e & m coding- physician care manager documentation release...
TRANSCRIPT

E & M Coding- Physician Care Manager Documentation Release 6.05 pp7
Physician Care ManagerPhase II Setup
E&M Coding
Release 6.05Priority Pack 7
Copyright© by MEDICAL INFORMATION TECHNOLOGY, INC.MEDITECH Circle, Westwood, MA 02090
(781) 821-3000This information is proprietary and should be treated accordingly

E & M Coding- Physician Care Manager Documentation Release 6.05 pp7
Physician Documentation:E&M Coding Setup Guide
Table of Contents
Introduction…General Info & 1995 vs. 1997… 2
Dictionaries… 3Level of Care Dictionary… 4Link Code Category to Query… 5E&M Components by Template… 6Query Dictionary… 7Group Response Dictionary… 8Template Dictionary… 9EMR Toolbox Parameters… 10User Preferences… 11Bullet, Box, and Exam Dictionaries… 12Encounter Dictionary... 13Classifications Dictionary… 14
Functionality…Using E&M Coding… 15Code Visit Screen… 16Printing from PCM… 17Printing the Coding Report… 18

E&M Coding Introduction
The E&M Coding guidelines are standard guidelines created by the Healthcare Financing Administration (HCFA). They are used to calculate the appropriate charge for a patient's visit based on the level of care that a physician provided to that patient. Billing is determined based on a number of factors, including the body systems reviewed, the history obtained, and the examination provided. These areas are broken down into three categories: History, Exam, and Medical Decision Making. The level achieved in each of these categories combined will determine the overall Level of Care provided.
Charges are not automatically calculated according to what level of care the physician selects in Physician Documentation. A coder will still need to review the visit to determine the charge, but a printed copy of Physician Documentation's Coding Report can be used to help determine the charges. (Beginning with 5.6sr5, PD will be able to send billing information from PD to B/AR due to changes in DDP #7397.)
1995 Guidelines vs. 1997 Guidelines
MEDITECH can utilize the 1995 or 1997 E&M Coding Guidelines, depending on what your facility uses. The Exam section is the differentiating factor between the two. The level of Exam with the 1997 guidelines is determined based on very specific criteria. For this reason, the 1997 guidelines introduce the Bullet, Box, and Exam dictionaries to MEDITECH. These dictionaries are discussed in a subsequent section of this document.
The 1995 guidelines do not utilize the Bullet, Box, and Exam dictionaries for the Exam portion, but rather the Code Category dictionary. Both the 1995 and 1997 guidelines use Code Categories for the History portion.
Building Process
In order to utilize E&M Coding, your facility will need to attach queries and group responses to hardcoded Code Categories and Bullets. The Code Categories and Bullets are standard coding categories and will be delivered by MEDITECH. By linking Code Categories and Bullets to queries, Physician Documentation can recognize the level of care the physician has achieved and offer a "suggested" selection (in the History and Exam categories, but not in the Medical Decision Making category).
Queries may be linked in a few different ways, all of which will be covered over in this document (Link Code Category routine, Template Mass Edit, MIS Query dictionary and MIS Group Response dictionary).

E&M Coding DictionariesClinical>Dictionaries>Documents>E&M Coding
The E&M Coding dictionaries all may be accessed under the Documentation dictionary menu in the:

Level of Care Code Dictionary Clinical>Dictionaries>Documents>E&M Coding
The Level of Care dictionary is where setup is done for the “Level of Care” that a physician may choose when coding the visit. The definition of each level is created here (i.e. how much documenting needs to have been done in order to achieve this level).
Mnemonic: The five-digit numeric mnemonic defined according to the coding guidelines
Name: The name of the Level of Care as seen by the physician when coding the visit.
Extent of History: The level of documenting related to the patient’s history that the physician should achieve in order to reach this level of care. (The History, Exam, and Medical Decision Making categories come together to define the Level of Care.) The choices are Problem Focused, Expanded Problem Focused, Detailed, and Comprehensive.
Extent of Examination: The level of documenting related to the patient’s exam that the physician should achieve in order to reach this level of care. The choices are Problem Focused, Expanded Problem Focused, Detailed, and Comprehensive.
Extent of Medical Decision Making: The level of medical decision that the physician should use in order to reach this level of care. The choices are Straight Forward, Low Complexity, Moderate Complexity, and High Complexity.
Number of Required Components: How many of the above three categories (History, Exam, and Medical Decision Making) need to be reached in order to achieve this level of care.

Link Code Category to Query Clinical>Dictionaries>Documents>E&M Coding
Queries may be linked to code categories by using this routine.
The Code Categories listed on the top portion of this dictionary are hardcoded. In order to attach a query to one of the categories, highlight the desired category, click into the Queries portion of the screen and enter the query mnemonic that should be linked to this category.
Linking a code category to a query allows the system to automatically calculate a suggested level of care that a physician has achieved. The system will look to see how many queries with code categories have been answered.
If code categories are not attached to queries, then the system cannot calculate a suggested level of care for users.
Code categories are used specifically to calculate the history category (1995 and 1997) and the exam category (1995 only).

