endocrine testing protocols
DESCRIPTION
protocol doing endocrine testsTRANSCRIPT

Cushings:
Screening: 2/3 screening test positiveConfirmatory testingLocalisation testing
Screening tests:
24 Hour Urine Collection: two samples measuring urine free cortisollevels > 2x Upper limit of normal considered positiveconfounders (Obesity, Depression, Anorexia may increase levels slightly)
•
Diurnal rhythm: either salivary or serum cortisol level:midnight cortisol <50nmol/l (high sensitivity) but recent studies suggest cut off of <207nmol/l better specificity Salivary cortisol levels (<4nmol/l) considered normal
•
Low dose 1mg overnight dexamethasone suppression test:1mg Betamethasone given orally between 23:00 and 0:00 with serum 8:00am cortisol measuredsuppression below 50nmol/l considered normalfalse positives related to increased dexamethasone metabolism e.g. phenytoin, phenobarb, rifampicin), renal failure and depression
•
CONFOUNDERS: See table 3
Confirmatory tests:
Formal low dose 2mg 48hr Dexamethasone suppression test:pt given 0.5mg betamethasone (8 doses) every 6 hours starting at 12:00. Subsequent doses given every 6 hours (18:00, 0:00, 6:00, 12:00, 18:00, 0:00, 6:00) and serum cortisol at 8:00 taken
Suppression to <50nml/l considered normal and excludes cushings
•
Localizing tests:
Measure ACTH (EDTA tube on ice) levels <1.1pmol/l suggests ACTH independence
•
Levels >2.2pmol/l suggest ACTH dependence (note levels often much higher)
CRH Stimulation Test: very good to confrim cushings and localised itBld drawn at -15min and 0mins for ACTH and cortisol. Pt given 1µg/kg CRF iv. Blood taken at 15, 30, 60, 90, 120 mins for ACTH and Coritsol Interpretation: ACTH increase of >35% above basal in pts with Cushings disease but not in ectopic ACTH. Increase of cortisol by >20% at 30-45mins suggests cushings disease rather than ectopic secretion. (note poor discriminator of pseudocushings)
•
DEX-CRH test:improved diagnostic accuracy in confirming cushings and differential diagnosis:
•
Betamethasone 0.5mg given orally for as for 48hr dex suppression test: ==> pts with Cushings disease suppress by at least 50% (urinary cortisol / serum cortisol) whereas cushings syndrome does not (measured at 8:00) Basal ACTH and cortisol taken at -15mins and 0mins.Pt given 1µg/kg CRH ivi 2hrs (NBNB) after 8:00 cortisol and ACTH levels done at 15, 30, 60, 90, 120mins.Cortisol level > 38nmol/l at 15 mins post CRH suggests cushings disease
Inferior Petrossal Sinus Sampling:gold standard for diagnosing cushing's disease, but invasive and higher comlication rate.Catheters placed via left and right femoral veins into left and right inferior petrossal sinuses via xray screening. Peripheral large bore line placed to sample peripheral blood.Baseline samples for Prolactin (to confirm position in IPS) as well as Cortisol
•
Cushings Testing09 August 201011:38 AM
Pituitary Function Testing Page 1

Baseline samples for Prolactin (to confirm position in IPS) as well as Cortisol and ACTH obtained at -15, -10, -5 and 0 mins. CRH given ivi at dose of 1µg/kg via peripheral vein.Blood drawn for ACTH and Cortisol at 2, 5, 10 and 15 mins from all three catheters (L and R IPS and Peripheral line)
Pituitary Function Testing Page 2

Growth Hormone Suppression Test:75g oral glucose load given in 300-500ml water ingested over 5 minsBlood for Glucose and GH taken at 0, 30, 60, 90, 120, 150 mins Levels of GH > 1ng/ml confirm acromegalyMeasure Prolactin and IFG-1 at basline also
IGF -1:Single blood test, Long half life, elevated level also confirm diagnosisBut levels fluctuate and affected by renal dysfunction and hepatic dysfunction, nutrition and DM
TSH Test: TRH inhibits GH release.TRH given 200mg IVI with GH measured at 0, 20, 60minsNormal response is a fall in GH concentration but in 60% of pts with Acromegaly have paradoxical rise in GH levels.
GHRH measurement:Done if MRI of pituitary shows no tumourOften pancreatic source
Cure in Acromegaly:
Pts on Somatostatin therapy random IGF1 and GH are sufficient for assessmentDiscordant results: 30% of pts will have discordance between GH and IGF levels mostly N GH with elevated IGF1NOTE patients on Pegvisomant ==> monitor IGF1 levels only
Controlled acromegaly : suppressed GH levels during OGT and Normal IGF1 3-6/12 post neurosurgery
Acromegaly:09 August 201001:51 PM
Pituitary Function Testing Page 3
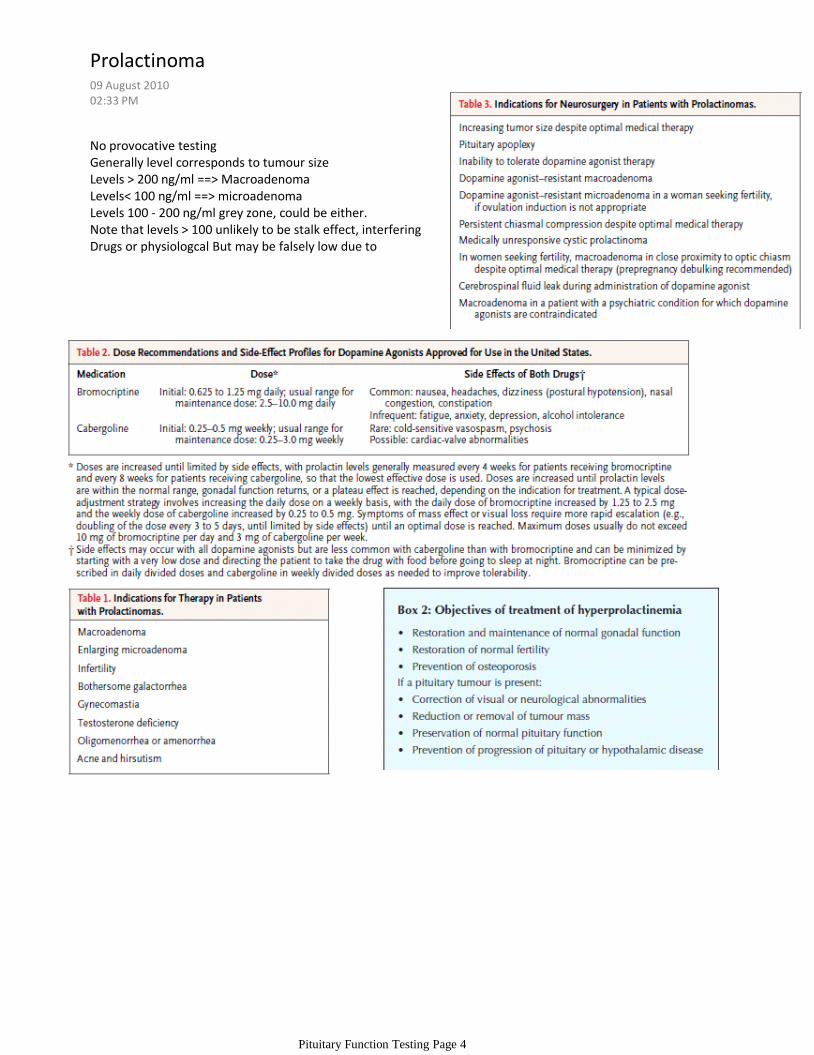
No provocative testingGenerally level corresponds to tumour sizeLevels > 200 ng/ml ==> MacroadenomaLevels< 100 ng/ml ==> microadenomaLevels 100 - 200 ng/ml grey zone, could be either.Note that levels > 100 unlikely to be stalk effect, interferingDrugs or physiologcal But may be falsely low due to
Prolactinoma09 August 201002:33 PM
Pituitary Function Testing Page 4

