Disability (loss of function)
Individuals consulting for other complaints

What should be examined?
Scope of the examination
Back
Upper Extremities
Lower Extremities
Systemic PE

Physical Examination will tell us …
Source of pain Inflammatory or not Pattern and extent of
joint involvement single, few, multiple axial, appendicular distal vs proximal,
small vs large Localized or systemic

Requirements for a good PE
Enough room and light Sufficient exposure of parts to be
examined while considering privacy Relaxed and comfortable patient and
examiner Good working knowledge of anatomy Adequate medical history

Physical ExamMUST REMEMBER!!! Examine each joint, not only the source of
complaint. Assess each joint separately. Perform an orderly exam including the spine,
the upper and lower extremities. Proper positioning- as appropriate to the
examination being done

Maneuvers in the PE
Inspection Palpation Range of motion Measurements

Inspection: still & in motion
Posture Contours Symmetry Deformities Atrophy/hypertrophy Masses or nodules
Swelling Redness Skin lesions Instability Abnormal movements

Posture, Contour, Symmetry

Deformity

Swelling and Redness

Redness, Skin Lesion
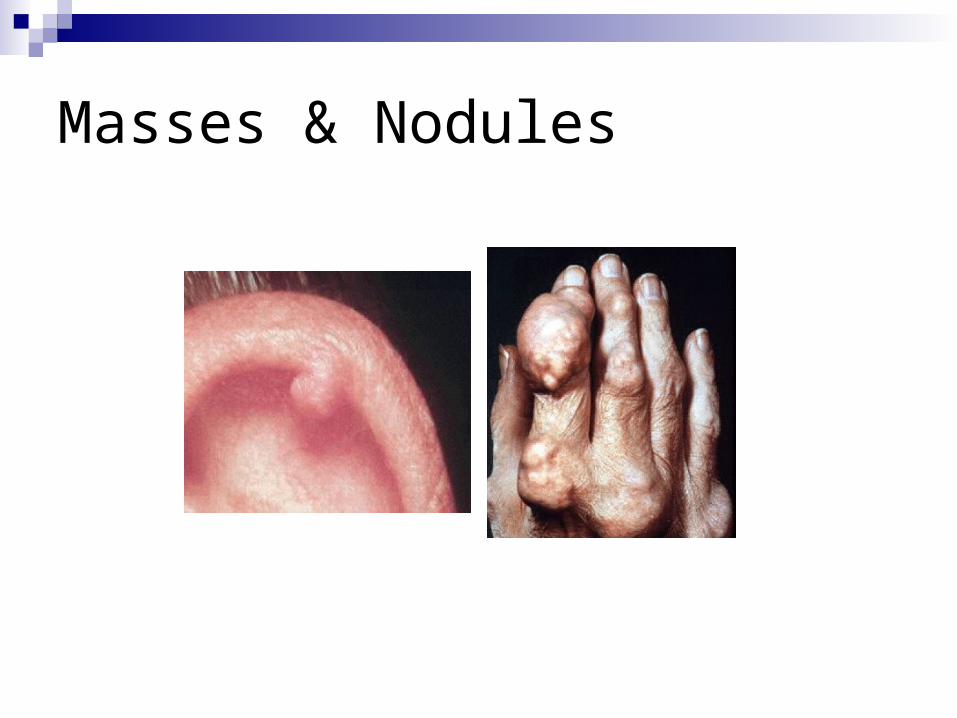
Masses & Nodules

Discrepancies e.g. Atrophy
Localized Generalized Document by
measuring limb circumference

Instability
Diseased joints are able to move into abnormal positions
due to joint surface damage or to laxity of ligaments
passive maneuver by examiner observation of active movement during
weightbearing and walking wobbling, “movement” of bones, “giving-way”

Maneuvers in the PE
Inspection Palpation Range of motion Measurements
Palpate the joint, surrounding tissues and the muscles of the limbs and back

Palpation
Increased Warmth
Tenderness
Swelling- bony, soft tissue, effusion

Tenderness
Unusual sensitivity to touch or pressure
Grade I- pain only
II- pain and wincing
III- wincing and withdrawal
IV- palpation not tolerated

Swelling Bony swelling- osteophyte
& new bone formation
Synovitis- edematous
synovium, boggy swelling,
usually tender
Effusion- excessive fluid in
joint cavity, bulge sign

Swelling
Localized periarticular swelling does not communicate with main joint
cavity infrapatellar bursitis Pitting edema of tissues over a joint

Maneuvers in the PE
Inspection Palpation Range of motion Measurements

Range of motion
Requires knowledge of normal motion of particular joints
Active or Passive When should ROM test be deferred

Limitation of Motion
Comparison with an unaffected joint of the opposite extremity to evaluate individual variations
Increased muscle tension may result in what appears to be significant decreased ROM
May be due to limitation in the joint itself or the periarticular structures
Active motion limited- joint or periarticular problem
Only active motion limited-periarticular problem

