epidemiology and control of malaria during pregnancy m. james eliades, md, mph centers for disease...
TRANSCRIPT

Epidemiology and control of malaria during pregnancy
M. James Eliades, MD, MPHCenters for Disease Control and
PreventionDivision of Parasitic Diseases

Objectives of talk
Discuss the epidemiology of malaria during pregnancy in sub-Saharan Africa
Present evidence for current intervention strategies
Mention gaps in our knowledge
Epidemiology

Malaria during pregnancy: bad news 50 million women in malaria endemic areas become
pregnant each year (UNICEF)
Malaria during pregnancy most widely evaluated in sub-Saharan Africa and estimated to account for:• 400,000 cases of severe anemia in pregnant
women (Guyatt 2001)
• ~ 35% of preventable low birth weight (Steketee 2001, Guyatt 2004)
• 3-8% of infant mortality (Steketee 2001, Guyatt 2001)• 75,000 - 200,000 infant deaths annually
(WHO/UNICEF Africa Malaria Report 2003)

Distribution of Malaria
Where in the World is Malaria Found?
Malaria during pregnancy
Maternal and perinatal effects depend on intensity of transmission: Plasmodium falciparum in high transmission areas is most well studied - responsible for most morbidity & mortality

Transmission intensity
“Stable” malaria• Prevalence
persistently high• Transmission can
continue with few vectors
• Collective immunity is high
• P. falciparum• Young children and
pregnant women at greatest risk
• Type: sub-Saharan Africa
“Unstable” malaria• Variability in space
and time• Disease fluctuates
(inc. epidemics)• Collective immunity
is low• P. vivax, also P.
falciparum• All ages at risk• Type: S.E. Asia

Malaria in Pregnancy
Transmission levels effect consequences of disease• Low transmission/little or no immunity
Symptomatic Severe malaria Anemia Adverse birth outcomes
• Moderate to high transmission/immunity Asymptomatic Severe anemia Low birth weight

Malaria during pregnancy:stable transmission areas
Asymptomatic infection
Nutrient transport
Placental sequestration
Low birth weight
Risk of infant mortality
P. falciparum malaria
Anemia
Acquired immunity - high 1st & 2nd pregnancies at
greatest risk Prevention essential

Malaria during pregnancy:unstable transmission areas
P. falciparum malaria
Clinical illness
Severe disease
Risk to mother(death)
Risk to fetus(stillbirth, abortion)
Acquired immunity - low
All pregnancies affected equally
Recognition and case management needed in addition to prevention
Vulnerable groups among pregnant women
Primigravidae Adolescents HIV-positive women Women in rural areas
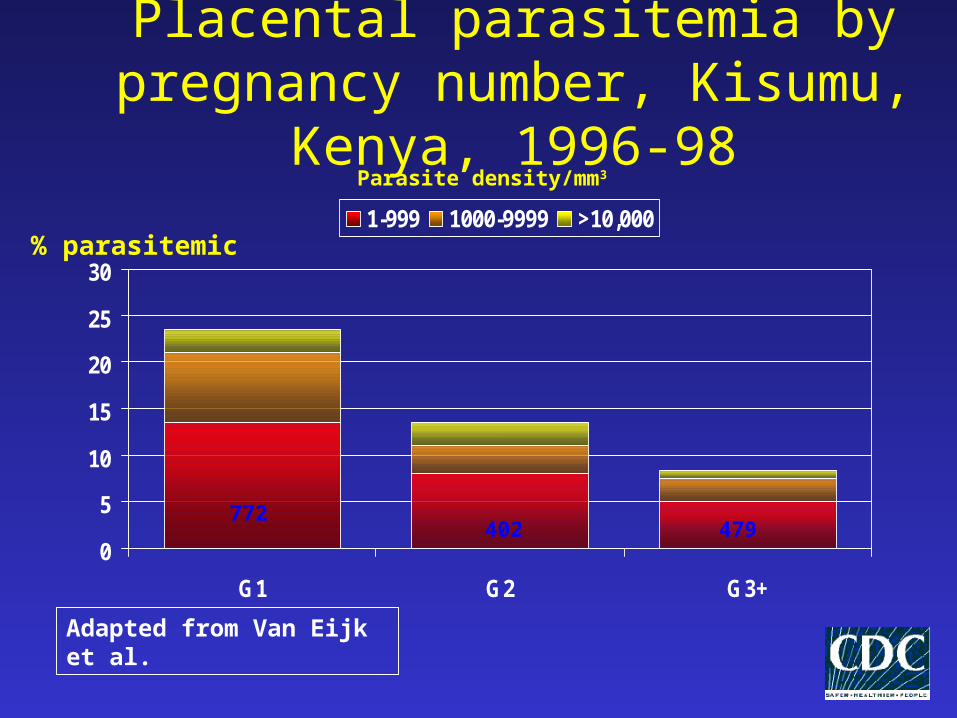
Placental parasitemia by pregnancy number, Kisumu, Kenya, 1996-98
0
5
10
15
20
25
30
G1 G2 G3+
1-999 1000-9999 >10,000
Parasite density/mm3
% parasitemic
772402 479
Adapted from Van Eijk et al.
Effects on Maternal Health
Severe anemia• Proportion in all gravidities attributable to
malaria: 26%• Approximately 400,000 cases per year
Effects on Birth Outcome
Low Birth Weight 20% of LBW deliveries, 35% of preventable LBW Responsible for at least 100,000 infant deaths
• Intrauterine growth retardation (IUGR)• Preterm delivery
Stillbirth• Twice the risk with placental malaria(OR 2.19)

