evidence-based rationale - o-wm.com · evidence-based rationale for utilizing regranex ......
TRANSCRIPT

Evidence-Based Rationalefor Utilizing REGRANEX® (becaplermin) Gel, 0.01% as an Adjunct to Standard of Care Indicated for Diabetic Foot Ulcers (DFUs)
Supplement to WOUNDS January 2014
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
This supplement was not subject to the peer-review process of WOUNDS. Supported by Smith & Nephew, Inc.
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 1 1/7/14 4:30 PM

2
TM1528-0813_REG_0856_ClinMono_M_3.indd 2 1/7/14 1:33 PM

Table of ContentsIntroduction ......................................................................................................................................................... 4
About the authors ............................................................................................................................................... 4
Important Safety Information ............................................................................................................................ 5
1 Burden of DFU ................................................................................................................................................ 6
1.1 Epidemiology of DFUs and associated morbidity ........................................................................................ 6
1.2 Mortality associated with DFUs ................................................................................................................... 7
1.3 Financial burden ......................................................................................................................................... 8
1.4 Evaluation of diabetic foot ulcers ................................................................................................................ 8
1.5 Good ulcer care .......................................................................................................................................... 10
1.6 Unacceptably low healing rates with current standard of care ..................................................................... 11
1.7 Treatment guideline bibliography ................................................................................................................. 11
2 Pharmacology and biological action of growth factors in wound healing ............................................... 12
2.1 Role of growth factors in healing ................................................................................................................. 12
2.2 Role of PDGF in the healing process ........................................................................................................... 12
2.3 PDGF—Its composition .............................................................................................................................. 13
2.4 PDGF-BB—Its role in healing ...................................................................................................................... 13
3 REGRANEX® (becaplermin) Gel, 0.01% ........................................................................................................ 14
4 Boxed Warning ............................................................................................................................................... 15
5 Contraindications/warnings and precautions/drug interactions/use in specific populations/ clinical pharmacology/toxicology/patient counseling information ........................................................... 16
6 Clinical efficacy .............................................................................................................................................. 19
6.1 Phase 3 studies .......................................................................................................................................... 19
6.2 Adverse reactions ....................................................................................................................................... 22
6.3 Clinical trial summaries ............................................................................................................................... 23
7 Dosage and administration ........................................................................................................................... 24
Summary ............................................................................................................................................................. 25
References .......................................................................................................................................................... 26
3
TM1528-0813_REG_0856_ClinMono_M_3.indd 3 1/7/14 1:33 PM

About the authorsEliot Mostow MD, MPH Dr. Eliot Mostow is a professor and chair of the Dermatology Section at Northeast Ohio Medical University (NEOMED) as well as associate professor of Clinical Dermatology at Case Western Reserve School of Medicine’s Department of Dermatology. He began his focused interest in wound care working with Dr. David Steed at the Wound Healing and Limb Preservation Clinic at the University of Pittsburgh in 1992 as a faculty member of the Department of Dermatology. In 1993 he became a founding member of Wound Care Associates of Akron, Inc., which provided staffing at a newly formed multidisciplinary wound healing clinic at Akron General Medical Center. Since then, he has continued his association with Akron General and now runs the Clinical Research Program for the Wound Center. In that role he has coordinated programs in clinical research, health service research, and participated in industry-sponsored trials including the current HP-802 trial with Smith & Nephew.
Matthew Regulski DPM Dr. Matthew Regulski, a practicing foot and ankle surgeon, is the medical director of the Wound Care Institute of Ocean County. Dr. Regulski is also co-director of the Center for Wound Healing and Hyperbaric Medicine at Community Medical Center, as well as being involved at the Wound Care Center at the Kimball Institute. He has been the principal investigator for several clinical trials for chronic leg ulcers and diabetic foot ulcers and has authored several peer-reviewed articles for the treatment of chronic wounds. He is an accomplished speaker for several wound care conferences and is a wound care certified physician. Dr. Regulski is a fellow of the Academy of Physicians in Wound Healing and a fellow of the American Professional Wound Care Association. He is a national delegate for the Association for the Advancement of Wound Care and a member of the Wound Healing Society.
IntroductionThe number of people with diabetes is increasing in both the United States and around the world. It is estimated that, by 2030, approximately 366 million individuals will have diabetes, compared with 171 million in 2000.1 In the United States, the projections are staggering. There are currently 24 million people with diabetes in the US; this number is expected to increase to over 40 million diagnosed and undiagnosed people during the next 25 years.2 Diabetic foot ulcers (DFUs) are a common complication of diabetes that often includes serious repercussions such as infection, amputation, and increased mortality risk.3
The goal of this supplement is twofold:
• Highlight the societal impact of DFUs and current expert recommendations for good ulcer care
• Present the evidence-based rationale for the use of REGRANEX® Gel, when appropriate, as standard adjunctive therapy (ie, in addition to good ulcer care practices) in the treatment of the lower extremity diabetic ulcers that extend into the subcutaneous tissue or beyond and have an adequate blood supply.
4
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 4 1/7/14 4:30 PM

Important Safety InformationWARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCY
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study. REGRANEX® Gel should only be used when the benefits can be expected to outweigh the risks. REGRANEX® Gel should be used with caution in patients with known malignancy.
Indications and usage:
REGRANEX® (becaplermin) Gel is indicated for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and have an adequate blood supply. REGRANEX® Gel is indicated as an adjunct to, and not a substitute for, good ulcer care practices.
Limitations of use:
• The efficacy of REGRANEX® Gel has not been established for the treatment of pressure ulcers and venous stasis ulcers
• The effects of REGRANEX® Gel on exposed joints, tendons, ligaments, and bone have not been established in humans
• REGRANEX® Gel is a non-sterile, low bioburden preserved product that should not be used in wounds that close by primary intention
REGRANEX® Gel is contraindicated in patients with known neoplasm(s) at the site(s) of application. REGRANEX® Gel is contraindicated in patients with known hypersensitivity to any component of the product (e.g., parabens).
Malignancies distant from the site of application have been reported in both a clinical study and in postmarketing use.
In clinical trials, erythematous rashes occurred in 2% of patients treated with REGRANEX® Gel or placebo; none occurred in patients receiving good ulcer care alone. Burning sensation at the site of application and erythema have been reported during post-approval use of REGRANEX® Gel.
Please see accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
5
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 5 1/7/14 4:30 PM
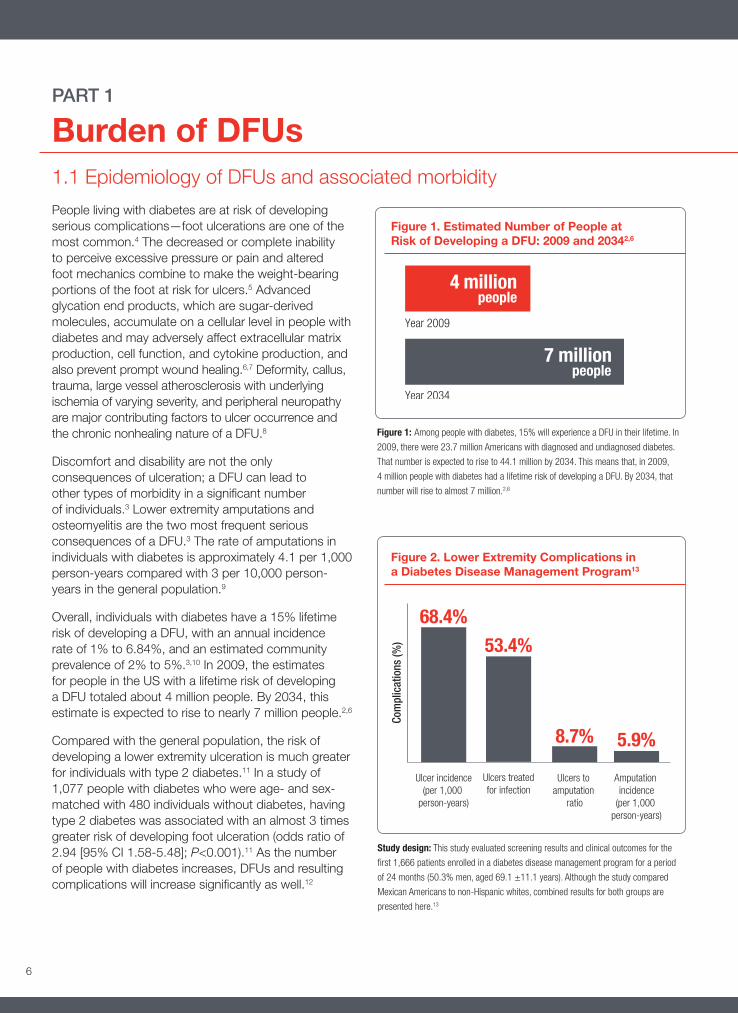
Figure 1. Estimated Number of People at Risk of Developing a DFU: 2009 and 20342,6
People living with diabetes are at risk of developing serious complications—foot ulcerations are one of the most common.4 The decreased or complete inability to perceive excessive pressure or pain and altered foot mechanics combine to make the weight-bearing portions of the foot at risk for ulcers.5 Advanced glycation end products, which are sugar-derived molecules, accumulate on a cellular level in people with diabetes and may adversely affect extracellular matrix production, cell function, and cytokine production, and also prevent prompt wound healing.6,7 Deformity, callus, trauma, large vessel atherosclerosis with underlying ischemia of varying severity, and peripheral neuropathy are major contributing factors to ulcer occurrence and the chronic nonhealing nature of a DFU.8
Discomfort and disability are not the only consequences of ulceration; a DFU can lead to other types of morbidity in a significant number of individuals.3 Lower extremity amputations and osteomyelitis are the two most frequent serious consequences of a DFU.3 The rate of amputations in individuals with diabetes is approximately 4.1 per 1,000 person-years compared with 3 per 10,000 person-years in the general population.9
Overall, individuals with diabetes have a 15% lifetime risk of developing a DFU, with an annual incidence rate of 1% to 6.84%, and an estimated community prevalence of 2% to 5%.3,10 In 2009, the estimates for people in the US with a lifetime risk of developing a DFU totaled about 4 million people. By 2034, this estimate is expected to rise to nearly 7 million people.2,6
Compared with the general population, the risk of developing a lower extremity ulceration is much greater for individuals with type 2 diabetes.11 In a study of 1,077 people with diabetes who were age- and sex-matched with 480 individuals without diabetes, having type 2 diabetes was associated with an almost 3 times greater risk of developing foot ulceration (odds ratio of 2.94 [95% CI 1.58-5.48]; P<0.001).11 As the number of people with diabetes increases, DFUs and resulting complications will increase significantly as well.12
PART 1
Burden of DFUs1.1 Epidemiology of DFUs and associated morbidity
Figure 1: Among people with diabetes, 15% will experience a DFU in their lifetime. In
2009, there were 23.7 million Americans with diagnosed and undiagnosed diabetes.
That number is expected to rise to 44.1 million by 2034. This means that, in 2009,
4 million people with diabetes had a lifetime risk of developing a DFU. By 2034, that
number will rise to almost 7 million.2,6
Study design: This study evaluated screening results and clinical outcomes for the
first 1,666 patients enrolled in a diabetes disease management program for a period
of 24 months (50.3% men, aged 69.1 ±11.1 years). Although the study compared
Mexican Americans to non-Hispanic whites, combined results for both groups are
presented here.13
Figure 2. Lower Extremity Complications in a Diabetes Disease Management Program13
6
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 6 1/7/14 4:30 PM
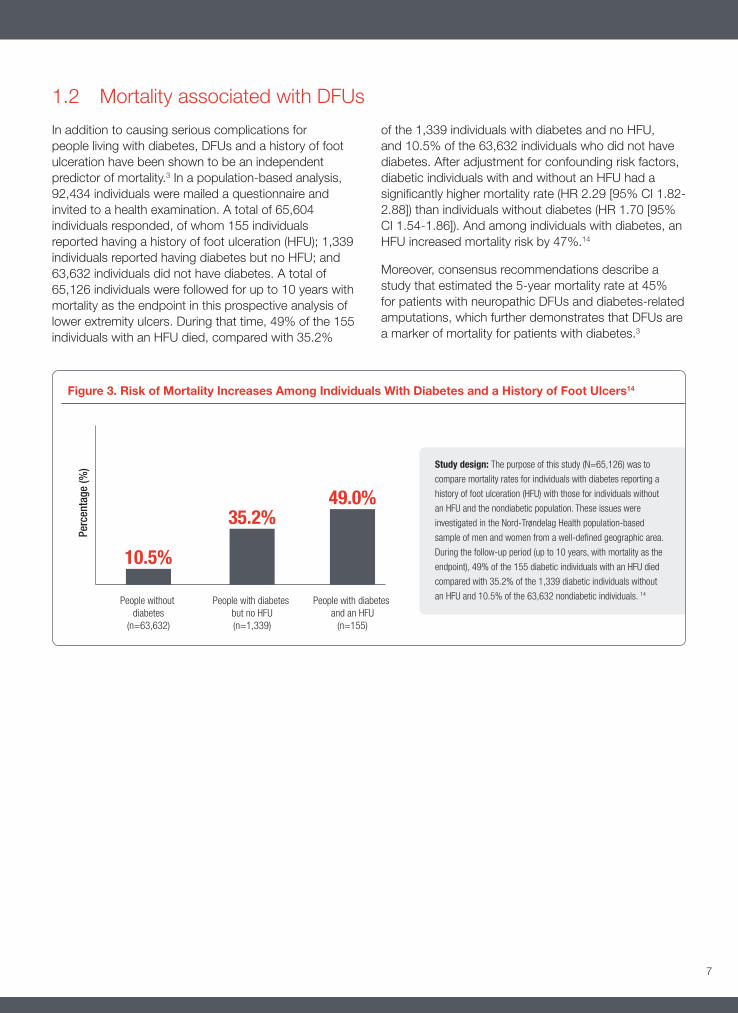
Figure 3. Risk of Mortality Increases Among Individuals With Diabetes and a History of Foot Ulcers14
1.2 Mortality associated with DFUs
In addition to causing serious complications for people living with diabetes, DFUs and a history of foot ulceration have been shown to be an independent predictor of mortality.3 In a population-based analysis, 92,434 individuals were mailed a questionnaire and invited to a health examination. A total of 65,604 individuals responded, of whom 155 individuals reported having a history of foot ulceration (HFU); 1,339 individuals reported having diabetes but no HFU; and 63,632 individuals did not have diabetes. A total of 65,126 individuals were followed for up to 10 years with mortality as the endpoint in this prospective analysis of lower extremity ulcers. During that time, 49% of the 155 individuals with an HFU died, compared with 35.2%
of the 1,339 individuals with diabetes and no HFU, and 10.5% of the 63,632 individuals who did not have diabetes. After adjustment for confounding risk factors, diabetic individuals with and without an HFU had a significantly higher mortality rate (HR 2.29 [95% CI 1.82-2.88]) than individuals without diabetes (HR 1.70 [95% CI 1.54-1.86]). And among individuals with diabetes, an HFU increased mortality risk by 47%.14
Moreover, consensus recommendations describe a study that estimated the 5-year mortality rate at 45% for patients with neuropathic DFUs and diabetes-related amputations, which further demonstrates that DFUs are a marker of mortality for patients with diabetes.3
Study design: The purpose of this study (N=65,126) was to
compare mortality rates for individuals with diabetes reporting a
history of foot ulceration (HFU) with those for individuals without
an HFU and the nondiabetic population. These issues were
investigated in the Nord-Trøndelag Health population-based
sample of men and women from a well-defined geographic area.
During the follow-up period (up to 10 years, with mortality as the
endpoint), 49% of the 155 diabetic individuals with an HFU died
compared with 35.2% of the 1,339 diabetic individuals without
an HFU and 10.5% of the 63,632 nondiabetic individuals. 14
7
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 7 1/7/14 4:30 PM

