duelo de insulinas superbasales: tresiba vs toujeo
TRANSCRIPT

UG
C E
ND
OC
RIN
OLO
GÍA
Y
N
UT
RIC
IÓ
N
HO
SP
IT
AL
V
IR
GE
N M
AC
AR
EN
A. S
EV
IL
LA
DTRA UGC: DRA MARTINEZ BROCA
FEAS: DRA RABAT, DR.MARTIN , DRA.CUESTA, DRA GONZALEZ,DRA
HERNANDEZ, DR TORRES, DRA.SERRANO, DRA CAMPOS, DR.MORALES,
DRA GARCIA, DRA OLIVA, DRA TOUS, DR. JIMENEZ, DRA MENDEZ
ENFERMERIA: MAR CASADO, CARMEN POLVILLO, PEPA MUÑIZ, SAFA
ALMUSTANI, ANA Mª MORALES, JOSEFA BARRIOS , Mª DOLORES GARCIA
INVESTIGACION: IRENE CABALLERO,ALICIA JUSTEL ,MARIA ESLAVA,
MARISA MOYA, MARIA LUISA GARCIA, MARIA JOSE POLVILLO, MARIA
DUQUE, CARLOS GARCIA, PILAR ALARCON, MARIA CORONEL, JOSE
MANUEL CARRETERO.SILVIA SALAZAR MIR: LUNA FLORENCIO, MARIA
SEVILLANO, ROCIO DOMINGUEZ, REYES RAVE
@EndoMAC
11 AÑOS CUIDANDO, FORMANDO E INNOVANDO EN DIABETES
HDDHOSPITAL DE DIA DE DIABETES
HOSPITAL VIRGEN MACARENA. SEVILLA
AÑOS
@C
ris
tob
_M
ora
les

¿EXISTEN DIFERENCIAS ENTRE LAS SUPERBASALES?


