enroll now! - brochure.fringebenefitsgroup.combrochure.fringebenefitsgroup.com/languageline_oe...
TRANSCRIPT

» MEC Preventive Services
» Medical Coverage
» Other Benefit Options
» FAQ’s
» Missed Premium
» Additional Programs
» Important Notices
Highlights:
Minimum Essential Coverage (MEC)
As a valued OnLine Interpreters team member, we continually seek to provide you with benefits that deliver excellent coverage and valuable options for you and your family. With that in mind, we are pleased to off offer a Minimum Essential Coverage (MEC) program. The MEC is designed to provide you and your family preventive services and to meet the “Individual Mandate” under the Affordable Care Act (ACA) in order to avoid being subject to tax penalties during the time that you are covered.
If you are currently enrolled in the fixed indemnity program you can continue with this program separately or in addition to the MEC program to help supplement your healthcare costs.
We are providing you with affordable options that will meet your coverage requirement. Please carefully review the coverage options to determine which plan might be right for you and your dependents. The plans offered are not major medical insurance and not designed to protect you from cost associated with chronic illnesses or diseases.
OPEN ENROLLMENT WILL BE HELD NOVEMBER 30TH - DECEMBER 16TH!
Enroll by one of two methods: 1) Go online to www.TheAmericanWorker.com and enroll yourself in the coverage of your choice. 2) Call the Enrollment Center at 1-800-690-7731 and speak with an Enrollment Representative to answer your questions and process your elections.
LanguageLine Solutions is contributing 75% of the cost of the coverage for employee only coverage in MEC plan!
You will not be eligible to enroll in the MEC program after your initial enrollment period, unless you experience a qualified life event, or at a later annual open enrollment period.
COVERAGE IS EFFECTIVE, DECEMBER 25, 2016 IF A DEDUCTION FOR THE MEC PLAN IS TAKEN FROM YOUR DECEMBER 30, 2016 PAYCHECK.
Enroll Now!OPEN ENROLLMENT
NOVEMBER 30TH - DECEMBER 16TH
Enroll Now!

