epidemiology and control of cholera by dr. awatif alam
Post on 21-Dec-2015
224 views
TRANSCRIPT

EPIDEMIOLOGYEPIDEMIOLOGYANDAND
CONTROLCONTROLOFOF
CHOLERACHOLERA
BYBY
DR. AWATIF ALAMDR. AWATIF ALAM

IDENTIFICATION:IDENTIFICATION:
- An acute bacterial disease (enteric), - An acute bacterial disease (enteric),
- sudden onset of profuse watery - sudden onset of profuse watery stools, stools,
- occasional vomiting, - occasional vomiting,
- rapid dehydration, acidosis ,- rapid dehydration, acidosis ,
- circulatory collapse.- circulatory collapse.
Prognosis:Prognosis:
* Asymptomatic infection occur * Asymptomatic infection occur much more frequently than much more frequently than clinical illness,clinical illness,
* In severe cases (untreated) , * In severe cases (untreated) , death can happen (within few death can happen (within few hours ) ,hours ) ,
* C.F.R ≈ 50%, but with proper * C.F.R ≈ 50%, but with proper Rx, C.F.R.Rx, C.F.R. < 1%.< 1%.
DIAGNOSIS:DIAGNOSIS:
- Confirmed by culturing Cholera - Confirmed by culturing Cholera vibrio of serotype 01 from vibrio of serotype 01 from feceas ,feceas ,
oror
- significant rise in titer of - significant rise in titer of antitoxic antibodies, antitoxic antibodies,
oror
- presence of agglutinating or - presence of agglutinating or virbiocidal antibodies.virbiocidal antibodies.
Infectious Agent:Infectious Agent:
Group A – Vibrio cholerae Serogroup 01Group A – Vibrio cholerae Serogroup 01 (which includes)(which includes)
-- El-TorEl-Tor - classical or true :- classical or true :
INABA, Hikojima, or OGAWAINABA, Hikojima, or OGAWA
True cholera vibrio is demonstrated by:-True cholera vibrio is demonstrated by:- - presence of specific O antigen and - presence of specific O antigen and
- no hemolysis of goat or sheep RBCs if - no hemolysis of goat or sheep RBCs if added to suspension of these cells.added to suspension of these cells.
Group B – non cholera Vibrios.Group B – non cholera Vibrios. (Non pathogenic to man)(Non pathogenic to man)
- Most vibrio strains elaborate enterotoxin - Most vibrio strains elaborate enterotoxin resulting in similar resulting in similar clinical pictureclinical picture
- In any single epidemic one particular - In any single epidemic one particular type type tends to be dominanttends to be dominant
(presently (presently El Tor biotypeEl Tor biotype is predominant is predominant except in Bangladesh, where the except in Bangladesh, where the classicalclassical biotypebiotype has reappeared). has reappeared).

In 1992, a new serogroupIn 1992, a new serogroup – a genetic – a genetic
derevative of the EL TOR biotype – derevative of the EL TOR biotype – emerged in Bangladesh and caused emerged in Bangladesh and caused an extensive epidemic.an extensive epidemic.
It has now spread over large parts of AsiaIt has now spread over large parts of Asia
and is termed and is termed Vibrio Cholerae o139Vibrio Cholerae o139
“ “ BENGAL”.BENGAL”.
Occurrence:-Occurrence:-
- During During 19th century19th century pandemic cholera pandemic cholera repeatedly spread from India to most of repeatedly spread from India to most of the world.the world.
- During - During Ist half of 20th centuryIst half of 20th century, the , the disease was confined largely to Asia disease was confined largely to Asia
(except for severe epidemic in Egypt in (except for severe epidemic in Egypt in 19471947).).
- - Since 1961Since 1961, cholera spread from Indonesia, cholera spread from Indonesia
to Western Europe , and AFRICA. to Western Europe , and AFRICA.