NP
H
@cristob_morales
BA
SA
LES
1
.0

DUELO DE SUPERBASALES @
cris
tob
_m
orale
s

LA INSULINA DEL SXXI
SUPERBASALES
Evidencia
Ensayos clínicos
Experiencia
Vida Real
Preferencia
Voz del paciente
@cristob_morales
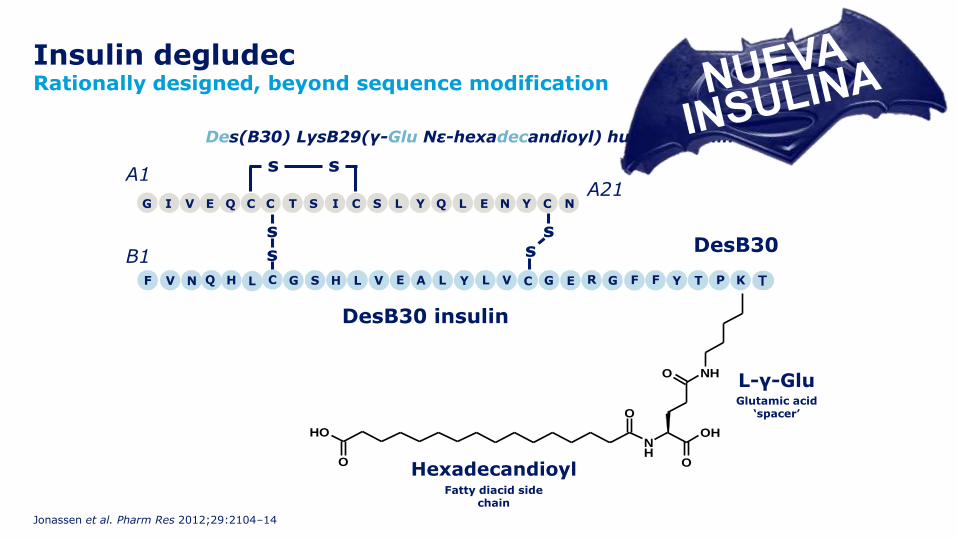
Insulin degludecRationally designed, beyond sequence modification
Jonassen et al. Pharm Res 2012;29:2104–14
NH
O
OH
O NH
O
OH
O
DesB30 insulin
DesB30
T
Des(B30) LysB29(γ-Glu Nε-hexadecandioyl) human insulin
s
ss
s
A1
B1
A21
s s
T YG EE CYCC NLQLSISQVI NC
PTYY FFF GGG REE CC VLLAVLHSLHQNV K
L-γ-GluGlutamic acid
‘spacer’
NH
O
OH
O NH
O
HexadecandioylFatty diacid side
chain
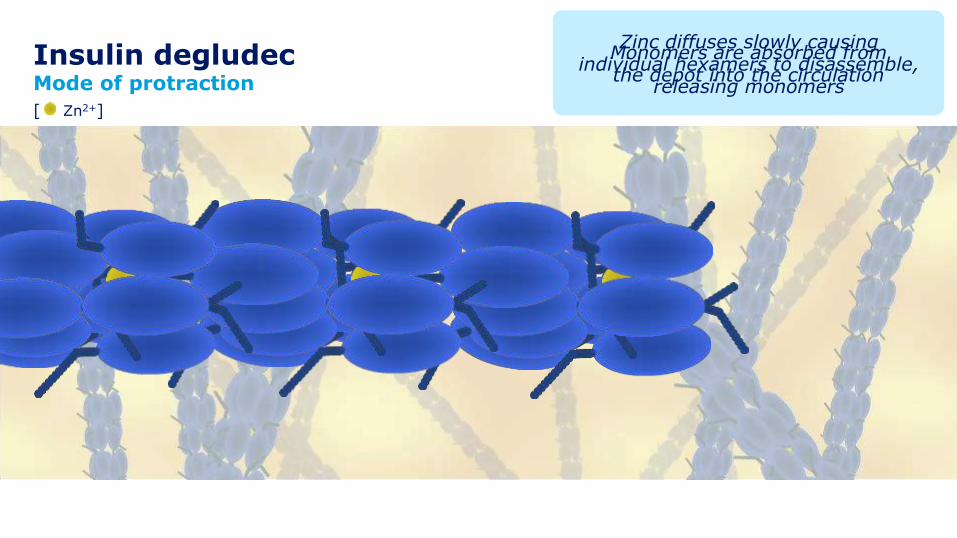
Insulin degludecMode of protraction
Jonassen et al. Pharm Res 2012;29:2104–14
Monomers are absorbed from the depot into the circulation
Zinc diffuses slowly causing individual hexamers to disassemble,
releasing monomers
[ Zn2+]
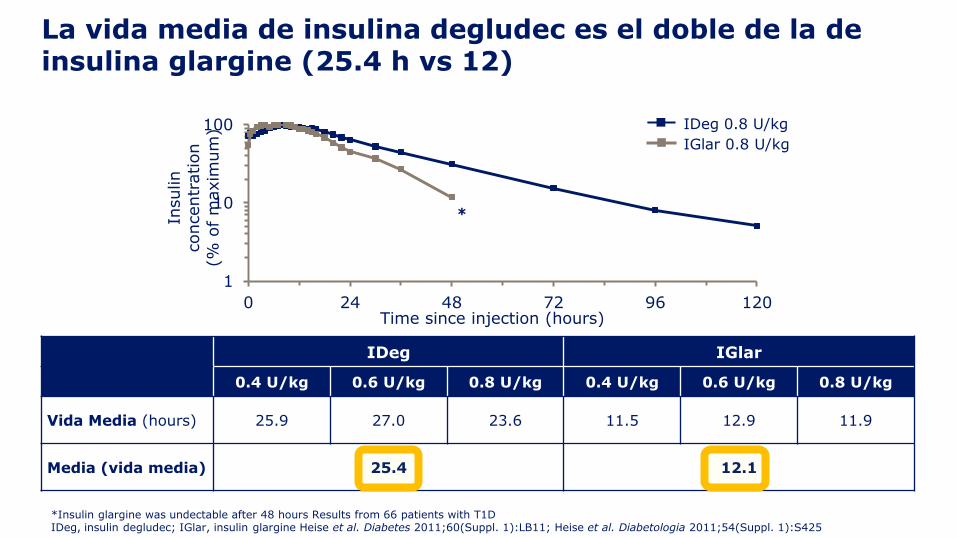
La vida media de insulina degludec es el doble de la de insulina glargine (25.4 h vs 12)
1
10
100
0 24 48 72 96 120
Insulin
concentr
ation
(% o
f m
axim
um
)
Time since injection (hours)
*
IDeg 0.8 U/kg
IGlar 0.8 U/kg
*Insulin glargine was undectable after 48 hours Results from 66 patients with T1DIDeg, insulin degludec; IGlar, insulin glargine Heise et al. Diabetes 2011;60(Suppl. 1):LB11; Heise et al. Diabetologia 2011;54(Suppl. 1):S425
IDeg IGlar
0.4 U/kg 0.6 U/kg 0.8 U/kg 0.4 U/kg 0.6 U/kg 0.8 U/kg
Vida Media (hours) 25.9 27.0 23.6 11.5 12.9 11.9
Media (vida media) 25.4 12.1
0 2 4 6 8 10 12 14 16 18 20 22 24
Time (hours)
0
1
2
3
4
5
6
GIR
(m
g/k
g/m
in)
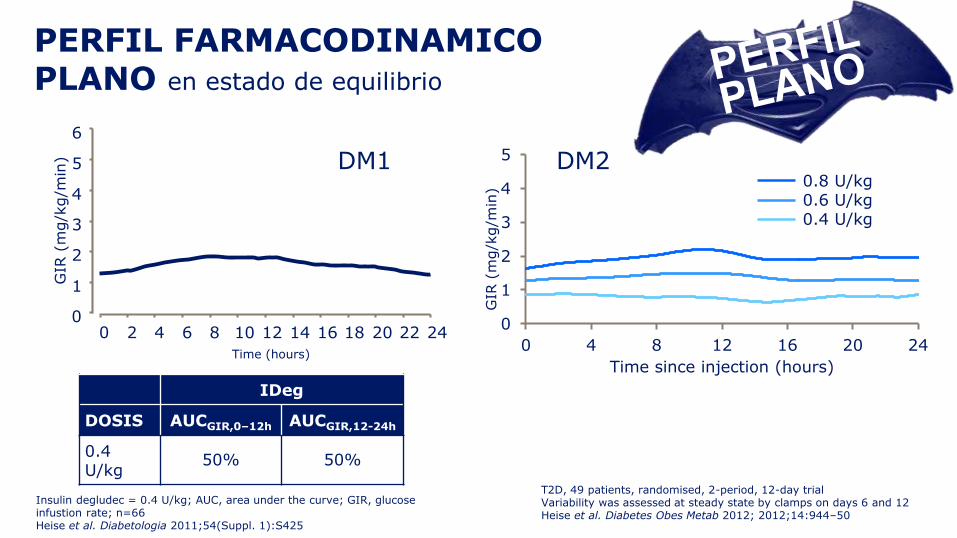
PERFIL FARMACODINAMICO PLANO en estado de equilibrio
IDeg
DOSIS AUCGIR,0–12h AUCGIR,12-24h
0.4 U/kg
50% 50%
Insulin degludec = 0.4 U/kg; AUC, area under the curve; GIR, glucose infustion rate; n=66Heise et al. Diabetologia 2011;54(Suppl. 1):S425
0
1
2
3
4
5
0 4 8 12 16 20 24
GIR
(m
g/k
g/m
in)
Time since injection (hours)
0.8 U/kg0.6 U/kg0.4 U/kg
T2D, 49 patients, randomised, 2-period, 12-day trialVariability was assessed at steady state by clamps on days 6 and 12Heise et al. Diabetes Obes Metab 2012; 2012;14:944–50
DM1 DM2
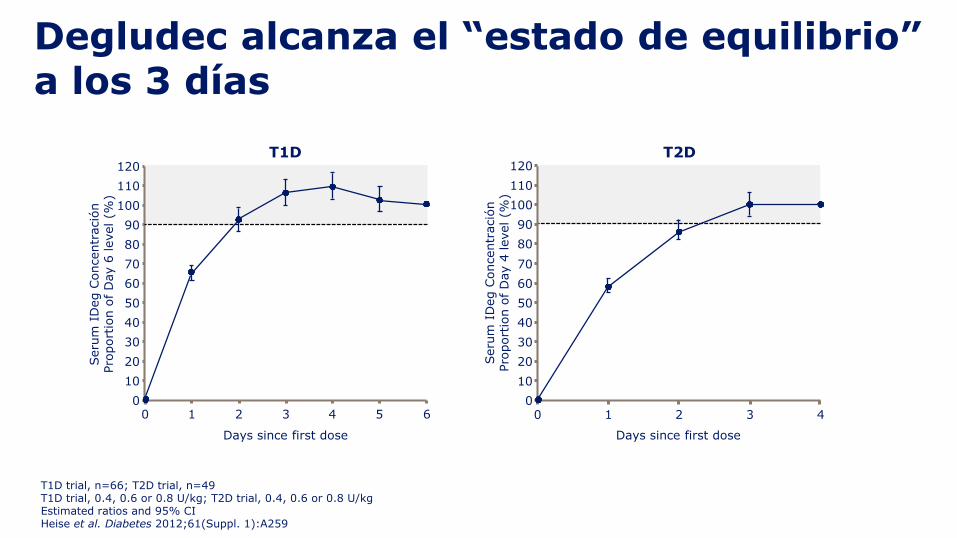
Degludec alcanza el “estado de equilibrio” a los 3 días
54320 1 6
Days since first dose
Seru
m I
Deg C
oncentr
ació
nPro
port
ion o
f D
ay 6
level (%
)
120
110
100
90
80
70
60
50
40
30
20
10
0
T2D
0 1 2 3 4
Seru
m I
Deg C
oncentr
ació
nPro
port
ion o
f D
ay 4
level (%
)
120
110
100
90
80
70
60
50
40
30
20
10
0
Days since first dose
T1D
T1D trial, n=66; T2D trial, n=49T1D trial, 0.4, 0.6 or 0.8 U/kg; T2D trial, 0.4, 0.6 or 0.8 U/kgEstimated ratios and 95% CIHeise et al. Diabetes 2012;61(Suppl. 1):A259
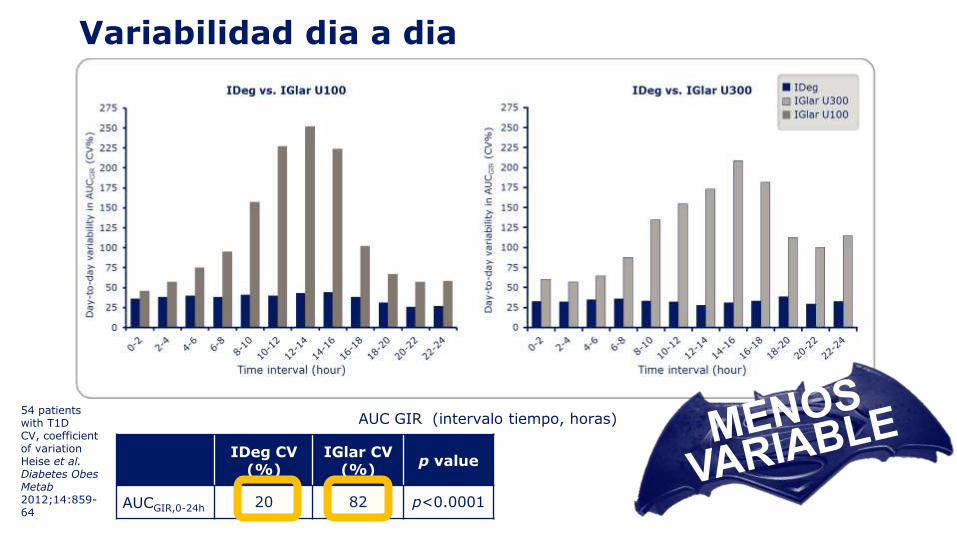
Variabilidad dia a dia
AUC GIR (intervalo tiempo, horas)
IDeg CV (%)
IGlar CV (%)
p value
AUCGIR,0-24h 20 82 p<0.0001
54 patients with T1DCV, coefficient of variationHeise et al. Diabetes ObesMetab2012;14:859-64
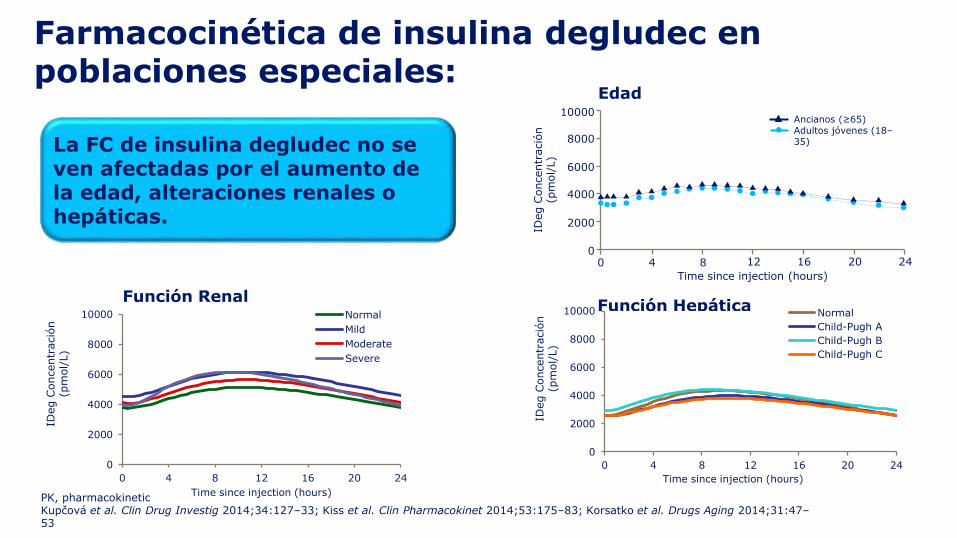
Farmacocinética de insulina degludec en poblaciones especiales:
Edad
Función HepáticaFunción Renal
Ancianos (≥65)Adultos jóvenes (18–35)La FC de insulina degludec no se
ven afectadas por el aumento de la edad, alteraciones renales o hepáticas.
0
2000
4000
6000
8000
10000
0 4 8 12 16 20 24
IDeg C
oncentr
ació
n(p
mol/
L)
Time since injection (hours)
Normal
Mild
Moderate
Severe
0
2000
4000
6000
8000
10000
0 4 8 12 16 20 24
IDeg C
oncentr
ació
n(p
mol/
L)
Time since injection (hours)
Normal
Child-Pugh A
Child-Pugh B
Child-Pugh C
0 4 8 12 16 20 24
Time since injection (hours)
2000
4000
6000
8000
10000
IDeg C
oncentr
ació
n
(pm
ol/
L)
0
PK, pharmacokineticKupčová et al. Clin Drug Investig 2014;34:127–33; Kiss et al. Clin Pharmacokinet 2014;53:175–83; Korsatko et al. Drugs Aging 2014;31:47–53
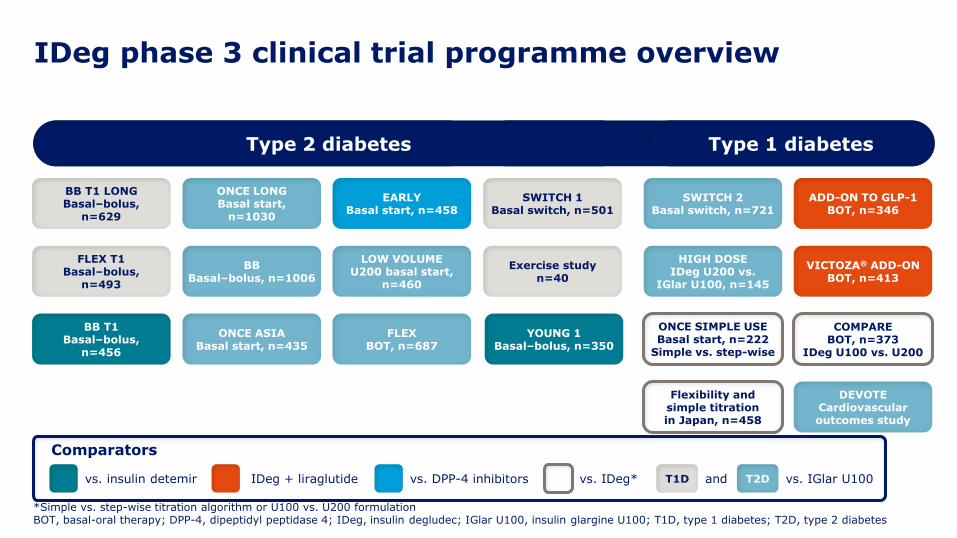
IDeg phase 3 clinical trial programme overview
*Simple vs. step-wise titration algorithm or U100 vs. U200 formulationBOT, basal-oral therapy; DPP-4, dipeptidyl peptidase 4; IDeg, insulin degludec; IGlar U100, insulin glargine U100; T1D, type 1 diabetes; T2D, type 2 diabetes
Phase 3a Phase 3b
BBBasal–bolus, n=1006
ONCE LONGBasal start,
n=1030
BB T1 LONGBasal–bolus,
n=629
FLEX T1Basal–bolus,
n=493
EARLYBasal start, n=458
LOW VOLUMEU200 basal start,
n=460
ONCE ASIABasal start, n=435
FLEXBOT, n=687
BB T1Basal–bolus,
n=456
vs. insulin detemir vs. DPP-4 inhibitors andT1D vs. IGlar U100T2D
SWITCH 1Basal switch, n=501
Exercise studyn=40
YOUNG 1Basal–bolus, n=350
ONCE SIMPLE USEBasal start, n=222
Simple vs. step-wise
Flexibility and simple titration in Japan, n=458
SWITCH 2Basal switch, n=721
HIGH DOSEIDeg U200 vs.
IGlar U100, n=145
VICTOZA® ADD-ONBOT, n=413
COMPAREBOT, n=373
IDeg U100 vs. U200
DEVOTECardiovascular outcomes study
ADD-ON TO GLP-1BOT, n=346
IDeg + liraglutide
Comparators
Type 1 diabetesType 2 diabetes
vs. IDeg*

