emerging trends and developments in medicaid payment ahla annual meeting june 29, 2015-july 1, 2015...
TRANSCRIPT

EMERGING TRENDS AND DEVELOPMENTS
IN MEDICAID PAYMENT
AHLA ANNUAL MEETINGJune 29, 2015-July 1, 2015
Washington, D.C.
Jennifer L. Evans Joel M. HammePolsinelli P.C. Powers Pyles Sutter & Verville,
P.C.
1

SYNOPSIS OF SESSION Overview of the Medicaid program Provider rights of action involving Medicaid
reimbursement Medicaid eligibility expansion under the
Affordable Care Act (ACA) Health insurance exchange subsidies and
Medicaid Developments and issues in Medicaid
managed care
Emerging Trends And Developments In Medicaid Payment
2

Medicaid (Title XIX of the Social Security Act, 42 U.S.C. § 1396 et seq.) enacted at same time as Medicare (Title XVIII, 42 U.S.C. § 1395 et seq.). Social Security Act Amendments of 1965, P.L. 89-97 (July 30, 1965)
Unlike Medicare which is 100% federally funded and administered, Medicaid is a cooperative federal-state program, voluntary, and jointly funded by the federal government and participating states
◦ United States Department of Health and Human Services (HHS) and the Centers for Medicare and Medicaid Services (CMS)
◦ Single State Medicaid Agencies
3
Medicaid Background

States must comply with federal Medicaid standards, including requirements as to the contents of their state plans, to qualify for federal financial participation (FFP)
States are not required to participate but all states do as well as the District of Columbia, Puerto Rico, U.S. Virgin Islands, Guam, and American Samoa
There are significant variations in state Medicaid programs in terms of
◦ Eligibility for benefits
◦ Covered services
◦ Program administration (e.g., reimbursement)
4
Medicaid Background (Cont’d)

Some contrasts with Medicare◦ Eligibility
Elderly (Medicare)
Indigent (Medicaid)
◦ Funding and administration 100% federal (Medicare)
Federal-state collaboration (Medicaid)
◦ Coverage Broader post-acute coverage in Medicaid (long term
care services)
Medicaid Background (Cont’d)
5
Mandatory
Physician services Lab and x-ray services Inpatient hospital Outpatient Hospital EPSDT for individuals under 21 Family planning Rural and federally qualified health
center (FQHC) services Nurse midwife services Nursing facility (NF) services for
individuals 21 and over Home health for certain
populations
Expansion Medicaid Essential Health Benefits
(“Benchmark Coverage” and “Benchmark Equivalent Coverage”)
Optional
Prescription drugs Clinic services Dental services, dentures Physical therapy and rehab Prosthetic devices, eyeglasses Primary care case management Institutions for individuals with
intellectual disabilities, formerly intermediate care facilities for the mentally retarded (ICF/MR) services
Inpatient psychiatric care for individuals under 21
Personal care services Hospice services Alcohol and Drug Treatment
Medicaid Background (Cont’d)Benefits
6

Different types of Medicaid include different eligibility criteria and benefit coverage
Mandatory Coverage Populations Optional Coverage Populations Medicaid Expansion Coverage (Optional
with states under Supreme Court’s decision in National Federation of Independent Business v. Sebelius –- NFIB, 132 S.Ct. 2566 (2012))
Medicaid Background (Cont’d) Eligibility
7

Mandatory Categorically Needy With Various Income Guidelines
◦ Pregnant women
◦ Infants up to age 1
◦ Children ages 1-5
◦ Children ages 6 to 19
◦ Parents at state’s 1996 AFDC levels (likely less than 50% FP Guidelines)
◦ Elderly and disabled persons receiving Supplemental Security Income (SSI)
Optional Categorically Needy: higher income, resources Optional Medically Needy: higher income, greater medical needs Medicaid Expansion Population – Non-Custodial Adults – Up to
138% of Federal Poverty Level (FPL)
8
Medicaid Background (Cont’d)Eligibility (Cont’d)