1.4 Evaluation of DFUs
1.3 Financial burden of DFUs
Recently, consensus recommendations were published to assist clinicians in advancing the treatment of neuropathic DFUs through straightforward and practical approaches to good ulcer care.3 These recommendations provide a comprehensive framework for optimum management of a DFU, beginning with a complete evaluation of the patient, including medical history, comorbidities that influence wound healing, glycemic control, and issues specific to the ulcer. 3 The recommendations also state that an evaluation should include a physical examination with neurologic, musculoskeletal, vascular, and laboratory assessment, as well as a review of nutritional status. Additional attention should be paid to factors that may have led to wound formation or that may impair healing.3
The consensus recommendations state that the evaluation must consider dermatological changes, ulcer characteristics, wound edges, wound bed, wound base, periwound skin, exudate, presence of necrosis, and any associated pain, as well as a probe for sinus tracts or a positive probe-to-bone test.3 The classic signs and symptoms of infection—heat, pain, redness, and swelling—are not always present or may be diminished due to a decreased immune response with diabetes.3 Therefore, the guidelines recommend observing the ulcer for secondary signs of infection such as exudate, delayed healing, friable or discolored granulation tissue, foul odor, and pocketing at wound base.3
DFUs and the resulting complications are a tremendous financial burden to the healthcare system and society.8 A total of 85% of lower-extremity amputations are associated with diabetic complications, and almost all of these are preceded by a foot ulcer. In 2004, approximately 71,000 nontraumatic lower-limb amputations in the United States were performed on patients with diabetes.15
In 2007, the treatment of diabetes and its complications in the US generated at least $116 billion in direct costs (2007 US dollars) with at least 33% of the costs linked to treatment of foot ulcers. Compared to patients with diabetes but without foot ulcers, the cost of care for patients with diabetes and a foot ulcer is approximately
5.4 times higher in the year after the first ulcer episode and 2.8 times higher in the second year.16
In 2001, the costs of diabetes-related amputations were estimated to be $38,077 per amputation. The average costs for foot ulcer care in the United States were estimated to be $13,179 per episode, with costs increasing with severity of ulceration.15
If current trends continue, the CDC estimates that 1 in 3 Americans will develop a foot ulcer in their lifetime, highlighting the need for foot ulcer prevention programs in people living with diabetes, in order to reduce the risk of unnecessary amputations.15
8
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 8 1/7/14 4:30 PM

Figure 4: The initial evaluation of the diabetic foot ulcer must be comprehensive and systematic to ascertain the parameters that might have led to its onset and to determine the
presence of factors that can impair wound healing.17
From Frykberg RG, Zgonis T, Armstrong DG, et al. J Foot Ankle Surg. 2006;45(5 Suppl):S-19. Reprinted and adapted with permission from Elsevier.
9
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 9 1/7/14 4:30 PM

1.5 Good ulcer care
Several classification systems exist for staging foot ulcers. Although no single system has been universally adopted, the 3 classification systems used most often are the Wagner system, the University of Texas San Antonio (UTSA) system, and the PEDIS system.17
Specific to the treatment of DFUs, the recommendations include comprehensive good ulcer care with sharp debridement at frequent intervals,
infection control, local pressure off-loading, provision of a moist interactive wound-healing environment, and, depending on response to these treatments, consideration of advanced therapy.3
A critical component of good wound care is patient adherence to the multiple aspects of care, including dietary compliance for good glycemic control and following prescribed regimens for medications.6
DEBRIDEMENT
The chronic wound environment differs from the acute wound, which, in a nonimmunocompromised host, will usually heal.18 In addition to the decreased immune response in an individual with diabetes, chronic wounds fail to heal for multiple reasons, including local ischemia, necrotic tissue, and overwhelming bacterial load, any of which can lead to prolonged inflammatory response and delayed healing. The noxious cellular
and molecular environment that results from prolonged inflammation prohibits healthy healing through growth factor deficiencies, faulty receptor site function, and poor cell proliferation.3 Therefore, good ulcer care of a DFU requires that the chronic wound environment be addressed first through debridement. Debridement may be surgical/sharp, enzymatic (eg, collagenase), autolytic (eg, occlusive), mechanical (wet-to-dry dressing, lavage), or biologic (larval).3
Debridement: Cold steel surgical debridement initially and then as needed based on condition of the wound (maintenance)
Infection control:
• Bacterial colonization ≠ infection
• Infection is diagnosed from clinical findings whenever possible. Purulent secretions are present or >two or at least two principal symptoms of inflammation (eg, redness, warmth, swelling, and pain or tenderness)
• Given that patients with diabetes are typically immunocompromised, clinicians should also look for secondary signs of infection including exudate, delayed healing, friable granulation tissue, discolored granulation tissue, foul odor, pocketing at the wound base, and wound breakdown
• Culture: — Levine swab technique — Quantitative biopsy (for bone only) — Testing (not universally available) via polymerase chain reaction assay, oligonucleotide array
• Off-loading: — Total contact cast (TCC) — Instant TCC
Advanced therapies:
• Use 4-week treatment endpoint to assess need for advanced therapies
• If wound is not progressing toward healing (percent wound area reduction <50%), then advanced techniques should be considered
• All previous assessment and treatment standards should continue to be utilized
Table 1. Components of Good Wound Care3
From Snyder RJ, Kirsner RS, Warriner RA, Lavery LA, Hanft JR, Sheehan P. Ostomy Wound Manage. 2010;56(suppl 4):S19. Used with permission.
10
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 10 1/7/14 4:30 PM