9225 PACIENTES
7637 PACIENTES
16.862
PACIENTES
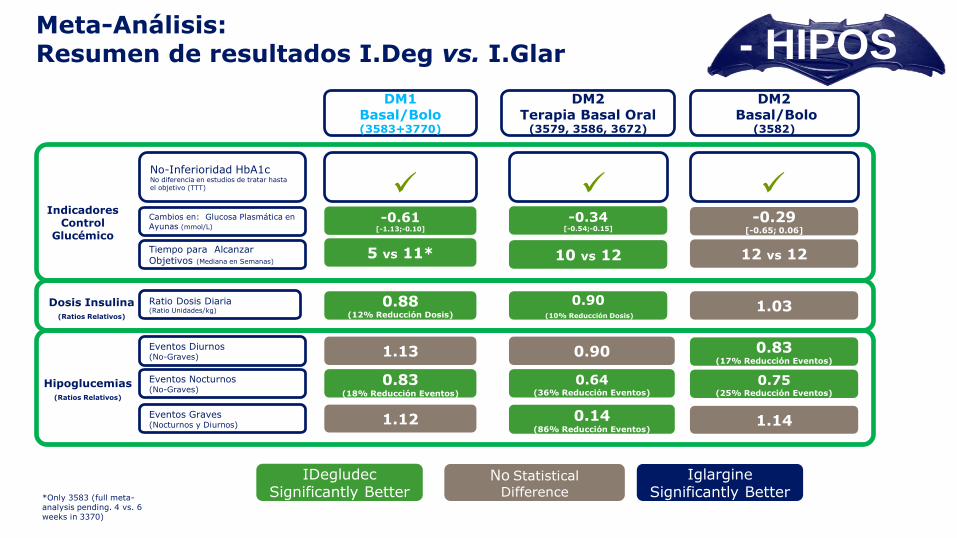
DM1 Basal/Bolo (3583+3770)
1.13
0.83(18% Reducción Eventos)
1.12
DM2Terapia Basal Oral
(3579, 3586, 3672)
DM2 Basal/Bolo
(3582)
0.90
0.64(36% Reducción Eventos)
0.14(86% Reducción Eventos)
0.83 (17% Reducción Eventos)
0.75(25% Reducción Eventos)
1.14
Eventos Nocturnos(No-Graves)
Eventos Diurnos(No-Graves)
Eventos Graves(Nocturnos y Diurnos)
-0.61 [-1.13;-0.10]
-0.34 [-0.54;-0.15]
-0.29 [-0.65; 0.06]
Cambios en: Glucosa Plasmática en Ayunas (mmol/L)
No-Inferioridad HbA1c No diferencia en estudios de tratar hasta el objetivo (TTT)
5 vs 11* 10 vs 12 12 vs 12Tiempo para Alcanzar Objetivos (Mediana en Semanas)
Indicadores Control
Glucémico
Hipoglucemias (Ratios Relativos)
0.88 (12% Reducción Dosis)
0.90(10% Reducción Dosis)
1.03 Ratio Dosis Diaria (Ratio Unidades/kg)
Dosis Insulina(Ratios Relativos)
*Only 3583 (full meta-analysis pending. 4 vs. 6 weeks in 3370)
IDegludec Significantly Better
Iglargine Significantly Better
No Statistical
Difference
Meta-Análisis: Resumen de resultados I.Deg vs. I.Glar - HIPOS
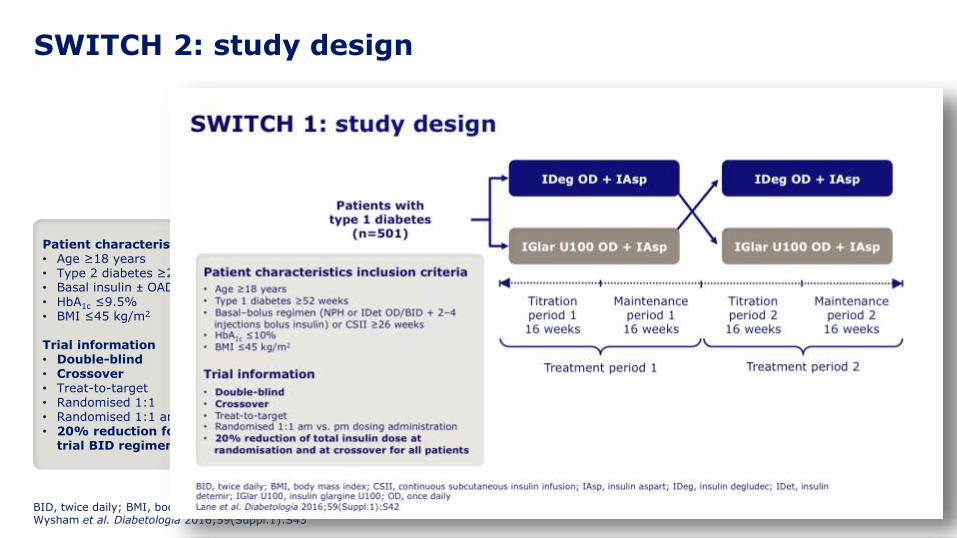
SWITCH 2: study design
BID, twice daily; BMI, body mass index; IDeg, insulin degludec; IGlar U100, insulin glargine U100; OAD, oral antidiabetic drug; OD, once dailyWysham et al. Diabetologia 2016;59(Suppl.1):S43
Maintenanceperiod 2 16 weeks
Maintenance period 116 weeks
Titration period 1 16 weeks
Titration period 2 16 weeks
Treatment period 1 Treatment period 2
IDeg OD ± OADs
IGlar U100 OD ± OADs
Patients withtype 2 diabetes
(n=721)
IDeg OD ± OADs
IGlar U100 OD ± OADs
Patient characteristics inclusion criteria• Age ≥18 years• Type 2 diabetes ≥26 weeks• Basal insulin ± OADs ≥26 weeks• HbA1c ≤9.5%• BMI ≤45 kg/m2
Trial information• Double-blind• Crossover• Treat-to-target• Randomised 1:1• Randomised 1:1 am vs. pm dosing administration• 20% reduction for total insulin dose for pre-
trial BID regimen