Low birth weight

Effects on Birth Outcomes: Low Transmission Settings
In Africa• LBW: 9.3%• Preterm delivery: 8.6%• Stillbirths: 3.7%
Outside Africa• LBW: 16.0%• Preterm delivery: 11.0%• Stillbirths: 3.0%

Neonatal Mortality Rates by BirthweightMangochi, Malawi
September 1987 - June 1989
Adapted from Steketee et al.
0
200
400
600
800
1000
<1500 1500-1999 2000-2499 2500
Death
s p
er
1000 L
ive B
irth
s
800
300
49 26
31 11.7 2.4 1.0Relative Risk

Pathophysiology
Placenta
Sequestration of parasites in the placenta• Red blood cells infected with P. falciparum
attach to placenta
Can be present without peripheral parasitemia
Increased susceptibility of primigravidae
Congenital Malaria
Can occur with all four species Parasites cross the placenta and enter
the fetal circulation Immunity of mother affects severity
• Non-immune: stillbirth, perinatal death, fever/anemia/jaundice/splenomegaly up to six weeks post-delivery
• Immune: usually asymptomatic; parasties rapidly cleared
HIV Among Pregnant Women in sub-Sahara Africa
Estimated 27 million people in Africa living with HIV/AIDS
55% of sub-Sahara Africa adult HIV infection in reproductive-age women
Estimated increase in MIP attributable to HIV is 5.5% and 18.8% for populations with HIV prevalence of 10% and 40%
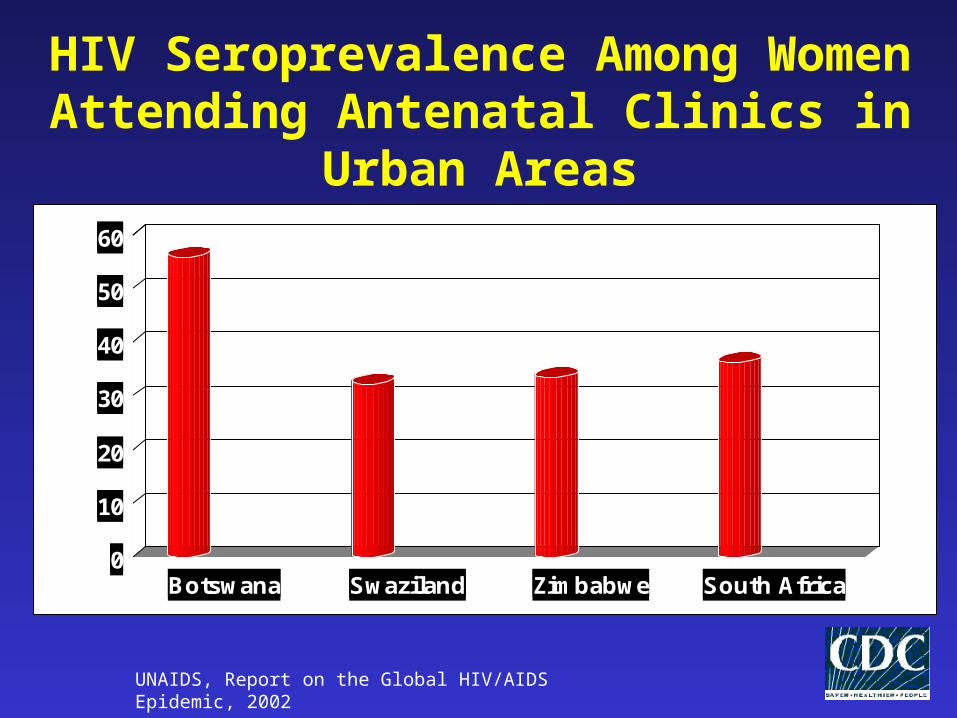
0
10
20
30
40
50
60
Botswana Swaziland Zimbabwe South Africa
HIV Seroprevalence Among Women Attending Antenatal Clinics in Urban
Areas
UNAIDS, Report on the Global HIV/AIDS Epidemic, 2002
HIV+ women have higher prevalences
and densities of parasitemia
All parities affected
Risk of infant mortality higher in
babies born to mothers co-infected
with HIV and placental malaria
• Increased vertical transmission of HIV?
HIV & Malaria During Pregnancy