Medicaid Beneficiaries – 69.7 million (2014) (more than one in five Americans; Medicare enrollment was about 52.7 million at that time, though the numbers overlap because some individuals are dually eligible)
Medicaid Spending - $449.4 billion (2013) (about 15% of total national health expenditures; Medicare spending was approximately $585.7 billion or 20% of total national health expenditures)
Separately, the Children’s Health Insurance Program (CHIP) covers about 8.1 million children who would otherwise be uninsured from families with modest incomes too high to qualify for Medicaid. Title XXI of the Social Security Act (42 U.S.C. § 1397aa et seq.), enacted as part of the Balanced Budget Act of 1997, P.L. 105-33 (Aug. 5, 1997)
9
Medicaid Background (Cont’d)

Some Historical Background◦ When enacted, Medicaid had no payment standards
for Medicaid rates. Unlike Medicare which utilized a “reasonable cost” standard. 42 U.S.C. § 1395x(v)(1)(A)
◦ In 1968, statutory language was added to ensure that Medicaid rates did not exceed “reasonable charges” consistent with efficiency, economy, and quality of care as established by Medicare. P.L. 90-248, § 237 (Jan. 2, 1968) (see 42 U.S.C. § 1396a(a)(30)). This established a ceiling but not a floor for Medicaid rates
10
Medicaid Reimbursement And Provider Rights Of Action

Some Historical Background (Cont’d)◦ In 1972, Congress added a minimum Medicaid rate
standard for Medicaid skilled nursing facilities and intermediate care facilities effective July 1, 1976. It required Medicaid rates to be set on a “reasonable cost-related basis” using cost finding methods developed by the states and approved federally. P.L. 92-603, § 249 (Oct. 30, 1972) (formerly, 42 U.S.C. § 1396a(a)(13)(E))
◦ Federal regulatory efforts to postpone the effective date of Section 249 were thwarted in the courts. E.g., Alabama Nursing Home Ass’n v. Califano, 433 F. Supp. 1325 (M.D.Ala. 1977)
11
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
Some Historical Background (Cont’d)◦ Section 249 was replaced in 1980 by the Boren
Amendment which required states to make findings and assurances that their Medicaid rates for skilled nursing facilities and intermediate care facilities were “reasonable and adequate to meet the costs which must be incurred by efficiently and economically operated facilities in order to provide care and services in conformity with applicable state and federal laws, regulations and quality and safety standards.” P.L. 96-499, § 962 (Dec. 5, 1980, effective October 1, 1980) (formerly, 42 U.S.C. § 1396a(a)(13)(A))
12
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)

Some Historical Background (Cont’d)◦ The Boren Amendment was extended to Medicaid
rates for inpatient hospital services in 1981. P.L. 97-35, § 2173(a)(1) (Aug. 13, 1981) (also requiring consideration of hospitals serving disproportionate numbers of low income patients with special needs)
◦ Boren Amendment contained both procedural (findings and assurances) and substantive (rate adequacy) duties for state Medicaid agencies and triggered a significant amount of litigation over Medicaid rates. See also 42 C.F.R. §§ 447.205-.256 (reflecting Boren Amendment standards)
13
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
Some Historical Background (Cont’d)◦ Meanwhile, in 1989, Congress amended 42 U.S.C. §
1396a(a)(30)(A) to specify that Medicaid rates be adequate to enlist sufficient providers to assure that Medicaid beneficiaries have equal access to services. P.L. 101-239, § 6402(a) (Dec. 19, 1989)
◦ In 1990, the Supreme Court ruled that providers had a private right of action to enforce the Boren Amendment. Wilder v. Va. Hosp. Ass’n, 496 U.S. 498 (5-4 decision) (enforcement under 42 U.S.C. § 1983 -- violation of federal rights under color of state law)
14
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)

