ec 301 149 - eric - education resources information center · it discusses successful...
TRANSCRIPT

ED 345 390
AUTHORTITLE
INSTITUTIONSPONS AGENCY
PUB DATENOTEAVAILABLE FROM
PUB TYPE
EDRS PRICEDESCRIPTORS'
IDENTIFIERS
ABSTRACT
DOCUMENT RESUME
EC 301 149
LePorel Philip; Janicki, Matthew P.The Wit To Win: How To Integrate Older Persons withDevelopmental Disabilities into Community AgingPrograms.New York State Office for the Aging, Albany.New York State Developmental Disabilities PlanningCouncil.; New York State Office of Mental Retardationand Developmental Disabilities, Albany.9174p.
New York State Office for the Aging, 2 Empire StatePlaza, Albany, NY 12223-0001.Guides - Non-Classroom Use (055)
MF01/PC03 Plus Postage.Accessibility (for Disabled); *Agency Cooperation;*Community Programs; Demonstration Programs;*Developmental Disabilities; Federal Legislation;Federal State Relationship; Gerontology; Long RangePlanning; Needs Assessment; Networks; *Older Adults;*Program Development; *Social Integration; StatePrograms*New York
This information rich "How To" guide presents ways tohelp elderly persons with developmental disabilities find and usegeneric community programs for senior citizens. It discu3sessuccessful methodologies, addresses programmatic features, and offersideas to improve accessibility and resources at the community level.The information is based on experiences of four county-baseddemonstration projects in New York. Initial sections review projectbackground, explain important concepts (such as developmentaldisabilities), and identify problems this population has in usinglocal services. The next three sections describe functions of thenational and state aging network and of the developmentaldisabilities system, and how these two systems differ. The followingsection identifies specific aging program opportunities and howpersons with developmental disabilities can participate. A section onhow to get started stresses the importance of networking. Remainingsections give guidelines on how to select programs, how to involveparticipants, how to support integration, and future trends. Nineappendices include a project overview, a listing of districtdevelopmental services offices, New York aging and developmentaldisability netwcrks and local offices for the aging, an annotatedbibliography of 20 items, a statement of rights and assumptions, andvarious memoranda. (DB)
************************************************************************ Reproductions supplied by EDRS are the best that can be made *
* from the original document. *
*****************************************A*****************************

r,
Le'D.
, A
U.S. OtIMXTIMINT Of EDUCATION
Moe of Edreationei 'hoard+ end Improvement
EDUCATIONAL RESOURCES INFORMATIONCENTER IERIC)
01(his dxurnent has boon reproduced asmewed from the person or orgenizabon
originating ItMinor changes have boon made to improve
ropioduchon quality
Points of viivo or OPinions$tated in this ewe.
mem do not necesmnly repreeent *AcridOIRI position or poNcy
to
ST COPY IR
2
14.
S
"PERMISSION TO REPRODUCE THISMATERIAL HAS BEEN GRANTED BY
6t.vri,,,(
TO THE EDUCATIONAL RESOURCESINFORMATION CENTER (ERIC)."

New York State Officefor the Aging
for additional copie.; of The Wit To Win, contact:New York State Office for the Aging2 Empire State Plaza, Albany, NY 12223-0001
1-800-342-9871( toll-free in New York State)
518 486-2727This Handlx)ok was produced with funding from the New York
State Developnental Disabilites Planning Council and from theOffice of Mental Retardation and Developmental Disabilities.
Other Community Integration in Aging and DevelopmentalDisabilities Project Publications:
Serving Seniors with Severe DisabilitiesCasebook of Integration Experiences
Building the Future: Planning and Community Develop-ment in Aging and Developmental Disabilities
Contact Community Integration Project in Aging& Developmental Disabilities
New York State Office of Mental Retardationand D6 velopmental Disabilities
44 Holland Ave., Albany, NY 12229

The Wit To Win
How To IntegrateOlder Persons
With Developmental DisabilitiesInto Community Aging Programs
byPhilip Le Pore
Matthew P. Janicki
19901991
New York State Office for the AgingMario M. Cuomo, Governor Jane G. Gould, Director
4

He drew a circle that shut me out -
Heretic, rebel, a thing to flout.But Love and I had the wit to win:We drew a circle that took him in!
Outwitted - Edwin Maritharn
About the authors
Matthew P. Janicki, Ph.D.Dr. Janicki is director for Aging Services for the New York
State Office of Mental Retardation and Developmental Disabilities inAlbany, New York. He has authored numerous/ articles concerning aging, rehabilitation, and mentalretardation and developmental disabilities and is thesenior co-editor of Aging and Developmental Disabili-ties: Issues and Approaches. He established and chairsthe special interest group on aging within the
, American Association on Mental Retardation andthe special interest group on developmental disabili-ties within the Gerontological Society of America. He
is also principal investigator of the New York Community IntegrationProject in Aging and Developmental Disabilities.
Phillip LePore, MPAMr. LePore is director of the Aging and Developmental Dis-
abilities Technical Assistance Project at the New York State Office forthe Aging. Since 1970 he has been actively involvedin the development of aging programs in New YorkState, helping to set up and guide many area agen-cies on aging, nutrition and RSVP programs.
He has also directed the Senior Center Acquisi-.ion and Renovation Grant Program and the Recrea-tion for the Elderly Program as well as helping toinitiate the development of New York State's SeniorGames Program.
AcknowledgementsThe authors thank the following: Iasin Wu for taking the Integration project
from an idea to a reality; Peggy Williams, Mary Petrakos Terranova, Jack Searles,Teresa Galbier and Christine Sears for their efforts in making the local demonstrationprojects a success; Dwight Jensen for the otiginal draft; and Stocky Clark, RobertO'Connell, John Wren and Richard Wendover for their thoughts and support of theproject.
Phii LePore, New York State Office for the Aging
Matthew Janicki, Office of Mental Retardation and Developmental Disabilities

Contents
Introduction i
How it Began 1
General Concepts To Know About 3
Problems Using Local Services 6The Ag Network 8The Developmental Disabilities System 14How the Aging and Developmental DisabilitiesSystems Differ 17
Aging Program Opportunities 19
How to Get Started 22
How to Select Programs 24How To Involve Participants 30How To Support Integration 43Future Trends 46Appendices 48
Project Overview NYS OMRDD D/BDSOsDistrict Developmental Services OfficesNY Aging and Developmental Disability NetworksLocal Offices for the AgingResourcesRights and AssumptionsMemorandum of Understanding: AoA and ADDMemorandum of Understanding: SOA and OMRDDMemorandum of Understanding: New York City agencies
& OMRDD
7
Introduction
This manual is a guide for service providers in both the aging and de-velopmental disabilities networks. The guide describes ways to help elderlypersons with developmental disabilities find and use generic community pro-grams for senior citizens. It discusses successful methodologies, addresses pro-grammatic features and offers ideas and suggestions for readers as they begin totry to improve accessibility and use resources in their own community.
How to Integrate Older Adults is the result of a multi-year initiativeamong the New York State Office for the Aging, Office of Mental Retardationand Developmental Disabilities, and the Developmental Disability PlanningCouncil to first identify barriers and then develop and test strategies for inte-grating older persons with developmental disabilities within aging networkprograms.
The information was distilled from the actual experiences of fourcounty-based demonstration projects which tested the feasibility of helpingolder New Yorkers with developmental disabilites access and use a variety oflocal aging service programs. These included nutrition programs, senior centersand social adult day care programs. The demonstration projects were located inboth rural and urban areas of New York State and were under the auspice ofboth aging and developmental disabilities agencies. During the first year of theProject, they successfully integrated more than 70 older New Yorkers withdevelopmental disabilities into community aging programs.
Most important, we learned that to successfully integrate older personswith developmental disabilities we must expand the way we think about peopleand their limitations. Seniors with developmental disabilities can be success-fully placed in a variety of generic community aging programs; enjoy participat-ing with their age peers; and it given the opportunity to participate, be ac-cepted.

How It BeganIn the early 1980s, the collective efforts of
the State Office for the Aging (SOA), the Officeof Mental Retardation and Developmental Dis-abilities (OMRDD), and the New York State De-velopmental Disabilities Planning Council(DDPC), produced a series of initiatives focusingon the aging of the state's older disabled popula-tion. The OMRDD produced a major publicpolicy report in 1983 and the agencies jointly helda statewide conference on this issue in 1985. Bothembarked on major internal analyses on thedirection to take with further program develop-ment.
This led to recommending a series ofdemonstration initiatives, to be underwritten bythe Developmental Disabilities Planning Council,that would test out the feasibility of integratingolder persons with lifelong disabilities into agingnetwork programs. Following a call for proposals,the DDPC awarded several development grantsacross the state that would promote integration.
The SOA Aging & DevelopmentalDisabilities integration FeasibilityDemonstration Project
Thus the Aging & DevelopmentalDisabilities Integration Feasibility DemonstrationProject was born. Its task was to test the feasibil-ity of serving elderly persons with developmentaldisabilities within aging network programs. Theproject was based on the hypothesis that localgeneric aging service programs such as seniorcenters, nutrition sites and social adult day careprograms could readily serve persons with develop-mental disabilities. An integral question was,"Could it help older persons with developmentaldisabilities mainstream or enhance their skills,while having an equally neutral or positive effecton the regular participants at these sites?"
The Project was undertaken in two- phases. The first phase analyzed the barriers to
integration and formulated strategies to addressthose barriers. This effort resulted in the publica-tion of a report on the barriers and strategies (orrecommendations) for overcoming them. Readersare referred to the publication Barriers to andStrategies for the Integration of Older Persons with
Developmental Disabilities within Aging NetworkService,s (NYS Office for the Aging, 1987) for afull description.
The second phase involved setting up andevaluating four county-based demonstrationprojects. These were set up to test the projectintegration feasibility premise by actually attempt-ing to integrate seniors with developmentaldisabilities into a variety of community agingprograms. Each project was allowed to develop itsown integration methodology. The progress ofthe local demonstrations was carefully monitoredand assessed by SOFA.
The four demonstration projects set astheir goal to aid some 55 developmentally dis-abled seniors access and use community agingprograms. At the end of the first year of theProject the goal had been well exceeded. Some70 older persons with developmental disabilitieshad been successfully integrated into 15 discreteaging service sites.
The local demonstration projects used avariety of staffing patterns to assist in the integra-tion process; these included:
volunteer companions
paid companions
paid staff, and
shared staff
The older persons who participated inthe demonstrations were integrated into:
senior nutrition sites
senior centers, and
social adult day care programs
The local demonstration programsconducted the integration process both by makingindividual placements and by making groupplacements at one time.
What did we learn from the Aging andDevelopmental Disabilities Integration FeasibilityProject?
Elderly persons with developmentaldisabilities can be successfully integratedinto existing aging programs.
Elderly persons with developmentaldisabilities can and do benefit from
1
9

being integrated into local aging serv-ices programs. [For example, manyformed new friendships or eacties previously unavailable to them.]
Integration can be successfullyachieved using different methodologies.
The means of successfully integratingolder persons with developmentaldisabilities involves networking wi_hinterested agencies, service providers,and people.
Assessment of the demonstrations showedus that our original hypothesis had merit and thatour suppositions were workable. Our conclusionwas based on the analysis of data and documenta-tion collected during site monitoring visits andfrom pre- and post-assessments of the individualsserved, other elderly site users, and site staffattitudes. The assessment data of the individualsserved indicated improvements in the followingareas:
interpersonal skills
self concept, and
self esteem
Further, assessments of site staff andparticipants showed positive responses to thejoint use of aging network community programsby elderly persons who have developmental dis-abilities.
The diversity of the local county demon-stration projects enabled the Stace Office for theAging to gather valuable information about arange of programmatic features, including:
appropriateness of sites
planning processes
integration methodolony
barriers to integration
staffing
user suitability
networking, and
interagency coordination
Madeline
Madeline moved intoa family care homeand is attending DayCare on a daily basis.At first, her behaviorwas generally uncoop-erative and with-drawn. She is begin-ning to be more in-volved. While a staffmember was showingthe Center to some-one that Madelineknew, Madeline tookhold of his arm andspontaneously beganto give him a guidedtour.
She is now affection-ately known as theCenter tour guide - arole of which she isextremely proud.
2I I

Audrey
A udrey has had noinvolvement in com-munity activities andhas lived with herelderly mother.
On her first visit today care it was likewatching a blossomopen. Her enthusiasmand joy for being withothers influenced ev-eryone. Audrey at-tempted every activityoffered - asked forhelp as needed and ex-pressed her delightwith the "new world"by her happiness andjoy. Everyone aroundher feels wonderfuljust to be with her.
General Conceptsto Know About
The term developmental disabilitiesencompasses a variety of conditions. These caninclude autism, cerebral palsy, epilepsy, mentalretardation, learning disabilities, and other neuroIogi-cal impairments. These disabilities are not mentalillnesses, nor are they diseases. Instead, theyconstitute a lifelong mental of physical impair-ment which became apparent during childhoodand has hampered an individual's ability toparticipate in mainstream society, either sociallyor vocationally. In addition, some people withone disability, such as mental retardation, canalso have another disability, such as epilepsy.
The developmental disabilities definitioncontains the following elements; the disabilitymust -
( 1 ) have originated before the personattains age twenty-two,
(2) have continued or can be ex-pected to continue indefinitely,
(3) constitute a substantial handicapto that person's ability to functionnormally in society.
(4) result in substantial functionallimitations in three or more of thefollowing life activity areas: self-care,receptive or expressive language,learning, mobility, self-direction,capacity for independent living, oreconomic self-sufficiency.
In recent years, much attention has beengiven to the rights of people with disabilities.The efforts of many interest groups have resultedin legislation that is designed to improve accessi-bility in buildings, increase education and em-ployment opportunities, increase access to socialservices, and offer realistic portrayals of personswith disabilities in the media.
These developments - resulting from therecognition that people with disabilities arepeople first and consequently are valuable andequal members of society -- help people who hav,disabilities lead more satisfying, productive lives.
However, many people still view indi-viduals with disabilities as lesser people - to be
1 I
=1111.11M
3
';'

pitied, feared or ignored. These attitudes mayarise from a fear of someone who is different inany way or simply from a lack of informationabout disabilities. As much as the disability itselfmay affect a person's life, being treated as a lesserperson prevents a person with a disability fromleading a productive life and enjoying the sameopportunities as others.
This manual gives suggestions on how torelate to people with disabilities, how to lookbeyond the disability and appreciate the individ;ual's abilities and personality -- the things thatmake each of us unique and worthwhile,
Understanding "developmentaldisabilities"
The best way to understand what adevelopmental disability is, is to think of it as acondition that an individual may have had sincebirth or childhood, has prevented him or herfrom being hilly independent, socially or voca-tionally, as an adult, and continues on into oldage.
Developmental disabilities may cause aperson to be slower in their thinking or less agilein their movements. They may be associatedwith impaired speech or social judgement. Whensevere, they may also be associated with otherimpediments such as seizures or impaired move-ment, and deficits in sensory, language, and socialabilities.
Such disabilities are important to identifyand understand during childhood and adoles-cence, since much can he done to help peopleachieve maximum independence within thebounds of their disability. With old age, suchconsiderations are less important since thepressures of work and competition are minimal.These lifelong disabilities mirror, in many ways,the impairments that are associated with late lire.The importance of accurate diagnosis is lessenedwith old age. The critical factors for assessmentare the functional skills or limitations of theindividual.
Some of these conditions, in their moresevere forms, that fall under the rubric "develop-mental disabilities," arc briefly described below:
(4'Autism is a condition characterized kw
severe disorders in learning and behavior thatbegin in early childhood and have a marked effecton informational learning, developmental rateand sequences, responses to environmentalevents, communication, and interpersonalrelations. It is not a mental illness, but is possiblycaused by a physical disorder of the brain. Per-sons mildly affected by autism might simplyappear naive or eccentric. Those more severelyaffected are withdrawn and may display repetitiveor unusual behavior, such as rocking, and mayalso be mentally retarded.
It is rare to see a person diagnosed withautism in old age since there is a mellowing effectof the symptoms during mid-life. Most olderpersons who were autistic as children are consid-ered to be mentally retarded in old age. Other-wise little else is known about the interaction ofage and autism.
Cerebral palsy is a group of dysfunctionscharacterized by difficulty in muscular control andsensory functions, affecting mobility, speech andarm and hand movements. Cerebral palsy isusually attributed to brain injury before birth andis often associated with low birth weight. How-ever, brain damage or injury at any time can causemuch the same symptoms.
The effects of cerebral palsy can be mildto severe. The severe forms are associated withdevelopmental delay and motor impairment, andthus an individual is considered to be develop-mentally disabled.
Individuals with certain forms of cerebralpalsy often have severe speech problems, thuscausing the observer to think they are mentallyretarded, which is not always true..There is nocure for cerebral palsy, but many of the problemsthat people with cerebral palsy experience can beeffectively aided by various therapies and pros-thetic and computer assisted technologies. Linkis known about the interaction of aging andcerebral palsy with the exception that withadvancing age women with cerebral palsy appealto have a greater mortality rate than men. Physi-cally, because of a lifetime of muscular dysfunc-tion, age appears to have a much more deleteriouseffect. Many older persons with cerebral palsylose nriscular abilities sooner. The co-prevalenceof arthritis among older persons with cerebralpalsy is also high.
4
!2

When with an older person with severeforms of cerebral palsy:
Speak directly to the individual, notto a friend or companion.
Try to give your whole, unhurriedattention if the person has difficultyspeaking.
Do not comple te the speaker's sen-tences; let the puson finish.
Do nor be afraid to ask the person torepeat something.
Epilepsy involves a number of disordersof the nervous system that result in abnormalelectrical charges of brain cells. These causesudden seizures, muscle convulsions, and partialor total less ot consciousness. Persons who haveminimal or mild seizures are not developmentallydisabled. Most persons with epilepsy are notmentally retarded. Only the severe forms ofepilepsy fall into the category of a developmentaldisability and in these instances, the individualmay also have mental retardation.
Seizures are a primary characteristic ofepilepsy, but they can be controlled or preventedby the use of medication. Most seizures last onlya few minutes and many individuals receiveenough of a warning to avoid falling or becominginjured.
Little is known about the interaction ofaging and having seizures over a lifetime. Epi-demiological studies appear to indicate a shorterlife expectancy, particularly among those indi-viduals with multiple disabilities (such as epilepsyand mental retardation).
If an older individual has a seizure:
Keep calm - you cannot stop a seizureonce it has started.
Do not restrain the person.
Clear the area of hard, sharp, or hotobjects which could injure the individual. If the_person is lying down, place a pillow or rolled-upcoat under the person's head.
Mental retardation is defined as subaver-age intellectual functioning that originates during
the developmental period and ic associated withimpairment in adaptive behavior, Mentallyretarded persons characteristically have limitedability to learn and difficu!..y in using what theyhave teamed. Mental retardation has a variety ofcauses, including premature birth, genetic abnor-malities, malnutrition, exposure to toxic agents,or social deprivation.
The level of mental retardation variesgreatly from person to person. Although oneindividual may eventually be integrated withinthe mainstream of society, another individualwho is more disabled may always require somedegree of supervision. Most people with mentalretardation are capable of learning to care forthemselves and to function in society.
Some persons with mental retardationmay have difficulty fitting in socially because oflimited soc:al judgement -- however, with guid-ance and practice most problems can be over-come.
With advanced age, older persons withmental retardation generally experience the samerate of physical and medi,:al problems as otherseniors. Cont:ary to some beliefs, persons withmental retardation do not normally age earlierthan other age peers of the same cultural orsocioeconomic background.
One major difference is among personswith Down syndrome, a prevalent cause of mentalretardation. Persons with Down syndrome do ageearlier and appear to stiffer a greater co-incidenceof Alzheimer's disease. Early aging occurs in thefourth decade and about one of three olderpersons with Down syndrome shows the behav-iors associated with Alzheimer's disease (usuallyby the mid-50s).
When communicating with an olderperson with mental retardation:
Use easily understandable sentences.
Give instructions that are clear andconcise.
Talk to the person as a person -- talkto adults as adults, not as children.
Take more time to listen and under-stand what the person is saying.
Neurological impairments is a term thatencompasses a diverse group of conditions, all ofwhich relate to some form of central nervous
13

system dysfunction. Included in the definitionare conditions such as severe learning disabilities,spina bifida, Tourette's syndrome, neurofibrotnatosis,Prader-Willi syndrome, and sensory impairments.Many of these conditions are rare and are usuallyfound in children and adolescents, somewhatamong adults, but rarely among seniors.
Among seniors, the lifetime effects of alearning disability may be seen in an individual'sinability to read, write, or readily recognizesymbols.
Little is known about the effects of agingupon other conditions considered to be neurologi-cal impairments, with the exception that, inmany instances, these conditions are associatedwith a shortened lifespan. Many persons withsevere neurological dysfunctions do'not live toold age.
Problems Using LocalServices
The definitions of the various disabilitiesprovide many clues to the kinds of difficultiesolder adults with developmental disabilities mayface. Many of them continue to have troubleexpressing themselves. Many have difficultygetting about and the conjunction of impairmentsassociated with aging may make getting aboutever more difficult. Many have physical difficul-ties that lead to other problems. Many have nothad the richness of experiences available to otherolder adults over the lifespan. These are some ofthe problems that older persons with develop-mental disabilities may experience.
However, within the context of theseproblems there are other systemic problems foundwithin both the aging and disabilities networksthat arise when older adults try to use mainstreamsenior services. The New York State Office forMental Retardation and Developmental Disabili-ties and the State Office for the Aging found thatthe following barriers or obstacles to integrationoften occur:
- attitudinal
information and communication
financial
programmatic
- education and training
M orning coffee is avery special time.The seniors willdiscuss what theyhave done during theweek and what theyplan to do over theweekend. One time,they were talkingabout a dance theyplanned to attend.They started happilyteasing one anotherabout who woulddance with whom!
One senior was veryupset because hercase manager hadscheduled a dentalappointment for heron the same day thatshe was to attendday care. She was sotroubled about miss-ing day care, shecursed all the wayto, during, and backfrom the dentist.
6
14