1.7 Treatment guideline bibliography
1.6 Unacceptably low healing rates with current standard of care
Good wound care is vital in the management of a DFU but does not always result in complete healing.3,20 Statistically, despite good ulcer care, about half of all diabetic foot ulcers may still fail to heal.20 Unfortunately, wounds that do not show a progression toward closure in the first few weeks of standard ulcer care have demonstrated a low probability for successful healing.21 Even in the controlled setting of clinical trials aimed at healing persistent DFUs, the current standard of care results in low rates of healing.3 In a meta-analysis of 10 control groups from clinical trials where the controls received good standard wound care, 24.2% of DFUs healed over 12 weeks (19.5%-28.8%) and 30.9% over 20 weeks (26.6%-35.1%).22
Several adjunctive therapies have been investigated in an effort to improve the healing rate of DFUs and prevent the costly and debilitating complications of a chronic ulcer. Clinically, advanced therapies are often reserved for an advanced and poorly healing DFU. However, because clinical trials have shown that becaplermin, as well as two living-skin equivalents, accelerate DFU healing, the consensus recommendations state that advanced therapies should be considered as options early in the management of a DFU.3
Snyder RJ, Kirsner RS, Warriner RA, Lavery LA, Hanft JR, Sheehan P. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Ostomy Wound Manage. 2010;56(4Suppl):S1-S24.
Snyder RJ, Hanft JR. Diabetic foot ulcers—effects on quality of life, costs, and mortality and the role of standard wound care and advanced-care therapies in healing: a review. Ostomy Wound Manage. 2009;55:28-38.
Lipsky BA, Berendt AR, Cornia PB, et al. Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132-e173.
Steed DL, Attinger C, Colaizzi T, et al. Guidelines for the treatment of diabetic ulcers. Wound Repair Regen. 2006;14:680-692.
If surgical debridement is the method of choice, it may not need to be weekly, but should be often enough to prevent the accumulation of necrotic or fibrinous tissues. Frequent debridement changes the wound physiology by removing nonviable tissue, matrix metalloproteinases, and biofilm, and promotes a healthy wound environment with a greater production of growth factors.3 Dressings that maintain a moist wound but control excess exudations are important in promoting a healthy wound environment.19
INFECTION CONTROL
DFUs that are potentially infected require additional evaluation, according to guidelines developed by the Infectious Diseases Society of America (IDSA).19 The recommendations for a patient with a suspected infected DFU include assessment of the patient’s overall health and examination of the affected foot or limb, as well as the infected wound. Osteomyelitis should be considered as a potential complication of any infected
deep or large foot ulcer, especially one that is chronic or overlies a bony prominence.19 Magnetic resonance imaging is the most specific and sensitive imaging test for osteomyelitis.3 The IDSA guidelines recommend that all infected DFUs be treated with antibiotic therapy, but caution that antibiotics without the use of comprehensive good wound care are not likely to be effective.19
OFF-LOADING
True off-loading that decreases pressure and strain rates is critical in improving the healing of a DFU. The more aggressive off-loading techniques, such as total contact casts and cast walkers, have been shown to produce significantly better healing rates than pads or shoe insoles, but effective off-loading can be obtained with an ankle brace or similar device fixed to the foot bed, if the patient adheres to the regimen. Bed rest, wheelchairs, or crutches have not been shown to improve healing rates.3
11
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 11 1/7/14 4:30 PM
PART 2
Pharmacology and biological action of growth factors in wound healing2.1 Role of growth factors in healing
Growth factors are required at each phase of healing (hemostasis, inflammation, proliferation, and remodeling) and are important during reestablishment of the integrity of the extracellular matrix, angiogenesis, and reepithelialization.23,24 Analysis of wound fluid from chronic wounds, as compared with acute surgical wounds, demonstrates increased protease levels, increased proinflammatory cytokine levels, and a reduction in growth factor levels.5 The prolonged
inflammatory response in chronic wounds and an inflammatory cell population that differs from the cell population associated with acute injury impede cell proliferation and repair.18 A series of multiple mechanisms, including decreased cell and growth factor response, leads to diminished peripheral blood flow and decreased endothelial cell proliferation, and contributes to the lack of wound healing in diabetes.25
2.2 Role of PDGF in the healing process
All phases of wound healing are controlled and regulated by growth factors.23,26 Growth factors are released by cells that are important to wound healing, including platelets, macrophages, endothelial cells, keratinocytes, smooth muscle cells, and fibroblasts. Platelet-derived growth factor (PDGF) is an integral part of this healing process. In order for PDGF to affect would healing, it has to be present at the site of the wound, and the cells in the wound area must express PDGF receptors. Early observations revealed that PDGF is released by platelets and secreted by activated macrophages, thrombin-stimulated endothelial cells, smooth muscle cells of damaged arteries, activated fibroblasts, as well as by epidermal keratinocytes, suggesting that PDGF is indeed present in the wounded area. PDGF acts on several cell types involved in wound healing. It stimulates mitogenicity and chemotaxis of fibroblasts and smooth muscle cells and
chemotaxis of neutrophils and macrophages. It also stimulates macrophages to produce and secrete other growth factors of importance for various phases in the healing process. Moreover, PDGF has been shown to stimulate production of several matrix molecules, such as fibronectin, collagen, proteoglycans, and hyaluronic acid. PDGF may also be of importance at later stages of wound healing because it stimulates contraction of collagen matrices in vitro, implicating a role in wound contraction in vivo. Moreover, PDGF stimulates the production and secretion of collagenase by fibroblasts, suggesting a role in the remodeling phase of wound healing.23
12
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 12 1/7/14 4:30 PM

2.3 PDGF—Its composition
2.4 PDGF-BB—Its role in healing
PDGF is found in human platelets and is sequestered within specialized alpha granules. These alpha granules release PDGF from the platelet during clot formation or when the platelet comes in contact with a wettable surface.28
PDGF is a dimeric protein of approximately 25 kDa and composed of 2 disulfide-linked polypeptide chains. PDGF exists in 3 different isoforms: PDGF-AA (2 alpha chains), PDGF-AB (an alpha and a beta chain),
and PDGF-BB (2 beta chains).29 PDGF-AA induces αα-receptor homodimers, PDGF-AB induces αα-receptor homodimers or αβ-receptor heterodimers, and PDGF-BB induces all 3 dimeric combinations of α- and β-receptors. Because there are differences between α- and β-receptors in their binding specificity of PDGF isoforms and in the signals they transduce, the response of a cell to PDGF stimulation will be determined by which of the two receptor types the cell expresses.23
Activation of the β-receptor stimulates chemotaxis in cell types such as fibroblasts and smooth muscle cells, which, in turn, express both α- and β-receptors, but tend to express higher levels of β-receptors. In keeping with this understanding, the homodimer PDGF-BB has been shown in preclinical studies to promote the formation of granulation tissue at the wound site and to stimulate wound healing.29
PDGF-BB initiates several steps of the healing process, including the stimulation of cell division, chemotaxis of fibroblasts and smooth muscle cells, chemotaxis of neutrophils and macrophages, and stimulation of macrophages to produce and secrete other growth factors necessary in the healing of chronic wound environments.23
Table 2. Role of PDGF in the 4 Phases of Healing23,24,27
13
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 13 1/7/14 4:30 PM

PART 3
REGRANEX® (becaplermin) Gel, 0.01% REGRANEX® (becaplermin) Gel, 0.01% is a human platelet-derived growth factor that is indicated as an adjunct to good ulcer care for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and that have an adequate blood supply.30 Becaplermin is a recombinant human PDGF-BB isoform in a sodium carboxymethylcellulose gel.29
The efficacy of REGRANEX® Gel has not been established for the treatment of pressure ulcers and venous stasis ulcers and has not been evaluated for the treatment of diabetic neuropathic ulcers that do not extend through the dermis into subcutaneous tissue (Stage I or II, IAET staging classification) or ischemic diabetic ulcers.30
The effects of REGRANEX® Gel on exposed joints, tendons, ligaments, and bone have not been established in humans.30
REGRANEX® Gel is a non-sterile, low bioburden preserved product. Therefore, it should not be used in wounds that close by primary intention.30
An analysis of DFU healing rates synthesized from the reported results of 4 clinical trials of becaplermin determined that administration of becaplermin gel, in conjunction with good wound care, increased the probability of healing by 39% compared with placebo gel (50% vs 36%).29
Figure 5. A schematic representation of the PDGF-BB protein molecule31
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
14
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 14 1/7/14 4:30 PM

PART 4
Boxed WarningAs with all growth factors, there is a potential risk for cell proliferation. In a retrospective study of a medical claims database, cancer rates and overall cancer mortality were compared between 1,622 patients who used REGRANEX® Gel and 2,809 matched comparators. Estimates of the incidence rates reported below maybe under-reported due to limited follow-up for each individual. The incidence rate for all cancers was 10.2 per 1,000 person years for patients treated with REGRANEX® Gel and 9.1 per 1,000 person years for the comparators. Adjusted for several possible confounders, the rate ratio was 1.2 (95% confidence interval 0.7-1.9). Types of cancer varied and were remote from the site of treatment. The incidence rate for mortality from all cancers was 1.6 per 1,000 person years for those who received REGRANEX® Gel and 0.9 per 1,000 person years for the comparators. The adjusted rate ratio was 1.8 (95% confidence interval 0.7-4.9).30
As a result, the FDA required the addition of the following Boxed Warning to the product information30:
WARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCY
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study.
REGRANEX® Gel should only be used when the benefits can be expected to outweigh the risks. REGRANEX® Gel should be used with caution in patients with known malignancy.
Figure 5. A schematic representation of the PDGF-BB protein molecule31
Indications and usage:
REGRANEX® (becaplermin) Gel is indicated for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and have an adequate blood supply. REGRANEX® Gel is indicated as an adjunct to, and not a substitute for, good ulcer care practices.
Limitations of use:
• The efficacy of REGRANEX® Gel has not been established for the treatment of pressure ulcers and venous stasis ulcers
• The effects of REGRANEX® Gel on exposed joints, tendons, ligaments, and bone have not been established in humans
• REGRANEX® Gel is a non-sterile, low bioburden preserved product that should not be used in wounds that close by primary intention
REGRANEX® Gel is contraindicated in patients with known neoplasm(s) at the site(s) of application. REGRANEX® Gel is contraindicated in patients with known hypersensitivity to any component of the product (e.g., parabens).
Malignancies distant from the site of application have been reported in both a clinical study and in postmarketing use.
In clinical trials, erythematous rashes occurred in 2% of patients treated with REGRANEX® Gel or placebo; none occurred in patients receiving good ulcer care alone. Burning sensation at the site of application and erythema have been reported during post-approval use of REGRANEX® Gel.
15
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 15 1/7/14 4:30 PM

PART 5
Contraindications/warnings and precautions/drug interactions/use in specific populations/clinical pharmacology/toxicology/patient counseling information30
CONTRAINDICATIONS
REGRANEX® Gel is contraindicated in patients with known neoplasm(s) at the site(s) of application.
WARNINGS AND PRECAUTIONS
Cancer and Cancer Mortality
REGRANEX® Gel contains becaplermin, a recombinant human platelet-derived growth factor, which promotes cellular proliferation and angiogenesis. The benefits and risks of becaplermin treatment should be carefully evaluated before prescribing. Becaplermin should be used with caution in patients with a known malignancy.
Malignancies distant from the site of application have occurred in becaplermin users in both a clinical study and postmarketing use, and an increased rate of death from systemic malignancies was seen in patients who have received 3 or more tubes of REGRANEX® Gel.
In a follow-up study, 491 (75%) of 651 subjects from two randomized, controlled trials of becaplermin gel 0.01% were followed for a median of approximately 20 months to identify malignancies diagnosed after the end of the trials. Eight of 291 subjects (3%) from the becaplermin group and two of 200 subjects (1%) from the vehicle/standard of care group were diagnosed with cancers during the follow-up period, a relative risk of 2.7 (95% confidence interval 0.6-12.8). The types of cancers varied and all were remote from the treatment site.
In a retrospective study of a medical claims database, cancer rates and overall cancer mortality were compared between 1,622 patients who used REGRANEX® Gel and 2,809 matched comparators.
Estimates of the incidence rates reported below may be under-reported due to limited follow-up for each individual.
The incidence rate for all cancers was 10.2 per 1,000 person years for patients treated with REGRANEX® Gel and 9.1 per 1,000 person years for the comparators. Adjusted for several possible confounders, the rate ratio was 1.2 (95% confidence interval 0.7-1.9). Types of cancers varied and were remote from the site of treatment.
The incidence rate for mortality from all cancers was 1.6 per 1,000 person years for those who received REGRANEX® Gel and 0.9 per 1,000 person years for the comparators. The adjusted rate ratio was 1.8 (95% confidence interval 0.7-4.9).
The incidence rate for mortality from all cancers among patients who received 3 or more tubes of REGRANEX® Gel was 3.9 per 1,000 person years and 0.9 per 1,000 person years in the comparators. The adjusted rate ratio for cancer mortality among those who received 3 or more tubes relative to those who received none was 5.2 (95% confidence interval 1.6-17.6).
Application Site Reactions
If application site reactions occur, the possibility of sensitization or irritation caused by parabens or m-cresol should be considered. Consider interruption or discontinuation and further evaluation (eg, patch testing) as dictated by clinical circumstances.
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
16
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 16 1/7/14 4:30 PM

