endoscopic third ventriculostomy: indications, surgical...
TRANSCRIPT
TI/rkish Nc"rosl/rgery 12: 65 - 73, 2U02 (ataltcpc: EI/doscopic Third VClllriw/n,;t"11l.11
Endoscopic Third Ventriculostomy:Indications, Surgical Technique, And Potential Problems
EndoskopikEndikasyon, Cerrahi
U~iinciiTeknik
Ventrikiilostomi:ve Potansiyel Problemler
Ocuz C::AT AL TEPE
Hacettepe University School of Medicine, Department of Neurosurgery, Ankara - Ti.irkiye
Abstract: Endoscopic third ventriculostomy is becomingmore popular as an alternative to shunting in themanagement of obstructive-type hydrocephalus. The goalof this procedure is to fenestrate the floor of the thirdventricle between the mamillary bodies and theinfundibular recess, and thus establish flow of
cerebrospinal fluid between the ventricles and the basalsubarachnoid spaces. Obstructive hydrocephalus is themain indication for endoscopic third ventriculostomy, butthis procedure is also currently used to treat a "vide rangeof hydrocephalic patients. In this surgical technique,various anatomic variations and technical difficulties can
lead to complications. However, in cases where thisprocedure is indicated, good knowledge of third ventricleanatomy and experience with endoscopic surgery can yieldsuccess rates of up to 80%.
Key ,"Vords: Hydrocephalus, neuroendoscopy, thirdventricle, ventriculostomy
INTRODUCTION
The past decade has witnessed a resurgence ofendoscopic third ventriculostomy in neurosurgery.Dandy was the first to do a third ventriculostomy in apatient in 1922 and a year later, in 1923, Mixter carriedout the first endoscopic procedure in neurosurgeryusing a small ureteroscope and performing a thirdventriculostomy procedure endoscopically (5,11). Tn
Ozet: Endoskopik U<;uncti Ventriklilostomi obstri.iktif tiphidrosefali tedavisinde son ytllarda giderek artan birilgiyle ~anta alternatif olarak kulla111lmaktadlr.Endoskopik u<;uncii ventrikiilostomide ama<; u<;unci.iventrikiil tabamnda mamiller cisimcikler ve infundibtiler
reses arasmda bir fenestrasyon olu ·turmak ve ventrikliJersistem ile basal subaraknoid ara!lklar arasll1da serbest BOS
dolal1lm ve emilimini saglamaktlr. Esas olarak obstrtiktiftip hidrosefali vakalannda endike ise de gtini.imtizde dahageni~ bir hasta grubunda kullamlmaktadJr. Bu cerrahiteknikte bazl anatomik varyasyonlar ve potansiyel teknikgti<;li.ikler komplikasyonlara neden olabilmektcdir.BununJa beraber dogru endikasyon, konan vakali1rdayeterli ventriklil i<;ianatomi bilgisi ve endoskopik cerra hitecri.ibesi ile %80 oranlannda ba~cm elde edilebilmektedir.
Anahtar Kelimeler: Hidrosefali. ti<;unci.i ventriki.il,noroendoskopi, ventriklilostomi,
the pre-shunt era, this procedure was one of the mostfrequently performed surgical procedures in themanagement of hydrocephalus. However, due to highcomplication and mortality rates, the procedure wasgradually abandoned and replaced with a new surgicaltechnique, shunting. Technical problems such asinsufficient illumination, poor lenses, and the fact thatscopes were not equipped with cameras ,,-ere at leastpartially responsible for the poor outcomes in that time.
65
Tllrki"h NCllrosllrgery 12: 65 - 73, 2002
These issues were some of the main reasons the
procedure was set aside. Decades after this methodwas initially used, Guiot (1963) and Vries (1978) reintroduced the procedure to neurosurgery bypublishing their endoscopic third ventriculostomy(ETV) series with zero mortality and low complicationrates (4,6,17). In addition to these encouraging results,technological innovations and advancements in thisfield, such as more powerful light sources andillumination, and miniature-size video cameras and
optic systems, helped to produce thinner and smallerendoscopes. High rates of shunt-related complicationsand clinical problems in hydrocephalus patients alsoprompted new searches for ways to better managehydrocephalus. As a result, ETV re-gained popularityin neurosurgery, with a large number of series showingpromising results in the 1990s.