Study 2. Placental parasitemia by HIV status and pregnancy number, Kisumu, Kenya,
1996-98
0
5
10
15
20
25
30
35
40
G1 G2 G3 G1 G2 G3
1-999 1000-9999 >10,000
Parasite density/mm3
% parasitemic
HIV (+) HIV (-)
231 159 197 772 402 479
Total n = 2263Summary RR = 1.63 (1.41-1.89), p<0.001

Intermittent preventive therapy by HIV status and SP efficacy
05
101520253035404550
Case 2-dose Monthly
Per
cent
par
asite
mia
HIV (+)
HIV (-)
Management

Current strategies

Options for malaria control during pregnancy
Drugs• Chemoprophylaxis
• Intermittent preventive treatment during pregnancy (IPTp)• Febrile case management
Insecticide Treated Nets (ITNs) Prevention and treatment of anemia
• Hematinic supplementation• Nutritional counseling
Vaccines?

Chemoprophylaxis: no longer a recommended strategy in high
transmission areas Most regimens require weekly or more frequent dosing
• Chloroquine (CQ) is the most commonly used drug Usefulness limited by:
• Difficulty in delivering and sustaining intervention
• Poor adherence to regimen
• Side effects of CQ (especially itching)
• Rising levels of P. falciparum resistance to CQ
• Poor program effectiveness of CQ chemoprophylaxis

Intermittent Preventive Treatment for pregnancy (IPTp)

Intermittent preventive treatment (IPTp): an alternative strategy
Most studied regimen: Sulfadoxine-pyrimethamine (SP) 2 curative courses (3 tablets)• One course during second trimester• One course during third trimester
Inexpensive Easily deliverable (can be given under direct
observation) Safe Efficacious