Pituitary Function Testing Page 5

Table 1. Guidelines for initial clinical evaluation of a
child with growth failure
Evaluation Key elements
Birth history Gestational age, birth weight and length, delivery type, birth trauma, hypoglycemia, prolonged jaundice.
Past medical
and surgical history
Head trauma, surgery, cranial radiation, CNS
infection.
Review of
systems
Appetite, eating habits, bowel movements.
Chronic
illness
Anemia, Inflammatory Bowel Disease,
cardiovascular disease, renal insufficiency, etc.
Family
history
Consanguinity, parents and siblings' heights,
family history of short stature, delayed puberty.
Physical examination
Body proportions (upper/lower segment ratios, arm span), head circumference, microphallus, dysmorphism, and midline craniofacial abnormalities.
Growth
pattern
Crossing of percentiles, failure to catch-up.
Screening
Tests
FBC, ESR, TFT's, UA, IGF1, IGFBP3, Bone age
(and a Karyotype for females)
Summary of diagnosis of GH deficiency:
height >2.25 SD below the mean for age or >2 SD
below the midparental height percentile;
1.
growth velocity <25th percentile for bone age: 2.bone age >2 SD below the mean for age; 3.low serum insulin-like growth factor 1 (IGF-1) and/or
insulin-like growth factor binding protein 3 (IGFBP3);
4.
other clinical features suggestive of GH deficiency. 5.
Children with severe GH deficiency can usually be
diagnosed easily on clinical grounds, and fail GH stimulation tests. Studies have shown that despite clinical evidence of GH deficiency, some children may pass GH
stimulation tests (11). In the case of unexplained short stature, if the child meets most of the following criteria, a trial of GH treatment should be initiated (1):
Height more than 2 SD below the mean. 1.Neonatal hypoglycemia, microphallus, prolonged
jaundice, or traumatic delivery.
2.
Although not required, a peak GH concentration after
provocative GH testing of less than 10 ng/ml.
3.
Consanguinity and/or a family member with GH
deficiency.
4.
Midline CNS defects, pituitary hypo- or aplasia,
pituitary stalk agenesis, empty sella, ectopic posterior pituitary (‘bright spot’) on MRI.
5.
Deficiency of other pituitary hormones: TSH, PRL,
LH/FSH and/or ACTH deficiency.
6.
Key elements that may indicate GH deficiency are:
Biochemical evaluation of GH deficiency:
Stimulation testing: GH provocation utilizing arginine, clonidine,
glucagon, L-Dopa, insulin, etc. This practice generally measures pituitary reserve-or GH secretory ability-rather than endogenous secretory status. Trained individuals should perform the GH
stimulation test according to a standardized protocol, with special care taken with younger children/infants.
1.
GH-dependent biochemical markers: IGF1 and IGFBP3: Values below
a cut-off less than -2 SD for IGF1 and/or IGFBP3 strongly suggest an abnormality in the GH axis if other causes of low IGF have been excluded. Age and gender appropriate reference ranges for IGF1 and
IGFBP3 are mandatory.
2.
24-hour or Overnight GH sampling: Blood sampling at frequent
intervals designed to quantify physiologic bursts of GH secretion.
3.
IGF generation test: This test is used to assess GH action and for the
confirmation of suspected GH insensitivity. GH is given for several days (3-5 days) with serum IGF-1 and IGFBP-3 levels measured at the start and end of the test. A sufficient rise in IGF-1 and IGFBP-3
levels would exclude severe forms of GH insensitivity (11, 21).
4.
As growth hormone is secreted in a pulsatile manner (usually 6 pulses in 24 hours and mainly during the night) with little serum GH at any given time, several methods have been recommended to assess the adequacy of GH secretion:
Diagnostic test for GH deficiency:
Need 2 different abnormal tests to diagnose GH deficiency as 10% of N children have abnormal response to single test•But rise of GH > 10ng/ml on any test excludes GH deficiency•
Screening test: GH level after 10 mins of vigorous exercise >10ng/ml (no guide what constitutes vigorous)•Insulin Hypoglycaemia test:•
Growth Hormone Deficiency09 August 201002:57 PM
Pituitary Function Testing Page 6
Insulin Hypoglycaemia test:overnight fast, risk of seizure, need experienced personell, normal glucose at begin of testRequirements: 10-25% dextrose infusion available, IV infusion with N/S at beginning, constant supervision, no Hx of hypoglycaemic seizuresRegular insulin 0.075 - 0.1 U/kg in saline given as bolus. In 20-40 min a 50% drop in glucose levels occur. GH and cortisol and ACTH should increase (GH > 10ng/ml)Samples for GH and cortisol glucose taken at 0, 30, 45, 60, 75 and 90 minsGlucose should fall to <2.2mmol/l and cortisol should increase to >550mmol/l
•
Arginine infusion: 0.5g/kg infused over 30 mins ==> measure GH after 30 mins•Blood collected for GH at 0, 30, 60, 90 and 120 minsOral levodopa (125mg if <20kg and 250mg if >35kg and 500mg >35kg) measure GH •Clonidine Stimulation: (0.1-0.15mg/m2 given orally)•IGF 1 measurement and IGFBP3 are low in most with GH deficiency (but low in starvation, liver pathology and psychological deprivation)•
Pituitary Function Testing Page 7