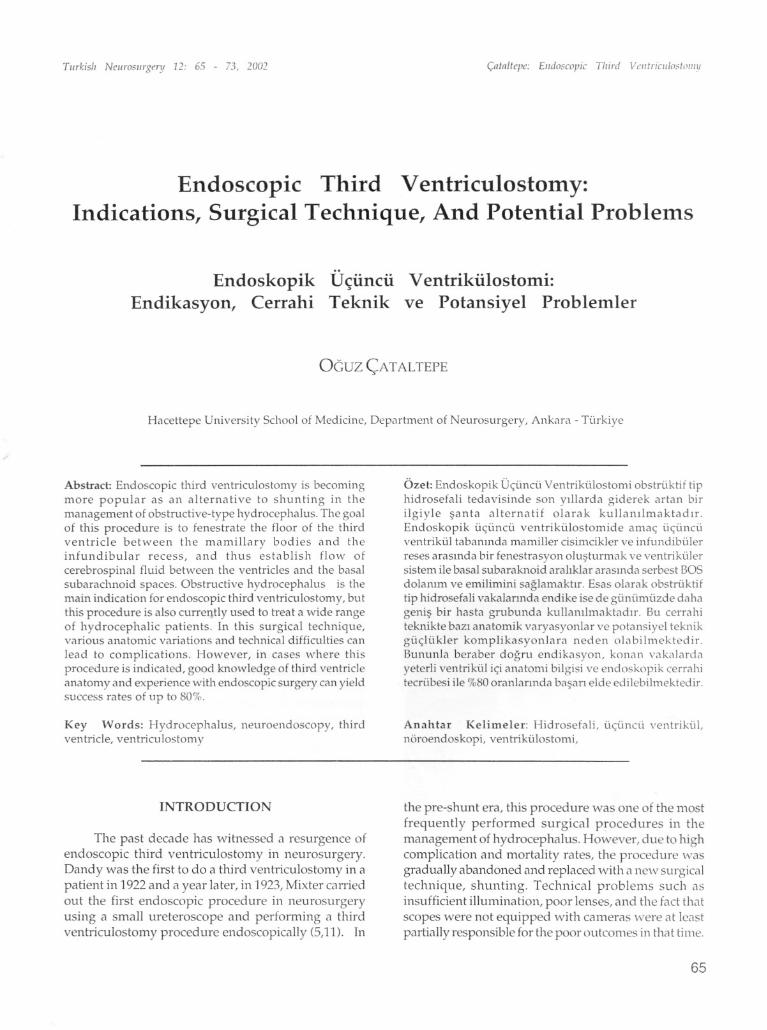
The goal of ETV is to provide free flow ofcerebrospinal fluid (CSF) between the ventricularsystem and the basal cisterns. This is done byfenestrating the floor of the third ventricle between themamillary bodies and the infundibular recess (Figure1). When this is done, the CSF in the ventricular systemcirculates through the prepontine cistern, reaches thecortical subarachnoid space, and is absorbed by thearachnoid villi. Compared the shunt placement, ETVoffers a more natural physiological solution tohydrocephalus. It is associated with lower complication
Fig. I: Preopera ti ve MRI scan of a pa tien t showsdownward bulging of the third ventricular floorand the appropriate point for renestration at thefloor (arrowhead). Notice the bowing of the thinnedcorpus callosum (arrow).
66
(alnllepe: Elldoscopic Third VClltriCIII""lolHll
rates, avoids implantation of foreign material, andeliminates shunt-related complications such as oyerdrainage. As a result of these benefits, ETV is no\\"accepted as a mainstay treatment modality forobstructive hydrocephalus.
ENDOSCOPIC SYSTEMS ANDINSTRUMENT AnON
Endoscopic surgical systems have undergonerevolutionary changes in the last two decades, thanksto technological advancements such as rod lenssystems, fiber optic technology, and better illuminationwith powerful light sources and high resolution.Neuroendoscopic systems can be divided into twomain categories: rigid and flexible endoscopes. Thesehave different indications for use, and each has its own
advantages and disadvantages. In rigid endoscopes,the view angles vary from 0 to120 degrees. Those with0-30 degree view angles provide appropriate opticaland anatomical orientation for straightforward cases.The outer diameters of rigid endoscopes are usually3.8-6.2 mm, but may be larger or smaller dependingon the endoscope used. The main advantages of rigidendoscopes over flexible endoscopes are better imagequality, wider and multiple working channels, stability,and adaptability to stereotactic frames. Thedisadvantages of these instruments are larger diameterand limited maneuverability. Flexible endoscopes arethinner and less traumatic than rigid endoscopes. Theirouter diameter is 2.3·4.6 mm, and their main advantageis superior maneuverability. The main disadvantagesof these scopes are narrower working channels andpoor image quality.
The neuroendoscopic armamentarium hasexpanded continuously during the last decade. Themost widely used and specially designedneuroendoscopic instruments are probe-perforators,Fogarty catheters, biopsy and grasping forceps,scissors, mono- and bipolar cauteries, suction tips, andlaser wires (4,6). Although there are many speciallydesigned neuroendoscopic tools, most straightforwardETV procedures can be performed with a few basicinstruments.
INDICA nONS FOR ENDOSCOPICTHIRD VENTRICULOSTOMY
The classic indication for ETV is non
communicating hydrocephalus, in which the patienttypically presents with dilated lateral and thirdventricles, and a normal fourth ventricle. However,
today there is a much wider spectrum of indications

Turkish Neurosurgery 12: 65 - 73, 2002
for this procedure, including normal-pressurehydrocephalus. Some of the main reasons for thisextensive range are increased capability ofneuroendoscopic systems due to major improvementsin the field; improved expertise of surgeons; increasednumbers of reports with favorable long-term results;and increased numbers of shunt-related problems withhigh social and personal costs. Today, the indicationsfor ETV are somewhat subjective. Some surgeonsprefer to use this method even if the success rate ofETV in that specific patient group is only 20-30%. Therationale behind this is offering the patient a chance atshunt-free life. I agree with other authors who havestated that the indications for ETV should be divided
into two groups (Table 1) (17). However there is stillsignificant disagreement on this subject. Althoughthere is consensus on good outcome after ETV inpatients with late-onset hydrocephalus, there is seriousdebate about other indications, such as ETV in
newborns, or patients with myelomeningocele. Someauthors believe that the ETV? success rate is low for
patients who have previously had shunts because theirsubarachnoid spaces are presumed to be obliterated.In contrast, other researchers have reported goodsuccess in these cases, and are convinced that this
patient group should be managed by shunt removaland ETV (11,17). The patient group withmyelomeningocele and hydrocephalus is alsocontroversial. Most authors have reported pooroutcome after ETV in these individuals, and haveattributed this result to obliterated and abnormal CSF
pathways, deformed ventricular anatomy, and athickened and obstructive massa intermedia. On the
other hand, Sayers and Natelson reported relatively
Table 1: Indications for endoscopic thirdventriculostomy.