Intermittent preventive treatment-- the two dose SP strategy
Weeks of gestationConception Birth
20 3010
Course 124-28 wks
Course 230-36 wks
Fetal growth velocity
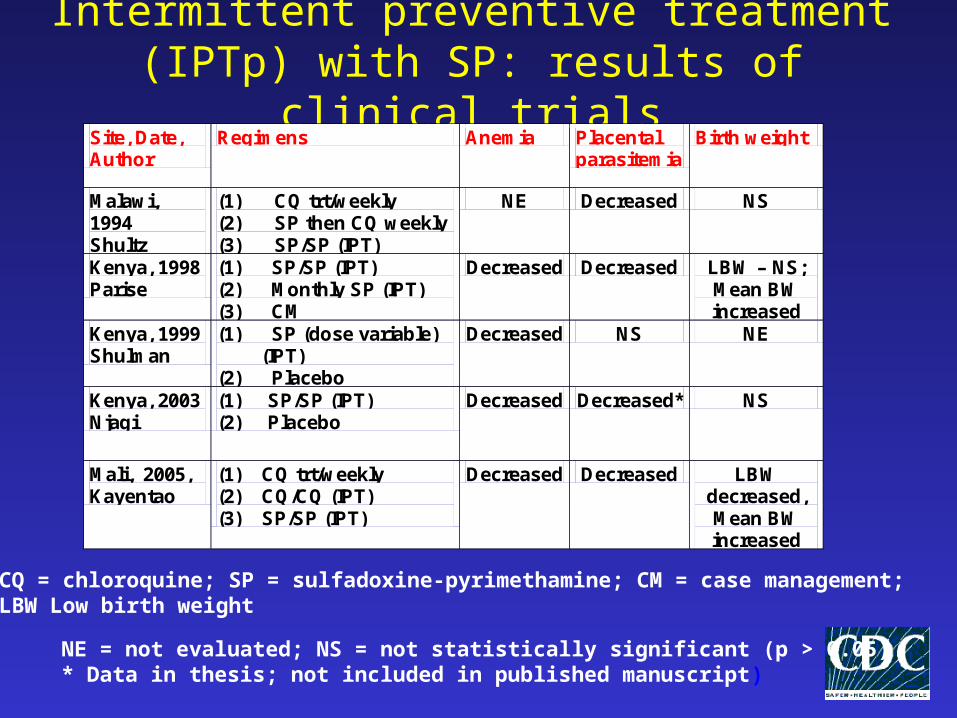
Intermittent preventive treatment (IPTp) with SP: results of clinical trials
Site, Date, Author
Regimens Anemia Placental parasitemia
Birth weight
Malawi, 1994 Shultz
(1) CQ trt/weekly (2) SP then CQ weekly (3) SP/SP (IPT)
NE Decreased NS
Kenya, 1998 Parise
(1) SP/SP (IPT) (2) Monthly SP (IPT) (3) CM
Decreased Decreased LBW – NS; Mean BW increased
Kenya, 1999 Shulman
(1) SP (dose variable) (IPT)
(2) Placebo
Decreased NS NE
Kenya, 2003 Njagi
(1) SP/SP (IPT) (2) Placebo
Decreased Decreased* NS
Mali, 2005, Kayentao
(1) CQ trt/weekly (2) CQ/CQ (IPT) (3) SP/SP (IPT)
Decreased Decreased LBW decreased, Mean BW increased
NE = not evaluated; NS = not statistically significant (p > 0.05)* Data in thesis; not included in published manuscript)
CQ = chloroquine; SP = sulfadoxine-pyrimethamine; CM = case management; LBW Low birth weight
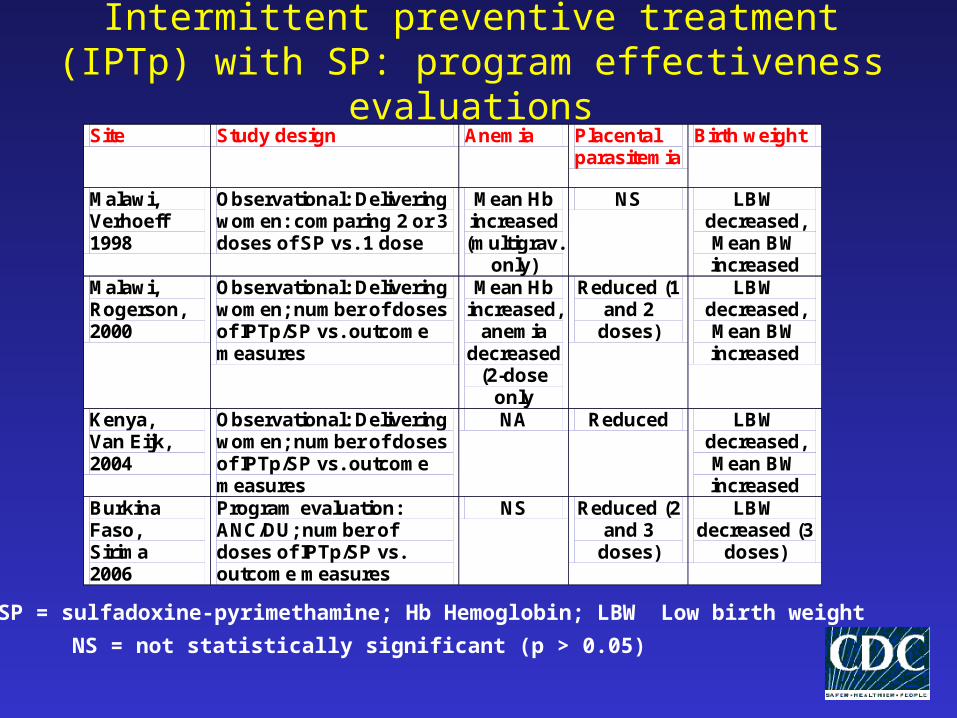
Intermittent preventive treatment (IPTp) with SP: program effectiveness evaluations
Site Study design Anemia Placental parasitemia
Birth weight
Malawi, Verhoeff 1998
Observational: Delivering women: comparing 2 or 3 doses of SP vs. 1 dose
Mean Hb increased (multigrav.
only)
NS LBW decreased, Mean BW increased
Malawi, Rogerson, 2000
Observational: Delivering women; number of doses of IPTp/SP vs. outcome measures
Mean Hb increased,
anemia decreased
(2-dose only
Reduced (1 and 2
doses)
LBW decreased, Mean BW increased
Kenya, Van Eijk, 2004
Observational: Delivering women; number of doses of IPTp/SP vs. outcome measures
NA Reduced LBW decreased, Mean BW increased
Burkina Faso, Sirima 2006
Program evaluation: ANC/DU; number of doses of IPTp/SP vs. outcome measures
NS Reduced (2 and 3
doses)
LBW decreased (3
doses)
NS = not statistically significant (p > 0.05)
SP = sulfadoxine-pyrimethamine; Hb Hemoglobin; LBW Low birth weight

IPTp with SP: summary of evidence and benefits
2 doses of IPT with SP is associated with: • Reduction in 3rd trimester maternal anemia • Reduction in placental malaria parasitemia• Reduction in low birth weight
At least 2 doses required for optimal benefit Monthly dosing more beneficial in HIV+
women Regimen is safe and well tolerated