SWITCH 2: hypoglycaemia risk – inclusion criteria
eGFR, estimated glomerular filtration rateWysham et al. Diabetologia 2016;59(Suppl.1):S43
Total
n %
Number of patients 720 100.0
Patients with increased risk of developing severe hypoglycaemia with at least one a, b, c or d criterion:
546 75.8
a. Experienced ≥1 severe hypoglycaemic episode within the last year 118 16.4
b. Moderate chronic renal failure (eGFR 30–59 mL/min/1.73m2) 159 22.1
c. Hypoglycaemic symptoms unawareness 129 17.9
d. Exposed to insulin for ≥5 years 356 49.4
e. Recent hypoglycaemia episode within the last 12 weeks 478 66.4
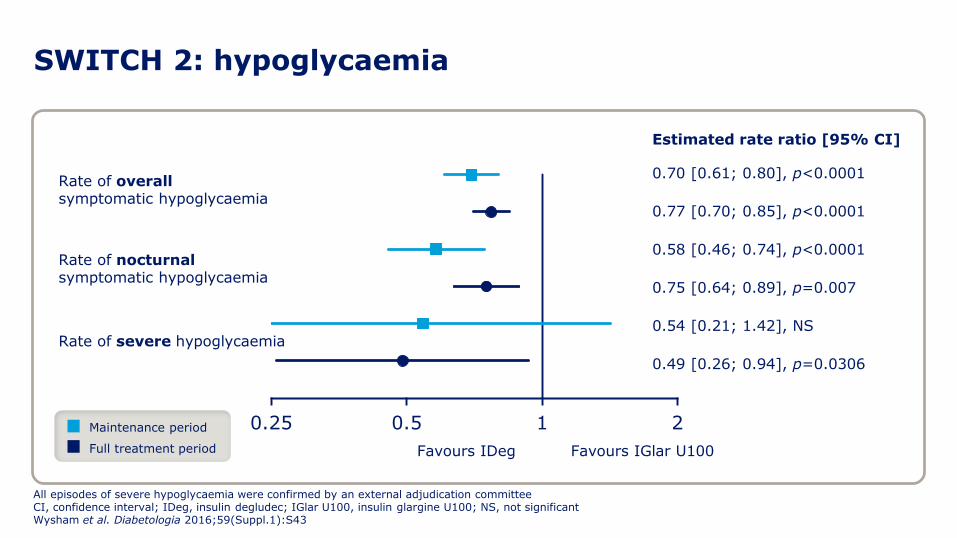
SWITCH 2: hypoglycaemia
All episodes of severe hypoglycaemia were confirmed by an external adjudication committeeCI, confidence interval; IDeg, insulin degludec; IGlar U100, insulin glargine U100; NS, not significantWysham et al. Diabetologia 2016;59(Suppl.1):S43
0.25 0.5 1 2
0.77 [0.70; 0.85], p<0.0001
0.49 [0.26; 0.94], p=0.0306
Estimated rate ratio [95% CI]
Rate of overallsymptomatic hypoglycaemia
Rate of severe hypoglycaemia
Favours IGlar U100Favours IDeg
0.75 [0.64; 0.89], p=0.007
Rate of nocturnalsymptomatic hypoglycaemia
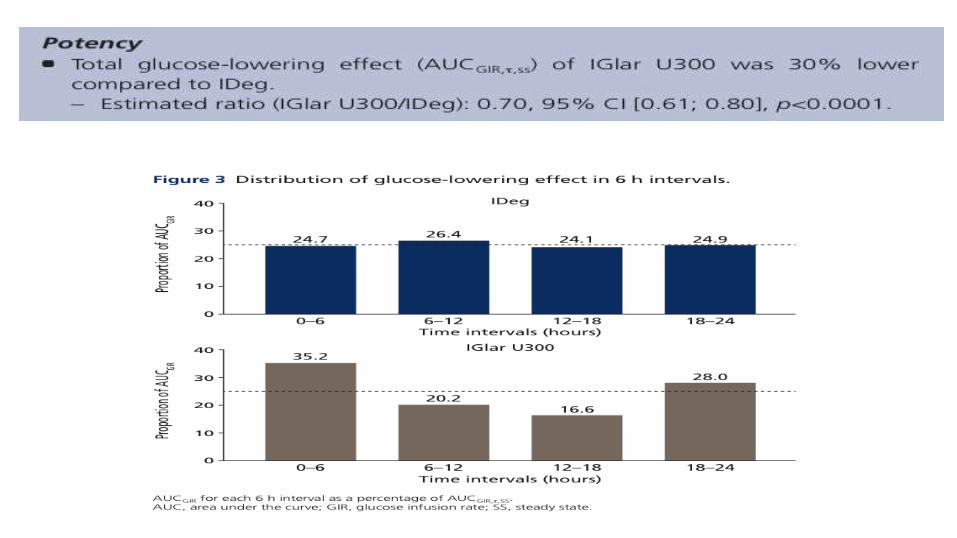
0.70 [0.61; 0.80], p<0.0001
0.58 [0.46; 0.74], p<0.0001
0.54 [0.21; 1.42], NS
Maintenance period
Full treatment period