Strong Indications:Delayed-onset aqueduct stenosisCongenital aqueduct stenosisObstructive hydrocephalus caused by pineal andposterior fossa tumorsObstruction of the foramina Magendi and LuschkaShunt malfunction in a patient with obstructivehydrocephalusShunt malfunction in older patients with spinabifida
Weaker Indications:
Neonates with aqueduct stenosisMyelomeningoceleCommunica ting hydrocephalusNormal-pressure hydrocephalus
(:ataltepe: EI/doscopic Third VelltriCll/o,;toIllY
high success rate in this patient group, and claimedthat these individuals have sufficient CSF flmv in the
cortical subarachnoid spaces (1).
The importance of the age at the time of ETV hasalso been widely discussed. Some researchers havereported poorresults in newborn and infants, and haveemphasized the negative effect of young age onoutcome, whereas others disagree with thisexplanation 00,13,16). Cinalli et al. reported nodifference in results between children younger than 6months old and an older pediatric age group, andconcluded that the age of a child is not acontraindication for ETV procedure(5).
The main contraindications for ETV are historyof radiotherapy, significantly distorted ventricularanatomy, abnormally narrow prepontine space due totumor or vascular lesion, ectatic basilar artery, vascularlesions on the floor of the third ventricle, prematurity,intraventricular hemorrhage, and infection involvingthe ventricles/meninges.
PREOPERATIVE EVALUATION
Appropriate patient selection criteria andappropriate indications are prerequisites for goodsurgical outcome with ETV. Careful assessment withpreoperative magnetic resonance (MR) imaging iscritical in order to avoid complications during surgeryand achieve a good outcome. The anatomical detailsof related structures must be carefully evaluated,including the size of the lateral ventricles, thirdventricle, and foramen of Monro; the anatomy andlocation of the basilar artery and its reli1tionship withthe floor of the third ventricle; the wid th of the
prepontine space; and the aqueductal anatomy. Also,a preoperative MR flow study should be obtained as abaseline (20). The surgeon should take all these featuresinto account before deciding to perform ETV andestimating the potential for success with this procedure.Drake described some clinical and radiographicfeatures that favor good outcome with ETV and maybe useful for predicting outcome (Table II) (7).
SURGICAL TECHNIQUE
The patient is placed in supine position and thehead is elevated to 20-30 degrees with slight flexion ofthe neck. This is done to prevent postoperativepneumocephalus and reduce the risk of subduralhematoma. An incision is made in the scalp and a burrhole is drilled on or just in front of the coronal sutureon the mid-pupillary line. The optimal entry point for
67

Turkish Neurosurgery 12: 65 - 73, 2002
Table 2: Favorable clinical and radiographicalfeatures for ETV (7)
Clinical Features:Cause of hydrocephalus in high or intermediatesuccess group (see above)Age>6 months at time of hydrocephalus diagnosisAge>6 months at time of procedureNo prior radiotherapyNo history of hemorrhage or meningitisPatients previously shunted
Radiographic Features:Clear evidence of ventricular non-communication
Obstructive pattern of hydrocephalusAqueductal anatomic obstructionLack of aqueductal flow void on T2 MRI
Favorable Ventricular Anatomy:Width of foramen of Monro sufficient to
accomodate endoscopeRigid >7mmFlexible> 4mm
Thinned floor of third ventricleDownward bulging floor, draped over clivusBasilar artery posterior to mamillary bodies
Absence of structural abnormalities
AVM or tumor obscuring floor of third ventricleEnlarged massa intermediaInsufficient space between mamillary bodies,basilar artery, and clivusBasilar artery ectasia
ETVwas found as 8 mm anterior to the coronal suture
and 28 mm lateral to the midline in a study(12). Aftera burr-hole of approximately 1cm diameter is created,the dura is opened in cruciate fashion and a peel-awaycannula (12F) or rigid sheath (7 111m),depending onthe endoscopic system used, is introduced into thefrontal horn of the lateral ventricle. The endoscope isthen passed through the cannula into the frontal horn(see accompanying CD). The foramen of Monro islocated by following the choroid plexus, anterior septal,and thalamostriate veins, and the endoscope is passedthrough this opening and placed into the thirdventricle. In normal subjects, the mean sagittal diameterof the foramen of Monro is 2.9 mm and the vertical
diameter is 5.1 mm (19). This foramen is usuallyconsiderably enlarged in hydrocephalic patients, andthe endoscope can usually pass through easily withoutinjuring the fornix. Once the endoscope is in the thirdventricle, the infundibular recess, tuber cinereum,mamillary bodies, massa intermedia, aqueduct, andposterior commissure can be observed from anteriorto posterior. The optic recess, lamina terminalis, and
68
C;:ntn/tepe: Elldoscopic TI/ird ",,"friel/h'_-lilll/ll
suprapineal recess can be seen if the instrument is awide angled rigid or flexible endoscope.
Success with ETV is closely related to thesurgeon's knowledge of third ventricle anatomy, as theventricular system can be navigated and ,vorked onthrough the use of anatomical landmarks. Themamillary bodies are bright white-yellow roundedstructures in the floor of the third ventricle, and can beseen just after the scope enters this cavity. If theendoscope is maneuvered anteriorly and superiorlyupon entry, the small pink-red infundibular recess(color due to vascularity of the hypothalamic portalsystem) can be observed. The tuber cinereum is atriangular and often transparent area between themamillary bodies and the infundibular recess, and itincludes the arcuate nucleus of the hypo thaIalTIUS.Inhydrocephalic patients, the tuber cinereum is usuallyvery thin and translucent, and the dorsum sella, clivus,and basilar artery can easily be seen be'1eath it.Fenestration is performed at the tuber cinereum at themidway between the infundibular recess and theintermamillary point. Ideally, the site of fenestrationshould be away from the basillary tip. onnally, themean distance between the infundibular recess andmamillary bodies is 6 mm (range,3.5-9mm). The meandistance between the basillary artery and theinfundibular recess in the normal setting is 10.5±2.3mm, whereas the corresponding distance inhydrocephalus patients is 12±3.7 mm (9). If theventricle floor is translucent, the basilar artery may beseen and fenestration is performed distant from it. It isalso critical to fenestrate at the above-mentioned mid
point, because more lateral fenestration may cause athird nerve injury.