Minimum Essential Coverage (MEC) As mandated by the Affordable Care Act (ACA), all individuals must purchase health insurance that meets certain requirements beginning January 1, 2014 in order to avoid paying a penalty tax. Minimum Essential Coverage (MEC) - ACA Preventive Only Plan is the coverage level that is required to avoid the “Individual Mandate” coverage penalty under the ACA.
In 2016, individuals who did not obtain MEC faced a tax. It was the greater of 2.5% of adjusted household income or $695 per adult plus $347.50 per child. For tax year 2017, the percentage option will remain at 2.5%, but the flat fee will be adjusted for inflation.
There are 68 preventive services covered at 100% under the required government list of Preventive and Wellness Benefits when utilizing an in-network provider and are not subject to a deductible. A full list of the covered services is included on the next page.
WHAT IS IT?Minimum Essential Coverage or MEC for short, is coverage that satisfies the Individual Mandate under the Affordable Care Act. An individual is required to have coverage under this new law or they will face penalties. When you file your taxes, you will need to provide the IRS with information regarding your healthcare coverage. This plan you are being offered will satisfy this new requirement and you won’t be subject to any fines.
WHAT DOES THIS PLAN COVER?The Preventive Only plan covers 68 specific tests and procedures that the government has outlined and requires that all plans cover these at 100% coverage – which means there is no cost to you and there are no limits on the coverage.
WHAT DOESN’T IT COVER?This plan won’t help you if you are sick or if you’ve already been diagnosed with an illness or ailment. We offer another benefits program – the fixed indemnity plans – that can help you if you get sick or have a chronic condition.
WHY SHOULD I ENROLL?The Preventive Only Plan will help you stay healthy and hopefully will allow you to catch any problems in their early stages, so that there is a greater likelihood of a quick recovery. Procedures are covered at 100% - so there is no cost to you and there is no limit on the number of times the plan can be used. Also, it’s priced very affordably.
CAN I USE ANY DOCTOR?No, with the Preventive Only plan you are required to see a First Health network provider. The plan does not cover out-of-network providers. You can call Member Services at (800) 656- 4577 for assistance in finding a network provider or research for yourself at www.yourmedbenefits.com.
WHAT WILL HAPPEN IF I DON’T SIGN UP ?If you don’t enroll during Open Enrollment , you will have to wait till next year, unless you have a qualifying event. If you don’t get qualifying coverage this year, you may be subject to tax penalties when you file your taxes.
IS THIS MAJOR MEDICAL OR SIMILAR TO COVERAGE ON THE EXCHANGE?No, the Preventive only plan is not major medical and only covers the 63 procedures.
Fixed Indemnity BenefitsFixed Indemnity Benefits pay a set dollar amount for non-preventive medical services you may need that are not covered under MEC such as doctor’s office or emergency room visits if you get sick, hospital stays, surgery, lab work or X-rays. These benefits do not meet the ACA requirements but do pay in addition to other coverage you may have. Claims payments can be made to the service provider or directly to the individual as a reimbursement. With a low cost, these benefits can really help to supplement your medical expenses.
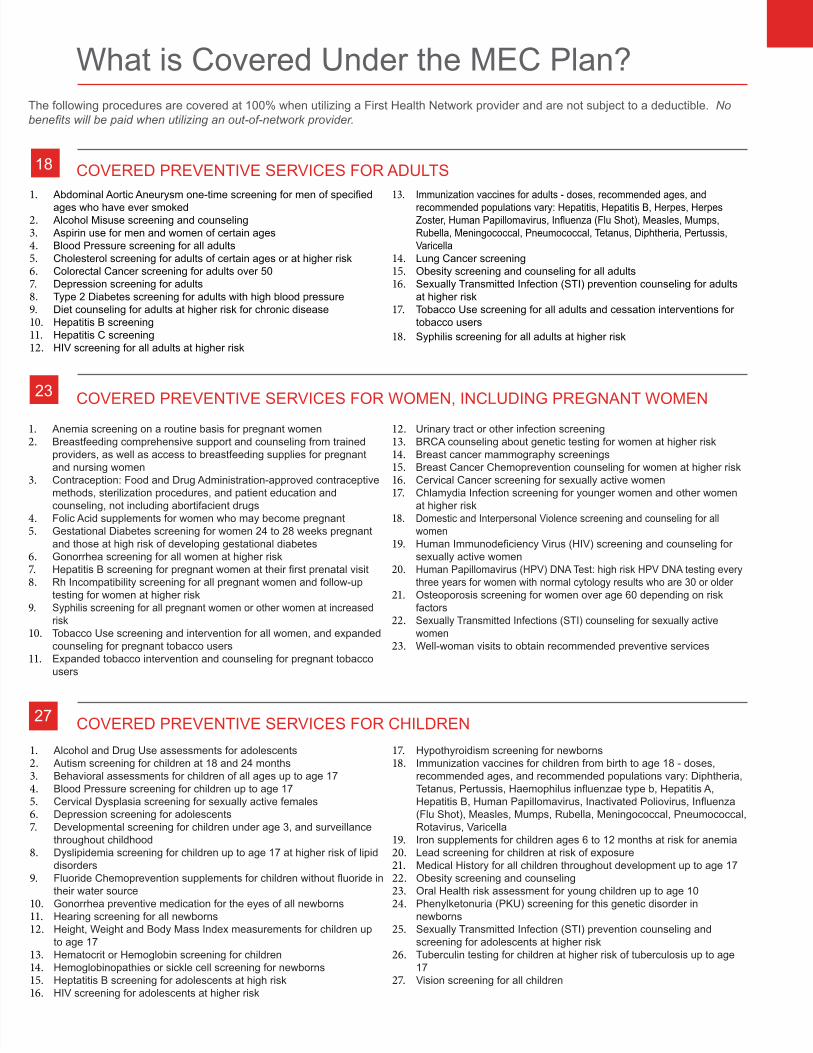
What is Covered Under the MEC Plan?
COVERED PREVENTIVE SERVICES FOR ADULTS18
COVERED PREVENTIVE SERVICES FOR WOMEN, INCLUDING PREGNANT WOMEN 23
COVERED PREVENTIVE SERVICES FOR CHILDREN27
The following procedures are covered at 100% when utilizing a First Health Network provider and are not subject to a deductible. No benefits will be paid when utilizing an out-of-network provider.
1. Abdominal Aortic Aneurysm one-time screening for men of specified ages who have ever smoked
2. Alcohol Misuse screening and counseling3. Aspirin use for men and women of certain ages4. Blood Pressure screening for all adults5. Cholesterol screening for adults of certain ages or at higher risk6. Colorectal Cancer screening for adults over 507. Depression screening for adults8. Type 2 Diabetes screening for adults with high blood pressure9. Diet counseling for adults at higher risk for chronic disease10. Hepatitis B screening11. Hepatitis C screening12. HIV screening for all adults at higher risk
13. Immunization vaccines for adults - doses, recommended ages, and recommended populations vary: Hepatitis, Hepatitis B, Herpes, Herpes Zoster, Human Papillomavirus, Influenza (Flu Shot), Measles, Mumps, Rubella, Meningococcal, Pneumococcal, Tetanus, Diphtheria, Pertussis, Varicella
14. Lung Cancer screening15. Obesity screening and counseling for all adults16. Sexually Transmitted Infection (STI) prevention counseling for adults
at higher risk17. Tobacco Use screening for all adults and cessation interventions for
tobacco users18. Syphilis screening for all adults at higher risk
1. Anemia screening on a routine basis for pregnant women2. Breastfeeding comprehensive support and counseling from trained
providers, as well as access to breastfeeding supplies for pregnant and nursing women
3. Contraception: Food and Drug Administration-approved contraceptive methods, sterilization procedures, and patient education and counseling, not including abortifacient drugs
4. Folic Acid supplements for women who may become pregnant 5. Gestational Diabetes screening for women 24 to 28 weeks pregnant
and those at high risk of developing gestational diabetes6. Gonorrhea screening for all women at higher risk 7. Hepatitis B screening for pregnant women at their first prenatal visit 8. Rh Incompatibility screening for all pregnant women and follow-up
testing for women at higher risk 9. Syphilis screening for all pregnant women or other women at increased
risk 10. Tobacco Use screening and intervention for all women, and expanded
counseling for pregnant tobacco users 11. Expanded tobacco intervention and counseling for pregnant tobacco
users
12. Urinary tract or other infection screening13. BRCA counseling about genetic testing for women at higher risk 14. Breast cancer mammography screenings15. Breast Cancer Chemoprevention counseling for women at higher risk 16. Cervical Cancer screening for sexually active women 17. Chlamydia Infection screening for younger women and other women
at higher risk 18. Domestic and Interpersonal Violence screening and counseling for all
women 19. Human Immunodeficiency Virus (HIV) screening and counseling for
sexually active women 20. Human Papillomavirus (HPV) DNA Test: high risk HPV DNA testing every
three years for women with normal cytology results who are 30 or older 21. Osteoporosis screening for women over age 60 depending on risk
factors 22. Sexually Transmitted Infections (STI) counseling for sexually active
women 23. Well-woman visits to obtain recommended preventive services
1. Alcohol and Drug Use assessments for adolescents2. Autism screening for children at 18 and 24 months3. Behavioral assessments for children of all ages up to age 174. Blood Pressure screening for children up to age 175. Cervical Dysplasia screening for sexually active females6. Depression screening for adolescents7. Developmental screening for children under age 3, and surveillance
throughout childhood8. Dyslipidemia screening for children up to age 17 at higher risk of lipid
disorders9. Fluoride Chemoprevention supplements for children without fluoride in
their water source10. Gonorrhea preventive medication for the eyes of all newborns11. Hearing screening for all newborns12. Height, Weight and Body Mass Index measurements for children up
to age 1713. Hematocrit or Hemoglobin screening for children14. Hemoglobinopathies or sickle cell screening for newborns15. Heptatitis B screening for adolescents at high risk16. HIV screening for adolescents at higher risk
17. Hypothyroidism screening for newborns18. Immunization vaccines for children from birth to age 18 - doses,
recommended ages, and recommended populations vary: Diphtheria, Tetanus, Pertussis, Haemophilus influenzae type b, Hepatitis A, Hepatitis B, Human Papillomavirus, Inactivated Poliovirus, Influenza (Flu Shot), Measles, Mumps, Rubella, Meningococcal, Pneumococcal, Rotavirus, Varicella
19. Iron supplements for children ages 6 to 12 months at risk for anemia20. Lead screening for children at risk of exposure21. Medical History for all children throughout development up to age 1722. Obesity screening and counseling23. Oral Health risk assessment for young children up to age 1024. Phenylketonuria (PKU) screening for this genetic disorder in
newborns25. Sexually Transmitted Infection (STI) prevention counseling and
screening for adolescents at higher risk26. Tuberculin testing for children at higher risk of tuberculosis up to age
1727. Vision screening for all children