Water Deprivation Testing and a basic Approach to Polyuria.
C17/C20 Chemical Pathology: GSH
Definition: Polyuria is defined as > 2.5ml/kg/hour urine production in children or > 2500 ml/day in adults
Initial investigation = random S-Osm and U-Osm
1)- S-Osm > U-Osm
Psychogenic1.Hypothalamic Disease e.g. sarcoid2.Drugs – thiazides, chlorpromazine, anticholinergics3.
Polydypsia
Disorders of Water intake and Output
Central DI1.Drug inhibition of AVP ( opiate antagonists)2.
Vasopressin Deficiency
Congenital1.Aquired2.
Chronic renal disease (post ATN, transplant rejection, post obstructive uropathy)
Hypokalaemia ( incl aldosteronism)
Hypercalcaemia ( incl hyperparaT)
Drugs: Lithium, methoxyflurane, demeclocycline
Systemic disease: myeloma, sjogrens, amyloid, sickle cell anaemia
Nephrogenic DI
Prior to Water Deprivation testing, exclude treatable aquired causes of nephrogenic DI:HypokalaemiaHypercalcaemiaDrugs: Lithium/Diuretics
2) – S-Osm < U-Osm
Osmotic Diuresis
Glucose: DM
NaCl: Salt wasting renal disease e.g chronic pyelonephritis, Barters syndr, Fanconi syndr, diuretics, hypoaldosteronism
Urea: CRF, recovery phase of ATN
Other: mannitol
Surgery/trauma/infection/granuloma/infarction/tumor( craniopharyngiomas)
Causes of Central DI
Diabetes Insipidus10 August 201011:21 PM
Pituitary Function Testing Page 8

Idiopathic : decreased ADH fibres present in adolescence, 40% have antibodies VS ADH neurons
Familial Central DI (AR and AD) have decrease ADH neurons: rare
DIDMOAD (Wolfram synr) = ADom, DI, DM, optic atrophy and deafness.
Placental vasopressinase may cause cause DI in pregnancy.
X linked Nephrogenic DI: boys, mutated V2 receptor and decreased adenylate cyclase activity
Mutations of the aquaporin II gene (boys and girls ) AR.
Inherited causes of Nephrogenic DI
Water deprivation Test:
Principle: The aim of water deprivation testing is to further investigate patients with polyuria/polydypsia and dilute urine with a low osmolality. It is used to differentiate primary polydypsia from DI in the first phase and then to distinguish AVP deficiency (Central DI) from AVP insensitivity (nephrogenic DI ) in phase II.
Phase I: Patients are kept NPO and if DI is present, they will continue to dehydrate beyond normal physiological set points. If a patient demonstrates significant dehydration as measured by a S-Na of > 145mmol/l, and/or a S-Osm of > 300 mOsm/kg (measured) and/or a >3% weight loss and a low Urine osmol within 8 hours of fasting they have an inability to retain water and have diabetes insipidus.
If they are able to concentrate their urine above 650mOsm/kg within 8 hours NPO and do not reach dehydration set points they most likely have primary polydypsia.
Some forms of partial DI take longer than 8 hours to reach dehydration end points. In these cases the first phase of the testcan be extended to12 - 18 hours before they reach dehydration targets.
Patients with primary polydypsia (psychogenic/drugs/thirst centre defects) initially produce dilute urine that gradually begins to concentrate as they fast. It can sometimes take longer than 8 hours for these patients to produce concentrated urine as their hypertonic renal medullary portal systems are often washed out and time is required for this to correct itself, they do not however reach dehydration set points even after 12 – 18 hours NPO.
Some patients yield equivocal results in phase I that are difficult to interpret. These patients can be given a therapeutic DDAVP trial under close supervision. Patients with central DI show an improvement, those with nephrogenic DI show none and those with primary polydypsia develop hyponatraemia; these patients must be watched closely.
Water deprivation should only be performed if the baseline S-Osm is < 295 mOsm/kg
In full blown DI patients, phase I can be extremely uncomfortable as thirst increases dramatically and patients must be kept away from fluids with vigilance. Blood and urine chemistry should also be measured rapidly and the results reported within a short time so as to minimize unnecessary prolongation of phase 1
Phase II: Once dehydration is achieved DDAVP (desmopressin) is given IM/IV (1µg) or intra-nasally (10-20µg) and free access to water is allowed. Central or cranial DI patients show a good response and are able to concentrate their urine and decrease the volume reaching a target U-Osm of 650 mOsm/kg within 2 – 4 hours. Patients with Nephrogenic DI demonstrate no response and continue to produce a large volume of dilute urine. (Note:-only DI patients go into phase II and get DDAVP). Please be careful when allowing central DI children free access to water after giving DDAVP, during phase I they become extremely thirsty and when allowed to drink they can take in too much water too soon and this, combined with DDAVP’s renal actions can result in severe fluid overload and reciprocal hyponatraemia.
Target Cutoff values for Dx of DI during water deprivation Testing
Initial S-Osm Final S-Na Final S-Osm U-Osm % weight change
Phase I < 295 mOsm/kg ≥145 mmol/l ≥300 mOsm/kg < 650mOSM/kgplateau for >3hr
≥3%
Phase 11 / / // 650 mOsm/kg /
Pituitary Function Testing Page 9