Fenestration of the floor of the third ventricle maybe performed using a blunt probe, Fogarty catheter,the endoscope itself, special scissors, a coagubtor, or anumber of other instruments, depending on thesurgeon's preference. We use an angled blunt probedesigned for this purpose (see CD, Cases 1-3), andangle the tip of the probe toward the dorsum sella soas not to injure the basilar artery during fenestration.As mentioned above, the floor of the ventricle is usuallyquite thin in patients with hydrocephalus, and can beeasily punctured with a blunt probe. However, in somecases it may be relatively thick, and the surgeon mayprefer to use coagulation or sharp fenestrationtechniques in these cases (see CD, Cases 2 and 4).However, I do not recommend using coagulation tofenestrate the floor, as this may damage vascul(lrstructures below and m(lYc(luse therm(l] injury to thehypothalamus.

Tlirkisiz Nwroslirgery 12: 65 - 73, 2002
After the floor of the third ventricle is punctured, .the fenestrated site is enlarged using a 3F Fogartycatheter. The catheter is passed through the puncturehole, its balloon is inflated, and the catheter is then
withdrawn to enlarge the hole. Using this method, afenestration of 5-6 mm diameter is created. It is
important to remember that the Fogarty catheter mayinjure vascular structures and the third cranial nervebelow, and should not be advanced into the prepontinespace too much. The proximal end of the balloon.should be visible to the surgeon. Once this enlargedpassageway is formed, the endoscope is inserted intothe prepontine space to explore the basilar artery andits tributaries, the pons, the dorsum, and the clivus. Itis not uncommon to observe a second membrane, often
connected to the Lilliquest membrane, in theprepontine space. The main purpose of this explorationis to ensure there is no other membrane obstructingfree CSF flow in the prepontine space. If there is suchan obstructing membrane, it must also be fenestratedwith a blunt probe and enlarged with a Fogartycatheter, as described above (see CD, Case 9). After
the prepontine space has been explored, the endoscopeis withdrawn into the third ventricle and the examiner
will observe pulsations of the floor along with"flapping" of the edges of the newly created openingas CSF flows through indicating a patentventriculostomy (see CD).
It is not unusual to observe some bleeding duringfenestration, especially if the floor is thick and vascular.However, this is easily stopped by irrigating the fieldwith Ringer's lactate for awhile. Another way to stophemorrhage from the edges of the new opening is toinflate the Fogarty balloon just at the level of theopening so that it compresses the edges. The inflatedballoon should be kept in place for 15-30 seconds. Whenthe procedure is complete, the endoscope is withdrawnslowly, exploring the third and lateral ventricles toensure there is no acti ve bleeding. A piece of Gelfoam®is placed in the burr-hole and the scalp is closed instandard fashion. Some surgeons leave a ventriculardrain in place after ETV. The purpose of this is tomeasure intracranial pressure (ICP) and be able todrain CSF if necessary. At our center, we do not placea ventricular drain if there are no peroperativeproblems.
Another endoscopic procedure that can beperformed alone or in addition to ETV isaqueductoplasty (see CD, Cases 10 and 11). Ifaqueductoplasty is planned, the burr-hole should beplaced 2-3 cm in front of the coronal suture. Theendoscope is inserted into the third ventricle as
C;:l1tnltepe: Elldoscopic Third \lclltriCII/o,toIiZY
described above, but is directed posteriorly, in contrastto what is done in ETV. The massa intermedi<l is often
thin in hydrocephalic patients due to increased dist<lncebetween the thalam.i. The endoscope is advanced aboveor below the massa intermedia, depending on thepatient's anatomy. The posterior commissure, pinealrecess, and aqueduct are explored. If there isaqueductal stenosis, the aqueduct appears like a "fishmouth." If there is an aqueductal web or bands, thesemembranes can be perforated with scissors or a Fogartycatheter. In case of aquedlldal stenosis, a Fogartycatheter is introduced into the aqueduct without <lnyforce. The balloon is inflated slightly and kept inflatedfor 10-15 seconds. Thereafter, the balloon is detlated,the catheter is advanced further, and the balloon is re
inflated and held in position again for 10-15 seconds.These steps are repeated until the Fogarty can beadvanced into the fourth ventricle with no resistance.
It is very important not to force the catheter if there issignificant resistance in the aqueduct. If this is the case,the procedure should be abandoned rather than injurethe periaqueductal structures with the catheter. If thepatient has long-segment stenosis and the surgeon isconcerned about the long-term patency of this passage,an aqueductal stent may also be considered.
POTENTIAL PROBLEMS
Although ETV is a straightforward procedure,there are a number of potential problems. Most of theserelate to variations in third ventricle anatomy (]5,19).Thick and opaque third ventricular floor is one of themost frequently encountered variations, with anapproximate frequency of 16% (18) (see CD, Cases 2<lnd 4). Another significant detail in preoperative MRIassessment is the the distance between the pons andclivus in prepontine space. If this distance is smallerthan 4 mm, a fully inflated 3F Fogarty catheter balloonmay compress the basilar artery and pons. In thesecases the procedure the fogarty should be inflated lessthan usual (see CD, Case 5).
