economic evaluations of clinical pharmacy services: 20062010
TRANSCRIPT

Economic Evaluations of Clinical Pharmacy Services:
2006–2010
Daniel R. Touchette,1,* Fred Doloresco,2 Katie J. Suda,3 Alexandra Perez,4 Stuart Turner,5
Yash Jalundhwala,1 Maria C. Tangonan,1 and James M. Hoffman6
1Center for Pharmacoeconomic Research, Departments of Pharmacy Practice and Pharmacy Administration,
University of Illinois at Chicago, Chicago, Illinois; 2Department of Pharmacy Practice, University at Buffalo,
Buffalo, New York; 3Department of Clinical Pharmacy, University of Tennessee Health Science Center, Memphis,
Tennessee; 4Department of Sociobehavioral and Administrative Pharmacy, Nova Southeastern University, Fort
Lauderdale, Florida; 5Ernest Mario School of Pharmacy, Rutgers University, Piscataway, New Jersey; 6St. Jude
Children’s Research Hospital and the University of Tennessee Health Science Center, Memphis, Tennessee
Studies have consistently evidenced the positive clinical, economic, and humanistic benefits of pharma-cist-directed patient care in a variety of settings. Given the vast differences in clinical outcomes associ-ated with evaluated clinical pharmacy services (CPS), more detail as to the nature of the CPS isneeded to better understand observed differences in economic outcomes. With the growing trend ofoutpatient pharmacy services, these economic evaluations serve as viable decision-making tools inchoosing the most effective and cost-effective pharmacy programs. We previously conducted three sys-tematic reviews to evaluate the economic impact of CPS from 1988 to 2005. In this systematic review,our objectives were to describe and evaluate the quality of economic evaluations of CPS publishedbetween 2006 and 2010, with the goal of informing administrators and practitioners as to their cost-effectiveness. We searched the scientific literature by using the Medline, International PharmaceuticalAbstracts, Embase, and Cumulative Index to Nursing and Allied Health Literature databases to identifystudies describing CPS published from 2006 to 2010. Studies meeting our inclusion criteria (originalresearch articles that evaluated CPS and described economic and clinical outcomes) were reviewed bytwo investigators. Methodology used, economic evaluation type, CPS setting and type, and clinical andeconomic outcome results were extracted. Results were informally compared with previous systematicreviews. Of 3587 potential studies identified, 25 met inclusion criteria. Common CPS settings werehospital (36%), community (32%), and clinic or hospital-based ambulatory practices (28%). CPS typeswere disease state management (48%), general pharmacotherapeutic monitoring (24%), target drugprograms (8%), and patient education (4%). Two studies (8%) listed CPS as medication therapy man-agement. Costs were evaluated in 24 studies (96%) and sufficiently described in 13 (52%). Clinical orhumanistic outcomes were evaluated in 20 studies (80%) and were sufficiently described in 18 (72%).Control groups were included in 16 (70%) of 23 studies not involving modeling. Study assumptionsand limitations were stated and justified in eight studies (32%). Conclusions and recommendationswere considered justified and based on results in 24 studies (96%). Eighteen studies (72%) involvedfull economic evaluation. The mean � SD study quality score for full economic evaluations (18 stud-ies) was 60.4 � 22.3 of a possible 100 points. Benefit-cost ratios from three studies ranged from1.05:1 to 25.95:1, and incremental cost-effectiveness ratios of five studies were calculated and reported.Fewer studies documented the economic impact of CPS from 2006–2010 than from 2001–2005,although a higher proportion involved controlled designs and were full economic evaluations. Evalua-tions of ambulatory practices were increasingly common. CPS were generally considered cost-effectiveor provided a good benefit-cost ratio.
R E V I E W O F T H E R A P E U T I C S

KEY WORDS clinical pharmacy services, cost, cost-effectiveness, benefit-cost, cost-utility, outcomes, eco-nomic evaluation.(Pharmacotherapy 2014;34(8):771–793) doi: 10.1002/phar.1414
Health care costs in the United States havecontinued to rise for decades, requiring healthcare institutions to identify and adopt efficientmeans of controlling these costs. Although thepositive economic value of inpatient-based clini-cal pharmacy services (CPS) is already wellestablished, recent changes to health care policyand the transition of CPS to ambulatory care set-tings require the evaluation of the effectivenessand costs.1–4 Evidence evaluating CPS can leadto improvements in and justification for thedelivery of such services, decreasing costs aswell as improving health outcomes.Within the past few decades, pharmacy ser-
vices have undergone an immense transforma-tion from solely focusing on medicationdispensing and delivery to involving pharmacistsin delivering individualized specialized care aspart of health care teams. Clinical pharmacistsare experts in promoting safe and rational medi-cation use.5 CPS improve disease management,use of rational drug therapy, health promotion,and disease prevention through the use ofapplied knowledge, gathered experience, formedjudgment, and evidence-based practices, as wellas continuing education.5, 6
Recently, two major changes in policy haveplayed an essential role in molding the provisionof CPS. First, the Medicare Prescription Drug,Improvement and Modernization Act (MMA) of2003 recognized the pharmacist’s role in manag-ing medication therapy by establishing reim-bursement for medication therapy management(MTM) services delivered to Medicare patientsunder Medicare Part D.7, 8 Second, the PatientProtection and Affordable Care Act of 2010 sup-ported the integration of pharmacists withinmultidisciplinary health teams in Patient-Cen-tered Medical Homes (PCMHs) in whichreimbursements are on a fee-for-service basis.9
These two policies demonstrate the steady andsustained evolvement of CPS.A recent policy paper published by the AARP
(formerly known as the American Association ofRetired Persons) Public Policy Institute is pro-posing changes in Medicare Part D to heightenpatient participation in MTM programs and torequire Part D plans to increase coverage forMTM services.10 Additionally, the Patient Pro-tection and Affordable Care Act of 2010 HealthCare Reform has introduced the implementationof Accountable Care Organizations (ACOs) thatextend the interprofessional model of PCMHs inenhancing patient-centered care.9 Studies havealso consistently evidenced the positive clinical,economic, and humanistic benefits of pharma-cist-directed patient care in a variety of settings;however, many of these studies used less thanoptimal economic assessments of CPS.2–4, 11
Additionally, given the vast differences in clini-cal outcomes associated with evaluated CPS ser-vices, more detail as to the nature of the CPS isneeded to better understand observed differencesin economic outcomes.We previously conducted three systematic
reviews to evaluate the economic impact of CPSfrom 1988–2005.2–4 With the American Recov-ery and Reinvestment Act of 2004 (ARRA)requesting further implementation of compara-tive effectiveness research, and with the growingtrend of outpatient pharmacy services, these eco-nomic evaluations serve as viable decision-mak-ing tools in choosing the most effective andcost-effective pharmacy programs.1, 12, 13 Thusthe objectives of this study were to describe andevaluate the quality of economic evaluations ofCPS published between 2006 and 2010, with thegoal of informing administrators and practitio-ners as to their cost-effectiveness.
Methods
Article Retrieval, Screening, and Data Collection
A systematic review of scientific literature da-tabases, including Medline, International Phar-maceutical Abstracts (IPA), Embase, andCumulative Index to Nursing and Allied HealthLiterature (CINAHL), for the years 2006–2010inclusive was conducted to determine potential
Funding: James Hoffman’s contributions were supportedin part by the American Lebanese Syrian Associated Chari-ties (ALSAC).
*Address for correspondence: Daniel R. Touchette, Asso-ciate Professor, Department of Pharmacy Systems Outcomesand Policy, University of Illinois at Chicago College ofPharmacy, 833 Wood Street, M/C 886, Chicago, IL 60612;e-mail: [email protected].� 2014 Pharmacotherapy Publications, Inc.
772 PHARMACOTHERAPY Volume 34, Number 8, 2014

economic evaluations for review. Search termsused for the initial Medline and CINAHLsearches were as follows: “cost and cost analysis,”“cost benefit analysis,” “economics, pharmaceuti-cal” combined with “pharmaceutical services,”“delivery of health care,” “interdisciplinary com-munication,” “interdisciplinary,” “patient careteam,” “pharmacy service,” and “hospital.”Search terms used for the Embase database wereas follows: “health economics,” “health carecost,” “economic evaluation,” “cost benefit analy-sis,” “cost effectiveness analysis,” “drug cost,”“pharmacoeconomics,” “cost utility analysis,”“cost minimization analysis,” “cost,” “drug cost,”“hospital cost,” “hospitalization cost” combinedwith “pharmaceutical care,” “clinical pharmacy,”“pharmacy,” “interdisciplinary,” “interdisciplin-ary communication,” and “health care delivery.”Searches were further refined to include onlyclinical trials, guidelines, and systematic reviewsor meta-analyses, and to exclude non-Englisharticles, review articles, editorials, and incom-plete or unoriginal articles. In addition, the indi-vidual authors of this review contributed anyarticles within their personal collections, andClinicalTrials.gov and references of relevant arti-cles were searched to identify additional poten-tially eligible manuscripts.Each abstract was evaluated by two authors.
For inclusion, each study was required to be ori-ginal research; to assess a CPS, defined as apatient-level interaction by a clinical pharmacist,whether as a sole clinician or as part of a team;and to include an economic assessment (mea-surement of costs to provide the service, eco-nomic outcomes, or both). Studies involvingteam-based care were included only when thepharmacist was part of the evaluative team formost or all patients and was not included as partof the team on a solely consultative basis. Stud-ies that were only published in abstract form oronly reported clinical or humanistic outcomes,with no accompanying economic assessment,were excluded. When the abstract had insuffi-cient detail to assess inclusion, the text of thefull article was reviewed.After the review of abstracts for inclusion cri-
teria, full-text articles were obtained for allaccepted abstracts and were assigned to twoauthors for review.14 The data obtained fromeach article were recorded in a structured data-base designed in REDCap application (REDCapv.4.3.11; Vanderbilt University, Nashville, TN,USA, 2011), a secure Web-based application forbuilding and managing online surveys and
databases. The categories of data included in theabstraction form were citation details; articleclassification, including type of pharmacist inter-action (e.g., with patient, with physician); inclu-sion and exclusion criteria; objective;perspective; setting; study design; descriptions ofsites, patients, and intervention; structure of CPSincluding the degree of pharmacist autonomy,pharmacist training, access to clinical data bythe pharmacists involved; program costs; out-comes measured; type of economic evaluation;results; and quality assessment. If discrepanciesarose between the two reviewers with respect toany area of the data abstraction, the article wassubjected to a third reviewer. Continued dis-crepancies or uncertainty was discussed amongthe entire group of reviewers until consensuswas achieved.
Study Classification and Data Analysis
Articles for the review were categorized byusing a modified version of the structure in thisstudy.15 This classification involved denotingwhether the article compared alternative inter-ventions and whether the study collected infor-mation on both costs and outcomes of thediffering arms. The studies were also subcatego-rized based on the type of empirical studydesign and type of economic evaluation per-formed. Studies were also evaluated on whetherthey were a partial evaluation, such as a costdescription or outcomes description, or a fulleconomic evaluation.Where possible, the perspectives of studies
were classified as societal, health care payer,provider, or patient. Setting was categorized asaffiliated with a university, academic medicalcenter, or other teaching institution, as well asaccording to location and type.The type of CPS provided was described. Spe-
cifically, CPS were categorized as disease statemanagement, a CPS primarily directed atpatients with a specific disease state or diagno-sis; general pharmacotherapeutic monitoring,CPS that encompasses a broad range of activitiesbased primarily on the needs of a specific clinicor panel of patients; pharmacokinetic monitor-ing, target drug program, patient education,wellness program or immunization service,MTM, and health screening or laboratory testingservice.The structure of the CPS included the degree
of pharmacist autonomy, pharmacist training,and access to patient clinical data. Degree of
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 773