The State Office for the Aging's report,Barriers to and Srfategies for the Integration of OlderPersons wim Developmental Disabaities within AgingNetwork Services, offers a fuller explanation ofeach of these barriers or obstacles. An abstract ofthe key points follows:
Attitudinal barriersAging network personnel often overesti-
mate the difficulties of dealing with persons widadevelopmental disabilities. These personnelexpress concerns that they would not know whatto do in case of a seizure or if the disabled personshould act "strange." They also fear that includ-ing persons with developmental disabilities mightupset thcir regular clientele at congregate sites.
Developmental disabilities system person-nel are sometimes overprotective. Some mightlack sensitivity to the special needs of olderdevelopmentally disabled persons. Some believethat "we can do it better than anyone else," thusignoring the potential benefits of integration forthe older developmentally disabled person.
Some families of persons with develop-mental disabilities are overprotective, and someare reluctant to use a formal caregiving system ofany kind.
Some older persons with developmentaldisabilities fear change, the loss of friends, or theact of going out alone. That makes them reluc-tant to participate in aging network programs.Because they generally have learned to be passivein the presence of authority figures, the freeenvironment at senior sites can be problematicanj, in itself, a barrier.
Perhaps the greatest attitudinal barrier tointegration is the problem of negative stereotypesabout developmental disabilities and olderpersons with developmental disabilities amongnon-disabled persons. Disabled persons aresubject to prejudices resulting from assumptionsthat they are childlike, have problem behaviors,and look different.
Non-disabled persons of all ages, includ-ing elderly persons are often reluctant to sharecommon services with peers who have disabilities.
Information and communicationbarriers
The lack of substantive informationabout older persons with developmental disabili-ties is an impediment to integration.
The lack of communication amongagencies can pose special problems. Neithersystem knows much about the other.
Confidentiality of records and problemsin sharing information can be a barrier.
The lack of a comprehensive intake andreferral system can impede coordination and theuse of generic aging services by older persons withdevelopmental disabilities.
Financial barriersThe current program overload and
shortage of funds, coupled with a lack of fiscalincentives to support special initiatives, clearlycontribute to the absence of linkages that couldexpand integration.
Fragmented funding sources is an obstacleas is competition for limited financial resourcesand the tendency to preserve traditional spans ofresponsibility.
Another barrier is the regulatory andcompliance standards required by the develop-mental disabilities system for reimbursement.
Programmatic barriersSocial services programs have different
staffing and program standards than health-related and habilitation programs, so coordinatingthe two can be difficult.
Developmental disability system require-ments for active treatment and gual-based pro-gramming of persons with developmental disabili-ties can be seen as insensitive to the needs ofsome older individuals who may necessarily bemore "retired" than active.
The aging network lacks staff memberstrained and experienced in providing supervisedcare to persons with developmental disabilities.
The absence of adequate transportation isa major problem.
1 5
ABM
7

The architectural design of some agingservice sites make them inaccessible to seniorswith disabilities.
Education and training barriersThere is a lack of adequately trained
professionals who know about both aging anddevelopmental disabilities and who understandthe means needed to mee: the programmatic andlife support needs of older persons with develop-mental disabilities.
Agencies lack funding for cross-networktraining activities.
Some professionals resist cross-networkintegration.
The Aging NetworkThe term Aging Network refers to the
system responsible for furnishing services topersons aged 60 and over. That system is part ofa national network on aging established by theOlder Americans Act and headed by the U.S.Administration on Aging. It is comprised of 57State Units on Aging, some 664 Area Agencieson Aging, 721 state and local advisory councilsand thousands of nutrition and aipportive serviceproviders operating at the community level.
In New York State the aging network iscomprised of state and local government agenciesas well as a large variety of community levelservice provider agencies.
Role of the State Officefor the Aging
The lead agency at the State level is theNYS Office for the Aging. Under the federalOlder Americans Act and New York Statestatute, the State Office has responsibility for awide range of planning, coordinating and fundk..i.7,activities. In addition, it serves as the State levelfocal point for aging concerns and advocacy. Ingeneral terms, the Office is responsible for thefollowing:
Management and administration
Designation of planning andservice areas
Development of intrastate funding formulas
State plan development
Service system development
Needs assessment
Establishment of priorities
Systems development
Program development
Services development
Program operations
Training
Advocacy
Policy and program design
Pooling and coordination
Community involvement
Capacity-building and technfcalassistance
In New York, the State Office for theAging supports and monitors a network ofcounty-wide aging offices throughout the State.The local county aging offices (also called areaagencies on aging), are, with few exceptions, partof county government. The non-governmentalaging offices provide the same services as theircounty government counterparts, but have privatenot-for-profit sponsorship. In New York City, theaging office is a city government agency andserves all five boroughs.
There are 59 local aging offices represent-ing all of the counties in New York State as wellas the St. Regis Mohawk Indian Reservation, andthe Senec Nation of Indians (which includes theCattaraugus and Allegany Reservations) - theseare the only Indian Reservations so designatedeast of the Mississippi.
Role of Local Aging OfficesThe local aging offices have the responsi-
bility to plan, coordinate, advocate and facilitatethe development of comprehensive servicedelivery systems at the local level to meet thelong and short term needs of older persons intheir designated service.. area.
8
6

Each local aging office prepares a multi-year plan and annual updates which identify theneeds of older persons, existing services, and gapsbetween needs and services. The plan alsoidentifies objectives, priorities and specifies whichservices will be provided to meet those needs.
Local aging offices are responsible forseeing that the following categories of services areprovided via a provider agency or if unavailable,then, directly by their office:
Services associated with access toservices (transportation, outreach, andinformation and referral).
In-home services (homemaker andhome health aide, visiting and tele-phone reassurance, chore maintenance,and supportive services for families ofelderly victims of Alzheimer's diseaseand the neurological and organic braindisorders of the Alzheimer's type).
Legal assistance
The following are examples of the kind ofservices provided by a local aging office eitherdirectly or through a service delivery contractwith a provider agency in the community.
Information and ReferralFrequently, older people need services but
do not know where to turn to receive them. Bycalling the aging office, senior citizens are linkedwith appropriate services and provided necessaryinformation.
OutreachThis service provides outreach workers to
staff community gathering points (such as nutri-tion sites) and to make home visits where neces-sary. Outreach workers help those who are inpoor health, who live in isolated areas or whohave low income get the services and or informa-tion they need. They provide entitlement coun-seling for a wide range of services and benefitsavailable to older people. Senior citizens whoneed assistance from an outreach worker canschedule a visit by calling the aging office tosecure a visit by an outreach worker.
In-Home ServicesA case manager does a needs assessment
and recommends services; prepares a service plan;and monitors the continuing provision of servicesneeded to maintain a person in their home. In-Home services are provided by the New YorkState EISEP program (Expand& In-Home Servicesfor the Elderly Program). EISEP provides non-medical in-home services to disabled elderlypersons who need supportive services.
TransportationTransportation for senior citizens to
medical and other necessary appointments may beprovided by volunteer drivers who are reimbursedfor mileage or by an aging office van with a fulltime driver. Shopping assistance may also beavailable.
EscortEscort may be provided by the county
aging office's outreach staff who accompanysenior citizens if they need extra help in arrangingfor needed services
Public InformationTo keep senior citizens up to date on
programs, services, and other information ofinterest to older people, mor aging offices publisha newsletter which is mailed monthly or bi-monthly. Other publications may also include: adirectory of county services; a financial organizer;a long term care directory and a senior discountmerchants directory. In addition, newspaperarticles, speaking engagements and radio an-nouncements are prepared and used to makeimportant information available to older resi-dents.
Alzheimer's Disease and RelatedDisorders Support Groups
Some aging offices offer support groups,individual counseling, resource materials and amonthly newsletter to help family and caregiversof people with Alzheimer's disease and relateddisorders.
9
1 7

Congregate MealsA congregate meal program offering hot,
nutritious meals is provided in a variety of loca-tions and sites by the aging oflice's Senior Nutri-tion Program. Monthly menus are published andposted at all nutrition program sites.
Home Delivered MealsMeals can be delivered if a senior is frail,
disabled and or homebound. Frozen meals readyto reheat are available for weekends and for areaswhich do not have daily delivery in some coun-ties. These home delivered meals are providedunder the New York Supplemental NutritionAssistance Program.
Nutrition Education and CounselingThe aging office's Registered Dietitian
provides informative programs on nutritionduring regular visits to nutrition program sites.The Registered Dietitian may also write articlesfor the monthly newsletter as well as preparenutrition tips to include with home deliveredmeals and provide individual nutrition counselingas needed.
RecreationRecreation programs, activities and
services may be directly furnished by the agingoffices at a variety of sites including nutritionprogram locations. In addition, aging officesprovide information about the state SeniorGames Program and may sponsor local SeniorGame Programs.
Visiting and Telephone ReassuranceAn aging office, sometimes in coopera-
tion wih the Retired Senior Volunteer Program,may provide trained volunteers to call or visitolder people who are homebound and/or physi-cally or socially isolated.
Home Helper/HandymanThis referral service provides senior
citizens who need assistance in maintaining a
home, performing routine or seasonal chores,personal care, or minor home repairs with a list ofpeople in their area who are eager to do therequested work. The program also providesemployment to senior citizen workers as well asmaking information about competent workersavailable to senior citizens.
Enriched HousingThis service may be provided by a county
aging office under the regulation of the New YorkState Department of Social Services. Eligibleresidents of senior housing complexes may arrangefor assistance with personal care, shopping,cooking and housework through the EnrichedHousing program.
Energy AssistanceThe aging office assists senior citizens in
meeting their energy needs by providing energyinformation, outreach and assistance with appli-cations for HEAP (Home Energy AssistanceProgram). By screening applications, the countyaging office certifies those over 60 who are eli-gible to receive federally funded energy assistanceand related programs such as Weatherization, Proj-ect SHARE, Care and Share, and Energy Conserva-tion Bank.
An aging office also assists people who areineligible for these programs in solving fuelrelated problems. The Energy Program Coordina-tor and Office for the Aging outreach workersprovide entitlements counseling for a wide rangeof programs and benefits available to older people.
Discount CardsSenior citizens over 60 may be able to
obtain a discount card from the local aging office.Discount cards and a merchants' directory make itpossible for senior citizens to purchase goods atlower cost.
Adult Day CareAdult day care may be provided for older
people who are disabled, live in isolated areas, orwho need some assistance in order to remain
10
I s

Lucille
F or the first time inLucille's life she is func-tioning at a higher levelthan some of her peers.
She constantly watchesout for others, especiallyAlzheimer's patientswho wander.
During luncheon tripsshe helps staff membersby holding purses andcoats or pushing wheel-chairs.
She loves the involve-ment here, and enjoysparticipating as a con-tributing member of thecenter.
independent and active in their communities.Adult day care offers smportive services in agroup setting. Programming includes a hot meal,socialization, recreation, individual and familycounseling, and training in skills needed toremain independent despite one or more handi-capping conditions.
Insurance CounselingInsurance counseling may be provided by
the local aging offices. The service helps olderpeople with health insurance problems throughcounseling, policy review sessions, explanation offorms, and through infonnative workshops.
Legal ServicesLegal services are provided by the aging
office via a subcontract with a community legalaide agency. The service is designed to improvethe availability of legal services to the elderly,including representation on matters affectingtheir rights, entitlements, benefits, and othermatters directly affecting their general welfare andindependence. Referrals to private lawyers aremade when appropriate.
RespiteThe aging office may provide a respite
program which will allow caregivers of olderfamily members to prearrange for care when avacation or necessary absence from home isplanned or for regular weekly respite for thecaregiver.
How Aging Programs are FundedThe State Office for the Aging receives
funding, in part, from the following:
the Federal Older Americans Act,and
State fimding authorized for programssuch as the Supplemental NutritionProgram (SNAP); Community Servicesfor the Elderly Program (CSE); theExpanded In-Home Services Program(E1SEP).
1 1

Through these statutes the State Officefunds the local aging offices to provide a range ofaging service programs.
Funding for Local Aging OfficesThe local aging offices draw upon the
State Office funding to provide mandated serv-ices. In addition, they are also free to attractother funding to support services they want toprovide. Depending upon the funding source thelocal aging office may or may not have broaddiscretion in deciding what types of services tosupport.
Local aging office programs and servicesare supported by the following funding sources.
Older Americans Act Title III-B -Federal Funds
Under Title III-B funding, 90% of thefunds provided to the local aging office must beused for social services. Up to 10% may be usedfor office administration. Title III-B funds can beused to provide the following services:
Transportation/Outreach
Information and Referral/LegalServices
Public Information Advocacy Om-budsman
Home Helper/Handyman/ID/Dis-count Cards
Insurance Counseling/Escort
Friendly Visiting & Recreation
Telephone Reassurance
Older Americans Act Title III-C -Federal Funds
Uncicr Title III-C funding, 90% of thefunds provided to the local aging office must beused for nutrition program services. Up to 10%may be used for program administration. TitleIII-C funds are used to provide the followingservices:
Home Delivered Meals
Congregate Meals
Nutrition Education
Outreach
SNAP-Supplemental NutritionAssistance Program - State Funds
New York State SNAP funding providesadditional funding for home delivered meals tofrail, isolated, or homebound senior citizens.SNAP funds are also used to provide the follow-ing services:
SNAP Home Delivered Meals
Nutrition Education
Nutrition Counseling
Outreach
Older American Act Title V SeniorEmployment Program - Federal Funds
Title V funding supports the SeniorEmployment Program. Under Title V, part-timeemployment opportunities are developed tor lowincome persons 55 and older. The fundingsupports worker's wages and benefits. Theseworkers assist with the following services:
Transportation
Outreach
Adult Day Care
Community Services for the Elderly -State Funds
Community Services for the Elderly(CSE) State funding is used to provide planning,coordination, and services for the frail elderly.The following services may be supported underCSE:
Adult Day Services
Outreach Service
Alzheimer's Support Groups
In-Home Services
Transportation
Case Management
12
9

Sue
Sue was not in-volved in commu-nity activities andwas very depend-ent on her motherfor care.
Since attending thesenior center, shehas blossomed. Sheenjoys the camara-darie of others, andis very vocal. Sheparticipates inactivities, and isbeginning to func-tion more inde-pendently.
Andy
A ndy is a veryquiet gentlemanwho rarely inter-acted in commu-nity activities.
Since attending theSenior Center hehas become veryverbal. He enjoysattending luncheontrips and shows in-creasing involve-ment.
Respite Services
Telephone Reassurance
Home Delivered Meals
Other FundsAs mentioned earlier, local aging offices
are free to secure funding from other sources toexpand existing services or provide new servicesnot covered by the previously mentioned funding.The following are examples of some additionalservices and their funding sources:
Senior Recreation funded by theState Recreation for the Elderly Pro-gram.
Enriched Housing-self supporting(regulated by the New York StateDepartment of Social Services) as anadult home with a combination ofFederal SSI, and state subsidies.
HEAP (Home Energy AssistanceProgram) provides low income seniorswith a grant to cover winter heatingcosts. HEAP is funded by a FederalEnergy Assistance Grant.
Adult Day Care programming fundedby a member item legislative grant-in-aid.
Senior Companion Program fundedby an Action (Federal VolunteerAgency) grant.
Special Note About FundingThe State and Federal funding sources
used by local aging offices to provide servicesgenerally require a "local match". The localmatch varies from 10% to 25% and dependingupon the program, may be cash or in-kind.
The Older Americans Act DisabilityAmendments
When the Older Americans Act Amend-ments of 1987 (PL 100-175) were signed into lawin November, 1987, this legislation contained anumber of new provisions specifically addressingolder Americans with lifelong disabilities.
13
21

A number of the provisions called uponthe federal Commissioner of the Administrationon Aging to develop new initiatives addressingthe needs of older Americans with a disability,develop linkages with the Administration onDevelopmental Disabilities, and promote greateraccess for older Americans with a disability toOlder Americans Act services.
Other provisions called upon the stateunits on aging and the area agencies on aging todevelop stronger linkages with state and localdisability agencies, promote more effectivecommunity long term care services, and conductneeds assessments, program development and casefinding efforts. The provisions also definitivelyspelled out the inclusion of older Americans withdisabilities into Older Americans Act services.
Specifically, the following disabilityrelated provisions were incorporated into theOlder Americans Act:
Two new terms were added to the Act:disability and severe disability.
Disability refers to a mental orphysical impairment, or a combinationof mental and physical impairments,that results insubstantial functionallimitations in one or more of thefollowing areas of major life activity: (a)self-eare, (b) receptive and expressivelanguage, (c) learning, (d) mobility, (e)self-direction, (0 capacity for independ-ent living, (g) economic self-sufficiency,(h) cognitive functioning, and (i)emotional adjustment.
Severe disability refers to a severe,chronic, condition that is attributableto mental or physical impairment, or acombination of mental and physicalimpairments, that (a) is likely tocontinue indefinitely; and (b) results insubstantial functional limitation inthree or more of the major life activitiesnoted above.
The Commissioner of the Administrationon Aging (AoA) is required to undertake anumber of activities, including:
develop planning linkages with theAdministration on DevelopmentalDisabilities.
advise, consult and cooperate withthe Administration on DevelopmentalDisabilities, the federal agency thatadministers the Developmental Disabili-ties and Bill of Rights Act (the Com-missioner of the Administration on De-velopmental Disabilities is in turnrequired to reciprocate in areas relatedto the purposes of the Older AmericansAct).
The state aging agency is to coordinateplanning, identification, assessment of needs, andservices for older individuals with disabilities withthe state agency with primary responsibility forindividuals with disabilities, and develop collabo-rative programs, where appropriate, to meet theneeds of such older individuals with disabilities.
Area agencies on aging are required toundertake outreach efforts to identify individualseligible for assistance under the Act, includingolder individuals with severe disabilities.
Area agencies on aging can offer meals ata nutrition site to younger persons who aredisabled who reside at home with and accompanyolder individuals who are eligible under the Act.
For an excellent description of the historyand general provisions of the Older AmericansAct of 1965, as amended, see An Orientation to theOlder Americans Act, a manual published by theNational Association of State Units on Aging(Washington, DC, July, 1985).
The DevelopmentalDisabilities System
The term developmental disabilitiessystem refers to the many agencies, both privateand public, which plan, coordinate, administer,offer, or finance services for persons of all ageswho are developmentally disabled. Early effortsto develop services for persons with such disabili-ties were primarily focused on children withmental retardation. However, the field of devel-opmental disabilities has matured with therealization that its efforts must include all facetsof the lifespan and all types of disabilities thatimpede typical growth and development.
OverviewEarly advocacy for equal educational op-
14
'2 2

portunities kd to the pgssage of PL 94-142, theEducation for All Handiczoped Children Act.With the implementation oi" this Act (and itsamendments), individuals wi handicappingconditions were expected to be fully integratedwithin the mainstream of societ is opportunitiesand activities.
Recent revisions to that Act have donethe same for preschoolers, and amendments tothe Vocational Rehabilitation Act, for work ageadults. With the inclusion of disability-relatedprovisions in recent amendments (PL 100-175)to the Older Americans Act, the same expecta-tions have been set for older individuals withlifelong disabilities.
For persons with developmental disabili-ties, reaching old age always was a reality; how-ever, it was a reality that was subordinated toother developmental concerns. In the past, mostpersons with severe developmental disabilitieshad a relatively short lifespan and many adultswith developmental disabilities spent much oftheir lives in public institutions. Consequently,their aging was not of immediate concern.
However, increased longevity, resultingfrom more readily available services and improvedhealth status, and the added visibility of manyelderly persons with developmental disabilitiesnow living in the community, have contributedto a greater awareness of their lifespan develop-ment and aging.
In New York the developmental disabili-ties services system is divided by agency and age.
Infants with disabilities are the responsi-bility of the health system with support from theOffice of Mental Retardation and DevelopmentalDisabilities.
Children with disabilities are the respon-sibility of the education system; those childrenwho are substantially handicapped, as well astheir families, can also receive services from theOffice of Mental Retardation and DevelopmentalDisabilities.
Adults, minimally handicapped, may bethe recipients of services from the vocational re-habilitation agency; those persons mare disabledand needing special services receive themthrough the Office of Mental Retardation andDevelopmental Disabilities.
Role of the Office of MentalRetardation andDevelopmental Disabilities
The Office of Mental Retardation andDevelopmental Disabilities (OMRDD) is the stateagency with authority and responsibility, underthe state's mental hygiene law, to provide servicesto persons with developmental disabilities. TheOMRDD is organized into 20 regional or districtoffices. (See Appendix for listing of the districtoffices).
The OMRDD serves as a replator ofservices, as well as a major provider. Combined,the OMRDD and its vast network of provideragencies provide for some 4,000 foster family carehome spaces, 10,000 community residence spaces,and 40,000 adult day program spaces. The agencyalso operates a family support program that aidsfamilies with a disabled member through respite,and other support services.
The driving philosophy of the OMRDDand its provider network is to maximize thecommunity integration and mainstreaming ofpersons with developmental disabilities.
In the area of senior services, the agencyand its network operate numerous group homes orcommunity residences which predominantly serveseniors. The agency has also expanded its FamilySupport Program, by having local adult day careprograms underwritten by this program. In 1989,the OMRDD also expanded its adult day trainingcapacity to include senior day programs.
Programs and Services for OlderPersons with DevelopmentalDisabilities
The program options available to olderNew Yorkers with a developmental disabilityinclude:
supportive apartments
community residences
foster family care homes
day treatment programs
15
23