Medical Coverage Options
MEC
MEC Preventive 68 procedures are covered at 100%, when utilizing a First Health provider
FIXED INDEMNITY
Doctor’s Office Benefit $60 per day, 6 days per person per year
Hospital Admission Benefit $500 per confinement
Daily In-Hospital Indemnity - Intensive Care - Mental Illness - Substance Abuse - In-Patient Skilled Nursing
$200 per day, 500 days lifetime max$400 per day, 30 days per person per year$100 per day, 30 days per person per year
$100 per day, 30 days per person per calendar year$100 per day, 60 days per in-patient stay
Surgical Indemnity Benefit - Daily Inpatient Surgical - Daily Outpatient Surgical - Daily Outpatient Minor Surgical - Outpatient Benefit Maximum - Anesthesia
$1,000 per day, 1 day per year$500$100
1 day per year30% of Surgical Benefit
Outpatient Diagnostic X-Ray $100 per testing day, 3 days per person per year
Outpatient Diagnostic Laboratory $85 per testing day, 3 days per person per year
Outpatient Diagnostic Advanced Studies Indemnity Benefit $100 per testing day, 3 days per person per year
Emergency Room Benefit for Illness Only $75 per day, 4 days per person per year
*The above benefits are underwritten by Nationwide Life Insurance Company
ADDITIONAL PROGRAMS
First Health Network Doctors and Hospitals
Prescription Drugs Discount Pharmacy Program
Discount Program
Included Teladoc, Medical Bill Saver™, Counseling, Nurseline™, Chiropractic/Vision/ Hearing discounts
BI-WEEKLY RATESEmployee Only $11.73
Employee + Child $51.61
Employee + Spouse $65.53Family $88.36
Nationwide Insurance and the Nationwide framemark are service marks of Nationwide Mutual Insurance Company.
The MEC preventative procedures are provided through a self-insurance plan with employer contributions made on your behalf. The Fixed Indemnity benefit is underwritten by Nationwide.

