equine laminitis gary m. baxter. definitions inflammation of the laminaeinflammation of the laminae...
TRANSCRIPT

Equine Laminitis
Gary M. BaxterGary M. Baxter

Definitions
• Inflammation of the laminaeInflammation of the laminae– Numerous inciting causesNumerous inciting causes
– Laminitis vs. “founder”Laminitis vs. “founder”
• Separation of the dermal and epidermal Separation of the dermal and epidermal junction junction – Attachment of coffin bone to hoof wallAttachment of coffin bone to hoof wall
• Displacement of the coffin boneDisplacement of the coffin bone– RotationRotation
– SinkingSinking
– Combination of the twoCombination of the two

Coffin Bone Displacement

Clinical Forms
• Gastrointestinal/toxicGastrointestinal/toxic– Grain overload, grass founderGrain overload, grass founder– Metritis, retained placenta, colitis, colicMetritis, retained placenta, colitis, colic
• Musculoskeletal/mechanicalMusculoskeletal/mechanical• Metabolic/localMetabolic/local
– Cushing's diseaseCushing's disease– Metabolic syndromeMetabolic syndrome– Corticosteroids Corticosteroids
• IdiopathicIdiopathic

Predisposing Factors
• Systemic illness (toxemia)Systemic illness (toxemia)• Excessive carbohydrate/grassExcessive carbohydrate/grass• Metabolic/weight problemsMetabolic/weight problems
– Increased glucose/insulin resistanceIncreased glucose/insulin resistance
• Older horses and maresOlder horses and mares– Non-Thoroughbred breedsNon-Thoroughbred breeds
• Unilateral lamenessUnilateral lameness• Long toe/low heelLong toe/low heel
– Hard surfacesHard surfaces

Stages of Laminitis
• Developmental – before clinical signsDevelopmental – before clinical signs• AcuteAcute
– Clinical signs onlyClinical signs only– No movement of coffin bone on radiographsNo movement of coffin bone on radiographs
• ChronicChronic– Movement of coffin bone within hoof Movement of coffin bone within hoof
• Subacute? Subacute? – In between the acute and chronic stagesIn between the acute and chronic stages

Clinical Signs
• Lameness especially when turnedLameness especially when turned– Worse on hard surfacesWorse on hard surfaces
– Shifting weight between limbsShifting weight between limbs
• Increased digital pulsesIncreased digital pulses
• Heat over dorsal hoof wallHeat over dorsal hoof wall
• Both front feet commonly affectedBoth front feet commonly affected– All four feet (very sick horses)All four feet (very sick horses)
– Both rear feet (draft horses?)Both rear feet (draft horses?)
– Single foot (excessive weight-bearing)Single foot (excessive weight-bearing)

Laminitis

Disease Process
• Variable developmental periodVariable developmental period– Grain overload – 24-72 hoursGrain overload – 24-72 hours
• Much happening in foot before laminar Much happening in foot before laminar damage and clinical signsdamage and clinical signs
• Minimal control over initial laminar Minimal control over initial laminar damagedamage
• Many horses with mild acute/subacute Many horses with mild acute/subacute laminitis may not be recognized laminitis may not be recognized

Gross Pathology
1.1. Edema - compartment Edema - compartment syndromesyndrome
2. Hemorrhage2. Hemorrhage
3. Laminar separation3. Laminar separation
4. Structural damage4. Structural damage

Physiologic Alterations• HypertensionHypertension
• Sympathetic stimulation/tachycardiaSympathetic stimulation/tachycardia
• Systemic/local coagulopathySystemic/local coagulopathy
• Metabolic alterationsMetabolic alterations
Causes of Laminitis?
• Several potential theoriesSeveral potential theories– Vascular theoryVascular theory– Toxic/enzymatic theoryToxic/enzymatic theory– Traumatic/mechanical theoryTraumatic/mechanical theory– Glucose/insulin resistance theoryGlucose/insulin resistance theory
• Common end-result in the foot?Common end-result in the foot?– InflammationInflammation– Breakdown of basement membrane of laminaeBreakdown of basement membrane of laminae– Separation of sensitive and insensitive laminaeSeparation of sensitive and insensitive laminae