Protocol:
Patients are allowed free fluids overnight and may take a light breakfast. Nicotine and caffeine are avoided.
Baseline bloods and a urine sample is obtained and the bladder voided. the patient is weighed after voiding urine
The patient is then kept NPO and blood and urine samples are collected every two hours, the patient is weighed and the urine volume over the preceding 2 hours measured and noted
Phase I continues until the dehydration cutoff values are achieved, in equivocal cases fasting is allowed for up to 18 hours.
If the patient does not achieve a dehydration cutoff and is able to achieve a U-Osmol of > 650 mOsm/kg within a maximum of 18 hours, a diagnosis of primary polydypsia is made and testing aborted
If dehydration targets are reached and urine osmol remains less than serum osmol. Phase II is begun
At the onset of phase II ,adult patients are given 1 ug DDAVP iv/sc/im and allowed free access to water
Urine osmol and volume is measured at ½ hourly intervals thereafter for 2-4 hrs. If an osmol of > 650 is achieved a diagnosis of central DI is made. If < 10% increase in U=Osm over 4 hours occurs, a diagnosis of nephrogenic DI is made. If the 4 hour U-Osm is < 650 but more than a 10% concentration in urine has occurred a diagnosis of partial nephrogenic DI is made.
Please arrange with C-17 core laboratory to have personnel available for stat serum and urine osmolarity measurements during testing
The S-Osm can be calculated initially to exclude an osmolar gap (ethanol)
After baseline measurements as per the accompanying table only S-Na, S-Osm and U-Osm need to be measured during the test. Results can be expressed graphically if the data sheet is filled in.
Pituitary Function Testing Page 10

GSH Chemical Pathology
Water Deprivation Test
Patient
sticker
Referring Dr
Date
Phase 1 Phase 2
Baseline 1hr 2hr 3hr 4hr 5hr 6hr 7hr 8hr 30 min 60 min 90 min 120 min
Time
BP
Pulse
Weight(kg)
S-Li
S-Ca (corr)
S-urea
S-Na
S-K
S-gluc
S-creat
S-Osm:calc
S-Osm:meas
U-vol:ml
U-Osm:meas
Heparin
Clotting
Fluoride
Pituitary Function Testing Page 11
Synachten stimulation test:
Use 1µg synacthen if testing for pituitary failureUse 250µg Synacthen if testing for primary adrenal failure
Adrenal evaluation:250µg given IVICortisol and ACTH measured prior to Synacthen and at 30mins Increase above 550mmol/l excludes addisons
1µg Synacthen test:Baseline ACTH and cortisol. Synacthen given and blood for cortisol taken at 30 mins post.Normal response if cortisol > 550mmol/l
•
Insulin Induced Hypoglycaemia test:See test for GH deficiency. Cortisol should be >550mmol/l in face of hypoglycaemia <2.2mmol/lTrue test of pituitary reserve to stress. Rarely performed due to risks.
•
Metyrapone stimulation test:Metyrapone inhibits 11 B Hydroxylase preventing cortisol formation ==> reduced negative feedback ==> rise in ACTH and ==> rise in cortisol precursor (11 deoxycortisol). Also true test of ACTH secretion be Pituitary30mg/kg Metyrapone given orally at midnightmeasure 11 deoxycortisol level at 8amRise to > 0.2nmol/l (7µg/dl) considered normal
Useful in borderline cases where ACTH stimulation equivocal
•
CRH Stimulation test:•CRH (ovine) given at 1µg/kg IVI provokes a peak ACTH response in 15 mins and peak cortisol response in 30-60 mins (measure at 15mins intervals)Different responses:Primary adrenal insufficiency: exaggerated ACTH response with elevated basal levelsSecondary adrenal insufficiency: Absent ACTH response with Tertiary (hypothalamic disease) Delayed peak in ACTHbut overlap in acth response of N pts with pts with secondary adrenal insufficiency
Pituitary Evaluation:Various tests available. Theory ==> in absence of regular stimulation by ACTH, adrenals atrophy so N response to ACTH severely blunted
Hypocortisolism09 August 201011:39 AM
Adrenal Funtion Page 12

24hr Urine fractionated Metanephrines (current gold standard for diagnosis)
•
Plasma free metanephrines if available has high sensitivity and specificity•MRI for localisation, Ideally not contrasted CT as can cause hypertensive crisis
•
Table 3. Drugs that may cause false positive elevations of plasma and urinary catecholamines or metanephrines
Catecholamines
Metanephrines
NE E NMN MN
NE, norepinephrine; E, epinephrine; NMN, normetanephrine; MN, metanephrine. +++, substantial increase; ++, moderate increase; +, mild increase if any; - , little or no increase; *, indicates a drug that can also cause direct analytical interference with some methods. Adapted from Eisenhofer and Pacak (88).
Tricyclic antidepressants
Amitriptyline (Elavil), Imipramine (Topfranil), Nortriptyline (Aventyl)
+++ - +++ -
a-Blockers (non-selective)
Phenoxybenzamine (Dibenzyline)
+++ - +++ -
a-Blockers (a1-selective)
Doxazosin (Cardura), Terazosin
(Hytrin), Prazosin (Minipress)
+ - - -
ß-Blockers
Atenolol (Tenormin), Metoprolol (Lopressor),
Propranolol (Inderal), Labetolol (Normadyne)*
+ + + +
Calcium channel antagonists
Nifedipine (Procardia), Amlodipine (Norvasc),
Diltiazem (Cardizem), Verapamil
+ + - -
Vasodilators
Hydralazine (Apresoline), Isosorbide
(Isordil, Dilatrate), Minoxidil (Loniten)
+ - unknown unknown
Monoamine oxidase inhibitors
Phenelzine (Nardil), tranylcypromine
(Parnate), Selegiline (Eldepryl)
- - +++ +++
Sympathomimetics
Ephedrine, Pseudoephedrine (Sudafed),
Amphetamines, Albuterol (Proventil)
++ ++ ++ ++
Stimulants
Caffeine (coffee*, tea), Nicotine
(tobacco), Theophylline
++ ++ unknown unknown
Miscellaneous
Levodopa, Carbidopa (Sinemet)* ++ - unknown unknown
Cocaine ++ ++ unknown unknown
Phaeochromocytoma:09 August 201004:21 PM
Adrenal Funtion Page 13