E&M Components by TemplateClinical>Dictionaries>Documents>E&M Coding
This dictionary allows for all of the components of a single template to be attached to code categories and bullets from one screen. Upon opening, this dictionary will prompt users to enter the Document Template mnemonic of the desired template.
The top section displays the Document Sections (in the Section box) that belong to the chosen template. When selecting any defined section, the Question Sets associated to that Section display, along with the associated Queries.
Users can click on any Question to open up the Query, allowing the user to attach one of the hardcoded Code Categories to each Query. This will bring up a lookup into the Code Category dictionary. In addition, users can also associate one of the hardcoded Bullets to the Query.
In order to attach Group Response Element Bullets. users can highlight a Group Response (if a group response is attached to the query), then click the lookup button (or F9) in the footer to associate the response to one of the hardcoded bullets. Bullets are used to calculate the Exam category when using the 1997 guidelines. If using the 1995 guidelines, bullets do not need to be setup.

Query Dictionary Clinical>Dictionaries>Documents
Code Categories and Bullets can also be attached to Queries directly from the Query Dictionary.
Code Category: Attach the applicable code category to the query here. Code categories are used to calculate the level of history (1995 and 1997 guidelines) and level of exam achieved (1995 only).
Bullets: Attach the applicable bullets to the query here. Bullets are used to calculate the level of exam (1997 guidelines only) achieved.

Group Response Dictionary Clinical>Dictionaries>Documents
Bullets may also be attached directly in the MIS Group Response dictionary.
Each group response element may have bullets attached to it. This can be accomplished by highlighting the desired Element Name and then selecting the Bullets section below. The Bullets section will do a lookup into the hardcoded Bullets dictionary.
Bullets are used to calculate the level of Exam provided when using the 1997 guidelines (the 1995 guidelines do not utilize bullets).

Document Template Dictionary Clinical>Dictionaries>Documents
Each template that should utilize E&M Coding needs to have the appropriate Levels of Care attached to it.
Coding Routine Header: This is a free-text field that is used to identify the header that should appear above the Levels of Care on the Code Visit screen in Physician Documentation. Multiple headers may be used to differentiate different coding guidelines (i.e. New Patient vs. Established Patient).
Levels of Care: This is where the Levels of Care (built in the Levels of Care Code dictionary) are attached to templates. These Levels of Care will appear on the Code Visit screen in Physician Documentation as options that may be selected by the end-users.

EMR Toolbox Parameters Clinical>Dictionaries>EMR – view only
E&M Guidelines Parameter: This prompt enables E&M Coding and determines what guidelines your facility uses. The choices are 1995, 1997, or Both. If Both is selected, then the system will automatically use the guideline (1995 or 1997) that calculates the highest level of care. These settings can be set different for each defined Facility, as well as for each user (explained below).

User Preferences Clinical>Dictionaries>EMR
E&M Code Guidelines: This field determines the E&M Coding Guidelines that are used by individual users. The global settings done in the EMR Toolbox Parameters are the default; the setting entered here will override the setting for the selected user.
The choices are 1995, 1997, or Both. If Both is selected, then the system will automatically use the guideline (1995 or 1997) that calculates the highest level of care.

Bullet, Box, and Exam DictionariesClinical>Dictionaries>Documents>E&M Coding
The Bullet, Box, and Exam dictionaries are dictionaries that contain hardcoded entries used for the Exam portion of the 1997 coding guidelines.
These dictionaries do not need to be built, as they already contain the hardcoded entries. Bullets are attached to queries and group responses in the methods discussed earlier in this document (the E&M Components by Template, Query, and Group Response dictionaries).
Why these dictionaries are used:
The 1997 guidelines have standard exam guidelines and each exam consists of system/body areas in boxes. An exam will meet a certain level based on the number of bullets documented within a box. In addition, certain boxes are “shaded.” This is significant for a comprehensive level of exam and is all calculated in the background.
The 1995 guidelines do not utilize these dictionaries.

Encounters Type DictionaryClinical>Dictionaries>Documents>E&M Coding
When users select the Code Visit button from the main Physician Documentation screen, they can choose to code the visit. The system will then prompt users to choose an Encounter type. The selected encounter type will affect what levels of care are available to be chosen.
Name: This is the name of the encounter, which users will be able to select.
Level of Care Codes: These are the levels of care that are presented to the user after the “encounter” is chosen.