autonomy was rated as “low” if others, such asphysicians, had full control and all interventionsrequired approval prior to implementation;“medium” if pharmacists could intervene freelyin some aspects of the CPS but requiredapproval for other areas; and “high” if the phar-macists were able to intervene freely in the CPS,such as when collaborative agreements were inplace. The level of pharmacist training was cate-gorized as a pharmacy residency, board certifica-tion, number of years of work experience, orcompletion of program-specific training. Accessto clinical data, such as medical records or com-puterized clinical information for those involvedin the CPS, was rated as “low” if the data werelimited to information collected at the time ofpatient visit and a medication profile only,“medium” if pharmacists had access to informa-tion collected at the time of the patient encoun-ter or medication profile in addition to a limitedset of clinical data from one other source, and“high” if pharmacists had access to informationcollected at the time of the patient encounter orinformation available from a medication profilein addition to a comprehensive set of clinicaldata from multiple other sources.The quality of every article was evaluated by
using five questions addressing the presence orabsence of a comparator and the degree towhich economic, clinical, and humanistic out-comes were evaluated and described. For fulleconomic evaluations, the Quality of Health Eco-nomics Studies instrument was applied.16
Results
Search Results
Using the specified search criteria, 3587potentially relevant papers were initially identi-fied from the search. The full text of 317 poten-tially relevant manuscripts was reviewed.Twenty-five unique economic evaluations evalu-ating 24 different studies that met all inclusioncriteria were included. One study, the MEDMANstudy, was represented by two distinct economicevaluations.17, 18 Figure 1 shows the numbers ofstudies excluded at each step of the review.Evaluations were published in 17 different jour-
nals. In 12 of 25 cases (48%), evaluations werepublished pharmacy journals, with 13 of 25 (52%)published in nonpharmacy journals. The mostcommon journals in which publications appearedwere The Journal of the American Pharmacists Asso-ciation (4 of 25 [16%]) and Family Practice,
International Journal of Pharmacy Practice, Phar-macy World & Science, and Pharmacoeconomics,each publishing two manuscripts (8%). In con-trast to previous systematic reviews of this topic,none of the evaluations were published in theAmerican Journal of Health-System Pharmacy orPharmacotherapy, and only one evaluation waspublished in The Journal of Managed CarePharmacy.
Objectives and Setting
Economic evaluation was included as a pri-mary or secondary objective in 22 of 25 studies(88%). The study perspective was either stated oridentifiable in all but 5 of 25 (20%) of the reports.Studies were conducted from the perspective ofthe health care payer (11 of 25), provider (11 of25), and patient (1 of 25); two of the studies wereconducted from two perspectives.17, 19 No studiesused the societal perspective.With regard to where the study was con-
ducted, the origins of the studies were Europe(13 of 25 [52%]), United States (9 of 25 [36%]),Canada (2 of 25 [8%]), and Australia (1 of 25[4%]). None of the identified studies were con-ducted in Asia or Africa. Seven studies (28%)involved an academic faculty member or resi-dent to provide the clinical service or were con-ducted at an academic medical center, 13 of 25(52%) were conducted in nonacademic settings,and 5 of 25 (20%) were unclear.Clinical pharmacist services were delivered in
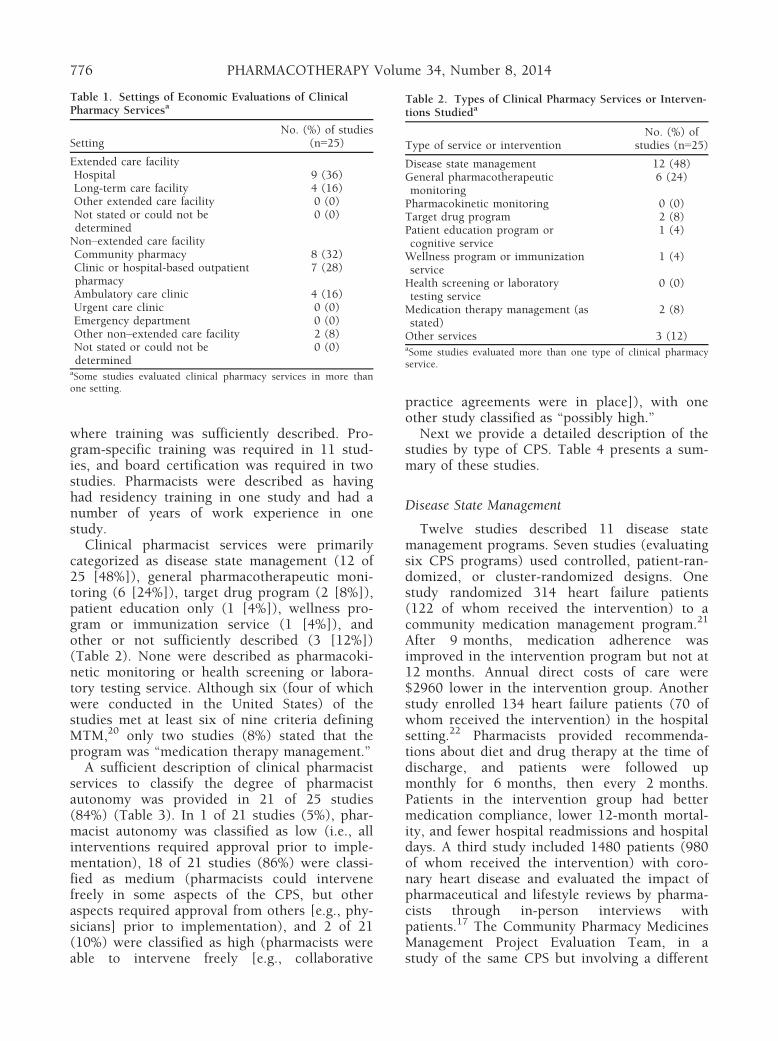
an extended and acute care setting in 13 studies(Table 1). Extended and acute care settingsincluded the hospital setting in nine studies(36%) and long-term care facility in four studies(16%). CPS were provided in ambulatory andcommunity settings in 13 studies. Ambulatoryand community settings included communitypharmacy (8 [32%]), clinic or hospital-basedindependent ambulatory pharmacy practices (7[28%]), physician-run ambulatory care clinics(4 [16%]), and the patient’s home or work (2[8%]). None of the evaluated studies claimed tobe part of a medical home.
Methods Used
A variety of study designs were used, with 8studies (32%) using a randomized posttestexperimental design, 5 (20%) a quasi-experi-mental design, 4 (16%) a preexperiment design(i.e., nonrandomized posttest without pretest-ing), 3 (12%) a before-and-after design (i.e.,
774 PHARMACOTHERAPY Volume 34, Number 8, 2014