Critical Illness (C.I.) Benefit Amount (Includes first occurence of one of the following covered conditions: End-Stage Renal Failure, Heart Attack, Life Threatening Cancer, Major Organ Transplant, Stroke) Employee (Age reductions apply): $10,000 Spouse: $5,000 Child (6 mos to 26 yrs): $2,500 Life Benefit Amount Employee (Age reductions apply): $10,000 Spouse: $5,000 Child (6 mos to 26 yrs): $2,500 Infant (10 days to 6 mos): $400
AD&D Benefit Amount Employee (Age reductions apply): $10,000
Accident Expense Benefit Amount Per Person, per occurrence: $2,500
Dental Care:Annual Deductible:Annual Maximum:Preventative and Diagnostic(routine exams and cleanings, fluoride treatment, x-rays)
Basic Treatment: (extractions, fillings, endodontics, periodontics)
Major Treatments(crowns, dentures)
Orthodontia:
$50 per covered person$500 per covered personPlan pays 100% of Usual & Customary Rate (UCR)
Plan pays 60% of UCR after a 6 months waiting period
Plan pays 50% of UCR after a 12 months waiting period
Not covered
Premium Bi-Weekly Employee Only $12.16 Employee + Child $21.89 Employee + Spouse $30.41 Family $32.84
Vision Care:Annual Maximum:Co-insurance: Routine Exam: Lenses/Frames or Contacts:
DENTAL / VISION
SHORT-TERM DISABILITY
CRITICAL ILLNESS (C.I.) / LIFE / AD&D / ACCIDENT
$300 per covered person80%1 every 12 months1 pair every 24 months
Premium Bi-Weekly Employee Only $12.36 Employee + Child $22.25 Employee + Spouse $26.41 Family $28.26
Premium Bi-Weekly Employee Only $3.04
This benefit is payable for non-occupational injuries and sickness only.
Benefit Amount:Waiting Period:Max Benefit Period:
$125 per week15 Days26 Weeks
Other Great Benefit OptionsBelow are critical illness/life/accident, short–term disability (STD) and dental/vision benefits which can also be purchased. All plans are insured by Nationwide Life Insurance Company. Please review these plans and make the choice that best suits your needs. The Enrollment Center can answer your questions regarding eligibility and how the plan works.

Benefit Detail Plan Pays DescriptionHospital Admission Benefit: $1,000 • Benefit payable only once during any period of confinement.
• Requires a 24 hour hospital stay.Daily In-Hospital Benefit: $100 per day • Benefit payable per day.
• Up to a lifetime maximum of 500 days of confinement.• Requires a 24-hour hospital stay.
Intensive Care Benefit $200 per day • Double the daily in-hospital benefit will be paid, up to a maximum of 30 days per calendar year.
Mental Illness Disorder $50 per day • $50 per day will be paid up to $5,000 per cal year maximum and lifetime maximum of $30,000.
In-Patient Skilled Nursing Facility
$50 per day • $50 per day will be paid up to a maximum of 60 days per confinement. • The confinement is covered only if it follows a covered hospital stay of at least 3 days.
Substance Abuse $50 per day • $50 per day will be paid, up to a maximum of 30 days per calendar year.• Lifetime maximum is $30,000.
Bi-Weekly PremiumEmployee Only $ 7.70 Employee + Child $13.86Employee + Spouse $19.25Family $24.40
INPATIENT HOSPITAL
Nationwide Insurance and the Nationwide framemark are service marks of Nationwide Mutual Insurance Company.
Other Great Benefit OptionsThe Inpatient Hospital Benefit provides coverage based on a schedule of benefits per service. This benefit is insured by Nationwide Life Insurance Company. Please review these plans and make the choice that best suits your needs. The Enrollment Center can answer your questions regarding eligibility and how the plan works.

Frequently Asked QuestionsWHEN CAN I ENROLL?If you do not enroll during Open Enrollment, you will not be able to make changes during the year unless you experience a qualified status change. Newly hired employees may enroll within 60 days of their date of hire.
WHO IS ELIGIBLE TO ENROLL?You and your eligible dependents may enroll. An eligible dependent is an employee’s spouse and child(ren) from birth to age 26.
WILL I RECEIVE AN ID CARD?Yes, you will receive three ID cards along with information about each coverage you elect. These will be mailed to your home address.
WHO CAN I CONTACT IF I HAVE QUESTIONS ABOUT MY BENEFITS?Contact Member Services, toll-free at 1-800-517-4791. They are open Monday through Friday from 7:00 a.m. to 7:00 p.m. Central Time.
WHAT IS THE MEC PREVENTIVE COVERAGE?This is coverage that satisfies the Individual Mandate under the Affordable Care Act. An individual is required to have coverage under this new law or they will face penalties. When you file your taxes, you will need to provide the IRS with information regarding your healthcare coverage. This plan you are being offered will satisfy this new requirement and you won’t be subject to any fines during the period for which you are covered.
HOW WILL MY PREMIUMS BE PAID?Premiums will be paid through payroll deductions on a bi-weekly basis. Benefit deductions will be on a pretax basis. Elections cannot be changed during the plan year, unless you have qualifying event, per IRS code rules. The term life/AD&D, dependent life and short-term disability premiums will be deducted on an after-tax basis.
HOW DO I SUBMIT A MEDICAL CLAIM?There are two ways to file a claim for benefits under this plan:
Option 1 - Present your ID card to the provider at the time of service. If the provider will file the claim with the insurance company on your behalf, then you do not have to pay for the services in advance. The insurance carrier will pay that benefit to the provider. You would be responsible for paying the provider any billed amount that the insurance company does not pay them.
Option 2 - Pay the full billed amount to the provider and submit a claim for reimbursement to the insurance carrier. When filing a claim for reimbursement, you need to provide the certificate or member number from your insurance booklet and original bill for service which includes the patient name, date of service, diagnosis code and itemized charges, along with a reimbursement form. Benefit will be payable to you.
CAN I USE ANY DOCTOR FOR PREVENTIVE SERVICES?No, with the Preventive plan you are required to see a First Health network provider. The plan does not cover out-of-network claims. You can call Member Services at 1-800-517-4791 for assistance in finding a network provider or go to www.yourmedbenefits.com.
WHAT WILL HAPPEN IF I DON’T SIGN UP FOR MEC PREVENTIVE COVERAGE?If you don’t enroll, you will have to wait until the next annual open enrollment period, unless you have a qualifying event. If you don’t get qualifying coverage this year, you may be subject to Individual Mandate tax penalties when you file your taxes.
HOW DO I GET REIMBURSED FOR MY CONTRACEPTIVE PRESCRIPTIONS?Contraceptive prescriptions are covered at 100% under all medical plans as a preventive service. You will need to pay out of pocket when picking up your prescription. Then you will complete and submit a reimbursement form for payment.