ICD Diagnosis Classifications Dictionary Info Systems>MIS>Dictionaries>Coding
Users can choose a Primary Diagnosis (and Additional Diagnoses) and Procedure(s) to be included with the coding. The Classifications dictionary allows the diagnoses and procedures to be sub-categorized.
Name: Enter a name descriptive of the entry. This name can appear in Lookups and on reports to further define this dictionary entry.
Subclasses: Enter the ICD subclasses of this ICS classification..
Groupings: Enter the groups of ICD codes you want include in this ICD classification.After you enter the group names, enter the range of codes included in those groups at the From and To fields. This looks to the ICD Diagnosis Dictionary..
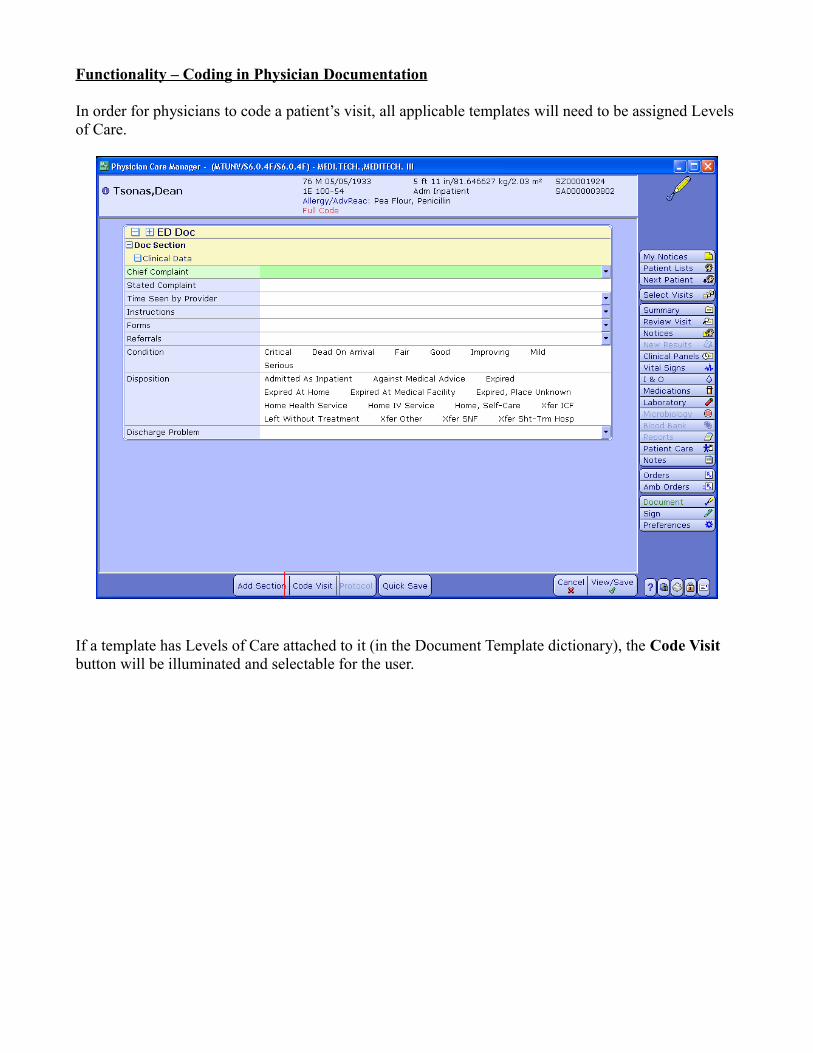
Functionality – Coding in Physician Documentation
In order for physicians to code a patient’s visit, all applicable templates will need to be assigned Levels of Care.
If a template has Levels of Care attached to it (in the Document Template dictionary), the Code Visit button will be illuminated and selectable for the user.

Code Visit Screen
If the physician has answered queries that are linked to code categories and bullets, then they may receive a suggested level of History and Exam. Suggested selections become colored in a green font. Users may choose against the “suggested” level and the Coding Report will keep track of the “suggested” selections and actual selections.
To see a definition of how much is required in the History, Exam and Medical Decision Making sections to reach a certain level, users may click on the header of each. A pop-up window will explain what each level's's (i.e. “Problem Focused”) definition is. Please note that the system cannot suggest a recommended level for Medical Decision Making; that must be manually selected by the user.
The user may choose a Level of Care at the top and it will indicate what is required in the History, Exam and Medical Decision Making sections with asterisks. If the user has not chosen the recommended choice for any portion, the font will become colored in red. Comments may be added at the bottom to explain choices.
Users may associate Diagnoses, Procedures, and Time Spent with Patient.

Printing the Coding Report
Reports may be printed directly from Physician Documentation or from the PCM database.
Once a user has documented a visit with E&M Coding, the Visit Report button may be used from the footer of the Document screen to print the report.
Documented Codes can be reported by a Document Date range.

Printing the Coding Report
Printing from the database may be done from the E&M Coding – Code Report menu options found under Reports.
Reports may be selected for printing by looking up the information by patient name, document date, and registration date.
When printing, users have the choice of including the Query Details (details of what responses the user chose that resulted in their level of cares) and Event Details (details of the selections, including recommended versus selected) or not.