historical control), 3 (12%) a noncomparative(i.e., single group) posttest design, and 2 (8%)solely used decision modeling. Of these, 16 of23 studies (70%) had a concurrent or historicalcontrol, and 15 of 16 studies (94%) with a con-trol group applied statistics to compare the twogroups. Although seven of the studies incorpo-rated some type of model, two of the studiesexclusively used a modeling methodology. Moststudies collected primary data (24 of 25 studies[96%]), whereas five studies used data from pre-viously published sources (one exclusively andfour augmenting primary empirical data).
With the exception of two modeling studiesand one study that evaluated prescriptions andnot people, the number of intervention sub-jects could be determined in 22 of 25 studies(88%). The median number of interventionstudy subjects enrolled was 293 (range: 58–1452). The median number of study sites was 2(range: 1–44).
Pharmacist Practice Activities
Additional training, certification, or experi-ence was required in 13 of 14 studies (93%)
Figure 1. Schematic of the literature search methods and screening results.
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 775
where training was sufficiently described. Pro-gram-specific training was required in 11 stud-ies, and board certification was required in twostudies. Pharmacists were described as havinghad residency training in one study and had anumber of years of work experience in onestudy.Clinical pharmacist services were primarily
categorized as disease state management (12 of25 [48%]), general pharmacotherapeutic moni-toring (6 [24%]), target drug program (2 [8%]),patient education only (1 [4%]), wellness pro-gram or immunization service (1 [4%]), andother or not sufficiently described (3 [12%])(Table 2). None were described as pharmacoki-netic monitoring or health screening or labora-tory testing service. Although six (four of whichwere conducted in the United States) of thestudies met at least six of nine criteria definingMTM,20 only two studies (8%) stated that theprogram was “medication therapy management.”A sufficient description of clinical pharmacist
services to classify the degree of pharmacistautonomy was provided in 21 of 25 studies(84%) (Table 3). In 1 of 21 studies (5%), phar-macist autonomy was classified as low (i.e., allinterventions required approval prior to imple-mentation), 18 of 21 studies (86%) were classi-fied as medium (pharmacists could intervenefreely in some aspects of the CPS, but otheraspects required approval from others [e.g., phy-sicians] prior to implementation), and 2 of 21(10%) were classified as high (pharmacists wereable to intervene freely [e.g., collaborative
practice agreements were in place]), with oneother study classified as “possibly high.”Next we provide a detailed description of the
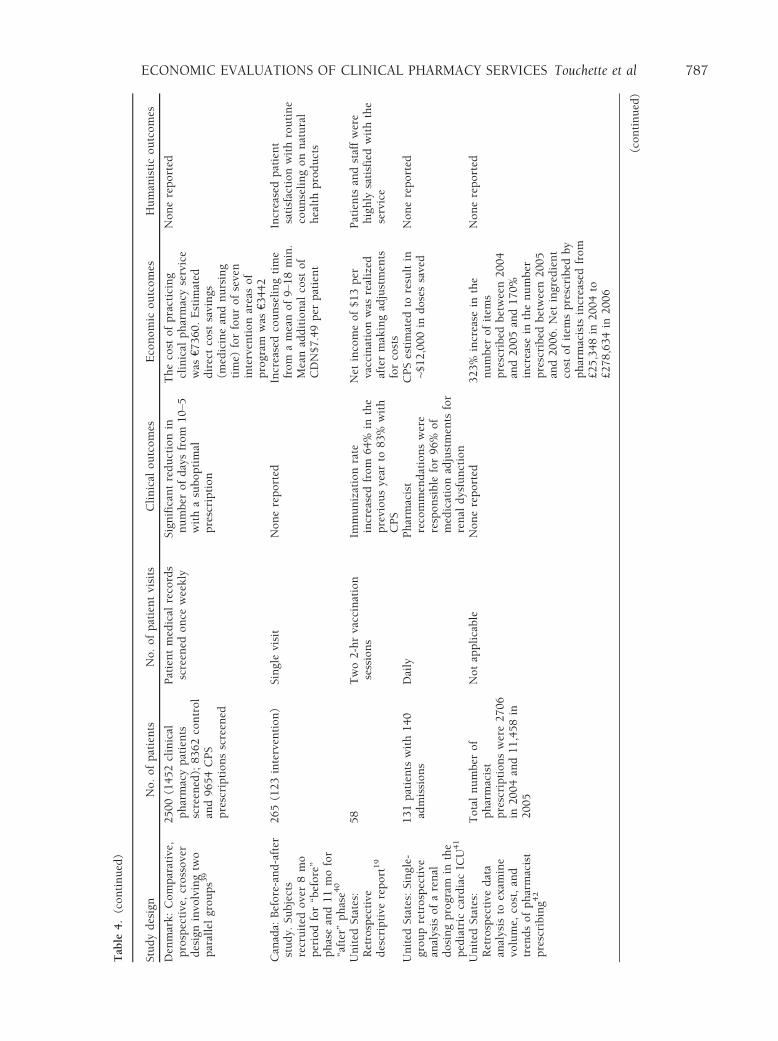
studies by type of CPS. Table 4 presents a sum-mary of these studies.
Disease State Management
Twelve studies described 11 disease statemanagement programs. Seven studies (evaluatingsix CPS programs) used controlled, patient-ran-domized, or cluster-randomized designs. Onestudy randomized 314 heart failure patients(122 of whom received the intervention) to acommunity medication management program.21
After 9 months, medication adherence wasimproved in the intervention program but not at12 months. Annual direct costs of care were$2960 lower in the intervention group. Anotherstudy enrolled 134 heart failure patients (70 ofwhom received the intervention) in the hospitalsetting.22 Pharmacists provided recommenda-tions about diet and drug therapy at the time ofdischarge, and patients were followed upmonthly for 6 months, then every 2 months.Patients in the intervention group had bettermedication compliance, lower 12-month mortal-ity, and fewer hospital readmissions and hospitaldays. A third study included 1480 patients (980of whom received the intervention) with coro-nary heart disease and evaluated the impact ofpharmaceutical and lifestyle reviews by pharma-cists through in-person interviews withpatients.17 The Community Pharmacy MedicinesManagement Project Evaluation Team, in astudy of the same CPS but involving a different
Table 1. Settings of Economic Evaluations of ClinicalPharmacy Servicesa
SettingNo. (%) of studies
(n=25)
Extended care facilityHospital 9 (36)Long-term care facility 4 (16)Other extended care facility 0 (0)Not stated or could not bedetermined
0 (0)
Non–extended care facilityCommunity pharmacy 8 (32)Clinic or hospital-based outpatientpharmacy
7 (28)
Ambulatory care clinic 4 (16)Urgent care clinic 0 (0)Emergency department 0 (0)Other non–extended care facility 2 (8)Not stated or could not bedetermined
0 (0)
aSome studies evaluated clinical pharmacy services in more thanone setting.
Table 2. Types of Clinical Pharmacy Services or Interven-tions Studieda
Type of service or interventionNo. (%) of
studies (n=25)
Disease state management 12 (48)General pharmacotherapeuticmonitoring
6 (24)
Pharmacokinetic monitoring 0 (0)Target drug program 2 (8)Patient education program orcognitive service
1 (4)
Wellness program or immunizationservice
1 (4)
Health screening or laboratorytesting service
0 (0)
Medication therapy management (asstated)
2 (8)
Other services 3 (12)aSome studies evaluated more than one type of clinical pharmacyservice.
776 PHARMACOTHERAPY Volume 34, Number 8, 2014

Table 3. Description of Pharmacist Training, Role, and Autonomy for Clinical Pharmacy Services
Pharmacist training Pharmacist role Level of pharmacist autonomy
United Kingdom: Communitypharmacist training occurredover a series of three events.Pharmacists received trainingdesigned and delivered by theCentre for Pharmacy Post-Graduate Education17, 18
The medicines management service wasdelivered from community pharmacypremises by community pharmacists.Pharmacists performed an initialconsultation informed by the extractedmedical data supplied by the researchers.Further consultations were providedaccording to pharmacist-determinedpatient need. Consultations includedassessments of the following: therapy,medication compliance, lifestyle (e.g.,smoking cessation, exercise, and diet) andsocial support (e.g., difficulties incollecting prescriptions and openingbottles). Recommendations were recordedon a referral form that was sent to the GPwho returned annotated copies to thepharmacists
Medium. Pharmacists could makerecommendations but not directchanges
United States: None described21 Protocol-driven medication history of allprescription and OTC drugs andassessment of patient medicationknowledge and skills. Patient-centeredverbal instructions and written materialsabout medications were provided topatients. Pharmacist monitored patients’medication use, health care encounters,and body weight. Communication withphysicians and clinic nurses was on an as-needed basis
Medium. Pharmacists providedverbal and written advice topatients but did not appear tohave prescriptive authority
Spain: None described22 Pharmacists were involved with givinginformation on disease, diet, and therapyon the day of hospital discharge. Patientswere provided with the contact numberand name of the pharmacist in casequestions arose. In addition, thepharmacist called the patient monthly forthe first 6 mo of therapy and then onceevery 2 mo
Medium. The pharmacist couldintervene and makerecommendations about diet anddrug therapy but could notprescribe medications
United Kingdom: 20 pharmacistsattended a 1-wk training courseincluding lectures andworkshops on the followingtopics: cardiovascular disease,Scottish Prescribing Analysisdata, prescribing indicators,repeat prescribing systems, druginformation, formularies,evidence-based medicine,communication, implementingguidelines, and an orientation tothe study. An additional 1-dayworkshop was held after 1 wk,and a feedback session was heldafter 6 mo once all pharmacistshad started work in practice toshare experiences and to answerany logistical or clinical queries23
Pharmacists were asked to conduct a singlereview of the patient’s medical records andrecommend to the GP changes for action.Recommendations were communicated toGPs by using a study referral form andwere not systematically followed up.Medication reviews were conducted byusing a form adapted from a nationaltemplate, and compliance assessment wasconducted
Medium. The pharmacists couldmake recommendations to thephysician but not prescribe
(continued)
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 777

Table 3. (continued)
Pharmacist training Pharmacist role Level of pharmacist autonomy
United Kingdom: Pharmacists hadextensive experience ofcommunity pharmacy practice24,25
An enhanced pharmacy review was carriedout in general practice surgeries. Theintention was that patients would receivebetween three and six consultations withthe pharmacist over a period of 10–12 wks. The pharmacist had access topatient notes. At the consultation, thepharmacist explored prescription andOTC medications being used by thepatient, including alternative andcomplementary therapies. All patientswere assessed for NSAID safety andsuitability based on medical andmedication history. The pharmacistaddressed knee pain control and providedrecommendations to continue, add, orchange medications, or provided a GPreferral. The pharmacist also discussedrelevant self-help measures that thepatient could take
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
Australia: Training was providedto intervention pharmacists only.Pharmacists undertook a woundmanagement training coursedeveloped and delivered by theDepartment of Pharmacy Practiceat Monash University, Australia.The course covered woundetiology, physiology of woundhealing, pathophysiology ofchronic wounds, factorsimpacting on wound healing,and wound management. Thecourse also included case studiesand practical hands-on sessions.Course participants were notformally assessed26
Nurses and the pharmacist met at leastweekly to identify new wounds anddiscuss treatment options within theprotocol. Between face-to-face meetings,pharmacists and nurses discussed casemanagement by telephone. Pharmacists inthe control arm did not participate inwound management
Medium. Pharmacists had someautonomy to work with thenurses to suggest woundmanagement techniques
United States: Participatingpharmacists receivedcardiovascular certificate trainingrecognized by the NorthCarolina Center forPharmaceutical Care, a service ofthe North Carolina Associationof Pharmacists27
Medication assessments were provided bycare managers including a comparison ofthe patient’s treatment regimen with thoserecommended in national guidelines.Blood pressure was checked at baseline aswell as during care manager visits. Lipidpanels were measured at baseline and atleast annually. Recommendations weremade to patients’ physicians, mostcommonly through faxes, when potentialimprovements in therapy were identified
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
(continued)
778 PHARMACOTHERAPY Volume 34, Number 8, 2014

Table 3. (continued)
Pharmacist training Pharmacist role Level of pharmacist autonomy
United States: Participatingpharmacists received asthmacertificate training recognized bythe North Carolina Center forPharmaceutical Care, a service ofthe North Carolina Associationof Pharmacists28
Patients received education by a certifiedasthma educator and regular long-termfollow-up by pharmacists (reimbursed formedication therapy management by healthplans) including scheduled consultations,monitoring, and recommendations tophysicians. Patients were provided anasthma action plan. Medicationassessments were provided including areview of patterns of reliever andcontroller medication use. Inhalertechnique, symptom frequency, andtriggers were assessed
Medium. Recommendations weremade to patients’ physicians,most commonly through faxes,when problems or the potentialfor improvements in therapywere identified
United States: Participatingpharmacists completed a trainingprogram in diabetes offered by aprovider of continuing pharmacyeducation accredited by theAccreditation Council onPharmacy Education or hadotherwise been certified fordiabetes care (e.g., CertifiedDiabetes Educator, certified in aspecialty approved by the Boardof Pharmaceutical Specialties)29
Community-based pharmacists providedpatient self-management care servicesthrough scheduled consultations within acollaborative care management model.During regularly scheduled visits,pharmacists applied a prescribed processof care that focused on clinicalassessments and progress toward clinicalgoal and worked with each patient toestablish self-management goals. Inaddition, they worked with other healthcare providers and could recommendadjustments in the patients’ treatmentplans when appropriate
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
Germany: None described30 The clinical pharmacist attended surgicalintensive care unit ward rounds once/week. Orders for select antifungal agentswere supervised by the clinicalpharmacist, and interventions were madewhen necessary
High. The pharmacist attendedrounds and was approved theuse of certain drugs. Pharmacistscould change prescriptions asneeded
United States: Critical care–trained pharmacist with a doctorof pharmacy degree. Noadditional training specified31
The pharmacist evaluated and monitoredmedication therapy for all adult patientson the neurosurgical service, regardless oflocation within the institution. Prior torounds, the pharmacist reviewed allpatient profiles, laboratory data, andmicrobiologic cultures. During rounds, thepharmacist participated in patient careplan development and evaluated necessarychanges to the medication regimen. Afterrounds, the pharmacist entered medicationorders into the computerized providerorder entry system. The pharmacistsubsequently monitored pharmacologicchanges initiated on morning rounds
Medium. The pharmacist attendedrounds and provided inputregarding therapy but did notappear to have prescriptiveauthority
United States: None described32 One clinical pharmacist provided thepatients’ physicians with writtenrecommendations to optimize medicationtherapy in the intervention group. For thecomparison group, the same pharmacistproposed recommendations that remainedconcealed from the physicians but weredocumented in a study database
Medium. The pharmacist couldmake recommendations to thephysician but not prescribe
(continued)
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 779