Other anatomic variations relate to the natureof the ventricle floor. The floor of the third ventricle
may be steep because the upper level of the dorsumand infundibular recess are elevated compared tothe mamillary bodies. Puncturing a steep ventriclefloor can be very difficult (see CD, Case 6). It can<llso be challenging to puncture a floor that isunusually resistant. If the floor is stretchedexcessively during puncturing attempts,postoperative diabetes insipidus and fever relatedto hypothalamic injury may develop. In addition, itmay not be possible to visualize the basilar artery
69

Turkish Neurosurgery 12: 65 - 73, 2002
and dorsum if the floor is thick and opaque, and thisincreases the risk of vascular injury during puncturing.Basilar artery injury is most serious potentialcomplication of ETV, and this can be lethal. The locationof the basilar artery should be clearly established bothpre- and peroperatively, fenestration should beperformed anterior to this vessel, and cautery shouldnot be used to perforate the floor.
Hypervascular ventricular floor is anotherpotential problem in ETV, and may cause significantbleeding during fenestration (see CD, Case 7).Although it is not common, spontaneous fenestrationof the floor of the third ventricle may also be seen. Thesefenestrations are usually small and partial; thus,standard fenestration with a 3F Fogarty catheter shouldbe created even if the surgeon notes spontaneousfenestrations in the floor during the procedure (see CD,Case 8).
Another potential problem during ETV is upwardbulging of the ventricle floor. The floor can herniateupward and obliterate the third ventricle, making itvery challenging to find the fenestration hole again andcontinue the procedure (1). Dilation of the infundibularrecess may also cause problems during surgery. Theanterior third ventricle may herniate into the sella inthese cases, and fenestration may unintentionally createan opening into the sella.
As stressed above, careful preoperative MRIassessment is important to avoid unwanted problems.Knowing the basilar artery anatomy and location arealso very significant factors for planning andperforming successful ETV. Missing an ectatic oranteriorly placed basilar artery during preoperativeMRI evaluation can lead to catastrophe. It should benoted that the basilar artery may be found moreanterior to the mamillary bodies than normal in up to12.9% of patients, especially in older individuals(Figure 2) (9).
Finally, in some cases, the ventricle anatomy maybe completely disrupted with almost all anatomicallandmarks absent (8). These cases are especiallychallenging, and the surgeon's experience is mostimportant determinant of successful outcome (see CD,Case 9).
POSTOPERATIVE EVALUATION
Ventricle size often does not change after ETV.Reports state that only 16-33% of patients have smallerventricles after this procedure (3,14). Although
70
Fig. II: MRI scan of an older hydrocephalic p<ltient showsanteriorly and upwardly displaced basibr <Irtery(arrowhead). Notice the tenting effect of basibrytip on the third ventricular floor.
observations of flapping of the edges of the fenestrationsite during the procedure implies patency of theventriculostomy and free CSF flow, this sign alone notvery reliable. Findings indicating clinical improvementare considered more valuable for assessing the successor failure of ETV. Clinical findings such as resolutionof papilledema, normalization of ICP, relaxation of thefontanelles, and stable head circumference indicate a
successful procedure.
Several objective tests can also be used toevaluate success. Per- or postoperative flov" studiesperformed with radiopaque or radioisotopematerials may also be useful for assessing patencyafter ETV. Another option is to le<1ve an externalventricular drain in place <1ndmonitor normalizationof rcp postoperatively. However, it is important toremember that rcp may remain high for the first fewdays post-surgery (adaptation period), and this doesnot indicate failure. Today, MR flow studies are themost widely used and reliable postoperative testsfor assessing success of ETV. These studies providedetailed information on the subject's CSF flowdynamics. Sagittal T2-weighted turbo inversionrecovery MR images may provide informationregarding the absence or presence of flow void inthe aqueduct. However, if the aqueduct is smallerthan 1 mm diameter, there may be no signal voideven though there is some flow. Flow-sensitivecardiac-gated cine phase-phase contrast MR imagesare used for quantitative and qualitative CSF flowstudies, and this is one of the most frequently usedmethods for assessing patency in these cases (Figure3 and 4) (8,9,20).
Tllrkish Neurosurgery .12: 65 - 73, 2002
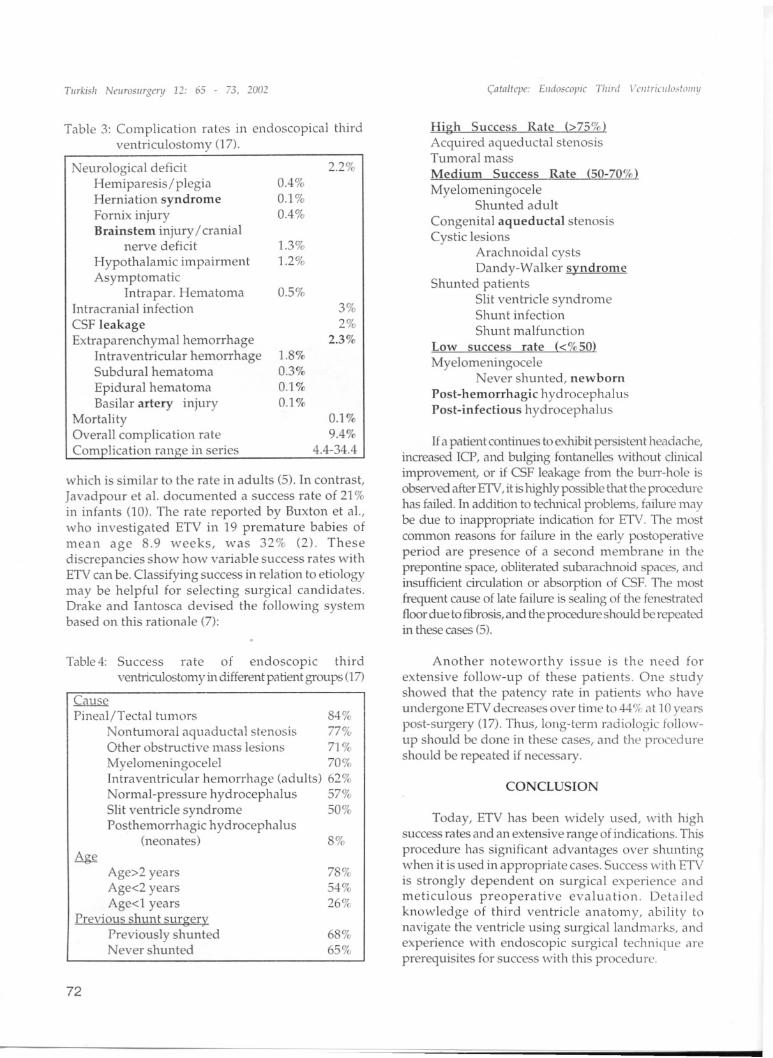
COMPLICA nONS
As noted above, the most serious complicationof ETV is basilar artery injury. Although very rare,this can lead to pseudoaneurysm or even death.Injuries that occur during floor puncture are morecommon. These include damage to thehypothalamus, pons, cerebral peduncle, and thirdcranial nerve. The most frequent surgicalcomplication in ETV is bleeding, and this usuallyoccurs due to injury of the ependymal vessels orchoroid plexus. To avoid these complications, it isvery important to remember that significantneurovascular structures may be very close to theendoscope during the procedure, even if they arenot directly in view. Table III shows approximaterates of various complications of ETV based onpublished series (17).