SWITCH 1: hypoglycaemia
All episodes of severe hypoglycaemia were confirmed by an external adjudication committeeIDeg, insulin degludec; IGlar U100, insulin glargine U100Lane et al. Diabetologia 2016;59(Suppl.1):S42
0.25 0.5 1 2
0.94 [0.91; 0.98], p<0.05
0.74 [0.61; 0.91], p<0.05
Estimated rate ratio [95% CI]
Rate of overallsymptomatic hypoglycaemia
Rate of severe hypoglycaemia
Favours IGlar U100Favours IDeg
0.75 [0.68; 0.83], p<0.05
Rate of nocturnalsymptomatic hypoglycaemia
0.89 [0.85; 0.94], p<0.0001
0.64 [0.56; 0.73], p<0.0001
0.65 [0.48; 0.89], p<0.05
Maintenance period
Full treatment period
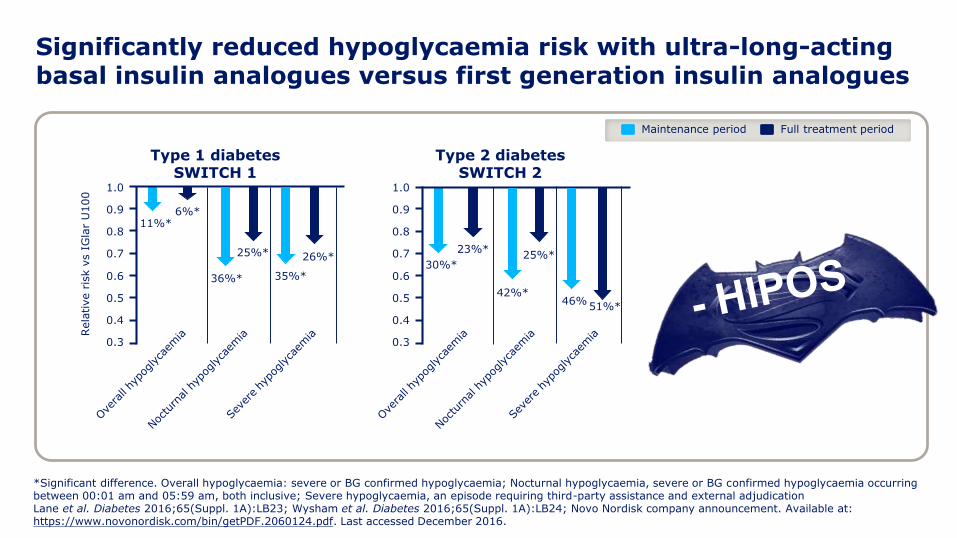
Significantly reduced hypoglycaemia risk with ultra-long-acting basal insulin analogues versus first generation insulin analogues
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
Rela
tive r
isk v
s I
Gla
rU
100
Type 1 diabetes SWITCH 1
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
Type 2 diabetesSWITCH 2
36%*
11%*
35%*30%*
42%*46%
25%*
6%*
26%*23%*
25%*
51%*
*Significant difference. Overall hypoglycaemia: severe or BG confirmed hypoglycaemia; Nocturnal hypoglycaemia, severe or BG confirmed hypoglycaemia occurring between 00:01 am and 05:59 am, both inclusive; Severe hypoglycaemia, an episode requiring third-party assistance and external adjudicationLane et al. Diabetes 2016;65(Suppl. 1A):LB23; Wysham et al. Diabetes 2016;65(Suppl. 1A):LB24; Novo Nordisk company announcement. Available at: https://www.novonordisk.com/bin/getPDF.2060124.pdf. Last accessed December 2016.
Maintenance period Full treatment period