Table 3. (continued)
Pharmacist training Pharmacist role Level of pharmacist autonomy
United States: Postgraduatequalification in pharmacypractice or recent continuingprofessional development intherapeutics. Pharmacists alsoattended a 2-day training coursethat included lectures onprescribing for the elderly,adverse drug reactions,improving adherence, andcommunication skills33
Pharmacists visited patient homes twice toeducate them about their drugs, removeout-of-date drugs, inform GPs of drugreactions or interactions, and inform thelocal pharmacist if an adherence aid wasneeded
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
Switzerland: Senior clinicalpharmacist. No additionaltraining specified34
Pharmacists participated in clinical wardrounds and reviewed daily allnonformulary prescriptions and case notes
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
United Kingdom: Two trainingsessions covered the theory andpractice of pharmaceutical care,practical exercises incollaborating with GPs, andinvolving patients and caregiversto construct, implement, andmonitor a pharmaceutical careplan35
All recruited patients receivedpharmaceutical care adapted to Britishprimary care
Not described
United States: Board-certifiedgeriatric pharmacist. No study-specific training was described36
The pharmacist was included on aninterprofessional team. The pharmacistprovided drug information to unit nursingstaff, nurse practitioners, and physiciansfor all of the transitional care unitpatients. Other provided services includedconsultations on medically complexpatients and those experiencing potentialmedication-related problems, routine drugregimen review for all patients on theunit, improving geriatric transitional care,and in-services on relevant topics. Thepharmacist provided formal and informaleducation on geriatric pharmacology andevolving pharmacotherapy literature to allfaculty
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
Switzerland: Hypotheticalservice37
The hypothetical “clinical pharmacist” wasnot described
Not described
Canada: None described. Usedpharmacists in an existingclinic38
The pharmacist-managed anticoagulationservices pharmacist met patients once toreview medical history and to discusstreatment objectives, possible adverseevents, the need for frequent INR tests,and drug and food interactions. Warfarinwas initiated according to an institution-approved protocol, and follow-up wasconducted by telephone. Laboratoryresults were available through anetworked computer system
Not described. Although notstated, it is inferred thatpharmacists had autonomy toadjust warfarin dose according toa protocol, which would beconsistent with a high level ofautonomy
Denmark: No additional trainingwas described39
Patients’ medical records were screenedonce\week for suboptimal prescriptionswithin the 10 target intervention areas. Ifjustified, the clinical pharmacist woulddiscuss the prescription with the wardphysician
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
(continued)
780 PHARMACOTHERAPY Volume 34, Number 8, 2014

economic evaluation, found no significant differ-ences in primary clinical outcomes, but patientsatisfaction was better in the interventiongroup.18 The total British National Health Ser-vice cost was statistically significantly higher inthe intervention group (mean difference: £147).A fourth study evaluated the impact of pharma-cists’ reviews of the medical records of patientsin 43 general practices in Scotland involving 706angina patients (340 of whom received the inter-vention) and 1308 hypertensive patients (656 ofwhom received the intervention).23 A 7.6%increase in antiplatelet drug use was found, withno significant cost differences at 1 year. A fifthstudy evaluated enhanced pharmacy review,community physiotherapy, or usual care involv-ing 325 adults 55 years or older with knee painin 15 general practices in North Staffordshire,United Kingdom.24, 25 Improvements in the glo-bal assessment were observed at 3 months in thepharmacist review group, but 12-month clinicaloutcomes were not affected.25 Monthly medica-tion costs were decreased by £0.89 per personbetween the first and final consultation. A sixthstudy involved 21 Australian nursing homes and342 uncomplicated leg and pressure ulcers in176 patients.26 The proportion of healed wounds
was higher in the intervention arm versus thecontrol arm (61.7% vs 52.5%), and woundshealed faster (mean 82 vs 101 days). Treatmentresulted in decreased nursing time and a reduc-tion in the cost of care by $358 (Australian dol-lars) (p=0.006).Three studies used quasi-experimental or pre-
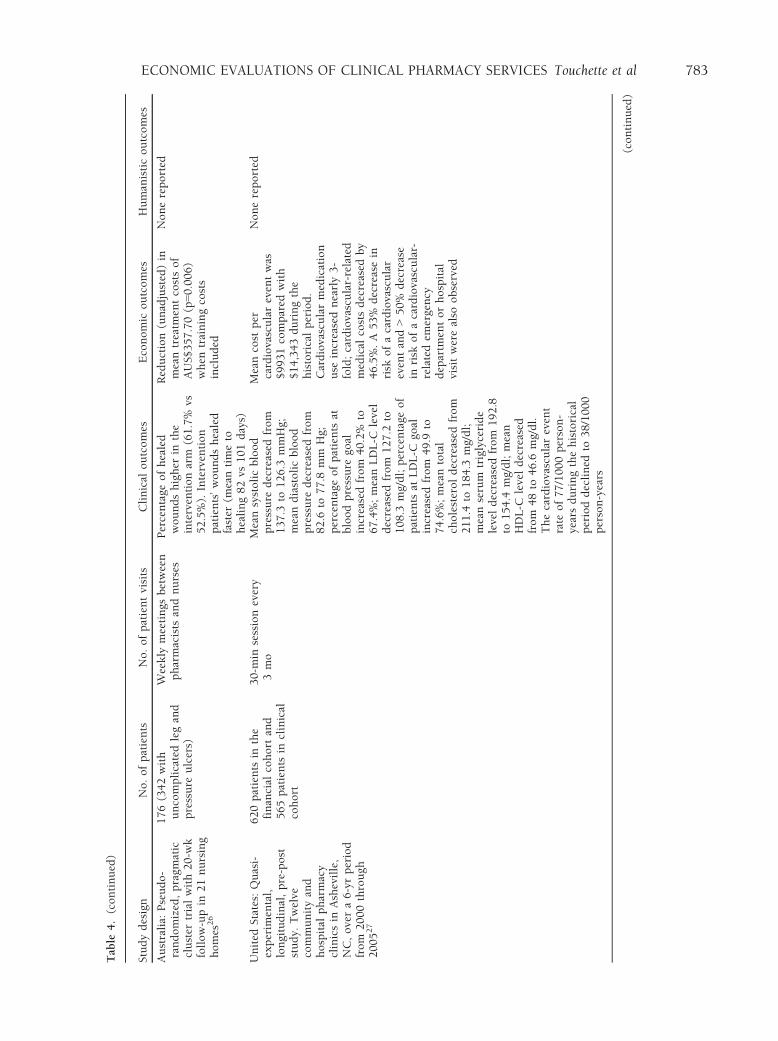
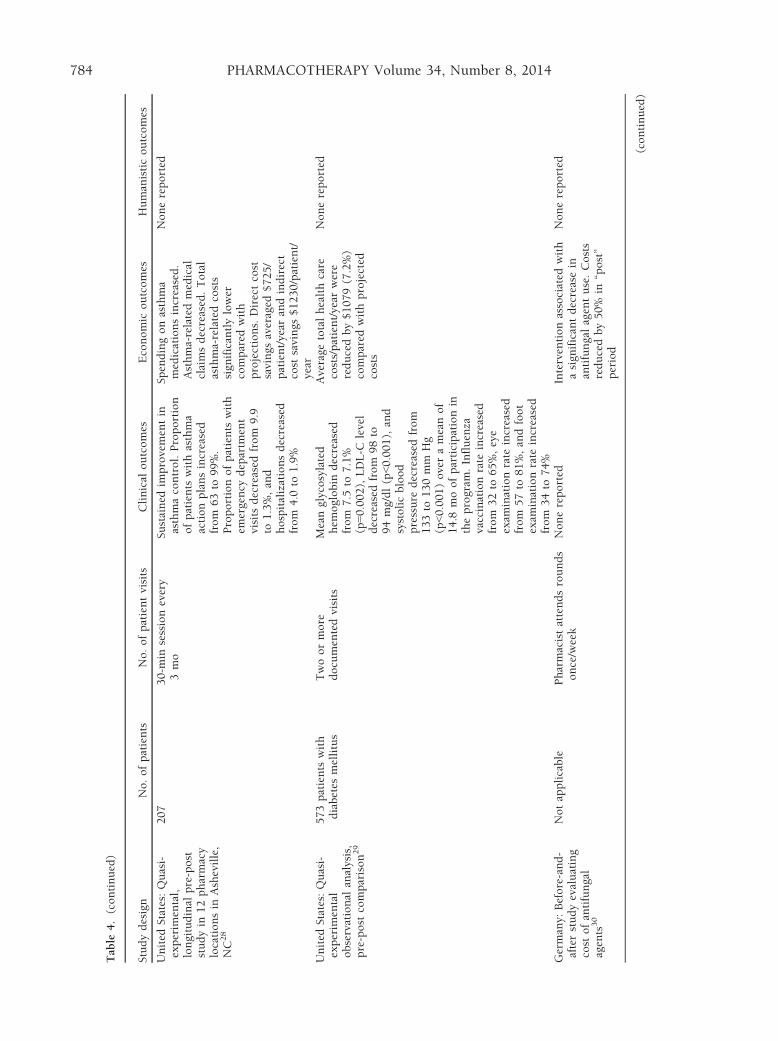
post study designs. The first study evaluated ahypertension and dyslipidemia clinical pharma-cist service provided at 12 community and hos-pital and pharmacy clinics in a cohort of 620patients.27 Mean blood pressure and low-densitylipoprotein-cholesterol (LDL-C), high-densitylipoprotein-cholesterol, and triglyceride levelswere improved, and the cardiovascular eventrate declined from 77 to 38 per 1000 person-years during the study period. A second study,in a similar program of 207 patients withasthma, found that objective and subjective mea-sures of asthma control were improved, andemergency and hospital visits decreased.28 Directand indirect costs were decreased by $725/patient/year and $1230/patient/year, respectively.The third involved 573 patients with diabetesmellitus from 10 employer sites.29 Glycosylatedhemoglobin, LDL-C level, and blood pressurewere improved at 12 months, and total health
Table 3. (continued)
Pharmacist training Pharmacist role Level of pharmacist autonomy
Canada: None described40 Patients were given the opportunity todiscuss questions regarding natural healthproducts. Pharmacists followed a stepwisecounseling approach on a telephonicfollow-up interview
Low. Pharmacists answeredpatient questions only
United States: Vaccination serviceimplemented by the pharmacyresident, resident preceptor, andthe residency program director19
The pharmacy resident conducted a chartreview on the day before the vaccinationservice to identify and screen for potentialcontraindications for vaccination amongthe participants based on Centers forDisease Control and Preventionrecommendations, such as documentedhypersensitivity to eggs or components ofthe influenza vaccine, documented currentacute febrile illness, or documented pastsevere adverse reactions to flu vaccination
Medium. Pharmacistsadministered vaccines
United States: Not described.Existing clinic41
The intensive care unit pharmacy staffevaluated creatinine clearance and patientmedication profiles daily. Pharmacistsrecommended medication dosing to themedical team in accordance withinstitutional guidelines
Medium. Pharmacists could makerecommendations to thephysician but not prescribe
United Kingdom: “Suitablytrained.” Qualification required,but not described42
Supplementary prescribing High. Does not require physicianoversight. Pharmacists haveprescriptive authority
United Kingdom: Hypotheticalservice43
The hypothetical service with “additionalpharmacists” was not described
Not described
GP = general practitioner; INR = international normalized ratio; NSAID = nonsteroidal antiinflammatory drug; OTC = over the counter.
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 781