senior day programs
sheltered workshop programs
supportive work programs
respite and other family supports
Supportive apartmentsThese are a form of community residence
where from one to three adults live by them-selves, but receive drop-in supervision. Thisresidential model is for those adults who are themost capable. They usually serve as a bridge toindependent living. These are operated by thestate OMRDD and its network of voluntaryagencies. Referrals for admission can be made tothe agency which operates the program.
Community residencesCommunity rcsidences or group homes
may take many forms. One is the supportedcommunity residence which is funded by Statefunds. These residences provide housing for up to14 adults. Generally, these residences providehousing for adults who are more independent andvocationally and socially capable. There are over30 such residences across the state which providehousing for older and elderly adults.
A variation of this residence is the ICF-MR/community residence, which is fundedthrough Title XIX Medicaid funds. These resi-dences provide housing and active treatment toindividuals who have greater dependency andcare needs.
Community residences have shift staffwho provide supervision, companionship, train-ing and other support services. They are operatedby both the state OMRDD and its network ofvoluntary agencies. Some 17% of the residentsare elderly. Referrals for admission can be madeto the agency which operates the residence.
Foster family care homesFoster family care homes are the oldest
residential model in New York. These homes,supported by State funds, provide for board andcare, as well as some training for adults who needsome level of supervision. Foster family carehomes are private homes, certified to be uses as
housing for up to 4 adults with developmentaldisabilities. Some 34% of the foster family careresidents are elderly.
A variation of this residential model ispersonal care homes. These are foster family carehomes where one or both of the home's ownersare certified to provide Medicaid reimbursablepersonal care services. Residents of personal carehomes are generally more dependent and dis-abled. The foster family care program is operatedby the OMRDD. Referrals for admission can bemade to the OMRDD's district office.
Day treatment programsDay treatment programs are day programs
funded by Title XIX Medicaid funds. Theseprograms provide a range of habilitation activitiesand therapies that comprise a program of activetreatment. Currently, some 40 day treatmentprograms across the state provide specializedservices to seniors.
These programs are similar in structure tomedical model adult day care programs. Seniorday treatment programs are operated by both thestate OMRDD and the voluntary agencies.Referrals for admission can be made to the agencyoperating such a program.
Senior day programsSenior day programs are built upon the
social adult day care model. They are funded bystate and local funds on a 50%/50% basis. Theseprograms, originally "day training" programs, aredesigned to provide a range of habilitation andsocial activities for seniors. Currently some 25senior day programs are operating across the state.
OMRDD is experimenting with 100%state funded senior day programs; in 1989, sixsuch programs were funded as demonstrations.Senior day programs are operated by both thestate OMRDD and the network of voluntaryagencies. (For information about these demon-strations, refer to New Directions for Seniors: SeniorDay Program Demonstrations, available fromOMRDD - see appendix.) Referrals for admissioncan be made to the agency operating such aprogram.
16

Sheltered workshop programsThe state's network of sheltered work-
shops provides vocational training and workservices to adults of all ages. Many seniors arestill enrolled in workshops or are admitted forwork training. Sheltered workshops are operatedby disability agencies, both those that specializein mental retardation and those whose clienteleinclude persons with various physical or socialdisabilities.
Such programs are funded by varioussources, including contract income, grants, andstate funds from the OMRDD, other disabilityagencies, and the Office of Vocational Rehabili-tation. Referrals for admission can be madedirectly to the workshop or through the Office ofVocational Rehabilitation.
Supportive work programsSupportive work programs involve
placing the worker in a competitive production orse vice work setting. Such programs are usuallyoperated in conjunction with sheltered workshopsand provide job coaches and on-site supervisionto aid the worker to adapt to the job and jobtasks. Referrals for admission can be made to theagency operating such a program.
Respite and other family supportsThe OMRDD's family support program is
designed to assist a person with a developmentaldisability who resides with his or her familyreceive special supports to help him or her remainat home. Referrals can be made to the agencyoperating such a program or to the OMRDDdistrict office.
How the Aging andDevelopmental DisabilitiesSystems Differ
The disability system has its rcots in twosignificant movements in the United States:
the vocational rehabilitation legisla-tion and program initiatives thpt
addressed the needs of returning dis-abled World War I veterans and led tothe development of a system of voca-tional rehabilitation services -- whicheventually included other persons whosedisabilities may have been congenital ororiginated in childhood - such as mentalretardation and the other developmen-tat disabilities.
the parent advocacy movement thatfollowed World War II and parentorganizations such as the Associationsfor Retarded Children (now Associa-tions for Retarded Citizens) which ledthe fight for legislation and funding ofspecial services within specialized orgeneric settings dedicated to personswith mental retardation.
The derivation of the professionals thatcomprise the disability system's workforce also isdifferent. Much of the technology upon whichthe mental retardation derived disability system isbased is drawn from special education andrehabilitation - and is directed toward impartingnew learning. Because its roots are in education,its focus is on individual training and develop-ment.
The language and orientation of develop-mental disabilities services reflects this back-ground. For example, needs are assessed onindividuals, services are planned around an"individual program plan," the terminology usedis "habilitation" and "training," and most inter-ventions/services are directed toward the individ-ual within the context of a setting that is individ-ual-oriented.
The aging network's roots offer a differenthistory. Special services to elders have been partof our social fabric for years, but the basis was insocial services and various generic and informalcommunity supports necessary to maintainnormal functioning as long as possible.
As an extension of generic communitysocial services, the network's services were notuniversally focused until the passage of the OlderAmericans Act in 1965. When specializedservices evolved, a major focus was on sites andsettings that could draw together diverse servicesthat could be used by elderly persons in thecommunity.
17
25

The technological emphasis in manyaging network programs is not on the individual,but on service provision and the availability ofsocial environments for socialization and com-panionship -- the focus is on the group. Ingeneral, the aging network is a group orientedmodality and the rehabilitation technology that isdrawn into it is based upon mitigating the prob-lems associated with aging and maintaining inde-pendence as long as possible.
With regard to aging network programs,such as multipurpose senior centers, adult day careprograms, congregate meals sites, and the commu-nity-based activity centers that make up a greatpart of the aging network's services, this differ-ence is exemplified by:
the lack of case orientation (asopposed to the disability system wherecase managers are an important ingredi-ent),
consumer freedom to come and go(as opposed to the disability systemwhere intake and discharge form a"gatekeeper" function),
assessment based upon functionalneed identifiers (as opposed to thedisability system where diagnostics andclinical descriptors are prevalent),
sustenance of functional abilities andsocialization (as opposed to the disabil-ity system where there is a continualemphasis on new learning and train-ing), and
a temporal orientation, providingservices to a age-specific clientele(opposed to lifespan, "cradle to grave"care and case management in thedisability system).
A fuller explanation of these differencescan be found in Aging and Disabilities: The Inter-section of Needs and Resources, a training manualfor workers in aging and developmental disabili-ties agencies produced by the Center on Aging atthe University of Maryland. (See Appendix) .
John
J ohn attended a ptateschool for much of hisadult life. He was dein-stitutionalized and livesin an adult home. Ini-tially he was in a daytreatment program. Stafffelt that John was toohigh functioning for thatprogram and referredhim to a seniors' pro-gram. He began in aspecial transition-assis-tance program. After ashort time, John was ableto participate in theprogram independently.
Eventually, John becamea Retired Senior Volun-teer. He assists others inwheelchairs and assistssenior center staff indecorating for parties,clean-up, and movingfurniture. John alsoattends a peer supportgroup for others withdisabilities to discusspositives add negatives oftheir community pro-gram. John is well-likedby all and has become anintegral member of thesenior center.
18

Aging ProgramOpportunities
Many local offices for the aging support anumber of congregate programs for older personswhich may also be suitable for some older personswith developmental disabilities. The programsmay be directly operated by the office for theaging or provided via subcontract by a communityagency. As a general rule, the programs are opento any person aged 60 and over.
The types of congregate programs whichoffer participation opportunities for seniors withdevelopmental disabilities include social modeladult day care programs, senior centers, and seniornutrition programs. We'll go over each of thesein more detail and explain how they can beuseful.
Social Adult Day Care ProgramsSocial Adult Day Care Programs are
congregate programs which provide a structuredenvironment for seniors who are frail and/orrequire supervision. The programs offer partici-pants the opportunity for socialization and usuallyhave daily programming built around recreationand other structured activities. Assistance withpersonal care is usually provided. Transportationmay also be furnished. The programs have anutrition component, typically a hot lunchtimemeal, Social Adult Day Care Programs do nothave to be certified, but usually function withingeneral standards for such programs. Sites tend tobe open 5-9 hou.s a day, 3-5 days a week. SocialAdult Day Care Programs generally have a dailyfee; most charge from between $17 to $30.
Participation By Persons WithDevelopmental Disabilities:
Social model adult day care programs aresimilar in many respects to the day training or dayhabilitation programs operazed for adults byagencies serving persons with developmentaldisabilities. Becm,e of their similarities, manyolder adults with dP.velopmental disabilities canreadily adapt to the settings and programs.Admission is usw.11y facilitated when operai.orsmeet the individual being referred and determinethe extent of similarity with existing users.
Under the SOA Integration Feasibiliti Demon-stration Project many older persons with develop-mental disabilities were successfully placed in daycare programs.
Indeed, we observed no problems at anyof the sites. The comments of one of the demon-stration site directors echoed those of the otherprogram administrators when the director notedthat the day care setting created an environmentin which hidden talents blossomed. He reportedthat many of the older persons with developmen-tal disabilities tended to function at or above thelevel of the "regular" seniors in his day careprogram. "Integration" he said, "is not an issuein day care because most attending have the samelevel of disability."
Senior Center ProgramsSenior centers are usually community
facilities used for the organization and provisionof a spectrum of servicPs for persons aged 60 andover. Most senior centers are open daily from 9am to 5 pm. Participation is ust ally free though amembership card and monthly newsletter may beoffered for a small fee.
Senior center programs typically offerparticipants opportunities for creative expression(arts and crafts) and for social interaction (danc-ing events, cards, billiards, bingo, etc.). Recrea-tional activities such as cards, conversation andwatching the latest turn of the weekday soaps onthe center TV, are the most popular. Somecenters have extensive program arrays which mayinclude physical conditioning activities, collegelevel courses, programs on computers, as well asopportunities for participating in organizedvolunteer activities. Generally, all senior centersoffer a midday hot meal to participants.
Participation By Persons WithDevelopmental Disabilities:
Senior centers can offer those personswith developmental disabilities who are able toparticipate, an opportunity to grow and functionin a relatively unstructured and unsupervisedenvironment. Older persons with developmentaldisabilities who were successfully placed in seniorcenters under the SOFA Integration FeasibilityDemonstration Project showed, as a group,marked improvements in social interactions,
19

social behavior and in developing friends andfriendships.
Senior centers are social institutions andas such are bound by the social groupings thatform in them. Care must be given that personsyou iategrate into senior centers are not isolated.Those persons with the greatest chance of bene-fiting are individuals with a strong sense of socialself, willingness to get involved in novel activi-ties, and ability to function within fairly unstruc-tured circumstances.
Senior Nutrition ProgramsCommunity nutrition programs are the
most numerous type of congregate programs forsenior citizens. Under the nutrition program, hotmidday meals are provided for seniors aged 60 andover, 3 to 5 days a week. Spouses and compan-ions under age 60 or persons with developmentaldisabilities under the care of nutrition programparticipants are also eligible to participate.
Seniors are requested to contribute aspecific amount toward the meal, which isplanned by a nutritionist. The suggested dona-tion is usually between one and three dollars.Most programs use an unmarked envelope systemto allow a person to contribute what ever he orshe can afford.
Nutrition program services are providedin a wide variety of facilities, such as seniorcenters, churches, town halls, schools and inbuildings owned by community groups, such asthe VFW.
Local nutrition program sites tend to takeon many of the characteristics of a senior center.The sites sometimes serve as the only focal pointand meeting place for seniors in the community.Often following the meal, announcements ofcommunity events will be made and a recrea-tional activity will be offered for those who canstay. Unlike a senior center, activities, ic offered,are usually concluded before mid-afternoon. Mostnutrition-only sites open by mid-morning andclose right after lunch if a planned activity is notheld.
Beverly and her sister livein an adult home. A relative,who claimed to be their legalguardian, was neglecting herresponsibilities for theirfinances and medical care.The adult home administra-tor had been "fighting" withthe guardian for the pastthree years on the sameissues. It developed that therelative was not the legalguardian and therefore hadno legal right to make deci-sions for the sisters.Help was sought from sev-eral legal agencies, includinga protection and advocacyagency (P&A), but all re-fused the case. The adulthome was requesting legalguardianship and had agreedto become representativepayee for the sisters. Aftermany phone calls, a meetingof all agencies which hadbeen contacted about thecase was convened. TheP&A finally agreed to takethe case.
Meanwhile, the sisters wereenrolled at a senior centerwith a Senior Companion.They now attend part-timeand the attorney at the P&Ais following up with surro-gate court to appoint legalguardians for the women.
20
28

Participation By Persons WithDevelopmental Disabilities:
Nutrition program sites offer the opportu-nity for seniors with developmental disabilities tobe a part of a daily community group and tosocialize with others while enjoying a middaymeal. Under the SOA Integration FeasibilityDemonstration Project a number of older personswith developmental disabilities successfullyparticipated in the hot meal program and in theactivities which followed.
Nutrition sites typically have minimalstaffing, consequently the persons you select touse a nutrition site should be able to take care ofthemselves or even help others. Site managersare especially appreciative of volunteers who canhelp set up the meal and pick up after. At somesites, older persons with developmental disabili-ties helped with the staging of the meal program.
The Benefits of Participation inLocal Aging Programs
Participation provides a link to thecommunity which should be part of the depend-ent adult's lifestyle, when that is possible and ap-propriate.
Participation offers a break from routine.
Participation provides an entry into a"normal" community group which can have astimulating and positive effect on the day-to-daybehavior and feelings of the dependent adult.
Participation provides exposure to avariety of experiences which tend to challengeintellectual capacity and make life more interest-ing and pleasant. For seniors with developmentaldisabilities as well as for the well-elderly seniors,local senior citizen programs can and do forestallmental and physical deterioration that mightotherwise occur.
Persons working in local communityaging programs of the type described above haveoffered specific reasons why they find the place-ment of older persons with developmentaldisabilities valuable. They say participation intheir program offers older persons with develop-mental disabilities the following opportunities:
an environment in which they can
Jesse
Jesse lives at the de-velopmental center.He was assigned aSenior Companionand now participatesthree days 1 week atthe senior center.Jesse has never beforehad the opportunityto participate in acommunity program.For the first time inhis 78 years he isnow socializing andinvolving himself inactivities offered atthe senior center. Theresponse from otherparticipants has beenvery positive. Staff atthe developmentalcenter state that onthe days he attendsthe senior center heappears at the break-fast table with a largegrin on his face.
29

spend time with others their own age,
alternate programs for daily activities,
opportunities for socialization ratherthan isolation at home,
programs appropriate and interestingfor them,
opportunities for retirement and forsocial and recreational activities,
activities close to their homes,
a gain in self-confidence,
an increase in the degree of comfortthe individuals feel as part of a group,
the chance to learn new skills, and
the chance to learn that sometimesthey can function at near, or evenabove the level of non-disabled peorle.
Site Staff ReportWhen asked about the contributions the
seniors with developmental disabilities made totheir programs, site staff from the local demon-stration projects offered the following comments:
It has helped our regular program partici-pants to know how lucky they are just togrow old and not have a handicap.
Offered a new enlightenment for the wellelderly about developmental disabilities andwhat it means to be developmentallydisabled.
It makes our participants more aware andmore sensitive to the problems of otherpeople.
My seniors appreciate their own good healthfrom having seniors with developmentaldisabilities in their everyday life.
Makes our seniors reach out more andappreciate what they have both physicallyand mentally.
They ( the seniors with developmentaldisabilities) are usually cheerful andenthusiastic about program activities whichcontributes in a beneficial way to the
collective good spirits of the whole group.
They (the seniors with developmentaldisabilities) are often willing to volunteertheir time and abilities (to help the programrun better) ."
They help to monitor (in a day care setting)lower functioning frail elderly seniors whowander or may choke. They observebehavior and alert staff of potential prob-lem.s.
They show love and concern even withtheir disabilities.
They show they are human beings needinglove and care too.
They contribute friendship, help fellowseniors and chalknge established values andideas about individuals with developmentaldisabilities.
Now that we have identified the pro-grams most appropriate for integration efforts, weare ready to explain how to carry out integration.
How to Get Started:Networking
Getting started involves networking.Networking describes the sometimes informal, butdecidedly crucial, process of reaching out, makingcontacts, sharing information and building trustto help make things happen. One of the demon-stration project administrators from an agencyserving elderly persons with disabilities in Buffalo,N.Y., stressed the relationship of networking tointegration this way: she said, "The process ofintegrating older persons with developmentaldisabilities into local aging programs is a processof networking."
Successful networking involves ongoingcommunication and "base building" by havingthe people you know help put you in contact withthe people you need to know. Networking servesvarious functions:
Networking helps to identify a base ofinterest and build a constituency able tolend support, influence and help whennecessary.
22
3 0

Networking opens the doors toopportunity. Doors which might notopen any other way.
Networking is an essential process forbringing the two systems (aging anddevelopmental disabilities) together.
Networking for IntegrationTo successfully network, it is helpful to
identify the steps and sequence of steps needed tobring about the results you want to occur. Aswith all processes, the actual sequences will varywith location, the groups you are working with,and your own style. However, consider the fol-lowing steps:
Identify a core group of people fromyour system who are interested inintegration. Ask the people you knowto refer you to those they feel shouldalso be involved in initial discussions.
Meet informally as a small group toidentify needs and barriers, considerdirections and delineate resourcesavailable to help with integrationactivities.
Identify others in your system whoshould be involved in a general meetingon integration.
Meet as a larer group to review thesubjects discussed in the small group anddetermine consensus.
Identify the single person in eithersystem to be the liaison with providersin the aging network and its :ocal agingoffice and the developmental disabilitiesagencies.
If you have contacts in either networkwho are supportive of the integrationconcept, invite them to participate inyour large group meeting.
Ask the contacts to help you (ifnecessary) set up an introductorymeeting with the local agingoffice director. The introductorymeeting has several purposes:
to explain that you represent anetwork of provider agencies andorganizations serving seniors inthe developmental disabilities
community.
to share your need for place-ment opportunities in local agingprograms for seniors who may beeligible.
to invite the aging officedirector or the representative youmet with to attend a larger groupmeeting with your network todiscuss aging and developmentaldisabilities.
Ask the aging representative to alsoinvite others from their network toattend your meeting.
Similarly, ask the local developmentaldisabilities program administrator tosuch a meeting to help draw in the keyofficials.
Use the large group aging/develop-mental disabilities meeting to dialoguebetween networks and to begin to chartfuture directions for integration activi-ties. Try to come out of this initialmeeting with the following:
preliminary steps which shouldbe taken, and
a commitment to continue thetwo network dialogue and a datefor the next meeting.
If possible, meet with a core group ofkey people from both networks who arewilling to look at special concerns.
Remember, at the group meeting (if itisn't too large) to have all involvedintroduce themselves and their agency,and if time allows, tell what they do.
Networking and the networking meetingsset the stage for building the relationships neededto make integration a reality.
Setting Up Local Task ForcesIn several of the localities in which the
demonstration programs were conducted, localagency staff and administrators developed taskforces or committees on aging and developmentaldisabilities. A listing of such task forces or com-mittees is given in the appendix.
23
31