Crepitus palpable &/or audible grating or crunching
sensation produced by motion. arises when roughened articular or extra-
articular surfaces are rubbed together by active motion or by manual compression
fine or coarse – depending on rough the opposing cartilage surfaces are
differentiate from cracking sounds caused by the slipping of ligaments or tendons over bony surfaces- normal joints

Doing the Actual PE
Rapid Screen- GALS
Extensive PE
GALS Step 1- Ask 3 basic questions
Have you any pain or stiffness in your muscles, joints, or back?
Can you dress yourself completely without any difficulty?
Can you walk up and down stairs without any difficulty?

GALS Step 2- Gait
Symmetry Smoothness of
movement Normal stride length Normal heel strike,
stance, toe-off, swing through
Able to turn quickly

Heel Strike, Stance, Toe Off, Swingwidth of the base should be 2-4 in from heel to heel flexion of the knee during toe off and swing

GALS Step 3- Inspection from Behind
Straight spine Normal & symmetric paraspinal
muscles Normal shoulder & gluteal
muscle bulk Level iliac crests No popliteal cysts nor swelling No hindfoot swelling or
abnormality

GALS Step 4: Inspection from the side
Normal cervical & lumbar lordosis
Normal thoracic kyphosis

GALS Step 5. “Touch your toes.”
Normal lumbar spine (and hip) flexion

GALS step 6: Inspection from the front- ArmsPlace your hands behind your head (elbows out)- normal glenohumeral,
sternoclavicular, & acromioclavicular joint movement by your side (elbows straight)- full elbow extension In front (palms down)- no wrist/finger swelling or
deformity; able to fully extend fingersTurn your hands over- normal supination/pronation; normal
palmsMake a fist- normal grip powerPlace the tip of each finger on the tip of the thumb- normal
fine precision, pinch

GALS step 6: Inspection from the frontLegs Normal quadricep
bulk/symmetry No knee swelling or
deformity No forefoot/midfoot
deformity Normal arches No abnormal callous formation
Spine “Place your ear on your
shoulder.”Normal cervical lateral
flexion

Regional Examination
BackUpper ExtremitiesLower Extremities

Back
Look: Contour, Deformity, Mass, Skin lesion
Feel: spinous processes, paravertebral muscles, SI joint
Move: cervical, lumbar; Schober’s test for spine flexibility

Back: Look1="Vertebra prominens" Spinous process of C7
2= 2nd Lumbar vertebra
3= L4-5 inter vertebral space
4= Iliac crests
5= Dimples of Venus / Sacroiliac joints
1= Cervical lordosis
2=Thoracic kyphosis
3= Lumbar lordosis
4= Sacral kyphosis

Back: Feel & Move

Back flexibility: Schober’s test

TMJ
Look Feel Move
Put picture here

Shoulder
Inspection Look for symmetry
between both shoulders Check the skin for any
signs of current or past pathology
Identify the clavicle, deltoid & biceps muscles, bicipital groove, scapula

Shoulder
PalpationAssess the soft tissue tone, consistency, size
and shape of muscles, and tendernessCheck the axilla for lymph nodes

Shoulder
Look- swelling, redness
Feel- tenderness
Move- circumduction

Elbow
In a staight arm, the "elbow bump" can be at, and sometimes even above, the condyles.
In a bent arm, the triangle is quite pronounced.
Humero-ulnar joint (hinge) is main articulation, radio-ulnar & humero radial

Elbow jointInspection With palms facing anterior or in
anatomic position, note the valgus angle made by the forearm and the upper arm
Palpation Palpate the bony structures:
Medial and lateral epicondyles, Medial and lateral supracondylar line of the humerus, Olecranon & Radial head
Palpate the soft tissue structures Medial aspect: ulnar nerve, wrist
flexors and pronators Posterior aspect: olecranon
bursa, triceps muscles Lateral aspect: wrist extensors,
lateral collateral ligament, annular ligament
Anterior aspect: cubital fossa
Range of motion: flexion, extension at humeroulnar
articulation forearm supination, pronation at
proximal and distal radioulnar joints
passive

Wrist and Hand
•True wrist/radiocarpal articulation- biaxial ellipsoidal joint (radius, triangular fibrocartilage, 3 carpal bones)
•Distal RU joint is a pivot joint
Palmar flexion & dorsiflexion
Radial & ulnar deviation
Pronation & supination

Wrist
Keep in mind that there are 6 dorsal passageways and 2 palm tunnels through which pass nerves, arteries, veins and tendons.
Some anatomic structures worth mentioning are the carpal tunnel and the median nerve

