eclectic medicine part 2
TRANSCRIPT

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 1/107
PART II.
DISEASES OF THE RE SP IRATORY SYSTEM.
I . DISEASES OF THE NOSE.
ACUTE RH INITIS.
S y n o n y m s .—Acut e Nasal Cat ar rh ; Acut e Coryza; Cold in t he H ead .
Def in i t ion .—An acute catarrhal inflammation of the Schneiderianmembrane, resulting in more or less obstruction of the nasal passages,an d a tt ended by a serous or sero-mu cous secretion.
Et i o l o g y .—Among th e predisposing cau ses m ay be m ent ioned a ge, th edisease being more common in early life, especially in children, whilethe aged are comparatively immune. Hypertrophy of the mucousmembrane, with narrowing of the passages, polypi, and adenoids,favors t he disease.
The most common exciting cause is exposure to draughts of air andsudden atmospheric changes, so common during the early winter andspring months. The chilling of the body by wet feet during inclementweather is a very common cause. It may arise from the inhalation of irrit an t vapors, dust , or pollen.
At times it appears in epidemic form, which would suggest a specificgerm. It also occur s a s a symptom of severa l diseases, su ch as mea sles,scarlet fever, an d th e febricula s.
P a t h o l o g y .—During the early stage, the mucous membrane is dry,red, and swollen, which causes obstruction of the nasal passages andrenders the breathing difficult; this condition is soon followed by aprofuse serous or sero-mucous secretion, which in turn may becomepurulent.
S y m p t o m s .—One of the earliest symptoms is sneezing, whichan nounces to the pa tient t he fact th at he is ta king cold; th is is a tt endedby chilliness, headache, and often slight fever, the temperaturereaching 100° or 101°. The pulse is full and rapid, the face slightlyflushed, the skin dry and hot, the urine scanty and high-colored, and
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 2/107
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 3/107
T r e a t m e n t .—If seen a t t he very beginning, th e disease can usu ally beaborted by a single dose of fifteen or twenty drops of specific gelsemiumtaken at bed-time, or a few drops of the following:
Camphor a nd
Turpent ine 2 ounces each .Alcohol 1/2 ounce. M.
Sig. Of this eight or ten drops on sugar may be taken every three orfour hours.
If it be a weeping cold, a half grain of powdered opium, taken at bed-time, rarely fails to cut short the disease. When this agent is used, thepatient must be instructed to keep his bed the following half day toavoid t he s ickn ess t ha t so often follows the u se of opium .
Diaphoretic pwd. 3 grains, and quinine, 5 grains, taken at night, arealso good t o abort a cold. When th ese mea ns fail to abort th e disease, th etr eat ment will var y according to th e symptoms present .
Bryonia.—When the secretion is glairy, aconite and bryonia will givegood results, while if the eyes burn or there is an acrid secretion fromthe nose and an overflow of the tear-ducts, rhus tox. will replace thebryonia.
Local Treatment .—Alkaline nasal washes may be used with benefit inth e ear ly sta ges; a weak solut ion of bora cic acid, sodium bicar bona te, orcommon salt being among the best. Later, and when the secretion isthick, a few drops of camphor menthol and albolene solution, placed oncotton and introduced into the nostril, and allowed to remain for five orten minu tes, will give good r esult s.
CHRONIC R HINITIS.
S y n o n y m s .—Chronic Nasal Catarrh; Rhinitis Hypertrophica; RhinitisAtr oph ica ; Ozena .
Def in i t ion .—A chronic inflammation of the nasal mucous membrane,often involving the nose and pharynx, and characterized byhypertrophy of the membrane and turbinated bones, an offensive
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 4/107
secret ion, an d an impa irment or loss of th e sense of smell.
Et i o l o g y .—The most common cause is recurring attacks of tlie acuteform, though syphilis and tuberculosis come in for a large share ingiving rise to the disease. The inhalation of irritants, mentioned as a
cau se in t he acute form , ma y also be responsible for th e chr onic var iety.The disease is m ost comm on in children , an d not infrequent ly is due t oadenoids in th e na so-pha rynx.
P a t h o l o g y .—The pa th ological chan ges noted in chronic na sal Ca ta rr hdepend upon the form or stage of the disease, there being threevarieties:
1. In simple chronic catarrh there is irritability of the mucousmembrane, which becomes congested and swollen, causing more or less
obstruction to the free passage of air. There is a profuse secretion of athick, tenacious mucus. In time the inferior tur-binate becomeshypertrophied, and the disease passes from the simple form to thehypertrophic.
2. In the hypertrophic variety, which usually follows the abovementioned form, there is thickening of the mucous membrane andenlargement of the inferior turbinated bodies, so that the passage isnearly or quite obstructed, the patient breathing through the mouth.Often aden oids develop in t he n aso-pha rynx, which necessita tes m out h-
breathing altogether. There may be swelling of the Eustachian tubes,which renders the patient dull of hearing. As in the simple form, therema y be profuse secret ion of thick, viscid mucus.
3. In atrophic rhinitis there is thinning of the mucous membrane, withconsequ ent widening of th e air-passa ge. The m embra ne is pa le, relaxed,and secretes an offensive, purulent material, which, drying, formscrusts or scabs, and, when removed, leaves an excoriated surface. Inth is form th e sense of smell is destr oyed.
S y m p t o m s .—The most common and prominent symptom is theobstructed nasal breathing, due to hypertrophy of the membrane andturbinated bodies. The patient sleeps with the mouth open, thebreathing being sonorous. The secretion drops into the naso-pharynx,an d is rem oved by frequ ent ha wking.
T h e E c le c t i c P r a c t i c e o f Me d i c i n e -P AR T I I I - R e s p i r a t o r y D i s e a s e - P a g e 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 5/107
An examination of the nose reveals its true character. In the atrophicform , the fetid odor is t he m ost cha ra cter istic symptom. Nasa l breat hingmay be somewhat difficult owing to dried crusts; but when these arerem oved, th e na sal pa ssa ges are foun d a bnorma lly roomy. The sense of smell is dest royed.
Inspection shows the mucous membrane thin and covered with grayishor yellowish crusts, the removal of which leaves an excoriated surface,th ough seldom an ulcer. Severe h eada che is qu ite comm on in t his form .
T r e a t m e n t .—Where there is much hypertrophy of the mucousmembrane, and especially of the turbinated bodies, the patient shouldbe referred to a specialist, as operative measures promise more speedyrelief. In t he ear ly sta ges, and when t he h ypert rophy is not ma rked, thegenera l pra ctitioner ma y tr eat th e case qu ite successfully.
The treatment will be both local and general. Where the patient is ableto tr avel, mild, equa ble, an d dry clima tes sh ould be advised.
Clean liness is of great import an ce in th is disease. To at tem pt t o medicat ea case of chr onic rhinitis with out th oroughly cleansing t he pa ssa ges is t ocourt defeat. This may be accomplished by the use of an atomizerthrowing a coarse spray. Boracic acid, a three-per-cent solution of pyrozone, a norma l sa line solution, a Seller's t ablet dissolved in wat er,and glyco-thymolin, are among the best remedies for this purpose.
Having thoroughly cleansed the nostrils, we should use a tonic,astringent, or antiseptic solution, according to the condition of themem bra ne, car e being used to avoid str ong solutions. Ha ma melis,pota ssium chlora te, an d similar rem edies will prove u seful. For ozena , adouche or spray of glyco-thymolin, well diluted, will give good r esu lts .
Nearly all cases will need general treatment as well as local. There iseither defective inet aboh'sm or impaired digestion, u sua lly both , an d t hetreatment will be to break down feeble tissue, stimulate the excretoryorgans to eliminate the detritis, and at the same time supply good,
nourishing ma teria l, properly prepared, to build up th e system.
Well-regulated outdoor exercise increases oxidation of the tissues, andalso shar pens th e appet ite. A good t onic, like nu x vomica an d h ydrast isor th e compoun d t onic mixtu re, will be of grea t benefit.
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 6/107
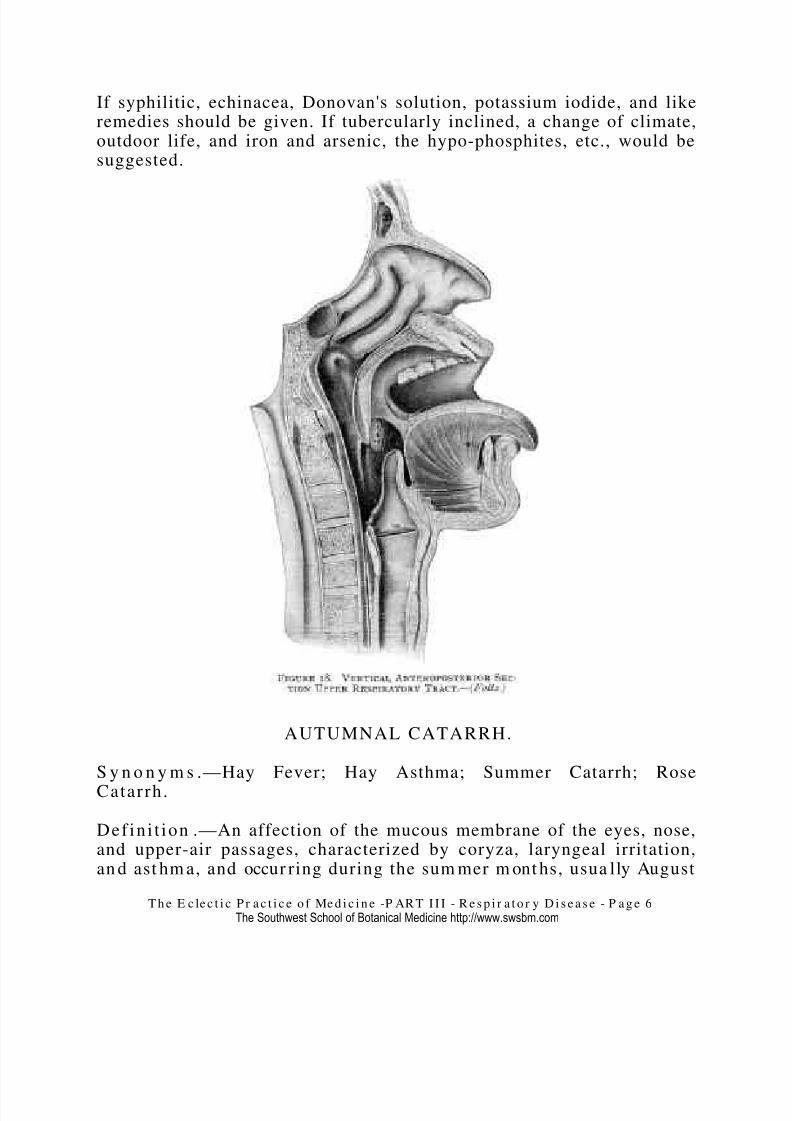
If syphilitic, echinacea, Donovan's solution, potassium iodide, and likeremedies should be given. If tubercularly inclined, a change of climate,outdoor life, and iron and arsenic, the hypo-phosphites, etc., would besuggested.
AUTUMNAL CATARRH.
S y n o n y m s .—Hay Fever; Hay Asthma; Summer Catarrh; RoseCatarrh.
Def in i t ion .—An affection of the mucous membrane of the eyes, nose,and upper-air passages, characterized by coryza, laryngeal irritation,an d ast hm a, and occur ring during the sum mer m ont hs, usua lly August
T h e E c le c t i c P r a c t i c e o f Me d i c i n e -P AR T I I I - R e s p i r a t o r y D i s e a s e - P a g e 6The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 7/107
an d September, and disappear ing with th e first h eavy frost.
Et i o l o g y .—The predisposing cause is the possession of a peculiaridiosyncrasy, which is so subtle as to escape detection. It developssuddenly, occurs each year with almost mathematical precision, and,
once acquired, the habit is seldom ever lost, but grows more confirmedwith each year. The conditions favoring this peculiar habit are race,tem pera men t, mode of life, age, sex. educat ion, and h eredit y.
Race.—It is a litt le singular, but t he E nglish an d th e American s ar e th eprincipal sufferers from hay fever, it being extremely rare in Norway,Sweden, Denmark, France, Italy, Spain, and Russia, and when found isgenerally confined to the English resident. Dr. Jacobi, of New York, afew years ago, stated that he never had met with a case in a German.The French people seem singularly exempt, though the nervous
temper am ent largely predomina tes in tha t ra ce.
Temperament .—While all persons suffering from hay fever are notnecessarily extremely nervous or excitable, yet it is largely a nervouslesion, and is found most frequently in persons of an active, energetic,and nervous temperament.
Education .—Another peculiar feat ur e of this disease is, th at it is a lmostent irely confined to th e educat ed or cultu red class an d t hose who enjoysocial position. McKenzie states that he never met a case in hospital
practice, while Blakely reports forty-eight cases, every one of whichbelonged to the educated class, and Wyman reports forty-nine out of fifty-five cases as belonging t o the cult ur ed class.
Mode of Life.—Although pollen is supposed to be the most commoncause, it is a recognized fact that the class of people who are mostexposed to this exciting cause seldom have the disease; namely, thoseresiding in the country, and agricultural laborers. Beard found onlyseven cases, out of two hundred recorded, in persons living in thecoun tr y. No doubt th e quiet of th e coun tr y allays th e ner vous irrita bility
th at is so often incited by city life.
Heredity .—Heredity undoubtedly plays some part in favoring thedisease, since a history of the disease in some of the relatives can befoun d in from twen ty t o th irt y per cent of all cases of ha y fever.
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 8/107
Age.—It seldom occur s in th e extr emes of life, th ough Mc-Kenzie report sth at he m et with a case in a child two years of age, and cases ha ve beenrecorded when it first occurred after the age of sixty. From puberty toth e age of th irt y is th e most preva iling period.
S ex.—Males a re more frequen t sufferers th an fema les, owing, no doubt ,to great er exposur e t o the exciting cau se.
Exciting Cause.—The most common cause is the pollen of variousplants, though dust may act as the irritant, and sometimes emotionalexcitement is sufficient to bring on an attack in one possessing thepeculiar idiosyncrasy.
S y m p t o m s .—The disease comes on more or less sudden ly with a senseof tight ness or const riction of the h ead, a bur ning or itching sensa tion in
the eyes, especially in the inner canthus, and also in the nose andthroat. Soon violent sneezing occurs, accompanied by a profuse waterydischa rge from t he n ose a nd eyes.
The eyes, nose, and cheeks become swollen, and the patient has theappea ra nce of having a long crying spell. The m ucous mem bra ne of th enose becomes hyperemic and swollen, which obstructs nasal breathing.Often the irritation extends to the larynx and bronchi, giving rise tohay asthma.
An attack may be confined to the nose and eyes, coryza being thetroublesome symptoms; but in the most severe cases the throat andbronchi become involved, the asthma and coryza going together. Thepatient breathes with difficulty, paroxysms of coughing occur atintervals, and the patient presents a depressed and worn appearance.These attacks, varying from the mild to exacerbations of the mostintense character, according to exertion, weather, and the presence of irritating pollen, dust, etc., last from four to six weeks, or till frosts cutshort th e disease.
D i a g n o s i s .—The disease is easily recognized by the sudden onset of sneezing and severe coryza—these symptoms occurring in a person of aneurotic temperament—and the almost mathematical precision of itsret ur n, Augus t a nd Sept ember, an d its defiance to medicat ion, leave nodoubt as t o its identity.
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 9/107
P r o g n o s i s .—The pr ognosis is favora ble as t o life, but u nfavorable as t ocure, unless the patient removes to some climate where the excitingcau se possesses n o power to influen ce th e sensit ive ner vous system .
T r e a t m e n t .—Where the patient is financially able to profit by such
advice, he should be advised to visit the lake resorts of Michigan—Petosky, Mackinac, and the Soo being a few of the manyplaces of this character where he may get relief; also the Adirondacks,the White Mountains, or a sea voyage. He should go a few days beforethe fever's annual return or as soon as it occurs, and remain till afterfrost.
Sterilizing the nasal chambers with Dobell's solution, as recommendedby Hollopeter, and followed by plugging the nose with cotton saturatedwith a mild solution of menthol in albolene, affords great relief.
Internally, specific belladonna, ten drops to a half a glass of water, ateaspoonful every one, two, or three hours, has given good results.Sticta pulmonaria is also a good agent where the coryza is marked,accompanied by asthma and a dry, hard cough. Specific aralia isan oth er r emedy th at should not be overlooked.
EPISTAXIS.
S y n o n y m .—Nosebleed.
Def in i t ion .—Hemorrhage from the nose, arising in the cavity or insinuses leading int o it.
Et i o l o g y .—Bleeding from the nose is quite a common occurrence,especially in early life and may be due to local or constitutionalcond itions . The m ost comm on local cau se is in jury to th e vessels, whichin the nose are very superficial; thus a fall, a blow, or picking thenose—a very common habit in children—or even sneezing, often resultsin obstinate bleeding. The introduction of foreign bodies, quite common
in children, may be the exciting cause. Nasal polypi and malignantgrowth s ma y also be responsible for t he t rouble.
The const itut iona l cau se ma y be due t o a chan ge in th e blood itself, or itmay be due to a diseased condition of the blood-vessels, or it may arisefrom obstruction to the pulmonary circulation, and it may possibly, at
T h e E c le c t i c P r a c t i c e o f Me d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 10/107
tim es, be vica rious. Hemoph ilia or th e hem orr ha gic diat hes is often givesrise to the most severe and persistent types. Typhoid fever is oftenaccompan ied or preceded by n osebleed.
S y m p t o m s .—In plethoric individuals there may be a sense of fullness
in the head, flushing of the face, and throbbing of the carotids, asprodromes. The bleeding varies in quantity and character; thus it mayslowly drip, drop by drop, for hours, or it may flow almost in a stream,passing downwards into the pharynx; the patient may swallow largequantities, to be vomited up as black coagula, which is sometimesmistaken for hema temesis.
Should th e hemorr ha ge cont inue for h our s, the pa tient becomes a nxiousand alarmed at his condition, the pulse becomes small and quick, andth e patient sh ows mar ked depression.
T r e a t m e n t .—Generally, local measures are the only ones that need tobe used. Pr essing th e finger firm ly against th e affected r ide for severalminu tes is often sufficient, or firm pressu re a gainst th e facial a rt ery forsevera l minu tes m ay be effective.
The use of tannin and the iron preparations I do not like, as they areapt to irritate the mucous membrane, and when the hard clot isrem oved, th e h emorrh age often break s out afresh. The injection of veryhot wat er is somet imes very useful.
Pledget s of cott on in chloro-sept ic ha s given me good resu lts .
When th e bleeding persists, notwithsta nding these m easur es, the n oseshould be thoroughly tamponed. A pledget of common cotton (notabsorbent ), to which a str ing is firmly tied, should be push ed far enoughback to get beyond the bleeding points; then more pledgets are to becrowded in t ill th e nostr il is firm ly packed. The h emorrh age ceasin g, thetampon may be allowed to remain ten, twelve, or twenty-four hours,though blood in the nose very soon decomposes and becomes quite
offensive.
To remove the tampon, great care must be used or the hemorrhage willbe renewed. The tampon should be softened with warm water, when itwill readily slip from the n ost ril upon slight t ra ct ion of th e str ing, whichhas been carried to the side of the nose and fastened by an adhesive
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 11/107
strip.
Where the hemorrhage is passive and consists of a continued oozing,th e first t rit ur at ion of char coal will give good result s, th ree t o five gra insevery two hour s. Oil of erigeron, or cinn am on, m ay be u sed successfully,
an d ergot h ypoderm ically, when t he h emorrh age is very stu bborn .
I I . DISEASES OF TH E LARYNX.
ACUTE CATARRH AL LARYNGITIS .
S y n o n y m .—Croup.
Def in i t ion .—An acute catarrhal inflammation of the larynx,
cha ra cter ized by a hoarse croupal cough.
Et i o l o g y .—The most common cause is cold, induced by suddenatmospheric changes so common in the early spring and late fallmonths. The inhalation of irritating vapors may give rise to it andcertain articles of food may produce it; thus, in one of my own children,hot oyster-soup would invariably bring on an attack, usually while thechild was still at th e ta ble.
The disease occur s m ost frequen tly in children between t he a ges of two
and six years, and when appearing in the adult is of a different typeth an croup in children, a nd will necessitat e a separa te description.
P a t h o l o g y .—Although a true inflammation of the mucous membrane,th ere is not such ma rk ed cha nges as one would expect from t he severityof the clinical sympt oms. Th ere is h yperemia of th e mu cous mem bra ne,which is r ed, tumid, an d slight ly swollen.
At first the membrane is dry, but soon a glairy, tenacious mucus issecreted. Edema of the larynx is seen in several types. There may be
slight hemorrhage in the mucous membrane, and erosions may be seenon the vocal cords and portions of the larynx. The changes, however,are not sufficient to account for the severe dyspnea so often met with incroup, and must be accounted for by spasmodic contraction of theintr insic mu scles of th e laryn x. In ra re cases u lcera tion of the lar ynx isnoted.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 12/107
S y m p t o m s .—The symptoms vary with the age of the patient. In thechild the croupal symptoms are characteristic, while in the adult theyar e ent irely different , each n eeding a separ at e considera tion.
In the Child .—Catarrhal or Mucous Croup.—Dr. Scudder's descriptionof th e disease being so rea list ic, I repr oduce it h ere.
“Frequently, for a day or two before the attack, the child will liave hadsymptoms of cold, with a slight cough. Both the cough and voice arefrequently a little hoarse and rough, and would be recognized by aperson acqua inted with t he disease as croupy.
“The a tt ack of croup occur s m ost frequen tly in t he n iglit, t hough it ma ybe in t he da ytime. The child seems t o be su ffering from a cold dur ing th e
evening, but is put to bed without probably a thought of danger. Butalong about t he middle of th e night t he pa ren ts a re a roused by th e childstarting out of sleep with difficult respiration, a hoarse voice, andcroupa l cough .
“The respiration is rough and whistling, the cry hoarse and feeble,except when a great effort is made, when it becomes shrill and piping.At first th e difficulty of respira tion is int erm itten t, but after a n h our ortwo it becomes perm an ent , and t her e is a peculiar wh istling or gur glingsoun d as th e air passes int o an d out of th e larynx.
“As the disease progresses the difficulty of respiration becomes moremarked, and the cough is hoarser, has a peculiar metallic tone, and thevoice sinks to a wliisper. If the child sleeps, mucus accumulates in thethroat, the breathing becomes more and more difficult, until at last thechild wakes with symptoms of asphyxia.
“At first the skin is dry, the temperature is increased, and the pulse isfull and hard; but as the respiration becomes more difficult, a cold,clammy perspiration breaks out, the extremities become cold, and the
pulse frequen t an d feeble. The disease ru ns its cour se in from t welve totwent y-four hours, t erm inat ing in a subsidence of th e disease or dea th .”
Laryngitis in the Adult .—It usually commences with a slight chill,soreness, and stiffness of the throat, difficulty of swallowing, a sense of constriction and a desire to clear the throat. Following the chill, febrile
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 13/107
action comes up, and is quite intense, considering the extent of theinflammation. Then a dull pain is felt in the throat, the sense of const riction is ma rk edly increa sed, an d th ere is tendern ess on pr essur e;the voice is harsh, hoarse, or stridulous, and there is a frequent dry,short cough.
If the throat is now examined, the fauces will be found red and tumid,and when the tongue is pressed down, the epiglottis may be seen erect,swollen, and red. In the course of from twelve to twenty-four hours theinflamma tion ha s m ar kedly diminished the apert ure of the glott is, th evoice becomes small, piping, whispering, and soon suppressed. Thebreathing is difficult, inspiration being sibilus, shrill, prolonged, andlaborious, the larynx being forcibly drawn down on each attempt toinflate th e lun gs.
The cough is stridulous and convulsive, and is attended by attacks of spasm of the glottis, which threaten suffocation; the expectoration isscanty and viscid, and removed with difficulty. In the last stage of thedisease, the patient exerts all his power in respiration, sitting uprightan d grasp ing objects in r each to bring int o play the extern al inspira torymuscles. The countenance is pale and anxious, the lips livid, and theeyes almost start from their sockets, the extremities are cold, andcovered with a clammy perspiration. Soon a low delirium, or coma,comes on, the pulse becomes more feeble and intermittent, imminentsymptoms of asph yxia appear , an d th e patient ra pidly sinks.
Fortunately, the termination is not so serious in most cases, and, aftertwenty-four or forty-eight hours, the cough is attended by expectorationof mu cus, with relief to th e dry, sibilan t respira tion an d a subsidence of all the grave symptoms, though the voice remains hoarse for severaldays.
D i a g n o s i s .—In the child, the hoarse, metallic (croupal) cough, withhoarseness and change of voice, is sufficient evidence of croup, but itdoes not inform us wh ich of th e th ree var ieties it is.
In mu cous croup, th ere is t he slight febrile a ction to distinguish it fromthe spasmodic variety, and the evident presence of mucus in the larynxmanifested by the rattling sound heard on auscultation and incoughing, which distinguishes it from th e pseu do-mem bra nous form .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 14/107
In the adult, the hoarse voice, sibilant respiration, cough, and sense of soreness and constriction in the larynx enables one to recognize thedisease.
P r o g n o s i s .—The p rognosis is n ear ly always favora ble.
T r e a t m e n t .—Aconite seems to possess a peculiar affinity for thelarynx, and in acute cases it is one of our surest remedies. Add two tofive drops of the specific tincture to a half a glass of water, and give ateaspoonful every ten, twenty, thirty, or sixty minutes. It quiets theirrit able larynx a nd favora bly influences th e fever a nd in flam ma tion. Inconnection with this, drop doses of stillingia liniment may be used, andalso rubbed over the larynx. It is a good plan to alternate one drop of the stillingia with one teaspoonful of the aconite mixture every tenminutes.
When t he r espirat ion is dr y, sibilant , and labored, wring a sponge out of hot wat er, an d dr op a few drops of stilling-ia liniment on it, an d h old tothe mouth, the patient inhaling the medicated steam. In very severecases, however, inhalations of steam from hot water and vinegar andhops will give bett er r esults .
Lobelia .—When th ere is dyspn ea, a dd fifteen or t went y drops of specifictincture of lobelia to the aconite solution. Cloths wrung out of hot waterand pinned snugly around the throat, with a dry binder over the wet
one, ass ists in pr oducing relaxat ion.
Potassium , bichromate is often used with benefit a fter th e inflamm at ionha s spen t its force, th e voice rem ainin g hoar se an d h usk y. Of th e secondtrituration, add five grains to a half a glass of water, a teaspoonfulevery h our .
The acetous tincture of lobelia and sanguinaria, used by the earlyEclectics, is a very successful remedy, though not pleasant. It should begiven often enough to produce na usea , but n ot car ried to emesis.
Acetous Emetic Tincture 1/2 ounce.Simple Syrup a nd
Water 2 oun ces each. M.