0.5 1 2
BEGIN BB T1 LONG2 (52)
Trial ID (Sem.)
BEGIN FLEX T1†1 (26)
BEGIN BB T2 LONG3 (52)
BEGIN ONCE LONG4 (52)
BEGIN LOW VOLUME5 (26)
BEGIN ONCE ASIA6 (26)
BEGIN FLEX T21 (26)
Rate ratio [95% CI]
Dosis Diaria Total (DM1 & 2)
0.89 [0.84;0.93]
0.87 [0.81;0.94]
1.03 [0.97;1.10]
0.97 [0.89;1.05]
0.89 [0.82;0.98]
0.80 [0.71;0.90]
0.90 [0.82;0.99]
†The ratios reported in Mathieu et al. 2013 (Table 2) deviate from those above as the publication analyses all IDeg patients (i.e. both the forced flex and standard arms)References: 1. Data on file, DOF-MA-IDeg-24APR2013-001, Novo Nordisk A/S; 2. Heller et al. Lancet 2012;379:1489–97; 3. Garber et al. Lancet 2012;379:1498–507; 4. Zinman et al. Diabetes Care 2012;35:2464–71 (+ supplementary online data); 5. Gough et al. Diabetes Care 2013;36:2536–42; 6. Onishi et al. J Diabetes Investig 2013;4:605–12 (+ supplementary online information)
Pacientes DM T1 la dosis total diaria de Ideg fue un 12% significativamente menor que la de IGlar(p<0.0001)1
Pacientes DM T2 insulino naïve, la dosis total diaria fue un 10% menor que con IGlar (p=0.0004)1
- DOSIS
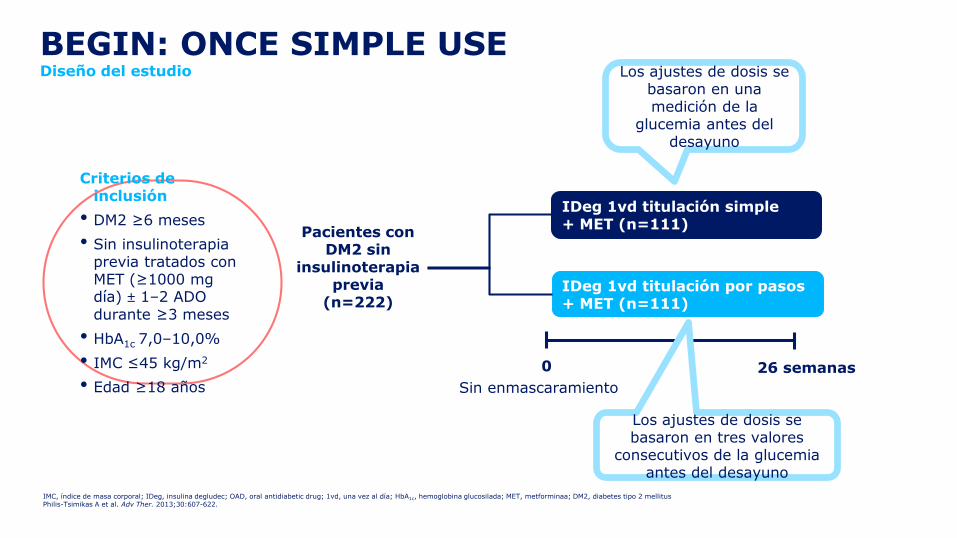
IDeg 1vd titulación simple+ MET (n=111)
IDeg 1vd titulación por pasos+ MET (n=111)
Pacientes con DM2 sin
insulinoterapia previa
(n=222)
0 26 semanas
BEGIN: ONCE SIMPLE USEDiseño del estudio
IMC, índice de masa corporal; IDeg, insulina degludec; OAD, oral antidiabetic drug; 1vd, una vez al día; HbA1c, hemoglobina glucosilada; MET, metforminaa; DM2, diabetes tipo 2 mellitusPhilis-Tsimikas A et al. Adv Ther. 2013;30:607-622.
Criterios de inclusión
• DM2 ≥6 meses
• Sin insulinoterapia previa tratados con MET (≥1000 mg día) ± 1–2 ADO durante ≥3 meses
• HbA1c 7,0–10,0%
• IMC ≤45 kg/m2
• Edad ≥18 años Sin enmascaramiento
Los ajustes de dosis se basaron en una medición de la
glucemia antes del desayuno
Los ajustes de dosis se basaron en tres valores
consecutivos de la glucemia antes del desayuno