Insecticide treated bed nets (ITNs)
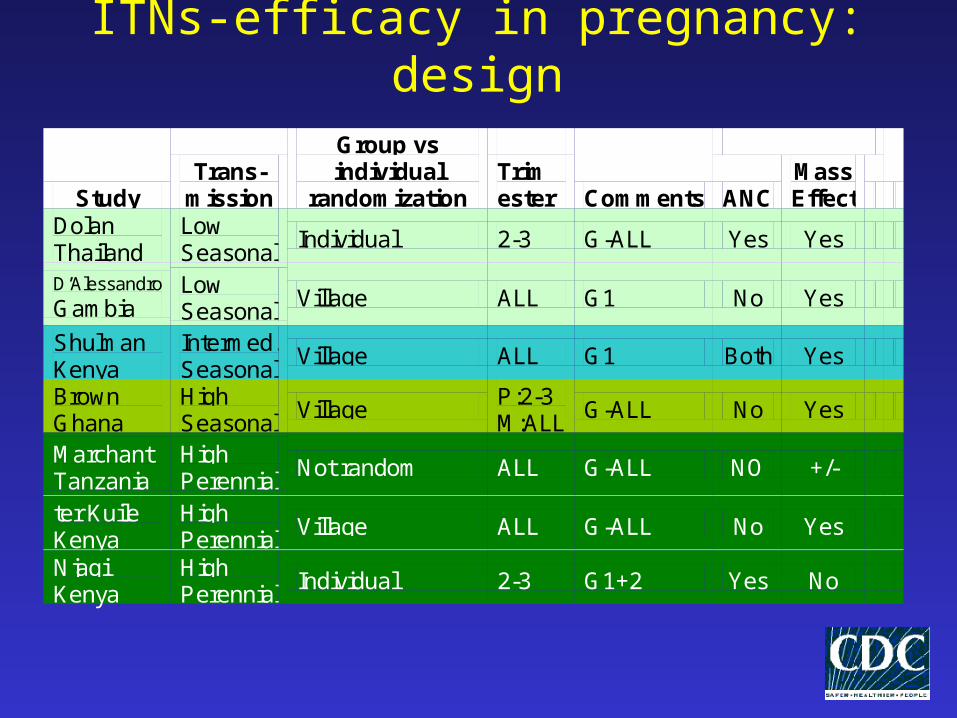
ITNs-efficacy in pregnancy: design
Study Trans-
mission
Group vs individual
randomization Trim ester Comments ANC
Mass Effect
Dolan Thailand
Low Seasonal
Individual 2-3 G-ALL Yes Yes
D’Alessandro
Gambia Low Seasonal
Village ALL G1 No Yes
Shulman Kenya
Intermed. Seasonal
Village ALL G1 Both Yes
Brown Ghana
High Seasonal
Village P:2-3 M:ALL
G-ALL No Yes
Marchant Tanzania
High Perennial
Not random ALL G-ALL NO +/-
ter Kuile Kenya
High Perennial
Village ALL G-ALL No Yes
Njagi Kenya
High Perennial
Individual 2-3 G1+2 Yes No

ITNs during pregnancy
Meta analyses of 5 RCTs (4 from Africa, 1 from Thailand)
In Africa, ITNs reduced• placental parasitemia in all pregnancies
(RR=0.79 [0.63-0.98])• LBW (RR=0.77 [0.61-0.98]) and
stillbirths/abortions in G1-4 (RR=0.67 [0.47-0.97])*
In Thailand, ITNs reduced anemia and stillbirth/abortions in all pregnancies
Source: Gamble 2006

Case management of malaria and anemia
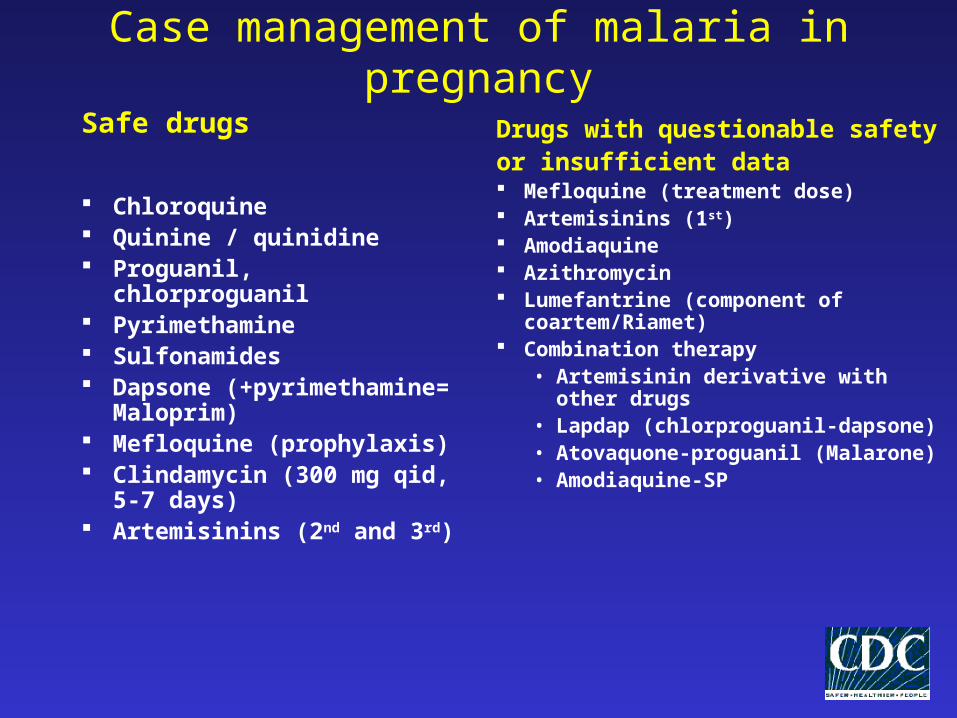
Case management of malaria in pregnancy
Safe drugs
Chloroquine Quinine / quinidine Proguanil, chlorproguanil Pyrimethamine Sulfonamides Dapsone (+pyrimethamine=
Maloprim) Mefloquine (prophylaxis) Clindamycin (300 mg qid, 5-
7 days) Artemisinins (2nd and 3rd)
Drugs with questionable safetyor insufficient data Mefloquine (treatment dose) Artemisinins (1st) Amodiaquine Azithromycin Lumefantrine (component of
coartem/Riamet) Combination therapy
• Artemisinin derivative with other drugs
• Lapdap (chlorproguanil-dapsone)• Atovaquone-proguanil (Malarone)• Amodiaquine-SP