Sig. A teaspoonful every twenty, thirty, or sixty minutes, till relaxation
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 4The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 15/107
is produced.
CHR ONIC LARYNGITIS.
S y n o n y m .—Minister s’ Sore-th roat .
Def in i t ion .—Chr onic cat ar rh al inflam ma tion of the larynx.
Et i o l o g y .—Repeated attacks of acute laryngitis may finally result inthe chronic form, though continuous use of the voice, especially in theopen air, is the most common cause. The inhalation of tobacco-dust isalso a not uncommon cause, cigar-makers frequently being sufferersfrom this disease.
P a t h o l o g y .—The mucous membrane is red or violet-colored, isthickened and sometimes presents a granular appearance. The vocalcords share in the alteration, while erosion of the mucous membrane,with occas iona l ulcera tion, is a r ar e condit ion.
S y m p t o m s .—Chronic laryngitis usually comes on slowly andinsidiously, th e pat ient being har dly awa re th at h e is suffering from aserious disease u nt il it is confirm ed. The first symptom is soreness of thethroat when speaking, with a sense of constriction, slight alteration of the voice, cough, and expectoration, which comes on after slight
exposure, or overexertion of the larynx. These symptoms areameliorated in a short time, and the patient thinks it is only a slightcold, from which he is recovering. As time passes, however, the attacksbecome m ore frequen t, last longer , and do not so rea dily disappear.
When the disease is fully established, there is a constant uneasysensa tion in t he region of the la rynx; the voice is seriously alt ered, an dthere is a constantly annoying cough, with expectoration. Theexpectorat ion is at first scan ty an d mu cous; but a s th e disease a dvancesit is m uco-puriform , sanious, concret ed int o lum ps, or cons ists of almost
pure pus. Hemorrhage occurs in the latter stages, sometimes in verylarge qua nt ities.
If the throat is examined, we notice the evidence of chronicinflammation of the fauces, pharynx, epiglottis, and we reasonablysuppose that the mucous membrane of the larynx corresponds in
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 5The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 16/107
appearance; with the laryngoscope we are enabled to view the internalsur face of th e lar ynx, an d det ermin e its condition quite a ccur at ely.
A person su fferin g from “min ister s’ sore-th roat ,” or chr onic lar yngitis, isvery subject to cold, and every chan ge in th e weat her or s light exposur e
is followed by an increase of the disease. A very important part of thetr eat men t of every case, therefore, will be directed to obviat e th is.
The impairment of the general health is usually in direct ratio to theseverity of the local affection. At the commencement, the patientcomplains simply of debility, with some failure of the digestive organs,an d sometimes t orpor of th e secret ions. When it h as progressed for somemonths, he is unable to attend to business; there is loss of flesh andstrength; there is marked impairment of the digestive functions and of th e excret ion.
Fr equently th e system becomes so depressed th at tu bercles a re depositedin the lungs, the symptoms of phthisis are developed, and the diseaseru ns a r apid cour se to a fat al term inat ion.
D i a g n o s i s .—We diagnose chronic laryngitis by the unpleasantsensations in the region of the larynx, the cough, and by inspection of the throat, and the absence of physical signs of other diseases of therespirat ory appara tus.
P r o g n o s i s .—Minist ers ’ sore-th roat can be readily cur ed in th e ma jorit yof cases, if th e per son will give th e vocal organ s r esty usu a lly from fourto twelve mont hs will be requ ired. The pr ognosis in confirmed la ryn gitisis not favora ble, as but few have th e pat ience necessa ry to persist in t heuse of remedies until a cure is effected. It can be cured, but it requirestime and perseverance; otherwise the disease is as fatal as confirmedphthisis.
T r e a t m e n t .—The treatment will be both local and systemic, A carefulexamination is to be made, and if there be an elongated uvula or
enlarged tonsils, these conditions must be corrected if we are to deriveth e best resu lts from medicat ion.
The chief remedies that specifically influence the larynx are specificcollinsonia, stillingia, penthorum, potassium bichromate, calciumsulphide, and san guina ria. Where the t issues are congested and dusky,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 17/107
collinsonia will be found a reliable agent. Add one dram to water fouroun ces, and give a tea spoonful every th ree h our s.
Penthorum .—Where the tissues are dry, with violet color, penthorumwill be th e a gent, one or t wo drops every t hr ee or four hours.
Potassium Bichromate.—Where, th e voice is hoar se, an d wh ere t her e isloss of voice, the second trituration of potassium bichromate in two orth ree gra in doses will be efficient .
Sanguinaria.—Where there is a tickling sensation in the larynx,cau sing an almost const an t, ha cking cough, use sa nguinar ia.
Stil l ingia .—The hoarse, husky voice will require stillingia; the tincturema y be used, but th e stillingia liniment , I th ink, gives th e bett er resu lts.
One dr op on su gar every one, two, or t hr ee hours.
Calcium Sulphide.—Where the expectoration is of a muco-purulentcharacter, calcium sulphide, second trituration, will be found to givegoad r esults.
When t her e is great irrita bility, cau sing a ha rd cough, with loss of sleep,a quarter of a grain of codein should be given till the irritabilitysubsides.
It seems a lmost su perfluous to say, th e pat ient m ust rest t he voice whileundergoing the treatment. Local measures are very important, andconsist of gargles, spra ys, an d packs to th e th roat. Where t he t issues of the pharynx are involved and show the same dusky hue as the larynx,a gargle of hamamelis will be found useful. If ulceration be present,list erine is beneficial used in t he sa me way.
The most successful local treatment, however, is that obtained by theuse of the spray. The small hand-spray atomizer may be used, thoughbetter results follow the use of the steam or compressed-air atomizer.
The r emed ies used will be selected with referen ce to th e cond ition of th epart affected, and will be sedative, stimulant, narcotic, tonic, andastringent. Where there is irritation with dryness, and a tenacioussecretion of viscid mucus, an infusion of lobelia will be found beneficial.When t her e is an ir rita ble cough, prevent ing rest, vinegar of opium a ndlobelia is a useful spray. If the tissues are lax, and a tonic is needed,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 18/107
hydra stis ma y be used, or a n a str ingent solut ion of ta nn ic acid, alum, oran infusion of red -oak bar k or yellow root, a s u sed by the ea rly Eclectics.For ulcera tion, pota ssium or iodin ma y enter th e mixtur e. The ph ysicianha s a lar ge field of rem edies from wh ich t o select, a nd if he be car eful a sto the condition of the larynx, he can select the remedy with a great
deal of confidence.
The cold pack at night, with a dry binder pinned snuglv around theth roat, followed by flushin g the t hr oat an d chest with cold water in th emorn ing, will do mu ch t o preven t t ak ing cold.
A change of climate is nearly always beneficial; an ocean voyage orresidence in the pine woods for a few weeks, often accomplisheswonders. Smoking and the use of alcoholic liquors are to be positivelyforbidden.
SP ASMODIC LARYNGITIS.
S y n o n y m s .—Spasmodic Croup; Laryngismus Stridulus; Spasm of theLarynx.
Def in i t ion .—A disease of the larynx occurring in neurotic individuals,usua lly in children from six mont hs to six year s old, th ough occas iona llyin t he adult .
Ricket s predispose to th is affection, and, in t hose suscept ible, the disea semay arise as a reflex disturbance from intestinal parasites, fromdent ition, from ir rit at ion of th e prepu ce, from indigestion, or it ma y ar isefrom the. ordinary causes that give rise to croup, cold being the mostcommon. In rare cases the disease, a spasmodic contraction of theadductor mu scles of th e laryn x is due to emotional excitemen t.
P a t h o l o g y .—Soon after a severe attack, the mucous membranebecomes congested and swollen, which continuing the spasmodic action
of the intrinsic muscles, may result in inflammation. Edema of theglott is and n eighboring tissues is not un comm on.
S y m p t o m s .—The disease usually comes on suddenly, the child beingaroused from sleep with a start, there being great difficulty inbreat hing. The child h as a hoarse, croupal cough, t he voice soon sinks to
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 19/107
a whisper, an d th e breat hing becomes shr ill an d str idulous. Spasm of the glottis occurs, the child becomes cyanotic, and for several secondsholds his breath; this is followed by relaxation of the spasm, when thechild utters a shrill, piping cry. In a few minutes relief is experienced,and the child drops to sleep, the breathing being comparatively easy.
After a short period the child is again awakened by another paroxysm,an d a r epetition of th e first a tt ack occur s: th us t he disease is ma de up of paroxysms and remissions.
During th e remissions th e skin is m oist a nd t he pu lse regular, sh owingan absen ce of inflam ma tory symptoms. These a tt acks follow two or th reenight s in succession.
At other times the child will be attacked suddenly with difficultbreath ing, there being n o cough or h oar seness. These a tt acks term inate
in a high-pitched crowing inspiration. They may occur during the dayas well as a t night. Dur ing an at ta ck, th e child's face becomes livid an danxious, and in rare cases convulsions occur. Occasionally it provesfat al, th e child choking to death .
D i a g n o s i s .—We diagnose spasmodic croup by an absence of inflammatory symptoms, the dry, sibilant respiration, the shrill, pipingcry, the absence of the mucous rattle, and the spasmodic character of the at tack.
P r o g n o s i s .—Although a severe attack presents a frightful picture, thedisease very ra rely termina tes fata lly.
T r e a t m e n t .—The rem edies for spa sm odic croup will form th e basis forlaryngitis str idulus in t he older pa tient . If th e disease is not very severe,drop doses of stillingia liniment on sugar every ten or twenty minutes,and an application of the same rubbed over the larynx every hour, willoften be the only remedy needed. When very severe, the compoundtincture of lobelia and san-guinaria (King's acetous emetic tincture)may be given every ten, twenty, or thirty minutes, till relaxation is
produced. It is n ot necessary to produce emesis.
A flannel cloth wrung out of hot water and applied to the throat, and adry binder covering the wet one, will assist greatly in producingrelaxat ion. Should th e child be una ble to get its br eat h, insert th e fingerinto the lar ynx and h ook u p th e epiglott is.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 20/107
In addition to the above treatment, inhalations of steam from hops,ta nsy, or lime-wat er sh ould be used. An ordina ry tea pot m ay be used, tothe spout of which may be attached a short piece of hose and conveyedto th e face of th e child.
Intubation or tracheotomy should be resorted to only in extreme cases,an d where th e patient's life is thr eatened.
After the attack is over, the case should be thoroughly examined toascertain the exciting cause. When due to reflex disturbance, we mavexpect a return of the disease unless the exciting cause be removed;hence any wrongs of the stomach, digestion, or of the bowels, parasites,hemorrhoids, or other rectal troubles, or wrongs of the reproductiveappa ra tu s, should be corr ected.
Spasmodic croup is often distinctly periodic, when quinine should beadministered. For the hoarseness, that sometimes continues for severaldays, stillingia liniment or potassium bichromate, the second or thirdtr itur at ion, will usu ally be all tha t is r equired.
ED EMATOUS LARYNGITIS.
S y n o n y m s .—Edem a of the La rynx; Submu cous Lar yngitis.
Def in i t ion .—An infiltration of the mucous membrane of the larynxwith serum , usua lly due to inflam ma tion.
Et i o l o g y .—Edem a of th e larynx m ay a rise from injuries to th e mu cousmembrane by swallowing a hard, rough, or sharp body, as a spicula of bone, or by the application of a caustic to the larynx. It may be due toan extension of inflam ma tion of th e neck and ph ar ynx, or, in ra re cases,to acute catarrhal laryngitis. Some drugs will give rise to it, notablypota ssium iodide.
It may arise as a complication in certain infectiousdiseases,—diphtheria, erysipelas, typhoid fever, hydrophobia, scarletfever, influenza, etc. Tubercular, syphilitic, and malignant diseases of th e larynx ma y be accompa nied by edema .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 21/107
It genera lly accompa nies dr opsy, due t o kidney or car diac lesions .
P a t h o l o g y .—The mucous membrane of the upper portion of thelarynx, the rim of the glottis, and the covering of the epiglottis areinfiltrated with serum. The effusion into the sub-mucous tissues of the
ar yteno-epiglott is folds ma y be so exten ded a s t o include th e r espirat orypassage.
S y m p t o m s .— “The disease commences with a continually increasingimpediment to respira tion, a nd a feeling of fullness a nd const riction an dcontinuous desire to clear the throat, as if caused by some foreign body;the voice becomes hoarse, croupal, then sharp, stridulous, whispering,an d is th en lost complet ely; th ere is a h oar se, convu lsive cough , with fitsof suffocation, causing great agony. While inspiration is prolonged,stridulous, and exceedingly difficult, expiration is comparatively easy.
This feat ur e is so ma rk ed as t o be pat hognomonic of th e disease.
“There is no fever, but as the disease progresses the pulse becomesfrequen t, sm all, and irregular . The difficulty of breat hing increases; th efits of coughing and suffocation are more frequent; symptoms of asphyxia are very apparent; the cerebral functions are disturbed; andat last dea th ensu es from inability to inflate t he lun gs.”
D i a g n o s i s .—The difficult, labored respiration and easy expiration willsuggest t he cha ra cter of the disease, while a laryngoscopic examina tion
rem oves all doubt .
P r o g n o s i s .—The prognosis is unfavorable unless relief be obtained byprompt su rgical inter feren ce.
T r e a t m e n t .—If due to inflamma tion,—
Aconit e 3-5 drops.Apocynum 5-10 drops.Wat er 4 oun ces. M.
Sig. Teaspoonful every h our .
Cloth s wru ng out of ice-wat er a nd applied to the t hr oat , with sma ll bitsof ice held in the mouth, affords some relief. If no fever be present,cactus, convallaria, or strophanthus may be combined with the
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 22/107
apocynum. Jaborandi and pilocarpin have been used with benefit byproducing profuse diaphoresis. Where no relief is experienced bymedication or scarification, intubation should be tried, and, this failing,as a last resort tr acheotomy should be perform ed.
P SE UDO-MEMBR ANOUS LARYNGITIS.
S y n o n y m s .—Membra nous Croup; Lar yngeal Diphth eria.
Def in i t ion .—An inflammation of the larynx, characterizedanatomically by ihe formation of a false membrane; clinically, by ashrill, piping respiration, dry, metallic cough, the voice sinking to awhisper.
Et i o l o g y .—There has been much discussion as to whethermembranous croup and laryngeal diphtheria are one and the samedisease, and although it is now generally recognized by the professionas one disease, and alth ough h ealth officers r equire mem bra nous croupto be reported as infectious, I am sure that I have seen cases wherethere is no evidence of infection and no symptom of diphtheria; hence itma y be classed a non-cont agious mem bra nous croup.
As proof I report a recent case: I was called to see a child two years oldwho had been suffering, as I learned, for five days with cough and
difficult breathing. Home remedies had been faithfully used, but thechild grew gradually worse. At my first visit I found the child laboringfor breat h, int err upt ed by th e dry, met allic, croupal cough; th e cry waspiping, and the labored breathing showed the opening of the larynxwas very small. The tongue was but slightly coated, appetite good, noodor from breath, skin moist, secretions from kidneys and bowels good.In fact, ha d it not been for t he labored breat hing an d croupal cough t hechild would have needed no medical aid. The membrane graduallylessened the caliber of the larynx, and, despite steam inhalations andinternal medication, the child grew gradually worse so that intubation
was required to preserve life. Within ten minutes after the tube was inplace, th e child dropped into a quiet sleep, th e breat hing was a s quiet a sthat of a healthy babe, and, to all appearance, the disease was at anend. The tube was allowed to remain four days, during which time thechild drank freely of milk, slept quietly, and made no complaint. Therewas n ot a single symptom of diphth eria.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 2The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 23/107
The cau se of non-contagious membra nous croup is no doubt th e sam e asthat of catarrhal croup, although just why in the one case a plasticexuda te is form ed, it is impossible to say.
P a t h o l o g y .—This is a true inflammation of the mucous membrane,which is attended by a plastic exudate, forming the pseudo-membrane,which varies in thickness from one-sixth to one-fourth of an inch, andconsists of mucus, epithelial cells, and an obscure fibrous structure. Insome cases it is but loosely attached, while in others it is removed withdifficulty.
S y m p t o m s .— “The coming on of an attack of pseudo-membranouscroup may sometimes be recognized for three or four days, or even aweek. The child does not seem sick, an d plays about th e house as u sua l,
but ha s some cold, an d t he pa ren ts notice some h oar seness of voice an dcough. We will notice, however, a peculiar metallic resonance to thevoice, cry, and cough, but more especially that there is a dry andwhistling respiration. This is so marked that the breathing may behear d a cross the room.
“"The attack of croup most frequently comes on at night, as in othercases. In the evening it is noticed that there is more hoarse-ness of thevoice and the cough is somewhat croupal, but as the child breathesprett y well an d does not seem sick, the pa rent s flatter th emselves t ha t it
is but a cold, and will give no trouble. The mother has told me of goingto- th e child's bed or crib, att ra cted by t he peculiar whistling respira tion,impressed that there was something wrong, but fearing ridicule if shesent for t he ph ysician.
“As the time passes, the child becomes restless from difficult breathing,has slight attacks of cough in his sleep, which are clearly croupal. Inanother hour or two he awakes with a start, and assumes a sittingposition, evidently suffering much from difficult respiration, which isincrea sed by t he at ta cks of coughing.
“The symptoms are now very marked, the respiration is sibilus orwhistling, and difficult, the cough hoarse and metallic, the voiceroughened or sun k t o a wh isper, and th e cry shr ill and piping; tlie skinis dry, the pulse hard and increased in frequency, the urine scanty, andthe pat ient restless and u neasy.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 3The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 24/107
“As the disease progresses, there is a gradual increase of all thesesymptoms, but especially of difficult respiration, which is constant. Thecough is spasmodic in its character, and when it comes on, the patientsuffers very greatly from want of air. After a time, evidences of
asphyxia appear in the bluish lips, distended veins, leaden appearanceof the surface, cold extremities, dullness of the nervous system, andfinally coma an d deat h.
“The entire duration of the final attack will be from six to forty-eighthours.”
D i a g n o s i s .—The constantly increasing difficulty of respiration, thewhistling, sibilant sound of the air as it passes through the narrowedlarynx, the dry, ringing, metallic cough, and the piping cry can hardly
be mist ak en for a ny other form of croup.
P r o g n o s i s .—This is a grave disease, and the prognosis must beguarded. In very young children the outlook is unfavorable, owing tothe small size of the larynx. An unfavorable prognosis will be madewhere t he pu lse becomes sm all an d feeble, the sk in r elaxed, extr emitiescold, th e respir a tion gaspin g, an d th e face cyan ot ic.
T r e a t m e n t .—I can not do better than reproduce the treatment asgiven in Scudder 's “Disea ses of Children ,” which is as follows:
“The indications of treatment in this case are: To produce relaxation of the intrinsic muscles of the larynx, and thus give freedom to therespiration while we pursu e th e ma in tr eatm ent; to lessen inflamma toryaction and obtain free secretion of mucus, for the purpose of effectingthe detachment of the false membrane; and, finally, to effect therem oval of th is.
“To fulfill the first indication, we employ inhalations of. the vapor of water, or water and vinegar, or lime-water, as will be hereafter named.
With this we direct the continuous application to the throat of flannelcloth s wrun g out of hot water, in th e mean time bath ing the th roat withthe compound stillingia liniment. These are important means, andsh ould n ever be neglected .
“Ther e a re t wo plan s for a ccomplishing t he s econd indication. The one is
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 25/107
by the use of the tincture, of veratrum viride or aconite, aided byinhalations of lime-water, and is very good treatment and muchpleasanter than the use of nauseates. I prescribe the veratrum in theproportion of ten drops t o wat er four oun ces, a t easpoonful every fift eenminutes, until it produces a marked influence upon the pulse; then in
smaller doses, to contin ue it s effect .
“Aconite is preferred where the pulse is small and frequent, and it isadm inistered in t he u sua l sma ll doses: Tinctu re a conite. 2 drops; wat er,4 ounces; a teaspoonful every fifteen minutes. If the child is verysensitive to the action of the remedy, the dose should be still furtherreduced, and if we find the lips dry and contracted, and the childgrasping at its mouth with its hands, it should be suspended andveratru m administered.
“If th e tongue is pallid, and sh ows sm all spots of red, ph ytolacca m ay becombined with the medicine. If the little patient is dull and stupid andwants to sleep, give belladonna. If there is a sharp stroke of the pulse,an d th e child moves its h ead r estlessly backward a nd forwa rd, th rowingit backward as if it would bury the occiput in the pillow, give it rhus.This remedy is also indicated by the shrill cry as if frightened, andsudden sta rt ing from sleep. Gelsemium is indicat ed by th e flushed face,bright eyes, an d cont ra cted pupils, with rest lessness an d grea t irr itat ion.These remedies ar e secondar y, it is tru e, but it is a case t ha t r equires a llthat we can do, and if by one of these we strengthen the aconite and
verat ru m, we give our pa tient a n a dditiona l cha nce.
“What the physician needs most of all is a steady hand. The treatmentrequires t ime, and we mu st not get excited. If th e pat ient is growing noworse, we should feel satisfied for a time; if there is but slowimprovement, as marked by more ease of respiration, a bettercirculation, warmth, and moisture of the feet, legs, and forehead, wefeel encour aged, an d hold fast to the tr eat men t.
“The use of lime-water as an inhalation is a very important part of the
treatment. It is claimed that it alone is sufficient to arrest theinflamma tory action a nd cause th e detachment of th e membra ne; an d Ihave employed it with success when other means have failed. Theveratrum has also proven very successful alone, and the two will fulfillth e first two cond itions .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 5The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 26/107
“The other and older plan of treatment is by the use of the nauseantemet ics, an d, if proper ly used, will give excellent result s. I ma y add t ha tif improperly used—i. e., so as to irrita te t he st oma ch with r etching an dineffectu al effort s to vomit—th ey will has ten th e fat al t erm ina tion.
“Of th ese r emedies I prefer: Acetous tin ctu re of lobelia, a cetous tin ctu reof sanguinaria, 1 ounce use; molasses, 1 ounce; chlorate of potash,finely powdered, 1/2 ounce; let them be combined with heat, and addthe potash. We give this in doses of a teaspoonful every ten or fifteenminutes, until nausea is induced; then in smaller doses, so as tocontinue the nausea without vomiting. The greater and more constantthe nausea without efforts at vomiting, the greater the success of thetreatment.
“Using th e hot applicat ions t o th e th roat, an d th e inha lations of vinegar
and water, we continue the nausea for some hours, at least until wehave evidence of secretion, and the commencing detachment of the falsemembrane. This will readily be detected by the moist sound of respir at ion, an d a gu rgling, na pping soun d in th e act of cough ing. If th echild is breathing pretty freely, we may wait for the removal of themem bra ne by the cough, as it will be brought awa y by shreds .
“But if, with the loosening of it, it seems to be drawn upward inexpiration, and downward with inspiration, tending to block up thepassages and producing evident symptoms of asphyxiation, we carry
our remedies to thorough a nd pr ompt emesis.
“Generally it will be well enough to prepare an infusion of thecompoun d powder of lobelia a nd capsicum for u se a t t his t ime, as we willhave established a degree of tolerance for the other preparation.Occasionally we will meet with a case requiring prompt relief. Here thechild will be turned on its abdomen; and a finger introduced into themouth, drawing the tongue forward, and exciting the fauces, will befollowed by a forcible expulsive effort, and the membrane will bedetached. A case of this kind occurred in my practice; the membrane
became detached and entirely stopped the larynx, the child wasasphyxiated, and would have died in five minutes. I snatched it fromthe mother, turned it on its face, inserted my finger as far down as thelarynx; a forcible effort at vomiting ensued, and the whole membranewas removed at once, being a perfect cast of the larynx. The childrecovered.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 27/107
“To the above treatment I would add the nitrate of sangui-naria whenthe membrane becomes loosened and is coughed up in small shreds:Nitrate of sanguinaria, 1/8 grain; rub in mortar with boiling water, 4ounces; when dissolved, add a teaspoonful of good, sharp cider-vinegar.
The dose is a tea spoonful every hour.
“Where the child grows worse despite the above treatment, andstruggles for breath, intubation should be performed. The tube shouldrema in th ree or four days.
“Convalescence demands much care. The child should avoid draughts of air. A good tonic should be administered and stillingia liniment orpotassium bichromate given for hoarseness that follows, and tostren gthen a nd t one up t he weakened laryngeal tissues.”
I I I . DISEASES OF THE BRONCHI .
ACUTE BRONCH ITIS.
S y n o n y m s .—Tracheo-Bronchit is; Cold on t he Chest .
Def in i t ion .—An inflammation of the mucous membrane of thebronchial tubes, varying greatly in intensity; hence it has received
different classificat ion. Th us, in th e milder form s, it is t erm ed su bacuteor cold on the chest; in the more severe types, acute or sthenicbronchit is, while in elderly people an d t hose of feeble vita lity it is t erm edasthenic bronchitis. The inflammation also involves the mucousmembrane of the trachea; hence the more proper name, tracheo-bronchitis, and where the disease is actively acute, the nares, pharynx,an d larynx sha re in th e inflamma tory process.
Formerly the extension of the inflammation to the bronchioles. waster med capillary bronchitis; but as t his is att ended with a n involvement
of the air-cells, giving us pneumonia as well, it is now classed asbroncho-pneumonia. Should the inflammation stop short of the lungs,capillary bronchitis would be a proper term. The disease is both acutean d chr onic.
Et i o l o g y .—Among the predisposing causes are: Age, children, and
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 7The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 28/107
elderly people being very susceptible; debility, resulting frommalnutrition; defective drainage, poor ventilation, overcrowding,insufficient food and clothing, or other diseases; occupations, certaintr ades, whereby irr itan t pa rt icles are inha led, such as st eel, bra ss, wood,coal, and tobacco working, etc.; also the fumes of sulphurous acid,
chlorine, and bromine. Sedentary habits also render one moresu sceptible th an a m ore exposed life. Children sh ielded from every dra ftof air by overanxious mothers,. and who wear an excess of woolenswhereby the system is weakened, are very susceptible to inflammatorycond itions of th e ches t .
The exciting cause is usually atmospheric changes; sudden changes inthe weather, which so frequently occur in the spring and fall, wherebyth e pat ient cat ches cold, are fru itful sour ces. Also gett ing th e feet wet , orsudden chilling after exertion, may insure the disease. There is also an
epidemic condition different from influenza, that prevails during someseasons.
Bronchitis is also a common attendant on some diseases, as typhoidfever, whooping-cough, measles, and other exanthematous affections.The disease ma y be acut e or chronic.
P a t h o l o g y .—The mucous membrane of the trachea and bronchi iscongested and swollen, at first dry, but soon covered with mucus, whichat first is clear, glairy and viscid, but soon becomes opaque, and finally
muco-purulent. There is swelling of the mucous glands, and some of thesma ller bronchial t ubes ar e dilat ed; in th e more severe cases t he sm allertu bes are choked with mucus. The ciliated epith elium desquam at es an dth e sub-mu cosa becomes in filtr at ed with leukocytes.