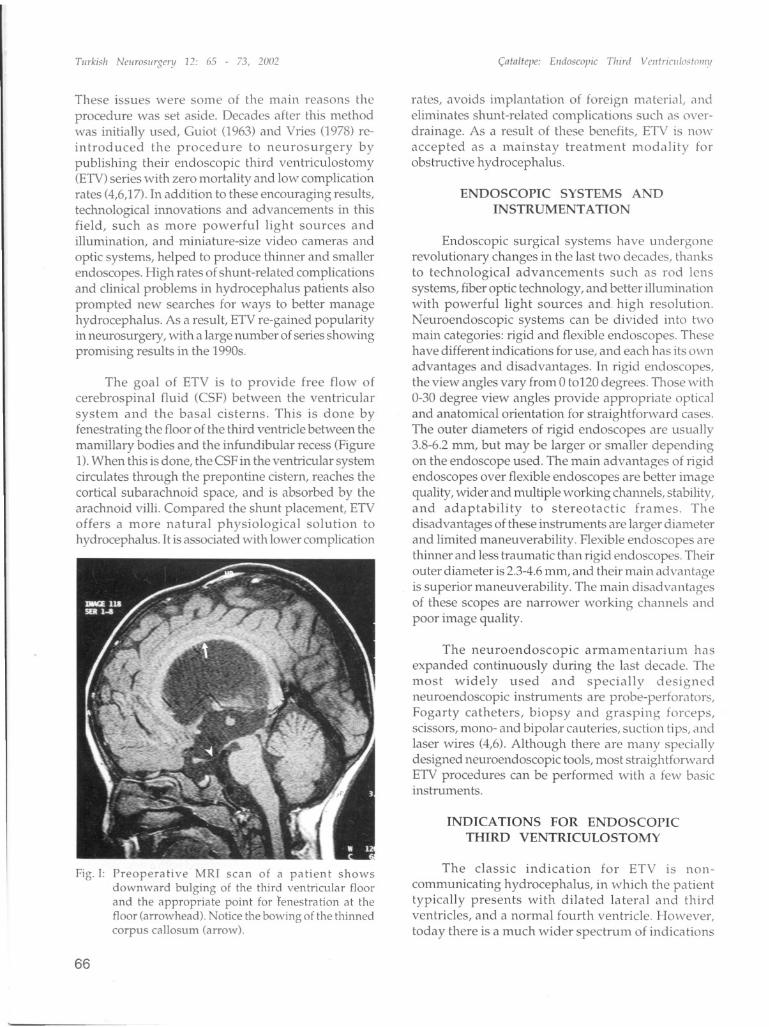
Fig. III: Early postoperative Cine PC MR image of apatient shows continuous caudal flow throughventricu!ostomi site between the third ventricle
and prepontine space which implies a patentfenestration (arrows). Notice the presence ofcaudal flow in cervical subarachnoid space as welland absence of any flow void in the aqueduct ofSylvii.