Some Historical Background (Cont’d)◦ In 1997, Congress repealed the Boren
Amendment and replaced it with language as to state Medicaid agencies’ duties to furnish public notice regarding rates. P.L. 105-33, § 4711(a) (Aug. 5, 1997). At the same time, Congress left 42 U.S.C. § 1396a(a)(30)(A), the “equal access” provision, untouched
◦ Medicaid providers mounted court challenges to Medicaid rates under the “equal access” provision
15
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
Some Historical Background (Cont’d)◦ Issues arose as to whether Medicaid providers had
a private right of action to enforce the “equal access” statute either through § 1983 or under the constitutional Supremacy Clause
◦ More recent Supreme Court case law as to § 1983 private rights of action in non-Medicaid cases had created questions as to whether it could be a vehicle for enforcing the “equal access” standard against states. E.g., Gonzaga Univ. v. Doe, 536 U.S. 273 (2002)
16
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
Some Historical Background (Cont’d)◦ In Douglas v. Indep. Living Ctr. Of S. Cal., Inc., 132 S.Ct.
1204 (2012), the Supreme Court granted certiorari to decide whether the “equal access” provision could be privately enforced through the Supremacy Clause even though the Court had never resolved the issue of whether § 1983 furnished such a right of action
◦ Ultimately, due to changed circumstances (CMS had later approved some challenged plan amendments and the state withdrew others), the Court avoided (5-4) deciding the issue and remanded the case to the Ninth Circuit which had previously found private rights of action under the Supremacy Clause
17
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)

Some Historical Background (Cont’d)◦ In Armstrong v. Exceptional Child Center, Inc., No.
14-15 (U.S.), the Court granted certiorari to decide the same question. The Ninth Circuit and a federal district court in Idaho had found that the “equal access” statute could be privately enforced through the Supremacy Clause and that the state’s Medicaid rates for habilitation services violated the “equal access” provision
18
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)

Some Historical Background (Cont’d)◦ 5-4 Decision in Exceptional Child Center (March 31,
2015) held that there was no right of action through the Supremacy Clause for Medicaid providers to sue state officials for alleged equal access violations
◦ Majority Opinion (written by Justice Scalia with concurrences by Chief Justice Roberts, Thomas, Breyer [in part], and Alito)
◦ Concurring Opinion (Justice Breyer)
◦ Dissenting Opinion (written by Justice Sotomayor joined by Justices Kennedy, Ginsburg, and Kagan)
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
19

Implications of Exceptional Child Center◦ What should HHS be doing?
1) Implement “equal access” regulations. Currently, there are no such regulations, though HHS proposed some previously. 76 Fed. Reg. 26,342 (May 6, 2011)
2) Modify existing regulations to eliminate Boren Amendment standards (42 C.F.R. §§ 447.205-.256)
3) Since all of the provisions previously discussed apply to Medicaid fee-for-service (FFS) providers, HHS should strengthen standards and agency oversight of Medicaid managed care rates. See later discussion on Medicaid Managed Care
4) Create procedures for Medicaid providers and beneficiaries to be part of the plan amendment review, waiver review, and general oversight process
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
20

Implications of Exceptional Child Center (Cont’d)◦ Likely state efforts to use decision to bar
beneficiary and provider suits on wide array of other Medicaid statutory requirements
◦ As a joint federal-state program, state statutes, regulations, and contracts are relevant and may create actionable rights in state tribunals
Medicaid Reimbursement And Provider Rights Of Action (Cont’d)
21
Terms of Medicaid Eligibility Expansion◦ Incomes of 138% or less of the FPL, not pregnant,
not entitled to or enrolled for Medicare Part A, Medicare Part B, or Medicaid as of December 1, 2009 under state plan or waiver
◦ Mandatory expansion as of January 1, 2014
◦ Entitled to benchmark or benchmark equivalent coverage
Medicaid Eligibility Expansion Under the ACA
22

Terms of Medicaid Eligibility Expansion (Cont’d)
◦ Enhanced federal match rates to cover the expansion population. Basically, with some exceptions: Calendar Year (CY) 2014 - 100%
CY 2015 - 100%
CY 2016 - 100%
CY 2017 - 95%
CY 2018 - 94%
CY 2019 - 93%
CY 2020 and thereafter - 90%
Medicaid Eligibility Expansion Under the ACA (Cont’d)
23