S y m p t o m s .—Simple catarrhal bronchitis, or cold on the chest, beginsas a common cold; there is languor, with frequent chilly sensations,which are alternated with flashes of heat. There is increased secretionfrom the nose; the throat is dry and rough, which causes the patient tomake frequent attempts to clear it. The voice is hoarse, and a short
hacking cough soon develops. The skin is dry, the urine scanty, andth ere is const ipation.
As t he cough develops, ther e is a sense of cons tr iction of the chest , witha dull pain in t he m edian line. The first twent y-four or fort y-eight hoursth e cough is t ight , and t her e is but litt le expectorat ion, th e mu cus being
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 8The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 29/107
clear a nd viscid; but with in a nother twent y-four hours th e cough is notso dry and hard, the mucus becomes more profuse, changes color,becoming yellow, and is ra ised more easily. There is n ow a n aba tem entof all the symptoms, and the patient is convalescent by the sixth oreight h day. In th e more a cut e form s t he chill is quite m ar ked, followed
by an active gra de of fever.
The skin is hot, dry, and constricted, the urine is scanty and high-colored, an d th ere is const ipation. The t hr oat is dry, red, an d somewhatswollen, the voice hoarse and rough. A hard, dry bronchial coughfollows reaction, which is attended by a dull pain in the chest. Therespira tion is hu mid, and t her e is a sense of oppression in t he chest. Thetongue is coat ed, and t here is m ore or less heada che.
The fever may be quite active, although remittent in character. On
auscultation the dry, sibilant rhonchus is heard, followed within forty-eight hours by a mucous rhonchus, which becomes more marked assecretion increases. At first the mucus is viscid and tenacious andsomet imes st rea ked with blood, but soon cha nges, becoming opaque an dfinally mucopurulent. With free expectoration, the sufferings of thepat ient ar e relieved; he s leeps well, th e cough being m ore s evere in th eear ly mornin g, owing to accum ulat ion du ring th e night.
When occur ring in youn g children an d in elderly people, th e pr ostr at ionis much greater, the cough harassing, greatly distressing the patient.
The respira tion is m ore labored, an d th ere is more or less dyspnea . Theexpectorat ion in th e old is more water y in cha ra cter . The cough ispersisten t, occur ring in pa roxysms. In children th e inflamm at ion is m oreapt to extend to the smaller tubes, and the oppression of the chest isconsequently great. The respiration is embarrassed. Auscultation givesmu cous r honchu s, the sm aller tu bes being choked with mu cus.
D i a g n o s i s .—The diagnosis is easily made. The coryza, dry-ness of throat, the dry bronchial cough, and sibilant respiration, call ourattention to the chest. Auscultation gives us the dry rhonchus the first
twenty-four hours, followed by the mucous rhonchus. Percussion givesresonan ce, showing conclusively th at th e lun gs ar e n ot involved.
P r o g n o s i s .—The prognosis is generally favorable, though where itoccurs in delicate children there is a marked tendency in theinflammation to extend to the lung, giving rise to broncho-pneumonia.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 2 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 30/107
In old and feeble patients whose vitality has become exhausted, theprognosis will be gua rded.
T r e a t m e n t .—The treatment for bronchitis by the use of specificremedies is very satisfactory; the disease is shortened, the distress
mitigated, and the patient rendered comfortable without the use of opiates. Our first object is to control the fever, thereby arresting theinflammatory process; just in proportion as we are able to modify thesymptomatic fever, do we modify the cough, and early establishsecretion.
Veratrum .—In a cut e inflam ma tion of th e respirat ory appa ra tu s, th ere isusually excessive power in the heart's action as evidenced by the full,bounding pulse, and veratrum in full doses succeeds, not only inreducing the force and frequency of the pulse and lowering the
tem pera tu re, but also modifies the cough. Vera tr um , 20-60 drops; wat er,4 oun ces; aconite wh ere t he pu lse is sm all an d frequen t, either in childor adult, calls for this agent. Aconite, 5 drops; water, 4 ounces.Teasp oonful every h our :
Bryonia.—This is one of our best cough rem edies, an d is called for wher ethere is pain in the chest, sharp in character, a vibratile pulse beingadditiona l evidence for its use, ten drops added t o th e sedat ive mixtur e,or it m ay be given on a ltern at e hour s.
Lobelia .—Where t her e is dyspnea a nd a sense of oppression in th e chestan d t he pulse is full and oppressed, t his r emedy will be especially useful.In children , where t he sm aller tu bes are choked with mu cus, th ere is nobetter agent ; ten or fifteen drops being a dded to th e aconite m ixtu re.
Eupatorium .—This will be useful in t hose cases wh ere t he t empera tu reis high, yet the skin is inclined to be moist, and the pulse is full andresp ira tion difficult ; add ten to twent y drops to th e ha lf glas s of wat er.
Sanguinaria.—Wliere there is a constant tickling in the throat, this
agent will be of use. Put one-fourth grain of the nitrate of sanguinariain mortar, and rub it down with four ounces of boiling water; addenough syru p to render pa lat able, an d give tea spoonful every hour.
Ipecac.—Where t her e is irr itat ion of any m ucous mem bra ne, ipecac willbe foun d beneficial. Where t her e is exten sion t o th e lung tissu e an d th e
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 31/107
cough is hacking in character, add ten drops to the usual amount of water , and give every hour.
Local Applications.—The only local application needed will be theflann el cloth sprea d with lard or vaselin a nd t horoughly dusted with t he
compound emetic powder. Where this produces too much counterirritation, rub throat and chest with stillingia liniment. The antisepticsare not usually called for in this disease, although there may be anoccasional call for them. Good nursing is, of course, necessary. Thepatient must be kept quiet in bed, and a fluid but nourishing dietadministered. The patient should not be dismissed until the cough isthoroughly subdued: if this course were carried out, there would befewer cases of chronic bronchit is.
CHRONIC BRONCHITIS .
Def in i t ion .—An inflam ma tion of th e mu cous mem bra ne of th e tr acheaand bronchi, that has existed beyond the period of acute inflammation,and has lost the acute symptoms of sthenia. It may be primary,following the acut e or secondary.
Et i o l o g y .—Chronic inflammation is of frequent occurrence, and mayresu lt from ma ny cau ses. A badly trea ted a cut e bronchitis or one wherethe patient stops treatment before a thorough cure is effected, often
results in the chronic form. Neglect is a very common cause; the acutesymptoms giving way, the patient, in his hurry to be about, pays butlittle heed to his cough, and before he realizes it, it has become firmlyestablished. Sometimes it comes on very slowly; the patient coughs inth e wint er a nd spring when ever exposed to cold, but with t he a rr ival of pleasant weather the cough disappears, to return more severely withth e first a tt ack of cold weat her ; by th e following spr ing th e chr onicity isso well established that fair, pleasant weather, while mitigating thepar oxysms, does n ot ent irely relieve th e sufferer, a nd th e disease is wellestablished.
Again, a pneumonia may set up a subacute bronchitis, which persistsafter th e primar y lesion h as su bsided.
Organic heart disease, especially of the right heart, is sometimesresponsible for this condition, as may be chronic Bright's disease.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 1The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 32/107
Rheumatism, syphilis, tuberculosis, and chronic alcoholism may also beimport an t factors in giving rise to the disease.
Old people are very prone to this affection, especially if they aresufferers from any organic disease and are not carefully sheltered in
inclement weather. Children are not often troubled, unless it followswhooping-cough or mea sles.
P a t h o l o g y .—The mucous m embr an e presen ts very differen t condit ions .In some, th e epithelial layer will have disappear ed over a large su rface,the mucous membrane becoming quite thin, or there may be thickeningof the mucous membrane, with infiltration ; in others, there is more orless ulceration. Again, there will be atrophy of the mucous follicles, drybronchitis; in others, hypertrophy, with increased secretion—bronchorrhea.
The mucous membrane presents a livid violet color, in the place of thelight red of the acute form. Where the disease is of long standing, withsevere paroxysmal coughing, there is dilalation of the tubes,bronchiectasis. The changes in other organs are not so constant, beingseconda ry a nd th e resu lt of complicat ions .
S y m p t o m s .—In chronic bronchitis we have to consider both local andconstitutional symptoms. Of the local, the cough, the expectoration, andthe respiration are the most prominent. Cough is the most troublesome
and characteristic feature, being persistent and annoying, usually of adeep bronchial character, or short and hacking; again, asthmatic, withdifficulty in breathing, causing exhaustion. It may be dry and ringingin cha ra cter where bu t litt le mucus is secret ed, or m oist a nd loose whereth e secretion is profuse.
There is generally but little pain, although, when the paroxysms aredifficult and long continued, there is soreness in the substernal region.The expectoration varies greatly in regard to quantity, appearance, andconsist ency, depending up on th e t ype of the d isease, of which th ere a re
three forms: (a) Dry catarrh, the catarrhe sec of Laennec; (b)Bronchorr hea serosa; (c) Pu tr id bronchitis.
Dry Catarrh.—This form is characterized by severe and prolongedparoxysms of coughing, but attended by little or no expectoration ; theexpectoration, when present, is tough and viscid and removed with
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 33/107
difficulty. After th e par oxysms, th e respira tion is h ur ried an d ast hm at ic,the face being flushed and the patient quite exhausted. This form isusually found in elderly people. There is often emphysema, and notinfrequent ly hear t disease is a ssociated with th is type.
Bronchorrhea .—In this form, the secretion is profuse and expectorationabundant and easily expelled; each paroxysm of coughing is attendedwith a free expectoration of a watery character, mucopurulent, or fetidand of a greenish color. Where the mucus is purulent and offensive, itmay be the beginning of dilatation of the tubes and fetid bronchitis.From two to four pints may be expectorated in twenty-four hours. Aftera night's rest the paroxysms of coughing are prolonged and severe, inorder to remove th e accum ulat ion of th e night.
Putrid Bronchitis.—In this form the expectorated material is abundant
and fetid, the odor being characteristic of the decomposition of animalma tt er. This ma y be associated with tu berculosis of th e lung, empyemawith lu ng perfora tion, dilata tion of th e tu bes, abscess or gan grene of th elung, although the odor may be present independent of these. “Theexpectoration is usually copious, and, upon standing, separates intothree layers, of which the uppermost is composed of frothy mucus, theinter mediat e of a serous liquid, an d t he lowest of a th ick sedimen t whichpresen ts a gran ular appea ra nce, an d is ma de up chiefly of sma ll yellowma sses, th e so-called Ditt rich's plugs. These plu gs ar e char acteristic of fetid bronchitis, and are the causes of the fetor. On microscopic
examination, the Dittrich's plugs are seen to be composed of micro-organisms, chief among which is the Leptothrix pulmonalis; they mayalso contain pus corpuscles, fat granules, and crystals of margarin.(Anders.)
P h y s i c a l S i g n s .—The physical signs depend upon the type, but are socharacteristic that, taken with the symptoms above described, adiagnosis is readily ma de. Thus, in t he dr y form , ausculta tion r eveals adry, whistling, or sibilant rhonchus, and, upon percussion, a resonanceis elicited sh owing tha t th e lun gs ar e not involved. Wher e th e secret ion
is profuse, the mucous rhonchus is heard, and if the smaller tubes areinvolved, a slight crepitant sound may be heard. Where there is greatrelaxation of the mucous membrane, with the secretion increased, aflapping or gu rgling sound is hea rd.
G e n e r a l S y m p t o m s .—These depend upon several conditions. If there
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 34/107
is no serious complicat ion, t he general h ealth ma y be but litt le affectedand the patient may follow his vocation with but little interruption.There is usually more or less emaciation, but aside from this, and ahu rr ied r espira tion after exertion, h e complains but litt le.
Where there is organic complications, the symptoms peculiar to theaffected organ are generally so prominent that our attention is at oncedirected to it. Thus cardiac trouble would be known by the sense of weight and oppression in the region of the heart, the dyspnea being ama rked symptom. The pain of rh euma tism a nd gout ar e cha ra cteristic,while Bright 's disease ha s a t ra in of symptoms th at ar e not m isleading.
Where the lungs become involved, especially if the disease is of years'standing, the patient rapidly loses flesh and strength, is compelled totake to his bed, hectic fever and night-sweats follow, and the patient's
condition resembles tha t of pht hisis.
D i a g n o s i s .—The diagnosis is usua lly ma de with bu t litt le difficult y, th eonly disease with which it might be confused being phthisis, and if webear in mind that in phthisis there is fever and loss of flesh and greatprost ra t ion, while in br onchit is th e hea lth is compar a tively good, we candistinguish the two without much difficulty. In phthisis we get localizeddullness, usually in the apex, while in bronchitis there is resonance onpercussion. Th e h istory will also th row much light on th e case, a lthoughthe physical signs are the ones upon which most dependence is to be
placed.
P r o g n o s i s .—The prognosis will depend upon the length of time thepatient has been affected, his previous history, and the complicationsexisting. Bronchitis being so many times secondary to diseases that of th emselves ar e serious, our prognosis m ust be gua rded.
T r e a t m e n t .—One who can profit by our advice we would send toSouthern California or Florida for the winter months, for nothing canta ke t he place of cha nge of clima te,—a war m, even tem pera tu re, where
th e pat ient can rem ain out of doors th e most of his t ime, being especiallydesirable. Unfortunately the greater number of our patrons can notbear t he expense, and we ha ve to do th e best we can at home. Except ininclement weather, our patient must have plenty of outdoor air; butwhen the weather is wet and disagreeable, we must insist on hiskeeping indoors .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 35/107
His sleeping apartment should be large and well ventilated. In themorning th e pat ient is to flush t he n eck a nd chest with cold water , to befollowed by thorough rubbing with a dry, coarse towel, till the skin hasa h ealth y glow and a ll moistu re disappear s.
All nau seat ing remedies sh ould be a voided, as we do not wish t o distu rbthe stomach; for in order to make a good blood—an important factor inth e tr eatm ent—we mu st ha ve good digestion. We must also see tha t th eexcret ory organ s a re in good cond ition.
The general treatment would look to a correction, where possible, of theprimary lesions. The diet should be nourishing and easily digested,while pas tr ies and r ich desser ts should be avoided. The bitt er t onics an drestoratives may be called for; yet, unless each remedy is given for a
direct purpose, our patient will fare better without them. The cough isth e m ost distr essing feat ur e, an d one t ha t calls loudly for relief. This willyield more satisfactorily to direct medication than by giving the usualexpectora nt compoun ds.
Drosera.—Where t he cough is dry a nd hoarse, a dd from fifteen to th irtydrops of drosera t o ha lf a glass of wat er. A teaspoonful every one or t wohour s will give good results .
Sanguinaria.—Where there is laryngeal irritation, a tickling in the
throat, and a persistent cough, sanguinaria must not be overlooked, asit is one of our best agen ts for th is condit ion.
S ticta Pulm onaria.—Where the cough is hard and dry, sticta alone, orin combinat ion with br yonia , will be th e rem edy.
Ammonium Carbonate.—Where the mucous membrane is relaxed andthe secretion profuse, from three to six grains of the carbonate of ammonium will give good results; syrup of tulu and simple syrup maybe the vehicle for its adm inistr at ion.
Calcium Sulphide will be the remedy in fetid bronchitis. Where thecough is irritable and persistent, preventing sleep, an opiate may benecessa ry. In su ch cases,
Codein su lphate 5 gra ins.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 5The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 36/107
Syrup Tu lu 2 ounces. M.
Sig. Teaspoonful every one, two, or t hr ee hour s.
Inhalations will be of much benefit, where there is but little secretion,
th ere being dryness of th e mu cous mem bra ne. If th e larynx be involved,it will be doubly indicated. Steam inhalations, in which eucalyptus,lobelia, a nd hops a re used, will prove very h elpful.
Stillingia liniment in drop doses on sugar is a good remedy for a nightcough. Esculus glabr a is an excellent r emedy wher e ther e are as th ma ticsymptoms.
A persistent hacking cough will frequently yield to the following coughmixtur e when a ll oth ers fail:
Specific Lobelia 1 drachm.Comp. Spir its of Lavender 2 drachmsWater an d
Simple Syrup 2 ounces each . M.
Sig. Teaspoonful every one, two, or t hr ee hour s.
Counter Irritation .—The older practitioners obtained splendid resultsfrom the old compound tar plaster, though few patients today would
suffer t he u se of it. In th e place of th is, we may u se a t ha psia plast er.
BRONCHIECTASIS.
Def in i t ion .—Dilat at ion of the Bronchia l Tubes.
Et i o l o g y .—Any condition that impairs the vitality and tonicity of themucous tissues predisposes to bronchiectasis, for dilatation dependsupon a weakened condition of the mucosa, sub-mucosa, and muscular
tissues, whereby they atr ophy, perm itting th e weak ened tu be to dilat e.
Age also favors t he disea se, being most comm on in adult and m iddle life.Sex also predisposes to this condition, males suffering much morefrequen tly th an fema les.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 6The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 37/107
The disease is usu ally the resu lt of chr onic bronchitis, chr onic phth isis,broncho-pneumonia, emphysema, influenza, and sometimes it is due tomea sles an d whooping-cough .
It may be due to a pressure from an aneurysm or tumors, and where
the walls are greatly weakened, the presence of heavy mucus may besufficient to cau se dilat at ion.
In r ar e cases it is congenit al.
P a t h o l o g y .—The disease may be general or local, and the dilatationmay be cylindrical, saccular, or irregular, all forms of which may beseen in t he sam e lun g.
In ra re cases, th e dilat at ion is confined t o a single tube, an d m ay a ffect
but one side, though u sua lly th e ent ire circum ference of th e walls sha rein th e cha nge.
The most common form is where many of the tubes are involved, thedilatation commencing at the second or third division, and continuingth roughout as a cylindrical or sa ccular enlar gement combined.
The mucous membrane, in rare cases, may remain unchanged, thoughgenerally there is thinning or atrophy. Occasionally the mucousmembrane is congested and thickened, the result of the inflammatory
action. The cylindrical epithelium may be replaced by pavementepithelium.
There is usually a thinning of the muscular tissues, though, in rarecases, there may be thickening due to inflammatory changes. Thecont ent s of th ese cavities var y both in qua nt ity and qua lity. In some t hemu cus a ppears but litt le cha nged, th ough m ore profuse th an in health ,while in oth ers it shows grea t deteriorat ion; in fact, is composed of blood,pus, and not infrequently pulmonary tissue, and casts of the tubes; insuch cases it is very fetid. Still in other s, th e mu cus becomes inspissat ed
and sometimes calcified. Ulceration sometimes occurs in the mostdependent portion of the cavity. There is usually a diseased condition of the near pulmonary tissue, the change depending largely upon theprimar y disease cau sing the dilat at ion.
S y m p t o m s .—The general symptoms present a wide range, depending
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 38/107
upon the primary lesions and enfeeblement of vitality occasioned bythem. The most characteristic symptom is the paroxysmal coughoccurring in the morning, after a night's rest, to remove theaccumulated secretion that has taken place. Change of position, whenlying down, may bring on a paroxysm of coughing, by emptying the
cont ent s of a cavity int o the t ube a bove it.
The expectorated material is usually of a brownish or greenish color,mucopurulent in character, and disgustingly fetid. On standing, itseparates into three layers,—an upper, which is brown and frothy; amiddle, thin, sero-mucus; and a lower, consisting of granular debris.Examined microscopically, the sputum is found to contain pus cells, oilglobules, fatty acid crystals, fragments of lung tissue, and variousmicro-organisms.
Dyspnea occurs after severe exertion, though respiration is but littledisturbed when the patient is at rest. Hemorrhage seldom occurs,though a t times the sput um may be streaked with blood.
P h y s i c a l S i g n s .—The physical signs depend upon the size of thecavities, t heir loca tion, superficial or deep, whet her empt y or filled withsecret ions , and also the condit ion of th e lung t issue.
Auscultation reveals amphoric sounds where the cavity is large andempty. Mucous ra les a re h ear d over var ious port ions of the chest.
Percussion .—After a fit of coughing the cavity is emptied, andpercussion at this time gives a high-pitched tympanitic note; when thecavity is full, the percussion note is dull. Deep-seated cavities are noteasily detected by percuss ion.
D i a g n o s i s .—The diagnosis is not always easy, though the physicalsigns already mentioned should enable one to make but few mistakes.The cavities are to be differentiated from tubercular cavities; but if wekeep in mind certain characteristics of each disease, there will be but
litt le difficulty.
The cavity in bronchiecta sis is nea rly always locat ed in t he ba se of th elung, and the physical signs most prominent posteriorly; while intuberculosis the cavities are usually found in the apex of the lung, andth e physical signs ar e most prominent an ter iorly. Sput um is foul,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 39/107
abundant, and devoid of tubercle bacilli in bronchiectasis. Intuberculosis, the sputum is often blood-streaked, is not so fetid, and isrich in tubercular bacilli. In bronchiectasis there is no fever, nosweat ing, an d th e pat ient is in bett er flesh. In t uberculosis, fever, night -sweats, and emaciation are characteristic. In one the history is that of
bronchit is; in th e oth er, th at of tu berculosis.
P r o g n o s i s .—Unfavorable as to cure, though the patient may live foryears.
T r e a t m e n t .—The general health of the patient must be maintained,and the administration of the bitter tonics, the hypophosphites, iron,arsenic, and like remedies will form a part of the general treatment. Awarm, equable climate is desirable, where the patient can be out of doors th e most of th e time.
Calcium sulphide will be indicated to counteract the suppurativeprocesses which ar e cont inua lly presen t. Inh alat ions of eucalyptu s,iodine, creosote, tu rpent ine, ca rbolic, etc., will corr ect to some exten t thefetid breat h, an d incidenta lly benefit th e pat ient.
ASTHMA.
S y n o n y m s .—Spasmodic Asthm a; Nervous Asth ma ; Bronchia l Asth ma .
Def in i t ion .—A paroxysmal dyspnea, due to alterations in the smallerbronchial tubes of a spasmodic and temporary character, and attendedby more or less const itut iona l symptoms.
Et i o l o g y .—Heredity, sex, season of the year, and age predispose toast hm a. It h as been est imat ed th at in fifty per cent of all cases t her e is afamily history of paroxysmal dyspnea. More males suffer from asthmath an fema les, th e ra tio being a bout two to one. If we except h ay a sth ma ,wint er an d early spring are th e mont hs m ost favora ble to th is disease.
About thirty per cent of all cases occur before the age of ten, twelve percent between th e ages of ten an d twent y, an d eight y per cent before t heage of forty.
Exciting Cause.—All writers agree that there is an abnormal condition
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 3 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 40/107
of the respira tory cent er or of its pa th s of comm un icat ion, but th e exactna tu re of th e exciting cau se or cau ses is not kn own.
It ma y be due, in some cases, t o bronchial irr itat ion, or acute bronchitis;at least this may give rise to a paroxysm. Inhalations of certain vapors
or fumes, or irrita ting dust , and sometimes t he odor of plant s or an imals,is sufficient t o bring on a n a tt ack.
A very large per cent of cases are due to reflex causes, the disturbancebeing at a distant part, as the stomach, uterus, ovaries, urethra, orrectum. Emotional excitement may be the excitant, or it may besecondary to obstructive rhinitis, or growths in the nasal passages,car diac lesions , hepat ic wrongs, and chr onic nephr itis.
P a t h o l o g y .—There are no characteristic anatomical changes in
asthma. In some there is hyperemia of the bronchial mucosa, witli acharacteristic exudate. In others there may be slight thickening of themucosa, and in a great many there are no perceptible changes, showingclearly its reflex cha ra cter .
Where t he disease is seconda ry, the a na tomical chan ges are confined t othe primary organ; as in cardiac asthma, the changes will be in thehear t; in r enal ast hma , in t he kidneys, etc.
S y m p t o m s .—The a tt ack genera lly begins su ddenly, th ough prodroma l
symptoms are not uncommon, and consist of a sensation of uneasinessor constriction in the larynx, oppression or tightness in the chest; chillysensations, digestive disturbances, profuse diuresis, and markeddepression of spirits.
The attack most frequently commences in the night, after the patienthas gone to sleep, he being awakened by a sense of suffocation orinability to fill his lun gs. The dyspnea is ma rk ed, an d th e pat ient desireshis window thrown open that he may get fresh air. There is greatanxiety; the face becomes pale, often cyanotic, showing imperfect
aeration of the blood; the pulse is rapid but feeble; the face, andsomet imes t he ent ire body, is covered with a cold sweat; th e extrem itiesbecome cold, an d t he t empera tu re n ot infrequen tly becomes subn orm al.The patient is unable to lie down, the most comfortable position being asitting posture, the hands grasping some object for support, thusbringing to his assista nce tlie accessory m uscles of respira tion.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 0The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 41/107
The breathing is characteristic, being of a wheezing character that canbe hea rd for qu ite a dista nce. Alth ough , owing to spasmodic cont ra ction,the air enters the lung with difficulty, the patient experiences stillgreater labor in expiration or emptying the lungs, the wheezing being
more pronoun ced on expirat ion t ha n on inspira tion.
The dyspnea is increased by paroxysms of coughing, which at first arequite severe a nd at ten ded by expectorat ion of a t ena cious viscid mu cus.Lat er t he cough is looser a nd t he m ucus ra ised with ea se.
The sp ut um of asth ma is cha ra cter istic an d consist s of sma ll, jelly-likeballs floating in their mucin. These balls, “perles” of Laennec, aremu cous molds of th e sm all bronchioles, an d when un rolled ar e foun d t obe spiral in form, known as Curschmann's spirals, he being the first to
describe th em. There a re a lso foun d in m an y cases, octa hedr al crystals,asthma crystals, first described by Leydon. They are identical with thecrysta ls foun d in sem en a nd in th e blood in leukem ia.
P h y s ic a l Si gn s .—Inspection r eveals t he chest lar ge an d bar rel-sha ped,due t o ina bility t o expel th e air from t he lun gs.
Per cussion usu ally gives hyper-resona nce, th ough somet imes th e note isnormal.
Auscultation in the early stage reveals sibilant rales, of various gradesin pitch, becoming m oist a s t he d isease pr ogresses.
The du ra tion of th e par oxysms is var iable, last ing from a few minu tes t ohours, or da ys. Often th e pat ient experiences relief toward m orn ing, an dth rough t he da y is compa ra tively comfort able, although t he brea th ing ishu rr ied. The following night ther e is a repetit ion of th e experience of theprevious night, which may continue for several nights before obtainingcomplete relief. Somet imes m ont hs elapse before th ere is a recurr ence,th e frequ ency depending somewhat upon th e exciting cau se.
D i a g n o s i s .—The diagnosis is easy, the paroxysms of dyspnea usuallyoccurring in the night, the wheezing respiration and the peculiarspu tu m, leave no room for doubt .