Table
4.SummaryofStudiesofEconomic
EvaluationsofClinical
PharmacyServices
andTheirOutcomes
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
United
Kingd
om:Cost-
minim
izationanalysis
alongsidemulticenter,
randomized,controlled
trialwith12-m
ofollow-
up17,18
1480(980intervention
and500control)
Initialconsultationat
studystart,withfurther
consultationsbased
on
pharmacist-determined
need
Sign
ificantdifferenceswere
notfoundin
anyofthe
clinical
outcomes
includingappropriate
medicationsas
defined
by
theNational
Service
Framew
ork
andself-
reported
medication
compliance
TotalNHScost
increased
betweenbaselineand
follow-upin
both
groups
(from
£1243to
£1286
[3%]in
thecontrolgroup
andfrom
£1410to
£1433
[2%]in
theintervention
group).Cost
of
pharmaceuticals
was
higher
intheintervention
group(£769.20vs
£742.3,
p=0.04).Intervention
subject
costswerehigher,
controllingforbaseline
differences(p=0.001)
Satisfactionwithcare
was
higher
inintervention
subjects
United
States:
Randomized
prospective
controlled
trialwith12-m
ofollow-
up21
314heart
failure
patients
(122intervention)
9moofCPSwere
provided;number
of
visits
werenotprovided
Sign
ificantdifference
inadherence
of10.9%
favoringCPSat
9mo.
Nonsign
ificantdifference
of3.9%
favoringCPSat
12mo
19.4%
fewer
emergency
departm
entandhospital
admissions.Annual
direct
healthcare
costswere
$2960lower
inCPSgroup
Nonereported
Spain:Randomized
prospectiveopen
clinical
trialin
the
hospital
setting.
Enrolleeswerefollowed
upfor1yr2
2
134(70interventionand
64control)
3(follow-upvisits
were
perform
edat
2,6,and
12moafteradmission)
Compliance
was
betterin
interventionsubjects(85%
vs74%)at
1yr
Mortalityrate
higher
inthecontrolgroupat
12mo(30%
vs13%
inthe
interventiongroup,
p<0.05)
Interventionsubjectswere
readmittedless
frequently
(difference
=32%
at12mo).Controlsubjects
usedmore
hospital
resources
(mean9.6
vs5.9
hospital
daysper
person)
at12mo
Nosign
ificantdifferences
inqualityoflife.
Satisfactionwithcare
higher
inintervention
subjects
United
Kingd
om:
Randomized
controlled
trialwith12-m
ofollow-
up23
706anginapatients
(340
intervention)and1308
hyp
ertensive
patients
(656intervention)
Singlereview
ofpatient
medical
recordswithout
system
atic
follow-up
7.6%
improvementin
prescribingofantiplatelet
drugs.Few
ercardiovasculardisease–
relatedvisits
byangina
patients
Adjusted
costswerehigher
forinterventionsubjectsat
alltimepoints
Nonereported
United
Kingd
om:
Randomized
controlled
trialwith12mofollow-
up.Economic
evaluationonly
evaluated
pharmacist
interventions2
4,25
325in
threegroups.106
pharmacistintervention
subjectsevaluated
ineconomic
report
Meanof3.2
consultations
per
patientover12mo
Improvementin
3-m
opain
scoresbutnotat
6or
12mo
Totalmonthly
prescribing
cost
was
£575(m
ean£5
.42
per
person).Totalmonthly
cost
ofprescribingat
the
final
consultationwas
£480(m
ean£4
.53per
person)
Nonereported
(continued)
782 PHARMACOTHERAPY Volume 34, Number 8, 2014
Table
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
Australia:
Pseudo-
randomized,pragm
atic
cluster
trialwith20-w
kfollow-upin
21nursing
homes
26
176(342with
uncomplicatedlegand
pressure
ulcers)
Weekly
meetings
between
pharmacists
andnurses
Percentage
ofhealed
woundshigher
inthe
interventionarm
(61.7%
vs52.5%).Intervention
patients’woundshealed
faster
(meantimeto
healing82vs
101days)
Reduction(unadjusted)in
meantreatm
entcostsof
AUS$357.70(p=0.006)
when
trainingcosts
included
Nonereported
United
States:Quasi-
experim
ental,
longitudinal,pre-post
study.
Twelve
communityand
hospital
pharmacy
clinicsin
Asheville,
NC,overa6-yrperiod
from
2000through
200527
620patients
inthe
financial
cohort
and
565patients
inclinical
cohort
30-m
insessionevery
3mo
Meansystolicblood
pressure
decreased
from
137.3
to126.3
mmHg;
meandiastolicblood
pressure
decreased
from
82.6
to77.8
mm
Hg;
percentage
ofpatients
atbloodpressure
goal
increasedfrom
40.2%
to67.4%;meanLDL-C
level
decreased
from
127.2
to108.3
mg/dl;percentage
of
patients
atLDL-C
goal
increasedfrom
49.9
to74.6%;meantotal
cholesteroldecreased
from
211.4
to184.3
mg/dl;
meanserum
triglyceride
leveldecreased
from
192.8
to154.4
mg/dl;mean
HDL-C
leveldecreased
from
48to
46.6
mg/dl.
Thecardiovascularevent
rate
of77/1000person-
yearsduringthehistorical
perioddeclined
to38/1000
person-years
Meancost
per
cardiovasculareventwas
$9931compared
with
$14,343duringthe
historicalperiod.
Cardiovascularmedication
use
increasednearly3-
fold;cardiovascular-related
medical
costsdecreased
by
46.5%.A53%
decreasein
risk
ofacardiovascular
eventand>50%
decrease
inrisk
ofacardiovascular-
relatedem
ergency
departm
entorhospital
visitwerealso
observed
Nonereported
(continued)
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 783
Table
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
United
States:Quasi-
experim
ental,
longitudinal
pre-post
studyin
12pharmacy
locationsin
Asheville,
NC28
207
30-m
insessionevery
3mo
Sustained
improvementin
asthmacontrol.Proportion
ofpatients
withasthma
actionplansincreased
from
63to
99%.
Proportionofpatients
with
emergency
departm
ent
visits
decreased
from
9.9
to1.3%,and
hospitalizationsdecreased
from
4.0
to1.9%
Spendingonasthma
medicationsincreased.
Asthma-relatedmedical
claimsdecreased.Total
asthma-relatedcosts
sign
ificantlylower
compared
with
projections.Directcost
savings
averaged
$725/
patient/year
andindirect
cost
savings
$1230/patient/
year
Nonereported
United
States:Quasi-
experim
ental
observational
analysis,
pre-post
comparison29
573patients
with
diabetes
mellitus
Twoormore
documentedvisits
Meanglycosylated
hem
oglobin
decreased
from
7.5
to7.1%
(p=0.002),LDL-C
level
decreased
from
98to
94mg/dl(p<0.001),and
systolicblood
pressure
decreased
from
133to
130mm
Hg
(p<0.001)overameanof
14.8
moofparticipationin
theprogram
.Influenza
vaccinationrate
increased
from
32to
65%,eye
exam
inationrate
increased
from
57to
81%,andfoot
exam
inationrate
increased
from
34to
74%
Average
totalhealthcare
costs/patient/year
were
reducedby$1079(7.2%)
compared
withprojected
costs
Nonereported
Germany:
Before-and-
afterstudyevaluating
cost
ofantifungal
agents30
Notapplicable
Pharmacistattendsrounds
once/week
Nonereported
Interventionassociated
with
asign
ificantdecreasein
antifungalagentuse.Costs
reducedby50%
in“post”
period
Nonereported
(continued)
784 PHARMACOTHERAPY Volume 34, Number 8, 2014
Table
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
United
States:Patients
admittedto
neurosurgical
service
2yrsbefore
and2yrs
afterCPS
implementation31
2156(1079post-
implementation)
Daily
monitoringby
pharmacist
Average
hospital
stay
decreased
from
8.56to
7.24days(p=0.003).Early
hospital
mortality
decreased
from
3.34to
1.95%
(p=0.06).
Sign
ificantlylower
postim
plementation
readmissionrate
(p=0.05)
Average
pharmacyand
intravenoustherapycost/
patientdecreased
from
pre-to
post-
implementation(from
$4833to
$3239)
Nonereported
United
States:
Prospective
controlled
studyin
twointernal
medicinepractices
over
1yr
32
243(127intervention)
Singlemedical
record
review
,although
pharmacistavailable
for
physicianquestions
Between-groupdifference
inthechange
inERvisits
per
1000patients
approached
statisticalsign
ificance
(p=0.054).CPSgroup
patients
more
likelyto
havemedication
nonadherence,untreated
indication,andmedication
choiceissues
addressed
Change
inmeanper
patient
per
year
medical
(excludingpharmacy)
cost
did
notdiffersign
ificantly
betweenthegroups
(p=0.711)
Nonereported
United
Kingd
om:
Pragm
atic,randomized,
controlled
trialwith6-
mofollow-up33
855patients
(415
intervention)
Pharmacists
werepaidfor
twohomevisits
Statisticallysign
ificant
increase
inem
ergency
readmissionsand
nonsign
ificantreductionin
deathsin
theCPSgroup
Average
cost
per
interventiongrouppatient
was
£1695compared
with
£1424forcontrolpatients
Gainof0.0075QALY
withCPSin
698patients
forwhom
QALYdata
wereavailable.
Increm
entalcost
per
QALYgained
inthe
interventionwas
£54,454
Switzerland:Prospective,
observational
studyin
atertiary
700-bed
university
hospital
settingover32wks3
4
1444patients
CPSconducted
for70of
224days
213pharmaceutical
interventionsrecorded
51interventions(24%)
considered
tobedirectly
cost
savingwithout
affectingcare
withamean
per
personsavingof
€10.11(extrapolatedto
€1158forayear).Cost-
relevantinterventions
estimated
toequal
€10,731
incost
avoidance,not
countingtheeffect
on
lengthofstay,adverse
drugeventrate
and
possible
litigationcosts
Nonereported
(continued)
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 785