The setting up of such a task force mayneed to be a precursor to other activities whenyour focus of activities is in a highly urbanizedmetropolitan area. Rural areas, composed of fewagencies and interested or affected staffers, cancome to cooperative decision making over a mealat a local restaurant. However, highly urbanizedareas, with a complexity of staff interactions,agency territories, and disparate funding andoversight sources, need a more structured broker-ing approach.
If your needs are to organize such a groupin a major metropolitan center, we would suggestthat you follow the suggestions outlined above inthe section on Networking for Integration, butdirect your activities in a more formalized man-ner. For example, to get such an effort off theground, you may need a formal auspice -- that is,the sanction and support of a formative groupwhose reputation and role is such that it will drawparticipants to the task force. Such an entitymight include:
the local government mental healthor mental retardation/developmentaldisabilities department
the local county aging office ordepartment
a university center on developmentaldisabilities or gerontology/geriatrics
a foundation
a community planning body orinteragency council
a health systems agency or similargroup
Secondly, there may need to be muchmore formal approach to setting up the group.You may need to do the following:
You may need to send formal lettersinviting participation to the participat-ing agencies and their representatives.
You may have to think about whospecifically to invite who will "spark"discussions and keep them withinobjectives of the group.
You may need a "charge" from agovernmental entity to enable you tocoalesce the agency participants arounda tangible objective.
The Hudson Network
t first began with a fewphone calls among col-leagues; then more. Itseemed as if the staff at anumber of Hudson Valleyagencies needed to talk.The common topic wasthe seniors they wereserving. One administra-tor, viewed by the othersas a leader in their area,decided to call a meeting.The informal meeting ledto another where stateand regional officials wereinvited.
The group decided tobecome more formal,adopt a name and haveregular meetings. Nowthey meet bi-monthly andinvite speakers. At themeetings they exchangeinformation, discuss howthey handle regulationsand program require-ments, and help eachother with program prac-tices and advocacy. Whatstarted with a few like-minded persons exchang-ing telephone calls, hasblossomed into a formalnetwork that has author-ity and influence.
24

In one area of the statea network was formedthrough the partnershipof a college-based insti-tute of gerontology, alocal ARC and a staffdevelopment unit at theregional developmentaldisabilities agency.
The network group dida local needs assess-ment, surveying agen-cies about the peoplethey served, the servicesthey provided, and whatwas needed in theircommunity, that endedup as a broadly distrib-uted report. Otheractivities have includeda monthly trainingseries and conferenceson aging and develop-mental disabilities.
Annually they hold anawards dinner and rec-ognize the contributionof someone amongstthem who has donesomething special forolder persons with a de-velopmental disability
You may need to have a formal chairor convener appointed (from either thegroup or by the sponsor) to help leadthe meetings and keep the agenda ontask.
You may need to break up youroverall group into committees that arecharged with specific tasks.
You may need to be more formal inyour recording of attendance andminutes of meetings; these will need tobe distributed in a timely manner priorensuing meetings.
You may need other "carrots" to keepparticipants involved; these mightinclude helping design a short and longrange plan; recommendations for budgetrequests or allocations; publicity orpublic education campaigns; legislationreview and lobbying; needs assessments;and policy review.
How to Select ProgramsAffording people with developmental
disabilities the opportunity to participate incommunity senior citizen programs is what theintegration effort is all about. For many seniorswith disabilities, integration into local agingprograms provides the first opportunity to joinwith peers and be part of a true communityprogram.
Integration hinges upon matching upprograms with the needs of disabled seniors anddisabled seniors with programs. However, it isnot as simple as it seems. Integration, if it is to besuccessfully achieved, involves networking,planning, and the implementation of a series ofcoordinated activities.
This begins the section describing theactivities that should be undertaken to promoteintegration. The information was distilled fromthe experiences of county-based demonstrationprojects which successfully integrated seniors withdevelopmental disabilities into a variety ofgeneric aging programs.
The sections that follow address a varietyof topics related to helping you get started with an
25
3 3

integration effort. In this chapter, we haveincluded the topics of selecting adult day care,senior centers, and nutrition programs; andconsiderations of site factors. In the next chapterwe will discuss the selection of participants, theconcept of retirement for persons with develop-mental disabilities, and integration approaches.
In the presentation of the topics whichfollow, the following assumptions have beenmade:.
that interest in integration is comingfrom the disability network, and
that program selection (as opposed toselecting participants) is the firstconsideration.
Program selectionWithin the aging network there are three
basic types of congregate community programs.In most cases, one or more of the following typesof programs can be found operating in yourcommunity.
Social Adult Day Care ProgramsThese programs typically provide daytime
care and activities for seniors who are frail and/orrequire supervision. Activities and programs tendto be individualized to meet the specific needsand abilities of participants. They serve as arespite for families who must provide for theirelderly relatives.
Other program models of day care alsoexist. Medical day care programs, operated byagencies certified by the Department of Health,admit seniors with medical care needs who do notneed to be in a 24-hour nursing care setting.Psychiatric day care programs, operated by mentalhealth agencies, serve persons on an out-patientbasis who have emotional problems or mentalillness.
Admission:Admission requirements for social adult
day care may vary from program to program.Usually a person must be 60 years of age or olderto participate and have an impairment whichrequires some assistance or guidance with activi-ties of daily living. Some programs also take
people who have become socially isolated or arein need of companionship and stimulation.Others admit younger persons who are chroni-cally impaired. In contrast to senior centers ornutrition programs, persons using adult day careprograms are admitted only after a preliminaryscreening process.
Contributions and Fees:Most day care programs charge a fee based
upon a daily or weekly rate. At some day careprograms a contribution is requested, with theamount determined according to the disabledindividual's or his/her family's ability to pay.
Program Evaluation:In evaluating what goes on at day care
sites look for the following:
Personal care activities
Nutrition programming
Physical and recreational activities
Social work services
Transportation
Day Care PrograM Advantages:Programming is oriented on the basis
of individual need.
Staff have experience with personswho have various disabilities andimpairments.
Non-disabled participants sharesimilarities in functional abilities witholder persons with developmentaldisabilities.
Day Care Program Disadvantages:Staff ratios at day care sites tend to be
lower than those found in the develop-mental disabilities network day trainingand day treatment programs.
Social adult day care programs do notoperate under a fixed set of standards soprogramming may vary in offerings andquality from site to site. The StateOffice for the Aging is currently devel-oping standards for social model daycare.
26
3 4
.011

Categorical funding kr social adultday care programming does not exist.Most programs receive only limitedfunding from a sponsoring agency (ifthere is one) and are chiefly supportedthrough participant fees. The limitedfunding often precludes being able toprovide formalized counseling and casework services.
Tips for integrating a social adult day careprogram
Ensure that the functional abilities ofthe person selected for integration aregenerally the same as other participants.
Go over the program with the indi-vidual so they know what to expectfrom the program.
Be sure the day care program manageris briefed on the person who is beingplaced; give particular emphasis to anyparticularities in behavior.
Be sure that emergency contacttelephone numbers for the case manageror other person responsible for theindividual are available at the programsite.
Senior Center ProgramsThese programs typically offer a slate of
weekly activities often including a daily, hotlunch time meal. Some program sites have TV,game, craft, and other activity rooms wheremultiple activities occur simultaneously. Depend-ing on the center site, some activities may bedirected by paid or volunteer leaders. Participa-tion in activities is voluntary and on a first-come,first-served basis. Senior center site users gener-ally tend to be healthy, active and self-selectingin what they do at the center.
Admission:
Senior center programs are typically opento all persons aged 60 and over and often are opento persons in their fifties as well. Some centerprograms may require the user to be a resident ofthe locality in which the site is situated, if theprogram is exclusively supported with funds fromthe locality.
Contributions and Fees:
In gc neral, senior centers do not chargefor use. Most offer a "membership card" to
participants for a small fee (usually a dollar or so).The card provides the participant with a sense ofbelonging and may also entitle the holder todiscounts from area merchants. At some centers,the purchase of a "card" helps support a monthlynewsletter or a special center activity. Mostcenter participants purchase cards even though itis voluntary.
Senior centers are typically supported by avariety of funding sources. The funding, as a rule,does not cover the level of programming generallyfound at most senior center sites, so participantsare usually asked to pay a small fee to help coverthe cost of certain activities or events.
Prcsram Evaluation:In evaluating senior center programs look
for:
Attitude, personality and enthusiasmof the center director or program leader.
Meeters and greeters; these are thefolks who help new people feel comfort-able when they show up at the centerfor the first time.
Outreach activities especially withregard to serving individuals withspecial needs (low income, minority,frail, isolated, disabled, impaired andinstitutionalized elderly). New partici-pants are the future life blood of anycenter. Interest and efforts in outreachcan indicate if the center has an interestin reaching out to community residents.
Extent of participant involvement inthe center programs.
Perception and status of the centerwithin the aging community.
Linkages the center has with otherservices, activities and opportunities inthe community.
Senior Center Program Advantages:Provides a "right at home right in the
community" experience.
Offers the opportunity to socialize andbe part of a daily community group.
Offers a diversity of activities.
Environment can be stimulating.
27
3 5

Senior Center Program Disadvantages:Staff are not likely to have had
experience with the needs of olderpersons with developmental disabilities.
Supervision is minimal.
Environment is relatively unstruc-tured.
There is a potential climate for biasand discrimination against participantswith developmental disabilities.
Tips for Integrating Senior Centers:Select participants based on their
ability to function in a program for thewell aged population.
Set up a staff-sharir :lationship, ifpossible.
Inform senior center sta., chat partici-pants are developmentally disabled, andinform them of any special needs theymight have.
Focus on the abilities of the partici-pants while being honest about their
Be prepared to be very flexible andaccommodating.
Minimize as much as possible theextras that are requested of center staff.
Take the time to acquaint yourselfwith both the aging and the develop-mental disabilities systems. Know thepeople you will be working with, whatconditions they are working under, and,therefore, who would be most likely tobe enthusiastic about helping personswho are developmentally disabled, andwho is most approachable?
Expect that there will be individualswho will not :ike or accept olderpersons with developmental disabilities,just as there are those who do not likeor accept other people for other reasons.
Provide individualized training to thepeople who have been selected in the
skills needed to make the transition to asenior center. Good hygiene practicesand social skills are particularly impor-tant to acceptance at senior center.
Nutrition ProgramsNutrition (or congregate meal) programs
are those sites where a hot midday meal is pro-vided in a congregate setting to persons aged 60and over. Persons under age 60 may be served ifthey are a spouse or are disabled and live with aperson age 60 or older. The setting for a nutritionprogram may be at a day care site, senior center orcommunity site such as a church, echool, townhall or community center, etc.
The primary purpose of the nutritionprogram is to serve the noon time meal to thosewho wish to participate. Nutrition sites serve as afocal point and meeting place for seniors. Oftenthey are the only available places in the commu-nity where seniors can meet. Many sites haveactivities and programs around the meal.
A complementary program to the seniornutrition program is the home delivered mealsprogram, where a home-bound senior can receivea hot noontime meal.
Admission:Participation is open to all persons aged
60 and over. Spouses and companions under age60 and persons with a disability under the care ofnutrition program participants are also eligible toreceive a meal.
Contributions and Fees1
Nutrition programs do not charge a fee.Participants are requested to make a contributiontoward the meal. The amount of the suggestedcontribution is posted at every nutrition site.Sites use an envelope system to allow a person tocontribute what he or she can afford In NewYork, sites generally ask for a donation of between$1.00 to $3.00, although the actual cost of themeal may be greater.
Site Evaluation:In evaluating nutrition program sites,
look at the following:
Attitude, personality and enthusiasmof the nutrition site r maga.
28
36

M ary came from Poland whenvery young. She married and hadfour children. Her husbandphysically abused her to the pointthat she began having seizures.She was placed in a state school,never to see her family again. Atthe time, she spoke very littleEnglish. When given an IQ test,her language barrier was nottaken into account, and she wasrated mentally retarded. Recentlydeinstitutionalized, she now livesin a community residence.
Mary exhibited many behaviorproblems but, nevertheless, wasplaced for a trial period at thesenior center. Her behavior prob-lems ceased and she has becomean accepted member of the cen-ter. She plays cards with a selectgroup of females and participatesin any activity offered. She hasbeen assigned a Senior Compan-ion. She attends part-time at thesenior center 2 id part-time at anadult day care program so thather medical needs can be moni-tored. Since her placement sherarely has behavior problems atthe residence. All Mary wantedwas an opportunity to sit backand enjoy life and at the age of76 she deserves that.
Involvement of the site council. Sitecouncils are participant groups whomeet to discuss how the meals, programsand other aspects regarding the site areworking.
Programming available at the site.
Policy for table selection. Find out ifparticipants are allowed to excludeothers by saving seats or if a "first to thetable best seated" policy is in use.
Nutrition Program Advantages:
Sites are found in most communities.
Provides a community location for ahot meal in the company of peers.
Social atmosphere provides opportu-nity to make friends.
Site offers the opportunity to volun-teer setting up the tables for the meal orhelping prepare meals for the homedelivered meals program if food prepara-tion is done on site.
Nutrition Program Disadvantages:
Most nutrition-only sites are open foronly a few hours a day.
Activity programming at sites is oftenlimited or non-existent.
Openness to new participants may bea problem.
Tips for integrating nutrition programs:
Find a buddy or companion who willaccompany the person on his or her firstfew visits.
Consider taking several peopletogether to the site so they will feelmore comfortable.
Work out the donation arrangementsbeforehand; make sure the person hasthe expected donation to give at thedoor.
Ensure that the person has reasonablygood eating skills so that he/she will not
29
3 7

stand out as different.
Brief the person on how the meals arepresented and ensure that he or she isexperienced with the style meal serviceused at the site.
Go over the week's menu beforehandso the person can express any concernsover food preferences before going; picka day when the meal served is some-thing that the person likes.
Use a site near where the person lives,so if they wish, they could walk to thesite.
Site Considerations:Based upon these descriptions, the types
of sites selected for integration depends upon thefollowing factors:
What types of sites are available?
Is the programming appropriate?
Is the site in the appropriate commu-nity or area?
Is the facility accessible to personswith developmental disabilities?
Is transportation to the site available ornot too expensive or difficult to find?
Are the hours of operation compat-ible with your staffing schedule?
Is the site manager or program direc-tor interested in working with you toprovide opportunities for your seniors?
Further thoughtsCongregate aging service programs
supported with Older Americans Act funds arerequired to be open to participation by all seniors,but, in reality, are constrained by funding limita-tions. Nutrition programs, for example, oftenlimit the number of meals they are able to serve atany one site and typically have a maximumnumber they can serve during any funding year.
Successful integration comes from coop-eration developed through understanding, com-passion, and sensitivity to needs of persons withdisabilities rather than the force of law.
As a general rule, local aging programsites can refuse to accept seniors who are unquali-fied for some valid reason other than that they aredevelopmentally disabled.
The best sites and programs for seniorswith developmental disabilities are those whichprovide the best opportunity for integration tosucceed.
The site manager, center director orprogram leader sets the climate for the site.
Do the followingInventory the aging program sites
in area.
Visit the sites, look at the facilities and stay long enough to get afeel for what is happening there.
Talk to the site director.
Talk to the participants.
Look for an environment thatencourages friendship.
Trust your gut level feelingsabout the appropriateness of thesite.
Try not to get "hung up" with asite director who may be reluctantto let persons with disabilitiesparticipate. Move on.. For everyreluctant program site director,several others stand ready andwilling to work with you.
How to Involve ParticipantsIn this chapter we cover the topics of
selecting participants, whether to integrate peopleindividually or in groups, and how to aeriallyconduct integration activities. Also covered areretirement considerations and preparatory stepsfor transitioning to retirement. Each of the areascovered in this chapter are related to how toengage the older person in the decision makingprocess about integration.
Selection of participantsThe participant selection process goes
hand in hand with the site selection process.
30

Both are interwoven and interdependent to theextent that a person who may fit in at one type ofsite may not work out at another type of siteeven though the programming there is similar.Therefore, a thorough knowledge of site opera-tion and climate for acceptance is essential and inmost cases a prerequisite, to selecting the peoplefor integration. One of the demonstration projectdirectors summed it up this way when she said,"Seniors who have developmental disabilitieshave struggled for acceptance their whole lifelong. This may be their final program. It shouldbe one with an atmosphere of acceptance."
One of the keys to integrating olderpersons with developmental disabilities intocertain types of community aging programs is infinding people who have the potential to beaccepted at the site. Acceptance at certain sites isessential to integration. Without acceptance bythe peer group, integration in its fullest sense, cannot really occur. Nowhere is acceptance moreimportant than at senior centers and nutritionsites.
Participant Selection for SeniorCenters and Nutrition Sites
Senior centers and nutrition sites areenvironments in which the emphasis is on socialskill and behavior than outright intelligence.This means persons who have appropriate socialbehaviors but lower cognitive abilities could beand should be considered for integration intosome senior centers and nutrition sites.
Senior centers and nutrition sites do nothave the ability or capacity to handle participantswith behavior problems. For these sites, considerseniors who do not have problem behaviors andthose with only occasional occurrences of aproblem behavior.
In general, persons considered forintegration into senior centers and nutrition sitesshould:
be 60 years of age or older
be continent
be self-medicating
be no danger to themselves or others
have appropriate skills in grooming,
hygiene, eating
have a minimum of problem behav-iors
have appropriate social behavior
have the capacity for appropriatesocial interactions
The demonstration sites of the Integra-tion Feasibility Demonstration Project were ableto integrate several persons with problem behav-iors into senior centers and nutrition sites. Inthese situations we carefully watched to see if thenew settings had an affect on behavior. We werepleased to find:
occurrences of problem behaviordeclined to virtually none or onlyoccasional.
there were no increases in problembehavior for any of the persons in thisgroup who were integrated into seniorcenters and nutrition sitcs.
social intenictior ,,proved dramati-cally.
social behavior improved.
The greatest improvement occurred inthe development of friends and friendships.
This positive outcome means that selec-tion of participants based upon hard and fast rulesmay, in fact, disqualify those with the potential togrow and benefit from the opportunity to be withpeers in a community environment. With that inmind and if a site (through its site manager ordirector) is willing to take a chance, we stronglysuggest trying also to integrate persons with minorbehavioral problems but assessed as having thepotential to grow and improve.
Participant Selection for Social AdultDay Care Programs
Unlike participants at nutrition sites andsenior centers, who tend to be "well" elderly,those attending social adult day care programs aretypically persons who have impairments whichlimit their activities of daily living. In thisregard, persons with developmental disabilitiesshare many similarities with the clientele servedat day care sites.
31
BEST COPY AVAILADLE
3 9