BEGIN: ONCE SIMPLE USE Conclusión
• La titulación simple deIDeg mejoró la HbA1c y nofue inferior a la titulaciónpor pasos de IDeg enpersonas con DM2
• Una proporción significativamente más elevada de personas con DM2 alcanzaron una HbA1c <7% con la titulación simple
HbA1c, hemoglobina glucosilada; IDeg, insulina degludec; DM2, diabetes tipo 2 mellitusPhilis-Tsimikas A et al. Adv Ther. 2013;30:607-622.
+ SIMPLE
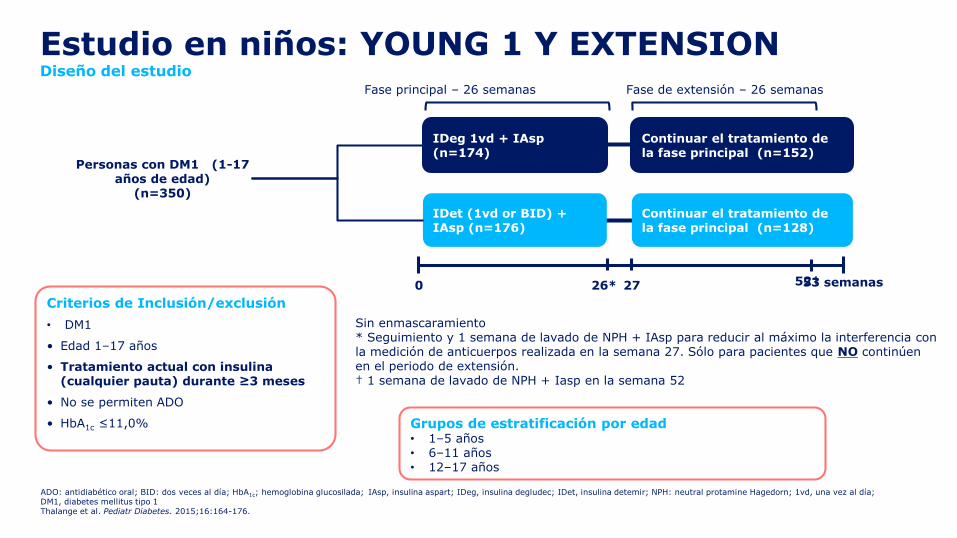
Estudio en niños: YOUNG 1 Y EXTENSION Diseño del estudio
ADO: antidiabético oral; BID: dos veces al día; HbA1c; hemoglobina glucosilada; IAsp, insulina aspart; IDeg, insulina degludec; IDet, insulina detemir; NPH: neutral protamine Hagedorn; 1vd, una vez al día; DM1, diabetes mellitus tipo 1Thalange et al. Pediatr Diabetes. 2015;16:164-176.
Criterios de Inclusión/exclusión
• DM1
• Edad 1–17 años
• Tratamiento actual con insulina (cualquier pauta) durante ≥3 meses
• No se permiten ADO
• HbA1c ≤11,0% Grupos de estratificación por edad• 1–5 años• 6–11 años• 12–17 años
Personas con DM1 (1-17 años de edad)
(n=350)
Continuar el tratamiento de la fase principal (n=152)
Continuar el tratamiento de la fase principal (n=128)
IDeg 1vd + IAsp (n=174)
Fase de extensión – 26 semanasFase principal – 26 semanas
0 26* 27
IDet (1vd or BID) + IAsp (n=176)
52†53 semanas
Sin enmascaramiento* Seguimiento y 1 semana de lavado de NPH + IAsp para reducir al máximo la interferencia con la medición de anticuerpos realizada en la semana 27. Sólo para pacientes que NO continúen en el periodo de extensión.† 1 semana de lavado de NPH + Iasp en la semana 52

Estudio en niños: YOUNG 1 y EXTENSION Conclusión
• El control de A1c fue comparable entre los grupos detratamiento
• Las tasas globales de acontecimientos adversos,acontecimientos adversos graves y parámetros deseguridad fueron comparables entre los grupos detratamiento
• IDeg ofrece una nueva alternativa al tratamiento de laDM1 en la población pediátrica
• En función de este ensayo, se aprobó eluso de Degludec (IDeg) en la poblaciónpediátrica con una edad ≥1 año

ESTUDIOS DE SEGURIDAD
CARDIOVASCULAR EN DM2

DEVOTE summary
CI, confidence interval; EAC, Event Adjudication Committee; HR, hazard ratio; IGlar U100, insulin glargine U100; MACE, major adverse cardiovascular events; N, number of patients at risk; PYO, patient-years of observation
• DEVOTE confirmed the cardiovascular safety of insulin degludec in
comparison with insulin glargine (both U100)
• DEVOTE reported 752 adjudication-confirmed severe
hypoglycemic events in a blinded head-to-head trial
• A 40% lower rate of severe hypoglycemia was confirmed at similar
levels of HbA1c
• A 53% lower rate of nocturnal severe hypoglycemia was confirmed
at a lower fasting plasma glucose
3-point MACE (primary)
HR: 0.91[0.78; 1.06]
Non-inferiority confirmed
p<0.001
Severe hypoglycemia
Rate ratio: 0.60 [0.48; 0.76]
p<0.001
Nocturnal severe hypoglycemia
Rate ratio: 0.47[0.31; 0.73]
p<0.001
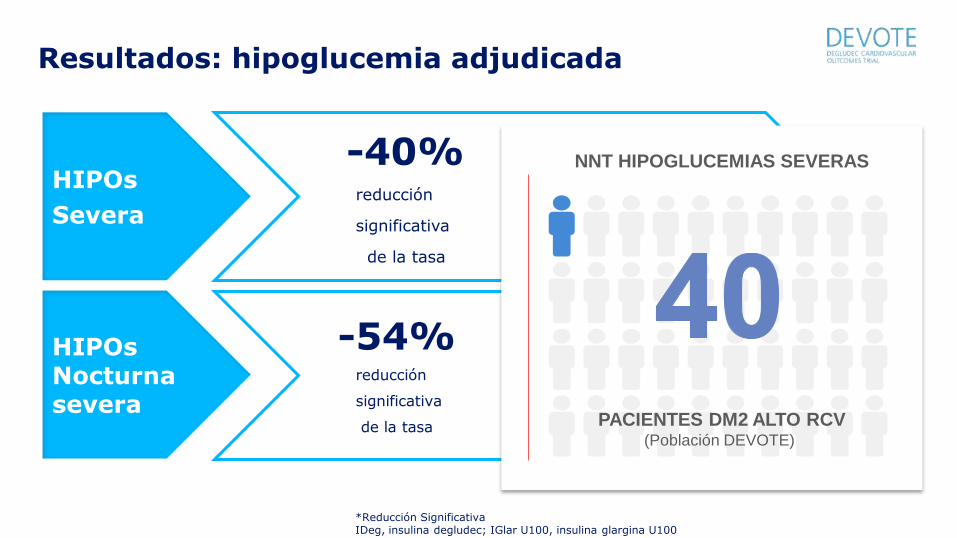
Resultados: hipoglucemia adjudicada
*Reducción SignificativaIDeg, insulina degludec; IGlar U100, insulina glargina U100
-40%*
HIPOs
Severa
-40% reducción
significativa
de la tasa
HIPOs Nocturnasevera
-54% reducción
significativa
de la tasa
-60
-40
-20
0
Reducció
nen
la
incid
encia
de …
-60
-40
-20
0
Reducció
nen
la
incid
encia
de …
-54%*
PACIENTES DM2 ALTO RCV(Población DEVOTE)
NNT HIPOGLUCEMIAS SEVERAS
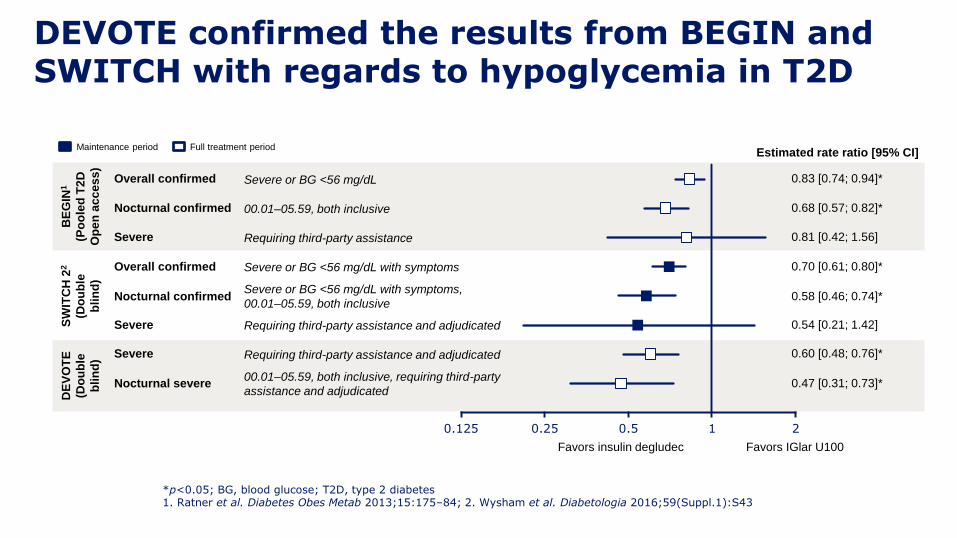
DEVOTE confirmed the results from BEGIN and SWITCH with regards to hypoglycemia in T2D
*p<0.05; BG, blood glucose; T2D, type 2 diabetes1. Ratner et al. Diabetes Obes Metab 2013;15:175–84; 2. Wysham et al. Diabetologia 2016;59(Suppl.1):S43
Maintenance period Full treatment period
0.68 [0.57; 0.82]*
Estimated rate ratio [95% CI]
0.83 [0.74; 0.94]*Overall confirmed
Nocturnal confirmed
0.81 [0.42; 1.56]Severe
0.58 [0.46; 0.74]*
0.60 [0.48; 0.76]*
0.47 [0.31; 0.73]*
0.54 [0.21; 1.42]
0.70 [0.61; 0.80]*Overall confirmed
Nocturnal confirmed
SevereSW
ITC
H 2
2
(Do
ub
le
bli
nd
)
DE
VO
TE
(Do
ub
le
bli
nd
)
Severe
Nocturnal severe
0.125 0.25 0.5 1 2
Favors IGlar U100Favors insulin degludec
BE
GIN
1
(Po
ole
d T
2D
Op
en
ac
ce
ss
)
Severe or BG <56 mg/dL
00.01–05.59, both inclusive
Requiring third-party assistance
Severe or BG <56 mg/dL with symptoms
Severe or BG <56 mg/dL with symptoms,
00.01–05.59, both inclusive
Requiring third-party assistance and adjudicated
Requiring third-party assistance and adjudicated
00.01–05.59, both inclusive, requiring third-party
assistance and adjudicated
Evidencia
Ensayos clínicos
Experiencia
Vida Real
LA INSULINA DEL SXXI
SUPERBASALES
Preferencia
Voz del paciente
@cristob_morales