P r o g n o s i s .—The prognosis is favorable-as to life, but few patients
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 42/107
dying from asthma, and only those where it is due to primary cardiaclesions; but it is unfavorable as to a permanent cure, unless due toreflex causes, when a correction of the exciting cause may give promptan d perma nent relief.
The permanent cures from medication, however, are not frequentenough t o warr an t a cur e by the u se of remedies.
T r e a t m e n t .—The treatment of asthma will be first to relieve theparoxysm, and then to ascertain, if possible, the exciting cause, anddirect our tr eatment toward a perman ent cure.
Lobelia is recognized by all schools as an efficient remedy during aparoxysm of asthma. To be effectual, however, it should be carried tothe point of nausea, and when the paroxysm is due to an overloaded
stomach, it should be carried to a thorough emesis. An infusion of theemet ic powder is quite effect ive wher e emesis is desir ed.
Perhaps the most successful agent is morphia, used hypodermically,one-four th to one-third of a grain being u sed a t a dose. The most ser iousobjection to this remedy is the danger of leading the patient into themorphine h abit.
The inhalation of chloroform will frequently give relief, but the effectsar e apt to be tr an sient. One or t wo perles of th e nitr at e of am yi, cru shed
in the handkerchief and inhaled, usually gives speedy relief. Thepat ient sh ould be in bed when t his is used, for t he a gent often producesdizziness a nd sometimes faintin g, an d if not in bed th e pat ient m ay fallto the floor. In very difficult breathing the agent may be giveninternally, a dram to simple syrup and water, 1 ounce each. M.Teaspoonful every thr ee or four hour s.
Inhalations from cigarettes made from lobelia, belladonna, andstramonium leaves proves of much benefit in many cases, or thecoar sely ground h erbs ma y be bur ned in a dish an d th e fumes inh aled.
Nitra te of pota ssium m ay be added to the oth er a gent s, and a dds mu chto it s effectiveness.
For the radical cure the case must be carefully studied, to find theexciting cau se or cau ses t ha t give rise to it. In one case it m ay be du e toendometritis or a diseased ovary; in another, rectal or urethral
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 43/107
disturbances are responsible for the paroxysms. In such cases, acur ett emen t, or possibly an ovar iotomy, will be th e only mea ns of relief,while the removal, of hemorrhoids, papilla, rectal pockets, fissures, etc.,will work wonder s in effectin g a per ma nen t cure.
Any wrongs in t he genera l health mu st be corr ected, an d such rem ediesas a esculus, grindelia, an d pent horum ma y be given th ree or four timesa day with the hope of overcoming the tendency to a return of thedisease.
The nose, larynx, and bronchi should receive a careful examination;an d if any local t rouble exists, it sh ould be r emoved. The pa tient shouldbe shielded from irr itat ing dust , pollen, gaseous or chem ical fumes, a ndan y and all form s of irr ita tion.
In some cases a cha nge of climat e promises t he only relief, alth ough it isdifficult to determine the right locality for each patient. One does betterin th e mount ains , while another derives more benefit in th e lake regionsof Wisconsin and Michigan, while the States of Florida, Texas, NewMexico, Ar izona, Colora do, and Ca liforn ia offer relief to others.
FIBR INOUS BRONCHITIS.
S y n o n y m s .—Pseudo-membranous Bronchitis; Croupous Bronchitis;
Plas tic Bronchitis.
Def in i t ion .—An acute or chronic inflammation of the bronchial tubesand characterized by the formation of a false membrane or fibrinouscasts.
Et i o l o g y .—Cert ain cond itions p redispose to th is affection, alth ough th especific cause' is not known. It occurs far more frequently in malesubjects than in the female, and between the age of twenty and forty,although it may occur at any period of life, and follows the breaking up
of wint er, or t he ea rly spring month s.
It is associated with tuberculosis and certain skin diseases, such aspemphigus, impetigo; and herpes. Heredity may play some part in itscausation. The inhalation of steam and noxious gases is sometimesfollowed by plast ic bronchitis ; while erysipelas , scar let fever, a nd oth er
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 44/107
infectious diseases ha ve preceded it.
P a t h o l o g y .—The exuda te or pseudo-mem bra ne is usua lly foun d in t helarge tubes, although not infrequently involving the smaller branches.The exudate is found upon the mucous membrane, and forms casts of
the tubes. These casts may be hollow or solid, being filled withleukocytes, blood corpuscles, epith elial cells, and sometim es t he Ch ar cot-Leydon crystals.
The composition of the casts is not very well understood, althoughgenera lly believed to be fibrinous. The cast s ar e expectorat ed in t heform of jelly-like mucus, and when placed in water may be unrolled,revea ling- th e cast s of th e bronchi.
S y m p t o m s .—The a cut e form , which is quite ra re, ma y result fat ally in
a short time, owing to the dyspnea, due to occlusion of the bronchi. Itbegins with a chill or rigor, followed by h igh febrile r eaction. The pu lseis sharp and frequent, the respiration hurried, with a sense of constriction in the chest. Dyspnea early comes on, attended byparoxysms of coughing. At first the cough is dry, with but littleexpectoration, though often of a bloody character. Soon secretionbecomes more profuse, and a paroxysm of coughing is followed byexpectoration of some of the casts, not infrequently a profusehem orr ha ge following.
With the subsidence of the fever, the secretion becomes more free, thedyspnea disappear s, and t he pa tient is convalescent. On t he other h an d,th e obstr uction m ay be so great as to lead t o fat al a sphyxiat ion.
Chronic Form .—The chronic form is usually milder in character andrecurs at regular intervals. The earlier symptoms are those of ordinarybronchitis; but a s t he disease pr ogresses, dyspnea becomes m ore m ar kedand the cough paroxysmal in character. Expectoration is more profusethan in the acute form, the jelly mass expectorated revealing completemolds of th e tu bes. The cast s ma y be foun d mixed with pus an d blood.
The genera l sympt oms a re t he sa me a s t hose of chr onic bronchitis. Thephysical signs do not differ m at eria lly from t hose of ord ina ry br onchit is.At first the dry, sibilant rhonchus is heard, changing to the mucous, assecretion becomes est ablished.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 45/107
D i a g n o s i s .—The diagnosis is made from ordinary bronchitis by thegreater dyspnea, the paroxysmal character of the cough, and findingth e cast s when t he sput um is placed in water. Fr om diphth eria, by thelaryngeal complicat ion a nd grave system ic sympt oms of th e latt er.
P r o g n o s i s .—The acute form is a grave disease, and the prognosisshould be guarded. The chronic form generally results favorably,although attacks may recur for years. Where there is a history of tu berculosis t he out look is not so favorable.
T r e a t m e n t .—The tr eat men t in t he a cut e form will be similar to tha t of pseudo-membranous croup, the object being to soften and dislodge themembrane. Inhalations of medicated steam, produced by addingeucalyptus, lobelia, hops, and remedies of like character, to boilingwater, will be found beneficial. Inhalation of lime-water is also to be
advised.
In ter na lly, lobelia or th e old an t ispasmodic tin ctu re will be foun d useful.With th e loosening of the m embra ne, san guinar ia will be foun d h elpfulas a stimulating expectorant. The chronic form will be treated on thesame lines as chronic bronchitis. The general health must be improved,an d th e local tr eat men t will corr espond with th at for t he chronic form .
IV. DISEASES OF THE LUNG.
LOBAR P NEU MONIA.
S y n o n y m s .—Croupous or Fibrous Pneumonia; Pneumonitis; LungFever; Inflam ma tion of th e Lungs, an d Wint er F ever.
Def in i t ion .—From time immemorial, the term pneumonia has beenused to designate an inflammation of the parenchyma of the lungs asdistinguished from inflammation of other parts of the respiratoryapparatus.
The more modern definition would be: an acute infectious disease,characterized by an inflammation of the lung tissue, in which there is,first, congestion or engorgement; second, exudation or consolidation;an d, th ird, resolution or suppu ra tion.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 5The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 46/107
G en e r a l R e m a r k s .—One ha s but to consu lt t he censu s reports in orderto be convinced that pneumonia is the most widespread and fatal of allacute diseases. There are few countries, indeed, where the death rateper one thousand does not run from 1.10 to 2.30 per cent, and themortality ranges from ten to forty per cent. In the United States,
strange to say, the death rate is higher in the Southern States than inthe North ern.
Another un pleasan t fact, according t o the censu s r eport s of 1870, 1880,and 1890, is that the death rate has slightly increased, and that in theState of Massachusetts, from the year 1852 to 1894, there has been aprogressive increase in the death rate. Osler, in his late addition, givesth e morta lity of pneu monia a t from twent y to fort y per cent .
To one who h as practiced Eclecticism , especia lly specific medicat ion, th is
morta lity seems almost incredible, and one is r eady t o believe tha t, justin proportion as the medication is heroic, the death rate increases. Thedisease is usually confined to one lung, when it is called singlepneu monia; when both ar e involved, double pneu monia.
Et i o l o g y .—Predisposing causes are age, sex, season, habits,environm ent , ra ce, an d previous a tt ack.
Age.—While no age is exempt , th e extr emes of life ar e more liable to th edisease. The greatest number occur before the fifth year, and perhaps
the least number between the ages of ten and fifteen years, and fromth is age increasing with each decade.
S ex.—Tha t sex predisposes t o pneum onia is rea dily shown by consu ltingthe census reports, and while this is explained in adults by greaterexposure to inclement weather by males, and also to greaterintemperance in the latter, it does not explain the greater frequency inma le infan ts.
Race.—The colored ra ce ar e not only more p rone to pneu monitis, but th e
morta lity is also great er.
S eason.—Pneumonia prevails more largely during the months of December, January, February, and March, beginning in December andreaching its climax in February and March; but few cases occurbetween t he m ont hs of April an d November.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 47/107
Climate.—Climate, perhaps, acts less as a predisposing cause thanseason, though r eport s sh ow a slight increa se in th e nu mber of cases inth e Sout hern Sta tes over th ose above the th irty-ninth para llel.
Habits .—The drink habit has made giant strides during the last fiftyyears in all the countries of the world, and the drink bill of the UnitedStates, according to official reports of the past year, amounted to onebillion dollars. This amount of alcohol was consumed in fermented anddistilled liquors, to say noth ing of th at vast a mount consu med in pa ten tmedicines, with which this country is flooded, and which the Americanpeople so blindly consume. Add to this a billion-dollar tobacco-bill and agrowing cocaine and morphine habit, and some light is thrown on theincreased morta lity.
Alcohol, nicotine, a nd th e n ar cotic drugs en ter th e blood a nd ar e carr iedto every tissue of the body, impairing the vitality of the whole. Alcoholdiminishes the sensibility and activity of alt nerve cells, and, bycombining with the free oxygen of the blood, impairs that vitalstimu lant an d ren ders it less efficacious in t he t issue chan ges of which itis so large a factor. Taken day after day, even by the so-called moderatedrinker, the blood loses its vivifying qualities, the natural metabolicchanges are impaired, toxic agents are retained, and the power of vitalresistance to pathogenic germs or toxins materially lessened. Not onlythis, but the offspring of the moderate drinker comes into the world
handicapped by a more feeble resisting power than that of theabstainer. If this follows the moderate use of alcoholic drinking, whatare we to expect from the habitual immoderate drinker? Drunkennessten ds to povert y with a ll its a tt endan t ills; poorly cloth ed, poorly housed,an d poorly fed children ma ke u p a very lar ge class in all our large cities,and when the germs of pneumonia invade the body, they find not onlya soil suitable for propagation, but with a vitality of so little resistingpower that the battle between the phagocytes and parasites is but ashort one.
Environment .—The increasing migration of the youth of both sexes tothe cities is another important factor in the problem. In 1850 thepopulation of the United States numbered twenty-three million people,of which twelve per cent lived in the cities. In 1900 the populationnumbered seventy-eight million people, of which twenty-six per centresided in the cities. One-fourth of the people, then, are quartered in
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 48/107
cities.
Exchanging the pure fresh air of the country for the smoke-begrimedand less pure air of the city workshops, stores, offices, and tenement-houses, in many of which a ray of sun never enters and where pure air
is an unknown quantity, they are compelled to take less oxygen intoth eir lun gs, a re depr ived of out door exercise, observe less regu lar hour s,suffer the mental strain of trying to solve the problem of how to keepth e wolf awa y from th e home, to say nothing of th e dissipat ions t ha t a reengendered by a life in the city, and we have all the conditions thatimpair digestion and assimilation of food, increase excitability of thenervous system, impair the action of secretion, and weaken the vitalresista nce of th e individual. A tr ip thr ough t he t enemen t dist rict of an yof our large cities, where the sanitary conditions are vile, will convinceth e most skept ical.
Previous Attacks.—Pneumonia leaves the person peculiarly susceptibleto future attacks, and it is not infrequent to find patients having theirth ird, four th , or fifth at ta ck.
Infectious Diseases.—Certa in infectious diseases a re very pr one to ha vepneumonia as a complication, notably typhus,. typhoid fever, measles,an d dysentery.
Exciting Cause.—The old idea that cold, exposure, and the sudden
arrest of the secretions was the direct cause of an attack of pneumoniastill has a very lar ge following, notwithst an ding th e genera l accepta nceby the profession that it is due to the micrococcus lanceolatus of Fraenkel. That cold figures very largely as a causal factor can not begainsa id, an d t he frequent at ta cks of pneu monia, following imm ediatelyafter a sudden chilling of the body and temporary arrest of thecutaneous secretions, causes a retention of excrementitious material inthe blood, and which, seeking to be eliminated through the lungs, setsup an irritation sufficient to produce an inflammatory condition.Whether these same excrementitious materials produce a toxin which
creates the inflammation; or whether these conditions simply preparethe soil for microbic invasion and afterwards infection,— theexperiment er of th e fut ur e will ha ve to determ ine.
Bacteriology.—The micrococcus lanceolatus, pneumococcus ordiplococcus pneumoniae of Fraenkel and Weichselbaum was first
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 8The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 49/107
discovered by Sternberg in September, 1880. In December of the sameyear, Pa steu r discovered th e sam e organ ism, not being awa re of a priordiscovery; neither one, however, recognized any relation existingbetween th e germ a nd pneu monia.
Stern berg's discovery resu lted from isolat ing th e micrococcus a s a r esu ltof inoculating rabbits with his own sputum, while Pasteur found thesa me coccus in th e saliva of a child dead of hydr ophobia. It wa s not u nt ilApril, 1884, that A. Fraenkel came to the conclusion that the organismdiscovered by Ster nberg a nd P as teu r, an d which h ad come t o be knownas th e coccus of sputu m septicemia, was th e cau sal factor of pneu monia,since it was t he organ ism most frequent ly foun d in th at disease.
In 1886, Fraenkel and Weichselbaum were able to demonstrate themicrococcus as the causal agent in m ost cases of pneumonia. These and
other experiments seem to justify the etiologist in naming this germ asthe specific cause of lobar pneumonia. We are not to forget, however,that this same organism is found in the saliva of twenty per cent of healthy individuals, and in many other diseases, such as pleurisy,pericar ditis, peritonitis, cerebro-spina l meningitis, an d other s.
This organ ism is a lance-sha ped coccus, u nited in pairs; hen ce th e ter mdiplococcus; and is found in health in the nose, Eustachian tubes, andlarynx, and in va rious diseases besides pneu monia.
P a t h o l o g y .—The r ight lung- is m ore frequent ly involved t ha n th e left,and one lobe, or one entire lung, rather than both lungs at the sametime. A reference to the following table compiled by Juergensen willshow th e relat ive frequen cy of the p ar ts affected:
Right Lung 53.70Right Upper Lobe 12.15Right Middle Lobe 1.77Right Lower Lobe 22.14Righ t Whole Lung 9.35
Left Lung 38.23Left Upper Lobe 6.96Left Lower Lobe 22.73Left Whole Lung 8.54Both Lungs 8.07Both Lungs, Upper Lobes 1.09
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 4 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 50/107
Both Lungs, Lower Lobes 3.34
The anatomical changes that take place in pneumonia have for yearsbeen considered un der th ree hea ds or st ages.
1. The st age of congest ion or en gorgement .
2. Sta ge of consolidation or r ed h epat izat ion.
3. Stage of gray h epat izat ion.
Stage of Engorgement .—In this stage there is hyperemia of the part orpar ts involved, which increases till there is m ar ked engorgement . At th istime the tissues are of a deep-red color, firmer in consistency andheavier than normal lung tissue, and, on making an incision, the cut
surfaces will be bathed in a bloody serum; there is still some crepitationon pressure, and the lung will still float. The capillaries are greatlydistended, the white corpuscles appear in great numbers, and thealveolar epithelium becomes detached and undergoes granulardegeneration. The hyperemia, with its accompanying redness, extendsinto the bronchi, which at first are dry, but this condition is soonreplaced by mucus. In the smaller tubes similar changes to that of theair vesicles take place.
This stage may occupy but a few hours or extend over a couple of days.
As a resu lt of th is engorgement , ther e is exuded int o th e air vesicles andsmaller bronchioles a fibrous exudate, in which are found epithelialcells, fibrin an d gra nu lar m at ter , thu s giving rise to the second sta ge, orconsolidation.
R e d H e p a t i za t i o n .—This sta ge takes its n am e from th e resemblan ce of th e affected pa rt s t o the liver. The volume of th e organ is increa sed, th ecolor is pu rplish or mottled, and frequent ly th ere is indent at ion from t heribs. The tissu e is now solid, no air in th e cells, no crepita tion, a nd th elung will sink if placed in wat er. The t issue is friable, an d m ay be ea sily
broken down.
The cut sur faces show a gra nu lar ma ter ial, consist ing of fibrinous plugs,alveolar epith elial cells, red corpuscles, an d leucocytes which h ave filledthe air vesicles. If a large portion of the lung be involved, the irritationextends to the pulmonary pleura, and this surface is soon covered with
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 51/107
a film of fibrous exudate, and the sac may contain a serous effusion.The interlobular t issue cont ains t he sa me chara cteristic exuda te.
Gray Hepatization .—This is the stage of resolution or diffusesuppu ra tion. The color of th e lung t issue, as t he n am e indicat es, loses its
dark-red color and becomes pale or grayish white. The tissue is morefriable and the granular elements less distinct, and, as fatty andgranular degeneration takes place, the exudate breaks down, becomesmoist, and, on making a section, a turbid, purulent fluid appears. Theair vesicles are filled with leukocytes, the fibrin and red corpuscleshaving disappeared; with this disintegration of the cellular elements,resolution is fully est ablished a nd t he a bsorben ts car ry it off.
Where the recuperative powers are feeble, this stage of grayhepatization may remain for several weeks, and if the exudation has
been quite extensive, abscesses may form, which may open into abronchus, or it may become encapsuled, undergoing caseousdegeneration.
Chan ges in Other Organ s.—The hea rt is frequ ent ly pa le an d flabby an dcontains large, firm clots, especially the right chamber, which can berem oved in th e sha pe of a cast . In n o oth er disease is t he coagula so firman d t enacious.
Per icar ditis occur s in about five per cent of th e cases, u sua lly when th e
left lung is involved or in double pneumonia. Osler found five cases inone hundred autopsies. Endocarditis is more frequent, sixteen beingreported in one hundred cases examined, five of which were of a simplecha ra cter , while eleven were of th e ulcera tive type.
Chronic interstitial inflammation and parenchymatous degeneration of th e kidneys may result.
The liver and spleen may show parenchymatous degeneration and areslight ly enla rged.
Croupous or diphtheritic inflammations are among the very rarecomplications, and when seen are usually in the form of a thin, flakyexudate.
G e n e r a l S y m p t o m s .—The period of incubation is usually of short
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 1The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 52/107
du ra t ion, n ot over twen ty-four or fort y-eight h ours , save in old people ordelicate subjects, when it may last for three or four days. During thisstage there may be catarrhal symptoms, with a short bronchial cough,oppression of the chest, and hurried respiration; headache and generalmalaise, make up the list. Usually, however, the onset is quite sudden,
being ushered in with a chill of pronounced character, lasting fromth irty to sixty minut es. This ma y occur while th e pat ient is at his work ,or may awaken him in the night. So pronounced is the chill that it ischaracteristic of this affection, no other acute disease comparing with it;for t his r eason it is one of th e ear liest d iagnostic sympt oms.
In children, a convulsion may replace the chill, while in old people asense of chilliness may replace the rigor. Febrile reaction follows, thetemperature rapidly rising to 104° or 105° within the first twenty-fouror forty-eight hours. The skin is hot, dry, and constricted, the face
flushed, especially the cheek of the affected side. The eyes are bright,pupils contracted, there is headache, and the patient is quite restless.The u rine is scant y and highly colored, an d th e bowels a re const ipated,th ough occasiona lly diarr hea is seen from th e beginning. The t ongue isdry and covered with a white, pasty coating; there is loss of appetite,and th e patient experiences great th irst.
His position in bed is another characteristic feature, the patient lyingupon th e affected side; by th is mean s th e lun g and pleura ar e held morequiet, an d th us t he a cute pa in is lessened.
After three or four days, the patient assumes the dorsal position. Ashort, dry, hacking cough is one of the early symptoms, which isat tended with but litt le expectoration. The breat hing is short a nd ra pid,expiration often being audible and accompanied by a “grunt;” there isunusual expansion of the chest, and the alæ nasi dilate forcibly oninspiration. The pulse is full and bounding, save in the aged and thoseof feeble vitality. Herpes of the lips occurs more frequently in this thanin an y oth er disease.
S p e c i a l S y m p t o m s .—Temperature.—The temperature rises rapidly,reaching 105° or 106° within fifteen or twenty hours. Having reachedth e ma ximu m height, it r un s a un iform cour se for from five to seven oreight days, there, being but from one-half to one degree differencebetween the evening and the morning temperature. This uniformity of temperature continues to the crisis, which takes place from the fifth to
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 53/107
th e. ten th day, when it ra pidly declines, frequen tly reaching the n orm alin eight or ten hours, and not infrequently becoming subnormal. In oldpeople, dru nk ar ds, and delicat e people, th e temper at ur e does not r un sohigh, rarely exceeding 103°.
Pain .—Pa in is a prominent symptom of most cases, th e exception beingwhere but a small portion of the interior portion of the lung is affected,or where the apex is the seat of the disease. The pain is sharp,lancinating, or throbbing in character, and usually in the region of thenipple. A full inspiration increases the pain; hence we find the patientgrasping the side as if to prevent the motion of the lung, and thebreathing is shallow. With the consolidation of the lung, the painbecomes m uch less severe, often disappear ing ent irely.
Respiration .—While th e respira tion is ra pid in a ll fevers, in p neu monia
it is cha ra cteristic, dyspnea being a ma rked feat ur e.
Following the chill, the respiration is short and rapid, ranging fromthirty to sixty in the adult, and from fifty to a hundred in the child. Asthe stage of engorgement passes to that of hepatization the breathingbecomes quite labored. When the cough is paroxysmal and when theexpectoration is unusually viscid, the breathing is very distressing, thepatient being propped up in bed, while he grasps some object to givegreat er freedom t o th e expira tory mu scles. The face ta kes on an an xiousexpression, and the gravity of the case is evident to the merest tyro in
medicine.
Cough .—Beginning with the invasion of the disease, a short, dry,hacking cough, attended by more or less pain, suggests a wrong of therespiratory appara tu s, and by th e th ird or fourt h da y it is cha ra cteristic,the patient using every effort to suppress the paroxysmal, frequentcough. In hard drinkers, or in feeble, aged patients, it may be muchlighter an d in some cases en tirely absent .
Expectoration .—The expectoration is often delayed for two or three
days, though a white, frothy mucus may be raised the first day. Themu cus is foamy or filled with litt le bubbles, and is rea dily recognized ascoming from the lun g. Occas iona lly a hemorr ha ge is th e first ma ter ialto appear .
By the second or third day the sputum is characteristic; thick, viscid,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 3The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 54/107
and so tenacious that it runs together in the vessel, which may beinverted without discharging it. Occasionally this tenacious, glueymucus is streaked with blood, though this more often occurs inbronchitis. By the fourth or fifth day the mucus has become opaque,an d is int ima tely mixed with blood, giving it a ru st y or ora nge color, and
so cha ra cter istic is this spu tu m a s to be pat hognomonic.
In low grades of the disease, and sometimes in old people, the mucusmay be of a watery character, and of a prune-juice color. The quantityvaries—in some it is very scanty, while in others it is very profuse. Asresolution t ak es place, th e rus ty color gives way t o a yellow mu cosity.
P h y s i c a l S i g n s .— Inspection .—As before remarked, the patient will befound lying upon the affected side if one lung be affected, or on theback if both lungs are involved. The first few hours may not reveal to
the eye the changes that are taking place; but, after twenty-four hours,inspection of the chest shows a restricted motion on the side involved,and increased expansion on the well side; and later, when completeconsolidation ha s t ak en place, th e expansive power en tirely disapp ear s.The frequency and difficulty of respiration and the dilation of the alæna si ar e not t o be overlooked.
Mensu ra tion will show an increa se in volum e on t he a ffected side.
Palpation .—The tactile fremitus is increased over the congested area,
while th e absen ce of expan sive power is very su ggest ive.
Percussion .—During the stage of engorgement, but little informationwill be gained on percussion, and if the inflammation be in the morecentral part of the lung, and but little of its circumference be involved,th e percussion note will be norm al. As t he exuda te t ak es place, however,th e dullness increases, an d in th e second st age is complete.
With th e beginning of resolut ion t he peculiar dead or flat note begins t odisappear, resonance becoming more marked each day, till the exudate
entirely disappear s an d th e lun g is restored to hea lth.