Primary aldosteronism (PA) is a group of disordersin which aldosterone production is inappropriatelyhigh, relatively autonomous, and non-suppressibleby sodium loading.Primary aldosteronism caused by adrenal adenoma, adrenal hyperplasia and glucocorticoid remediable aldosteronism
Aldosterone : renin ratio is gold standard screening testFour testing procedures (oral sodium loading, salineinfusion, fludrocortisone suppression, and captoprilchallenge) are in common use, and there is currentlyinsufficient direct evidence to recommend one overthe others.
Hyperaldosteronism:09 August 201004:42 PM
Adrenal Funtion Page 14

Adrenal Funtion Page 15

Adrenal Funtion Page 16

Figure 1. Clinical spectrum of steroid 21-hydroxylase deficiency
(from New MI, Dupont B Grumbach K, Levine LS. In: Stanbury JB, Wyngaarden JB. et al, eds. The Metabolic Basis of Inherited Disease, 5th ed. New York: McGraw-Hill, 1983:973-1000 with
permission).
Table 1. Clinical and Biochemical Features of Various Disorders of
Adrenal Steroidogenesis
Deficiency (Adrenal Disorder) Genital Ambiguity
Postnatal
Virilization
Diagnostic
Hormones
Treatment
I. 21-Hydroxylase
A. Classic
1. Salt wasting (SW)b F Yes 17OHP
4-A
Aldosterone
HC, 10-15 mg/m2/day orally (PO), and 9FF,
0.05 - 0.2 mg/day PO
2. Simple virilizing (SV) F Yes 17-OHP,
4-A
HC (same);
addition of 9aFF (same) if
renin
B. Nonclassic (symptomatic and
asymptomatic)
No Yes 17-OHP,
4-A
HC, 10-15
mg/m2/ day or dex, 0.25-0.5 mg/day h.s.,
or prednisone 5-10 mg/day
II. 3-Hydroxysteroid dehydrogenaseb
A. Classic M Yes 17-OHP HC and 9FF
Pts with ambiguous genitalia and 46XX karyotype•Apparent cryptorchid males•Infants present with shock hypoglycaemia and chemical findings compatible with CAH
•
Males and females with signs of virilisation before puberty•
Who to test:
Congenital Adrenal Hyperplasia09 August 201005:09 PM
Adrenal Funtion Page 17

A. Classic M(±F)
Yes 17-OHP
5 17-
OHPDHEA
4-A
HC and 9FF
as for SW 21-OHD
B. Nonclassic No Yes 17-OHPDHEA
HC as for
nonclassic 21-OHD
III. 11ß-Hydroxylase
A. Classic (hypertensive CAH) F Yes DOCS
4-A
PRA
HC, 10-15
mg/m2/day
B. Nonclassic No Yes SDOC
HC, dex, or prednisone as
for nonclassical
21-OHD
III. 17-Hydroxylase/ 17,20-lyase M No DOCB
HC, 10-15
mg/m2/daya
IV. Steroidogenic acute regulatory protein (StAR; congenital lipoid hyperplasia)b
M No None HC, 10-15 mg/m2/ day
9FF, 0.05-0.2
mg/daya
17-OHP: 17-Hydroxyprogesterone; 4-A:
4-Androstenedione; B: Corticosterone; S:
11-Deoxycortisol; DOC: Deoxycorticosterone; DHEA: Dehydroepiandrosterone; HC:
Hydrocortisone; 5 17-OHP: 17-
hydroxypregnenolone; 9FF:
fludrocortisone acetate; dex: dexamethasone; PRA: Plasma renin
activitya With addition of sex steroidreplacement
at puberty;b Salt wasting is a risk
17OH Progesterone levels > 242nmol/l in a random sample is diagnosistic of 21-Hydroxylase deficiency
•
If doubt use 250µg Synacthen test (gold standard in non classical CAH)Measure 17OH Progesterone at baseline and at 60 mins. Levels >45 nmol/l diagnostic of 21-Hydroxlase deficiency
•
Diagnosis of Classical CAH
Adrenal Funtion Page 18
Adrenal Funtion Page 19