Wrist
Palpation Bone palpation includes
the following: Radial and ulnar styloid
processes Tubercle of the radius Bones of the wrist: eight
carpal bones Scaphoid, navicular,
lunate, triguetrum pisiform, trapezium, trapezoid, capitate, hamate
Range of motion Flexion (80 degrees from
neutral) Extension (70 degrees
from neutral Ulnar and radial deviation

Hand
Inspection Ventral surface:
creases, thenar and hypothenar eminences, MCP joint area
Dorsal surface: MCP and soft tissue “valleys,” DIP’s and PIP’s, fingernails
MCPs
Hand
Palpation Thenar and hypothenar
eminences Palm aponeurosis Flexor and extensor
tendons Fingers: dorsal and palm
surfaces of MCP, PIP and DIP joints
Fingernails and nail fold capillaries
Range of motion MCPs- hinge joints
Fingers: Abd 20°, Flex (make a fist to touch palm crease), Add, Ext
1st CMC joint- saddle-shaped Thumb: opposition,
flexion/extension, abduction and adduction

Hip
Inspection: pelvic tilt, rotational deformity, muscle wasting, leg lengthPalpation: anterior joint line, greater trochanter, ischial tuberosityRange of motion (ball & socket joint)- F,E,Ab,Ad,R
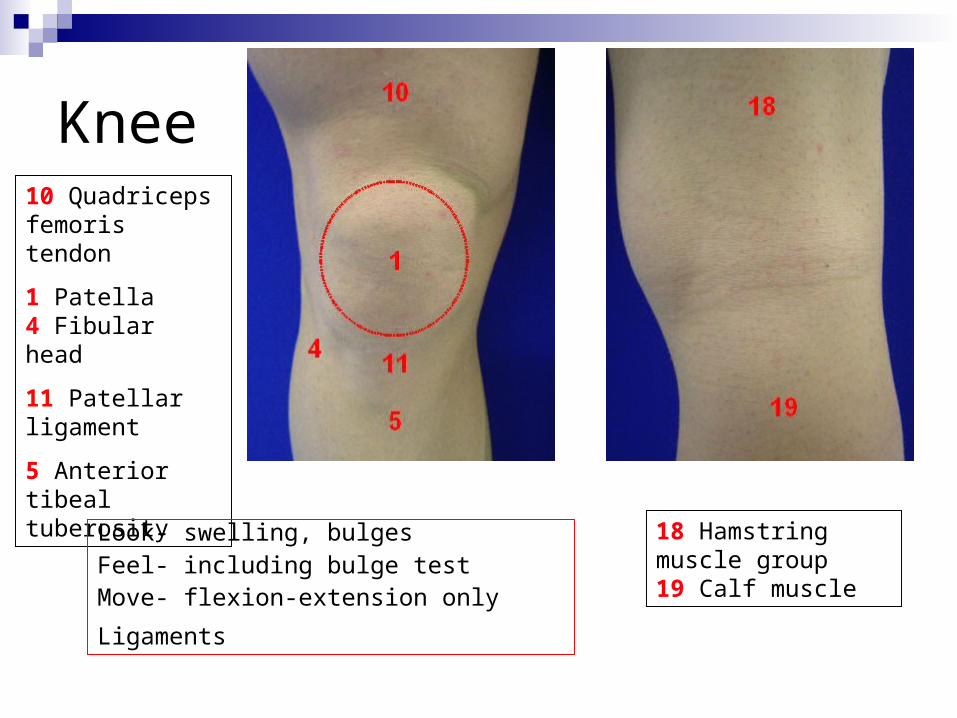
Knee10 Quadriceps femoris tendon
1 Patella4 Fibular head
11 Patellar ligament
5 Anterior tibeal tuberosity
18 Hamstring muscle group19 Calf muscle
Look- swelling, bulgesFeel- including bulge testMove- flexion-extension only
Ligaments

What is wrong here?
Test for effusions: Bulge test & Patellar ballotment

Ankle and Feet
True Ankle joint- distal ends of tibia & fibula and proximal part of body of the talus
- hinge joint; dorsi & plantar flexion
Subtalar joint- inversion & eversion

Toes

Maneuvers in the PE
Inspection Palpation Range of motion Measurements

Measurement
Reporting Your Findings
Inspection Palpation Range of Motion Measurements
Objectives in doing MSS PE
To screen for MSS problems among asymptomatic and symptomatic individuals
To determine if complaint in the back or limb is due to a MSS problem
To localize the MSS problem- intra or periarticular
To diagnose

Articular vs Non-articular Disease ARTICULAR EXTRA-ARTICULAR
ROM pain on active & more on active &
passive motion specific motion
Tender jt surface over bony
ness circumference prominences
along tendons
Pain generalized, well-localized
poorly localized superficial

Evaluation of patient with musculoskeletal complaint
Logical differentials Accurate diagnosis Performance of necessary diagnostic
tests Timely provision of appropriate
therapy