Supreme Court Decision in NFIB◦ 7-2 majority found mandatory Medicaid expansion
unconstitutionally coercive. But no bright line test or limiting principle
◦ 5-4 majority concluded that voluntary Medicaid eligibility expansion would be permissible
HHS Guidance on Ensuing Medicaid Expansion Issues◦ Timing of expansion?
◦ Implications of decision? Permanent? Changeable?
◦ Partial or phased expansion?
◦ Non-expansion states and the individual mandate?
State of the States
Medicaid Eligibility Expansion Under the ACA (Cont’d)
24
WA
OR
CA
NV
ID
MT
WY
COUT
NMAZ
TX
OK
KS
NE
SD
ND
MN
WI
IL
IA
MO
AR
LA
AL
TN
MI
PA
NY
VT
GA
FL
MS
KY
SC
NC
OH DEIN
WV
NJ
CT
MA
ME
RI
VA
NH
AK
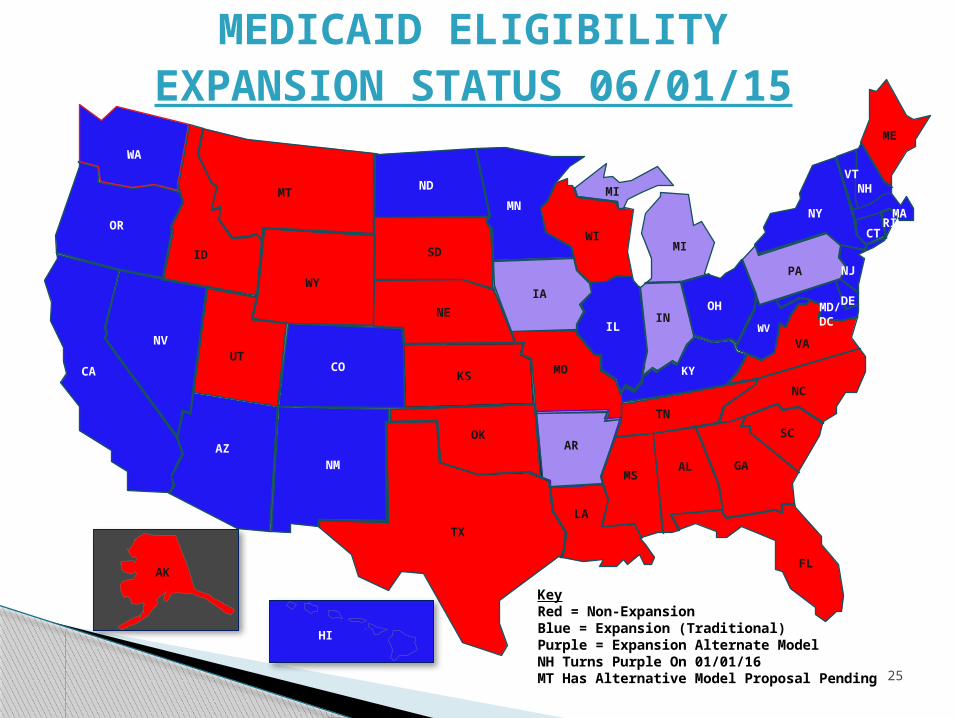
MEDICAID ELIGIBILITYEXPANSION STATUS 06/01/15
HI
MD/DC
MI
KeyRed = Non-ExpansionBlue = Expansion (Traditional) Purple = Expansion Alternate ModelNH Turns Purple On 01/01/16MT Has Alternative Model Proposal Pending 25

Medicaid Eligibility Expansion “Score Card” (as of 06/01/15)
◦ 30 expansion jurisdictions
24 traditional expansion
5 alternative model expansion (subsidies to purchase on exchanges)
1 alternative model waiver proposal pending
◦ 21 non-expansion states
Eligibility Expansion Litigation
◦ Low income and uncompensated care pools (LIPs and UCPs) used in various states to compensate providers for furnishing uncompensated care
◦ History of Florida’s LIP-spending ballooned from $1 billion annually to $2.6 billion annually
Medicaid Eligibility Expansion Under the ACA (Cont’d)
26