Polycystic Ovarian Syndrome:09 August 201011:39 AM
Ovarian Function Page 20
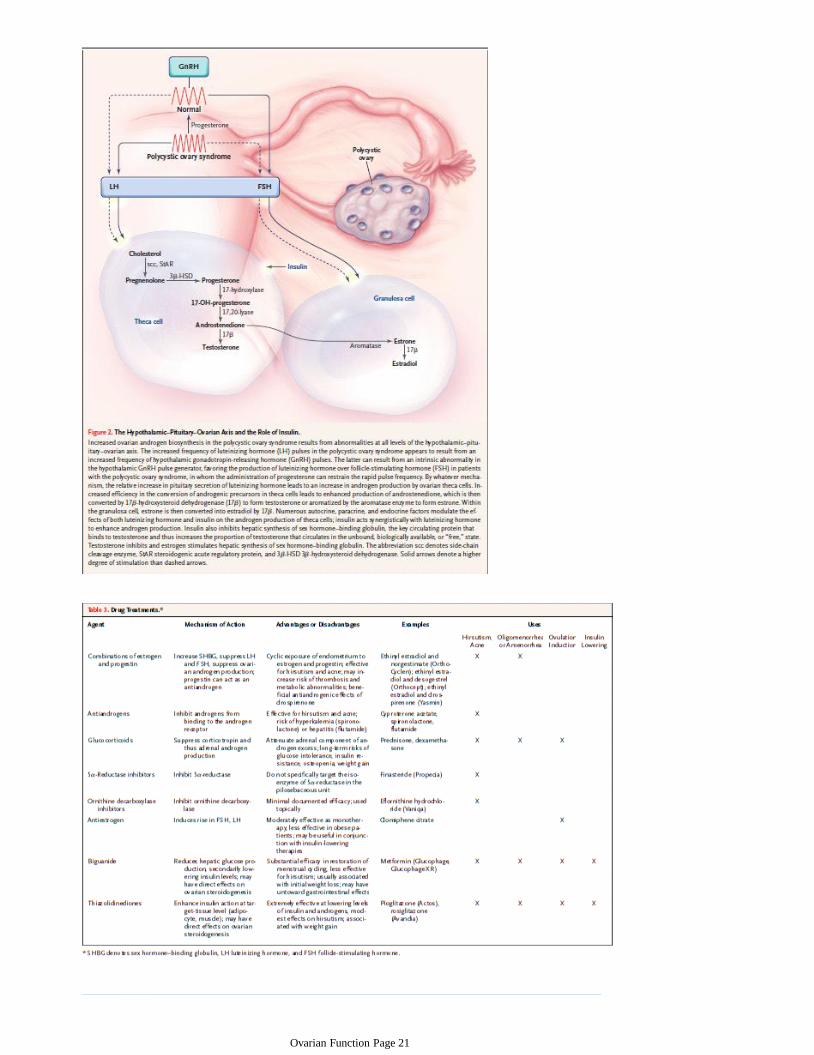
Figure 7. Pathophysiologic mechanisms associated with PCOS that may help
Ovarian Function Page 21
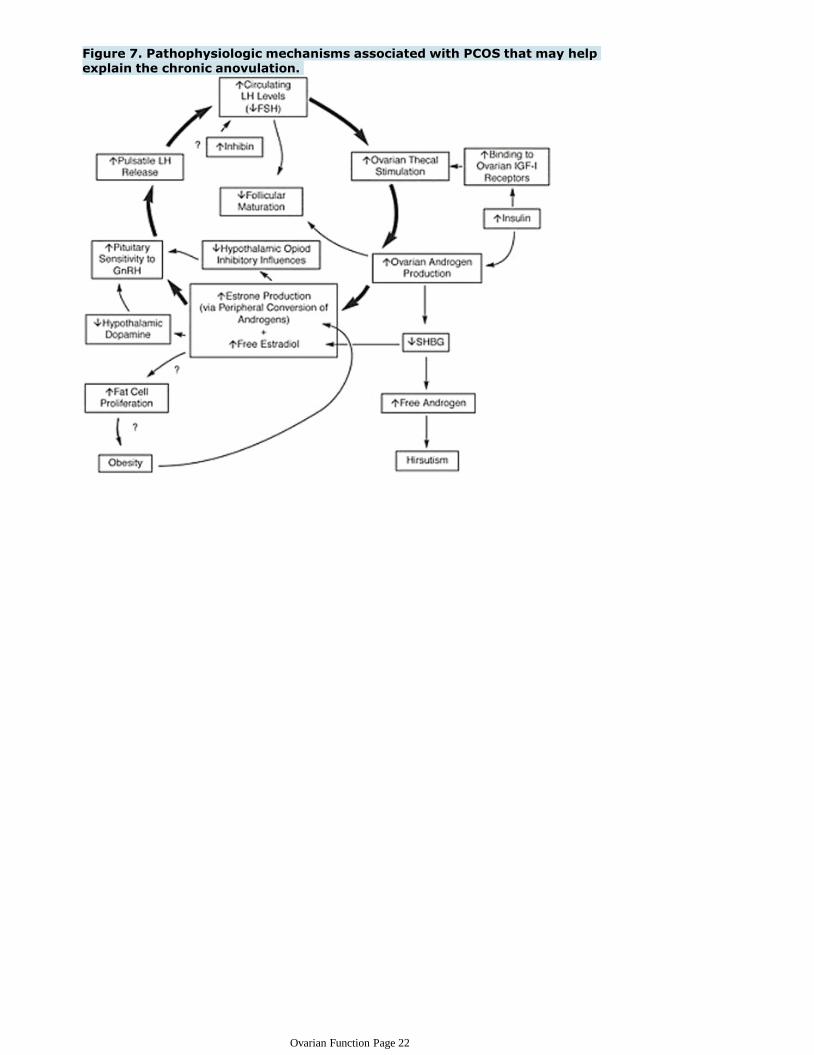
Figure 7. Pathophysiologic mechanisms associated with PCOS that may help explain the chronic anovulation.
Ovarian Function Page 22

Primary and Secondary Amenorrhoea10 August 201009:53 PM
Ovarian Function Page 23

Alterations in SHBG10 August 201009:54 PM
Ovarian Function Page 24
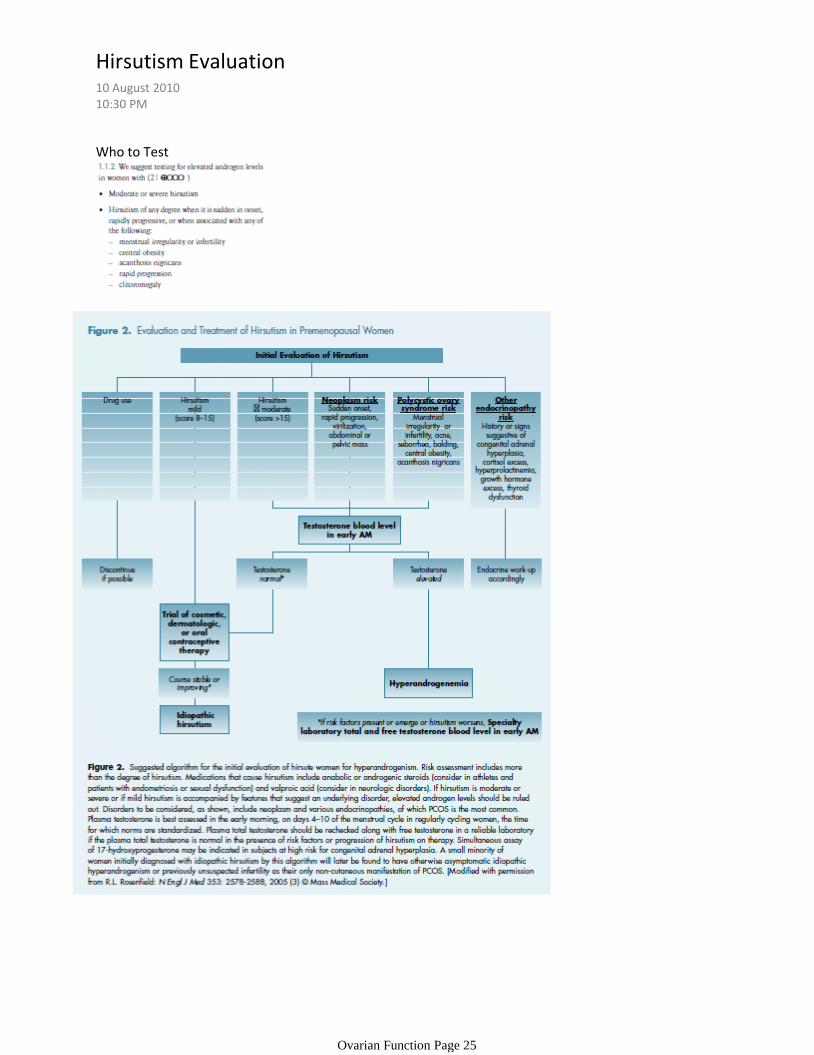
Who to Test
Hirsutism Evaluation10 August 201010:30 PM
Ovarian Function Page 25