In some cases, restoration is not complete for weeks or months; and insome, never. Percussion gives us valu able inform at ion in t hese cases.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 4The Southwest School of Botanical Medicine http://www.swsbm.com
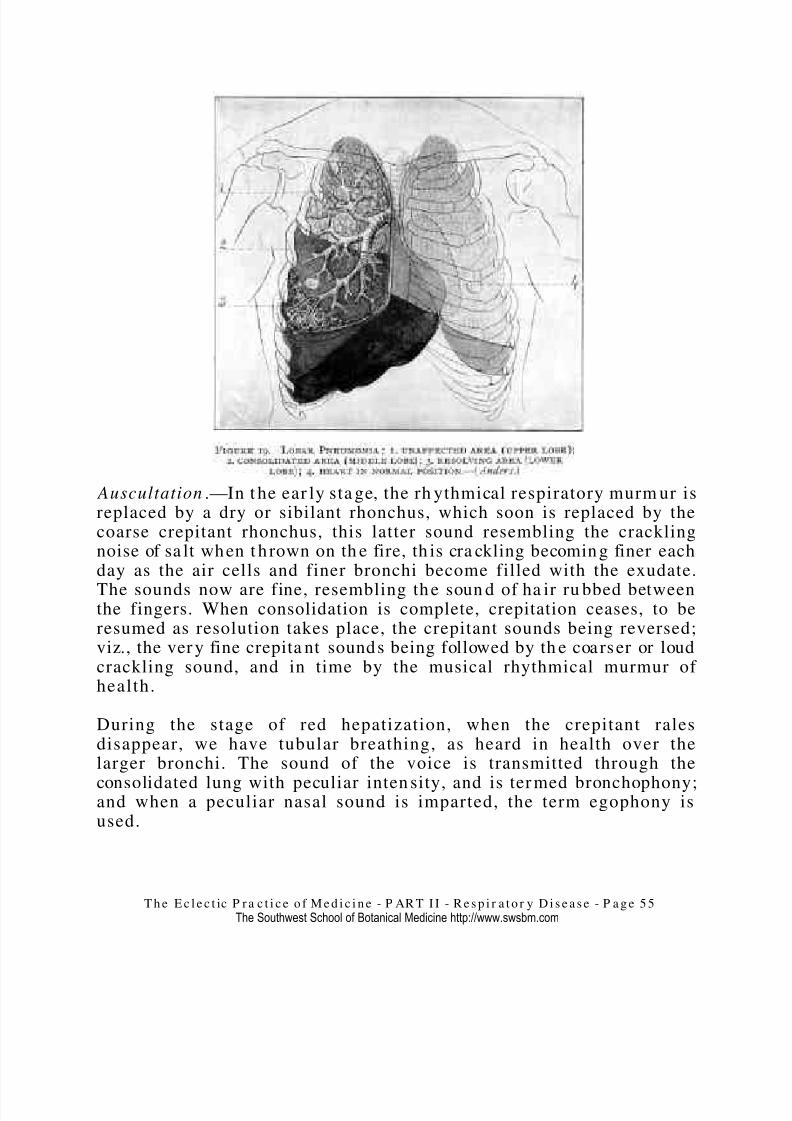
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 55/107
Auscultation .—In t he ear ly sta ge, the rh ythmical respiratory murm ur isreplaced by a dry or sibilant rhonchus, which soon is replaced by thecoarse crepitant rhonchus, this latter sound resembling the cracklingnoise of sa lt when t h rown on th e fire, th is cra ckling becomin g finer eachday as the air cells and finer bronchi become filled with the exudate.
The sounds now are fine, resembling th e soun d of ha ir ru bbed betweenthe fingers. When consolidation is complete, crepitation ceases, to beresumed as resolution takes place, the crepitant sounds being reversed;viz., the ver y fine crepita nt sounds being followed by th e coarser or loudcrackling sound, and in time by the musical rhythmical murmur of health.
During the stage of red hepatization, when the crepitant ralesdisappear, we have tubular breathing, as heard in health over thelarger bronchi. The sound of the voice is transmitted through the
consolidated lung with peculiar inten sity, and is ter med bronchophony;and when a peculiar nasal sound is imparted, the term egophony isused.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 5The Southwest School of Botanical Medicine http://www.swsbm.com
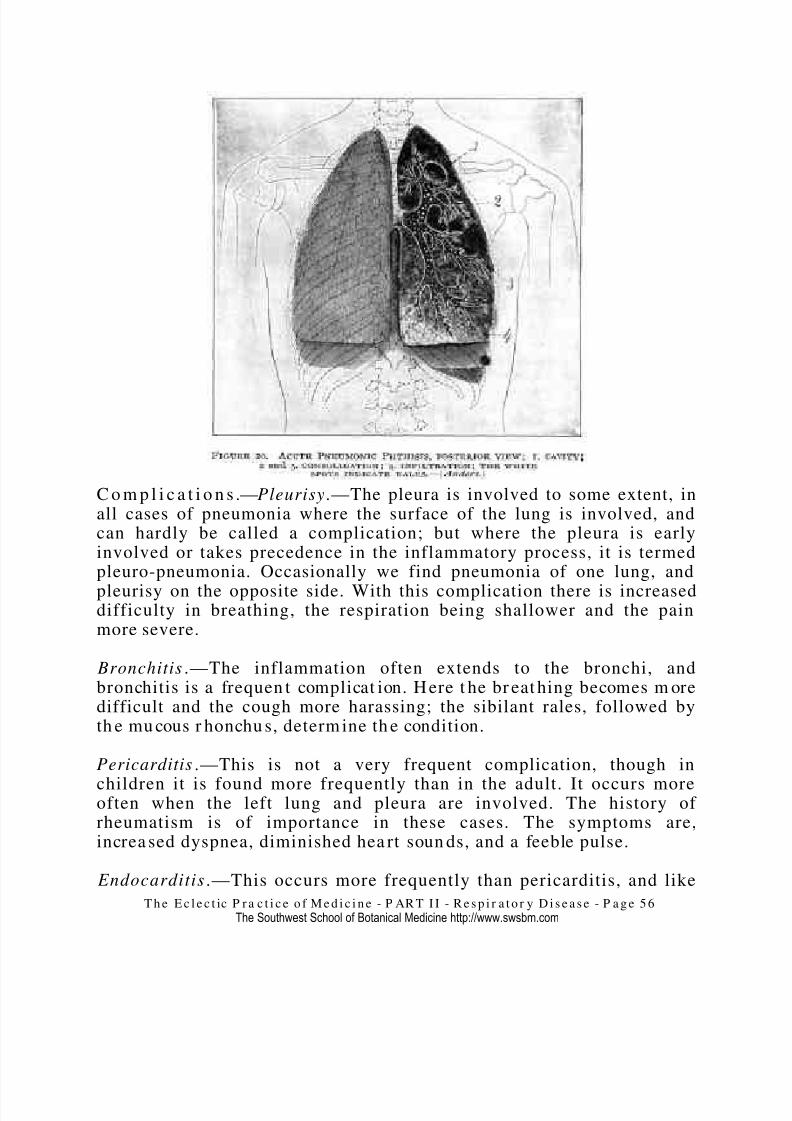
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 56/107
C o m p l i c a t i o n s .—Pleurisy.—The pleura is involved to some extent, inall cases of pneumonia where the surface of the lung is involved, andcan hardly be called a complication; but where the pleura is earlyinvolved or takes precedence in the inflammatory process, it is termedpleuro-pneumonia. Occasionally we find pneumonia of one lung, and
pleurisy on the opposite side. With this complication there is increaseddifficulty in breathing, the respiration being shallower and the painmore severe.
Bronchitis .—The inflammation often extends to the bronchi, andbronchitis is a frequen t complicat ion. H ere t he br eat hing becomes m oredifficult and the cough more harassing; the sibilant rales, followed byth e mu cous r honchu s, determ ine th e condition.
Pericarditis .—This is not a very frequent complication, though in
children it is found more frequently than in the adult. It occurs moreoften when the left lung and pleura are involved. The history of rheumatism is of importance in these cases. The symptoms are,increa sed dyspnea, diminished hea rt soun ds, and a feeble pulse.
Endocarditis.—This occurs more frequently than pericarditis, and like
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 57/107
the latter is more apt to occur when the left lung and pleura areinvolved. If valvular tr oubles h ave pr eviously existed, t her e is a great erten dency to th is complicat ion. The symptoms a re obscur e, even in severecases, the condit ions genera lly being discovered post -mortem.
Meningitis is a ser ious complicat ion, though n ot very frequ ent . It occur smore frequen tly in children of an a ctive ner vous temper am ent . It willbe recognized in the child by restlessness, rolling of the head, andsta rt ing in t he sleep.
Gastric Com plications .—These a re r ecognized in two condit ions,—one of irritat ion, and th e oth er, atony. In t he one, there is nau sea an d retchingand tenderness over the epigastrium; the tongue is narrow andelongated, reddened at tip and edges. With this condition theinflamm at ion is more active and t he tem perat ur e higher.
Where t her e is at ony, th e tongue is full, broad, an d h eavily coat ed. Theskin is not so dry an d ha rsh, an d th e temperat ur e does not r un so high.Resolution is delayed, and there is a greater tendency to congestion of other organs.
Jaundice is rot uncommon; when it occurs, all the symptoms are moreintense.
Typhoid Pneumonia.—While pneumonia is a frequent complication of
typh oid fever, ent eritis seldom occur s a s a complicat ion of pneum onia . Inth e ra re case where it occur s th e symptoms a re as follows:
“A protra cted chill; febrile rea ction comin g up slowly; the pu lse frequ ent ,soft, and fluent; heat of the surface not greater than natural; coldnessof extr emit ies; bowels easily acted upon or t endency to diar rh ea; limpid,frothy urine; dirty coating of the tongue; and especially that dullnessand indifference so characteristic of typhoid or typhus diseases. Theinflammation in this case is ataxic; there is difficult breathing andcough, with watery expectoration.
“Physical examination gives us rapidly increasing dullness onpercussion to a certain degree, at which point it remains, sometimes,dur ing the ent ire progress of th e disease; th ere is no crepita nt rh onchus ,and the mucous rhonchus sounds hollow and distinct. This condition isof variable duration, sometimes the disease is slow and protracted for
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 58/107
weeks; at oth er t imes it is r apidly fat al.” (Scudder .)
Recurrence.—There are few acute diseases in which there is arecurrence as often as in pneumonia. Each attack may be more severe,th ough t his is not necessa rily so.
D i a g n o s i s .—The diagnosis is usually not difficult. The sudden andmarked chill or rigor lasting from thirty to sixty minutes; the highfebrile reaction; the anxious expression on the face and the dusky redspot upon the cheek; the quick, shallow respiration; the short, dry,hacking cough; the sharp pain over the affected part; the sharp,crackling, crepitant rhonchus, followed by the fine crepitant rales; thedullness on per cuss ion; th e frothy spu tu m th e first twent y-four or fort y-eight hours, followed by rus ty expectorat ion,—ar e sympt oms th at ar e socha ra cter istic as to leave but litt le doubt , not only as t o th e disease, but
also as t o th e degree an d sta ge of th e inflamm at ion.
The doubtful case is found in old people, where the initial chill is eitherslight or entirely absent, and where the cough is slight or absent, andwhen the inflammation is deep-seated and but few physical signs arepresent.
P r o g n o s i s .—Although pneumonia is regarded as one of the most fatalof acute diseases, and, according to recent allopathic authorities, isprogressively increasing, I am sure that a very large per cent should
recover; th at th e mortality sh ould n ot be over from thr ee to five per cent.This may seem to be an extr avagant sta tement to one who has pr acticedthe treatment as advocated by the dominant school, but the record of Eclectic treatment in pneumonia will bear me out in the assertion. If seen ea rly, th e inflamm at ory pr ocess can be so modified tha t th e severertypes will be seldom seen , and a n ea rly conva lescence assu red.
T r e a t m e n t .—If th ere is an y one disease more t ha n an oth er t ha t showsthe superiority of Specific Medication over the old methods of treatm ent—and I might also add th e present methods tha t a re at tended
by a mortality of from twenty to forty per cent —it is pneumonia. Theexperience of the profession, for the last century or more, is that themore active or h eroic th e medicat ion, th e grea ter th e morta lity.
The expecta nt tr eatm ent, which is no medication , has yielded far betterresults than the old method of drugging, and while we would prefer
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 8The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 59/107
th at to the old, we believe tha t t here is still a m uch better wa y.
Pneumonia is a typical inflammatory disease, and if we have remediesth at will overcome t hese conditions, we cert ainly ha ve remedies th at ar ecurative.
G e n e r a l M a n a g e m e n t .—Where p ossible t he pat ient should be placedin a large, sunn y, an d well-ventilated r oom. Plent y of fresh air mu st beadmitted, though all draughts of air should be avoided. Thetemperature should be uniform, and not over 68° or 70°. The patientshould have a loose woolen night-dress, and only sufficient covering tokeep him comfortable. The care of the bed and secretions must be asscrupulous as in typhoid. Only one attendant should be with thepatient.
Diet .—The diet should be liquid and consist of milk in some form orbroths, and given at regular intervals. A good table water may be usedfreely.
Medication.—Wrongs of the circulation occupy the first place in manycases, but not in all. In some, wrongs of the blood itself precede allothers; while in another class, wrongs of the nervous system takeprecedence. Such being the case, conditions have to be met andovercome before we can effect a cure, and it is this prescribing fordefinite cond itions t ha t br ings about success.
If we keep well in mind the pathology of the different stages of thisdisease, we are not apt to become confused or go far wrong in thetr eat ment . Thu s, in t he first st age, there is usu ally an active condition of th e circulat ion; the hea rt beats r apidly, th e pulse being full, strong, and bounding; the capillar ies become full an d distended, giving us th e sta geof engorgement. If we are to relieve tills engorged condition, we mustslow the heart and circulation, and I know of no remedy that willaccomplish this end with such happy results as veratrum, if usedskillfully. It does not depress and weaken the heart like the coal-tar
products, but a cts k indly, slows th e pulse, redu ces th e temper at ur e, an drelieves the obstructed venous capillaries. Its action is uniform andeas ily cont rolled, even in t he lar ge dose.
Aconite is the r emedy where th e hear t 's action is ra pid, but th e pulse issmall but hard and wiry. It is generally prescribed in the sthenia of
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 5 9The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 60/107
children, while veratrum acts better in the adult. Should the heart beweak, as sh own by a sma ll, feeble pulse, aconite mu st not be given, sa vein th e very small dose.
Pilocarpus or jaborandi acts kindly, where there is high temperature,
great excitement of th e nervous system, an d a dr y, hot skin.
With these remedies as our sedatives, we have the foundation for asuccessful t rea tm ent , for t hey not only relieve engorgemen t in th e ear lystage, but materially assist in the removal of the exu-dates that follow,and, where carefully used, the second and third stages are so modifiedas t o fur nish bu t little need for a larm .
The indication for the remedies that have been so successfully used inpneum onia is as follows:
Veratrum .—One of the characteristic symptoms of the majority of pneumonia patients is a full, free, bounding pulse; in oth er words, t her eis an excess of heart power. Now, if we have a remedy that can reducethe force and frequency of the pulse, without reducing at t he same timethe vitality or resisting power, we have a remedy for this condition.Experience proves that we have such a remedy in veratrum. Ourprescription, then, for this active, sthenic condition, as marked by the
full, boundingpulse, will be this agent, and we will administer it asfollows:
Vera t rum 1 drachm.Sulphate of Morphia 1 gra in .Aqua 4 ounces. M.
Sig. Teaspoonful every one, two, or three hours as the symptomsindicate.
The morphia u sed is to coun ter act th e nau seat ing effects t ha t sometimesfollow th e use of vera tr um.
Jaborandi .—This is the remedy so highly extolled by some Eclectics,where the temperature is high, there is great excitement of the nervoussystem, an d where the skin is hot a nd dry:
Specific J aborandi 1 drachm.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 0The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 61/107
Aqua 4 ounces. M.Sig. Teaspoonful every h our .
Aconite.—While the average pneumonia patient has a full, strong,bounding pulse, th ere a re cases wher e just th e opposite condition exists;
th e pulse is small and frequent an d shows a defect in t he hea rt 's action,debility; the h ear t beats ra pidly to ma ke u p for wan t of power. We findthis pulse in children and patients of delicate constitution, andfrequently in old people. The heart needs a stimulant or tonic; in suchcases th e small dose of aconite slows the pulse and increases the tone of the heart by overcoming irritation and quieting the nervous system.Aconite in th e sma ll dose is not a depressa nt . The prescription her e willbe :
Aconit e 5 drops
Water 4 ouncesSig. Teaspoonful every h our .
Given in this way the heart is not depressed, nor the vitality of thepatient impaired. In the place of adding to the load the patient has tocar ry, we have relieved him of a p ar t of his bur den.
These three remedies form the foundation upon which we will build asuccessful treatment.
Bryonia.—This agent has been found of great value in diseases of thechest of an acute nature. When the pulse is hard and vibratile, andwhen the pain is sharp and lancinating, with flushing of the cheek, andthere is a hard, harassing cough, bryonia will be the remedy to giverelief. It a lso favors absorp tion of the exud at e. If t he pleu ra be involved,it is an additional reason for its use. It combines nicely either withaconite or veratrum, and can be dispensed with the sedative, or it maybe used separately, alternating each hour with the sedative. It shouldbe given in the small dose, not over five or ten drops in half a glass of water.
Asclepias.—This is another excellent remedy in diseases of therespiratory appara tu s, and occupies an import an t place in the t reat mentof pneumonia. It acts upon the sudoriferous glands, overcomes thedryness of the skin, relieves the tight, hard cough, modifies the sharppain, and h ast ens absorpt ion. It also ta kes the edge off the sharp pulse,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 62/107
adds t one t o th e hear t, an d quiets th e nervous system. To get t he besteffect s, give from five to ten drops in hot wa ter ever y one, t wo, or th reehours. It is especially useful in infant ile pneu monia with high fever an ddry skin.
Ipecac.—Ipecac, if given in small doses, is one of our best remedies inovercoming irritation of the mucous surfaces; and in children, wherethere is an irritating cough and the child is unable to obtain rest, thesmall dose, say five to ten d rops in h a lf a glass of wat er, will be foun d of great value.
Lobelia .—I would hardly know how to treat infantile pneumoniawithout the small dose of this old but valuable remedy. In those caseswhere the finer bronchioles become choked with the exudate, and thechild's breathing is labored, and there is a mucous rattle, I know of no
other agent that can take its place. In the adult, there is laboredrespiration, a sense of fullness and weight and oppression about theheart, while the pulse is oppressed or small and feeble. There isincrea sed secret ion of mu cus in t he respira tory passa ges, but th e patientseems unable to remove it. In these cases lobelia, five to ten drops, inwat er four oun ces, will give the best resu lts.
If the patient is seen early, few cases will need any other than theabove-na med r emedies, an d th e morta lity will be very low.
O c c a s i o n a l Re m e d i e s .— Macrotys.—When the patient complains of muscular soreness, or where there is a tendency to rheumatism,macrotys will prove an excellent agent, ten to twenty drops, in waterfour oun ces, a tea spoonful every h our .
Sanguinaria.—This is a good r emedy wher e th ere is a tickling sensa tionin the throat, resulting in an almost constant paroxysm of coughing. Ilike the action of nitrate of sanguinaria here better than that of thetinctur e and give,
Sa ngu inar ia 1/4 gra in .Aqua andSimple Syrup 2 ounces each . M.
Sig. Teaspoonful every h our .
Phosphorus .—Where the pulse is small, the skin cool, and temperature
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 2The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 63/107
subnormal, this is a good remedy to start up the fires and give thepat ient a cha nce for his life. Very ru sty spu tu m is also an indicat ion forth is agent.
S ticta Pulm onaria .—Where th e pat ient h as a ha rd, ra cking cough, with
pain in t he occiput an d between t he sh oulders, we should not forget t hisremedy; ten to thirty drops, to water four ounces, a teaspoonful everyhour.
C o m p l i c a t i o n s .—Gastro-Intestinal.—In some cases there is greatirritation of the stomach and bowels; so much so that neither food normedicine is retained. The tongue is red at the tip and edges, and it isnarrow and elongated; there is nausea and vomiting and retching,tenderness on pressure over the epigastrium, and frequently diarrhea.Respiration is shallow and painful; skin dry, and constricted.
Fortu na tely the rem edies t o give relief to th is irrita ble condition ar e alsouseful for the primary lesion—aconite and ipecac, with a sinapism overthe epigastrium. If the nausea persists, bismuth in mint-water will beuseful. Small bits of ice may be held in the mouth, thus allaying thethirst a nd quieting the nausea.
In place of this condition there may be atony; in either case, absorptionof food a nd rem edies is pr event ed. Here t he t ongue is br oad an d pa llid,with paleness of the mucous membranes, or there may be a heavy,pasty coat ing upon th e tongue. The temperat ur e is not so high as in th e
form er case, nor t he cough so cont inuous or h ar ass ing.
Nux Vomica.—If the tongue be broad and pale, with pallidity of themucous surfaces, five to ten drops of nux, in water four ounces, atea spoonful every h our , will be good m edica tion.
Podophyllin .—If the tongue be broad and full, with a dirty, yellowcoating, and a sense of fullness of the abdomen, and if there is a dirty,yellow, doughy skin, the bowels sluggish, the respiration oppressed, thesu perficial veins full a nd promin ent , Podoph yllin will do good s ervice. It
ma y be given in one-half-gra in doses every two, thr ee, or four hour s, tillthe bowels open and the tongue cleans, or we may use the secondtr itur at ion, th ree to five gra ins, in t he sa me way.
Antiseptics .—During some epidemics, there seems to be a tendency tosepsis, and t he sympt oms a re of th e typhoid type. The pr incipa l remedies
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 64/107
in th ese cases a re th e ant iseptics.
Sulphite of Sodium .—Where the tongue is moist, with a nasty, dirtycoating, a saturated solution of sulphite of sodium in table-spoonfuldoses every th ree h our s, is a m ost excellent rem edy.
Chlorate of Potassium .—Where the tongue has a moist, yellow, pastycoating, with a fetid breath, a saturated solution of potassium chloratean d phospha te of hydra stin , will be th e best rem edy.
Acids .—If the tongue be dry and grown, with redness of the mucousmembranes, then hydrochloric acid, C. P. 10 to 20 drops, to water andsyru p, two oun ces each, will replace the alka lies.
Echinacea .—When the tongue is full and of a dusky hue, and the
tissues of the same dusky color, echinacea from one to two drams, towat er four oun ces, a tea spoonful every hour , gives good result s.
Baptisia .—The tissues appear as though frozen, are full and dusky; thetongue is full an d pur plish in cha ra cter , while the expectorat ion is da rk ,thin, and of a prune-juice order; there is diarrhea of an offensivecha ra cter ,—with t hese conditions, bapt isia becomes a prominent agent :ten to thirty drops of the tincture, to water four ounces, a teaspoonfulevery h our .
Wrongs of th e N ervous S ystem .—Irr itat ion of th e ner vous system, with atendency to meningitis, will give us the flushed face, bright eyes, andcontracted pupils; the patient is restless, uneasy, and wakeful; thetemperature is high. To the appropriate sedative we add ten to thirtydrops of gelsemium , and give a tea spoonful every hour .
Rhus Tox.—Where there is irritation of the cerebro-spinal centers—aswill be shown by the sharp stroke of the pulse, the restless, irritablecondition, the sudden starting in the sleep, the contracted and pinchedfeatures—rhus tox. will be our most valuable remedy; five to ten drops,
in water four ounces, to which has been added aconite five drops; ateaspoonful every hour.
Belladonna .—There is not infrequently marked capillary congestion.The pulse is obstructed and feeble, the face is flushed and dusky, theextremities are cool, the eyes dull, and the pupils dilated, where the
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 4The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 65/107
pa tien t is inclined to doze or sleep m ost of th e time. With th ese evidencesof general congestion, we give belladonna 10 drops, to water fouroun ces, a tea spoonful every hour .
Quinia .—If periodicity is a marked feature and the tongue is moist,
quinia an d h ydrast in will prove beneficial.
Strychnia .—Where there is a feeble pulse, with tendency to heart-failure, strychnia, one-thirtieth grain every four or five hours, isdemanded.
Local Applications.—It will be difficult to convince some of the olderpra ctitioner s th at a pn eum onia pa tient will do as well, if not better , witha light flannel bandage over the chest, than the mush-jacket or the oldhop-poultice. I am sure that many patients have been harmed by the
improper application of the poultice. Where they are allowed to growcold, th ere is great dan ger of chilling th e pat ient. If th ey must be used,always have two poultices made, and while one is on the patient, theoth er m ay be in a st eam er on th e stove, and a s soon a s one begins t o getcold, have the hot one at the bedside so that it may immediately beplaced upon th e chest as th e oth er is rem oved.
A bett er pla n, h owever, is to sprea d a flann el or cott on cloth with lard,and dust emetic powder over the surface, and, after heating this,envelop t he ches t; or if but one lun g be involved, cover t he affected side.
Where the skin is very tender, this powder sets up too great anirritat ion, an d we resort to oth er mea sur es.
Libradol spread upon a cloth, and applied hot, will give good results. Itshould be renewed night and morning. These latter applications arelight, do not oppress the patient, are easily applied, and there is nodan ger of ta king cold while cha nging th em.
BRO N CH O - P N EU MO N I A .
S y n o n y m s .—Capillary Bronchitis ; Lobular Pneumonia; CatarrhalPneumonia.
Def in i t ion .—An in flam ma tion of th e ter min al bronchi, air-vesicles, andinterst itial tissu e of a few or m an y of th e lobules.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 5The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 66/107
Et i o l o g y .—This is peculiarly a disease of early childhood and oldpeople, though enfeebled vitality and prolonged sickness of any kindpredisposes to broncho-pneumonia. In children it is especially apt tofollow the infectious diseases that affect the bronchi and are attended
by a cough, such as measles, whooping-cough, influenza, diphtheria,an d scarlet fever.
Tubercular patients, especially where the lungs are involved, are.frequent subjects of this form of pneumonia. Typhoid fever, small-pox,an d diseases of like cha ra cter , ar e not infrequen tly complica ted with t hisdisease.
The inhalation of particles of food or broken-down material from thethroat, as from diphtheria or tonsillitis, may give rise to inflammation,
an d is kn own as inh alat ion or deglut ition pn eum onia.
The disease is seen most frequently in the winter and early spring-mont hs, when th e weat her is ma rked by sudden changes.
P a t h o l o g y .—The pathological changes are essentially those of bronchitis a nd of pneum onia in a bout eight y per cent of the cases, bothlun gs being involved.
The pleural cavities usually contain their normal amount of fluid,
though their surfaces, pulmonary and parietal, may exhibitinflamma tory pat ches—fibrinous pleurisy.
In most cases, the lung crepitates on handling, and will float whenplaced in water, though the small, mahogany-colored nodules founddistributed throughout the lung, when excised, sink in water. Thenodules are found in greater numbers in the posterior part of the lowerlobes. These nodules vary in size from a pinhead to a pea, and, whenpressed, a small amount of blood exudes. These nodules may be sonumerous as to resemble a hepatized lung; where these indurated
patches ar e few in nu mber, the int ervening lung tissue ma y be norm al,th ough usu ally it is congested or edema tous.
Surrounding the nodules, emphysematous lung-tissue is notinfrequ ent ly seen, with occas iona l collapsed a rea s—at electa sis.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 67/107
The bronchi, small and medium-sized, are the seat of catarrhalinflamm at ion, th e walls of which a re swollen an d infiltr at ed with roundcells. The exudate within the bronchi consists of leukocytes and micro-organisms.
Northrup speaks of a mechanical dilatation of the smaller bronchi,which occur s m ost frequ ent ly in th e lower lobes.
S y m p t o m s .—Primary Form .—Though a much rarer form than thesecondary, broncho-pneumonia sometimes begins as an acute primaryaffection, the symptoms being those of acute bronchitis. The usualprodroma l symptoms, ma laise, with loss of appet ite, precede th e initialchill, which is followed by febrile rea ct ion. The tem perat ur e is usua llybetween 100° and 103°. though in exceptional cases it may reach 104°or 105°.