Vascular Theory
• Too little blood to footToo little blood to foot
• Laminar ischemiaLaminar ischemia
• Reflex hyperemia – compartment Reflex hyperemia – compartment syndrome/reperfusionsyndrome/reperfusion
• Secondary inflammationSecondary inflammation
• Structural failure of laminaeStructural failure of laminae
Toxic/Enzymatic Theory
• Excessive blood to footExcessive blood to foot
• ““Trigger factors” within the blood Trigger factors” within the blood (from gut or uterus) initiate damage(from gut or uterus) initiate damage
• Several enzymes/mediators damage Several enzymes/mediators damage basement membranebasement membrane
• Secondary inflammation Secondary inflammation
• Structural failure of laminaeStructural failure of laminae

Mechanical Theory
• Different from “classic” GI formDifferent from “classic” GI form• Traumatic tearing of laminae from Traumatic tearing of laminae from
excessive weight bearing?excessive weight bearing?• Pain contributes to increased cortisolPain contributes to increased cortisol
– Increased insulin?Increased insulin?– Vasospasm of digital vessels?Vasospasm of digital vessels?
• Secondary inflammationSecondary inflammation• Structural failure of laminaeStructural failure of laminae

Glucose/IR Theory
• Hyperglycemia/insulin resistance Hyperglycemia/insulin resistance – Impaired blood flowImpaired blood flow– Direct effect of increased insulinDirect effect of increased insulin
• Impaired glucose uptakeImpaired glucose uptake– Laminar cells have high glucose requirementLaminar cells have high glucose requirement
• Secondary inflammationSecondary inflammation
• Structural failure of laminaeStructural failure of laminae

Diagnosis
• Clinical signsClinical signs– Increased digital pulsesIncreased digital pulses
– Heat over dorsal hoof wallHeat over dorsal hoof wall
– Variable lameness but often severeVariable lameness but often severe
– Heel-toe landing/hoof distortion in chronic casesHeel-toe landing/hoof distortion in chronic cases
– Pain over toe with hoof testersPain over toe with hoof testers
• Local anesthesiaLocal anesthesia– Improve with palmar digital, basi-sesamoid or abaxial Improve with palmar digital, basi-sesamoid or abaxial
blocksblocks
• RadiographyRadiography– Rotation, sinking or bothRotation, sinking or both

Chronic Laminitis

Radiology – “Rotation”

Radiology – “Sinking”

Radiology - chronic

Treatment/Prevention
Developmental – to prevent disease progressionDevelopmental – to prevent disease progressionAcute – to minimize severity of laminar damageAcute – to minimize severity of laminar damageChronic – to limit further movement of coffin boneChronic – to limit further movement of coffin bone
Treatment
• Remove or treat inciting causeRemove or treat inciting cause– Minimize toxemia or “trigger factors”Minimize toxemia or “trigger factors”– Mineral oil, flunixin meglumine, DMSOMineral oil, flunixin meglumine, DMSO
• Cushing’s – pergolideCushing’s – pergolide• Metabolic syndrome/IRMetabolic syndrome/IR
– Decrease glycemic index (CHOs)Decrease glycemic index (CHOs)– Pergolide and thyroxine?Pergolide and thyroxine?
• Mechanical Mechanical – Sling/ improve weight bearing on other limbSling/ improve weight bearing on other limb– Support of contralateral footSupport of contralateral foot

Treatment
• Dependent on stage of diseaseDependent on stage of disease– Cryotherapy (ice) in acute stage?Cryotherapy (ice) in acute stage?– Vasodilatory drugs?Vasodilatory drugs?– Anti-inflammatory drugsAnti-inflammatory drugs– Pain control (decrease sympathetic response)Pain control (decrease sympathetic response)
• Minimize toe length (remove shoe)Minimize toe length (remove shoe)– Bevel dorsal hoof wall of toeBevel dorsal hoof wall of toe
• Increase weight bearing surface areaIncrease weight bearing surface area– Styrofoam, sand, frog pads, soft puttyStyrofoam, sand, frog pads, soft putty– Corrective shoeing Corrective shoeing