Table
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
United
States:
Randomized
multiple
interruptedtime-series
designanalysis
of
pharmaceuticalcare
at2-m
ointervals.
Modeled
cost-utility
analysis35
Of760subjects
recruited,673reached
baselineand563had
medicationreviewed
Meanof8.3
review
sper
person
Reductionin
U.K.-MAI
score
overtime.
Reduction
innumber
ofdrugs
over
time
Onaverage,
pharmaceutical
care
costsan
estimated
£192/yrmore
than
usual
care
butyieldsslightly
greaterbenefits,nam
ely
0.019ofaQALY.
Increm
entalcost-
effectivenessratio
estimated
at~£
10,000/
QALYgained
Nonereported
United
States:
Retrospectivecontrolled
analysis36
339(163intervention)
Oneortw
ovisits
per
weekbyteam
ofgeriatric
doctor,nurse
practitioner,andgeriatric
pharmacist.Onemem
ber
ofteam
isonsite
5days/
wk
Nonereported
Sign
ificantlyshorter
lengths
ofstay
(unadjusted
difference
=6.5
days),
fewer
patientdays,and
lower
totalcharges
(unadjusted
difference
=$2297)
Nonereported
Switzerland:Ten
possible
interventions
weremodeled
fortheir
estimated
potential
impactonfailures3
7
Notapplicable
Notapplicable
Gainsin
qualis
(1quali=reductionofthe
criticalityindex
byone
point)
of1292forready-
to-use
syringes,1201by
employingclinical
pharmacists,and996from
double
checksbynurses
werepredicted
Cost–efficacyratiosof€0.54
per
qualigained
by
employingclinical
pharmacists,€0.71per
qualigained
from
double
checksbynurses,and
€0.72per
qualigained
for
ready-to-use
syringeswere
predicted
Nonereported
Canada:
Randomized
controlled
open
pragmatic
clinical
trial38
250(128intervention)
Asfrequentas
necessary
bytelephone.
Mean
follow-upwas
14.9
wks
inPMAS
Nodifference
intimein
therapeuticrange.PMAS
patients
weremore
frequently
supratherapeutic
(INR≥5).Fam
ily
physicianvisits
per
patient
year
werelower
inPMAS
patients
MaintainingPMAScost
was
~$123.80per
patientfor
firstyear.Fam
ilyphysician
visits
per
patientyear
were
lower
(difference
=0.4
visits
per
year)in
PMAS
patients
Nodifference
inQOL
outcomes
observed
(SF-
12andEuroQOLEQ-
5D)
(continued)
786 PHARMACOTHERAPY Volume 34, Number 8, 2014
Table
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
Denmark:Comparative,
prospective,crossover
designinvolvingtw
oparallelgroups3
9
2500(1452clinical
pharmacypatients
screened);8362control
and9654CPS
prescriptionsscreened
Patientmedical
records
screened
once
weekly
Sign
ificantreductionin
number
ofdaysfrom
10–5
withasuboptimal
prescription
Thecost
ofpracticing
clinical
pharmacyservice
was
€7360.Estim
ated
directcost
savings
(medicineandnursing
time)
forfourofseven
interventionareasof
program
was
€3442
Nonereported
Canada:
Before-and-after
study.
Subjects
recruited
over8mo
periodfor“before”
phaseand11mofor
“after”phase4
0
265(123intervention)
Singlevisit
Nonereported
Increasedcounselingtime
from
ameanof9–1
8min.
Meanadditional
cost
of
CDN$7.49per
patient
Increasedpatient
satisfactionwithroutine
counselingonnatural
healthproducts
United
States:
Retrospective
descriptive
report19
58
Two2-hrvaccination
sessions
Immunizationrate
increasedfrom
64%
inthe
previousyear
to83%
with
CPS
Net
incomeof$13per
vaccinationwas
realized
aftermakingadjustments
forcosts
Patients
andstaffwere
highly
satisfiedwiththe
service
United
States:Single-
groupretrospective
analysis
ofarenal
dosingprogram
inthe
pediatric
cardiacIC
U41
131patients
with140
admissions
Daily
Pharmacist
recommendationswere
responsible
for96%
of
medicationadjustments
for
renal
dysfunction
CPSestimated
toresultin
~$12,000in
dosessaved
Nonereported
United
States:
Retrospectivedata
analysis
toexam
ine
volume,
cost,and
trendsofpharmacist
prescribing42
Totalnumber
of
pharmacist
prescriptionswere2706
in2004and11,458in
2005
Notapplicable
Nonereported
323%
increase
inthe
number
ofitem
sprescribed
between2004
and2005and170%
increase
inthenumber
prescribed
between2005
and2006.Net
ingredient
cost
ofitem
sprescribed
by
pharmacists
increasedfrom
£25,348in
2004to
£278,634in
2006
Nonereported
(continued)
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 787

care costs were reduced by $1080 comparedwith projected costs but were increased by $698compared with baseline.Two studies used before-and-after study
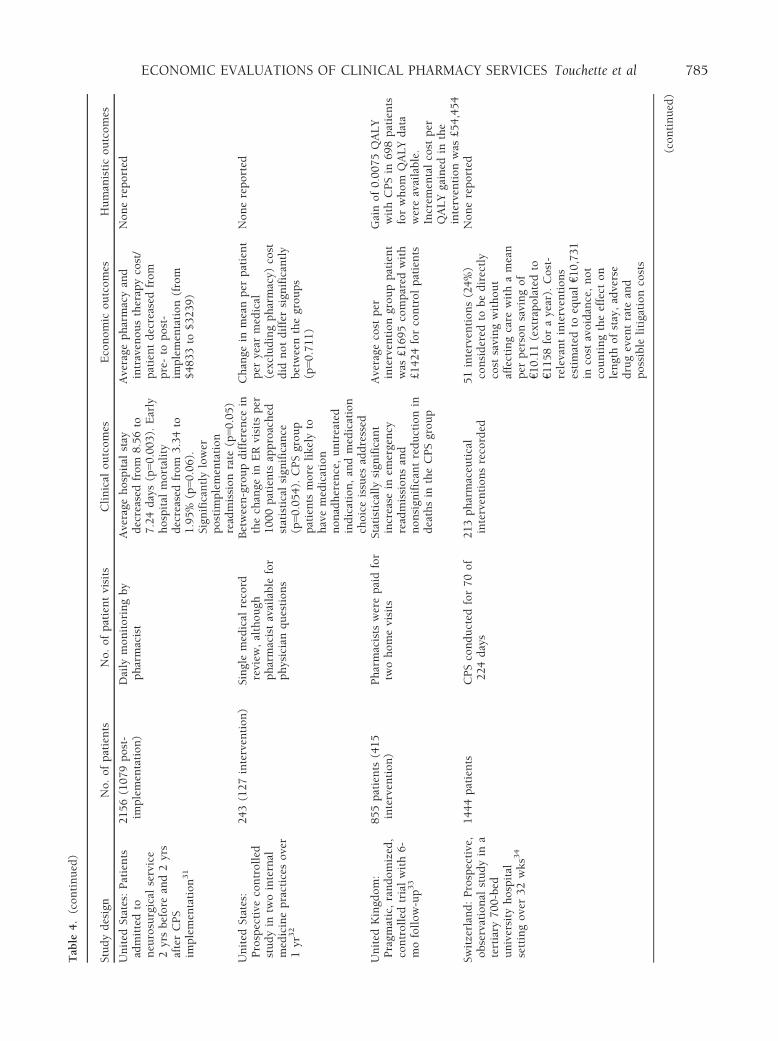
designs. The first evaluated the implementationof practice guidelines for the treatment of fungalinfections enforced by a clinical pharmacist inan unspecified number of patients.30 The clinicalpharmacist service was associated with anapproximate reduction in the cost of antifungalagents of over 50%. The second evaluated 2156neurology patients (1079 of whom received theclinical pharmacist-managed program) and11,250 clinical pharmacist interventions.31 Aver-age hospital stay, mortality, and pharmacy andintravenous therapy costs decreased by 1.3 days,1.4%, and $1594, respectively, after programimplementation.
General Pharmacotherapeutic Monitoring
Six studies were classified as having providedgeneral pharmacotherapeutic monitoring. Twoof these studies used a prospective randomizedtrial design. The first evaluated 243 adultpatients, 127 of whom received medication ther-apy optimization by a clinical pharmacist, fromtwo internal medicine practices.32 Interventiongroup patients were more likely to have medica-tion nonadherence, untreated conditions, subop-timal medication choice, and cost issuesaddressed. Medical care costs were not signifi-cantly different between groups. The secondevaluated the impact of pharmacist home visitsafter hospital discharge in 872 subjects (437 ofwhom received the intervention).33 A statisti-cally significant increase in emergency readmis-sions occurred in the intervention group, alongwith a nonsignificant reduction in deaths. Theaverage calculated difference in total cost of carewas £407 per person favoring the control group,whereas a difference of 0.0075 quality-adjustedlife-year (QALY) favored the intervention, result-ing in an incremental cost-effectiveness ratio(ICER) of £54,454 per QALY gained.Another group conducted a prospective obser-
vational study assessing clinical pharmacistinterventions on two wards of a single tertiaryhospital involving 1444 patients.34 In all, 148interventions concerning drug therapy weremade, with 83% adopted by physicians, 6%rejected, and 11% with unknown outcomes. Ofthese, 51 interventions were considered to becost saving, with an estimated 1-year cost avoid-ance of €10,731.T
able
4.(continued)
Studydesign
No.ofpatients
No.ofpatientvisits
Clinical
outcomes
Economic
outcomes
Humanisticoutcomes
United
Kingd
om:Model
comparingthree
hyp
othetical
program
sto
reduce
medication
errors
inhospitals4
3
Notapplicable
Notapplicable
Nonereported
Predictedmeanmonetary
CPScost
£0.21–
0.37millionandresulted
inanet
benefitof
£27.25millionovera5-yr
timehorizon.By
comparison,computerized
physicianorder
entryand
bar
codingprescriptions
resulted
inanet
benefitof
£31.5
and£1
3.1
million,
respectively
Nonereported
CPS=clinical
pharmacyservices;EuroQOLEQ-5D
=five-dim
ensionquality-of-life
scaledeveloped
bytheEuroQOLGroup;HDL-C
=high-density
lipoprotein-cholesterol;IN
R=international
norm
alized
ratio;LDL-C
=low-density
lipoprotein-cholesterol;
NHS=National
Health
Service;
PMAS=pharmacist-managed
anticoagulation
services;QALY=quality-adjusted
life-year;
SF-
12=12-Item
Short
Form
Survey;U.K.-MAI=medicationappropriatenessindex
adaptedforuse
intheUnited
Kingd
om.
788 PHARMACOTHERAPY Volume 34, Number 8, 2014