Initial screening for dayicale site integra-tion should be on the basis of how well theirfunctional ability and behavior, rather than theirdisability, coincides with that of the participantsalready enrolled in the program.
Since day care programming takes placein a social environment, individuals consideredfor integration should have the potential to adaptto a social setting and not have problem behav-iors or be a danger to themselves or others.Programming at day care sites is usually paced toan older, more dependent population so personsselected should be matched to the same activitylevel occurring at the site.
In general, persons selected for integra-tion into SOCial model adult day care programsshould:
be 60 years of age or older
be of no danger to themselves orothers
be able to function on a level compa-rable to the clientele being served in theprogram, and
not have problem behaviors
Social model day care programs may varyin their ability to serve persons who are:
not self medicating
incontinent
have dietary restrictions, or
(at the other end)
function at a high degree of inde-pendence
Contact the programs directly to find outif they are able to accept persons with theselimitations or capabilities.
Importance of ConfidentialitySince many older persons with develop-
mental disabilities may have been served whenthey were younger by the mental retardationsystem, some cautions apply with regard toconfidentiality of records and personal infonna-tion. Written permission is needed in order torelease Nrsonal or confidential information.
Exercising common sense when givingout information will help protect these individ-
ual's civil rights and avoid violations of themental hygiene law. As with any of the clienteleof a program, you should be sensitive to needs forconadentiality. Following these basic guidelineswill help you to make informed decisions.
The key point to keep in mind, is thateveryone has a right to privacy and not to havethe details of one's private life shared with others.
Before revealing information about anindividual served by your agency to someone else(whether it be another person using the program,someone from another agency, the press, orrelatives), stop and ask yourself whether it is thekind of information you would want releasedabout yourself. Even if you decide it is ok, go astep beyond and ask if it is the kind of informa-tion that might cause anyone to avoid or demeanthat individual, to dislike them, or to regard themas less than equal.
Another guideline you should alwaysfollow is "the need to know." Before revealinginformation about someone in your program, askyourself whether the person needs to know thatinformation. If not, don't reveal it. Also, don'task state or other private agencies to revealinformation about a person in your programwhich has no relevance to the service you areproviding.
The mental hygiene law prohibits therelease of personal or clinical information aboutindividllals with mental disabilities who are, orwho were, served by a sr-ate program. Don't askstaff of other programs to violate the law.
Participant Choiceintegration, if it is to be successful, also
involves giving the part'zipants a voice andchoice in the matter. Once a person has beenidentified as a candidate for integration, theyshould be given a choice as to whether or notthey would like to participatein the program. Ifthey are reluctant, it may help to arrange a visitfor them to see the site or to even participate on atrial basis. Often reluctance has to do with beingreticent, not wanting to change one's routine, orlosing familiar social contacts.
Those who agree to participate at theprogram site should be assessed on a regular basisby the developmental disabilities agency to
32
4('

determine how the setting is working out forthem. Sometimes a participant may find that heor she no longer wants to attend the program for avariety of reasons. 'These reasons may includefinding the other participants more disabkd thanoneself, not "connecting" with the activities androutines, or some other personal factor.
For example, we found one participant,who was attending a day care program on aregular basis, deciding that he no longer wantedto be around other "older persons" and wanted togo elsewhere. In this instance - self-image,derived from being seen with other older persons -was a factor (even though the participant wLsgenerally of the same chronological age). Thisphenomenon, by the way, is not uncommonamong many older adults. In another instance, aparticipant wanted to return to the workshop hewas previously in because he felt the loss of hisworkshop's week., check.
hen selecting participants for integra-tion, remember the following key points:
Participants need to be given a voiceand choice in helping to determinewhat is appropriate and what is workingfor them.
Participants' ongoing reaction to asite into which they have been intro-duced should be assessed on a regularbasis..
RetirementAmong persons who are not vocationally
impaired, there are often a number of considera-dons that impact decision-making related toretirement. One is related to the primary gainassociated with work, a salary; this is usuallysubstituted by Social Security Z)enefits or apension upon retirement. Another, is related tothe secondary gains associated with the workplace, such as friendships, a place to go, and thepersonal identity that is &fined by one's job.Further, most persons, wheA considering what todo upon leaving the workfors.e, think in terms ofwhat will replace work. This notion of replace-ment leads to "retiring to." It is easy to achieve"retirement from," but it is not that easy toachieve "retirement to."
For anyone, the social and personalchanges associated with retirement can often betraumatic when bridging does not occur as part of
ExwwwW/St
the transition process. For a person who isdisabled, and has been dependent upon his or herworkplace for social sustenance, the loss orchange of friends when moving to a new programcan pose a significant barrier. This is why select-ing among retirement options available to seniorsin the community can help to plan the "retire-ment to."
Some strategies that could mitigateproblems amciated with retirement for personswith developmental disabilities include:
the use of pre-retirement counseling
partial retirement (where the individ-ual slowly transitions from work toretirement), ond
increasing socialization through theuse of non-disabled "senior friends" andinvolvement in socialization programs.
A "senior friend" can help a person witha disability acclimate to new settings that offer re-tirement activities as well as serve as a bridge tothe friends he or she may have left in the worksetting. One source of such "senior friends" is theOMRDD's Senior Companion Program.
One area that poses problems for agenciesworking with retirement age individuals is thelack of a "pension policy." Most disabled indi-viduals do not receive earned social securitybenefits or pensions to use as income in retire-ment. For those individuals who are earningmoney in sheltered workshops or in some type ofday programming, the lack of money uponretirement :an become a major problem. Even ifthe actual amount received was small, the earnedmoney has strong symbolic value.
Many older workers who are developmen-tally disabled are reluctant to retire when they arefaced with the loss of their cherished income.This results in a dilemma: whei faced with adesire to stop working and relax but lose income,or continue to work and lose the freedom thatmay come from retirement, most elderly workerschose to continue to work. Consideration needsto be given to the impact of loss of income uponthe individual's retirement and acceptance of in-volvement in a new program site.
There is another side to this problem.Involvement in senior group activities that areoffered at senior centers, such an outing or a trip,may include a nominal fee. Further, even partici-
3EST COPY AVAILABLE
4 1
3 3

pating in the congregate meals program involvessome expense since sites ask for a donation. Anolder person should have the dignity associatedwith "paying your own way" since many senioractivities are peer oriented. This consideration ofmaintaining the older individual's dignity andself-respect when he or she moves from the worksetting to a local senior program, is very impor-tant.
Consequently, it is advisable to carefullyreview what concerns the older person may haveabout retirement and then employ a strategy thatwill bring about "retiring to." This may mean:
reviewing with the persons whatretirement means to him or her andwhat they want to do
discussing the retirement options
implementing phases to pre-retire-ment that employ visits, partial involve-ment in a new site, and pairing with a"buddy" to aid in the social adaptationto a new site.
Pre-Retirement preparation ActivitiesThe transition to senior age activities and
programs needs to be handled with sensitivity andcare. Like other people, a person with a lifelongdisability needs to experience life's milestones.The transition from worklife to retirement is oneof those transitions. Remember that retirementparties and retirement gifts are important, con-crete, transitional features. However, pre-retire-ment counseling and other types of preparationare also important. Transition formalities need tobe preceded by discussions of retirement andplanning for it.
It is important that a person who is ableto continue working be given the option ofcontinuing to work. That does not necessarilypreclude integration into the aging system pro-grams, because the integration can be done on apart-time basis, leaving time for employment.But the individual should always be offeredoptions, and the wishes of the individual shouldhe respected.
One problem can arise out of a situationin which the elderly person is no longer able toconduct his or her work to the satisfaction of thejob supervisor, and the job supervisor feels that
the person should leave work. Such a situationwill require special attention by the case workerand the caregiver. It could affect the success ofyour integration effort, so you should be aware ofwhat's happening.
In all situations, counselors need tosupport and encourage persons, especially in theearly stages of a new program. Let them knowretirement is normal and okay.
Pre-program visits for participantsThe person needs to be introduced to the
new program gently. There will be uncertaintyand there might be resistance. Remember uponretirement, the individual is leaving a familiarsetting and friends. Upon entering a new pro-gram you are expecting the individual to formnew social attachments and participate in new ac-tivities on their own.
As with other people, this is oftendifficult for persons with limited intelligence orwho are physically disabled. Positive reinforce-ment is critical at this stage.
If the person has been working, whetherin sheltered or supported employment or in thegeneral work force, the work ethic is likely to befirmly entrenched in that person's mind. Therehas been little preparation for retirement andlittle anticipation of it.
The person's informal social network isoften tied to the job. Wages, an importantingredient of our society, are an important issue tosuch individuals. Often when older persons leavea work setting they forfeit their weekly check.This can be an obstacle to integration and needsto be considered carefully.
Further thoughts on pre-retirement:Before changing the individual's
program engage him or her in a discus-sion ab it the process, what they canexpect from the change and the benefitand losses, and most importantly, whatthey would like to do.
Once, the transition has been agreedupon, engage in a formal transitionritual -- a party or ceremony for retire-
34

ment.
Try retirement planning within agroup, so a sense of solidarity is built upand provides a cushion for the change.
Find a means to replace the valuedworkshop check (if there is one) with aretirement pension check.
Try visits to places that the personmight like to go upon retirement, suchas the local senior center or nutritionsite.
Try a phased retirement process,through which the individual graduallydisengages him or herself from theircurrent program.
Integrating Individuals vs.Groups
Integration can be successfully achievedby placing people one at a time as well as byintegrating small groups into selected sites.While this manual is based on the premise thatpeople will be integrated as individuals - evenwhen several persons are placed at one time - it isalso possible for a group of people who have beentogether over a period of time to be successfullyintegrated into a local aging program. As youwill see, both approaches have advantages anddisadvantages.
Integration can be achieved in two ways:
Group integration
Individual integration
Group IntegrationOne of the Office for the Aging demon-
stration projects used group placement as anintegration methodology. The demonstrationproject was under the auspices of a developmentaldisabilities agency in a large city. The plan wasto integrate people who had been together foryears, as complete groups, into a number ofneighborhood senior centers.
Part of the rationale for the approach wasthat it might help to make for an easier transi-tion. It is not unusual for the participants atsome senior centers to form cliques making it
difficult for new people, irrespective of anydisability they may have, to comfortably partici-pate. At some older and well established neigh-borhood senior center sites it can be a barrierwhich can be difficult to circumvent.
By having the disabled seniors enter thesite as a group they, in effect, became their ownclique and the immediate pressure to be a part ofthe existing group was gone. Each member of thegroup was free to move out into the larger group,find other friends, join other cliques. But ifthings did not work out -- say, if a person wasrejected -- they could always return to the originalgroup.
By coincidence, in this example, theseniors were brought as a group of five to thecenter on a day when special festivities weretaking place and the mayor was visiting. In thecommotion of all that was ,oing on, the comingof the new participants went largely unnoticed.
To make group integration work and tostimulate the group within a group to interact, anessential ingredient was provided. The develop-mental disabilities agency assigned a full time staffperson to serve as a program aide at the seniorcenter. In addition to helping with the newparticipants, the aide found enjoyment in takingover and running the center's ceramics programfor all who were interested.
In this example of group integration, theaide was the necessary catalyst and was needed toassist with the additional work load and helpstructure activities which would bring peopletogether. Without the staff aide, it is unlikelythat the center would have taken on the addi-tional responsibility so easily or that meani .gfulintegration would have occurred at the sire.
The group (4-5 persons) integrationapproach offers some of the following advantages:
It is more efficient (timewise) tointegrate a group into a site than oneindividual at a time.
It tends to be a more cost effectiveway to achieve integration.
It provides a certain level of comfortto the seniors being integrated becausethey are attending the site with theirfriends.
35
4 3
It becomes attra:tive to the localaging program sin when staffing assis-tance is offered.
The group integration approach also hassome potential disadvantages:
It is a more difficult concept to "sell"in the aging community unless "perks"such as shared staff are provided.
Aging service sites are typically fearfulof the impact a group of seniors withdevelopmental disabilities might haveon the regular level of site participation.
It requires an ongoing effort at the siteto structure developmentally disabledseniors group participation into theexisting program.
Initially, the participation of a groupof developmentally disabled seniors islikely to be met with resistance from theregular participants.
Further thoughts concerning groupintegration:
Group integration at a number of seniorcenter sites was successfully achieved due to someof the following factors:
The developmental disabilities agencythat selected the people to be placedwas well known and respected in thecommunity in which it operates.
The senior center directors did nothave to be convinced to try groupintegration at their sites. They{{wanted" to see if it would work success-fully.
The developmental disabilities agencycoordinator for the integration projectwas skilled in working with the agingcommunity and sensitive to the needsand concerns of those staffing the agingservice programs in their area.
There was a willfr s on the part ofthe developmer !- Ailities agency toprovide nece: :ing assistance tothe aging sites.
Integration of individualsIn many ways, even if group integration is
being conducted, it still concerns the integrationof individuals.
The methodology for integrating peopleindividually varied only slightly among thevarious demonstration sites. Most importantly, allof the demonstration project directors stressed thefollowing: because integration involves moving aperson to a new setting, and away from where heor she have been, sensitivity is needed to ensurethat the person being integrated will not beshuffled from one site to another. They feltstrongly it was important to consider each suchmove as possibly the "last" move for that person.
The following are key points to rememberwhen integrating individuals:
The site manager or program directorshould fully understand the nature of thepersons' disability and the behaviorscommon to that disability. Keep inmind, most people don't know whatconstitutes "being developmentallydisabled" or what might be expected inthe way of attending behavior.
Always explain to the site manager orprogram director why this particularindividual needs to be placed and howthey will benefit from placement at thesite.
Always introduce the site manager orprogram director to the senior and theircompanion, if one is assigned. It may benecessary to spend the first day at thesite with the senior, companion and sitemanager to make everyone feel comfort-able.
Consider offering both the senior andthe site manager a trial visit at the site.Both may feel better if they know theyhave the option to change their mind.
Rather than have everything hinge onone visit, arrange for a series of trial visits andthen evaluate the experience with both the seniorand site manager.
36
4 4

To Tell or Not to TellThe question of whether the regular
program participants should know who is comingto join them is one that vexed some of our dem-onstration program coordinators. From their ex-periences there wasn't a clear verdict. It appearsthat site type, site staff and level of disability ofthe person being placed, hold the keys as to howthis should be handled.
Here are some general guidelines:
Most social adult day care participantsare in the program because they havefunctional impairments and need to besupervised. In this e .Lionment it isnot likely that it woukl be necessary tomake an announcement that a personwith a developmental disability will beparticipating.
Senior centers and nutrition sitestend to be highly social environments.In most cases, a person with any kind ofvisible deficit or differentness is going tobe noticed. The site manager may needto explain to the regular participantswhat is happening and enlist thesupport of the group so the new personis properly welcomed. Conversely,saying nothing and letting the individ-ual be Their own advocate may be asattractive.
Integration TipsSelect potential sites based on the
quality of leadership found at the site.
Set up a staff-sharing relationship, ifpossible.
Inform aging program staff of thenature of the developmental disability,and of any special needs the seniorsbeing integrated might have.
Focus on the abilities of the people tobe placed while being honest abouttheir limitations. Don't define them bytheir disabilities.
Be prep.ired to be very flexible and
accommodating.
Minimize as much as possible theextras that are requested of site staff.
Build in incentives which will makelocal senior programs want to takepersons with disabilitfrs.
Take the time to acquaint yourselfwith both the aging and the develop-mental disabilities systems. Get toknow the people you will be workingwith, what conditions they are workingunder, and, therefore, who would bemost likely to be enthusiastic aboutintegration. Find out who is mostapproachable.
Follow through on all assurances ofsupport that you make.
Answer the questions honestly andwithin the bounds of confidentiality,about those you wish to place. Alwaystry to focus on the person rather thanthe disability.
Respond quickly to concerns of allinvolved: seniors integrated, families,center staff, program staff, regularprogram users, and others. Making sureeveryone is as comfortable as possiblecan be the key to success, especiallyearly on.
Expect that there will be individualswho will not like or accept developmen-tally disabled seniors, just as there arethose who do not like or accept otherpeople for other reasons.
Provide those selected for integrationwith individualized training in the skillsneeded to make the transition into asenior center. Good hygiene skills areparticularly important to acceptance.
Do not define the program to theperson who is disabled as one in whichhe or she is "being integrated." Definethe program on its own terms withoutrelating it to this person's specialcircumstances. It is an opportunity tomakc new friends and do differentthings.
37
.1 5

Participant Selection TipsSelect people who can "make it."
Select people who would enjoy beingwith other people and have a positiveattitude toward socialization.
Select people who would want toparticipate in this kind of program.
Select people who would be able toderive positive benefit from the experi-ence.
Select people who would be physi-cally and emotionally ready for the give-and-take of social integration.
1,00k at the site first and ask "who arethe people who will be able to adaptand eventually fit in?"
How to Use Staff and CompanionsTo successfully carry out integration,
someone has to do the work. The effort needsstaff -- someone in-charge, one or more persons towork directly with the people being integrated,and some experienced persons to help guide, andevaluate the integration effort. The effort canalso use "buddies" or companions -- personsdrawn from age peers who wish to help and aidthe person with a disability.
While staff is needed, you do not need anempire. The leader of the effort can be someonewith other duties who works part-time to bringintegration about. Those who work with thepeople who are being integrated can be part-timeor even temporary employees. The professionalswho may be involved, need not be officially onstaff. They can be people from other agencieswho are willing to help, either voluntarily or on apaid basis.
Staffing for Different PurposesConsider staffing for these various rea-
sons:
First, depending on the size and scope ofthe integration effort, full or part time staff maybe needed to coordinate integration activities
between aging and developmental disabilitiesagencies.
Second, at the program site, thought hasto be given to the number and types of staffneeded to aide in the integration effort.
Third, staff sharing arrangements need tobe considered when additional staffing is neces-sary to the success of the effort.
As you see, setting up the staff can begeared toward various directions. The goal shouldbe to create, with the resources available, a staffthat can handle the effort you contemplate.
To conserve resources, build communica-tions, and enhance the chances for success ofyour integration effort, look for opportunities toshare resources and staffing with other agencies.Some examples drawn from the pilot projectsinclude:
an adult day care project director whoalso coordinated a county wide integra-tion effort.
staff from a developmental disabilityagency being shared with a senior centerto help with a small group of develop-mentally disabled seniors who wereintegrated into the center. The sharedstaff also helped the non-disabledpeople with the center's programs andactivities.
area agencies for the aging thatprovided office space and staff time forconducting integration efforts.
Staffing arrangements to make integra-tion happen are virtually limitless. The key is tobear in mind that it can be dont, and to look foropportunities to do it. Let's explore the differentaspects of staffing and some means to do it.
Depending on the size and scope of theintegration effort, full or part time staff may beneeded at an overall level to coordinate integra-tion activities between aging and developmentaldisability agencies. In the State Office for Aginglocal demonstration projects, the coordinationeffort was managed at a county level by perma-nent staff from either an aging or developmentaldisability agency supported with special fundingmade available by the State.
38

Staffing For Interagency CoordinationDuring the course of the demonstration
projects, we found that it makes sense to developa focal point or clearinghouse for coordinatingintegration activities. With a focal point, coordi-nation is enhanced. The sharing of informationand resources is also made most useful. A focalpoint also reduces duplication efforts and offers aneconomy of scale by concentrating the manpowerneeded to effect integration in one place.
Finding staff to coordinate is usually doneby identifying an agency and a staff memberwithin the agency who is interested and capableof serving as the focal point for helping withintegration activities. Once designated, network-ing activities can beOn (see How to (Jet Started -page 27).
Site StaffingThe majority of the local demonstration
sites did not require permanent staff to be addedat the locations where people were integrated.The demonstration sites did, however, usecompanions to assist with the entry process and insome cases, had the companions continue on atthe sites with the seniors who were integrated.(More about thy use of companions later in thischapter.)
The necessity for adding new or addi-tional staff to help the seniors who are integrated,varies according to the following factors:
site type (senior center, nutritionprogram, adult day care program),
level of disability and/or activity levelof the seniors being placed, and
number of persons being placed at thesite.
Senior centers and nutrition programsplanning to serve people with more pronouncedimpairments are likely to need additional staff.Day care programs tend to be familiar with seniorswho are impaired and may be able to cover newparticipants with existing staff, if operatingcapacity is not exceeded.
If only a few people are placed at a site,and they integrate well with the existing users, itis not likely that the number of permanent sitestaff will need to be increased.
One of the SOFA demonstration projectsintegrated groups of five people at one time intosenior centers. The scale of the integration effort,as well as the impact on the site required thatconsideration be given to increasing the staff ateach center. The developmental disabilitiesagency found an imaginative solution by using astaff sharing approach.
Shared StaffOne consideration an agency can give to
enhancing the potential for integration is toincrease the available staff at a senior program sitethrough a staff sharing approach. We found thatwhen this was tried within the demonstrationprojects, it proved to be very fruitful. In oneexample, the developmental disabilities agencyout-stationed full time staff at a number of seniorcenters.
This shared staff approach proved to bean innovative and successful solution to theproblem of increasing site staff and finding peoplewith the appropriate skills and knowledge to helpwith the seniors who would become part of thecenter's clientele.
For the center, it was an opportunity topick up a new staff member. This was an oppor-tunity warmly received because many seniorcenters are minimally staffed. The center directorwas particularly enthusiastic about the staffplacement. The out-stationed staff person ran thecenter ceramics program, and tended to the needsof five seniors with developmental disabilitieswho had begun using the site. The reaction fromthe out-stationed staff person was similarly enthu-siastic; she enjoyed the opportunity to becomeinvolved in the center's program.
Staff sharing is an option which tends tofit in nicely with the concept of service integra-tion. Site staff too, can be integrated to theadvantage of all concerned - the host agency, thereferring agency, the traditional users of theprogram, and the seniors who may already befamiliar with the staff person assigned to the hostagency. Also, when budget or hiring limitationsexist, staff sharing should be considered as a wayto address those concerns.
Do the following:
establish an area focal point 'r
4 7
,OMMEN
.39
clearinghouse for coordinating integra-tion efforts.
designate a person to have responsi-bility for coordinating integrationactivities.
consider sharing and out-stationingstaff with aging service providers asmeans of maximizing effectiveness andminimizing costs.
Use of Companions or VolunteersThe use of a "buddy system" or assigned
companions varied significantly among the SOFAdemonstration projects. Some of the projectcoordinators felt that the companions wereessential to the success of the integration effortthey mounted. Some found the companions tobe an impediment.
One demonstration project coordinator,expressed the importance of companions this way:"the use of companions can determine the successof a placement. Without them, integration maybe. jeopardized."
Another project coordinator was againstthe use of companions and didn't use any. Thereason stemmed from personal experiences wherecompanions, because of their own needs, fostereddependency when independent behavior was thegoal.
Our experience with the integrationdemonstration projects confirms that where it isappropriate and necessary, companions can be anintegral part of the integration process. Havingprogram companions provides some of the follow-ing advantages; it:
helps to ease the fears a new partici-pant may have
helps to ease the fears an agingprogram site manager may have
gives the community valuable andmeaningful volunteer opportunities
provides both companion and seniorwith an opportunity for companionshipand friendship
Finding companionsFinding companions to serve on a full or
even part time basis, can be a challenge. Manyprograms, however, have been successful infinding reliable volunteer companions to helpwith integration activities. Here are some guide-lines for finding companions:
Start within your own agency. See ifthe friends, relatives and acquaintancesof your regular agency work force areinterested in becoming companions.
Check with the following agencies forleads on potential companions:
- county aging office,
- voluntary action center,
- Green Thumb Program, and
other area volunteer organizationssuch as:
- Retired Senior Volunteer Pro-gram
- Senior Companion Program,
- other agencies using volunteers.
Also look for companions from amongthe following:
- retired special education teachers
- retired nurses
- churches and synagogues
- residential centers for seniorcitizens
- college volunteer programspreferring to work with seniors
- community civic groups
Advertise for companions in the localmedia. Get the assistance of a local advertisingagency to develop a catchy lead line advertise-ment. Like the Uncle Sam recruiting poster fornew Marines, aren't you too just looking for a"few good people"? See also, if the advertisingagency will donate their services.
Peers can also be companions. Withinthe broad range of possibilities is also the notionof having peers serve as companions. Several ofthe demonstrations used seniors with develop-mental disabilities as companions to persons in a
40