DRUG INTERACTIONS
It is not known if REGRANEX® Gel interacts with other topical medications applied to the ulcer site. The use of REGRANEX® Gel with other topical drugs has not been studied.
USE IN SPECIFIC POPULATIONS
Pregnancy
Pregnancy Category C. There are no adequate and well-controlled studies in pregnant women treated with REGRANEX® Gel. REGRANEX® Gel should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Animal reproduction studies have not been conducted with REGRANEX® Gel.
Nursing Mothers
It is not known whether becaplermin is excreted in human milk. Because many drugs are secreted in human milk, caution should be exercised when REGRANEX® Gel is administered to nursing women.
Pediatric Use
Safety and effectiveness of REGRANEX® Gel in pediatric patients below the age of 16 years have not been established.
Geriatric Use
Among patients receiving any dose of REGRANEX® Gel in clinical studies of diabetic lower extremity ulcers, 150 patients were 65 years of age and older. No overall differences in safety or effectiveness were observed between patients <65 years of age and patients ≥65 years of age. The number of patients aged 75 and older were insufficient (n=34) to determine whether they respond differently from younger patients.
CLINICAL PHARMACOLOGY
Mechanism of Action
REGRANEX® Gel has biological activity similar to that of endogenous platelet-derived growth factor, which includes promoting the chemotactic recruitment and proliferation of cells involved in wound repair and enhancing the formation of granulation tissue.
Pharmacodynamics
Clinical pharmacodynamic studies have not been conducted.
Pharmacokinetics
Ten patients with Stage III or IV (as defined in the International Association of Enterostomal Therapy (IAET) guide to chronic wound staging) lower extremity diabetic ulcers received topical applications of becaplermin gel 0.01% at a dose range of 0.32-2.95 μg/kg (7 μg/cm2) daily for 14 days. Six patients had non-quantifiable PDGF levels at baseline and throughout the study, two patients had PDGF levels at baseline, which did not increase substantially, and two patients had PDGF levels that increased sporadically above their baseline values during the 14-day study period.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
Becaplermin was not genotoxic in a battery of in vitro assays (including those for bacterial and mammalian cell point mutation, chromosomal aberration, and DNA damage/repair). Becaplermin was also not mutagenic in an in vivo assay for the induction of micronuclei in mouse bone marrow cells.
Carcinogenesis and reproductive toxicity studies have not been conducted with REGRANEX® Gel.
Animal Toxicology and/or Pharmacology
In nonclinical studies, rats injected at the metatarsals with 3 or 10 mcg/site (approximately 60 or 200 mcg/kg) of becaplermin every other day for 13 days displayed histological changes indicative of accelerated bone remodeling consisting of periosteal hyperplasia and subperiosteal bone resorption and exostosis. The soft tissue adjacent to the injection site had fibroplasia with accompanying mononuclear cell infiltration reflective of the ability of PDGF to stimulate connective tissue growth.
17
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 17 1/7/14 4:30 PM

PATIENT COUNSELING INFORMATION
Counsel patients to review and discuss any questions or concerns with their healthcare provider before starting REGRANEX® Gel and at regular intervals while receiving REGRANEX® Gel.
Patients should be advised that they should read the medication guide; hands should be washed thoroughly before applying REGRANEX® Gel; the tip of the tube should not come into contact with the ulcer or any other surface; the tube should be recapped tightly after each use; a cotton swab, tongue depressor, or other application aid should be used to apply REGRANEX® Gel; REGRANEX® Gel should only be applied once a day in a carefully measured quantity. The measured quantity of gel should be spread evenly over the ulcerated area to yield a thin continuous layer of approximately 1/16 of an inch thickness. The measured length of the gel to be squeezed from the tube should be adjusted according to the size of the ulcer. The amount of REGRANEX® Gel to be applied daily should be recalculated at weekly or biweekly intervals by the physician or wound care giver.
Step-by-step instructions for application of REGRANEX® Gel are as follows:
• Squeeze the calculated length of gel onto a clean, firm, nonabsorbable surface (eg, wax paper).
• With a clean cotton swab, tongue depressor, or similar application aid, spread the measured REGRANEX® Gel over the ulcer surface to obtain an even layer.
• Cover with a saline moistened gauze dressing.
— After approximately 12 hours, the ulcer should be gently rinsed with saline or water to remove residual gel and covered with a saline-moistened gauze dressing (without REGRANEX® Gel);
— It is important to use REGRANEX® Gel together with a good ulcer care program, including a strict non-weight-bearing program;
— Excess application of REGRANEX® Gel has not been shown to be beneficial;
— REGRANEX® Gel should be stored in the refrigerator. Do not freeze REGRANEX® Gel;
— REGRANEX® Gel should not be used after the expiration date on the bottom, crimped end of the tube.
Important Safety Information
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study.
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
18
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 18 1/7/14 4:30 PM

PART 6
Clinical efficacy6.1 Phase 3 studies
The importance of utilizing advanced therapies is well documented. Sometimes, however, clinicians use these therapies as a last resort, and may not be sure how soon to use them in the wound healing process.3 The effects of REGRANEX® Gel on the incidence of and time to complete healing in lower extremity diabetic ulcers were assessed in 4 randomized controlled studies. Of 922 patients studied, 478 received either REGRANEX® Gel 0.003% or 0.01%. All study participants had lower extremity diabetic neuropathic ulcers that extended into the subcutaneous tissue or beyond (Stages III and IV of the IAET guide to chronic wound staging). A total of 93% of the patients enrolled in these 4 trials had foot ulcers. The remaining 7% of the patients had ankle or leg ulcers. The diabetic ulcers were of at least 8 weeks’ duration and had an adequate blood supply. In the 4 trials, the median ulcer
size at baseline ranged from 1.4 cm2 to 3.5 cm2. All treatment groups received a program of good ulcer care consisting of initial complete sharp debridement, a non-weight-bearing regimen, systemic treatment for wound-related infection if present, moist saline dressings changed twice a day, and additional debridement as necessary. Patients were treated until complete healing, or for a period of up to 20 weeks. Patients were considered a treatment failure if their ulcer did not show an approximately 30% reduction in initial ulcer area after 8 to 10 weeks of REGRANEX® Gel therapy. The primary endpoint was incidence of complete ulcer closure within 20 weeks for all treatment arms. In each study, REGRANEX® Gel in conjunction with good ulcer care was compared to placebo gel plus good ulcer care or good ulcer care alone.30
Figure 6. Incidence of Complete Healing With REGRANEX® Gel vs Placebo Gel Across 4 Studies30
19
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 19 1/7/14 4:30 PM

The following summaries in this section highlight the details from the becaplermin phase 3 studies.
Summary of Steed DL et al. J Vasc Surg. 1995.
Steed and colleagues randomized 118 patients from 10 treatment centers in the US to receive either topical becaplermin 30 mcg/g or placebo gel. Participants had to have at least one infection-free ulcer with a surface area between 1 and 100 cm2. One to 2 weeks before randomization, the target ulcer was given a complete sharp debridement to remove all callus, necrotic tissue, and chronic granulation tissue. For participants in both groups, further surgical debridement was performed on ulcers as required throughout the treatment period. Becaplermin gel or placebo gel was applied to the target ulcer every 24 hours at a dose equivalent to approximately 2.2 mcg of becaplermin per square centimeter of ulcer surface area for at least 20 weeks or until complete wound healing was achieved, whichever occurred first. Complete healing was the primary endpoint and defined as 100% wound closure, no drainage present, and no dressing required. Patients (or caregivers) were instructed on the procedure for study gel application, dressing changes, and good wound care, and were then followed as outpatients. Sixty-one patients were randomized to receive becaplermin and 57 patients were randomized to receive placebo. There were no statistically significant differences between the 2 groups with respect to race, duration of ulcer, area of ulcer, and transcutaneous partial pressure of oxygen at the dorsum and wound edge. Fourteen of 61 (23%) becaplermin-treated patients and 18 of 57 (31.6%) placebo-treated patients discontinued the study before complete wound healing or 20 weeks of treatment.32
Complete wound healing was significantly greater in patients randomized to receive becaplermin compared with patients who received treatment with placebo. Twenty-nine of 61 (48%) patients in the becaplermin treatment group achieved complete wound healing during the study compared with only 14 of 57 (25%) patients in the placebo treatment group (P=0.01). The median reduction in wound area in the treatment
group was 98.8% compared with 82.1% in the group given placebo (P=0.09), and the rate of healing was significantly faster in the becaplermin treatment group compared to the placebo treatment group. From approximately Day 68 through the trial end, the becaplermin group demonstrated a 30- to 40-day decreased difference in time to complete wound healing compared with the placebo treatment group (P=0.01).32
When comparing the 2 treatment groups, there was no statistical difference in the number of times debridement was performed. A trend toward a greater recurrence rate of the target ulcer in the placebo treatment group (46%) compared with the becaplermin treatment group (26%) after a mean follow-up of 8.6 weeks did not reach statistical significance.32
Summary of Wieman TJ et al. Diabetes Care. 1998.
A multicenter, double-blind, placebo-controlled trial by Wieman and colleagues evaluated 2 concentrations of becaplermin gel, 30 mcg/g and 100 mcg/g against a placebo gel in a randomized phase 3 trial. A total of 382 patients with lower extremity ulcers who met the inclusion criteria from 23 treatment centers in the US participated in the study. Prior to randomization, sharp debridement was performed to remove all nonviable tissue and callus. Following debridement, patients were excluded if osteomyelitis was present or if the target ulcer was less than 1 cm, greater than 40 cm, or had a surface area greater than 100 cm2. Standard good wound care, including sharp debridement, was provided as needed to all participants throughout the study period. Patients were randomized to 1 of 3 parallel treatment groups with one group (n=124) treated with becaplermin 30 mcg/g, a second group (n=132) treated with becaplermin 100 mcg/g, and a third group (n=127) treated with a gel formulation that was identical to the one containing becaplermin. The primary efficacy endpoint was the percentage of patients with complete ulcer healing at the end of the 20-week study period, and the secondary endpoint was the time to achieve complete healing.33
Important Safety Information
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study.
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
20
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 20 1/7/14 4:30 PM
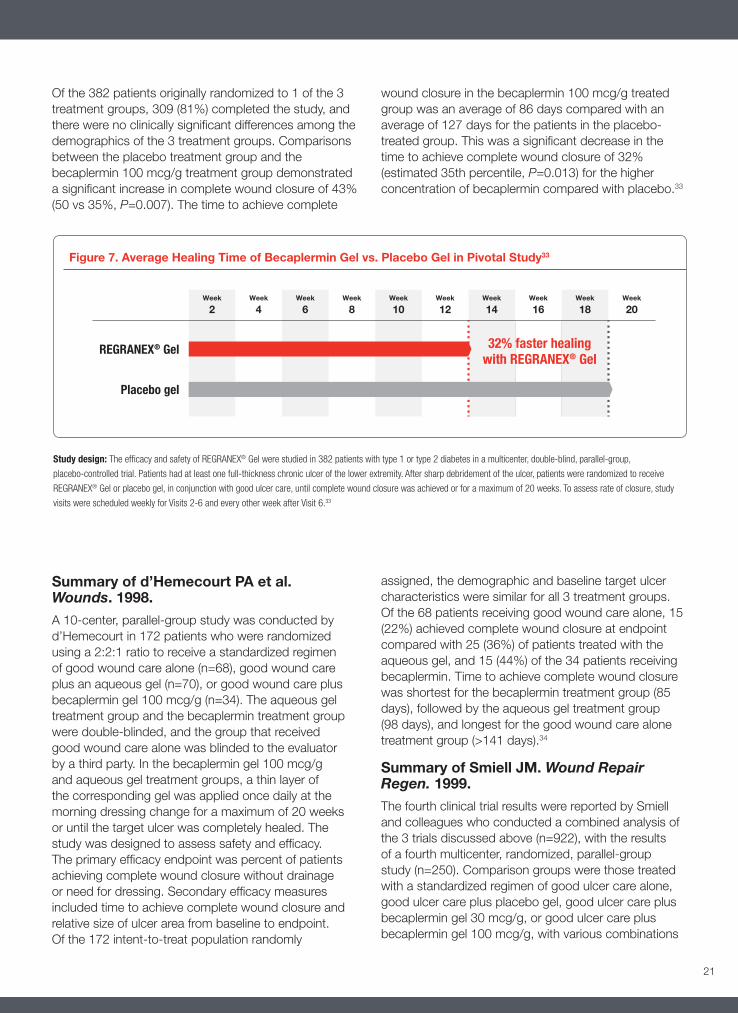
Figure 7. Average Healing Time of Becaplermin Gel vs. Placebo Gel in Pivotal Study33
Summary of d’Hemecourt PA et al. Wounds. 1998.
A 10-center, parallel-group study was conducted by d’Hemecourt in 172 patients who were randomized using a 2:2:1 ratio to receive a standardized regimen of good wound care alone (n=68), good wound care plus an aqueous gel (n=70), or good wound care plus becaplermin gel 100 mcg/g (n=34). The aqueous gel treatment group and the becaplermin treatment group were double-blinded, and the group that received good wound care alone was blinded to the evaluator by a third party. In the becaplermin gel 100 mcg/g and aqueous gel treatment groups, a thin layer of the corresponding gel was applied once daily at the morning dressing change for a maximum of 20 weeks or until the target ulcer was completely healed. The study was designed to assess safety and efficacy. The primary efficacy endpoint was percent of patients achieving complete wound closure without drainage or need for dressing. Secondary efficacy measures included time to achieve complete wound closure and relative size of ulcer area from baseline to endpoint. Of the 172 intent-to-treat population randomly
assigned, the demographic and baseline target ulcer characteristics were similar for all 3 treatment groups. Of the 68 patients receiving good wound care alone, 15 (22%) achieved complete wound closure at endpoint compared with 25 (36%) of patients treated with the aqueous gel, and 15 (44%) of the 34 patients receiving becaplermin. Time to achieve complete wound closure was shortest for the becaplermin treatment group (85 days), followed by the aqueous gel treatment group (98 days), and longest for the good wound care alone treatment group (>141 days).34
Summary of Smiell JM. Wound Repair Regen. 1999.
The fourth clinical trial results were reported by Smiell and colleagues who conducted a combined analysis of the 3 trials discussed above (n=922), with the results of a fourth multicenter, randomized, parallel-group study (n=250). Comparison groups were those treated with a standardized regimen of good ulcer care alone, good ulcer care plus placebo gel, good ulcer care plus becaplermin gel 30 mcg/g, or good ulcer care plus becaplermin gel 100 mcg/g, with various combinations
Study design: The efficacy and safety of REGRANEX® Gel were studied in 382 patients with type 1 or type 2 diabetes in a multicenter, double-blind, parallel-group,
placebo-controlled trial. Patients had at least one full-thickness chronic ulcer of the lower extremity. After sharp debridement of the ulcer, patients were randomized to receive
REGRANEX® Gel or placebo gel, in conjunction with good ulcer care, until complete wound closure was achieved or for a maximum of 20 weeks. To assess rate of closure, study
visits were scheduled weekly for Visits 2-6 and every other week after Visit 6.33
Of the 382 patients originally randomized to 1 of the 3 treatment groups, 309 (81%) completed the study, and there were no clinically significant differences among the demographics of the 3 treatment groups. Comparisons between the placebo treatment group and the becaplermin 100 mcg/g treatment group demonstrated a significant increase in complete wound closure of 43% (50 vs 35%, P=0.007). The time to achieve complete
wound closure in the becaplermin 100 mcg/g treated group was an average of 86 days compared with an average of 127 days for the patients in the placebo-treated group. This was a significant decrease in the time to achieve complete wound closure of 32% (estimated 35th percentile, P=0.013) for the higher concentration of becaplermin compared with placebo.33
21
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 21 1/7/14 4:30 PM