Antimalarials contra-indicated in pregnancy
Tetracycline Doxycycline Halofantrine Primaquine Tafenoquine Note: if serious illness, and where limited
number of drugs are available, it is necessary to balance the risk of maternal death with the hypothetical risks to the infant

Antimalarial drug policy
An antimalarial drug policy must balance between:
Access Rational use
Reduces development of resistance
Emphasis on regulation and controlled use (e.g. prescription only drugs)
• Equitable access to reduce mortality and morbidity
• Emphasis on community management (e.g. use of lay persons for distributing drugs)
High transmission areas• Women don’t feel sick- need prevention of
adverse effects• Prevention by IPT and nets
Low transmission areas• IPT will not necessarily keep the woman well• Prevention by nets• Any role for chemoprophylaxis in select areas?
Both areas need prompt appropriate febrile case management
Interventions depend on level of transmission
The Results of Preventing Infection
Reduce the risk of severe maternal anemia: 38%
Reduce the risk of LBW: 43% Reduce the risk of perinatal mortality:
27%

From Research to Policy to Implementation

African summit on Roll Back Malaria (RBM) – Abuja 2000
At least 60 percent of those at risk of malaria, particularly pregnant women and children under 5 years of age, benefit from the most suitable combination of personal and community protective measures such as insecticide-treated mosquito nets …
At least 60 percent of all pregnant women who are at risk of malaria, especially those in their first pregnancies, have access to intermittent preventive treatment.

Malaria during pregnancy: Research to program - a continuous
cycle
Programmatically relevant research
Policy changeProgram implementation
Monitoring & evaluation
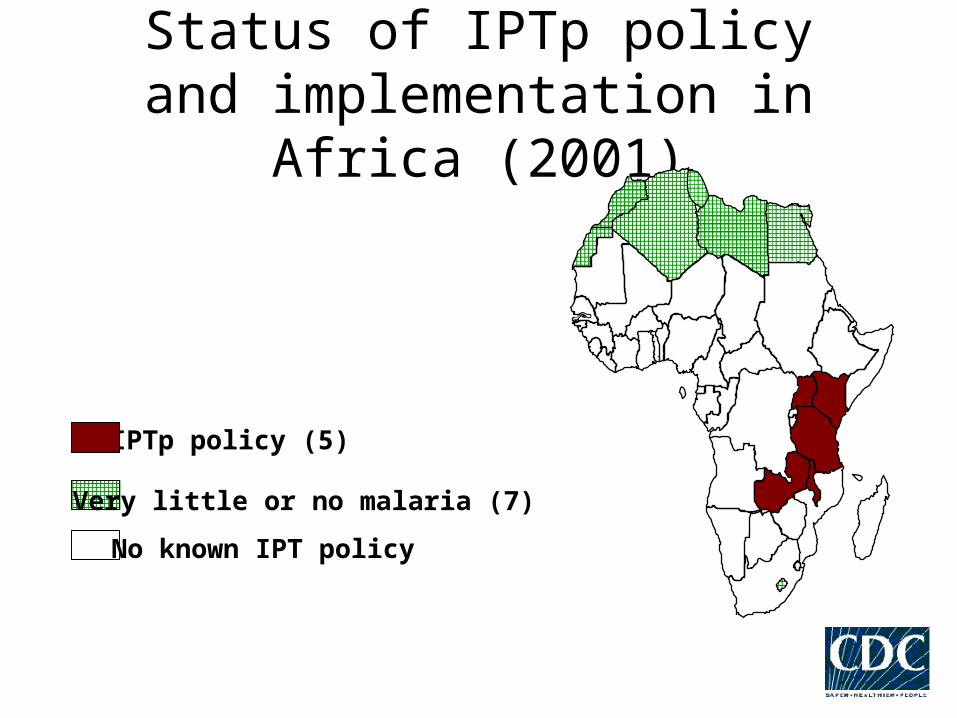
Status of IPTp policy and implementation in Africa (2001)
IPTp policy (5)
Very little or no malaria (7)
No known IPT policy