Missed Premium
DOES YOUR INCOME VARY FROM PAYCHECK TO PAYCHECK? SOME PAYROLL PERIODS MAY NOT HAVE ENOUGH FUNDS TO COVER THE COST OF YOUR BENEFITS.
You have 30 days to pay for the premiums that could not be deducted from your paycheck. If you do not pay the missed premiums within 30 days you will be unable to pay for them at a later date. If you carry the medical benefits and pay missed premium you will be responsible for the full premium, meaning the employee as well as the employer rate. If have missed premium deductions and want to find out the balance due or have questions about making payment, contact Member Services at 1-800-517-4791 or go online to www.TheAmerican Worker.com. You can authorize us to charge a credit/debit card or draft your bank account anytime you have had a missed deduction form your paycheck. This authorization can be setup online at www.TheAmericanWorker.com at any time or when you are enrolling.
HOW DO I PAY MISSED PREMIUMS?
To pay by credit/debit card or electronic check:
» Go to www.TheAmericanWorker.com. » If this is your first time visiting the site, use the “New User?” box and sign in using your Social Security
Number and date of birth (if requested, the Group ID is 97640). From there you will be prompted to verify your contact information (one time process) and setup a username and password. » If you have already created a user account select the “Returning User?” box and enter your username
and password. The Security Question tool can assist in instances where you cannot remember your username or password. » Once logged in, click “Billing” and follow the instructions.
To pay missed premiums by check or money order:
» Attach the payment to a missed premium form and write the group number, FV1220, on your payment. » Make sure the check or money order is written for the total amount due and is made payable to
Nationwide Life Insurance Company. » Mail your payment along with the missed premium form to:
Nationwide Life Insurance Company 11910 Anderson Mill Road, Suite 401 Austin, TX 78726

Additional Programs
FIRST HEALTH NETWORKThe First Health Network provides access to one of the nation’s largest and most respected networks. By going to a First Health provider you can reduce your out-of-pocket expenses and stretch your benefit dollars.
» Access to more than 490,000 provider locations across all 50 states and the District of Columbia » First Health logo on medical ID card for fast and easy recognition by the provider » Re-priced claims will be assigned directly to the provider to simplify the claims process
To find a provider online, visit www.yourmedbenefits.com. Members retain the ability to choose any doctor they wish and have those claims assigned under the illness and accident plans. All illness and accident benefits will pay as specified in the benefit provisions of the policy regardless of the provider chosen.
The MEC Preventive Plan requires First Health network use.
DISCOUNT HEALTH SAVINGS PROGRAMAdministered by New Benefits, Ltd. Your membership provides significant savings on the following services: » Vision » Hearing » Chiropractic » Vitamins & Diabetic Supplies
In addition, members also receive access to the following: » Teladoc » Health Advocate Services (Medical Bill SaverTM, Medical Health Advisor, NurselineTM) » Counseling Services
TELADOCAdministered by New Benefits, Ltd. Teladoc provides 24/7 access to a national network of U.S. board-certified doctors who can resolve many of your medical issues via telephone. Teladoc doctors can diagnose, treat and prescribe medication, when necessary, for medical issues including cold and flu symptoms, allergies, bronchitis, sinus problems, urinary tract infection, respiratory infection, pink eye, ear infection and more!
HEALTH ADVOCATE SERVICESAdministered by New Benefits, Ltd. » Medical Bill Saver™ - The Health Advocate Medical Bill Saver™ benefit can lower out-of-pocket costs on medical
bills not covered by insurance. Advocates will work with healthcare providers and attempt to lower the balance on any uncovered medical or dental bill over $400. » Medical Health Advisor - The services are organized around Personal Health Advocates, typically registered nurses,
supported by a team of medical directors and administrative experts, who assist individuals in getting the most value from their healthcare benefits. One call to Medical Health Advisor and we’ll help members resolve insurance claims and billing issues. Health Advocate does not replace health insurance, provide medical care or recommend treatment.
DISCOUNT PRESCRIPTION PROGRAMAdministered by New Benefits, Ltd. The neighborhood pharmacy program assures members the lowest price on prescription drugs, saving 10% to 85% on most prescriptions. It’s simple to use. The member simply presents the membership card to the pharmacist with the prescription. The pharmacist calculates the discount and the member pays the discounted price. No other forms required. Pharmacy locations may be obtained by contacting customer service at 800-800-7616. Pharmacy Discounts are Not Insurance and are Not Intended as a Substitute for Insurance. The discount is only available at participating pharmacies.