6.2 Adverse reactions
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.30
In a follow-up study from two randomized, controlled trials, an increased rate of cancer remote from the becaplermin treatment site was observed in subjects treated with REGRANEX® Gel.30
In clinical trials, erythematous rashes occurred in 2% of patients treated with REGRANEX® Gel (and good ulcer care) or placebo (and good ulcer care), and none in patients receiving good ulcer care alone. Patients treated with REGRANEX® Gel did not develop neutralizing antibodies against becaplermin.30
Clinical trial data also indicate that treatment with becaplermin gel was associated with adverse events that were similar in incidence and severity across all
study groups. In a pivotal clinical trial, 382 patients were evaluated for safety, including patients receiving becaplermin 100 mcg/g, becaplermin gel 30 mcg/g, and placebo gel. All patients also received standard good wound care. Treatment-emergent adverse events were generally related to the DFU or the patients’ diabetes, and the most common events were infection, cellulitis, skin ulceration, and osteomyelitis.33
Postmarketing Experience
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study.
Burning sensation and erythema have been reported during post-approval use of REGRANEX® Gel. Because post-approval adverse reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to the drug.30
of these regimens among the 4 studies. Statistical techniques were used in the combined analysis to establish homogeneity of treatment comparisons across studies. The primary outcome was a more precise assessment of the efficacy of becaplermin gel, with a focus on the difference between becaplermin 100 mcg/g and placebo gel.29
Homogeneity of treatment responses across the 4 studies was established for intent-to-treat population who had a baseline ulcer area of less than 10 cm2.
(n=874; 95%), and subsequent combined analyses were based on this population subgroup. The higher concentration of becaplermin of 100 mcg/g compared with placebo gel demonstrated a significantly greater probability of complete healing (P=0.007). Treatment with becaplermin gel 100 mcg/g significantly decreased the time to heal, with the 35th percentile of time to healing 30% faster compared with treatment with placebo gel (14.1 weeks vs 20.1 weeks, respectively; Kaplan-Meier estimates).29
Important Safety Information
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study.
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
22
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 22 1/7/14 4:30 PM

6.3 Clinical trial summaries
Clinical efficacy and safety trials of becaplermin
Steed DL and the Diabetic Ulcer Study Group. Clinical evaluation of recombinant platelet-derived growth factor for the treatment of lower extremity diabetic ulcers.32
d’Hemecourt PA, Smiell JM, Karim MR. Sodium carboxymethylcellulose aqueous-based gel vs becaplermin gel in patients with nonhealing lower extremity diabetic ulcers.34
Wieman TJ, Smiell JM, Su Y. Efficacy and safety of a topical gel formulation of recombinant human platelet-derived growth factor-BB (becaplermin) in patients with chronic neuropathic diabetic ulcers. A phase III randomized placebo-controlled double-blind study.33
Smiell JM, Wieman TJ, Steed DL, Perry BH, Sampson AR, Schwab BH. Efficacy and safety of becaplermin (recombinant human platelet-derived growth factor-BB) in patients with nonhealing, lower extremity diabetic ulcers: a combined analysis of four randomized studies.29
Robson MC, Payne WG, Garner WL, et al. Integrating the results of Phase IV (postmarketing) clinical trial with 4 previous trials reinforces the position that Regranex (becaplermin) Gel 0.01% is an effective adjunct to the treatment of diabetic foot ulcers.35
Mannari RJ, Payne WG, Ochs DE, Walusimbi M, Blue M, Robson MC. Successful treatment of recalcitrant, diabetic heel ulcers with topical becaplermin (rhPDGF-BB) gel.36
Margolis DJ, Bartus C, Hoffstad O, Malay S, Berlin JA. Effectiveness of recombinant human platelet-derived growth factor for the treatment of diabetic neuropathic foot ulcers.9
Table 3. Treatment-Emergent Adverse Reactions Reported in ≥5% of Patients in Pivotal Study33
Study design: The efficacy and safety of REGRANEX® Gel were studied in 382 patients with type 1 or type 2 diabetes in a multicenter, double-blind, parallel-group,
placebo- controlled trial. Patients were randomized to receive REGRANEX® Gel or placebo gel in conjunction with good ulcer care, until complete wound closure was
achieved or for a maximum of 20 weeks.33
Safety results: Most adverse events reported during the study were related to the ulcers, underlying conditions, or age of the patient. The incidences of the most common
treatment-emergent adverse events across all treatment groups are shown in Table 4. The incidence of treatment-emergent adverse events, particularly infection, such as
osteomyelitis and cellulitis, was similar across all treatment groups.33
Placebo gelBecaplermin gel
30 µg/gBecaplermin gel
100 µg/g
n 127 132 123
Disorders by body system or preferred term
Application site (%)Cellulitis 15 10 16
General (%)EdemaPain
4.71.6
5.3 6.1
5.75.7
Musculoskeletal system (%)Osteomyelitis 7.1 5.3 10
Resistance mechanism (%)Infection 20 20 20
Skin and appendage (%)Bullous eruptionSkin disorderSkin ulceration
3.13.99.4
5.33.011
4.95.715
Treatment-emergent AEs were those that occurred in ≥5% of patients.
23
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 23 1/7/14 4:30 PM

PART 7
Dosage and administrationREGRANEX® Gel is applied once daily. The site(s) of application are covered by a saline moistened dressing and left in place for approximately 12 hours. The dressing is then removed and the ulcer rinsed with saline or water to remove residual gel and covered again with a second moist dressing (without REGRANEX® Gel) for the remainder of the day. REGRANEX® Gel should be applied once daily to the ulcer until complete healing has occurred.30
The amount of REGRANEX® Gel to be applied should be recalculated by the physician or wound caregiver at weekly or biweekly intervals depending on the rate of change in ulcer area.30
If the ulcer does not decrease in size by approximately 30% after 10 weeks of treatment or complete healing has not occurred in 20 weeks, continued treatment with REGRANEX® Gel should be reassessed.30
When reassessing, it is important for healthcare providers to be aware of the Boxed Warning printed on the REGRANEX® Gel label30:
WARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCY
An increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX® Gel in a postmarketing retrospective cohort study. REGRANEX® Gel should only be used when the benefits can be expected to outweigh the risks. REGRANEX® Gel should be used with caution in patients with known malignancy.
REGRANEX® Gel is supplied in 15-gram tubes. A 12-month retrospective database analysis of 121 patients with a DFU illustrated that, on average, 1.5 tubes per patient were used.37
REGRANEX® Gel should be applied on a clean, nonabsorbable surface, such as wax paper, at home by the patient or caregiver once daily. An application aid is used to spread a thin, even layer (1/16 inch) over the entire ulcer area. Between applications, REGRANEX® Gel should be stored in the refrigerator.30
The amount of REGRANEX® Gel to be applied will vary depending upon the size of the ulcer area and should be calculated by the treating physician. The calculation consists of multiplying the longest part of the ulcer by the widest part of the ulcer in either inches or centimeters. When calculating in inches, the result is multiplied by 0.6. If calculated in centimeters, the result is divided by 4.30
Figure 8. Sample Dose Calculation for REGRANEX® Gel30
15 g REGRANEX® Gel tube: The dosing calculation
Centimeters: Ulcer length x ulcer width ÷ 4 Inches: Ulcer length x ulcer width x 0.6
Example calculation:
(4 cm x 2 cm) ÷ 4 = 2 cm Apply 2 cm of gel
(1 in x 2 in) x 0.6 = 1 1/4 in Apply 1 1/4 in of gel
Please see Important Safety Information on page 5 and accompanying full Prescribing Information, including Boxed Warning and Medication Guide.
24
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 24 1/7/14 4:30 PM

SummaryPeople living with diabetes are at risk for developing serious complications—foot ulcerations are one of the most common.4 Discomfort and disability are not the only consequences of ulceration; a DFU can lead to other morbidities, as well as increased mortality, in a significant number of individuals.3
In addition, the economic impact to society is considerable. For example, in 2001, diabetes-related foot ulcers and amputations were estimated to cost US healthcare payers $116 billion. On average, medical expenditures are thought to be 2.3 times higher in people with diabetes than without. Many of these expenditures are related to comorbidities associated with diabetes, such as diabetic foot ulcer and lower extremity amputation.38
Statistically, despite good ulcer care, about half of all diabetic foot ulcers may still fail to heal.7 Clinically, advanced therapies are often reserved for an advanced and poorly healing DFU. However, because clinical trials have shown that advanced therapies accelerate DFU healing, consensus recommendations state that they should be considered as options earlier in the management of a DFU.3
REGRANEX® (becaplermin) Gel, 0.01% is the only human platelet-derived growth factor that is indicated as an adjunct to good ulcer care for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and that have an adequate blood supply.30
Figure 8. Sample Dose Calculation for REGRANEX® Gel30
25
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 25 1/7/14 4:30 PM