Rapid assessment of burden of malaria during pregnancy
Survey at antenatal care:• peripheral malaria parasitemia and anemia
Survey at delivery units• Peripheral and placental parasitemia, birth
weight, and gestational age
Other modules: severe disease, health facility assessment, rapid ethnographic evaluation


Example: Burkina Faso Joint collaboration of CDC with JHPIEGO and
Burkina Faso Ministry of Health Baseline 2001 rapid assessment examined:
rates of peripheral and placental parasitemia, maternal anemia, and low birth weight • >22% of women had placental parasitemia despite
widespread use of chloroquine chemoprophylaxis Pilot intervention of IPTp with 3 doses of SP
begun in 2003; ITN distribution through NGO programs
Repeat rapid assessment (program evaluation) conducted in 2004

Burkina Faso – 2004 program evaluation
High coverage with IPTp at delivery units (DU) 3 doses: 46.9% 2 doses: 78.6% 1 dose: 93.5 %
High coverage with IPTp at antenatal clinics (ANC) - includes dose given on day of interview
3 doses: 20.9% 2 doses: 57.6% 1 dose: 96.2%

Burkina Faso Delivery Units2001 vs. 2004
2001 2004 Risk ratio P-value
Peripheral parasitemia (delivery)
29.4% 19.4% 0.66 <0.0001
Placental parasitemia
22.6% 15.9% 0.71 0.0002
Low birth weight
14.4% 12.2% 0.85 0.15
Note: Unadjusted
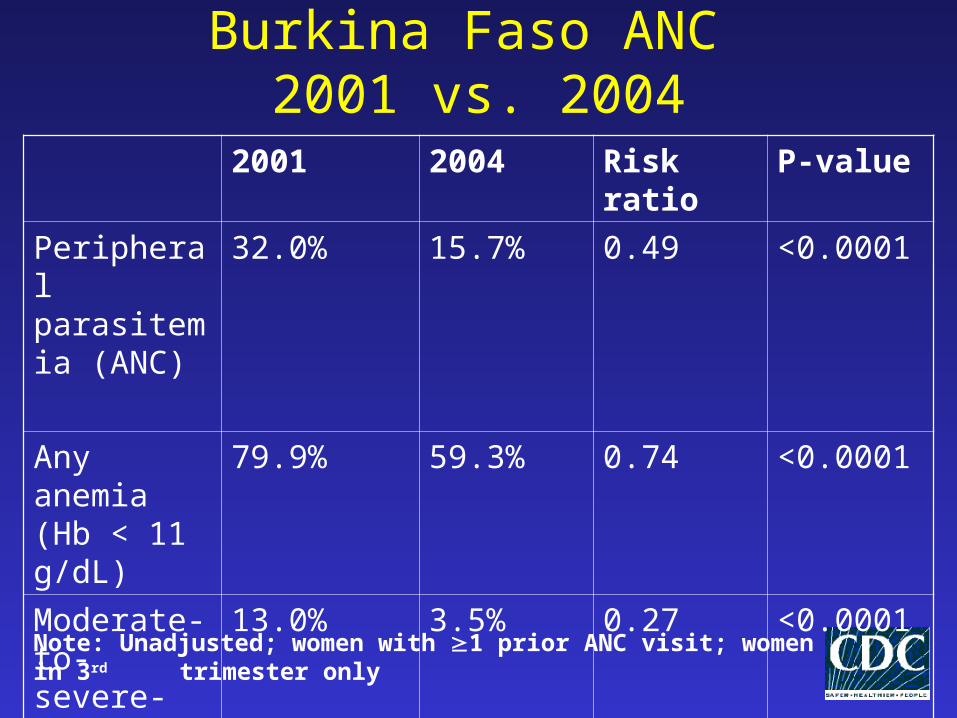
Burkina Faso ANC 2001 vs. 2004
2001 2004 Risk ratio P-value
Peripheral parasitemia (ANC)
32.0% 15.7% 0.49 <0.0001
Any anemia (Hb < 11 g/dL)
79.9% 59.3% 0.74 <0.0001
Moderate-to-severe-anemia
13.0% 3.5% 0.27 <0.0001
Note: Unadjusted; women with 1 prior ANC visit; women in 3rd trimester only
Burkina Faso – Conclusions and recent events
Package of ITNs and IPTp with SP (3 dose strategy) may have resulted in decreased proportion of women with anemia, peripheral parasitemia, and placental parasitemia when comparing pre-program (2001) and post program (2004) assessments
In February 2005, based on data from Koupéla, Burkina MoH adopted IPTp as national policy (2 doses of sulfadoxine-pyrimethamine)