OCCURRENCE:-OCCURRENCE:-
- During 1977 and 1978- During 1977 and 1978 outbreaks outbreaks were reported from were reported from Japan*,Japan*,
- - In 1983In 1983; ; 13 African countries13 African countries reported the disease,reported the disease,
- The - The Western hemisphereWestern hemisphere was free was free from cholera between 1911 – 1973 from cholera between 1911 – 1973
(except for 2 lab. acquired cases)(except for 2 lab. acquired cases)

OCCURRENCE:OCCURRENCE:
In 1991In 1991 cholera appeared in South America, cholera appeared in South America, ( it had been absent for > century ).( it had been absent for > century ).
Within a year it spread to 11 countries, and Within a year it spread to 11 countries, and through the continent.through the continent.
In 1992In 1992 large outbreaks began in India & large outbreaks began in India & Bangladesh.Bangladesh.
““Such outbreaks was caused by a previously Such outbreaks was caused by a previously unrecognized serogroup” ( O139\Bengal ).unrecognized serogroup” ( O139\Bengal ).
It is a more virulentIt is a more virulent variant of EL TOR biotype. variant of EL TOR biotype.


Cholera in Southern Sudan Cholera in Southern Sudan 28 Jan. – 3 March 2006 28 Jan. – 3 March 2006
Vibrio cholera Inaba hasVibrio cholera Inaba has
been lab. confirmed.been lab. confirmed. 5 634 cases and 127 deaths5 634 cases and 127 deaths C.F.R 2.25 %C.F.R 2.25 % For more details check:For more details check:
www.who.intwww.who.int

SIZE OF THE PROBLEM GLOBALLY:SIZE OF THE PROBLEM GLOBALLY: 140 000 – 290 000 cases were 140 000 – 290 000 cases were
reported reported between 1997- 1998.between 1997- 1998.
In 1999, global incidence was about In 1999, global incidence was about 254 000 , and Africa alone accounted 254 000 , and Africa alone accounted
for about 81% of the global total for about 81% of the global total number of cases.number of cases.
In 2000, multiple outbreaks were In 2000, multiple outbreaks were reported in populations in various reported in populations in various islands of islands of Oceania .Oceania .


Reservoir:- Reservoir:- Man :Man :
- A patient during - A patient during incubation incubation periodperiod (faeces)(faeces)
- A patient during - A patient during illnessillness
(faeces & vomitus)(faeces & vomitus)
- A patient during - A patient during convalescenceconvalescence (faeces)(faeces)
- Contact through - Contact through faecesfaeces

Mode of Transmission:-Mode of Transmission:-
A. Primary ingestion of A. Primary ingestion of water water (contaminated with faeces or vomitus of (contaminated with faeces or vomitus of patientspatients, or, or
to lesser extent to faeces of to lesser extent to faeces of carrierscarriers).). OROR B. Ingestion of B. Ingestion of foodfood contaminated by dirty contaminated by dirty
water, faeces, soiled hands or flies. water, faeces, soiled hands or flies.
C. Use of soiled articles (e.g. utensils, C. Use of soiled articles (e.g. utensils, clothes and bedlinen) “to lesser extent.”clothes and bedlinen) “to lesser extent.”
Poor sanitation transmits many diseases. Each Poor sanitation transmits many diseases. Each year 1.3 million children die from diarrhoeal year 1.3 million children die from diarrhoeal diseases alone. diseases alone. Ensuring safe methods of excreta disposal, Ensuring safe methods of excreta disposal, access to latrines at home and in schools, and access to latrines at home and in schools, and encouraging encouraging hand washing.hand washing.

INCUBATION PERIOD:INCUBATION PERIOD:
Few hours – 5 days.Few hours – 5 days.
“ “ The international I.P. is 5- days “.The international I.P. is 5- days “. Period of Communicability:Period of Communicability:
- For the duration of stool ve+ stage - For the duration of stool ve+ stage
(usually few days after recovery)(usually few days after recovery)
- Carrier state may persist for few months- Carrier state may persist for few months
*NOTE:*NOTE:
Effective antibiotic eg. (tetracycline) Effective antibiotic eg. (tetracycline) reduce the period of communicability. reduce the period of communicability.
Suscept. And Resistance:-Suscept. And Resistance:-
Susceptibility is general and variableSusceptibility is general and variable
Gastric achlorhydria increases the Gastric achlorhydria increases the risk risk
People with low S.E.S groups are at People with low S.E.S groups are at higher risk.higher risk.