day care program who were more profoundlydisabled.
Be sure to explain your needs and willing-ness to exchange volunteer duties with thosewho have scheduling o- transportation problems
In New York, a good source of seniorcompanions to aid adults with developmental dis-abilities is the NYS OMRDD Senior CompanionProject. Modelled upon the federal program setup under the National Domestic VolunteersServices Act, the NYS OMRDD Senior Compan-ion Project is totally state-funded.
There are senior companion programstations throughout the state and located withineach of the OMRDD's district offices. Under theprogram, low income senior volunteers arerecruited to work for 20 hours per week. Inreturn, they receive a tax-exempt stipend, mealsand transportation assistance.
Many senior companions in the OMRDDprogram are assigned to older persons withdevelopmental disabilities. A good number areassigned to senior program sites throughout thestate. For information on the NYS OMRDDSenior Companion Project write the program c/oNYS OMRDD, 44 Holland Avenue, Albany, NY12229-0001. Your program could qualify as avolunteer placement site.
Companion selectionAgencies and organizations using volun-
teers often have personality profiles to vide themin the selection process. Use a profile whichmeets your needs. Look for people who also havethe following qualities or potential for developingthe following qualities:
sensitivity,understanding,commitment,reliability, andpatience
Companions can also assist with siteactivities and provide care to those who need it.Finding a volunteer with leadership and activityskills is a special plus.
IntroductionsIntroducing the companion to the site
staff is an important part of a new companion'sorientation. Site staff introductions serve to buildconfidence and establish the foundation forcommunication between the parties involved.
If the plan is for the companion (and alsothe senior being placed) to blend in unobtrusivelywith the regular site participants, the initialcompanion/site staff meeting will help to estab-lish the ground rules for how that will be handledand bow emergencies will be managed.
The introductory meeting will also helpto assure the site staff that the companion is thereto help and that the new participant will not be aburden or mean extra work for them.
Once trained, the companion should bematched appropriately with the person who willbe attending the senior program site. The seniorsand companions generally need to becomeacquainted before going to a site. The method ofintroduction should follow the developmentaldisabilities agency's established protocol for suchmeetings. The meeting should also be assessed tofind out if compatibility problems exist.
lithe companion/senior match is success-ful, a site visit can be arranged. This should beviewed as an opportunity for the senior to deter-mine if he would like to continue on at the site.
Introducing a person to a site can also bedone with the assistance of a family member,caregiver, or case worker with whom the person iswell acquainted, if a companion is unavailable toassist.
lithe trial visits prove successful, thereshould be a follow up meeting between the sitemanager, companion, case worker responsible forthe person and the integration coordinator. Atthe meeting, the aging program site manager orprogram director should be given the following:
information related to the person'sneeds,
pertinent behavioral information,
information concerning possibleemergency needs, telephone numbers,etc.
information about the companionand where to call if the companion has
41

an emergency, and
any other information which willassist and prepare key site personnel tohelp with the needs surrounding theintegration of a developmentallydisabled person at their site.
Replar participation can follow, litheplan is for the companion and person to blend inunobtrusively into the site program, the compan-ion should keep an eye on the person withouthovering or being perceived by other people asthe guardian for a particular person.
While a companion's presence can serveas a security blanket of sons for the person, whomay have no other friends at the site, the com-panion's role, where appropriate, should be to en-courage and help the person to develop friendsand friendships. Ideally, it would be to get alongwithout the constant assistance of the compan-ion, if possible. Once genuine integration hasbeen accomplished, the companion may nolonger be needed at that site or for that particularperson.
Companions can be a valuable additionand asset to an integration effort. But consideralso that an integration effort built upon the useof companions is also an effort dependent uponthe availability of companions.
Training for Companions,Participants and Site Staff
Most developmental disabilities agenciesoffir a training program which can be appropri-ately tailored to prepare companions, participantsand aging program site personnel for integration.
Companions, like any other volunteers,benefit from well designed training activitizs.Most agencies using volunteers have a suitabletraining program which can be utilized in wholeor part, if appropriate.
The training program for companions,participants and aging program site personnelshould have the following purposes:
To explain the purpose of integration
To explain the similarities and the
A t one of thedemonstration sites,the 'buddy system'worked very well.Two new seniors,coming from thesame home were in-troduced to theadult day servicegradually. For acouple of weeksthey attended onlythe nutrition partof the day care.Once comfortablein the setting, theyasked if they couldparticipate in thewhole day careprogram. Thus,they were wel-comed into daycare.
One woman bringsin pictures she hasdrawn for the staffalong with wildflowers she haspicked. She saidshe thanks God forletting her come tothe Friday AdultDay Care Program.
42

differences between the disabled personand the mainstream person
To acquaint companions and staffwith the special needs of the disabledperson and the ways to handle thoseneeds
To acquaint companions and staffwith action to be taken in case specialproblems arise
To explain the reason why participa-tion is so important for persons withdisabilities
To explain developmental disabilitiesand mental illness (the differencebetween mental retardation and mentalillness is not often understood)
To explain their role and what isexpected
The NYS OMRDD has a training packetspecifically for the training of new senior com-panion volunteers. This orientation packet canbe usei to train companions drawn from othersources. To obtain a copy of this training/orientation packet write the program cio NYSOMRDD, 44 Holland Avenue, Albany, NY12229-0001.
Additional Training ResourcesThere are a number of resources you can
tap to aid in training staff, participants andvolunteers in better understanding aging anddevelopmental disabilities. These include:
the training curriculum on develop-mental disabilities available through theOMRDD's district office staff develop-ment units.
the training curriculum on aging anddevelopmental disabilities availablethrough the OMRDD's bureau of agingservices.
the training program availablethrough the University of Rochester'sAging and Developmental DisabilitiesTraining Program.
the training available through thenetwork of area agencies on aging.
For information on the training programofferings at the University of Rochester's Aging &Developmental Disabilities Training Program,contact the Program's Director, University ofRochester, Box 671, Medical Center, 601Elmwood Avenue, Rochester, NY 14642; 71,:275-2986.
How to Support IntegrationThe integration process also involves a
number of aspects which support an integrationeffort and make it successful. These supportaspects include:
funding
outreach
public relations
record keeping
monitoring and evaluation
In this last section you will find adviceand information on these various supportingaspects.
FundingFinancial supports for older persons with
developmental disabilities using aging networkprograms can come from a number of sources.OMRDD funds both residential and day servicesin a variety of ways. With regard to day services,currently no dedicated funding exists that specifi-cally is set aside for seniors. However, existingprogram funding can be adapted to finance aseniors program. For example, for seniors livingat home, $1000 a year is available under thefamily support program. Family support moniesare available from the DDSO. Such monies canbe used to pay for respite in adult day care andother special assistive services.
In other instances, when the seniors are"620 eligible," that is, they had been institution-alized for a specified period and otherwise meeteligibility requirements under section 620 of thesocial services law, they can be supported by100% funding from the state to the program viathe county community services board. Again,such funding can pay for adult day care services.
In other circumstances, when the county
43
5 1

will agree to pay the local share, day trainingmonies can be made available under the localassistance program. In these instances, suchmonies can be used to pay for adult day careservices. Another potential funding source is theday training innovations initiative currentlybeing tried out in several counties. Under thisfunding, the state pays 100% of the costs of daytraining services.
Programs interested in OMRDD fundingshould contact their DDSO and discuss thealternatives available to them.
OutreachOur experience with the demonstration
projects indicated that less than half of personsaged 60 and over, who are developmentallydisabled, were known to the formal developmen-tal disabilities provider system. Given this, it isour expectation that you may wish to reach out toolder persons currently unknown to your agency.
The following is a list of a variety ofoutreach activities that can help to locate seniorswho may benefit from being placed in communityaging programs. In order to locate such people:
Use publicity releases or advertising tolet people in the community know whatyou're trying to do. Be sensitive as tohow you present your outreach effort tothe public.
Contact churches and church spon-sored social service agencies whoseleaders might have reason to be aware ofdisabled persons in the community.
Contact support groups, fund-raisingagencies, and volunteer groups thatwork with or for disabled people.
Contact caregivers of persons knownto be disabled to find out if they knowof other disabled individuals.
CAmtact adult homes, nursing homes,hospitals, senior citizen high rises andother congregate units, and shelterswhere disabled persons might live.
Contact the Department of SocialServices, home health care agencies, theAssociation for the Blind, adult day carecenters, Family Support Services, and
the local housing authority, as well asother agencies that might deal withdisabled individuals.
Consider enlisting student internsfrom local university departments ofsocial work and gerontology to gatherinformation about persons with de el-opmental disabilities in the community.
One problem an outreach effort canencounter is the matter of not being ccrtainwhether someone qualifies as being developmen-tally disabled, especially in the case of mentalretardation. An elderly person who is retardedbut who has lived a long time in the communitymight be able to pass as non-handicapped. Anelderly person who is functionally impaired andseems to have difficulty might seem to be re-tarded.
While the functional distinctions maynot really matter and since the important aspect isservice need, identification of a person with adevek\pmental disability is linked to being able totrace evidence of disability back to childhood.This identification may only prove useful ifadditional services are being requested of thelocality's developmental cl.isabilities providers --such as housing, family ',,upport services, or casemanagement. Such documentation may benecessary to release funds to support the services.
One outreach tool is a check of func-tional life indicators. They help show lifelongdeficits. Many local agencies use such tools.Check around to locate one useful to your pur-poses.
Networking helps in the outreach proc-ess. It is recommended that contacts be initiatedwith a broad number of local agencies. Talksbefore human service organizations can also helpin alerting the agencies of the outreach effort.
Public RelationsOne of the first decisions to be made is
whether an integration effort should be publicizedto the general public at all. In some localities itmay be valuable to do so and in others it maycause problems for the integration effort. For thisreason, it is important to know your locality inorder to decide whether publicity will be helpfulor harmful.
44
5 2

In a rural county, "grapevine" publicitymay precede published information. See if the"grapevine" can be used to help set the climate foracceptance. Newspaper articles can also behelpful in educating and informing the commu-nity of new developments. (See example of suchnewspaper stmies in the appendix.) In a smallcommunity such newspaper articles are likely toinclude people who attend the senior programsites. If local program participants are cliquishand do not readily accept strangers, then suchpublicity might lead to failure. Always considercarefully the possible impact of publicity.
In urban areas, human interest storiesusually tend to engender support. But, smallneighborhood programs where integration hasbeen tried and is successful, may find difficultygetting media exposure.
Public relations efforts can includearticles in general circulation and professionalpublications. It can include presentations to thegeneral public and to professional groups. It caneven include attending public hearings conductedby the aging system or the developmental disabili-ties system to discuss the issue.
It can include articles in newsletters forRSVP, home health care, and other agencies.The effort might include form letters to contactthe developmental disabilities network, volun-teers, agen-..ies, and others for information andreferrals. One useful way of handling suchinformation is to first send a letter, enclosing aflyer about the plogram, and then following upwith telephone call.
Another way is to make presentations todevelopmental disability system organizations andto volunteer organizations, visiting aging networkagencies and speaking with coordinators. Suchnetworking is very important. It is sometimesdifficult to contact the right people.
When considering a public relationseffort do the following:
keep in mind your geographic areaand ask yourself if the story will lead togreater or lesser receptivity by programusers?
use a personal touch to your stories,highlighting a "buddy" arrangement orpraising a volunteer.
give a human interest angle to a dis-abled senior. Often the outside worldhr o idea how hard life has been forinis person or what the opportunity toparticipate with peers now means tothem.
spend some time with the reporterfrom your local paper who covershuman interest stories -- this can helpin giving your story a proper framework.
Record KeepingExtensive record keeping has been a
hallmark of the developmental disabilities system.Naturally, when seniors from the disabilitiessystem become enrolled in local aging programs,reporting and monitoring requirements followthem. While there is an ongoing attempt madeto keep paper work to a minimum, there are in-stances where reporting requirements becomequite onerous. For aging program providersserving persons from the disabilities system, therule of thumb to follow is: if the paperwork isgoing to be too much, ask the disability agency toassume the responsibility for it.
It is reasonable for the aging programprovider to keep a minimum of records, usuallyattendance logs, information on acclimation, andother data that may be used to trigger payments.Goal planning and service plans should be left tothe referring agency. Participant records shouldbe kept in a locked cabinet to maintain theconfidentiality of all persons, disabled or non-disabled, who are using the program.
Of special value to both the aging anddisabilities regional networks will be your experi-ences with the problems you encountered and thestrategies you used to resolve the problems. Shareyour experiences.
Monitoring and evaluationMonitoring and evaluation should be an
ongoing part of the integration process. Underthe SOA demonstration project, the local dem-onstration programs monitored the progress of theintegration activity at aging program sites by usingthe following types of evaluations:
Site evaluation
45
r 3
Participant evaluation
A site evaluation is used periodically toidentify the responses of site staff and non-developmentally disabled site participants to theintegration of persons with developmental dis-abilities. By conducting site monitoring on aregular basis it is possible to identify and addressproblem areas as they come up.
A site survey should look at the follow-ing:
attitudes of the regular participants andsite staff toward participants with develop-mental disabilities
space sharing, interaction and participa-tion by the regular participants
development of friendships and interper-sonal relationships by the regular participantswith those who have disabilities
Potential problem areasA participant evaluation or assessment
should be used to periodically monitor the prog-ress of participants who have been integrated intolocal aging programs. Unlike typical user evalu-ations, we found the most useful information on apersons progress at a site to come from assessmentsmade of the following areas:
extent of social interactions with staff,other disabled peers, regular participants,strangers, etc.
friendships with staff, disabled peers, non-disabled peers and others.
increase or decrease in problem behaviorssuch as verbal and physical aggression,socially inapprcpriate behaviors, refusal toparticipate, withdrawal, stealing, etc.
Agencies using companions shouldmonitor the volunteer's progress and satisfaction.An approriate monitoring format can usually beobtained from a director of volunteer services.
Future TrendsUp to this point the manual has focused
on the integration of persons with developmentaldisabilities into aging network programs. The
developmental disabilities system however, offersa unique and exciting potential to serve non-developmentally disabled seniors who qualify for asocial model adult day care environment,
Throughout the state, agencies whichhave primarily served persons with mental retar-dation or other developmental disabilities arenow establishing and operating specialty programsopen to all seniors who might benefit. Many ofthese programs were originally built off themental hygiene system's "day training program"model. Now they are also serving non-handi-capped seniors in senior day programs. Theseprograms can be found in areas where:
social model adult ci y care does not exist
integration efforts have not yet begun orbeen successful
local resources are limited in terms ofoperating social model adult day care
developmental cisabilities agencies arewell established and have decided to offersenior services as part of their services' array
the disability agencks and county agingoffice have worked out an arrangement forthe site to be designed as an adult day careprovram
These programs offer an opportunity forolder persons who have functional limitationsthat are age-associated such as dementia, severemental degeneration resulting from Alzheimer'sdisease, or where severe physical limitationsrequire special care to benefit from an existingresource in the community.
Such programs serve as an a example ofprogrammatic integration. This means that theprogram, itself, has become integrated into thegreater aging network through a number ofmeans, such as:
being designated an adult daycare programsite by the county aging office
having the site be designated a congregatemeal site under Title III of the Older Ameri-cans Act
having the seniors who are enrolled in theprogram co-participate with other impairedseniors in activities developed by the countyaging office or one of its local agents, or
developing the site's program suchthat a portion of the enrollee's time is
46
5 ,f
R ecently an ARCopened a senior dayprogram in a countywithout any adult daycare program. Many ofthe adults in the ARCprogram, which in ap-pearance and manner islike many other seniorcenters, have retiredfrom workshops or em-ployment. They are freeto come whenever theywish and participate in arange of activities. Nowthe board has opened upthe program to otherseniors in the commu-nity, who because oflatelife impairments,need a similar program.A recent visitor com-mented that she couldn'ttell who was who.
spent at other locales, such as anotheradult daycare program, senior center oractivity program, or congregate meal site
One benefit of developmental disabilitiessenior day programs is that 11 le programs can offera transitional experience anu learning opportuni-ties. Disability programs tend to be highly struc-tured and focussed on goal-directed activities. Incontrast, aging network programs are relativelyunstructured, leaving participation and involve-merit in activities largely to the individual.
To experience satisfaction and success intransit ;oning to using community aging networkprograms, many disability agencies are recognizing
that individuals retiring to .:enior activities need aperiod of acclimation. This time helps relieve theconstant structure and prepares thtm for retire-ment where volition and self-definition are key toparticipation. These senior day programs serve asa bridge to community aging network programs.
How to Open OMRDD Senior Dayprograms to the Aging Community
As localities examine the costs of provid-ing special services to the seniors with impair-ments in their community, the notion of coopera-tive programming and site sharing will becomemore attractive. If you, as a service provider, areinterested in serving non-developmentally dis-abled seniors, do tile following:
contact the county aging office anddiscuss becoming designated as an adult daycaresite
contact the operator of the county nutri-tion program and discuss haying your seniorday program become a congregate meal site
discuss with your board the notion ofopening up enrollment to other seniors withsimilar functional deficits and needs
contact the senior companion projectcoordinator at your local B/DDSO and discussbecoming a senior companion program site
discuss with your county aging office howyou might enter into an agreement to sharetransportation responsibilities for seniors inyour local area
get listed in the county aging office's localresource directory as an adult daycare site,disabled seniors assistance service, or otherservice -- depending upon what you wish tooffer
participate in local senior day activitiesand fairs where aging network agencies displaytheir wares and promote their services
participate with the county aging office incasefinding efforts of homebound seniors withdisabilities who are currently unknown to thelocal care systems
47

APPENDICES Overview: The New York State
Office for the AgingAging - Developmental Disabilities
Demonstration Project
Project Name: The Aging/DevelopmentalDisabilities Integration Feasibility
Demonstration Project.Project Type: Three-year demonstration
April 1, 1986 - March 31, 1989.
Purpose: The purpose of the demonstrationproject was to test the feasibility of serving develop-mentally disabled elderly persons in congregatesettings such as senior centers, nutrition sites andsocial adult day care programs.
State Agencies Involved: The New YorkState Office of Mental Retardation and Developmen-tal Disabilities; the New York State DevelopmentalDisabilities Planning Council; the State Office for theAging.
Funding: The Project was funded withFederal monies from the New York State Develop-mental Disabilities Planning Council. The Projecthas an annual budget of $102,000. The State Officefor the Aging provides a 30% matching share. TheDevelopmental Disabilities Planning Council providesthe remaining 70%.
Project Operation: During Phase I theProject identified barriers and developed strategies forplacing developmentally disabled eldeily persons intoexisting aping network programs.
Phase 11 involved setting up and monitoringfour local county demonstration projects. Two urban(Erie and Monroe) and two rural (Madison andCattaraugus) counties were selected. Each localdemonstration project developed its own methodologyfor integrating developmentally disabled elderly intolocal aging network programs.
The local demonstration projects were underthe auspices of the following sponsors:
Erie - People Inc., (A not-for-profit agencywith a long history of serving persons with develop-mental disabilities) Buffalo, New York.
Monroe - Regional Council on Aging, Inc.,(Operator of the Carson Meyer Senior Center)Rochester, New York.
Madison - Madison County Office for the
48
5 6