(:nln/lcpe: Elldo5COpic Third Velllriclllo"lollIll
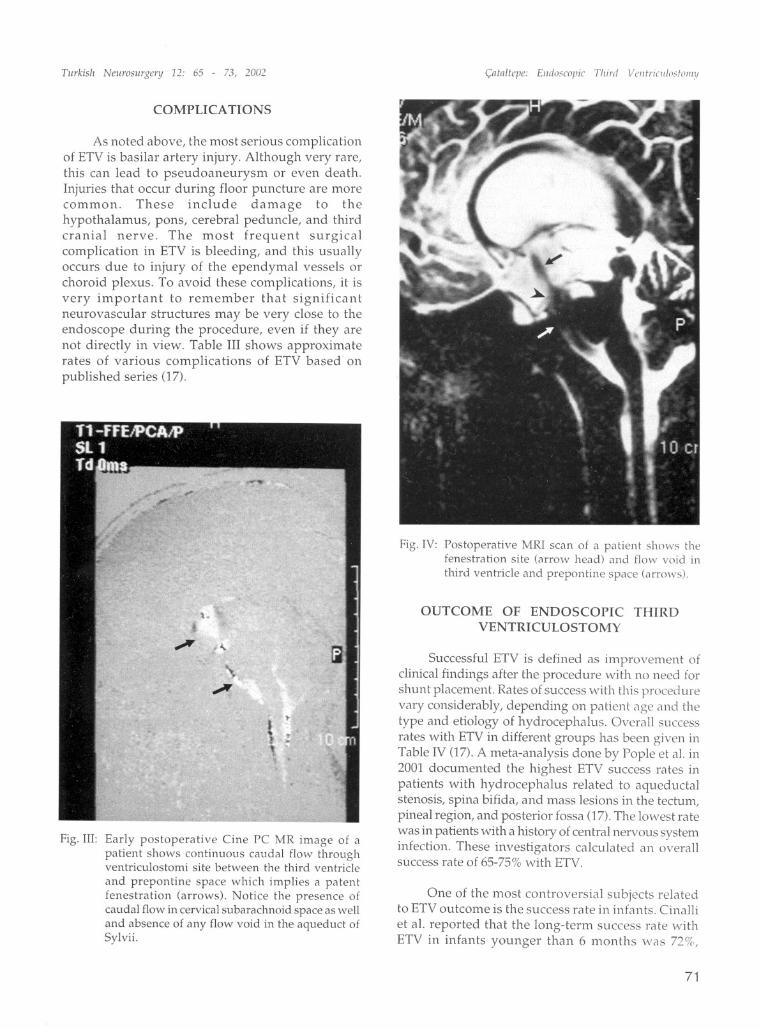
Fig. IV: Postoperative MRI scan of a patient sh()w~ thefenestration site (Clrrow head) and flow void in
third ventricle and prepontine space (arrows).
OUTCOME OF ENDOSCOPIC THIRDVENTRICULOSTOMY
Successful ETV is defined as improvement ofclinical findings after the procedure with no need forshunt placement. Rates of success with this procedurevary considerably, depending on patient age and thetype and etiology of hydrocephalus. Overall successrates with ETV in different groups has been given inTable IV (17). A meta-analysis done by Pople et al. in2001 documented the highest ETV success rates inpatients with hydrocephalus related to aqueductalstenosis, spina bifida, and mass lesions in the tectum,pineal region, and posterior fossa (17).The lowest ratewas in patients with a history of central nervous systeminfection. These investigators calculated an overallsuccess rate of 65-75%with ETV.
One of the most controversial subjects relatedto ETV outcome is the success rate in infants. Cinalliet al. reported that the long-term. success rate v,rithETV in infants younger than 6 months was 72%,
71
TlIrkish NellroslIrgery 12: 65 - 73, 1001 (:ntnltepe: EJI(ioscopic Third VCl/lricl/lo,tolll.'l
which is similar to the rate in adults (5). In contrast,
Javadpour et al. documented a success rate of 21%in infants (0). The rate reported by Buxton et al.,who investigated ETV in 19 premature babies ofmean age 8.9 weeks, was 32% (2). Thesediscrepancies show how variable success rates withETV can be. Classifying success in relation to etiologymay be helpful for selecting surgical candidates.Drake and Iantosca devised the following systembased on this rationale (7):
High Success Rate (>75%)Acquired aqueductal stenosisTumoral mass
Medium Success Rate (50-70%)
MyelomeningoceleShunted adult
Congenital aqueductal stenosisCystic lesions
Arachnoidal cystsDandy-Walker syndrome
Shunted patientsSlit ventricle syndromeShunt infectionShunt malfunction
Low success rate «%50)
MyelomeningoceleNever shunted, newborn
Post-hemorrhagic hydrocephalusPost-infectious hydrocephalus
. If a patient continues to exhibit persistent headache,mcreased ICP, and bulging fontanelles without clinicalimprovement, or if CSF leakage from the burr-hole isobserved after ETV, it is highly possible that the procedure
has failed. ~n addition to teclmical problems, failure maybe due to mappropriate indication for ETV. The most
col1;mon reasons for failure in the early postoperativepenod are presence of a second membrane in theprepontine space, obliterated subaraclmoid spaces, andinsufficient circulation or absorption of CSF. The mostfrequent cause of late failure is sealing of the fenestratedfloor due to fibrosis, and the procedure should be repeatedin these cases (5).
third
3%
2%2.3%
2.2%
0.1%9.4%
4.4-34.4
0.5%
1.8%0.3%0.1%0.1%
0.40/.
0.1%0.4%
1.3%1.2%
Table 3: Complication rates in endoscopicalventriculostomy (17).
Neurological deficitHemiparesis / plegiaHerniation syndromeFornix injuryBrainstem injury / cranial
nerve deficit
Hypothalamic impairmentAsymptomatic
Intrapar. HematomaIntracranial infection
CSF leakageExtraparenchymal hemorrhage
Intraventricular hemorrhageSubdural hematoma
Epidural hematomaBasilar artery injury
MortalityOverall complication rateCom lication ran e in series
Table 4: Success rate of endoscopic thirdventriculostomy in different patient groups (17)
Cause
Pineal/Tectal tumors 84%
Nontumoral aquaductal stenosis 77%Other obstructive mass lesions 71 %
Myelomeningocelel 70%Intraventricular hemorrhage (adults) 62%Normal-pressure hydrocephalus 57%Slit ventricle syndrome 50%Posthemorrhagic hydrocephalus
(neonates) 8%
Age>2 yearsAge<2 yearsAge<l years
Previous shunt surgeryPreviously shuntedNever shunted
78%54%
26%
68%65%
Another noteworthy issue is the need forextensive follow-up of these patients. One studyshowed that the patency rate in patients who haveundergone ETV decr~ases over time tC)44% ilt 10 yearspost-surgery (17). Thus, long-term radiolo<'ic follow-"up should be done in these cases, and the procedureshould be repeated if necessary.