Important NoticesFixed indemnity medical benefits provided under the Minor Illness and Accident plans.The Nationwide program is not intended or recommended to replace any comprehensive program of insurance in which you currently participate, or intend to participate. This plan is not designed to replace or provide major medical or catastrophic coverage. This brochure is for summary purposes only. The insurance benefits for the medical indemnity plan are underwritten by Nationwide Life Insurance Company. Additional information will be provided upon enrollment in the Program. Plan exclusions and limitations apply.
DISCLOSURESThe Discount Health Savings Program is NOT insurance. The plan is not insurance coverage and does not meet the minimum creditable coverage requirements under the Affordable Care Act or Massachusetts M.G.L. c. 111M and 956 CMR 5.00. This plan provides discounts at certain healthcare providers for medical services. This plan does not make payments directly to the providers of medical services. The plan member is obligated to pay for all healthcare services but will receive a discount from those healthcare providers who have contracted with the discount plan organization. This discount card program contains a 30 day cancellation period. The range of discounts for medical or ancillary services provided under the plan will vary depending on the type of provider and medical or ancillary service received. Member shall receive a full refund of membership fees if membership is cancelled within the first 30 days after the effective date. AR and TN residents: A refund of all fees will be issued if membership is cancelled within the first 30 days. Discount Medical Plan Organization: New Benefits, Ltd., Attn: Compliance Department, PO Box 671309 Dallas, TX 75367-1309, 800-800-7616. Website to obtain participating providers: MyMemberPortal.com.
The Discount Prescription Program is not considered “Creditable Coverage” under the Medicare Part D regulations. Medicare eligible individuals may have to pay higher costs if they delay enrolling in the Medicare Pharmacy plan.
Teladoc is not available to Idaho residents. © 2014 Teladoc, Inc. All rights reserved. Teladoc and the Teladoc logo are registered trademarks of Teladoc, Inc. and may not be used without written permission. Teladoc does not replace the primary care physician. Teladoc does not guarantee that a prescription will be written. Teladoc operates subject to state regulation and may not be available in certain states. Teladoc does not prescribe DEA controlled substances, non-therapeutic drugs and certain other drugs which may be harmful because of their potential for abuse. Teladoc physicians reserve the right to deny care for potential misuse of services. Teladoc phone consultations are available 24 hours, 7 days a week while video consultations are available during the hours of 7am to 9pm, 7 days a week.
MEC PREVENTIVE INFORMATION
This Plan is designed to provide Plan Participants with minimum essential coverage under the federal income tax rules. This Plan is designed so that Plan Participants may enroll in this Plan and not have to pay a federal individual income tax penalty. However, while you are enrolled in this Plan, you will not be eligible for a federal tax credit through a federal or state exchange (sometimes referred to as the insurance marketplace). If you do not enroll in this Plan, you may be eligible for a federal tax credit that lowers your monthly premium or a reduction in certain cost-sharing if you enroll in a health insurance plan through the federal or state exchange. This plan does not provide essential health benefits that an individual can purchase through the exchange.
NETWORK BENEFITS ONLYIMPORTANT: This Plan only pays benefits if you receive care through a Network Provider. No benefits are paid or provided if you receive care from an out of network provider.

1 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
This is only a summary. If you want more detail about your coverage and costs, you can get the complete terms in the policy or plan document at www.fbg.com or by calling 1-855-495-1190.
Important Questions Answers Why this Matters:
What is the overall deductible? $0 See the chart starting on page 2 for your costs for services this plan covers.
Are there other
deductibles for specific services?
No You don’t have to meet deductibles for specific services, but see the chart starting on page 2 for other costs for services this plan covers.
Is there an out–of–pocket limit on my expenses?
No There is no limit on how much you could pay during a coverage period for your share of the cost of covered service.
What is not included in
the out–of–pocket limit?
This plan has no out-of-pocket limit.
Not applicable because there’s no out-of-pocket limit on your expenses.
Is there an overall annual limit on what the plan pays?
No The chart describes any limits on what the plan will pay for specific covered services, such as office visits.
Does this plan use a network of providers?
Yes
For a list of participating providers, see www.firsthealthlbp.com
If you use an in-network doctor or other health care provider, this plan will pay some or all of the costs of covered services. Be aware, your in-network doctor or hospital may use an out-of-network provider for some services. Plans use the term in-network, preferred, or participating for providers in their network. See the chart starting on page 2 for how this plan pays different kinds of providers.
Do I need a referral to see a specialist?
No You can see the specialist you choose without permission from this plan.
NOTE: Only preventive services performed by specialists are covered by this plan.
Are there services this plan doesn’t cover?
Yes Some of the services this plan doesn’t cover are listed on page 4. See your policy or plan document for additional information about excluded services.