Eligibility Expansion Litigation (Cont’d)
◦ HHS statement of principles for reviewing further LIP extensions Coverage preferable to uncompensated care
payments; LIPs and UCPs should not pay for costs that would be covered by Medicaid eligibility expansion
Medicaid payments should support provider services to Medicaid and low income uninsured
Payment rate sufficiency
Medicaid Eligibility Expansion Under the ACA (Cont’d)
27

Florida’s Litigation◦ Scott v. U.S. Dept. of HHS, Case Nos. 3:15-CV-
00193-RS-CSK and 00195-MCR-EMT (N.D. Fla.)
◦ NFIB rationale-coercion
◦ Kansas and Texas amici curiae in support of Florida
The Irony◦ Rejecting 90%-100% FFP for actual coverage
while fomenting state budget problems because LIPs and UCPs are funded only at normal FFP rates
Medicaid Eligibility Expansion Under the ACA (Cont’d)
28

ACA Health Insurance Subsidies◦ Beginning in 2014, sliding scale tax credits to assist lower income
individuals not eligible for Medicaid to purchase health insurance on the exchanges
◦ Eligibility group – 100% to 400% of FPL
◦ NFIB means that, in non-expansion states, those below 100% FPL are not eligible for such subsidies but those between 100% and 138% of FPL are eligible
Medicaid Maintenance OF Eligibility (MOE) Under The ACA◦ MOE provisions
CHIP – sunsetted as of October 1, 2019
Medicaid – MOE terminates when exchange established by state is operational
Health Insurance Exchange Subsidies And Medicaid
29

Medicaid MOE Under The ACA (Cont’d)◦ Effect of NFIB
◦ Maine’s challenge to Medicaid MOE Mayhew v. Burwell, No. 14-1300 (1st Cir. Nov.
17, 2014), cert. denied, No. 14-992 (U.S. June 8, 2015)
Maine’s attempt to drop Medicaid coverage for 19 and 20 year olds rejected
MOE provision not unconstitutionally coercive
Health Insurance Exchange Subsidies And Medicaid (Cont’d)
30

King v. Burwell, No. 14-114 (U.S.) and Medicaid MOE◦ Challenge in King is the use of tax subsidies in states
not operating their own exchanges
◦ If challenge prevails, Medicaid MOE would extend until state establishes own exchange
◦ Only 14 jurisdictions operate own exchanges
◦ Only 1 non-expansion state operates its own exchange
◦ Three additional states received conditional HHS approvals on June 15, 2015 to operate their own exchanges. All are expansion states
Health Insurance Exchange Subsidies And Medicaid (Cont’d)
31

Purposes and Objectives of Medicaid Managed Care
The Growth of Medicaid Managed Care
◦ In 1992, 24 million Medicaid beneficiaries (8% of beneficiaries) were covered by managed care
◦ In 1998, 12.6 million Medicaid beneficiaries (41%) had managed care coverage
◦ By FY 2011, 39 million Medicaid beneficiaries (58%) were in managed care
◦ Estimated that, in 2015, 46 million Medicaid beneficiaries (73%) will be in managed care
◦ 39 states and the District of Columbia use Medicaid managed care and pay about $123.6 billion annually to managed care entities
Medicaid Managed Care
32

Proposed Medicaid Managed Care Rules. 80 Fed. Reg. 31,098 (June 1, 2015)◦ The Basics
Contract requirements Information requirements
◦ State requirements Enrollment Disenrollment
◦ Rights and protections for enrollees Informational rights Dignity and privacy rights Treatment options and alternatives Participation in care decisions Freedom from restraints and coercion
◦ Communication rights of health care professionals
Medicaid Managed Care (Cont’d)
33

Proposed Rules (Cont’d)◦ Managed Care Organization (MCO) fiscal
obligations Restrictions on marketing efforts No enrollee liability Solvency requirements
◦ Quality Assessment and Performance Improvement (QAPI) Access standards and care coordination Operational standards and quality programs External quality review
Medicaid Managed Care (Cont’d)
34

Proposed Rules (Cont’d)◦ Grievance system
Fair hearings Enrollee appeals
◦ Program Integrity Identification and return of overpayments Compliance programs Provider enrollment Sanctions
Medicaid Managed Care (Cont’d)
35

QUESTIONS AND ANSWERS
36