Unsanitary environment:Unsanitary environment:
WHO cholera 6th report stated WHO cholera 6th report stated factors favouring endemicity in factors favouring endemicity in
India India (lower Bengal area):(lower Bengal area): High density population,High density population, Increased humidity,Increased humidity, Abundance of uncontrolled H20 supply,Abundance of uncontrolled H20 supply, High salinity and organic water contents.High salinity and organic water contents.
**-**- An attack gives temporary immunityAn attack gives temporary immunity
(against a homologus serotype through a (against a homologus serotype through a rise in agglutinating, vibriocidal and rise in agglutinating, vibriocidal and antitoxin antibodies which all lead to antitoxin antibodies which all lead to resistance).resistance).

METHODS OF CONTROLMETHODS OF CONTROL A-Preventive measures:- A-Preventive measures:-
1- Sanitary disposal of human faeces 1- Sanitary disposal of human faeces (maintenance of fly proof latrines). (maintenance of fly proof latrines).
2- Protect, purify and chlorinate public 2- Protect, purify and chlorinate public
water supplies. water supplies.
(avoid cross connectns. with sewer syst.).(avoid cross connectns. with sewer syst.).
3- Control flies by spraying with insectici.3- Control flies by spraying with insectici.

4- Cleanliness in preparation of 4- Cleanliness in preparation of food,food,
5- Pasteurize or boil 5- Pasteurize or boil milkmilk ,,
6- Sanitary supervision of 6- Sanitary supervision of commercial commercial milkmilk production, production, storage and deliverystorage and delivery..

Control of patients, contact Control of patients, contact and environment:-and environment:-
Reporting to local health authority,Reporting to local health authority,
Cleanliness in preparation of food,Cleanliness in preparation of food,
Pasteurize or boil of milk and Pasteurize or boil of milk and sanitary supervision of commercial sanitary supervision of commercial milk productn. storage and delivery.milk productn. storage and delivery.

Isolation or hospitalization with Isolation or hospitalization with enteric precautions esp. for enteric precautions esp. for severely ill pts.severely ill pts.
eg. (effective hand washing + fly eg. (effective hand washing + fly control measures).control measures).
Disinfection of articles soiled with Disinfection of articles soiled with faeces or vomits of patients (by faeces or vomits of patients (by heat, carbolic acid or other effective heat, carbolic acid or other effective disinfectant).disinfectant).
Contacts:-Contacts:-
- Surviellance- Surviellance for 5-days. for 5-days.
- Chemoprophylaxis- Chemoprophylaxis with tetracycline. with tetracycline.
-- No immunization necessary.No immunization necessary.
- Investigate contacts with source - Investigate contacts with source of of
infection. infection.
- Specific Rx:-- Specific Rx:-
* Prompt fluid replacement using * Prompt fluid replacement using adequate volumes of electrolytes adequate volumes of electrolytes solutions, to correct dehydration. solutions, to correct dehydration.