References1. Wild S, Roglic G, Green A, Sicree R, King H. Global
prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047-1053.
2. Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the U.S. Diabetes Care. 2009;32:2225-2229.
3. Snyder RJ, Kirsner RS, Warriner RA, Lavery LA, Hanft JR, Sheehan P. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Ostomy Wound Manage. 2010;56(Suppl 4):S1-S24.
4. Kirsner RS. The standard of care for evaluation and treatment of diabetic foot ulcers. University of Michigan Medical School. The University of Michigan Health System’s Educational Services for Nursing. Barry University School of Podiatric Medicine 2010. http://www.barry.edu/includes/docs/continuing-medical-education/diabetic.pdf. Accessed July 9, 2012.
5. Mustoe TA, O’Shaughnessy K, Kloeters O. Chronic wound pathogenesis and current treatment strategies: a unifying hypothesis. Plast Reconstr Surg. 2006;117 (Suppl.): 35S-41S.
6. American Diabetes Association (ADA). Consensus development conference report on diabetic foot wound care. Diabetes Care. 1999;22(8):1354-1360. Presented at: Consensus Development Conference on Diabetic Foot Wound Care; April 7-8, 1999; Boston, MA.
7. Peppa M, Uribarri J, Vlassara H. Glucose, advanced glycation end products, and diabetes complications: what is new and what works. Clin Diabetes. 2003;21(4):186-187.
8. Snyder RJ, Hanft JR. Diabetic foot ulcers—effects on quality of life, costs, and mortality and the role of standard wound care and advanced-care therapies in healing: a review. Ostomy Wound Manage. 2009;55:28-38.
9. Margolis DJ, Bartus C, Hoffstad O, Malay S, Berlin JA. Effectiveness of recombinant human platelet-derived growth factor for the treatment of diabetic neuropathic foot ulcers. Wound Repair Regen. 2005;13:531-536.
10. Sibbald RG, Torrance G, Hux M, Attard C, Milkovich N. Cost-effectiveness of becaplermin for nonhealing neuropathic diabetic foot ulcers. Ostomy Wound Manage. 2003;49:76-84.
11. Walters DP, Gatling W, Mullee MA, et al. The distribution and severity of diabetic foot disease: a community study with comparison to a non-diabetic group. Diabetes Med. 1992;9:354-358.
12. Harrington C, Zagari MJ, Corea J, Klitenic J. A cost analysis of diabetic lower-extremity ulcers. Diabetes Care. 2000;23:1333-1338.
13. Lavery LA, Armstrong DG, Wunderlich RP, Tredwell J, Boulton AJM. Diabetic foot syndrome: evaluating the prevalence and incidence of foot pathology in Mexican Americans and non-Hispanic whites from a diabetes management cohort. Diabetes Care. 2003;26:1435-1438.
14. Iversen MM, Tell GS, Riise T, et al. History of foot ulcer increases mortality among individuals with diabetes: ten-year follow-up of the Nord-Trøndelag Health Study, Norway. Diabetes Care. 2009;32:2193-2199.
15. Carls GS, Gibson TB, Driver VR, et al. The economic value of specialized lower-extremity medical care by podiatric physicians in the treatment of diabetic foot ulcers. J Am Podiatr Med Assoc. 2011;101(2):93-115.
16. Driver VR, Fabbi M, Lavery LA, Gibbons G. The costs of diabetic foot: the economic case for the limb salvage team. J Vasc Surg. 2010;52(3 Suppl):17S-22S.
17. Frykberg RG, Zgonis T, Armstrong DG, et al; American College of Foot and Ankle Surgeons. Diabetic foot disorders: A clinical practice guideline (2006 revision). J Foot Ankle Surg. 2006;45(5 Suppl):S1-S66.
18. Guo S, DiPietro LA. Factors affecting wound healing. J Dent Res. 2010;89(3):219-229.
19. Lipsky BA, Berendt AR, Cornia PB, et al; Infectious Diseases Society of America. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132-e173.
20. Papanas N, Maltezos E. Benefit-risk assessment of becaplermin in the treatment of diabetic foot ulcers. Drug Saf. 2010;33(6):455-461.
26
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 26 1/7/14 4:30 PM

21. Steed DL, Attinger C, Colaizzi T, et al. Guidelines for the treatment of diabetic ulcers. Wound Repair Regen. 2006;14:680-692.
22. Margolis DJ, Kantor J, Berlin JA. Healing of diabetic neuropathic foot ulcers receiving standard treatment. A meta-analysis. Diabetes Care. 1999;22:692-695.
23. Heldin CH, Westermark B. Mechanism of action and in vivo role of platelet-derived growth factor. Physiol Rev. 1999;79:1283-1316.
24. Diegelmann RF, Evans MC. Wound healing: an overview of acute, fibrotic and delayed healing. Front Biosci. 2004;9:283-289.
25. Kolluru GK, Bir SC, Kevil CG. Endothelial dysfunction and diabetes: effects on angiogenesis, vascular remodeling, and wound healing. Int J Vasc Med. 2012;2012:1-30.
26. Steed DL. The role of growth factors in wound healing. Surg Clinic N Am. 1997;77:575-586.
27. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Heal Soc. 2008;16(5):585-601.
28. Stiles SD. The molecular biology of platelet-derived growth factors. Cell. 1983;33:653-655.
29. Smiell JM, Wieman TJ, Steed DL, Perry BH, Sampson AR, Schwab BH. Efficacy and safety of becaplermin (recombinant human platelet-derived growth factor-BB) in patients with nonhealing, lower extremity diabetic ulcers: a combined analysis of four randomized studies. Wound Repair Regen. 1999;7:335-346.
30. REGRANEX Gel Prescribing Information.
31. Smith & Nephew. Mechanism of action. http://www.regranex.com/about-overview.php. Accessed October, 13, 2013
32. Steed DL. Clinical evaluation of recombinant platelet-derived growth factor for the treatment of lower extremity diabetic ulcers. Diabetic Ulcer Study Group. J Vasc Surg. 1995;21:71-81.
33. Wieman TJ, Smiell JM, Su Y. Efficacy and safety of a topical gel formulation of recombinant human platelet-derived growth factor-BB (becaplermin) in patients with chronic neuropathic diabetic ulcers. A phase III randomized placebo-controlled double-blind study. Diabetes Care. 1998;21:822-827.
34. d’Hemecourt PA, Smiell JM, Karim MR. Sodium carboxymethylcellulose aqueous-based gel vs. becaplermin gel in patients with nonhealing lower extremity diabetic ulcers. Wounds. 1998;10:69-75.
35. Robson MC, Payne WG, Garner WL, Biundo J, Giacalone VF, Cooper DM, Ouyang P. Integrating the results of Phase IV (postmarketing) clinical trial with four pervious trials reinforces the position that Regranex (becaplermin) Gel 0.01% is an effective adjunct to the treatment of diabetic foot ulcers. J Applied Res. 2005;5:35-45.
36. Mannari RJ, Payne WG, Ochs DE, Walusimbi M, Blue M, Robson MC. Successful treatment of recalcitrant, diabetic heal ulcers with topical becaplermin (rhPDGF-BB) gel. Wounds. 2002;14:116-121.
37. Lantis JC II, Boone D, Gendics C, Todd G. Analysis of patient cost for recombinant human platelet-derived growth factor therapy as the first-line treatment of the insured patient with a diabetic foot ulcer. Adv Skin Wound Care. 2009;22:167-171.
38. Margolis DJ, Malay DS, Hoffstad OJ, et al. Economic burden of diabetic foot ulcers and amputations. Diabetic Foot Ulcers. Data Points #3 (prepared by the University of Pennsylvania DEcIDE Center, under Contract No. HHSA290200500411). Rockville, MD: Agency for Healthcare Research and Quality. January 2011. AHRQ Publication No. 10(11)-EHC009-2-EF.
27
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 27 1/7/14 4:30 PM

FULL PRESCRIBING INFORMATION
WARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCYAn increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX Gel in a postmarketing retrospective cohort study. REGRANEX Gel should only be used when the benefits can be expected to outweigh the risks. REGRANEX Gel should be used with caution in patients with known malignancy. [see Warnings and Precautions (5.1)]
1 INDICATIONS AND USAGE1.1 IndicationREGRANEX (becaplermin) Gel is indicated for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and have an adequate blood supply, when used as an adjunct to, and not a substitute for, good ulcer care practices including initial sharp debridement, pressure relief and infection control.
1.2 Limitations of UseThe efficacy of REGRANEX Gel has not been established for the treatment of pressure ulcers and venous stasis ulcers [see Clinical Studies (14)] and has not been evaluated for the treatment of diabetic neuropathic ulcers that do not extend through the dermis into subcutaneous tissue (Stage I or II, IAET staging classification) or ischemic diabetic ulcers.
The effects of becaplermin on exposed joints, tendons, ligaments, and bone have not been established in humans. [see Nonclinical Toxicology (13.2)]
REGRANEX Gel is a non-sterile, low bioburden preserved product. Therefore, it should not be used in wounds that close by primary intention.
2 DOSAGE AND ADMINISTRATIONFor topical use; not for oral, ophthalmic or intravaginal use.
The amount of REGRANEX Gel to be applied will vary depending upon the size of the ulcer area. To calculate the length of gel to apply to the ulcer, measure the greatest length of the ulcer by the greatest width of the ulcer in either inches or centimeters. To calculate the length of gel in inches, use the formula shown below in Table 1, and to calculate the length of gel in centimeters, use the formula shown below in Table 2.
Table 1: Formula to Calculate Length of Gel in Inches to Be Applied Daily
INCHES
Tube Size Formula
15g tube length × width × 0.6
2g tube (physician sample) length × width × 1.3
Using the calculation, each square inch of ulcer surface will require approximately 2/3 inch length of gel squeezed from a 15g tube, or approximately 1 1/3 inch length of the gel from a
FULL PRESCRIBING INFORMATION: CONTENTS*
WARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCY
1 INDICATIONS AND USAGE1.1 Indication1.2 Limitations of Use
2 DOSAGE AND ADMINISTRATION
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Cancer and Cancer
Mortality5.2 Application Site Reactions
6 ADVERSE REACTIONS6.1 Clinical Trials
Experience6.2 Postmarketing Experience
7 DRUG INTERACTIONS
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis,
Mutagenesis, Impairment of Fertility
13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
15 REFERENCES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the Full Prescribing Information are not listed.
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use REGRANEX® Gel safely and effectively. See full prescribing information for REGRANEX Gel.
REGRANEX® (becaplermin) gel for topical use. Initial U.S. Approval: 1997
WARNING: INCREASED RATE OF MORTALITY SECONDARY TO MALIGNANCYAn increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX Gel in a postmarketing retrospective cohort study. REGRANEX Gel should only be used when the benefits can be expected to outweigh the risks. REGRANEX Gel should be used with caution in patients with known malignancy. (5.1)
INDICATIONS AND USAGE
REGRANEX Gel contains becaplermin, a human platelet-derived growth factor that is indicated for the treatment of lower extremity diabetic neuropathic ulcers that extend into the subcutaneous tissue or beyond and have an adequate blood supply. REGRANEX Gel is indicated as an adjunct to, and not a substitute for, good ulcer care practices. (1.1)
Limitations of use:
• The efficacy of REGRANEX Gel has not been established for the treatment of pressure ulcers and venous stasis ulcers. (1.2)
• The effects of REGRANEX Gel on exposed joints, tendons, ligaments, and bone have not been established in humans. (1.2)
• REGRANEX Gel is a non-sterile, low bioburden preserved product. Therefore, it should not be used in wounds that close by primary intention. (1.2)
DOSAGE AND ADMINISTRATION
For topical use; not for oral, ophthalmic or intravaginal use. (2)
To calculate the length of REGRANEX Gel to apply, measure the greatest length of the ulcer by the greatest width of the ulcer in either inches or centimeters. (2)
Formula to Calculate Length of Gel to Be Applied Daily
Tube SizeInches or Centimeters
Formula
15g tube Inches: ulcer length × ulcer width × 0.6
15g tube Centimeters: ulcer length × ulcer width ÷ 4
DOSAGE FORMS AND STRENGTHS
Gel: 0.01% (3)CONTRAINDICATIONS
Known neoplasm(s) at the site(s) of application (4)
WARNINGS AND PRECAUTIONS
Malignancies distant from the site of application have been reported in both a clinical study and in postmarketing use. REGRANEX Gel should be used with caution in patients with a known malignancy. (5.1)
ADVERSE REACTIONS
Erythematous rashes occurred in 2% of patients treated with REGRANEX Gel (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch, or Healthpoint Biotherapeutics at 1-800-441-8227.
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.
Revised: 09/2012
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 28 1/7/14 4:30 PM