Status of IPTp policy and implementation in Africa (January 2005)
IPTp policy and widespreadIPTp program implementation (5)
IPTp policy and IPTp program implementation in progress (7)
IPTp policy but no implementation yet (3)
IPTp policy but extent of implementation unknown (4)
IPTp implemented on small scale by NGOs but no national policy: Liberia and Somalia
Very little or no malaria (7)
No known IPTp policy (25)
Malaria during pregnancy:gaps in knowledge and future
directions

MiP Consortium
Focused on addressing gaps in knowledge regarding all aspects of MiP
Initial funding for meetings and development of review papers from Bill & Melinda Gates Foundation
Full research agenda to be finalized in 2006 Comprehensive reviews (7) published as
part of an LID supplement

Technical Reviews1. Epidemiology and Burden of disease: M Desai, F ter
Kuile, F Nosten, R McGready, K Asamoa, B Brabin, R Newman
2. Pathophysiology and immunology: S Rogerson R Leke, et al
3. Drug safety and kinetics: S Ward, E Sevene et al4. Case management: F Nosten, R McGready, TK
Mutabingwa5. Prevention: C Menendez, F ter Kuile6. Implementation and Policy: J Crawley, A Palmer, K
Asamoa, R Steketee, et al7. Economics of malaria in pregnancy: E Worrall, A Mills8. Summary concept paper: B Greenwood, R Steketee and
P Alonso
Priorities: Epidemiology and Burden
What is the importance of MiP in low transmission areas including areas where P. vivax is the dominant parasite ? What is the impact of malaria in the first trimester ? Is malaria an important cause of maternal mortality in medium to high transmission areas?
Priorities: Pathogenesis and immunity
How does malaria cause severe anemia in pregnancy ? How does malaria cause low birth weight ? What impact will the introduction of effective control measures have on naturally acquired immunity to malaria ?Can malaria in pregnancy be prevented by:
partially effective pre-erythrocytic vaccines a ‘malaria in pregnancy’ vaccine (anti-cytoadherence)
Priorities: Case Management Can the diagnosis of malaria be improved ? Which drugs can be used to replace CQ and SP for the treatment of malaria in pregnancy and how can the efficacy of new drugs best be measured ? How are the pharmacokinetics of anti-malarial drugs (old and new) influenced by pregnancy ? Are there pharmacokinetic interactions between anti-malarials and ARVs ? Are anti-malarials safe in pregnancy (pharmacovigilance) ?
Priorities: Prevention of MiP
How can current preventive strategies (ITNs, IRS, IPT, repellents) be used together most effectively in different epidemiological situations:
low or high transmission areas with P. vivax infection low or high HIV prevalence
What drug(s) can be used to replace SP for IPT? Do they need to be long acting ? Are existing insecticides and new ones under development safe in pregnancy when used for ITNs or IRS ? Pharmacovigilance
Priorities: Economic aspects of MiP
What is the overall economic burden of malaria in pregnancy ? What are the comparative cost efficacies of different control measures in different circumstances ?
Priorities: Health systems research
How can usage of ITNs and IPT be scaled up most effectively and equitably in different situations ? How can malaria control in pregnancy be integrated into reproductive health and HIV management programmes more effectively ? Will new interventions be accessible, affordable and acceptable?
Overall priorities identified from technical reviews
New drugs for treatment New drugs for prevention Clarity on optimal methods of deploying
combinations of interventions in different epidemiological settings
Improved delivery of existing recommendations to achieve high coverage
Areas for PMI to think about
How to get women to attend all their ANC visits and earlier
Integrating MIP with other ANC services (PMTCT, EPI, Reprod, Nutrition)
Creating demand (quality, wanted services) Expanding commodity procurment to include
iron/folate Monitor efficacy of IPTp with SP resistance
rising

Resources MiP
• Strategic framework for malaria prevention and control during pregnancy in the African Region (WHO/2005)
English, French, Portuguese (soon)
• Rapid Assessment of Malaria during Pregnancy Toolkit (CDC/2005)• Malaria during Pregnancy Resource Package (JHPIEGO/2003)
English, French, Portuguese: all soon to be updated [email protected]
• Malaria in Pregnancy: Guidelines for Measuring Key Monitoring and Evaluation Indicators (WHO/Draft): available from CDC
IPTi• IPTi Consortium website: www.ipti-malaria.org

Questions?