2 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Copayments are fixed dollar amounts (for example, $15) you pay for covered health care, usually when you receive the service.
Coinsurance is your share of the costs of a covered service, calculated as a percent of the allowed amount for the service. For example, if the plan’s allowed amount for an overnight hospital stay is $1,000, your coinsurance payment of 20% would be $200. This may change if you haven’t met your deductible.
The amount the plan pays for covered services is based on the allowed amount. If an out-of-network provider charges more than the allowed amount, you may have to pay the difference. For example, if an out-of-network hospital charges $1,500 for an overnight stay and the allowed amount is $1,000, you may have to pay the $500 difference. (This is called balance billing.)
This plan may encourage you to use participating providers by charging you lower deductibles, copayments and coinsurance amounts.
Common
Medical Event Services You May Need
Your Cost If You Use an In-network Provider
Your Cost If You Use an
Out-of-network Provider
Limitations & Exceptions
If you visit a health care provider’s office or clinic
Primary care visit to treat an injury or illness Not Covered Not Covered ---None---
Specialist visit Not Covered Not Covered ---None---
Other practitioner office visit Not Covered Not Covered ---None---
Preventive care/screening/immunization No Charge Not Covered Certain age restrictions may apply.
If you have a test Diagnostic test (x-ray, blood work) Not Covered Not Covered ---None---
Imaging (CT/PET scans, MRIs) Not Covered Not Covered ---None---

3 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Common
Medical Event Services You May Need
Your Cost If You Use an In-network Provider
Your Cost If You Use an
Out-of-network Provider
Limitations & Exceptions
If you need drugs to treat your illness or condition
Generic drugs Not Covered Not Covered
FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Preferred brand drugs Not Covered Not Covered
FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Non-preferred brand drugs Not Covered Not Covered
FDA approved contraceptive methods as prescribed by a health care provider for women with reproductive capacity (not including abortifacient drugs).
Specialty drugs Not Covered Not Covered ---None---
If you have outpatient surgery
Facility fee (e.g., ambulatory surgery center) Not Covered Not Covered ---None---
Physician/surgeon fees Not Covered Not Covered ---None---
If you need immediate medical attention
Emergency room services Not Covered Not Covered ---None---
Emergency medical transportation Not Covered Not Covered ---None---
Urgent care Not Covered Not Covered ---None---
If you have a hospital stay
Facility fee (e.g., hospital room) Not Covered Not Covered ---None---
Physician/surgeon fee Not Covered Not Covered ---None---
If you have mental health, behavioral health, or substance abuse needs
Mental/Behavioral health outpatient services Not Covered Not Covered ---None---
Mental/Behavioral health inpatient services Not Covered Not Covered ---None---
Substance use disorder outpatient services Not Covered Not Covered ---None---
Substance use disorder inpatient services Not Covered Not Covered ---None---
If you are pregnant Prenatal and postnatal care Not Covered Not Covered ---None---
Delivery and all inpatient services Not Covered Not Covered ---None---

4 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Common
Medical Event Services You May Need
Your Cost If You Use an In-network Provider
Your Cost If You Use an
Out-of-network Provider
Limitations & Exceptions
If you need help recovering or have other special health needs
Home health care Not Covered Not Covered ---None---
Rehabilitation services Not Covered Not Covered ---None---
Habilitation services Not Covered Not Covered ---None---
Skilled nursing care Not Covered Not Covered ---None---
Durable medical equipment Not Covered Not Covered ---None---
Hospice service Not Covered Not Covered ---None---
If your child needs dental or eye care
Eye exam Not Covered Not Covered ---None---
Glasses Not Covered Not Covered ---None---
Dental check-up Not Covered Not Covered ---None---

5 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Excluded Services & Other Covered Services:
Services Your Plan Does NOT Cover (This isn’t a complete list. Check your policy or plan document for other excluded services.)
Acupuncture
Chiropractic care
Diagnostic testing (e.g. X-ray imaging, Labs)
Emergency medical transportation
Home Health Care
Imaging (CT/PET scans, MRIs)
Long-term Care
Office visit to treat an injury or illness
Rehabilitation services
Skilled Nursing Facility
Bariatric surgery
Cosmetic surgery
Durable Medical Equipment
Habilitation services
Hospice Care
Infertility Treatment
Natural / Cesarean Child birth
Prescription Drugs (except preventive)
Routine eye care (adult)
Surgery
Care when traveling outside the U.S.
Dental care (Adult)
Emergency Room services
Hearing aids
Hospital Room & Board
Inpatient or Outpatient Care
Non-preventive prenatal and postnatal care
Private-duty Nursing
Routine foot care
Urgent Care
Other Covered Services (This isn’t a complete list. Check your policy or plan document for other covered services and your costs for these services.)
• Please visit the Healthcare.gov for a complete and current list of Preventative Care Benefits that are required and covered under this plan.