2g tube (physician sample). For example, if the ulcer measures 1 inch by 2 inches, then a 1 1/4 inch length of gel should be used for 15g tubes (1 × 2 × 0.6 = 1 1/4) and 2 3/4 inch gel length should be used for a 2g tube (1 × 2 × 1.3 = 2 3/4).
Table 2: Formula to Calculate Length of Gel in Centimeters to Be Applied Daily
CENTIMETERS
Tube Size Formula
15g tube length × width ÷ 4
2g tube (physician sample) length × width ÷ 2
Using the calculations for ulcer size in centimeters, each square centimeter of ulcer surface will require approximately a 0.25 centimeter length of gel squeezed from a 15g tube, or approximately a 0.5 centimeter length of gel from a 2g tube. For example, if the ulcer measures 4 cm by 2 cm, then a 2 centimeter length of gel should be used for a 15g tube [(4 × 2) ÷ 4 = 2] and a 4 centimeter length of gel should be used for a 2g tube [(4 × 2) ÷ 2 = 4].
The amount of REGRANEX Gel to be applied should be recalculated by the physician or wound caregiver at weekly or biweekly intervals depending on the rate of change in ulcer area. The weight of REGRANEX Gel from 15g tubes is 0.65g per inch length and 0.25g per centimeter length.
To apply REGRANEX Gel, the calculated length of gel should be squeezed on to a clean measuring surface, e.g., wax paper. The measured REGRANEX Gel is transferred from the clean measuring surface using an application aid and then spread over the entire ulcer area to yield a thin continuous layer of approximately 1/16 of an inch thickness. The site(s) of application should then be covered by a saline moistened dressing and left in place for approximately 12 hours. The dressing should then be removed and the ulcer rinsed with saline or water to remove residual gel and covered again with a second moist dressing (without REGRANEX Gel) for the remainder of the day. REGRANEX Gel should be applied once daily to the ulcer until complete healing has occurred. If the ulcer does not decrease in size by approximately 30% after 10 weeks of treatment or complete healing has not occurred in 20 weeks, continued treatment with REGRANEX Gel should be reassessed. The step-by-step instructions for applying REGRANEX Gel for home administration are described under “Patient Counseling Information”. [see Patient Counseling Information (17)]
3 DOSAGE FORMS AND STRENGTHSGel: 0.01%; clear, colorless to straw-colored gel
4 CONTRAINDICATIONSREGRANEX Gel is contraindicated in patients with known neoplasm(s) at the site(s) of application.
5 WARNINGS AND PRECAUTIONS5.1 Cancer and Cancer MortalityREGRANEX Gel contains becaplermin, a recombinant human platelet-derived growth factor, which promotes cellular proliferation and angiogenesis. [see Clinical Pharmacology (12.1)] The benefits and risks of becaplermin treatment should be carefully evaluated before prescribing. Becaplermin should be used with caution in patients with a known malignancy.
Malignancies distant from the site of application have occurred in becaplermin users in both a clinical study and postmarketing use, and an increased rate of death from systemic malignancies was seen in patients who have received 3 or more tubes of REGRANEX Gel.
In a follow-up study, 491 (75%) of 651 subjects from two randomized, controlled trials of becaplermin gel 0.01% were followed for a median of approximately 20 months to identify malignancies diagnosed after the end of the trials. Eight of 291 subjects (3%) from the becaplermin group and two of 200 subjects (1%) from the vehicle/standard of care group were diagnosed with cancers during the follow-up period, a relative risk of 2.7 (95% confidence interval 0.6–12.8). The types of cancers varied and all were remote from the treatment site.
In a retrospective study of a medical claims database, cancer rates and overall cancer mortality were compared between 1,622 patients who used REGRANEX Gel and 2,809 matched comparators. Estimates of the incidence rates reported below may be under-reported due to limited follow-up for each individual.
• The incidence rate for all cancers was 10.2 per 1,000 person years for patients treated with REGRANEX Gel and 9.1 per 1,000 person years for the comparators. Adjusted for several possible confounders, the rate ratio was 1.2 (95% confidence interval 0.7–1.9). Types of cancers varied and were remote from the site of treatment.
• The incidence rate for mortality from all cancers was 1.6 per 1,000 person years for those who received REGRANEX Gel and 0.9 per 1,000 person years for the comparators. The adjusted rate ratio was 1.8 (95% confidence interval 0.7–4.9).
• The incidence rate for mortality from all cancers among patients who received 3 or more tubes of REGRANEX Gel was 3.9 per 1,000 person years and 0.9 per 1,000 person years in the comparators. The adjusted rate ratio for cancer mortality among those who received 3 or more tubes relative to those who received none was 5.2 (95% confidence interval 1.6–17.6). [see Boxed Warning]
5.2 Application Site ReactionsIf application site reactions occur, the possibility of sensitization or irritation caused by parabens or m-cresol should be considered. Consider interruption or discontinuation and further evaluation (e.g. patch testing) as dictated by clinical circumstances.
6 ADVERSE REACTIONS6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
In a follow-up study from two randomized, controlled trials, an increased rate of cancer remote from the becaplermin treatment site was observed in subjects treated with REGRANEX Gel. [see Warnings and Precautions (5.1)]
In clinical trials, erythematous rashes occurred in 2% of patients treated with REGRANEX Gel (and good ulcer care) or placebo (and good ulcer care), and none in patients receiving good ulcer care alone. Patients treated with REGRANEX Gel did not develop neutralizing antibodies against becaplermin.
6.2 Postmarketing ExperienceAn increased rate of mortality secondary to malignancy was observed in patients treated with 3 or more tubes of REGRANEX Gel in a postmarketing retrospective cohort study. [see Boxed Warning and Warnings and Precautions (5.1)]
Burning sensation at the site of application and erythema have been reported during post-approval use of REGRANEX Gel. Because post-approval adverse reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to the drug.
7 DRUG INTERACTIONSIt is not known if REGRANEX Gel interacts with other topical medications applied to the ulcer site. The use of REGRANEX Gel with other topical drugs has not been studied.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyPregnancy Category C. There are no adequate and well-controlled studies in pregnant women treated with REGRANEX Gel. REGRANEX Gel should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Animal reproduction studies have not been conducted with REGRANEX Gel.
8.3 Nursing MothersIt is not known whether becaplermin is excreted in human milk. Because many drugs are secreted in human milk, caution should be exercised when REGRANEX Gel is administered to nursing women.
8.4 Pediatric UseSafety and effectiveness of REGRANEX Gel in pediatric patients below the age of 16 years have not been established.
8.5 Geriatric UseAmong patients receiving any dose of REGRANEX Gel in clinical studies of diabetic lower extremity ulcers, 150 patients were 65 years of age and older. No overall differences in safety or effectiveness were observed between patients < 65 years of age and patients ≥65 years of age. The number of patients aged 75 and older were insufficient (n=34) to determine whether they respond differently from younger patients.
10 OVERDOSAGEThere are no data on the effects of becaplermin overdose.
11 DESCRIPTIONREGRANEX Gel contains becaplermin, a recombinant human platelet-derived growth factor for topical administration. Becaplermin is produced by recombinant DNA technology by insertion of the gene for the B chain of platelet-derived growth factor (PDGF) into the yeast, Saccharomyces cerevisiae. Becaplermin has a molecular weight of approximately 25 KD and is a homodimer composed of two identical polypeptide chains that are bound together by disulfide bonds. REGRANEX Gel is a non-sterile, low bioburden, preserved, sodium carboxymethylcellulose-based (CMC) topical gel, containing the active ingredient becaplermin and the following inactive ingredients: carboxymethylcellulose sodium, glacial acetic acid, l-lysine hydrochloride, m-cresol, methylparaben, propylparaben, sodium acetate trihydrate, sodium chloride, and water for injection. Each gram of REGRANEX Gel contains 100 mcg of becaplermin.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionREGRANEX Gel has biological activity similar to that of endogenous platelet-derived growth factor, which includes promoting the chemotactic recruitment and proliferation of cells involved in wound repair and enhancing the formation of granulation tissue.
12.2 PharmacodynamicsClinical pharmacodynamic studies have not been conducted.
12.3 PharmacokineticsTen patients with Stage III or IV (as defined in the International Association of Enterostomal Therapy (IAET) guide to chronic wound staging),1,2 lower extremity diabetic ulcers received topical applications of becaplermin gel 0.01% at a dose range of 0.32–2.95 µg/kg (7µg/cm2) daily for 14 days. Six patients had non-quantifiable PDGF levels at baseline and throughout the study, two patients had PDGF levels at baseline which did not increase substantially, and two patients had PDGF levels that increased sporadically above their baseline values during the 14 day study period.
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityBecaplermin was not genotoxic in a battery of in vitro assays (including those for bacterial and mammalian cell point mutation, chromosomal aberration, and DNA damage/repair). Becaplermin was also not mutagenic in an in vivo assay for the induction of micronuclei in mouse bone marrow cells.
Carcinogenesis and reproductive toxicity studies have not been conducted with REGRANEX Gel.
13.2 Animal Toxicology and/or PharmacologyIn nonclinical studies, rats injected at the metatarsals with 3 or 10 mcg/site (approximately 60 or 200 mcg/kg) of becaplermin every other day for 13 days displayed histological changes indicative of accelerated bone remodeling consisting of periosteal hyperplasia and subperiosteal bone resorption and exostosis. The soft tissue adjacent to the injection site had fibroplasia with accompanying mononuclear cell infiltration reflective of the ability of PDGF to stimulate connective tissue growth. [see Indications and Usage (1.2)]
14 CLINICAL STUDIESThe effects of REGRANEX Gel on the incidence of and time to complete healing in lower extremity diabetic ulcers were assessed in four randomized controlled studies. Of 922 patients studied, 478 received either REGRANEX Gel 0.003% or 0.01%. All study participants had lower extremity diabetic neuropathic ulcers that extended into the subcutaneous tissue or beyond (Stages III and IV of the IAET guide to chronic wound staging). Ninety-three percent of the patients enrolled in these four trials had foot ulcers. The remaining 7% of the patients had ankle or leg ulcers. The diabetic ulcers were of at least 8 weeks duration and had an adequate blood supply (defined as TcpO2>30 mm Hg). In the four trials, ninety-five percent of the ulcers measured in area up to 10 cm2, and the median ulcer size at baseline ranged from 1.4 cm2 to 3.5 cm2. All treatment groups received a program of good ulcer care consisting of initial complete sharp debridement, a non-weight-bearing regimen, systemic treatment for wound-related infection if present, moist saline dressings changed twice a day, and additional debridement as necessary. REGRANEX Gel 0.003% or 0.01% or placebo gel was applied once a day and covered with a saline moistened dressing. After approximately 12 hours, the gel was gently rinsed off and a saline moistened dressing was then applied for the remainder of the day. Patients were treated until complete healing, or for a period of up to 20 weeks. Patients were considered a treatment failure if their ulcer did not show an approximately 30% reduction in initial ulcer area after eight to ten weeks of REGRANEX Gel therapy.
The primary endpoint, incidence of complete ulcer closure within 20 weeks, for all treatment arms is shown in Figure 1. In each study, REGRANEX Gel in conjunction with good ulcer care was compared to placebo gel plus good ulcer care or good ulcer care alone.
In Study 1, a multicenter, double-blind, placebo controlled trial of 118 patients, the incidence of complete ulcer closure for REGRANEX Gel 0.003% (n=61) was 48% versus 25% for placebo gel (n=57; p=0.02, logistic regression analysis).
In Study 2, a multicenter, double-blind, placebo controlled trial of 382 patients, the incidence of complete ulcer closure for REGRANEX Gel 0.01% (n=123) was 50% versus 36% for
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 29 1/7/14 4:30 PM