A group of researchers conducted a random-ized multiple interrupted time-series study eval-uating pharmaceutical care in 760 subjects.35
The number of drugs used declined over time,with a corresponding increase in costs (£192)and QALYs (0.019) and a calculated ICER of ~£10,000/QALY gained. A second group con-ducted a retrospective controlled analysis of aninterprofessional team including a pharmacist in339 transitional care patients.36 The care teampatients had significantly shorter lengths of stay,fewer patient days, and lower total charges.Finally, a third group conducted a modelingstudy evaluating therapy failures and the critical-ity of those failures by the hypothetical additionof a pharmacist compared with nine otherpotential interventions.37 Employment of a clini-cal pharmacist was expected to result in 1201additional qualis (1 quali was defined as areduction of the criticality index by 1 point),second only to the use of ready-to-use syringes.The best cost-efficacy ratios were obtained foradding a clinical pharmacist (1 quali = 0.54 eu-ros), followed by double-checking medicationsby nurses (1 quali = 0.71 euros) and ready-to-use syringes (1 quali = 0.72 euros).
Target Drug Programs
Two studies evaluated target drug programs.The first conducted a randomized controlledopen pragmatic clinical trial involving 250 sub-jects, 128 of whom received pharmacist-man-aged anticoagulation services.38 No significantdifferences were observed in time in therapeuticinternational normalized ratio (INR) range orquality of life. First-year service costs were$123.80 per patient, and the number of familyphysician visits was reduced. The second evalu-ated 2500 subjects (1452 of whom received theCPS) and 18,016 prescriptions (9654 of whichwere prescriptions for patients receiving theCPS) in four orthopedic surgical wards in twohospitals using a modified prospective crossoverdesign.39 A significant reduction in the numberof days with a suboptimal prescription (differ-ence = 5 days) was observed in patients receiv-ing the pharmacist service. Although servicecosts were €7360, the program was estimated tosave €3442.
Patient Education Programs
A before-and-after study evaluated the impactof routine structured counseling on natural
health products in 265 patients visiting the phar-macy of a comprehensive cancer center.40
Patients were provided the opportunity to askquestions about natural health products, andpharmacists followed up with patients in a tele-phonic interview. The program increased patientsatisfaction with routine natural health productcounseling at an additional cost of $7.49 (Cana-dian dollars) per patient.
Wellness Program or Immunization Service
Another group conducted a retrospectivedescriptive evaluation of a screening initiative toidentify potential vaccine recipients in a seniorhousing complex.19 The immunization rateimproved from 64–83%, with a net income of$4.55 per vaccination provided.
Other Services
Three studies evaluated programs that couldnot be grouped into one of the previouslydescribed classifications. The first retrospectivelyevaluated 140 admissions from 131 pediatriccardiac surgery patients at risk for renal insuffi-ciency by using a noncontrolled posttestdesign.41 Pharmacists made 74 renal dosingadjustments at an estimated drug cost savings of$12,482.54. The second evaluated the volume,patterns, and costs associated with pharmacistprescribing in England in a noncontrolled post-test design study.42 Prescription costs increased10-fold from 2004 to 2006; the clinical impactof this increased prescribing by pharmacists wasnot evaluated. The third, by using a decisionmodel, evaluated the impact of hypotheticalpharmacist participation on ward rounds toreduce adverse drug events.43 In this model,when monetary valuations of the health impactof preventable adverse drug events wereincluded, ward pharmacists were anticipated tocost £0.21–0.37 million and result in ~£27 mil-lion in net benefits over a 5-year timeline.
Economic Analysis Quality
Included costs were well described (i.e., allimportant and relevant costs were identified) in13 of 25 studies (52%). Clinical or humanisticoutcomes were evaluated in 20 of 25 studies(80%) and were well described in 18 of 25 stud-ies (72%). Studies were considered full eco-nomic evaluations in 18 of 25 cases (72%).Objectives were considered clearly presented in
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 789

22 of 25 studies (88%), whereas perspectiveswere presented in 9 of 25 (36%). Uncertaintywas adequately addressed in 12 of 25 studies(48%). Incremental analysis was conducted in 7of 25 studies (28%). Methodologies for dataabstraction were stated in 17 of 25 studies(68%) and time horizons were stated in 9 of 25studies (36%). Study assumptions and limita-tions were stated and justified in 8 of 25 studies(32%) studies, whereas biases were adequatelydiscussed in 9 of 25 studies (36%). Conclusionsand recommendations were considered justifiedand based on results in 24 of 25 studies (96%).The funding source was disclosed in 17 of 25studies (68%). A Quality of Health EconomicStudies (QHES) score was calculated for the 18full economic analyses evaluated in our review.The mean � SD QHES score was 60.4 � 22.3 ofa possible 100 points (more than 75 points indi-cates high quality).
Benefit-Cost and Incremental Cost-EffectivenessRatios
Benefit-cost (B:C) ratio or ICER could becalculated for eight of the studies. B:C ratioswere not reported directly in any of the stud-ies, but they could be calculated in three stud-ies and ranged from 1.05:1–25.95:1. Althoughmany studies did not report benefits in mone-tary terms, five studies did sufficiently reporteffectiveness or utility so that an ICER couldbe calculated. The ICERs and their denomina-tors’ unit of measurement are reported inTable 5.
Discussion
This article is a continuation of a series of sys-tematic reviews of the economic value of clinical
pharmacist services.2–4 With the exception of amore exhaustive search strategy by including theEmbase and CINAHL databases and an increasedreporting of the nature and clinical outcomes ofthe CPS, our methods have remained consistent.In this latest analysis, the proportion of studieswith full pharmacoeconomic evaluationsincreased from 48% during 2001–2005 to 72%in this review (2006–2010). In addition, thequality of published studies improved. Forexample, in the last review, 37% of all studieswere purely descriptive,2 with 16% descriptivein the current review. In this review, studies fre-quently had a comparison group (84% of stud-ies), a vast improvement over our previousarticle in which only 43% of studies used a com-parison group. Among the full economic analy-ses, studies scored 60.4 points on the QHESscale for study quality. These results are similarto the QHES results of 30 economic analyses ofcare strategies for gastroesophageal reflux dis-ease (mean � SD score: 63.6 � 14.7) identifiedin another systematic review.16
Despite the improvement in study quality, thetotal number of full and partial economic evalu-ations decreased compared with previous peri-ods (104 articles during 1988–1995, 59 during1996–2000, 93 during 2001–2005,2–4 and 25during 2006–2010). Given our more comprehen-sive search strategy for the current period, thedecline in the number of articles is real, but thereasons for this overall decline are unclear. Thedecline may be due to any or all of the following:decline in research funding or in the number ofstudies funded evaluating CPS; changes in journalreview or publication patterns, requiring a higherstandard for publishing economic analyses; fewer“novel” clinical pharmacist services being initiated;or a perception that the justification of clinicalpharmacist services is no longer necessary. The
Table 5. Studies Evaluating Clinical Pharmacy Services with Calculable Benefit-Cost or Incremental Cost-EffectivenessRatiosa
Benefit-cost ratio ICER ICER denominator Reported by authors or calculated
1.05:1 Calculated22
15.4:1 Calculated21
14.73–25.95:1 Calculated43
Dominant Wound prevented Calculated39
CDN $8.33 VC Reported40
€0.54 Quali Reported37
£10,000 QALY Reported35
£54,454 QALY Reported33
ICER = incremental cost-effectiveness ratio; QALY=quality-adjusted life-years gained; Quali = reduction of the criticality index by 1 point;VC = satisfaction with complementary therapies subscale score.aSeven studies were considered partial economic evaluations. Benefit-cost or cost-effectiveness ratios could not be calculated for 10 full eco-nomic evaluations.
790 PHARMACOTHERAPY Volume 34, Number 8, 2014