A hard, dry cough, with a sense of constriction in the chest,accompa nied by a sh ar p pain, is a cha ra cter istic feat ur e. The respira tionis rapid, and in children may reach 60, 70, or even 80 per minute.Dyspnea is quite ma rk ed. The pu lse var ies from 120 to 140 per m inut e.Expectoration attends the cough after the first twenty-four hours, atfirst a glairy mucus, frequently tinged with blood, which later becomesmucopuru lent in chara cter.
S econd ary Form .—This is the form usually seen, and comes on more
gradu ally, th e ear lier symptoms being t hose of the preceding bronchitis.Not infrequently, the pneumonia complication is not suspected duringlife.
The first symptom to call attention to the true nature of the disease isthe sudden increase in the respiration, quickened pulse, and cyanoticappearance. The expectoration is muco-purulent in character. Thecough is hard and harassing, and is accompanied by pain andcons tr iction of th e ches t.
P h y s i c a l S i g n s .—In the primary form, the sibilant and mucous ralesar e the most prominent signs, the subcrepitant appearing as t he diseaseprogresses and the areas of the vesicular changes increase. In theseconda ry form , th e subcrepita nt fine, moist r ales ar e usu ally present.
Palpation usua lly reveals local a rea s of vocal fremitus .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 7The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 68/107
Percussion reveals areas of dullness, where much consolidation exists,but wher e deep-sea ted a nd confined to small spots, is negat ive.
C o m p l i c a t i o n s .—Cerebral complication is not a very rare occurrence,
the child becoming restless, the face is flushed, and the head is rolledfrom side to side; delirium m ay ensue, while a convu lsion is not u nu sua l.
Pleurisy may occur, and tuberculosis is not uncommon. Gangrene andabscess of th e lung is a m ore r ar e sequela.
D i a g n o s i s .—The diagnosis is readily made as a general rule. Thepersistent bronchitis with sudden rise of temperature, the dyspnea,hurried respiration, and the rapid pulse, together with the physicalsigns, a re su fficient to determ ine th e cha ra cter of the disease.
P r o g n o s i s .—The prognosis is favorable except in feeble, delicatebabies, an d in very old people.
T r e a t m e n t .—The treatment is similar to that of bronchitis or lobarpneumonia . The specific rem edies being given for specific conditions.
Aconite.—Where there is fever, with small, frequent pulse, there is nobetter remedy than aconite. This may be combined with any one of aha lf-dozen r emedies th at ar e frequent ly called for.
Rhus Tox.—Where t her e is restlessness a nd t he child is un able to sleep,the pulse quick and sharp, rhus goes nicely with the sedative aconite.Where the smaller tubes are choked up, and oppression is a markedfeat ur e, lobelia is th e rem edy par excellence.
Ipecac.—We sometimes meet a case where there is marked irritation.The cough is hacking and persistent; the tongue is red and pointed; thepulse is quick and hard; the child is cross and peevish. Here ipecacalone, or combined with t he sedat ive, is su re t o give good r esult s.
Tartar Emetic.—Where the cough is loose, and the bronchioles arechoked with mucus, there are few, if any, remedies that can take theplace of tartar emetic. It was a most effective remedy with my father,who used it for over forty years with the best results. Take about one-ten th of a gr ain of th e cru de dru g to a h alf a glass of wat er; teaspoonful
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 69/107
every hour . If na usea or vomit ing follow, add more wa ter .
CHR ONIC INTERSTITIAL PNE UMONIA.
S y n o n y m s .—Cirrhosis of the Lungs; Fibroid Pneumonia; FibroidInduration.
Def in i t ion .—A chr onic inflamma tion .of th e lungs, in which t he n orm alair-cells are replaced by fibrous or connective tissue, followed byindur at ion a nd a tr ophy of th e lun g.
Et i o l o g y .—It is not definit ely kn own wh y fibroid cha nges t ake place innormal tissue following inflammatory conditions. The disease is nearlyalways seconda ry, th e plast ic exudat e accompa nying th e prima ry lesion
becoming organized into fibrous tissue in place of being removed by theabsorbents. It may follow several pulmonary affections; thus, in lobarpneumonia, where resolution is long delayed, the exudate fills the air-cells, becomes organized, and the parenchyma of the lung is changedint o fibrous or conn ect ive tissue.
Broncho-pneumonia often precedes the disease, while atelectasis andchr onic bronchit is a re n ot infrequen t ly followed by cirr hosis of th e lun g.
Pleurisy.—Chronic pleurisy may be the forerunner of the lesion, the
process of tissue formation extending into the lung from the thickenedpleural m embrane.
As a primary cause may be mentioned long-continued inhalation of different kinds of dust; thus we have cirrhosis or phthisis from theinhalation of dust in the stoneyard, or from workers in iron, brass, orcoal, flour-mills, etc.
P a t h o l o g y .—The disease is nearly always confined to one lung,though, in very rare cases, both lungs may be involved, while localized
areas ar e the rule.
The a ffected lung becomes a tr ophied, an d, in extrem e cases, m ay be n olarger than the closed hand, Anders recording a case where themeasurements were only three by four inches. As a result of theshr inka ge of lung-tissu e, the h ear t, especially th e right side, un dergoes
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 6 9The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 70/107
hypertrophy. The indurated lung presents a rough or nodular surface,is hea vy, dense, tough, an d r esisting on section.
A cut surface shows the tissue dry and glistening and of variedappea ra nce, according t o the char acter of the irr itan t. The blood vessels
are atrophied, and, in some cases, show but a trace of their character.The alveolar structure in extreme cases is replaced by fibrous tissue.When tuberculosis exists, cavities of varying size and number arefound.
The fellow lung generally undergoes compensatory emphysema. Thepleura is generally very much thickened, and adhesions more or lessextensive between its free surfaces are found, and not infrequentlybetween th e pleura an d pericar dium.
S y m p t o m s .—When th e disease begins as a n a cut e pneum onia, th ere isnothing in the earlier stages to suggest its fibroid character. The usualtime for convalescence, from seven to ten days, having passed, and thedyspnea becoming a chief symptom, and the cough persistent orpar oxysma l, th e tru e na tu re of th e disease sh ould be suspected.
As it ordinarily begins, cough and dyspnea are among the firstprominent symptoms. On slight exertion, as climbing stairs or rapidwalking, the breathing becomes labored and hurried and the coughdistressing. The patient gradually loses flesh and strength, and the
common verdict is consumption. When the bronchi become dilated, thecha ra cter istic symptoms of bronchiecta sis ar e presen t.
There is n o fever; in fact, a subnorma l temper at ur e is quite comm on.
P h y s i c a l S i g n s .—Inspection shows a r etr action of th e affected side, anobliteration of the intercostal spaces due to the ribs closing the opening,an d a n imm obility of th e affected side ma de prominent by mensu ra tion.The heart will be inclined to the affected side. The chest wall isprominent on t he sound side, due to compen sat ory emph ysema.
Percussion .—Percussion shows a marked, difference in the twosides,—dullness or flat ness on th e a ffected side, with a tympa nitic notewhere a cavity exists , or due t o a dilated bronchus ; on th e opposite sideth ere is hyper-resonan ce.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 71/107
Auscultation .—Various sounds are revealed by auscultation. Wherecavities exist, t he cavern ous or am phoric soun d will be hea rd, other wisethe respiratory sound will be feeble and distant. Bronchial breathing isth e rule.
D i a g n o s i s .—The diagnosis is n ot rea dily ma de ear ly in th e disease, butas retraction of the affected side becomes prominent and the physicalsigns alrea dy noted ar e present , the diagnosis becomes ea sy.
P r o g n o s i s .—The disease is not curable, though life may be prolongedfor years. Recurring bronchitis is apt to accompany the disease, andacute pneumonia of the opposite lung may terminate the life. Rarely,deat h r esults from failure of th e right hea rt .
T r e a t m e n t .—The tr eatm ent consists in secur ing a better n ut rition a nd
building up the general health; good, nutritious food, an outdoor life ina suitable clima te, one where t here is a ma ximu m am oun t of sun shine,modera te a ltitude, and where t he clima te is dry.
The medicinal treatment will be symptomatic, selecting remedies forrelief of cough an d su ch oth er cond itions a s ma y ar ise.
P ULMONARY HE MORRH AGE.
S y n o n y m s .—Hemoptysis ; Broncho-pulmonary Hemorrhage:Bronchorrha gia; Pn eumorrha gia.
Def in i t ion .—An expectoration of blood, due to hemorrhage from themucous membrane of the bronchi, trachea, or larynx, and more rarelyfrom erosion or ru ptur e of cap illar ies in lung cavities or par enchyma toustissue.
B r o n c h o r r h a g i a .—When t he h emorrh age is from th e bronchial tu bes,the term bronchorrhagia should be used, while an escape of blood into
th e air-cells and interst itial tissue is known a s pneu -morrha gia.
Et i o l o g y .—Although hemoptysis is not necessarily a serious condition,occasionally occurring in young persons of seemingly good health, it isusually one of the early symptoms of pulmonary tuberculosis, andshould suggest t o th e physician a th orough examina tion of his pa tient .
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 72/107
The hemorrhage may result from congestion of the lungs, due either topulmonary lesions or from cardiac derangements, especially mitralaffections. In capillary bronchitis, not infrequently the distendedcapillaries give way, and hemorrhage results. Broncho-pneumonia,
especially when it is t he forer un ner of tuberculosis, may a lso be a cau se;severe congestion of the bronchi or ulceration of the larynx, trachea,and bronchi may also give rise to it by erosion of some of the arterialtwigs. It m ay accompan y ma ligna nt affections, infectious fevers , scur vy,purpura hemorrhagica, hemophilia, and other lesions. Cancer of thelung, gan grene, and a bscess mu st be regar ded as cau sal factors.
Pulmonary apoplexy, or an escape of blood into the air-cells andinter stitia l tissue, with or with out lacera tion of th e paren chyma , may bediffuse or circumscribed. It may be due to penetrating wounds or
ru ptu res of a t horacic an eurism.
Vicarious hemoptysis is most likely an early symptom of tuberculosisrat her t ha n a substitute for t he menstr ua l flow.
P a t h o l o g y .—There is, in most cases, rupture of the capillaries of thebronchial mucous membranes, which at first are swollen and red, butsoon become very pale. If tubercular cavities are formed, a rupturedaneurism is sometimes seen, or large bloodvessels eroded by ulceration.If pulmonary apoplexy has existed, the parenchyma may be lacerated;
oth erwise, th e air-cells a nd in ter stit ial tissue a re infiltra ted with blood,which gives th em a reddish-brown cast .
S y m p t o m s .—Usually the hemorrhage comes on suddenly, generallyafter some severe exert ion, or u ndue excitem ent from coughing, or greatvocal effort; while at other times it comes on when least expected, asduring sleep. One of my cases invariably had his hemorrhage aftergoing to sleep, though du ring t he da y his labor wa s quite s evere.
The first evidence of the hemorrhage is a welling up in the mouth of a
warm, salty fluid. The quantity varies greatly, though alwaysappearing to th e patient m uch lar ger t ha n it rea lly is. It m ay be th at amouthful may be coughed up every few minutes for an-hour or more,th en cease for severa l days or weeks. Again, an occas iona l mouth ful willbe expectorat ed for s evera l days in su ccession. Where t her e is a r upt ur eof an aneurysm there may be an alarming gush of blood that proves
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 73/107
rapidly fatal. One such case occurred in my practice about ten yearsago, when a child, suffering from pulmonary tuberculosis, suddenlystartled the mother by a frightful gush of blood, and died within fiveminutes.
Where the hemorrhage is profuse and prolonged, there is usually moreor less dyspnea, th e patient assu ming a distressed appear an ce an d soonbecoming anemic. The blood is usually bright red and frothy, containingair-bubbles, though where the blood wells up in the mouth withoutcoughing, th e pat ient is a pt to swallow more or less of it, an d when th isis spit u p or vomited it will be dar k a nd clott ed.
D i a g n o s i s .—This cons ists in det erm ining th e sour ce of th e hemorr ha ge.That from the lungs and smaller tubes is bright red and frothy. Fromthe posterior nares and pharynx, the expectoration is streaked with
blood and is airless. Fr om t he st oma ch, the blood is dar k a nd clott ed.
P r o g n o s i s .—Although hemoptysis usually signifies tuberculosis, it isnot necessarily of this character, and the patient may live for years,finally dying of other lesions. I have in mind a lady who, thirty-fiveyears a go, had s evera l hemorrh ages, and of whom it was sa id she woulddie early of consumption, who is still living, and has two growndaughters.
While alar m is usu ally felt by th e pat ient, immediat ely fat al resu lts very
seldom occur. I have known of only one such case in twenty-five yearsof practice. The prognosis, then, as to life, is generally favorable, savefrom the rupture of an aneurysm or erosion of large branches of thepulmona ry art ery.
T r e a t m e n t .—The patient should be placed in the recumbent position,an d his fear s a llayed as to th e resu lts of his a tt ack. All excitemen t is t obe avoided and the patient encouraged as to the outcome. Small bits of ice may be swa llowed, an d cold drin ks encour aged. Ga llic acid in five toten grain doses ma y be given every th irty or sixty minu tes, or a mixtur e
of oil of cinnamon and equal parts of oil of erigeron may be given, fiveto ten dr ops. on sugar , every twent y, th irty, or sixty minu tes.
Should the hemorrhage be active, with a full, strong, bounding pulse,add tincture of veratrum 1/2 drachm to water four ounces, and give atea spoonful every ha lf hour u nt il an impression is ma de upon th e liear t,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 74/107
when th e rem edy should be given every one or two hour s.
If the hemorrhage is passive in character, carbo. veg. will be a goodrem edy. Dr. Scudder placed great reliance upon t his a gent, an d, from itsuse in other passive hemorrhages, I would advise its use. Of the first
trituration, give two or three grains every hour. Mangifera indica isused where the hemorrhage is passive in character. Dose, three to fivedrops in wat er, every one, two, or t hr ee hours.
Lycopus Virginicus is a favorite remedy with Eclectics, and may begiven as a n infusion or th e spec. tinctu re. Wher e th e hemorrh age is dueto ca rd iac lesions , cactu s, digita lis, and like rem edies, will be given. Onemust not forget ipecac in these cases. It may be given to arresthemorrhage, but is especially useful during the interim of attacks. Thepowder in gra in doses or t he spec. tin ctu re m ay be given.
Of the domestic remedies, salt and alum should not be overlooked.Following an attack of hemorrhage, the patient should be kept quietand in the recumbent position for a few days, especially when thehemorrhage has been severe, and remedies given to counteract the lossof tone due t o th e hemorrh age.
The adm inistra tion of iron, th e bitt er tonics, an d a nu tr itious a nd eas ilydigested food will be good t rea tm ent . The pat ient, as he gains str ength ,should ta ke light exercise a nd be mu ch in t he open a ir. To allay fear of a
fut ur e hem orr ha ge, it is well to provide th e pat ient with a few ten-graingallic-acid powders, with instr uction to ta ke one a t th e first sympt om of an a ttack.
P ULMONARY ATE LE CTASIS.
S y n o n y m s .—Apneumatosis; Collapse of the Lung.
Def in i t ion .—A collapse of the air-vesicles of the whole or part of a
lung, an d which m ay be eith er congenita l or a cquired.
Et i o l o g y .—Congenital.—This form is usually due to causes thatprevent a prompt and complete establishment of the function of respiration a t birth , rath er th an disease of th e pulmona ry organs. Thusa protra cted la bor, a compr ession of the cord, or a placent al sepa ra tion,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 75/107
a premature birth, or a plugging of the bronchioles by mucous or liquoram nii, where t he child draws int o th e lar ynx these secret ions du ring aninspira tory effort before th e mout h h as clear ed the m at ern al out let, ma ygive rise to at electa sis.
When a cquired, it is always a seconda ry a ffection, a nd is usu ally due toobstruction or compression.
Cases due to obstruction are those preceded by measles, whooping-cough, diphtheria, influenza, bronchitis, or broncho-pneumonia; thebronchioles becoming filled with a viscid mucus or muco-pus, the airfails to ent er t he vesicles, and as soon a s t he a ir alrea dy present escapes,or is absorbed, collapse t akes pla ce.
When due to compression, it is from pleural or pericardial effusions,
anasarca, cardiac hypertrophy, or abnormal growths. Conditionsweakening the respiratory functions also favor atelectasis; thusparalysis of the pneumogastric nerve, enfeebled vitality, as in rickets,poor chest development, feeble inspiratory muscles, and when theenvironmen t ten ds t o lower vita l force.
P a t h o l o g y .—The collapse may involve quite a large area, diffuseatelectasis, or it may be confined to small patches, lobular atelectasis,the former being more marked when congenital. The affected portionsare airless, do not crepitate, and sink when placed in water. They are
slightly depressed from the general surface of the lung, are dense, andof a dark bluish or purplish color; when cut, a dark liquid may bepressed from t heir su rface.
If the disease is recent, the collapsed portions, after death, may beinflated through the bronchus; but if of long standing, the vessel istotally destroyed. The pleura usu ally rema ins norma l.
S y m p t o m s .—The symptoms are chiefly those of imperfect breathingand defective aeration of the blood, the severity of which depends upon
the rapidity of development and amount of lung tissue involved. Incongenital cases, the child comes into the world more or lessasphyxiated, the respiration is labored, and the child is more or lesscyanotic. It appears feeble, sleeps most of the time, nurses withdifficulty, or not at all, and has a feeble cry, or moans in its sleep. Thesurface is cool; the temperature normal, or subnormal. Muscular
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 5The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 76/107
twitching ma y be th e forer un ner of convu lsions a nd dea th .
In a cquired cases, the pr imar y lesion m ay so oversha dow th e at electa ticcondition as to be entirely overlooked, especially when but few vesiclesare involved. If preceded by bronchitis or broncho-pneumonia, which is
genera lly th e case, a nd if th e lesion be exten sive, th ere will be a suddenaggravation of all the symptoms. The breathing becomes very rapid, isshallow and arhythmic. The patient is restless, the nose, ears, andfinger-tips become blue, th e extrem ities ar e cold, an d t he t empera tu re isoften subn orm al.
The ph ysical signs depend upon t he exten t of th e collapsed t issue; thu s,if the patches are small and involve both lungs, the signs are negative,while if large patches are involved, the physical signs are those of aconsolida ted lun g.
D i a g n o s i s .—In th e congenita l form , where m ar ked en ough to give riseto characteristic symptoms, the diagnosis is comparatively easy. Theacquired form, however, is often quite difficult, associated as it is withcapillar y bronchitis, cat ar rh al pneu monia, an d lobar pn eum onia.
The sudden appearance of grave symptoms in bronchitis—such asquick, sha llow brea th ing, ra pid pu lse, cyan ot ic discolora tion, with fa ll of temperature—is the most important diagnostic feature. The absence of fever would be import an t in distinguishing it from pn eum onia.
P r o g n o s i s .—If congenital, and the child be feeble or premature, or thefetal circulatory openings remain unclosed, the prognosis isunfavorable; if, however, the lesion is slight and restorative measuresar e ear ly used, the pr ospects ar e more hopeful.
In acquired atelectasis, the prognosis is usually grave, though notnecessa rily fat a l. When th e result of whooping-cough or s evere broncho-pneumonia, th ere is usua lly a fatal t erminat ion.
T r e a t m e n t .—In infants, the air-passages should be cleared, and,where possible, artificial respiration should be practiced, and the childprevented from remaining too quiet. Its sleep should be disturbed atfrequent intervals, and crying and coughing provoked, thus securingforced inspiration. In premature births, the incubator has beensuggested as a possible means in prolonging life until nature can carry
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 77/107
on t he vital processes un aided by ar tificial hea t.
In the acquired form, in addition to the measure used for the primarylesion, capillary bronchitis, lobar pneumonia, whooping-cough, etc., thepatient should be instructed to change his position frequently, to avoid
lying on t he back for m ore t ha n a few minut es at a t ime, an d to practicefull inspiration at frequent intervals. In extreme cases, inhalation of oxygen is t o be advised.
P ULMONARY EMP HYSEMA.
Def in i t ion .—A dilat a tion of th e a ir-vesicles or a ru ptu re of th e vesicles,allowing the air to escape into the connective tissue. The forms of emphysema are: Hypertrophic or large-lunged emphysema, atrophic or
small-lunged emphysema, and compensating emphysema.
Et i o l o g y .—While it is tr ue t ha t, in ra re cases, emph ysema h as occur redwhere there has been no apparent cause other than a feeble conditionof the lung tissue, the strain of normal respiration being too great forthe vesicles, the common and almost invariable cause is the result of severe straining due to disease of the respiratory apparatus, or to thephysical exertion necessarily used in certain lines of work. Thus theblowing of wind instruments, or the strain upon the lung as used byglass-blowers.
The most frequen t cause is th e violent st ra in at ten ding the pa roxysm of coughing in bronchitis, whooping-cough, or asthma. Although found inall ages, it occurs more frequently after middle life, and more frequentlyin males than females, the greater exposure among the former readilyaccoun t ing for th e differen ce in sex.
P a t h o l o g y .—The characteristic change in the lungs is the loss of itselasticity from over-distention of the air-vesicles, and consequentweakening of the elastic tissue of the alveolar septa, As a result, the
lungs are of undue size, being greatly distended, and do not collapsewhen the chest is opened. The apices project above the clavicles, whilethe diaphragm is displaced downwards. The voluminous lungs crowdth e th ora x, giving it th e cha ra cter istic bar rel-sha ped th ora x.
In color, the lungs are gray, being almost bloodless, though they may be
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 7The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 78/107
streaked with pigment. To the touch they are soft, downy, and may piton pressure. They do not crepitate, and when placed in water floathigher than the normal lungs. The walls of the alveoli, from pressure,become very much distended and lose their elasticity. Often the septaare destroyed, causing the coalescence of several cells.
The bronchial mucous membrane shows chronic inflammation, and isfrequently bathed in muco-pus. The right heart is generallyhyper tr oph ied, due t o obstr uction of th e pulmona ry circulat ion.
Where there are pathological changes in a portion of, or in an entirelung, such as tuberculosis, adhesion pleurisy, and in lobar pneumonia,the other lung may become emphysematous from the increased work th rown u pon it, and is kn own a s compensa ting emphysema.
In elderly people, atrophy of the lung sometimes occurs, the alveolarwalls and septa completely atrophying; there is a coalition of air-cells,which gives rise to large a ir-sacs, though t he lung itself is m uch sm allerth an in health . This is known as senile emphysema.
S y m p t o m s .—There a re n o cha ra cter istic symptoms in t he ea rly stages,the disease coming on slowly and insidiously, the only symptoms beingth ose of th e primar y disea se, bronchit is, a sthm a , or wh ooping-cough .
The first notable symptom is dyspnea, which occurs often after slight
exertion, such as going upstairs or performing the daily duties morehurriedly than usual. A hearty meal may be attended by shortness of breath.
As the disease progresses, the dyspnea increases; at first the mostmarked obstruction is in expiration; but later, as in asthma, bothinspiration and expiration seem equally labored, and are attended bymore or less wh eezing.
Cyanosis.—As the disease progresses and the right ventricle becomes
involved, the patient takes on a cyanotic appearance. At first the lipsand fingers become blue, but as compensation gives way, or when thedyspn ea is severe, the face becomes p uffy an d very blue.
Cough .—This is due to the bronchitis, that usually precedes andaccompanies the emphysema, being worse in the fall and winter
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 79/107
months. Expectoration varies in quantity and consistency, andcorresponds to the type of bronchial inflammation. The general healthnaturally suffers, the patient losing flesh and strength. Thetemperature is normal or subnormal, while the pulse is feeble, thoughnot mu ch m ore frequent , save after exert ion.
The patient is slightly stooped, and becomes cachectic, owing to cardiacdistur ban ces with congestion of the viscera ; ther e is edema of the feet,th ough genera lly dropsy is ra re.
P h y s i c a l S i g n s .—Inspection reveals t he cha ra cter istic “bar rel-sha pedchest,” the thorax being rounder than when normal, the antero-posterior diameter being equal and sometimes greater than thetransverse. The sternum, scapulae, and clavicles are prominent. Theshoulders are drawn forward, and the patient appears stooped. The
interspaces of the ribs are widened on inspiration and expiration, andthe chest is raised and lowered as though a solid cage, rather thanexpan ded. The respira tory muscles ar e prominent.
The apex beat disappears, and epigastric pulsation is noticed. In theadvanced sta te t he veins of th e neck a re distended an d pulsat e.
Palpation reveals a diminished tactile fremitus, a feeble apex beat,which finally disappears, a distinct systolic shock over the ensiformcartilage, due to changes of the right heart, and a marked epigastric
pulsation.
Percussion gives a hyper-resonant or tympanitic sound, the usualcardiac dullness disappearing, owing to distention of the lungs; thenormal dullness over liver and spleen being much lower, owing todownward displacement.
Auscultation .—The vesicular respiratory murmur is lost, inspiration isshort, while respiration is prolonged. When bronchitis is present, therales peculiar to that affection are noticed. There is a pronounced
accent ua tion of the pu lmona ry second soun d.
D i a g n o s i s .—The diagnosis is comparatively easy, and scarcely can beta ken for any oth er disease. The cha ra cter istic “bar rel-shaped chest ,” th eabsence of the apex beat, the epigastric pulsation, the hyper-resonanceof the chest, the dyspnea and cyanotic appearance, are conclusive
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 7 9The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 80/107
evidence of emph ysema .
P r o g n o s i s .—While the patient may live for years, if too great physicalexertion is not used, the prognosis is unfavorable, the disease beingprogressive, fina lly term ina ting fat ally.
T r e a t m e n t .—Where possible, th e pa tient should be rem oved to a dry,equable climate. Any obstruction of the nasal cavities or pharynx bypolypi, adenoids, etc., should be removed. The diet should be carefullyselected, sugar and starchy foods restricted, and alcoholic beveragesprohibited. Such remedies as bryonia, ipecac, lobelia, sticta pul., tartaremetic, an d sa nguina ria will be useful in relieving t he br onchitis.
Cactus, strophanthus, crataegus, digitalis, and other cardiac remedieswill be used in th e lat ter s ta ges. Laxat ives an d diuret ics should be used
as m ay be indicat ed.
P ULMONARY ABSCE SS.
S y n o n y m s .—Abscess of th e Lungs; Suppura tive Pneu monitis.
Def in i t ion .—A collection of pus in the lung, accompanied bydegenera tion of tissu e.
Et i o l o g y .—Abscess of the lung is due to septic infection, followinginflammation. It may follow lobar or lobular pneumonia. It is prone tofollow aspiration or deglutition pneumonia, where septic conditions of nose and throat exist. Chronic tuberculosis is also accompaniedfrequ ent ly by abscess of th e lun g.
Embolic or metastatic abscesses are usually multiple, and are due toseptic material carried to the lung through the circulation, as fromma ligna nt endocar ditis, pyemia , pyoneph rosis, an d like cond itions .