REGRANEX Gel 0.003% (n=132) and 35% for placebo gel (n=127). Only REGRANEX Gel 0.01% was significantly different from placebo gel (p=0.01, logistic regression analysis).
The primary goal of Study 3, a multicenter controlled trial of 172 patients, was to assess the safety of vehicle gel (placebo; n=70) compared to good ulcer care alone (n=68). The study included a small (n=34) REGRANEX Gel 0.01% arm. Incidences of complete ulcer closure were 44% for REGRANEX Gel, 36% for placebo gel and 22% for good ulcer care alone.
In Study 4, a multicenter, evaluator-blind, controlled trial of 250 patients, the incidences of complete ulcer closure in the REGRANEX Gel 0.01% arm (n=128) (36%) and good ulcer care alone (n=122) (32%) were not statistically different.
Figure 1: Incidence of Complete Healing
In general, where REGRANEX Gel was associated with higher incidences of complete ulcer closure, differences in the incidence first became apparent after approximately 10 weeks and increased with continued treatment (Table 3).
Table 3: Life Table Estimates of the Incidence (%) of Complete Healing over Time of Study 2
REGRANEX Gel 0.01% (%)
Placebo Gel (%)
Week 2 1 0
Week 4 6 2
Week 6 9 6
Week 8 16 14
Week 10 23 18
Week 12 34 25
Week 14 37 28
Week 16 43 33
Week 18 46 34
Week 20 50 37
In a 3-month follow-up period where no standardized regimen of preventative care was utilized, the incidence of ulcer recurrence was approximately 30% in all treatment groups, demonstrating that the durability of ulcer closure was comparable in all treatment groups. In a randomized, double-blind study of REGRANEX Gel (100 mcg/g once daily for 16 weeks) in patients with Stage III or IV pressure ulcers, the incidence of complete ulcer closure was 15% (28/189) in the becaplermin group and 12% (22/190) in the vehicle control group. This difference was not statistically significant.
In two small, randomized, double-blinded studies of REGRANEX Gel (100 mcg/g once daily for 16 weeks) in patients with venous stasis ulcers, the combined incidence of complete ulcer closure was 46% (30/65) in the becaplermin group and 39% (26/67) in the vehicle control group. This difference was not statistically significant.
15 REFERENCES1. J. Enterostomal Ther 15:4, 1988
2. Decubitus 2:24, 1989
16 HOW SUPPLIED/STORAGE AND HANDLINGREGRANEX Gel is available in multi-use tubes in the following size:
15 g tube NDC 0064-0810-15
REGRANEX Gel is for external use only.
Store refrigerated at 2° – 8°C (36° – 46°F). Do not freeze. Do not use the gel after the expiration date shown at the bottom of the tube.
17 PATIENT COUNSELING INFORMATION[See FDA-approved patient labeling (Medication Guide)]
Counsel patients to review and discuss any questions or concerns with their healthcare provider before starting REGRANEX and at regular intervals while receiving REGRANEX.
Patients should be advised that:
• they should read the medication guide;
• hands should be washed thoroughly before applying REGRANEX Gel;
• the tip of the tube should not come into contact with the ulcer or any other surface; the tube should be recapped tightly after each use;
• a cotton swab, tongue depressor, or other application aid should be used to apply REGRANEX Gel;
• REGRANEX Gel should only be applied once a day in a carefully measured quantity [see Dosage and Administration (2)]. The measured quantity of gel should be spread evenly over the ulcerated area to yield a thin continuous layer of approximately 1/16 of an inch thickness. The measured length of the gel to be squeezed from the tube should be adjusted according to the size of the ulcer. The amount of REGRANEX Gel to be applied daily should be recalculated at weekly or biweekly intervals by the physician or wound care giver.
Step-by-step instructions for application of REGRANEX Gel are as follows:
• Squeeze the calculated length of gel onto a clean, firm, nonabsorbable surface, e.g., wax paper.
• With a clean cotton swab, tongue depressor, or similar application aid, spread the measured REGRANEX Gel over the ulcer surface to obtain an even layer.
• Cover with a saline moistened gauze dressing.
— after approximately 12 hours, the ulcer should be gently rinsed with saline or water to remove residual gel and covered with a saline-moistened gauze dressing (without REGRANEX Gel);
— it is important to use REGRANEX Gel together with a good ulcer care program, including a strict non-weight-bearing program;
— excess application of REGRANEX Gel has not been shown to be beneficial;
— REGRANEX Gel should be stored in the refrigerator. Do not freeze REGRANEX Gel;
— REGRANEX Gel should not be used after the expiration date on the bottom, crimped end of the tube.
Manufactured by: Healthpoint, Ltd. Fort Worth, TX 76107
U.S. Gov’t License # 1885
Marketed by: Healthpoint Biotherapeutics Fort Worth, TX 76107
REGRANEX is a registered trademark of Healthpoint, Ltd.
Distributed by: DPT Laboratories, Ltd. San Antonio, TX 78215
Part No. 129953-0912 Revised: September 2012
MEDICATION GUIDE REGRANEX® (RE’–GRAN–IX) (becaplermin) GelRead this Medication Guide before you start using REGRANEX and each time you get a refill. There may be new information. This information does not take the place of talking to your healthcare provider about your medical condition or your treatment.
What is the most important information I should know about REGRANEX?People who use 3 or more tubes of REGRANEX may have an increased risk of death from cancer.
• You should talk with your healthcare provider about the possible benefits and risks to you if you use more than 3 tubes of REGRANEX.
• If you already have cancer, you and your healthcare provider should carefully consider whether you will use REGRANEX.
If you decide to use REGRANEX, your healthcare provider will tell you how to use REGRANEX. See the section “How should I use REGRANEX?” below.
What is REGRANEX?REGRANEX is a man-made protein medicine that is used with other ulcer care practices (such as good wound care) to treat diabetic sores (ulcers) of your legs or feet that are deeper than just your skin, in people who have good blood supply to the legs.
It is not known if REGRANEX is effective for the treatment of pressure ulcers or ulcers that are due to poor blood flow (circulation). It is not known if REGRANEX is safe and effective in children under 16 years of age.
Who should not use REGRANEX?Do not use REGRANEX if you have a skin tumor at the area where you apply REGRANEX.
What should I tell my healthcare provider before using REGRANEX? Before you use REGRANEX tell your healthcare provider if you:• have cancer• have poor blood flow to your lower legs and feet• have allergies to any of the ingredients in REGRANEX.
See the end of this Medication Guide for a complete list of ingredients in REGRANEX.
• have any other medical conditions• are pregnant or plan to become pregnant. It is not
known if REGRANEX will harm your unborn baby.
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 30 1/7/14 4:30 PM

• are breast-feeding or plan to breast-feed. It is not known if REGRANEX passes into your breast milk.
Tell your healthcare provider about all the medicines you take, including prescription and non-prescription medicines, vitamins, and herbal supplements. Especially tell your healthcare provider if you apply other medicines to diabetic ulcers of your legs or feet. Know the medicines you take. Keep a list of them to show your healthcare provider and pharmacist when you get a new medicine.
How should I use REGRANEX?
• Use REGRANEX together with good ulcer care, as prescribed by your healthcare provider. This includes following your healthcare provider’s instructions about not putting weight on the affected leg and foot (non-weight-bearing).
• Use REGRANEX exactly as your healthcare provider tells you to use it.
• REGRANEX is for use on skin ulcers only. Do not use REGRANEX in your mouth, eyes, or vagina.
• REGRANEX comes as a gel. Your healthcare provider should tell you how often to use REGRANEX and how much REGRANEX to use.
• Your healthcare provider should check the size of your ulcer every 1 to 2 weeks.
• Your healthcare provider may change the amount of REGRANEX to be applied to your ulcer as the size of your ulcer changes. So, the amount of REGRANEX to be squeezed from the tube may change as the size of your ulcer changes.
• Close your REGRANEX tube tightly after each use.• Put the REGRANEX tube back in the refrigerator after
each use.• Use a cotton swab, tongue depressor, or other
application aid when you apply your REGRANEX. Do not let the tip of your REGRANEX tube touch the ulcer or any other surface.
• Apply REGRANEX one time each day.
Apply REGRANEX as follows: o Wash your hands well before you apply
REGRANEX. o Carefully measure the amount of REGRANEX that
your healthcare provider tells you to use. o Squeeze the amount of REGRANEX needed for
your ulcer on to a clean, firm, non-absorbable surface, such as wax paper.
o Use a clean cotton swab, tongue depressor, or similar application aid, to spread the REGRANEX gel in a thin layer over the surface of the ulcer on your foot or leg.
o Cover the area with a saline-moistened gauze dressing.
o After about 12 hours, gently rinse the ulcer with saline or water to remove the rest of the REGRANEX. Cover the ulcer with a new saline-moistened gauze dressing. Do not apply any more REGRANEX.
What are the possible side effects of REGRANEX?REGRANEX may cause serious side effects.
• See the section, “What is the most important information I should know about REGRANEX?”
• Common side effects of REGRANEX include: o Red skin rash o Burning at the application site
Tell your doctor if you have any side effect that bothers you or that does not go away.
These are not all the possible side effects of REGRANEX gel. For more information, ask your doctor or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
You may also report side effects to Healthpoint Biotherapeutics at 1-800-441-8227.
How should I store REGRANEX?
• Store REGRANEX in the refrigerator at 36°F to 46°F (2°C to 8°C).
• Do not freeze REGRANEX.• Do not use REGRANEX after the expiration date on
the bottom (sealed end) of the tube.• Throw away your REGRANEX that is out of date or no
longer needed for your treatment.
Keep REGRANEX and all medicines out of the reach of children.
General information about REGRANEX.
Medicines are sometimes prescribed for purposes other than those listed in a Medication Guide. Do not use REGRANEX for a condition for which it was not prescribed. Do not give REGRANEX to other people, even if they have the same symptoms that you have. It may harm them.
This Medication Guide summarizes the most important information about REGRANEX. If you would like more information about REGRANEX, talk to your healthcare provider. You can ask your healthcare provider or pharmacist for information about REGRANEX that is written for healthcare professionals.
What are the ingredients in REGRANEX?
Active ingredient: becaplermin
Inactive ingredients: carboxymethylcellulose sodium, glacial acetic acid, l-lysine hydrochloride, m-cresol, methylparaben, propylparaben, sodium acetate trihydrate, sodium chloride, and water for injection.
Manufactured by: Healthpoint, Ltd. Fort Worth, TX 76107
U.S. Gov’t License # 1885
Marketed by: Healthpoint Biotherapeutics Fort Worth, TX 76107
REGRANEX is a registered trademark of Healthpoint, Ltd.
Distributed by: DPT Laboratories, Ltd. San Antonio, TX 78215
Part No. 129953-0912 Revised: September 2012
This Medication Guide has been approved by the U.S. Food and Drug Administration.
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 31 1/7/14 4:30 PM

©2013 Smith & Nephew, Inc. All rights reserved.Regranex is a registered trademark of Smith & Nephew, Inc. TM1528-0813
TM1528-0813_REG_0856_ClinMono_M_3_ac.indd 32 1/7/14 4:30 PM