Aging (the area agency on aging), Morrisville, NY.Caugraugus - Cattaraugus County Office for
the Aging (the area agency on aging), Olean, NY.Phase Ill included the tabulation of data from
site and client evaluations as well as the developmentand publication of a project "How To" manual. Themanual was designed to be a guide for helping bothaging and developmental disabilities service providersto integrate developmentally disabled seniors intoappropriate local aging service programs.
The State Office for the Aging/Developmen-tal Disabilities Project was conducted with the supportof the New York State Office of Mental Retardationand Developmental Disabilities.
The Project findings include the following:Elderly persons with developmental
disabilities can be successfully integratedinto existing aging programs.
It is necessary to lay a foundation forinteragency cooperation at the local levelwhich includes communication amongproviders, sharing of information, andinteragency referrals.
Integration can be achieved usingdifferent methodologies including placingpeople individually or in small groups.
Programmatic and policy barriers need tobe addressed first for coordination andintegration to be successful.
Elderly persons with developmentaldisabilities can and do benefit from beingintegrated into local aging services pro-grams. For example, persons integratedinto seni..ir centers experienced an increasein new friendships and a decline in problembehaviors.
Personnel and financial resources areneeded to support integration activities.
It was necessay for the State to providead hoc technical assistance in order tofacilitate local cooperation.
Local integration demonstrationsexceeded the goal of placing 55 persons byactually integrating 70 persons into variousaging network programs.
Office of Mental Retardation and Develop-mental Disabilities Contact Person: Dr. MatthewJanicki, (518) 473-7855
State Office for the Aging Contact Person:Philip Le Pore, (518) 486-2727
New York State Developmental DisabilitiesPlanning Council Contact Person: Arthur Maginnis,(518) 432-82.33
5 7
49
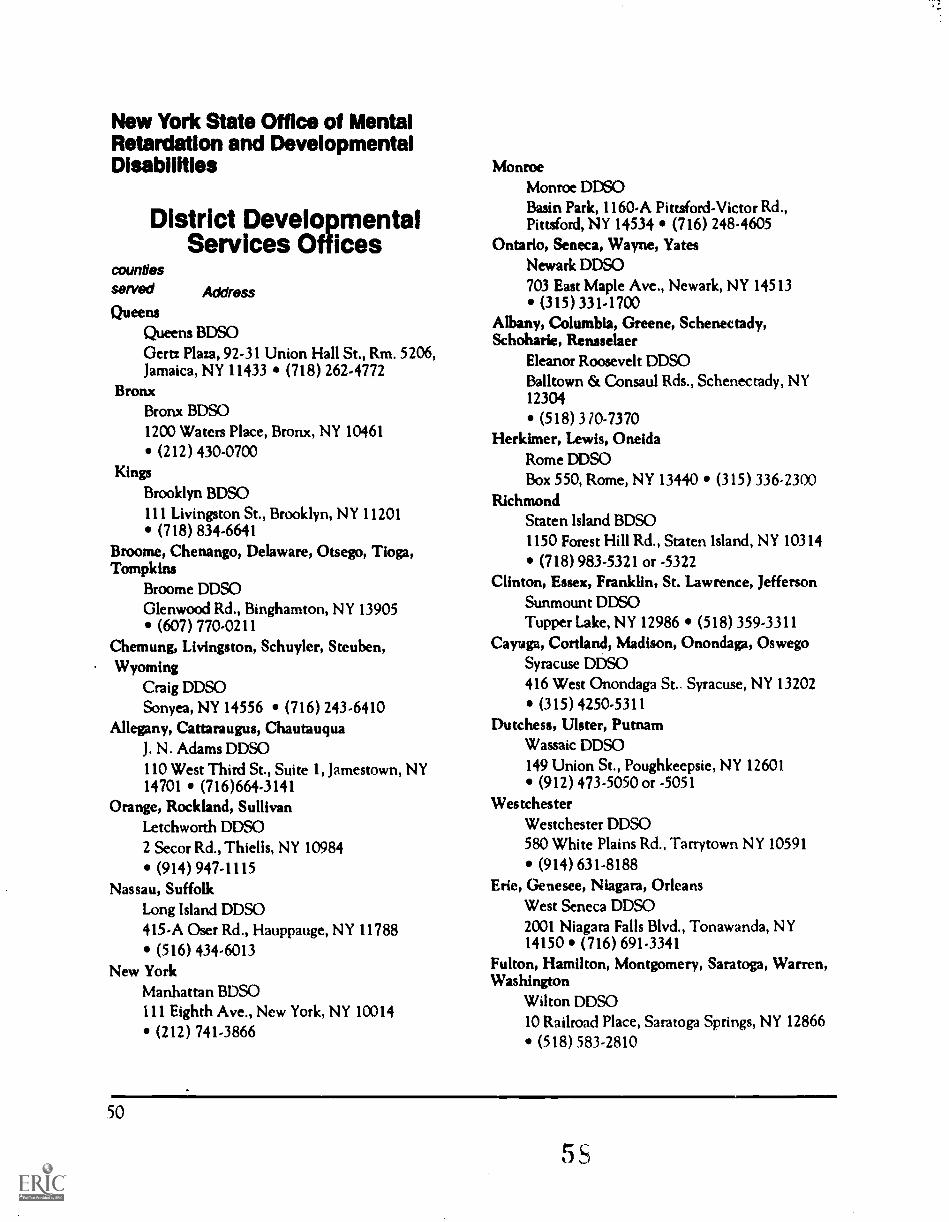
New York State Office of MentalRetardation and DevelopmentalDisabilities
District DevelopmentalServices Offices
countiesserved
QueensQueens BDSOGertz Plaza, 92-31 Union Hall St., Rm. 5206,Jamaica, NY 11433 (718) 262-4772
BronxBronx BDSO1200 Waters Place, Bronx, NY 10461
(212) 430-0700Kings
Brooklyn BDSO111 Livingston St., Brooklyn, NY 11201
(718) 834-6641Broome, Chenango, Delaware, Otsego, Tioga,Tompkins
Broome DDSOGlenwood Rd., Binghamton, NY 13905
(607) 770-0211Chemung, Livingston, Schuyler, Steuben,Wyoming
Craig DDSOSonyea, NY 14556 (716) 243-6410
Allegany, Cattaraugus, ChaumuquaJ. N. Adams DDSO110 West Third St., Suite 1, Jamestown, NY14701 (716)664-3141
Orange, Rockland, SullivanLetchworth DDSO2 Secor Rd., Thiel Is, NY 10984
(914) 947-1115Nassau, Suffolk
Long Island DDSO415-A Oser Rd., Hauppauge, NY 11788
(516) 434-6013New York
Manhattan BDSO111 Eighth Ave., New York, NY 10014
(212) 741-3866
Address
MonroeMonroe DDSOBasin Park, 1160-A Pittsford-Victor Rd.,Pittsford, NY 14534 (716) 248-4605
Ontario, Seneca, Wayne, YatesNewark DDSO703 East Maple Ave., Newark, NY 14513
(315)331-1700Albany, Columbia, Greene, Schenectady,Schoharie, Rensselaer
Eleanor Roosevelt DDSOBalltown & Consaul Rds., Schenectady, NY12304
(518) 370-7370Herkimer, Lewis, Oneida
Rome DDSOBox 550, Rome, NY 13440 (315) 336-2300
RichmondStaten Island BDSO1150 Forest Hill Rd., Staten Island, NY 10314
(718) 983-5321 or -5322Clinton, Essex, Franklin, St. Lawrence, Jefferson
Sunmount DDSOTupper Lake, NY 12986 (518) 359-3311
Cayuga, Cortland, Madison, Onondaga, OswegoSyracuse DDSO416 West Onondaga St.. Syracuse, NY 13202
(315) 4250-5311Dutchess, Ulster, Putnam
Wassaic DDSO149 Union St., Poughkeepsie, NY 12601
(912) 473-5050 or -5051Westchester
Westchester DDSO580 White Plains Rd., Tarrytown NY 10591
(914) 631-8188Erie, Genesee, Niagara, Orleans
West Seneca DDSO2001 Niagara Falls Blvd., Tonawanda, NY14150 (716) 691-3341
Fulton, Hamilton, Montgomery, Saratoga, Warren,Washington
Wilton DDSO10 Railroad Place, Saratoga Springs, NY 12866
(518) 583-2810
50
5

New York Aging & DD NetworkGroupsHudson Valley - Catskill Network on Aging
Alvah Canfield, Ph.D.Sullivan County ARC, IMIX 812, SouthFallsburg, NY 12779
(914) 434-3415
Westchester Interagency Geriatrics Task ForceSharon Ge lfandWestchester DDSO, 580 White Plains Ave.,Tarrytown, NY 10591(914) 631-8188
Western New York Consortium on Aging andDevelopmental Disabilities
Mary Petrakos TerranovaPeople, Inc., 1550 Hertel Ave., Buffalo, NY14216(716) 832-4444
Monroe County Council on Aging and Developmen-tal Disabilities
Jenny OvereynderUAPDD - Box 671, University of Rochester,601 Elmwocxl Ave., Rochester, NY 14642(716) 275-2986
SouthernTier Aging and Developmental DisabilitiesNetwork
Diane McDanielsOtsego Regional Center, Edmunston Pro-gram, RD 4, Box 51D, Oneonta, NY 13820(607) 965-8114
Rome DDSO Elderly Advisory CommitteeKathy BishopStaff Development, Rome DDSO, Box 550,Rome, NY 13440(315) 339-6750 ext. 327
Central New York Network on Aging & Develop-mental Disabilities
Angela Z. VanDerhoofOneida COunty ARC, 14 Arnold Ave., POBox 4759, Utica, NY 13504(315) 735-6477
orRonald Lucchino, Ph.D.Institute of Gerontology, Utica College,Burrstone Rd., Utica, NY 13502(315) 792-3129
Erie County Developmental Disabilities Subcommit-tee on the Elderly
Tena GarasHeritage Center, 101 Oak St., Buffalo, NY14203
(716) 856-4201
NYC Task Force on Aging and Mental Retardationand Developmental Disabilities
Marilyn HowardHunter-Brookdale Center on Aging, 425 E.25 St., New York, NY 10010(212)481-4350
North Country Aging and Developmental Disabili-ties Network
Manon BalchLexington Center, 465 North Perry St.,Johnstown, NY 12095(518) 762-0024
Cortland Area Task Force on Aging and Develop-mental Disabilities
Judith HayesSequin Community Services, Syracuse DSO,55 Tompkins St., Cortland, NY 13045(607) 756-5637
NYS OMRDDBureau of Aging Services
Matthew P. janicki, Ph.D.NYS OMRDD, 44 Holland Ave., Albany,NY 12229(518) 473-7855(518) 473-9695/FAX
NYS Office for the Aging - Aging and Developmen-tal Disabilities Project
Phil LePoreState Office for the Aging, 2 Empire StatePlaza, Albany, NY 12223-0001(518) 486-2727(518) 474-0608/FAX
51
5 9

Local Offices for the AgingListed by County
AlbanyCo Dept. for the Aging & Handicapped, 112
State St., Rm. 710, Albany, NY 12207 518 447-7180Allegany
Co. Office for the Aging, 17 Court St.,Belmont, NY 14813 716 268-9390Broome
Co. Office for the Aging, Co. Office Bldg.,Government Plaza, Binghamton, NY 13902 607778-2411Cattaraugus
Co. Dept. for the Aging, 255 N. Union St.Olean, NY 14760 716 373-8032Cayuga
Co. Office for the Aging, 160 Genesee St.,Auburn, NY 13021 315 253-1226Chautauqua
Co. Office for the Aging, Hall R. ClothierBldg., Mayville, NY 14757 716 753-4471Chemung
Co. Office for the Aging, 425 PennsylvaniaAve., Elmira, NY 14904 607 737-5520Chenango
Area Agency on Aging, Co. Office Bldg., 5Court St., Norwich, NY 1.3815 607 335-4624Clinton
Co. Office for the Aging, 137 Margaret St.,Plataburgh, NY 12901 518 565-4620Columbia
Co. Office for the Aging, 71 North 3rd St.,Hudson, NY 12534 518 828-4258Cortland
Co. Office for the Aging, Co. Office Bldg., 60Central Ave., PO Box 5590, Cortland, NY 13045607 753-5060Delaware
Co. Office for the Aging, 6 Court St., Delhi,NY 13753 607 746-6333Dutchess
Co. Office for the Aging, 488 Main St.,Poughkeepsie, NY 12601 914 431-2465Erie
Co. Dept. of Senior Services, 95 Franklin St.,Erie Co. Office Bldg., Buffalo, NY 14202 716 858-8526Essex
Co. Office for the Aging, Elizabethtown, NY12932 518 873-6301 Ext. 370Franklin
Co. Office for the Aging, Co. Court House, 63W. Main St., Malone, NY 12953 518 483-6767
FultonCo. Office for the Aging, 19 N. William St.,
Johnstown, NY 12095 518 762-0650Genesee
Office for the Aging, Batavia-GeneseeSenior Center, 2 Baak St.,Batavia, NY 14020 7163433-1611Greene
Co. Dept. for the Aging, 19 S. Jefferson Ave.,Catskill, NY 12414 518 943-5332Hamilton
See Warren/HamiltonHerkimer
Co. Office for the Aging, Co. Office Bldg.,109-111 Mary St., PO Box 267, Herkimer, NY 13350
315 867-1121Jefferson
Co. Office for the Aging, 250 Arsenal St. Wa-tertown, NY 13601 315 785-3191Lewis
Co. Office for the Aging, Lewis Co. OfficeBldg., PO Box 408, Lowville, NY 13367 315 376-5313Livingston
Co Office for the Aging, Livingston Co.Campus, Bldg 8, Mt. Morris, NY 14510 716 243-7520Madison
Co. Office for the Aging, Box 250, Rt. 20,Morrisville, NY 13408 315 684-9424Monroe
Co. Office for theAging, 375 Westfall Rd.,Rochester, NY 14620 716 274-7800Montgomery
Co. Office for the Aging, 380 Guy Park Ave,Amsterdam, NY 12010 518 843-2300Nassau
Co. Dept. of Senior Citizen Affairs, 400Countyseat Dr., 2nd Flr., North Wing, Mineola, NY11501 516 535-5814Niagara
Co. Office for the Aging, Switzer Bldg., 100Davison Rd., Lockport, NY 14094 716 439-6044Oneida
Co. Office for the Aging, Co. Office Bldg.,800 Park Ave., Utica, NY 13501 315 798-S771Onondaga
Metropolitan Commission on Aging, CivicCenter, 13th Flr., 421 Montgomery St., Syracuse. NY13202 31i 435-2362Ontario
Co. Office for the Aging, 3871 County Rd. 46,Canandaigua, NY 14424 7i6 .396-4041
OrangeCo. Office for the Aging, 60 Erie St., 3rd Flr.,
Goshen, NY 10924 914 294-5151 Ext. 1560
52

OrleansCo. Office for the Aging, Orleans Co.
Admin. Bldg., 14016 Rte 31, Albion, NY 14411716 589-5673 or 7004 Ext. 191Oswego
Co. Office for the Aging, Co. Office Com-plex, 70 Brunner St., PO Box 3080, Oswego, NY13126 315 349-3484Otsego
Co. Office for the Aging, Co. Office Bldg.,197 Main St., Cooperstown, NY 13326 607 547-4233Putnam
Co. Office for the Aging, 110 Old Rte. 6Bldg. A. Carmel, NY 10512 914 225-1034Rensselaer
Co. Dept. for the Aging, 1600 7th Ave.,Troy, NY 12180 518 270-2730Rockland
Co. Office for the Aging, Bldg. B, Health &Social Services Complex, Pomona, NY 10970 914354-0200 Ext. 2100St. Lawrence
Co. Office for the Aging, Sears Bldg.,Canton, NY 13617 315 379-2204Saratoga
Co. Office for the Aging, 40 South St.,Ballston Spa, NY 12020 518 885-2212Schenectady
Co. Office for the Aging, 117 Nott Terrace,Schenectady, NY 12308 518 382-8481Schoharie
Co. Office for the Aging, 122 E. Main St.,Cobleskill, NY 12043 518 234-4219Schuyler
Co. Office for the Aging, 336-338 W. MainSt., Montour Fails, NY 14865 607 535-7108Seneca
Co. Office for the Aging, 1 DiPronio Dr.,Waterloo, NY 13165 315 539-5655Steuben
Co. Office for the Aging, 117 E. Steuben St.,Bath, NY 14810 607 776-7813Suffolk
Co. Office for the Aging, 395 Oser Ave.,Haupauge, NY 11788 516 853-3610Sullivan
Co. Office for the Aging, 100 North St., NewCo. Government Ctr., Monticello, NY 12701 914794-3000Tioga
Co. Office for the Aging, 231 Main St.,Owego, NY 13827 607 687-4120Tompkins
Co. Office for the Aging, 309 N. Tioga St.,Ithaca, NY 14850 607 277-0148
UlsterCo. Office for the Aging, 1 Albany Ave.,
PO Box 1800, Kingston, NY 12401 914 331-9300Ext. 578Warren/Hamilton
Counties Office for the Aging, Warren Co.Municipal Ctr., Lake George, NY 12845 518761-6347Washington
Co. Office for the Aging, PO Box 58,Whitehall, NY 12887 518 499-2468Wayne
Co. Office for the Aging, 16 William St.,Lyons, NY 14489 315 946-5624Westchester
Co. Office for the Aging, 214 Central Ave.,White Plains, NY 10606 914 682-3000Wyoming
Co. Office for the Aging, 76 N. Main St.,Warsaw, NY 14569 716 786-8833Yates
Co. Area Agency on Aging, 5 Collins Ave.,Penn Yan, NY 14527 315 536-2368New York Cit:
Dept. for the Aging, 2 Lafayette St., NewYork, NY 10007 212 577-0848St. Regis-Mohawk
Office for the Aging, St. Regis-MohawkIndian Reservation, Hogansburg, NY 13655 518358-2272 Ext. 221Seneca Nation of Indians
Office for the Aging, 1500 Rte. 438, Irving,NY 14081 716 532-5778
53

Resources
Books on Aging and Disability
Aging and Developmental Disabilities: Issues and Approachesby Matthew Janicki and Henry Wisniewski.
This extensive text, containing 26 chapters by various experts in the field, covers various agingand biological processes, legal and advocacy considerations, epidemiology, research and planning, serviceissues and practices, and residential and day programming, and family concerns (427pp). It is availablefrom Paul H. Brookes Publishing (PO Box 10624, Baltimore, MD 21285 or call 800 638-3775).
Aging and Mental Handicapby James Hogg, Steve Moss and Diana Cooke.
The authors present a review of and ageing and mental handicap literature from a Britishperspective. Chapters cover background issues, epidemiology, medical and psychiatric issues, intelli-gence and adaptive behavior, work and retirement, interventions for changing behavior, residentialissues, and informal supports (411pp). It is available from Rout ledge Chapman and Hall, Inc. (29 West35th Street, New York, NY 10001).
Aging and Mental Retardation: Extending the Continuumby Marsha M. Seltzer and Marty Wyngaarden Krauss.
This American Association on Mental Retardation monegraph includes a review of communityand institutional-based day and residential programs currently in operation, and provides specific detailsof services models that appear to be particularly effective, as well as information on the role and structureof informal support networks (187pp). It is available from AAMR, (1719 Kalorama Road NW, Wash-ington, DC 20009 or call 800-424-3688).
Expanding Options for Older Adults with Developmental Disabilities: Practical Guide to AchievingComnumity Access
by Marion Stroud, Evelyn Sutton and Ruth Roberts.
This book is based upon the experiences of Dr. Roberts and her colleagues with Project AC-CESS in Ohio (251pp). It contains background information on aging, the developmental disabilities,the needs of elderly persons with a disability, community organization, and treatment planning and im-plementation. A companion book, Activities Handbook and Instructor's Guide, is also available (255pp).The Handbook contains helpful information on specific program activities. Both are available from
H. Brookes Publishing (PO Box 10624, Baltimore, MD 21285 or call 800 638-3775).
NIMMIAM
Other Useful Publications
All of Us: Strategies and Activity Ideas for Integrating Older Adults with Developmental Disabilitiesinto Senior Centers
by Eunice Thurman.
This 109pp monograph covers a variety of activity suggestions for involving seniors in the day-to-day program of a senior center. The activities are presented within a means to evaluate the seniorspotential for participation. It is available from Senior Center Integration Project, Kent Client Services,1225 Lake Drive, S.E., Grand Rapids, MI 40506
Aging and Disabilities: The Intersection of Needs and ResourcesDeveloped at the University of Maryland, this is a training manual for workers in aging and
developmental disabilities agencies that covers a variety of topic areas useful in the implementation ofintegration efforts. Copies of the training manual are available from the Center on Aging, University ofMaryland (College Park, MD 20742-2611 or call 301 454-5856).
Aging and Lifelong Disability: Partnership for the 21st Centuryby Edward F. Ansello and Thomas Rose.
This is a summary of an invitational conference held at the Wingspread Conference Center inRacine, Wisconsin in June, 1987. Discussion summaries provide overviews of the relevant issues facingthe states as they work toward integrating older Americans with developmental disabilities withinmainstream aging network programs (82pp). It contains a series of recommendations for action andsocial policy to aid in affecting integration. It is available from the University of Maryland's Center onAging (College Park, MD 20742-2611 or call 301 454-5856).
An Orientation Manual to the Older Americans Actby Susan Coombs Ficke.
This publication details the history and variou3 provisions of the Older Americans Act (asamended up to 1985). While not containing the provisions in the 1987 amendments, it is neverthelessand excellent compendium of easily retrievable information about the Act (122pp). It is available fromthe National Association of State Units on Aging (2033 K Street, N.W., Washington, DC 20006 or call202 785-0707).
Barriers and Strategies: Barriers to and Strategies for the Integration of Older Persons with Develop-mental Disabilities Within Aging Network Programs
Developed and issued by the New York State Office for the Aging, this 36 page monographoutlines the preliminary aspects of theState Office's Aging and Developmental Disabilities IntegrationFeasibility Demonstrazion Project, identifying the problems localities may encounter as they implementintegration projects of their own. The report outlines key actions at the state level and strategies to beemployed at the local level to implement integration activities. This report is available from the StateOffice for the Aging, (2 Empire State Plaza, Albany, NY 12223-0001 or call 518 486-2727).
55
Developing Adult Day Care: An Approach to Maintaining Independence for Impaired Older Personsby Helen Padula.
This publication offers helpful information on setting up and operating a social model adult daycare center (118pp). It is available from the National Council on the Aging, Inc., (600 MarylandAvenue, S.W., West Wing, Washington, DC 20024 or call 800 424-9046)
The Role of Adult Day Care in New York State's Long Tenn Care Service Continuumby the New York State Long Term Care Policy Coordinating Council.
This 66 page monograph is a report of the Long Term Care Policy Coordinating Council on thevarious issues related to adult day in New York. It is useful reading in order to understand the politicaland policy climate for expanding adult day care services in New York. Copies are available from theState Office for the Aging, Building Two, Empire State Plaza, Albany, NY 12223-0001.
Working with Developmentally Disabled Older Adults: A Training and Resource Manualby Margaret F. Sailer and Scott Jay Selkowitz.
A "how to" oriented manual on introducing and using a range of activities in programs specifi-cally designed for older adults with developmental disabilities (73pp). Available from the SoutheasternPennsylvania Rehabilitation Center (SEPRC) of Elwyn Institutes, (Baltimore Pike and Elwyn Road,Elwyn, PA 19063).
Age Pagesissued by the National Institute on Aging.
This booklet is a compilation of fact sheets, the Age Page, published by the National Institute onAging. These fact sheets offer practical advice on health promotion and related topics. Available fromthe National Institute on Aging (NIA) Information Center, (2209 Distribution Circle, Silver Spring,MD 20910 or call 301 495-3455).
Contemporary Issues in the Aging of Persons with Mental Retardation and Other DevelopmentalDisabilities
by Matthew P. Janicki, Marsha Mailick Seltzer and Mary WyngaardenKrauss
This 43 page monograph contains material that is useful as background. Areas covered includedefinition concerns; estimates of size; and demographic, health and functional, and family/social supportcharacteristics. The monograph also contains an extensive bibliography. Available from National Reha-bilitation bformation Center, (8455 Colesville Rd., Suite 935, Silver Spring, MD 20910 or call 800346-2742).
.56