Epidemic Measures:-Epidemic Measures:-1- Essential measures :1- Essential measures :
- Hygienic disposal of human faeces.- Hygienic disposal of human faeces.
- Adopting emergency measures to - Adopting emergency measures to assure a safe water supply (boiling assure a safe water supply (boiling and chlorination).and chlorination).
- Good food hygiene.- Good food hygiene.
Effective Food Hygiene Measures:
a- Cooking food thoroughly & eating it whilea- Cooking food thoroughly & eating it while still hot;still hot; b- Preventing cooked food from being b- Preventing cooked food from being
contaminatedcontaminated by contact with raw food by contact with raw food (water & ice), or with contaminated (water & ice), or with contaminated surfacessurfaces or flies.or flies.
c- Avoiding raw fruits or vegetables unless c- Avoiding raw fruits or vegetables unless they are they are first peeledfirst peeled..
d- d- Hand washingHand washing after defecation, esp. after defecation, esp. before contact with food or drinking water.before contact with food or drinking water.
2- Two available types of 2- Two available types of vaccinesvaccines which provide high level of protection which provide high level of protection for several months against for several months against
vibrio cholerae vibrio cholerae serotype o1serotype o1..
( Of use for travellers to endemic countries,( Of use for travellers to endemic countries, but not yet used for public health but not yet used for public health
purposes ).purposes ).
3- Notification ( of WHO & adjacent 3- Notification ( of WHO & adjacent countries) is required if any case is countries) is required if any case is first diagnosed in a country.first diagnosed in a country.

4- Health education in personal 4- Health education in personal hygiene.hygiene.
5- Search for source of infection.5- Search for source of infection.
6- Specific measures during 6- Specific measures during pilgrimage pilgrimage season.season.
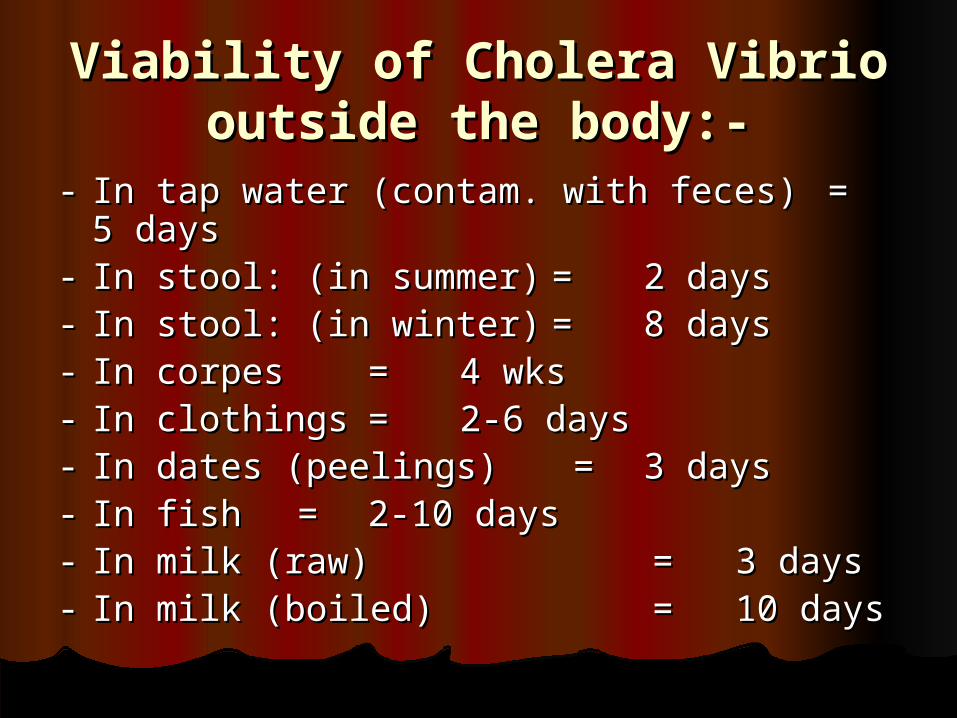
Viability of Cholera Vibrio Viability of Cholera Vibrio outside the body:-outside the body:-
-- In tap water (contam. with feces)In tap water (contam. with feces) == 5 5 daysdays
-- In stool: (in summer)In stool: (in summer) == 2 days2 days-- In stool: (in winter)In stool: (in winter) == 8 days8 days-- In corpesIn corpes == 4 wks4 wks-- In clothingsIn clothings == 2-6 days2-6 days-- In dates (peelings)In dates (peelings) = = 3 days3 days-- In fishIn fish = = 2-10 days2-10 days-- In milk (raw)In milk (raw) = = 3 days3 days-- In milk (boiled)In milk (boiled) = = 10 days10 days