CONCLUSION
Today, ETV has been widely used, with highsuccess rates and an extensive range of indications. This
proce~~re has significant advantages over shuntingwhen It ISused in appropriate cases. Success with ETV
is strongly dependent on surgical experience andmetIculous preoperative evaluation. Detailed
knowledge of third ventricle anatomy, ability tonavIgate the ventricle using surgical landmarks, and
experienc.e with endoscopic surgical technique areprereqUIsItes for success with this procedure.
72

Turkish Neurosurgery 12: 65 - 73, 2002
Note:The CD that accompanies this article shows some
ETV procedures that we performed at HacettepeUniversity Hospitals. The references made to the CDin the text identify actual images of the surgicaltechniques and anatomical details that are mentioned.
Correspondence: Oguz ~ataltepeHacettepe Tip Fakultesi HastanesiNbro§irurji Anabilim DahAltmdag, 06100Ankara, TurkiyePhone: (90) 312 3051715Fax: (90) 312311 1131E-mail: [email protected]
REFERENCES
1. Aalst JV, Beuls EA, Van Nie F, Vies JSH, Cornips EMJ:Acute distortion of the anatomy of the third ventricleduring third ventriculostomy. J Neurosurg 96;597-599,2002
2. Buxton N, MacArthur D, Malucci C, Punt J,Vloeberghs M: Neuroendoscopy in the prematurepopulation. Child's Nerv Syst 14;649-652, 1998
3. Buxton N, Turner B,Ramli N, Vloeberghs M: Changesin third ventricular size with neuroendoscopic thirdventriculostomy: A blinded study. J NeurolNeurosurg Psychiatry. 72;385-387,2002
4. Caemaert J: Endoscopic Neurosurgery, in SchmidekHH (ed), Operative Neurosurgical Techniques, fourthedition, Philadelphia: WB Saunders, 2000:535-570
5. Cinalli G, Sainte-Rose C, Chumas P, Zerah M, BrunelleF, Lot G, Pierre-Kahn A, Renier D: Failure of thirdventriculostomy in the treatment of aqueductalstenosis in children. J Neurosurg 90;448-454, 1999
6. Cohen AR, Perneczky A: Endoscopy and themanagement of third ventricular lesions, in ApuzzoMLJ (ed), Surgery of the Third Ventricle, secondedition, Baltimore: Williams and Wilkins, ']998:889936
7. Drake JM, Iantosca MR: Current systems forcerebrospinal fluid shunting and management ofpediatric hydrocephalus: endoscopic and imageguided surgery in hydrocephalus, in Schmidek HH(ed), Operative Neurosurgical Techniques, 41h edition,Philadelphia: WB Saunders, 2000:573-594
8. Fukuhara T, Vorster SJ, RuggieriP, LucianoMG: Third
(a ta It"!,,,: Elld,'scopic Tlli"t \ '''lItrilll/ostOIllY
ventriculostomy patency: comparison of findings at cinephase-contrast MRI and at direct exploration. AJNR20;1560-1566, 1999
9. Hayashi N, Endo S, Hamada H, Shibata T, Fukuda 0,Takaku A: role of preoperative midsagittal MRI inendoscopic third ventriculostomy. Minim InvasNeurosurg 42;79-82, 1999
10. Javadpour M, Malucci C, Brodbelt A, Golash A, May P:The impact of endoscopic third ventriculostonw on' themanagement of newly diagnosed hydrocepl~alus ininfants. Pediatr Neurosurg 35;131-135,2001
11. Jones RFC, Stening WA, Brydon M, Paed M: Endoscopicthird ventriculostomy. Neurosurgery 26;86-92, 1990
12. Kanner A, Hopf NJ, Grunert P: The 'optimal' burr holeposition for endoscopic third ventriculostomy: Resultsfrom 31stereotactically guided procedures. Minim InvasNeurosurg 43;187-189,2000
13. Kim SK, Wang KC, Cho BK: Surgical Outcome ofpediatric hydrocephalus treated by endoscopic thirdventriculostomy: prognostic factors and interpretationof postoperative neuroimaging. Child's Nerv Syst16;161-169,2000
14. Kulkarni AV, Drake JM, Armstrong DC, Dirks PB.Imaging correlates of successful endoscopic thirdventriculostomy. J Neurosurg 92;915-919, 2000
15. Morota N, Watabe T, Inukai T, Hongo K, Nakagawa H:Anatomical variants in the floor of the thrd ventricle:
Implications for endoscopic third ventriculostomy. JNeurol Neurosurg Psychiatry 69;531-534, 2000
16. Oka K, Yamamoto M, Ikeda K, Tomonaga M: Flexibleendoneurosurgical therapy for aqueductal stenosis.Neurosurgery 33;236-243, 1993
17. Pople IK, Edwards RJ,Aquilina K: Endoscopic methodsof hydrocephalus treatment. Neurosurg Clin NorthAmer 36;719-735,2001
18. Riegel T, Alberti 0, Hellwig D, Bertalanffy H: Oper<itivemanagement of third ventriculostomy in cases ofthickened, non-translucent third ventricular floor:Technical note. Minim Invas NeuTOsurg 44:65-09,2001
19. Rohde V, Gilsbach JM: Anomalies and variants of theendoscopic anatomy for third ventriculostomy. Minim[nvas NeliTOsurg 43;111-117,2000
20. Schroeder HWS, Schweim C, Schweim KH, Gaab l\1R:Analysis of aqueductal CSF flow after endoscopicaqlleductoplasty by using cine phase-contrast MRI. JNeurosurg 93;237-244,2000
21. Schwartz TH, Ho B,Prestigiacomo q,Bruce IN, FeldseinNA, Goodman RR: Ventricular volume following thirdventriculostomy. J Neurosurg 91:20-25,1999
73