6 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016 -12/23/2017 Summary of Benefits and Coverage: What this Plan Covers & What it Costs Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Your Rights to Continue Coverage:
If you lose coverage under the plan, then, depending upon the circumstances, Federal and State laws may provide protections that allow you to keep health coverage. Any such rights may be limited in duration and will require you to pay a premium, which may be significantly higher than the premium you pay while covered under the plan. Other limitations on your rights to continue coverage may also apply.
For more information on your rights to continue coverage, contact the plan at 1-855-495-1190. You may also contact your state insurance department, the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa, or the U.S. Department of Health and Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov.
Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact the plan at 1-855-495-1190 or the Department of Labor’s Employee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebsa/healthreform.
Does this Coverage Provide Minimum Essential Coverage? The Affordable Care Act requires most people to have health care coverage that qualifies as “minimum essential coverage.” This plan or policy does provide minimum essential coverage.
Does this Coverage Meet the Minimum Value Standard? The Affordable Care Act establishes a minimum value standard of benefits of a health plan. The minimum value standard is 60% (actuarial value). This health coverage does not meet the minimum value standard for the benefits it provides.
Language Access Services: Spanish/Español: Para obtener asistencia en Español, llame al the plan at 1-855-495-1190.
––––––––––––––––––––––To see examples of how this plan might cover costs for a sample medical situation, see the next page.––––––––––––––––––––––

7 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016-12/23/2017 Coverage Examples Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Having a baby (normal delivery)
Managing type 2 diabetes (routine maintenance of
a well-controlled condition)
About these Coverage Examples: These examples show how this plan might cover medical care in given situations. Use these examples to see, in general, how much financial protection a sample patient might get if they are covered under different plans.
Amount owed to providers: $7,540 Plan pays: $ 40 Patient pays: $ 7,500
Sample care costs:
Hospital charges (mother) $2,700
Routine obstetric care $2,100
Hospital charges (baby) $900
Anesthesia $900
Laboratory tests $500
Prescriptions $200
Radiology $200
Vaccines, other preventive $40
Total $7,540
Patient pays:
Deductibles $0
Copays $0
Coinsurance $0
Limits or exclusions $7,500
Total $7,500
Amount owed to providers: $5,400 Plan pays: $100 Patient pays: $ 5,300
Sample care costs:
Prescriptions $2,900
Medical Equipment and Supplies $1,300
Office Visits and Procedures $700
Education $300
Laboratory tests $100
Vaccines, other preventive $100
Total $5,400
Patient pays:
Deductibles $0
Copays $0
Coinsurance $0
Limits or exclusions $5,300
Total $5,300
This is not a cost estimator.
Don’t use these examples to estimate your actual costs under this plan. The actual care you receive will be different from these examples, and the cost of that care will also be different.
See the next page for important information about these examples.

8 of 8
Language Line Interpreters: MEC Plan Coverage Period: 12/25/2016-12/23/2017 Coverage Examples Coverage for: Individual & Family | Plan Type: PPO
Questions: Call 1-855-495-1190 or visit us at www.fbg.com. If you aren’t clear about any of the underlined terms used in this form, see the Glossary. You can view the Glossary at www.dol.gov/ebsa/healthcarereform or call 1-855-495-1190 to request a copy.
Questions and answers about the Coverage Examples:
What are some of the assumptions behind the Coverage Examples?
Costs don’t include premiums.
Sample care costs are based on national averages supplied by the U.S. Department of Health and Human Services, and aren’t specific to a particular geographic area or health plan.
The patient’s condition was not an excluded or preexisting condition.
All services and treatments started and ended in the same coverage period.
There are no other medical expenses for any member covered under this plan.
Out-of-pocket expenses are based only on treating the condition in the example.
The patient received all care from in-network providers. If the patient had received care from out-of-network providers, costs would have been higher.
What does a Coverage Example show?
For each treatment situation, the Coverage Example helps you see how deductibles, copayments, and coinsurance can add up. It also helps you see what expenses might be left up to you to pay because the service or treatment isn’t covered or payment is limited.
Does the Coverage Example predict my own care needs?
No. Treatments shown are just examples.
The care you would receive for this condition could be different based on your doctor’s advice, your age, how serious your condition is, and many other factors.
Does the Coverage Example predict my future expenses?
No. Coverage Examples are not cost
estimators. You can’t use the examples to estimate costs for an actual condition. They are for comparative purposes only. Your own costs will be different depending on the care you receive, the prices your providers charge, and the reimbursement your health plan allows.
Can I use Coverage Examples to compare plans?
Yes. When you look at the Summary of
Benefits and Coverage for other plans, you’ll find the same Coverage Examples. When you compare plans, check the “Patient Pays” box in each example. The smaller that number, the more coverage the plan provides.
Are there other costs I should consider when comparing plans?
Yes. An important cost is the premium
you pay. Generally, the lower your premium, the more you’ll pay in out-of-pocket costs, such as copayments, deductibles, and coinsurance. You should also consider contributions to accounts such as health savings accounts (HSAs), flexible spending arrangements (FSAs) or health reimbursement accounts (HRAs) that help you pay out-of-pocket expenses.