dramatic decline in economic evaluations of CPSin the United States was particularly surprising,given recent policy changes that allowed for thepayment of certain CPS.8, 44
Shifts in the type of journal published alsooccurred compared with the previous analysis.In this review, studies were published in 18 dif-ferent journals; the most common was the Jour-nal of the American Pharmacists Association (16%of studies). In the previous systematic reviews,articles were commonly published in the Ameri-can Journal of Health-System Pharmacy and Phar-macotherapy, but no publications were includedin these journals from 2006 to 2010. A higherproportion of studies were published in non-pharmacy journals (52%) compared with 26.9%in the systematic review covering 2001–2005.In most cases, CPS were either considered
cost-effective or had a favorable B:C ratio. Whencalculable, the B:C ratio ranged from 1.05:1 to25.95:1. However, notable exceptions were threelarge prospective multicenter studies conductedin the United Kingdom that showed no or mini-mal benefits in clinical outcomes and an addedcost with community-based CPS.17, 18, 33
As anticipated, we observed a continued shiftfrom CPS addressing targeted drug therapy andpharmacokinetic monitoring services to thoseaddressing general pharmacotherapy and diseasestate management. Compared with the previousreviews in this series, there was also a continuedshift from inpatient hospital-based services tooutpatient clinic- or community-based services.For the first time since we began this review,comprehensive economic evaluations were pri-marily conducted in countries outside the Uni-ted States and were often conducted at anational or regional level, involved multiplesites, and were more frequently conducted innonacademic community settings. This repre-sents a dramatic shift from previous reviews,where the vast majority of studies were con-ducted in U.S. academic hospital settings.2–4
This shift may also reflect a change in the man-agement of patients from the inpatient to theoutpatient setting and an increased focus onoptimizing medication use in patients withchronic conditions.45
Surprisingly, there were still few full economicevaluations of MTM services. Only two of theprograms were identified as MTM,27, 28 althoughseveral others met criteria for being consideredMTM.20 Neither of the MTM studies included aconcurrent control group. Without evidencesupporting the effects and value of MTM,
support for these programs by insurers maywane. Furthermore, the expansion of MTM ser-vices from targeted interventions without follow-up to more comprehensive services is unlikelyto occur in the absence of evidence supportingmore comprehensive programs.There were no studies published that evalu-
ated clinical pharmacist services in a medicalhome. Given the time frame of this review rela-tive to the introduction of the Patient Protectionand Affordable Care Act of 2010,44 this findingwas not surprising. However, we were anticipat-ing some published studies supporting the inclu-sion of clinical pharmacists in care teams,conducted in a setting similar to a medicalhome. This is likely to be a fruitful area forresearch in the near future.For the first time since we began publishing
this series, we saw more studies conducted incountries other than the United States. In particu-lar, 8 of 25 studies were conducted by investiga-tors primarily based in the United Kingdom, andthese studies accounted for five of the eight ran-domized controlled trials included in ourreview.17, 18, 23, 25, 33 All five studies receivedfederal funding from the U.K. government. Incontrast, five European studies, conducted inSwitzerland,34, 37 Spain,22 Germany,30 and Den-mark,39 included just one randomized controlledtrial22 and two studies of quasi-experimentaldesign.30, 39 Funding was acknowledged for justtwo of the studies and were from nonfederalsources.22, 39 Of the nine U.S. studies, just onewas a randomized controlled trial,21 and threeused quasi-experimental designs.27, 28, 32 The ran-domized controlled trial was the only federallyfunded study,21 three were cofunded by industryand/or professional pharmacy organizations,27, 28, 32
one was funded by an internal academic grant,36
and four were not funded.19, 31, 32, 41 From thesedata, there appears to be a strong associationbetween high-quality trial designs and competi-tive adequately funded federal funding opportu-nities. Also notable is the lack of publishedeconomic evaluations of CPS receiving federalfunding outside the United Kingdom.Important limitations of this systematic review
must be outlined. Although a comprehensivesearch strategy was used, it is possible that notall CPS economic evaluations were identified. Apublication bias may also be present. In addi-tion, due to the decrease in the number of pub-lished studies, we were unable to provide apooled B:C ratio estimate as we did in our previ-ous reviews.
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 791
Conclusion
A higher proportion of economic evaluationsof CPS used controlled designs and better meth-odologies, although overall fewer studies werepublished during the 2006–2010 period. Evalua-tions of ambulatory practices were increasinglycommon. In general, CPS were cost-effective orprovided a good B:C ratio. However, variabilityexists in both clinical outcomes achieved andthe subsequent cost-effectiveness of CPS. Futurestudies should focus on identifying specificaspects of CPS that contribute to improved clini-cal outcomes and efficiency.
References
1. Chisholm-Burns MA, Graff Zivin JS, Lee JK, et al. Economiceffects of pharmacists on health outcomes in the United States:a systematic review. Am J Health Syst Pharm 2010;67:1624–34.
2. Perez A, Doloresco F, Hoffman JM, et al. ACCP: economicevaluations of clinical pharmacy services: 2001–2005. Pharma-cotherapy 2009;29:128.
3. Schumock GT, Butler MG, Meek PD, Vermeulen LC, Aronde-kar BV, Bauman JL. Evidence of the economic benefit of clini-cal pharmacy services: 1996–2000. Pharmacotherapy2003;23:113–32.
4. Schumock GT, Meek PD, Ploetz PA, Vermeulen LC. Eco-nomic evaluations of clinical pharmacy services—1988–1995.The Publications Committee of the American College of Clini-cal Pharmacy. Pharmacotherapy 1996;16:1188–208.
5. Burke JM, Miller WA, Spencer AP, et al. Clinical pharmacistcompetencies. Pharmacotherapy 2008;28:806–15.
6. The definition of clinical pharmacy. Pharmacotherapy2008;28:816–7.
7. Ramalho de Oliveira D, Brummel AR, Miller DB. Medicationtherapy management: 10 years of experience in a large inte-grated health care system. J Manag Care Pharm 2010;16:185–95.
8. Anonymous. Public law 108–173. The Medicare prescriptiondrug, improvement, and modernization act of 2003. HR1.December 8, 2003. Available from http://www.cms.gov/CCIP/downloads/section_721.pdf. Accessed June 12, 2010.
9. The Publications Committee of the American Hospital Associ-ation. Patient-centered medical home: AHA research synthesisreport. 2010:2–21. Available from http://www.aha.org/research/cor/content/patient-centered-medical-home.pdf. Accessed July12, 2013.
10. Rucker NL. Medicare Part D’s medication therapy manage-ment shifting from neutral to drive. AARP. 2012:1–12. Avail-able from http://www.aarp.org/content/dam/aarp/research/public_policy_institute/health/medicare-part-d-shifting-from-neu-tral-to-drive-insight-AARP-ppi-health.pdf. Accessed June 27,2012.
11. Willett MS, Bertch KE, Rich DS, Ereshefsky L. Prospectus onthe economic value of clinical pharmacy services. A positionstatement of the American College of Clinical Pharmacy. Phar-macotherapy 1989;9:45–56.
12. Schumock GT, Pickard AS. Comparative effectivenessresearch: relevance and applications to pharmacy. Am J HealthSyst Pharm 2009;66:1278–86.
13. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US phar-macists’ effect as team members on patient care: systematicreview and meta-analyses. Med Care 2010;48:923–33.
14. Buscemi N, Hartling L, Vandermeer B, Tjosvold L, KlassenTP. Single data extraction generated more errors than doubledata extraction in systematic reviews. J Clin Epidemiol2006;59:697–703.
15. Drummond MF. Methods for the economic evaluation ofhealth care programmes, 3rd ed. New York, NY: Oxford Uni-versity Press; 2005.
16. Ofman JJ, Sullivan SD, Neumann PJ, et al. Examining thevalue and quality of health economic analyses: implications ofutilizing the QHES. J Manag Care Pharm 2003;9:53–61.
17. Scott A, Tinelli M, Bond C. Costs of a community pharma-cist-led medicines management service for patients with coro-nary heart disease in England: healthcare system and patientperspectives. Pharmacoeconomics 2007;25:397–411.
18. The Community Pharmacy Medicines Management ProjectEvaluation Team. The MEDMAN study: a randomized con-trolled trial of community pharmacy-led medicines manage-ment for patients with coronary heart disease. Fam Pract2007;24:189–200.
19. Lam AY, Chung Y. Establishing an on-site influenza vaccina-tion service in an assisted-living facility. J Am Pharm Assoc(2003) 2008;48:758–63.
20. American Pharmacists Association; National Association ofChain Drug Stores Foundation. Medication therapy manage-ment in community pharmacy practice: core elements of anMTM service (version 1.0). J Am Pharm Assoc (2003)2005;45:573–9.
21. Murray MD, Young J, Hoke S, et al. Pharmacist interventionto improve medication adherence in heart failure: a random-ized trial. Ann Intern Med 2007;146:714–25.
22. Lopez Cabezas C, Falces Salvador C, Cubi Quadrada D, et al.Randomized clinical trial of a postdischarge pharmaceuticalcare program vs regular follow-up in patients with heart fail-ure. Farm Hosp 2006;30:328–42.
23. Bond CM, Fish A, Porteous TH, Reid JP, Scott A, AntonazzoE. A randomised controlled trial of the effects of note-basedmedication review by community pharmacists on prescribingof cardiovascular drugs in general practice. Int J Pharm Pract2007;15:39–46.
24. Hay EM, Foster NE, Thomas E, et al. Effectiveness of commu-nity physiotherapy and enhanced pharmacy review for kneepain in people aged over 55 presenting to primary care: prag-matic randomised trial. BMJ 2006;333:995.
25. Phelan M, Blenkinsopp A, Foster NE, Thomas E, Hay EM.Pharmacist-led medication review for knee pain in olderadults: content, process and outcomes. Int J Pharm Pract2008;16:347–88.
26. Vu T, Harris A, Duncan G, Sussman G. Cost–effectivenessof multidisciplinary wound care in nursing homes: a pseudo-randomized pragmatic cluster trial. Fam Pract 2007;24:372–9.
27. Bunting BA, Smith BH, Sutherland SE. The Asheville Project:clinical and economic outcomes of a community-based long-term medication therapy management program for hyperten-sion and dyslipidemia. J Am Pharm Assoc (2003) 2008;48:23–31.
28. Bunting BA, Cranor CW. The Asheville Project: long-termclinical, humanistic, and economic outcomes of a community-based medication therapy management program for asthma. JAm Pharm Assoc (2003) 2006;46:133–47.
29. Fera T, Bluml BM, Ellis WM. Diabetes Ten City Challenge:final economic and clinical results. J Am Pharm Assoc (2003)2009;49:383–91.
30. Swoboda S, Lichtenstern C, Ober MC, et al. Implementationof practice guidelines for antifungal therapy in a surgicalintensive care unit and its impact on use and costs. Chemo-therapy 2009;55:418–24.
31. Weant KA, Armitstead JA, Ladha AM, Sasaki-Adams D, Ha-dar EJ, Ewend MG. Cost effectiveness of a clinical pharmaciston a neurosurgical team. Neurosurgery 2009;65:946–50; dis-cussion 50–1.
32. Altavela JL, Jones MK, Ritter M. A prospective trial of a clini-cal pharmacy intervention in a primary care practice in a capi-tated payment system. J Manag Care Pharm 2008;14:831–43.
33. Pacini M, Smith RD, Wilson EC, Holland R. Home-basedmedication review in older people: is it cost effective? Pharma-coeconomics 2007;25:171–80.
792 PHARMACOTHERAPY Volume 34, Number 8, 2014

34. Lampert ML, Kraehenbuehl S, Hug BL. Drug-related prob-lems: evaluation of a classification system in the daily practiceof a Swiss University Hospital. Pharm World Sci 2008;30:768–76.
35. RESPECT Trial Team. Cost-effectiveness of shared pharma-ceutical care for older patients: RESPECT trial findings. Br JGen Pract 2010;60:e20–7.
36. Blewett LA, Johnson K, McCarthy T, Lackner T, Brandt B.Improving geriatric transitional care through inter-professionalcare teams. J Eval Clin Pract 2010;16:57–63.
37. De Giorgi I, Fonzo-Christe C, Cingria L, et al. Risk and phar-macoeconomic analyses of the injectable medication process inthe paediatric and neonatal intensive care units. Int J QualHealth Care 2010;22:170–8.
38. Lalonde L, Martineau J, Blais N, et al. Is long-term pharma-cist-managed anticoagulation service efficient? A pragmaticrandomized controlled trial. Am Heart J 2008;156:148–54.
39. Buck TC, Brandstrup L, Brandslund I, Kampmann JP. Theeffects of introducing a clinical pharmacist on orthopaedicwards in Denmark. Pharm World Sci 2007;29:12–8.
40. Malfair Taylor SC, de Lemos ML, Jang D, et al. Impact onpatient satisfaction with a structured counselling approach onnatural health products. J Oncol Pharm Pract 2008;14:37–43.
41. Moffett BS, Mott AR, Nelson DP, Gurwitch KD. Medicationdosing and renal insufficiency in a pediatric cardiac intensivecare unit: impact of pharmacist consultation. Pediatr Cardiol2008;29:744–8.
42. Guillaume L, Cooper R, Avery A, et al. Supplementary pre-scribing by community and primary care pharmacists: an analy-sis of PACT data, 2004–2006. J Clin Pharm Ther 2008;33:11–6.
43. Karnon J, McIntosh A, Dean J, et al. Modelling the expectednet benefits of interventions to reduce the burden of medica-tion errors. J Health Serv Res Policy 2008;13:85–91.
44. Anonymous. Public law 111–148. Compilation of patient pro-tection and affordable care act. May 1, 2010. Available fromhttp://housedocs.house.gov/energycommerce/ppacacon.pdf.Accessed July 12, 2013.
45. Sibbald B, McDonald R, Roland M. Shifting care from hospi-tals to the community: a review of the evidence on quality andefficiency. J Health Serv Res Policy 2007;12:110–7.
ECONOMIC EVALUATIONS OF CLINICAL PHARMACY SERVICES Touchette et al 793