Videos
Aging... A Shared ExperienceThis 20 minute video, developed and distributed by the New York State Office of Mental
Retardation and Developmental Disabilities explores the twin themes of the effective community inte-gration and friendships among older persons who are developmental disabled. It is equally appropriatefor public education and staff training sessions. The videocassette (VHS format) is available from theBureau of Aging Services, NYS OMRDD, 44 Holland Avenue, Albany, NY 12229-0001 (518 473-7855).
When People with Developmental Disabilities AgeThis 18 minute video, produced by the Hunter Brookdale Center on Aging with funding from
the New York State Developmental Disabilities Planning Council, examines similarities and differencesamong older persons with developmental disabilities. It examines vision, hearing, mobility, stamina, andother physical aging areas and looks at the interaction of aging and Down syndrome and Alzheimer'sdisease. The video brings together information from experts in medicine, gerontology and developmen-tal disabilites and program managers, and is useful for staff/caregiver training on the aging of olderpersons with developmental disabilities. Available from: Director of Educational Services, Hunter-Brookdale Center on Aging, 425 East 25 Street, New York, NY 10010 (212 481-4350).
Reports on Aging and Developmental Disabilities
New Directions for Seniors: Senior Day Program DemonstrationsDeveloped and issued by the New York State Office of Mental Retardation and Developmental
Disabilities, this 20 pp report is available from the Bureau of Aging Services, NYS OMRDD, 44 HollandAvenue, Albany, NY 12229-0001 (518 473-7855).
Program Resources Directory for Older Persons with Developmental Disabilities, 1989Developed and issued by the New York State Office of Mental Retardation and Developmental
Disabilities, this 315 page report is available from the Bureau of Aging Services, NYS OMRDD, 44Holland Avenue, Albany, NY 12229-0001 (518 473-7855).
Report of the Committee on Aging and Developmental DisabilitiesDeveloped and issued by the New York State Office of Mental Retardation and Developmental
Disabilities, this 85 page report is available from the Bureau of Aging Services, NYS OMRDD, 44Holland Avenue, Albany, NY 12229-0001 (518 473-7855).
The Newest Minority: The Aging MR/DD Population in Oneida CountyDeveloped and issued by the Oneida County MR/DD Task Force, this 30 page report is available
frxn the Institute of Gerontology, Utica College, Burrstone Road, Utica, NY 13502 (315 792-3129)
57
f3 5

Basic Rights of Older Persons WithDevelopmental Disabilities
Dr. Paul Cotten, a leader in the area of work with older persons with developmental disabilities,has proposed in the book, Aging and Rehabilitation: Advance.s in the State of the An (Springer, 1985), thatStates consider the following Bill of Rights:
The right to an adequate standard of living, economic security, and protective work.
The right to humane services designed to help one reach his or her fullest potential.
The right to live as independently as one is capable and reside in the community of one'schoice, in as normal a manner as is possible.
The right to an array of services that is generally available to other older persons.
The right to retire "to something" rather than "from something."
The right to participate as a member of the community, having reciprocal interdependency.
The right to be considered a person and not merely "elderly" or "retarded."
The right to protected well-being, and to a qualified guardian, when required.
The right to be involved in setting one's own goals and making one's own decisions; and theright to fail if necessary.
The right to a positive future, having enough involvement with life to prevent a preoccupationwith death.
The right to be romantic, not asexual.
The right to sufficient activity and attention to permit continued integrity of self, individualidentity, and purpose.
The right to an interesting environment and lifestyle, with availability of sufficient mobility toprovide a variety of surroundings.
The right to live and die with dignity.
58
f3 6

Some Basic Assumptions
The New York State constitution affords all elderly people an equal oppommity to participate inthe activities in which they chose to be involved. A person with a disability has the right to decidewhether he or she wants to participate in any program. The choice should always be left to the individ-ual. But if the person is not given a chance, never knows about the choice, then that individual has noreal choice.
The elderly person with a developmental disability has a right to be integrated. Any form ofsegregation tends to harm both those who are segregated and those who segregate them. The lives ofboth groups are richer if everyone is free to participate in the programs that interest him or her and isnot barred from them because of such factors as physical or mental handicaps.
The elderly person with a developmental disability has the right to participate in programs forthe aging. The lack of such an opportunity can mean there is no opportunity to participate in social orrecreational programs at all.
Each individual should be accorded full legal and human rights without regard to age or disabil-ity. Each individual has a right to receive services in the least restrictive environment, and in a way thatrecognizes that individual's ability to benefit from participation. The services should be provided in amanner that is flexible, accessible, and appropriate, and that promotes the dignity of the individual.
59
6 7

Memorandum of Understanding Betweenthe Administration on Aging
and the Administrationon Developmental Disabilities
IntroductionThe Administration on Aging (AoA) was created under the Older Americans Act of 1965 and is the only
Federal agency devoted exclusively to the concerns and potential of America's older population. AoA servicesas the visible advocate on behalf of the elderly within the Department of Health and Human Services and otherFederal agencies and national organizations administering programs affecting older people. The major goal ofthe Administration on Aging is to help ulder people live more meaningful, independent, and dignified lives intheir own homes and communities for as long as possible.
The Administration on Developmental Disabilities (ADD) is the lead agency within the Department ofHealth and Human Services responsible for planning and carrying out programs which promote the self-suffi-ciency and protect the rights of the nearly four million Americans with developmental disabilities. The majorgoal of the Administration on Developmental Disabilities is to work in partnership with State governments, localcommunities and the private sector to increase the social and economic integration of individuals with develop-mental disabilities into the fabric of society.
The purpose of this agreement is to improve the coordination of programs administered by the Admini-stration on Aging and the Administration on Developmental Disabilities which relate to the welfare of olderpersons with developmental disabilities.
BackgroundIt is estimated that two out of every 1,000 older adults have a devekpmental disability. The total number
of elderly persons in the United States who are developmentally disabled is estimated to be as high as one-halfmillion persons. These older persons are in double jeopardy. Their problems are complicated by long-standingphysical or mental impairments and they frequently need individualized housing, day-care, and other supportiveservices. Assistance, through the provision of appropriate services, to this priority older population can be madeavailable and accessible within the community through a comprehensive, coordinated, community-based servicesystem. This system of services should be designed to enable older persons with developmental disabilities toattain and maintain emotional well being and independent living.
The Older Americans Act now contains many requirements for services to elderly disabled people andcooperation with agencies and organizations regarding the developmentally disabled. For example, the Actrequires the State Agency on Aging to establish and operate an Office of the State Long Term Care Ombuds-man. This Office is required to coordinate ombudsman services with the protection and advocacy systems for in-dividuals with developmental disabilities and mental illness established under Part A of the DevelopmentalDisabilities Assistance and Bill of Rights Act and under the Protection and Advocacy for Mentally Ill Individu-als Act of 1986.
With respect to the needs of elderly persons with severe disabilities, the Act requires State plan assurancesfor the coordination of planning, identification, assessment of needs, and services with State agencies primarilyresponsible for disabled, including severely disabled, persons. The State plan must also contain an assurance thatthe State will work with these agencies to develop collaborative programs to meet the needs of older individualswith disabilities.
There is a need for the Administration on Aging and the Administration on Developmental Disabilitiesto undertake the development of collaborative activities to improve the coordination of programs administeredby the Administration on Aging arid the Administration on Developmental Disabilities which promote the inde-pendence and well-being of older persons with developmental disabilities.
Scope of the AgreementThe immediate objective of this agreement is for the Administration on Aging and the Administiation on
Developmental Disabilities to discuss, and develop action plans for, joint initiatives which improve the coordina-
60
GS

tion of the Administration on Aging and the Administration on Developmental Disabilities programs andactivities in order to improve services to older persons with developmental disabilities, promote the integration ofthese individuals into the mainstream of society, and promote a better understanding of programs serving elderlyand disabled persons between the National Network on Aging and the Developmental Disabilities Network.
Under this agreement, the Administration on Aging and the Administration on Developmental Disabili-ties agree to jointly develop and implement initiatives in support of the goals and objectives outlined below andto undertake the development of other collaborative activities which promote the independence and well-beingof older persons with developmental disabilities.
Goal 1Promote a better understanding of programs serving elderly and disabled persons between the National
Network on Aging and the Developmental Disabilities Network.
Objectives1.To increase best practice and other information sharing/exchange between the Network on Aging andDevelopmental Disabilities Network.2.To stimulate linkages between the Ombudsman and Protection and Advocacy Programs.3.To explore potential linkages between the Aging Resource Centers and University Affiliated Pro-grams.4.To encourage the development of memoranda of understanding between the State DevelopmentalDisabilities Councils and State.Agencies on Aging.
Goal 11To demonstrate a commitment at the national level between the Administration on Aging and the
Administration for Developmental Disabilities regarding serving older persons with developmental disabilities.
Objectivesi.To provide policy guidance to National Network on Aging and the Developmental DisabilitiesNetwork on serving older persons with developmental disabilities.2.To promote training of Network on Aging and Developmental Disabilities staff and others regardiNthe abilities and unmet needs of older persons who are developmentally disabled.3.To increase collaboration and linkages between national organizations and Federal, State, and localaget.cies sming the older persons who are developmentally disabled.4.To jointly develop a priority area on elderly persons with developmental disabilities for the discretion-ary funds announcements.
Goal 111Improve services to older persons with developmental disabilities.
Objectives1.To identify the unmet needs of older persons with developmental disabilities.2.To facilitate the provision of quality services in intermediate care facilities whr .neet the needs ofolder persons who are mentally retarded.3.To promote training of health care professionals to provide services to older persons with developmen-tal disabilities.4.To promote naining of family caregivers on how to care for older persons with developmental disabili-
ties.5.To promote the successful integration of older persons with developmental disabilities in agingnetwork programs (mainstreaming those elderly persons whc are developmentally disabled as partici-pants and volunteers at senior centers and nutrition sites).
61

Administration of Memorandum of UnderstandingThe Administration on Aging and Administration on Developmental Disabilities jointly agree to:
1.Designate staff to be responsible for administering all aspects of this agreement; and2.Designate staff of Administration on Aging and the Administation on Developmental Disabilities tomeet regularly to review the progress of the joint agreement and to identify new joint initiatives.
Period of AgreementThis agreement is effective upon signature and shall continue in effect until terminated by either party.
AuthorityThe Economy Act of 1932, as amended (31 U.S.C. 1535)
Modification or Cancellation ProvisionThis agreement may be modified or amended by written agreement of both parties. Requires for modifica-
tion and amendments to the agreement may be initiated by either party through written notification to eitherparty.
CostsTo be determined upon the completion of specific action plans for dissemination activities and/or research
and demonstration projects.
Acceptance and Signature of Each Approving Party
Joyce T. Berry, Ph.D.Acting Commissioner on AgingAdministration on AgingU. S. Department of Healthand Human Services
Will WolsteinActing CommissionerAdministration on DevelopmentalDisabilitiesU. S. Department of Healthand Human Services
Date Date
62

Memorandum of UnderstandingRelative to Older New Yorkers with a Developmental Disability
Between the New York State Office for the Aging andthe New York State Office of Mental Retardation and Developmental Disabilities
This agreement, entered into by and between the New York State Office for the Aging (SOA) acting byand through the Director with Offices at 2 Empire State Plaza, Albany, New York, 12223-0001, and the NewYork State Office of Mental Retardation and Developmental Disabilities (OMRDD) acting by and through theCommissioner with offices at 44 Holland Avenue, Albany, New York, 12229,
WHEREAS OMRDD is the state agency responsible for providing residential and communii-y services forpersons with a developmental disability in New York State, and
WHEREAS SOA is the state agency responsible for implementing and stimulating programs and policiesboth through the aging network and other State agencies on behalf of all older New Yorkers,
WHEREAS Aging Network means agencies which receive monies administered by SOA,
WHEREAS the State and recent Federal Older Americans Act amendments recognize the increasingnumber of older persons with a developmental disability,
WHEREAS older New Yorkers with a developmental disability are eligible for aging network services,
WHEREAS both agencies agree that the integration of capable older New Yorkers with a developmentaldisability within aging network programs is feasible and warranted;
and, WHEREAS SOA and OMRDD believe a coordinated multi-agency approach can more effectivelymeet the needs of older New Yorkers with a developmental disability, SOA and OMRDD agree:
to establish and maintain an interagency services coordin?tion committee to address issues of commonconcern, coordinate planning and services, and resolve problems;
to encourage local coordination of planning, needs identification, and development of services betweenarea agencies on aging and OMRDD district offices and/or its constituent provider agencies;
to establish mechanisms for coordinating funding of services to older New Yorkers with a developmentaldisability includingersuring coverage of the additional costs stemming from provision of such services assupplemental staff at stance, transportation, or other activities within aging network services;
to assist area agencies on aging and OMRDD district offices or its constituent agencies to developarrangements for reimbursement of additional costs of aging network services;
to establish mechanisms to cover services reporting and case record sharing requirements;
to assist each other by sharing technical information, training resources, and providing cross-training toagencies providing services to older New Yorkers with a developmental disabilit, wi:,in both networks;
to cooperate on common projects involving grant or other external funding tha be of benefit toolder New Yorkers with a developmental disability; and
to encourage New York's colleges and universities to address the issues of aging among New York's olderpopulation of persons with a developmental disability.
Therefore, each of the agencies participant to this agreement agree to the following:
63
7 1
The State Office for the Aging agrees, only to the extent resources are available, to:
request the state's area agencies on aging to enter into a planning process with the relevant OMRDDdistrict office on specific service projects, and such planning processes would include not only AAAsand OMRDD/DDSO's, but also older adults from the planning and service areas;
share technical resources, such as videos, films, and publications, free of charge, with OMRDD and itsdistrict offices;
provide technical assistance in relevant areas to OMRDD, its district offices and its constituent agencies;
engage in advocacy activities on behalf of older New Yorkers with a developmental disability;
facilitate the assimilation of disability agency senior programs into the local aging network;
enter into cooperative endeavors that would benefit older NewYorkers with a developmental disabilityand their families; and
request the states college and university based centers of aging or geriatric education centers to developintramural and extramural activities related to aging and developmental disabilities.
OMRDD agrees, only to the extent resources are available, to:
request the OMRDD district offices to enter into a planning process with the state's area agencies onaging on specific service projects;
share technical resources, such as videos, films, and publications, free of charge, with SOA and thestate's area agencies on aging;
provide technical assistance in relevant areas to SOA and the state's area agencies on aging;
engage in advocacy activities on behalf of okier New Yorkers with a developmental disability;
enter into cooperative endeavors that would benefit older New Yorkers with a developmental disabilityand their families; and
share information on available funding support to aging network programs specifically or individuallyserving older New Yorkers with a developmental disability;
agree to assume the additional costs of providing services within aging network programs for older NewYorkers with a developmental disability;
assume the responsibility of recordkeeping and reporting requirements, set by OMRDD, for older NewYorkers in aging network programs and services for whom such requirements apply; and
to cooperate in cross-training endeavors directed toward local programs.
This memorandum of understanding is effective on the 31st day of January, 1989 and shall be in effectuntil terminated by either agency.
by Jane G. GouldDirectorState Office for the Aging
by Elin M. HoweCommissioner, State Office of MentalRetardation & Developmental Disabilities
64 72
BEST COPY AVAILABLE

Memorandum of UnderstandingConcerning Older New Yorkers with a Developmental Disability
Among
The New York City Department for the Aging,
The New York City Health and Hospitals Corporation,
The New York City Human Resources Administration,
The New York City Department of Mental Health, Mental Retardation and Alcoholism Services
and
The New York City Regional Office and the five borough Developmental Disabilities ServicesOffices of the New York State Office of Mental Retardation and Developmental Disabilities
Whereas, the New York State Office of Mental Retardation and Ikvelopmental Disabilities (OMRDD)and the New York State Office for the Aging (SOFA) have entered into an agreement on January 31, 1990, and
Whereas, New York State, New York City and recent federal Older Americans Act amendments recog-nize the increasing number of older persons with a developmental disability; and
Whereas, agencies which receive monies administered by SOFA, and agencies which receive moniesadministered by the City of New York (aging network) provide services to older persons in New York City; and
Whereas, older New York City residents with developmental disabilities are eligible for aging networkservices; and
Whereas, the New York City Regional Office (NYCRO) and the five borough Developmental DisabilitiesServices Offices (DDS0s) are the New York City district offices of OMRDD, responsible for providing residentialand community services for persons with developmental disabilities in New York City; and
Whereas, the New York City Department for the Aging (DFTA) is the duly designated area agency onaging, responsible for planning and developing programs and policies, both through the aging network and otherstate and county agencies, on behalf of all older persons in New York City, and
Whereas, the New York City Human Resources Administration (HRA), Division of Community Care andCommunity Services (CCSS), provides services to older and impaired persons who are able to remain in thecommunity by better integrating health, social and protective services and helping persons live independently intheir own homes as long as possible; and
Whereas, the New York City Health and Hospitals Corporation (HHC) is the public benefit corporationthat encompasses eleven acute care hospitals, five long term care facilities and a network of community basedoutpatient services; and
Whereas, the New York Department of Mental Health, Mental Retardation and Alcoholism Services(NYC DMHMRAS) is responsible for providing direction, planning, funding and oversight for the provision ofmental health, mental retardation and alcoholism treatment and prevention services to the residents of new YorkCity; and
Whereas, DF1 A, HHC, HRA, NYCDMHMRAS, NYCRO and the five borough DDSOs of OMRDD(The Agencies) agree that integration of capable older persons with developmental diaabilities in New York Citywithin aging network programs is feasible and warranted; and
Whereas, the Agencies believe a coordinated multi-agency approach can more effectively meet the needsof older persons in New York City with developmental disabilities.
Now, Therefore, The Agencies agree, only to the extent that resources are available:
to establish an Interagency Committee for Services to Older Persons with Developmental Disabilities consistingof members appointed by the commissioners of each agency,, to address issues of common concern, coordinateplanning and setvices, and explore ways to enter into cooperative endeavors that would benefu older individualswith developmental disabilities and their families;
to encourage local coordination among The Agencies of planning, needs assessment, advocacy activities anddevelopment of services on behalf of older New York City individuals with developmental disabilities;
65
7 3

to establish mechanisms for coordinatlig funding of services to older persons with developmental disabilities ,such as supplemental staff assistance, transportation or other activities within aging network services;
to assist each other by sharing tedmict.:, funding and other information, training resources, and by providingtraining to agencies who serve older persons with developmental disabilities;
to cooperate on common projects involving grants or other external funding that would benefit older personswith developmental disabilities;
to encourage New York City's colleges and universities to address the issues affecting New York City' s popula-tion of older persons with developmental disabilities;
Nothing in this Memorandum of Understanding shall permit any party to determine the availability ofresources for any other party.
This Memorandum of Understanding is effective on , 1991 and shall be in effect until termi-nated by any party.
Prema Mathai-Dayis, Commissioner, New York *City Department for the Aging
James M. Walsh, Associate Commissioner, New York City Regional Office OMRDD
Billy E. Jones, M.D., Commissioner, New York City Department of Mental Health, Mental Retardation andAlcoholism Services
J. Emilio Carrillo, M.D., President, Health and Hospitals Corporation
Barbara Sabol, Commissioner, Hun= Resources Agency, , Health and Hospitals Corporation
66
MllOIMI1=M-,'
74