Ovarian Function Page 26

Primary and Secondary Hypogonadism09 August 201011:39 AM
Testicular Function Page 27

Testicular Function Page 28

Gynaecomastia Investigation10 August 201009:54 PM
Testicular Function Page 29

Table 2. Drugs that induce gynecomastia by known mechanisms
Estrogen-
like, or binds to estrogen
receptor
Stimulate
estrogen synthesis
Supply
aromatizable estrogen precursors
Direct
Testicular Damage
Block
testosterone synthesis
Block
androgen action
Displace
estrogen from SHBG
Estrogen
vaginal cream
Gonadotro
pins
Exogenous
androgen
Busulfan Ketoconazo
le
Flutamide Spironolact
one
Estrogen-
containing embalming cream
Growth
Hormone
Androgen
precursors (ie androstene
dione and DHEA)
Nitrosurea Spironolact
one
Bicalutami
de
Ethanol
Delousing
powder
Vincristine Metronidaz
ole
Finasteride
Digitalis Ethanol Etomidate Cyproteron
e
Clomiphen
e
Zanoterone
Marijuana Cimetidine
Ranitidine
Testicular Function Page 30

Ranitidine
Spironolact
one
Table 3. Drugs that cause gynecomastia by uncertain mechanisms:
Calcium channel blockers (verapamil, nifedipine, diltiazem) 1.ACE Inhibitors (captopril, enalapril) 2.b blockers 3.Amiodarone 4.Methyldopa 5.Reserpine 6.Nitrates 7.
Cardiac and antihypertensive medications:
Neuroleptics 1.Diazepam 2.Phenytoin 3.Tricyclic antidepressants 4.Haloperidol 5.
Psychoactive drugs:
Indinavir 1.Isoniazid 2.Ethionamide 3.Griseofulvin 4.
Drugs for infectious diseases:
Amphetamines 1.Drugs of Abuse:
Theophylline 1.Omeprazole 2.Auranofin 3.Diethylpropion 4.Domperidone 5.Penicillamine 6.Sulindac 7.Heparin 8.
Others:
Testicular Function Page 31

Ambiguous Genitalia Workup Algorithm09 August 201011:40 AM
Ambiguous Genetalia Page 32