They may be due to perforations from without, and the lodgement of foreign bodies, such as bullets, this being common during the war. Itma y also be cau sed by abscesses of other pa rt s, as of the liver, spleen, orto car cinoma.
P a t h o l o g y .—The abscess may involve one or more lobules or engage
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 81/107
almost an entire lobe. The favorite location is the lower lobes, and theright more frequently than the left. They are generally situated at theanterior portion of the lung, and when in contact with the pleura giverise to purulent pleurisy by direct infection. When the abscesses aresma ll, they may be scat tered t hr oughout th e entire lung.
S y m p t o m s .—The symptoms are not characteristic. The fever is of aseptic type, with chill an d n ight -sweat s. Cavity signs a re u sua lly noted.There is cough, with expectoration of fetid pus, in which shreds of broken-down lung-tissue may be seen. The symptoms of the primarydisease sh ould a lso be ta ken in to considerat ion.
P r o g n o s i s .—The prognosis should be guarded. Where the previoushealth has been good and the environments are first-class, the outlook is h opeful, especially when following a cu te diseases. The chronic form is
less favora ble.
T r e a t m e n t .—The treatment will be antiseptic and reconstructive.Calcium sulphide should be given four times a day. Echinacea may beemployed to correct septic processess. Iron, quinia, and strychnia as arecons tr uctive, may be of mu ch ben efit.
The patient should reside in a climate where he may be much in theopen air and sunshine, good, nutritious, and easily digested foodfur nished, a nd th e secret ing organ s kept in good condition.
G AN G REN E O F TH E LU N G .
Def in i t ion .—A Putrefactive Necrosis of the Lung, either circumscribedor diffuse.
Et i o l o g y .—Gangrene of the lung can only occur where the organ haspreviously been weakened, hence is always a secondary affection.Putrefactive bacteria thrive in the necrotic soil, but whether the cause
or the result of the necrosis is a mooted question. It may follow lobarpneumonia, aspiration-pneumonia, broncho-pneumonia, fetidbronchitis, thrombosis of the pulmonary artery, rupture of a bronchus,from an ulcera ted or can cerous esopha gus, from pressu re du e to tum orsor th ora cic an eurism, a nd from sepsis due to protra cted a dynam ic fevers.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 1The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 82/107
P a t h o l o g y .—In the diffuse, when due to lobar pneumonia or theplugging of a large bra nch of th e pulmonar y art ery, a lar ge part ; of th elung becomes a dar k, greenish brown, or a black, fetid, pulta ceous ma ss,from the center of which softening rapidly proceeds, forming anirr egular cavity, cont ain ing a foul-smelling, disgust ing, green ish fluid.
In the circumscribed form, the disease may involve one or both lungs,usually selecting the dependent portions, and the right more often thanthe left. The part affected assumes a dark-brown or greenish hue,becomes soft, and early assumes a fetid purplish mass; necrosisbeginning in th e cent er, a cavity soon form s. If locat ed n ear th e pleura ,pu tr efaction ma y occur , giving rise to pyopneum oth ora x. A bronchitisis always an accompanying lesion, the bronchi containing an offensivean d often pu tr id mucus.
Not infrequen tly th ere is foun d in conn ect ion with this lesion, abscess of th e brain, liver, an d spleen.
S y m p t o m s .—In addition to the symptoms of the primary disease, thecough becomes more pronounced, and is attended by profuseexpectoration of a peculiarly offensive character. When allowed tosta nd, the expectora ted ma terial separa tes into thr ee layers; th e upper,a yellowish, turbid brown froth; the middle layer, a clear watery fluid;and the bottom layer, the heavier material, blood, pus, and shreds of lung tissue. The microscope reveals putrefactive bacteria, pus, elastic
tissue, fat , crysta ls, an d gra nu lar ma ter ial.
The respiration is slightly increased in frequency, and the breath isoffensive. Where erosion of the blood-vessels occurs, hemorrhages takeplace, somet imes of an ala rm ing cha ra cter .
There is some fever present in all cases; the patient loses flesh andstrength, becomes anemic, chills and night-sweats follow, and theevidence of sepsis is pronounced. There is dullness on percussion in theear lier s ta ges, followed by the sign of cavity form at ion in lat er st ages.
D i a g n o s i s .—The intense fetor of sputum and breath, the character of th e expectorat ion, th e septic fever, a nd gr eat ema ciation, ar e symptomsth at can ha rdly mislead one in n am ing the disease.
P r o g n o s i s .—Though n ot necessa rily fat al, th e disease is a lways grave.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 83/107
Where the former health of the patient has been. good and there is notu bercular ta int, a nd th e pat ient is youn g or in m iddle life, recovery willoccas iona lly ta ke p lace.
T r e a t m e n t .—The treatment is largely antiseptic, and the Eclectic
materia medica is rich in antiseptics. First in importance standsechinacea. This should be given every one or two hours, two drams, towat er four oun ces, a tea spoonful at each dose. Baptisia, sodium sulphite,hydrochloric acid, and potassium chlorate, with hydrastis, will eachha ve their special indicat ions for u se. Eucalyptu s used with a n a tomizerwill be found useful as a local remedy. The appetite should beencour aged by nu x vomica, h ydrast in, chiona nt hu s, etc. The diet sh ouldbe nourishing, easily digested, and given at frequent intervals.Dra ina ge by sur gical mea ns will ha ve to be cons idered in some cases.
P ULMONARY EDEMA.
S y n o n y m .—Edem a of the Lu ngs.
Def in i t ion .—A transudation of serum into the air-vessels, and ofteninto the bronchi an d inter stitial tissu e of th e lungs.
Et i o l o g y .—The edema may be general or local, according to the causesgiving r ise to th is cond ition.
General edema depends upon active or passive hyperemia, morefrequently the latter condition. It may also be caused by feeble heart-action due to dilatation, degeneration, or to pericarditis. Hydremiaresult ing from hepa tic cirr hosis, chr onic nephrit is, cachexia, or pr ofoun dan emia, ma y also be responsible for pulmonar y edema.
P a t h o l o g y .—The lun g is h eavy, th ough when placed in wat er it float s.It pits on pressu re, an d, when incised, exudes a blood-tinged seru m. Theedema is most m ar ked at t he base an d dependent portions of th e lun g.
S y m p t o m s .—In addit ion to th e sympt oms of the disease giving r ise tothe edema, there will be rapid respiration, marked dyspnea, coughattended by expectoration of frothy, bloodstained, serous material.Cyan osis is often very pronoun ced.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 3The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 84/107
Percussion reveals marked dullness, especially over the dependentportion of th e lungs.
Auscultation gives rales of varying character. General dropsy mayfollow.
P r o g n o s i s .—This is always a grave disease, though, when the causescan be rem oved, a cure occas iona lly resu lts.
T r e a t m e n t .—The treatment is largely directed to the primary disease.Such remedies as apocynum, strophanthus, convallaria, and kindredremedies will afford some relief.
The bowels should be kept open, the secretion of the kidneysma inta ined, th ough n ot overstimu lated, an d such remedies employed as
th e case ma y ca ll for from da y to day.
V. DISEASES OF TH E P LEUR A.
PLEURISY.
S y n o n y m .—Pleuritis.
Def in i t ion .—An inflammation, either local or general, of the pleural
membrane.
Var ie t i e s .—Pleurisy has been classified according to its etiological,pathological, and clinical phases, thus: Etiologically, into primary andsecondary, tubercular, carcinomatous, septic, traumatic, etc.;pa th ologically, into circum scribed and diffuse, dry, plast ic, or fibrinous,serofibrinous, purulent, and hemorrhagic; clinically, into acute andchronic.
ACUTE P LASTIC P LEUR ISY.
S y n o n y m s .—Dry P leurisy; Fibrinous Pleur isy.
Et i o l o g y .—This form may be either primary or secondary, The formeris where the inflammation occurs as an independent affection in a
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 85/107
person previously healthy. It does not occur as frequently as wasform erly diagnosed, ma ny cases, no doubt , being du e to a rh eum at ic ortu berculous cons titu tion.
Although various micro-organisms are found in all forms of pleurisy,
notably the bacillus of tuberculosis, the streptococcus pyogenes, thestaphylococcus, and the micrococcus lanceolatus, no specific germ hasbeen found as a causal agent. Associated with the above bacilli, havera rely been foun d t he colon bacillus, t he pr oteu s vulgaris, Fr iedlan der'sbacillus, a nt hr ax ba cillus, influenza bacillus, a nd oth ers.
The most comm on etiological factor is cont ra ctin g cold, either by suddenatmospheric changes, or exposure in damp cold weather, or suddencooling after severe exercise. Mechanical injuries occupy a prominentplace as causal agents. The winter and spring months serve as an
important factor in producing the disease, owing, no doubt, to suddenatmospheric changes. The disease occurs more frequently among menthan women, owing to greater exposure of the former. The tubercularand rheumatic taint must also figure as having some bearing in thesecases.
The second form is due to an extension, either acute or chronic, of inflammatory conditions of the lung or neighboring parts. Thus itfrequently accompanies croupous pneumonia, and is often present inbroncho-pneumonia, and is not a rare complication in hemorrhagic
infarct, abscess, and gangrene of the lung, and cancerous conditions. Itis nearly always present at some period in pulmonary tuberculosis, andin not a few cases is t he first symptom of th at dread disease.
It m ay also resu lt from hepa titis, or cardiac inflamma tions. .
P a t h o l o g y .—Within twenty-four hours the inflamed membranebecomes reddened, congested, and deeply injected, showing manyminute ecchymotic spots. The membrane, at first dry, loses its glossyappea ra nce and becomes du ll an d lust erless, and soon is covered with a
fibrinous exudate of a yellowish or reddish-gray color. When theexudate is profuse, it presents a shaggy appearance, due to the frictionof the pleural surfaces. This exudate is composed of fibrin, leukocytes,blood corpu scles, an d seru m in sm all quan tit y.
While the inflammation is active and the exudate is profuse, adhesions
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 5The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 86/107
of the pleura take place, owing to the presence in the exudate of embryonic round cells which develop blood-vessels and connectivetissu e. If th e inflamm at ion is of a m ild cha ra cter , the exuda te u nder goesfat ty degener at ion, an d is absorbed.
S y m p t o m s .—The symptoms of fibrinous pleurisy exhibit a wide rangeof sympt oms. In one case a stitch in th e side is the only remind er of th edisease, while in another the pain is of an excruciating character andth e prostra tion so great a s to speedily term inate in death , and betweenth ese extr emes a re foun d every gra de of sympt oms.
When t he disease is of th e prima ry form , it is usu ally ush ered in with achill or chilly sensations followed by febrile reaction, though generallynot of a very severe type, the temperature ranging from 101° to 103°,an d in r a re cases going to 104° or 105°.
The pu lse is sm all an d frequent , from 100 to 120. The secret ions ar e allmore or less a rr ested, th e tongue being more or less coat ed, the sk in dry,th e ur ine scan ty a nd high-colored, an d t he bowels const ipated.
Of the local symptoms, the patient complains of a sharp, lancinatingpain in t he affected s ide, usu ally in th e r egion, of th e nipple. The pain isincreased if the patient attempts to take a full inspiration, or if theaffected side is moved. As a result, we find the breathing shallow or
jerking, an d principally abdominal. For t he sa me r eason th e pat ient lies
on t he a ffected side, th at th e membra ne ma y be held quiet.
A short, dry, hacking cough adds to the patient's suffering. With theappea ra nce of th e exuda te t he pa in subsides, with a n a meliora tion of allsymptoms.
In some cases, the patient is seized with a hard chill, and, with febrilerea ction, t he t empera tu re r apidly reaches 104° or 105°. The pulse is fulland bounding; the face, at first flushed, soon becomes pinched andanxious. The pain is intense; the patient refraining from taking a full
inspiration, has the appearance of great anxiety. The pulse soonchanges, becoming feeble though rapid, prostration is extreme, anddea th m ay follow in fort y-eight or sevent y-two hour s.
When the disease is secondary, the symptoms of the primary diseasemay so overshadow the affection of the pleura as to escape notice,
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 87/107
though the stitch in the side, or an “uneasy” feeling, will call attentionto the pleur a, an d a physical examina tion will reveal th e tr ue condition.
P h y s i c a l S i g n s .—Inspection r eveals the m ovement of th e ches t will, onthe affected side, very much restricted, especially during the first forty-
eight hours. Palpation confirms what inspection reveals, whilepercussion gives a n orm al sound in t he ea rly sta ge of the disease, to befollowed by some dullness when exudation occurs. Auscultation revealsth e cha ra cter istic an d chief diagnostic sympt oms of pleurisy.
In the early stage the friction sound is heard, due to the rubbing of thedry, inflamed pleural surfaces, and is more pronounced at the end of inspiration. With the presence of exudation, the friction sound isincreased and is heard during expiration and inspiration. If deepbreat hing is en joined, th e sound is more pr onounced.
D i a g n o s i s .—If care is used, pleurisy can scarcely be mistaken for anyother affection. The only diseases that might be mistaken for pleurisyare pleurodynia and intercostal rheumatism. If we remember, however,that the friction sound is always present in pleurisy, and never in theoth er t wo affections, we can rea dily distin guish t he one from the other .
P r o g n o s i s .—The prognosis is usually favorable, though in rare cases itmay speedily terminate fatally.
T r e a t m e n t .—The earlier Eclectics obtained prompt results in thetreatment of pleurisy, and those who can not get into the way of smalldoses and specific t inctu res will find t he old way a successfu l one. ‘Tistr ue it is ra th er u npleasant , though, if th e pat ient is suffering int ensely,he is ready to subm it to any medicat ion t ha t pr omises relief.
Where the t ongue was full, pallid , and dirty , th e old compoun d powderof lobelia or the a cetous em etic tinctu re wa s given, at first in sm all dosesto produce profound nausea, and then carried to free emesis. Thisproduced relaxation, lowered the temperature, and eased the sharp,
lancinating pain. If the pain was intense, sudorific tincture, compoundtincture of Virginia snake-root, was given in teaspoonful doses, in hotwater, every one, two, or three hours. This not only relieved the painbut brought on gentle perspiration, and the patient was soonconvalescent.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 7The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 88/107
In the place of this rather unpleasant medication, we give the smalldose, an d equ ally efficient rem edies in th e form of specific tin ctu res.
Aconite.—For the small, frequent pulse, aconite is the sedative to beselected, five gtts . of the tinctu re, t o wat er four oun ces.
Asclepias .—Associated, or rather combined, with the aconite; we willfind a sclepias an excellent rem edy. Where t he pa in is severe an d m ovesabout, is not const an t a t one point, an d th e skin hot, eith er dr y or m oist,no better remedy can be given. From ten drops to one dram should beadd ed to wat er four oun ces; a t ea-spoonful every hour.
Bryonia.—This is th e rem edy of rem edies in resp ira tory lesion with chest pain. In pleurisy, the sharp, lancinating, stablike pains will call forbryonia. Ten drops to half a glass of water, and a teaspoonful every
hour.
Rhus Tox.—Where the patient is restless, and unable to sleep, or startssuddenly in his sleep with a sharp stroke to the pulse, telling us of irrita tion of th e cerebro-spina l cent ers; wher e th e tongue is reddened a ttip a nd edges a nd th ere is elevation of th e papilla, th e sma ll dose of rh uswill give good resu lts . Ten drops, to water four oun ces.
Veratrum .—In an extreme case there will be high temperature, thepu lse will be full, strong, and bounding . The face will be flush ed, th ere
will be throbbing of the carotids, and the pain is intense, agonizing incharacter. In such a case veratrum, 1 drachm; morph. 1/2 grain, towater four ounces; a teaspoonful every hour until the pulse feels theforce of the rem edy, when it sh ould be given every t wo or th ree h our s.
Local M easu res.—In most cases, libradol will afford relief, and is moresat isfactory t ha n a blister . In fact, t he da y for th e a pplicat ion, of blister sin pleurisy has gone by, and when an active counter-irritant isdema nded, th e ap plicat ion of chloroform to th e spot implica ted will giverelief.
A hypoderm ic of morph ia m ay be called for, wher e th e pa in is int ense incharacter and we can not wait for the slow effects of internalmedicat ion. Pa in sometimes kills or at least ha stens a fat al ter minat ion,and the strength of the patient may be greatly prolonged by the timelyuse of a hypodermic injection. It is only to be used, h owever, in cases like
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 8The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 89/107
th e one just na med. Should the pa in ret ur n in four , five, or six hours, adiaphoretic powder, administered before the pain becomes intense, willbe of mu ch benefit.
SERO-FIBR INOUS P LEURISY.
S y n o n y m s .—Suba cut e Pleur isy; Pleu risy with E ffus ion.
Et i o l o g y .—The causes of sero-fibrinous pleurisy do not differ fromthose of plastic pleurisy, the difference in the character of the exudatebeing, no doubt, due to different degrees of intensity in theinflammatory process or to the influence of the various lesions withwhich it is so frequently associated, such as croupous and bronchopneumonia, pericarditis, hepatitis, peritonitis, nephritis, typhoid fever,
carcinomatous conditions, and especially tuberculosis. The frequencywith which tuberculosis is preceded by pleurisy or pleuritic symptomsbeing proof that the blood is of a poor quality, hence the changedcharacter of the exudate. This is especially so where the exudate ispuru lent or hemorrha gic.
P a t h o l o g y .—Sero-fibrinous pleurisy may be the further developmentof the plastic variety, the serous exudate following later, or theexudation may be serous from the beginning. The pleural surfaces arecovered with a fibrinous exudate, varying greatly in character. In one,
it is in the form of a thin, smooth coating, while in another it will beth icker, a nd a ssu me a rough or sh aggy appear an ce owing to th e frictionof its su rfaces.
If there be no adhesions, the effusion collects in the most dependentportion of the pleura, and, if small in quantity, physical signs will beabsent. The amount varies from a few ounces to a gallon or more. Thefluid is usually clear, of a pale yellow or brown-green color, thoughsometimes turbid, of alkaline reaction, and contains red and whitecorpuscles, leuk ocytes, endothelial cells, th rea ds of fibrin, a lbumen, a nd
sometimes cryst als of cholest erin .
As the fluid increases in quantity, certain mechanical changes takeplace. At first the lung is but slightly retracted; but as the fluidaccumulates, the lung is crowded backwards, and from continuedpressure becomes almost bloodless and airless—atelectatic. The
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 8 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 90/107
mediast inum is drawn toward t he opposite side by tra ction of th e soun dlung. The heart also is slightly displaced. Where the effusion is in theright side, the diaphragm is pressed, crowding the liver downward,while the stomach, colon, and spleen suffer in the same way, if theexudat e be in th e left pleur a.
S y m p t o m s .—Acute sero-fibrinous pleurisy begins insidiously. Therema y be slight chilly sensa tions for one or more da ys, followed by more orless fever, th e tem pera tu re r an ging from 101° in t he m orn ing to 103° atnight. The pulse is generally small, but frequent, from 100 to 120 perminute. The urine is scanty, partly due to the fever, and partly todiminished art erial pressure.
In r a re cases , the invas ion is cha ra cter ized by a s evere chill, followed byhigh temperature, marked arrest of the secretions, sharp pain of a
tear ing or lancina ting cha ra cter, and m ar ked dyspnea a nd an irritat ingcough. The pa in is locat ed-beneat h th e nipple, an d is often referr ed to asa stit ch in t he s ide, th ough, in some cases, it is diffused an d a ffects th eentire side of the chest. In rare cases, diaphragmatic pleurisy, the painma y be in t he epigast ric, hypochondriac, or lumba r region.
If the effusion has been very slow in forming, there may be but littledyspnea, although the accumulation be large; generally, however,dyspnea is a characteristic symptom, the breathing being short andcatching, and, where the effusion is rapidly formed, the dyspnea is so
great t ha t t he pat ient is often u na ble to lie down.
Cough is an attendant symptom, beginning in the early stage,gradually declining as the exudate increases, again to return withabsorption of th e fluid. The cough is ha cking in char acter, an d at ten dedwith an expectoration of scanty mucus, which is not unfrequentlystreaked with blood. If bronchitis develops, the expectoration becomesquite profuse, an d if pneu monia at ten ds, the spu tu m is ru sty colored.
In rare cases, where the primary disease is of a malignant character, or
some severe chr onic disease, as n ephr itis, th e pleura l sympt oms m ay beabsen t, or so oversha dowed as to rem ain un noticed un til discovered by aphysical examination.
P h y s i c a l S i g n s .—Since the general symptoms of sero-fibrinouspleurisy are often obscured by the primary disease, it is therefore
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 0The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 91/107
import an t to car efully note t he m ore definite an d positive physical signs,which qu ite accur at ely determ ine th e sta ge and extent of th e lesion.
Inspection .—Inspection r eveals t he sa me conditions th at we find in dr yor plastic pleurisy; namely, increased frequency of respiratory
movement; but as the exudate accumulates, restriction of therespiratory movement can be noted, due to the gradual compression of the lung, and when a very large quantity of fluid is present, therespiratory movement may be entirely absent. There will also be abulging of th e middle an d lower pa rt of th e chest , th e int ercosta l spacesbeing effaced and the anteroposterior diameter of the chest beingincreased. The diaphragm is depressed and the shoulder elevated, theaffected side being perceptibly larger than its opposite fellow.
If the left chest be involved, the apex beat will be seen to the right of
the median line, in the third and fourth interspace; and if the rightchest be involved, the impulse will be seen to the left of the nipple, oreven t o th e axillary line in th e four th an d fifth inter space. This is quitenoticeable if th e pat ient be lean , with th in chest-walls.
Where there is resorption, we notice a gradual return to the normalcondition, provided the exudate does not become organized, andadh esion t ak es place. In su ch cases t her e is at rophy of th e affected side,which may result in marked deformity, there being retraction with anarrowing of the intercostal spaces, and a dropping of the shoulder,
produ cing, more or less, a cur vat ur e, the concavity being on t he affectedside.
Palpation confirms the physical signs revealed by inspection. Thus theexpansion movement is found to be much restricted, the interspaceswidened and effaced, apical beat displaced to the right or left, ascendingto the side affected. Fluctuation and edema are rarely found. Vocalfrem itus diminish es as t he fluid accum ulat es, an d finally ma y disap pearentirely. As resorption takes place, palpation reveals the progressivesteps towards recovery, and where deformity of the chest occurs,
palpat ion outlines th e exten t of th e tissue chan ges.
Mensuration .—In m easu ring th e affected side, we are t o rem ember t ha t,in right-handed adults, the right chest is the larger; hence themeasurement must be as to the expansion of the two sides, the affectedside showing one or two inches in excess a t t he en d of expira tion. Wher e
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 1The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 92/107
th ere is gr eat effus ion, t he a ffected side, of cour se, also shows an excessin measurement. There will be but slight difference between the sidesduring inspiration owing to expansion of the sound lung, while theaffected lun g rem ains airless.
Percussion .—Ea rly in t he d isease, percussion gives negative resu lts; butas soon as the fluid amounts to one pint, dullness is elicited, at firstposteriorly, and in .rare cases, in the infra-axillary region, the amountof effusion can be determined from time to time by the increaseddu llness. The du llness beginnin g imm ediat ely below th e line of fluid, thesound soon becomes flat, like that produced from percussing wood;hen ce th e term wooden.
Beginning at the base posteriorly, the fluid, as it fills the cavity,assumes the form of the letter S, being higher posteriorly. Except in
extreme cases, a point of resonance, tympanitic in character, is found just beneath the clavicle, and is known as “Skoda's” resonance. Wherethere is large accumulation of fluid, the dullness extends quite adistance below the diaphragm, owing to the depression of theviscera—the liver on the right, and the spleen on the left—and shouldnot be confused in t he m ind of th e opera tor. Unless a very lar ge amountof fluid be present, change of position will vary the dullness and helpdeterm ine th e exten t of th e exuda te. In percussion we ar e also to bear inmind t he slight chan ge in th e hear t position.
Auscultation .—In the early stage, the breathing is shallow and jerking,owing to pain, and t he n at ur al respirat ory mu rm ur is diminished; verysoon, however, crepitation is heard, either in the inframammary, theinfra-axillary or the infrascapular region, and while it may be heardboth dur ing inspira tion a nd expirat ion, it is more pr onounced at t he endof inspiration. It may be dry and creaking as of new leather, or it maysimulate pneumonia. As the fluid accumulates, the crepitant andrespiratory sounds become fainter, finally disappearing, to be replacedby bronchial breat hing.
While vocal resonance is greatly diminished or absent over the effusedmaterial, it often partakes of a nasal character near the border of thefluid, and resembles, somewha t, t he bleat ing of a goat ; hence is ter medegophony.
With resorption, we have these adventitious sounds reversed as the
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 2The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 93/107
fluid disappears, though a return to the normal respiratory murmur isoften delayed for m an y weeks.
SPECIAL CLINICAL FORMS OF ACUTE: SERO-FIBRINOUSPLEURISY.—Tuberculous Pleurisy.—This form does not differ
ma ter ially from th at just considered, save th e additiona l presence of th especific tu bercle and th e more cert ain ter mina tion in deat h. This form isnea rly always seconda ry to pulmonar y tu berculosis, and is pr eceded bysuch a history. In rare cases, the primary lesion may be located in thepleura and consist of but few areas of tubercles, or there may beinnu mer able deposits of sma ll tubercles miliar y.
The disease may run its course as an acute-fibrinous pleurisy, or themore insidious form of the subacute variety, or become prolonged aschronic pleurisy. Either form may be complicated by pericardial or
peritoneal tuberculosis. The exudate is sero-fibrinous in character, andnot infrequen tly is st ain ed with blood.
Diaphragmatic Pleurisy.—In this variety the diaphragmatic portion of the pleura is involved, the pain being located at the insertion of thediaphragm to the tenth rib and extending to the epigastric region. Thepain is intense, the patient assuming the sitting posture, slightly bentforwa rd. Th e r espirat ion is short , cat ching, an d chiefly thora cic. Nau seaan d vomiting often occur , which great ly adds t o the pat ient's su ffering,as does the cough which attends it. The effusion is generally small in
quantity, and may be either plastic, sero-fibrinous, or purulent. If purulent, there may be bulging of the intercostal spaces. Thetempera tu re ra nge is high in th is form , the pain m ore exquisite, and t hepatient presents a more a nxious expression th an in an y oth er form .
Encysted Pleurisy.—As the result of adhesion, the effusion may occupytwo or more circumscribed pockets, which may or may not communicatewith each other, and may occupy various positions. The symptoms arenot pronounced and therefore may be quite difficult of detection. Wherepercussion reveals circum scribed dullness, with resonan ce a t its border,
the character of the lesion would be suggested, which would justify anexplora tory punctur e with a t rocar .
Interlobar Pleurisy.—This form is usually preceded by, or associatedwith, sero-fibrinous pleurisy, and results from adhesions cutting off theinterlobar spaces from the general pleural sac. The encapsuled exudate
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 3The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 94/107
varies in size from a small egg to a cocoanut, and is found morefrequently in t he right side tha n in t he left, an d between th e upper a ndlower lobus , nea r t he r oot of th e lung.