Initial Foot Support

Corrective Shoeing

Foot Preparation
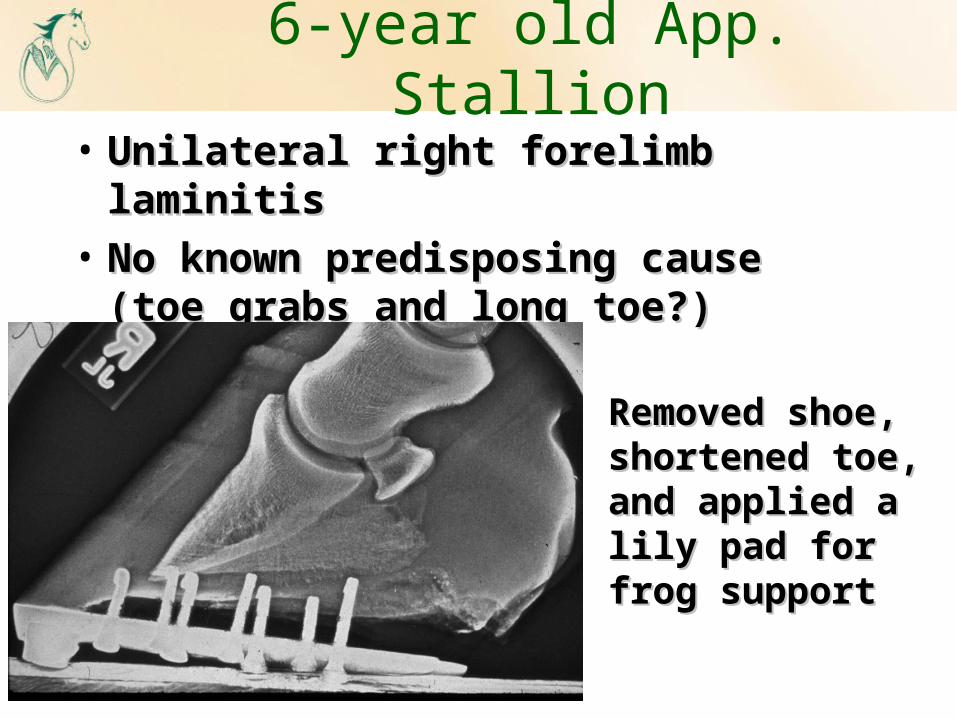
6-year old App. Stallion
• Unilateral right forelimb laminitisUnilateral right forelimb laminitis
• No known predisposing cause (toe No known predisposing cause (toe grabs and long toe?)grabs and long toe?)
Removed shoe, Removed shoe, shortened toe, shortened toe, and applied a lily and applied a lily pad for frog pad for frog supportsupport
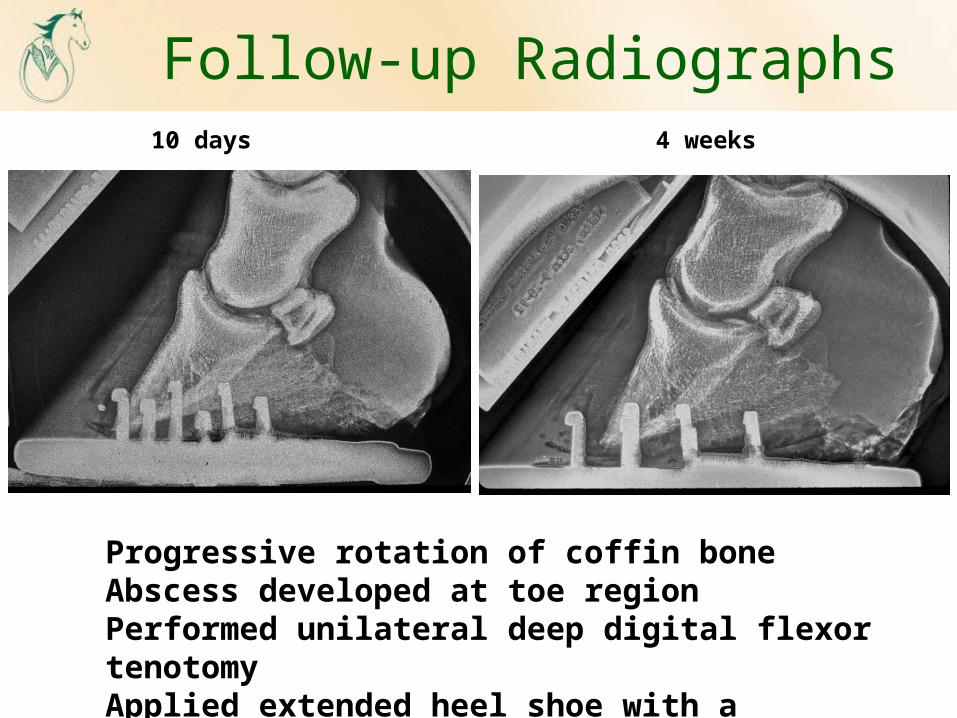
Follow-up Radiographs10 days 4 weeks
Progressive rotation of coffin boneAbscess developed at toe regionPerformed unilateral deep digital flexor tenotomyApplied extended heel shoe with a treatment plate

Thank you from CSU-VTH