Ambiguous Genetalia Page 33
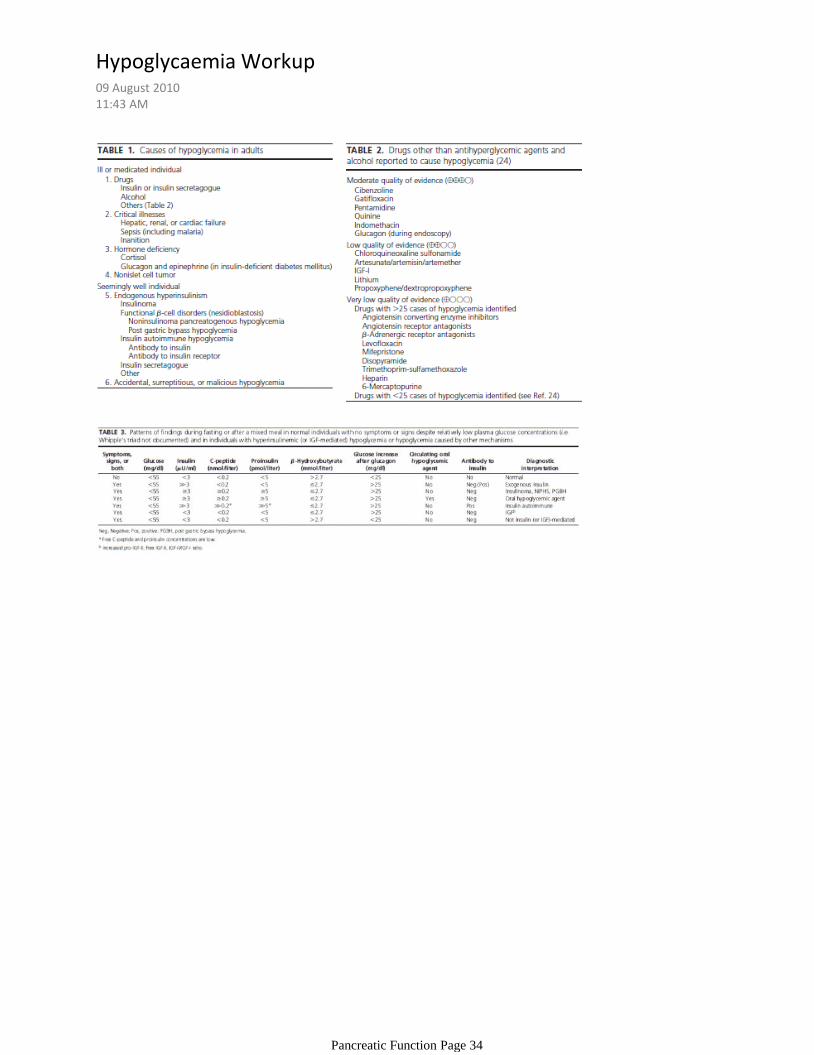
Hypoglycaemia Workup09 August 201011:43 AM
Pancreatic Function Page 34
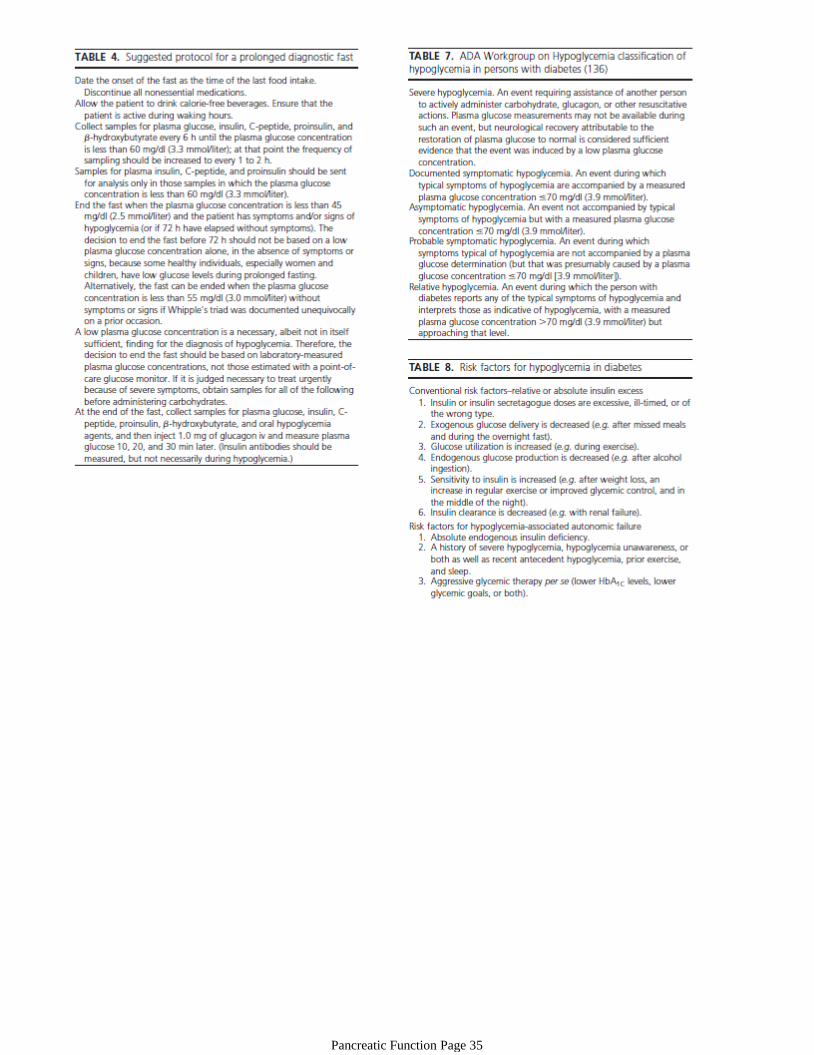
Pancreatic Function Page 35

2010 ADA Diagnostic Criteria
Diabetes Diagnosis10 August 201010:51 PM
Pancreatic Function Page 36

Diabetesguidelines ...
Pancreatic Function Page 37

Table 3. Diagnostic tests of cardiovascular autonomic neuropathy
TEST METHOD/ PARAMETERS
Resting heart rateBeat-to-beat heart rate
Variation*
>100 beats/min is abnormal.With the patient at rest and
supine (no overnight coffee or hypoglycemic episodes), breathing 6 breaths/min, heart rate monitored by EKG or
ANSCORE device, a difference in heart rate of >15 beats/min is
normal and <10 beats/min is abnormal, R-R inspiration/R-R expiration >1.17. All indices of HRV are age-dependent**.
Heart rate response to Standing* During continuous EKG monitoring, the R-R interval is measured at beats 15 and 30 after standing. Normally, a
tachycardia is followed by reflex bradycardia. The 30:15 ratio is normally >1.03.
Heart rate response to Valsalva maneuver* The subject forcibly exhales into the mouthpiece of a
manometer to 40 mmHg for 15 s during EKG monitoring. Healthy subjects develop tachycardia and peripheral
vasoconstriction during strain and an overshoot bradycardia
and rise in blood pressure with release. The ratio of longest R-R shortest R-R should be >1.2.
Systolic blood pressure response to standing Systolic blood pressure is measured in the supine subject. The
patient stands and the systolic blood pressure is measured after 2 min. Normal response is a fall of <10 mmHg, borderline is a fall of 10-29 mmHg, and abnormal is a fall of >30 mmHg
with symptoms.
Diastolic blood pressure response to isometric exercise
The subject squeezes a handgrip dynamometer to establish a maximum. Grip is then squeezed at 30% maximum for 5 min.
The normal response for diastolic blood pressure is a rise of >16 mmHg in the other arm.
EKG QT/QTc intervalsSpectral analysis
The QTc (corrected QT intevval on EKG) should be <440 ms.VLF peak
(sympathetic dysfunction)LF peak
(sympathetic dysfunction)HF peak
(parasympathetic dysfunction)LH/HF ratio
(sympathetic imbalance)
Neurovascular flow Using noninvasive laser Doppler measures of peripheral
sympathetic responses to nociception.
* These can now be performed quickly (<15 min) in
the practitioners' office, with a central reference laboratory providing quality control and normative
values. VLF,LF, HF =low, very low and high frequency
peaks on spectral analysis. These are now readily available in most cardiologist's practice.
** Lowest normal value of E/I ratio: Age 20-24:1.17,
25-29:1.15, 30-34:1.13, 35-30:1.12, 40-44:1.10, 45-49:1.08, 50-54:1.07, 55-59:1.06, 60-64:1.04,
65-69:1.03, 70-75:1.02 .
Cardiovascular Autonomic Function Tests09 August 201002:58 PM
Autonomic Function Page 38