The sympt oms ar e not char acteristic, an d a fter a long period of ill healt h
the abscess may discharge into a bronchus, the expectorated pus beingthe first indication of a chest lesion. When the abscess is large, thesympt oms will be more like t ha t of abscess of th e lung.
Hemorrhagic Pleurisy.—This variety is where blood is found in theeffused fluid, and in sufficient quantity to be recognized by the unaidedeye, and is nearly, if not always, associated with tuberculosis orcarcinomatous conditions of the lungs or pleura, or to Bright's disease,cirrhosis of the liver, or low forms of acute, infectious diseases. It issomet imes accident al an d th e result of pun ctu re by th e tr ocar .
D i a g n o s i s .—If care be taken in noting the physical signs, there will befew mistakes made in the diagnosis, though several lesions might bemistaken for it, if examined superficially. We are to differentiate sero-fibrinous pleurisy from pneumonia. In pneumonia, in addition to thesudden onset , ther e will be a higher r an ge of tem pera tu re, deep flush of the cheeks, the pain will be more diffuse, the cough attended byexpectoration of rusty sputum, and there will be a dull sound ratherth an a flat one on per cussion. Ther e will be but litt le or no distent ion of th e th ora x.
Palpation will reveal marked fremitus, save where there is obstructionof a br onchus . Ausculta tion gives crepita nt an d sub-crepita nt ra les, an dlater bronchial breathing and no friction sound; and, lastly, there willbe no displacemen t of neighboring organ s.
Hydrothorax is usually associated with renal or cardiac disease, haslittle or no fever, absence of sharp, stitchlike pain, no friction sound, isoften bilat era l, an d t he specific gra vity of the flu id is below 1.015, whileth at of pleur isy is above 1.017.
Pericardiac effusion may be mistaken for sero-fibrinous pleurisy of theleft side, but the history of the former, which tells of rheumatism, themarked dyspnea, the feeble heart-sounds, the normal position of theheart, and the resonance heard on the posterior chest-wall and at thebase of the lung in the postero-lateral region, will distinguish the one
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 95/107
from th e oth er.
Tum ors a nd cysts r eveal a different hist ory. They ar e rar ely at ten ded byfever, are not accompanied by uniform distention, the dullness is moreoften confined to the upper and middle portion of the lung, and the
respira tory mur mu rs a re a bsent owing to compr ession of th e lung.
Echin ococcus cyst of th e liver or a bscess might be mist aken by crowdingupward the lung, but the boundary-line of dullness will show convexity,and the history of the case will be of such a nature as to assistmaterially in fixing the disease, and the aspirating needle will removeall doubt .
P r o g n o s i s .—The prognosis is usually favorable, though much dependsupon the etiologic factor. Where the disease is primary, the affection
runs a much shorter and more favorable course. If secondary totuberculosis, or carcinoma, the outlook would be correspondingly bad,and the course of the disease would be of a longer duration. The fever,inflammatory stage, lasts from one to three weeks, during which theeffus ion ta kes place, and th is is followed by th e non-febrile st age, whichma y last for weeks or m ont hs.
T r e a t m e n t .—The treatment in the early stage will be sedative incharacter, for just in proportion to our ability to control theinflam ma tory process, will we cont rol the exuda tion of seru m.
Veratrum .—Occasionally we find a full, strong, bounding pulse showing excessive heart power, great excitation, and high grade of inflammation. With these symptoms the patient will be restless andsuffer excruciating pain. If not overcome, these conditions lead to graveresults. In such cases veratrum is one of the best remedies in thema ter ia m edica, a nd we give it in t an gible doses, car efully wat ching itseffects, h owever, an d as th e pulse comes u nder cont rol, the t empera tu refalls, the skin relaxes, and the pain subsides, we lessen the size andfrequency of the dose. Our prescription with the above indication would
read:
Vera t rum 1/2 drachms.Aqua 4 ounces. M.
Sig. Teaspoonful every one, t wo, or th ree h our s.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 5The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 96/107
Aconite.—Many cases will have the small, frequent pulse, and aconitewill replace the veratrum, but this remedy will always be used in thesma ll dose. Thus:
Aconit e 5 drops.
Aqua 4 ounces. M.Sig. Teaspoonful every h our .
Asclepias .—This is a splendid remedy in pleurisy. Where the pain iserratic, the skin dry, and the tissues tense, asclepias, one or two dramsto half a cup of hot water, a teaspoonful every thirty or sixty minutes,for several doses, will produce relaxation, diaphoresis, lessen pain, andcontrol inflammatory processes.
Bryonia.—This is one of the best remedies for inflammatory conditions
of the chest that we possess, for its usefulness is not confined to theacute stage, but is equally efficient where effusion exists. Where thepulse is quick and hard, where there is sharp, stablike pain, andflushed, bright cheek, bryonia, 10 drops; aqua 4 ounces; teaspoonfulevery hour, will prove very beneficial. Many times it will preventextensive effusion of serum, and, when present, it assists materially inha stening the pr ocess of resorpt ion.
Rhus Tox.—Where there is irritation of the cerebro-spinal centers, asshown in the small, sharp, hard pulse, elevated papilla on tongue,
restless condition of the patient, insomnia with burning sensation inchest, rhus tox., 10 drops; aqua 4 ounces; teaspoonful every hour, willgive result s.
Macrotys.—Where the pain is located in the muscular structure or isrheumatic in character, we add from a half to a teaspoonful of thetincture to the sedative solution. Where these remedies are faithfullygiven, the effusion will be limited in quantity, and generally will bereabsorbed. In the way of local measures, libradol is perhaps the mostefficient agent. It should be renewed as often as it becomes dry, which
will be about twen ty-four or t hir ty-six hour s.
Where the effusion is large in quantity and of long standing the oldcompound tar-plaster will serve a better purpose; it should remain onuntil it produces suppuration, when the surface will be dressed with asimple cerate. If the fluid produces dyspnea and medication fails to
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 6The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 97/107
bring about absorption, pa ra cent esis should be perform ed.
The patient should be sitting up, leaning slightly forward, and the armof the affected side thrown across the chest, with the hand on theopposite shoulder. A large aspirating needle, properly sterilized, is
introduced, if on the left side, in the seventh interspace in the mid-axillary line. The needle, with boring motion, is ma de to ent er t he chest
just above th e upper border of th e rib, the n eedle slightly upwa rd. If theright side be affected, the puncture is made in the sixth interspace inth e same way.
If there is a large quantity of fluid and it is of long standing, it is notbest to attempt to open the cavity. The amount drawn will dependsomewhat upon the effect it has upon the patient. From ten to twentyounces may be removed at one operation; but if dyspnea, cough, and
pain attends the operation, the needle must be at once withdrawn. If th e accum ulat ion be recent or an active fever be presen t, a m uch lar gerquantity may be withdrawn. On the removal of the needle, thepun ctu re is t o be covered with an adh esive str ip. If th e fluid repeat edlyaccum ulat es, th e pat ient is probably tubercular , and r ecovery is not aptto follow.
P U RU LEN T P LEU RI TI S.
S y n o n y m .—Empyemia.
Def in i t ion .—A suppur at ive inflamm at ion of the pleur a.
Et i o l o g y .—A sero-fibrinous pleurisy may be converted through thechest -walls or gener at ed from within. Not u nfrequent ly it resu lts from apenetrating wound, from a fractured rib, or from the aspiratory needle,where due cleanliness has not been observed. It may be due tomalignant disease of the lung or esophagus, and not infrequently fromabscess of th e liver or from car ies of rib or sp ine.
It is frequ ent ly due to tu berculosis, an d it m ay follow infectious diseases,especially croupous pneumonia, diphtheria, and scarlet fever, morerarely typhoid fever, measles, and whooping-cough. It has followed aperitonitis and the puerpera l sta te.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 7The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 98/107
Children a re peculiar ly subject t o th is form , it being estima ted t ha t one-third of all pleural effusions in children are purulent. The organismsmost frequently found in the purulent fluid are the staphylococcus, thestreptococcus, the tubercle bacillus, and the micrococcus lanceolatus.
P a t h o l o g y .—The effusion is usually general, though, as a result of adhesion, it may be encysted. Where the effusion is of long standing,the lung is generally pushed upward and backward, and is flat andalmost ent irely airless.
The pleur a is but litt le thickened if the effusion is recent , but wh ere it isof long standing, the membranes become thickened and leathery incharacter. Occasionally necrosis of its walls occur, and the purulentmaterial makes its escape, the direction it takes depending upon theam oun t of resista nce. When t he per fora tion occur s in t he pleur a costa tis,
it finds it wa y out war ds, somet imes r esulting in necrosis of a r ib. Shouldit perforate the pleura pulmonalis, it finds its way into the lung and isexpectorated through the bronchus, or it may perforate the diaphragm,and result in a fatal peritonitis. In rare cases it has penetrated thepericardium.
The char acter of the pu s var ies. Somet imes it is of a crea my consist ency;again of a sero-purulent form, or of a fibrinous-purulent material. Afterstanding, it separates into an upper greenish or yellowish-green,transparent fluid, and a lower layer of thick greenish pus. When not of
long standing, the odor is rather sweetish in character; but if of longstanding, and especially if associated with gangrene of the lungs orsept icemic cond ition, th e odor will be peculiar ly fetid.
S y m p t o m s .—The symptoms vary greatly, depending somewhat upontheir cause. Thus, if it occurs as a primary affection, the symptoms arethose of acute pleurisy, namely, chills, high febrile action, pain in theside, dyspnea, and cough attended by slight expectoration of a muco-purulent ma terial.
Should the pleurisy be associated with septicemic or pyemic conditions,the symptoms are typhoid in character, the tongue becomes dry andbrown, the mind wanders, or coma appears. Such cases generallyterm inate fata lly after run ning a sh ort course.
Quite often, the disease develops insidiously, with no marked local
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 8The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 99/107
symptoms t o direct a tt ent ion t o th e tr ue condition. The pa tient 's fever isirregular, night-sweats a tt end, and t he pat ient loses flesh a nd st rength.To render the true character of the disease more obscure, the purulentmaterial, having perforated the pleura, sometimes burrows along thespine to the iliac fossa, resembling psoas or lumbar abscess. When the
pus breaks in a bronchus, it is expectorated, and may be mistaken fortuberculosis.
P h y s i c a l S i g n s .—The ph ysical signs ar e pra ctically the sa me a s t hoseof sero-fibrinous pleurisy, and need not be repeated. A few additionalsigns would be greater bulging of the intercostal spaces, especiallywhere perforation occurs, the appearance of a red spot and fluctuationon palpation; enlargement of the superficial veins and edema of theintegument, especially in young subjects, would suggest purulent form.
D i a g n o s i s .—A positive diagnosis of this form of pleurisy can only bema de by with dra wing some of th e fluid with an aspirat ing or exploringneedle.
P r o g n o s i s .—Empyemia is always grave, though much depends uponthe age of the patient and the causes giving rise to it. More childrenrecover than adults. When the previous health has been good and thefamily history shows no trace of tuberculosis, the outlook is morefavorable.
Should ru ptu re of th e sac ta ke place extern ally, the outlook is somewhatfavorable, as it may be where it empties into a bronchus. With theevacuation of pus, there is a tendency to adhesion of its walls,effacemen t of th e cavity, an d r etr action of th e affected side.
T r e a t m e n t .—Where there is an accumulation of pus in the pleuralcavity, we can not expect mu ch h elp from int ern al m edicat ion u nt il afterthe cavity has been thoroughly drained. Irrigation should not be used,except in those cases where the fluid is fetid, and even here much careshould be observed as ther e is dan ger from collapse.
A free incision should be made, or a good sized trocar used, in the mid-axillary line, in the fifth or sixth interspace, proper aseptic measuresbeing used. The pa tient should be in t he sitt ing postu re wh en a ble. Afterthorough draining, the patient should take well-regulated respiratorygymn as tics, to increa se th e expans ive power of th e compr essed lun g.
T h e E c l e c t ic P r a c t i c e o f M e d i c i n e - P AR T I I - R e s p i r a t o r y D i s e a s e - P a g e 9 9The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 100/107
An efficient method is that used at the Johns Hopkins Hospital, andconsists in transferring- the water from one bottle to another by meansof expiration. Large bottles holding- at least a gallon, are used, and inthese, tubes are placed. By expiring through the tubes the water is
ma de to pas s from one bott le to the oth er. This exercise, to be of benefit,should be carried out systematically and persistently as the strength of the patient will permit. The cavity is thus obliterated by the expansionof the lung on the one hand, and the retraction of the chest wall on theother.
Following the operation for the removal of the pent-up fluids, we willput the patient upon the antiseptic remedy indicated. The chlorates,sulphates, mineral acids, the vegetable antiseptic, echinacea, baptisia,an d rem edies of like char acter will be used.
CHRONIC P LEURISY.
S y n o n y m .—Adhesive P leur isy.
Def in i t ion .—A chronic inflammation of the pleural membrane, with orwith out effus ion.
Et i o l o g y .—Chronic pleurisy with effusion may follow an attack of
acute sero-fibrinous pleurisy, or it may come on insidiously, or followempyemia; in either case, the causes, conditions, and symptoms arelargely th e sam e as t hose already considered, and need no repetition.
Chronic pleurisy may follow pleurisy with effusion, where the fluid haseither been absorbed or withdrawn, in which case there is retraction of th e a ffected side. Not infrequen tly it comes on insidious ly, being chr onicfrom t he onset , or it ma y follow acut e plast ic pleur isy; pneum onia is notinfrequently followed by this form of pleurisy.
P a t h o l o g y .—Wher e t he pleur isy ha s followed a sero-fibrinous effus ionor pyemia, the pleural surfaces are frequently left covered with afibrinous exudate, which undergoes organization, the surfacesbecoming a dher ent . In some cases th ere a re pr olongat ions from t his n ewconnective tissue, which extend into the interlobular septa of the lung.These extensive tissue changes prevent a free expansion of the lung,
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 0The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 101/107
which ultimately may result in fibroid phthisis. Cysts containing aserous fluid or inspissat ed pus, in which lime s alts ha ve been deposited,ar e somet imes foun d in th e adher ent pleur al walls.
Where the pleurisy is primary, the membranes become adherent from
the fibrinous exudate; but the connective tissue is more apt to beconfined to th e pleur al su rfaces, th e lung being left free.
When seconda ry t o tu berculosis, small tu bercle masses m ay be foun d inthe walls of the pleura. In some cases there is thickening of theadherent pleura, restricting the free expansion of the lung, and whereeffus ion h as proceeded, the d ry form rest riction a nd deform ity exist s.
S y m p t o m s .—Chronic pleurisy manifests itself by occasional sharp,lancinating pains through the affected part, especially after exertion,
much talking, coughing, etc. We call the pain sharp and lancinating,but it may be more properly described as an intense, sharp soreness,which catches the part during inspiration, and stops the movement atonce; the patient calls it a “stitch in the side.” In addition there isfrequen tly soren ess on pr essur e, or when th e ar m of th at side is moved.Respira tion is more frequen t t ha n u sua l and somewhat difficult; ther e ismore or less of a hacking cough, sometimes dry, but very frequentlyat ten ded with expectora tion, sometimes copious.
The general health is markedly affected; there is a loss of flesh and
str ength , th e appetite is poor, th e bowels ar e irr egular, the skin is ha rshand dry, the pulse 96 to 100, and there is much irritability of thenervous system. Usually there is hectic fever in the evening and night-sweat s, sometimes as m ar ked as in pht hisis.
P h y s i c a l S i g n s .—Inspection shows more or less deformity on theaffected side. The chest is flat, retracted, with slight curvature anddropping of the shoulder. Compensatory expansion is noted of theopposite chest. The apex beat is feeble, or ma y be ent irely absen t, wher eoverlapped by an emphysematous lung or when displaced behind the
sternum.
Percussion reveals more or less du llness, depending upon t he a mount of th ickenin g an d compr ession of the lun g.
Auscultation reveals a feeble respiratory murmur, and a cracking
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 1The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 102/107
fr iction sound.
D i a g n o s i s .—The history, together with the dyspnea, cough, pain inside, an d by noting t he ph ysical signs a lready men tioned, th e diagnosisis readily made.
P r o g n o s i s .—The prognosis will depend upon the previous history of th e pat ient, length of time a ffected, th e cau se, an d t he gener al conditionof health .
T r e a t m e n t .—As much, if not more, depends upon improving thegeneral health, as in treating the patient for the local lesion. If we cansucceed in giving the patient a good appetite, in aiding digestion, inestablishing secretion from the skin, kidneys, and bowels, and incontrolling the circulation and innervation, we will have but little
difficulty in checking the cough, relieving the pain, promotingabsorption, an d esta blishing a cur e.
To accomplish th e first, th e pat ient m ust be much in th e open su nsh ine,and, where possible, advise a change of climate, to one where there is ama ximu m of sun shine, equable temperatu re, and m edium altitude; th is,with a good bitter tonic, like nux and hydrastine phosphate, will domu ch in a ccomplishing th e first par t of th e cur e.
As t he a ppetite is sha rpen ed an d digestion improved, there will be better
assimilation and blood-making. Proper baths and the saline diuretics,the acetate, citrate or nitrate of potassium, largely diluted, improve thecondition of the skin, kidney, and bowels, and promote absorption if effus ion be present .
In the way of local treatment, nothing will give better results than theold compound tar-plaster, used until it promotes suppuration. If mucheffusion be present , th e pleura l cavity should be dra ined.
For the cough and pain, bryonia and asclepias are favorite remedies,
though lobelia, sanguinaria, ipecac, sticta, and like remedies, will oftenbe indicated. The antiseptics will sometimes be found useful, andechinacea, the mineral acids, the chlorates,, and sulphites will give goodresults.
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 2The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 103/107
PNEUMOTHORAX.
S y n o n y m s .—Sero-Pneumothorax; Pyo-Pneumothorax.
Def in i t ion .—A collection of air in the pleural cavity, and, since this is
nearly always accompanied by serum or pus, the terms sero-pneum oth ora x and pyo-pneum oth ora x are u sed interchan geably.
Et i o l o g y .—This is a condition of adult life, being rarely found inchildren, an d occur s in ma les more frequen tly tha n in females, the r at iobeing about two to one. The left chest is more frequently the seat of election.
Fr om sevent y to ninety per cent of all cases of pneu mothorax a re du e topulmona ry tu berculosis. Thus a tu bercular cavity ma y rupt ur e into the
pleural cavity, or a caseous mass, suppurating, may open into the sameand allow the entrance of air. The same conditions may result fromgangrene of the lungs, from abscesses, from broncho-pneumonia, or abronchial fistula may be established through emphysema; hydatids ormalignant condition of the lung or esophagus may also be responsiblefor th is lesion. Ru pt ur e of a ir-cells, from a severe pa roxysm of cough ing,as in wh ooping-cough , is a possible cause.
The condition may arise from perforation of the diaphragm due toperfora t ing ulcer of th e st oma ch, or from can cer of th e st oma ch or colon,
an d, in very r ar e cases, from a bscesses of th e liver.
Penetrating wounds, or the opening of subpleural abscesses in thepleur al cavity, is t he m ost direct mean s of lett ing air int o th e pleur a.
P a t h o l o g y .—In some cases, owing to th e valvelike a ction of th e tissuesat th e seat of perfora tion, th e pleura l cavity becomes so distended a s t odisplace the heart and spleen, and, if in the right side, the liver, andcrowd the atelectatic lung back against the spine. When the pleura ispunctured in this condition, the air escapes with a slight whistling
soun d. Usua lly ther e is but little difficulty in finding t he r upt ur e, quiteoften being locat ed in th e post erio-later al r egion of the lu ng between th eth ird and sixth r ibs.
The pleural surfaces are usually inflamed and covered with a fibrinousexudate of varying consistency. In nearly all cases there is present:
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 3The Southwest School of Botanical Medicine http://www.swsbm.com
8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 104/107
more or less sero-fibrinous or purulent fluid. Where tuberculosis exists,the walls are softened, and one or more perforations may be found.There may be a communication with a bronchus. The air is peculiarlyeffusive.
S y m p t o m s .—There is a wide range of symptoms in pneumothorax.They may be so slight as to escape notice, and the condition onlydetermined during an autopsy, or they may be so severe as to almostterminate the life of the patient, and between these extremes everygra de is foun d.
The onset is generally sudden, the patient not infrequently beingalarmed by the sensation of something having given away, and at thesame time experiences, with the first rush of air, an intense pain in theside, great difficulty in breathing, being attended by a quick, small,
thready pulse, coldness of extremities, and a pallid, anxious, or cyanoticappearance.
The dyspnea varies according to the amount of air and fluid present,and, where the opening is valvelike in character and egress of air isdifficult, the pleura may become greatly distended, compressing thelung of the affected side and causing rapid, shallow breathing, whichcau ses extr eme distress a nd a sense of suffocat ion. Where th e fluid ispur ulent , th ere is u sua lly some fever of a hectic cha ra cter .
P h y s i c a l S i g n s .—The cha ra cter of th e physica l signs va ry accord ing tothe amount of air present, and whether only air be present. Where bothair a nd fluid a re foun d, the ph ysical signs ar e distinct from t hose wherefluid is absent .
Inspection .—Inspection reveals t he inter spaces filled or bulging a nd th eaffected side immobile, while the mobility of the healthy side may beexaggerated. Where the communication with the pleura is free,permitting air to enter and escape, there will be little or no distention.The h eart seat is seen to be displaced.
Palpation .—The impulse of the heart is feeble and displaced, whiletactile fremitus is diminished above, and may be entirely absent belowwher e effus ion is present .
Percussion .—The tympanitic quality of the resonance on percussion will
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 4The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 105/107
depend u pon t he qua nt ity of air a nd t he degree of ten sion with which itis confined. Thu s, where t her e is a comm un icat ion with a br onchus , thepitch is higher when the mouth is closed, and lower when it is open.This is known as the “Wintrich Sign,” while the “cracked-pot” soundoccur s wher e th e air in t he pleur al cavity conn ects with th e out side air.
Where there is fluid in the pleura, a dull, flat sound is heard as far asth e fluid exten ds. Wher e th ere is great distent ion, th e percussion n ote ishigh pitched, and when there is great displacement of the heart,resonan ce ma y be hea rd in t he cardiac region.
Auscultation .—The natural rhythmic respiratory murmur is very feebleor entirely absent. What breath sounds are heard are feeble andamphoric in character. The respiratory murmur on the well side isexaggerated. If the ear be placed near the spine, bronchial breathingma y be hear d. A peculiar met allic or tink ling sound is sometimes h ear d,
and is supposed to be due to dropping of fluid from the upper surfaceint o the effused fluid.
The coin test is said to be characteristic and pathognomonic, and isperformed by placing a coin flat upon the chest and striking it withan oth er coin while the ea r of th e au sculta tor is placed at th e back of tliechest. The sound thus elicited is a peculiar metallic ringing or bell-likesoun d, not h ear d in an y oth er condition.
Hippocratic succussion is also characteristic, and consists of shaking the
patient while the ear is applied to the chest, when a splashing sound isheard.
D i a g n o s i s .—The diagnosis is usually not difficult owing to thecharacteristic physical signs. The bulging of the intercostal spaces; themore or less displacement of the apex beat; the tympanitic percussionnoted in the upper part of the chest, with dull or flat sound over thebase where the fluid is present; the absent or feeble respiratorymurmur; the amphoric breathing; the metallic tinkling sound as thedripping of water; the coin test of Trousseau, and the Hippocratic
succussion spla sh ,—ma ke the diagn osis compa ra tively easy.
P r o g n o s i s .—The prognosis depends largely upon the cause. Where itoccurs in individuals with good family history, arid where the previoushealth has been good, favorable prognosis can usually be made; butwhere it occurs in the advanced stages of phthisis, a fatal termination
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 5The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 106/107
ma y be looked for in a few weeks.
T r e a t m e n t .—The treatment is largely palliative or surgical. Thus,where t he pa in is severe, we ha ve to resort to a h ypoderm ic of morphia,though codein by mouth is preferable where the pain is less acute.
Where the tension is extreme, the chest may be punctured by anaspirat ing needle, and where pus is present it m ay be withdra wn as inempyemia. In pyemic conditions, anti-suppurative remedies would beindicated, and where dyspnea is marked, some relief may be obtainedfrom car diac stimulan ts a nd t onics.
HYDROTHORAX.
S y n o n y m s .—Thoracic Dropsy; Dropsy of the Chest; Dropsy of the
Pleura.
Def in i t ion .—A collection of serous fluid within the pleural cavitywith out inflamm at ion.
Et i o l o g y .—A secondary affection, being usually preceded by nephritisand cardiac lesions, causes of other forms of dropsy. It may also followprofound anemia due to chronic malaria, chronic enteritis, chronicdysentery, syphilis carcinoma, and occasionally it may be due to localcauses.
P a t h o l o g y .—Hydrothorax, unless due to cardiac affections, is usuallybilat era l. The qua nt ity var ies, an d is genera lly grea ter on one side tha nth e oth er. The ret ra ction of th e lung depends u pon t he qu an tity of fluidpresent , unless previous pleur al a dhesions ha ve tak en place. The fluid isfree, not circumscribed. The pleural membrane is somewhat pale, andgenerally smooth. The fluid is of low specific gravity, 1.910 to 1.912,alka line in cha ra cter , clear, an d of an am ber color.
S y m p t o m s .—The symptoms of the primary lesion may so obscure the
condition of the pleura that it may be present for a long time withoutbeing suspected. As the fluid increases, however, dyspnea becomes aprominent symptom, and where the fluid has accumulated in largequa nt ities may resu lt in ort hopnea, cyanosis, asth ma tic seizur es, cough,an d pr ofuse clamm y sweatin g ar e a lso comm on, especially when due t oheart lesions.
T h e E c l e c t ic P r a c t i c e o f Me d i c i n e - P A R T I I - R e s p i r a t o r y D i s e a s e - P a g e 1 0 6The Southwest School of Botanical Medicine http://www.swsbm.com

8/2/2019 Eclectic Medicine Part 2
http://slidepdf.com/reader/full/eclectic-medicine-part-2 107/107
The physical signs are similar to those of pleurisy with effusion, thoughth e friction sounds a re a bsent.
D i a g n o s i s .—The evidence of fluid in the pleural cavities without pain
or fever, and an absence of friction sounds, coupled with a history of lesions of the kidneys, heart, or prolonged anemia, would suggesthydrothorax.
P r o g n o s i s .—This depends lar gely upon t he pr imary lesion.
T r e a t m e n t .—Since hydrothorax is but a part of general dropsy, ourtr eat men t will be directed a long t he lines for a na sa rca. We will think of apocynum, strophanthus, convallaria, cratsegus, cactus, and suchrem edies as increa se absorption, th e action of th e kidneys, and a dd tone
to the heart .
Where dyspnea becomes the chief difficulty, the physician will have toresort to aspirat ion.