Código colores
Ventana de la dosis más grande
Dosis máxima 80 U
Click audible que nos confirma la administración de la dosis
El botón de administración no se extiende con ninguna dosis
Menor fuerza para
la administración
FlexTouch®: Una nueva generación
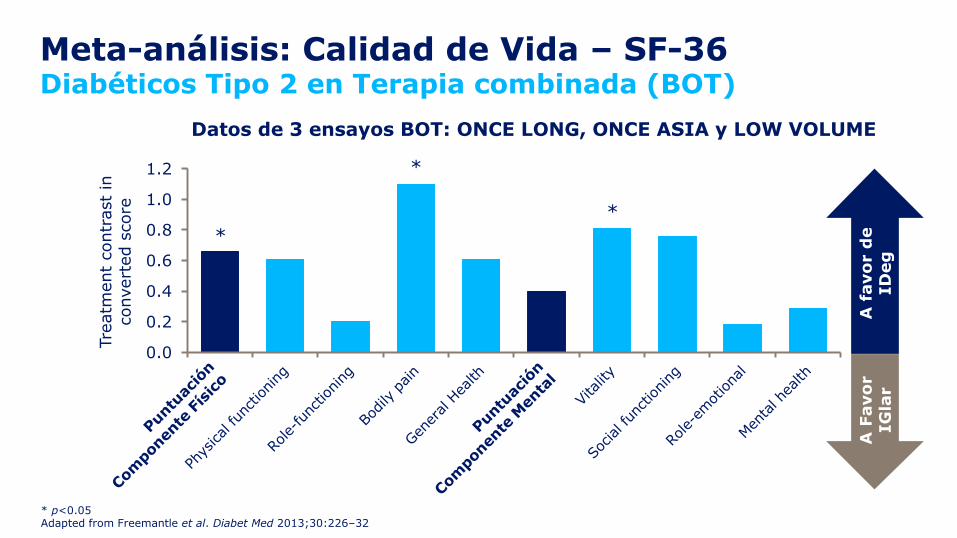
Meta-análisis: Calidad de Vida – SF-36Diabéticos Tipo 2 en Terapia combinada (BOT)
* p<0.05Adapted from Freemantle et al. Diabet Med 2013;30:226–32
Datos de 3 ensayos BOT: ONCE LONG, ONCE ASIA y LOW VOLUME
0.0
0.2
0.4
0.6
0.8
1.0
1.2
Tre
atm
ent
contr
ast
inconvert
ed s
core
A f
avo
rd
eID
eg
*
*
*
A F
avo
rIG
lar

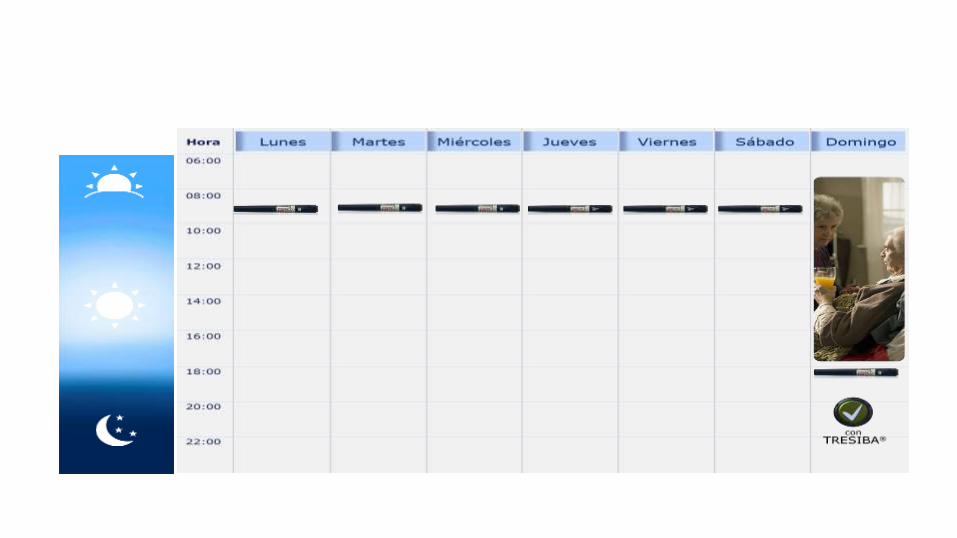
Insulina degludec regimen flexibleFlex Study” concepto: Dosis Flexible (Forzada)
mañana
Lunes Mar Mier Jue Vie Sab Dom
mañana mañana
noche noche noche noche40h 40h
8h
24h
8h
40h
Meneghini et al. Diabetes Care 2013;36:858–64; Mathieu et al. J Clin Endocrinol Metab 2013;98:1154–62

Insulin degludec: “Flexible” Treatment regimen
Insulin degludec: “Flexible” Treatment regimen

Insulin degludec: “Flexible” Treatment regimen
Preferencia
Voz del paciente
Evidencia
Ensayos clínicos
LA INSULINA DEL SXXI
SUPERBASALES
@cristob_morales
Experiencia
Vida Real

RESULTADOS VIDA REAL: comercializada en españa desde ene16
ENSAYOS
CLINICOS
VIDA
REAL
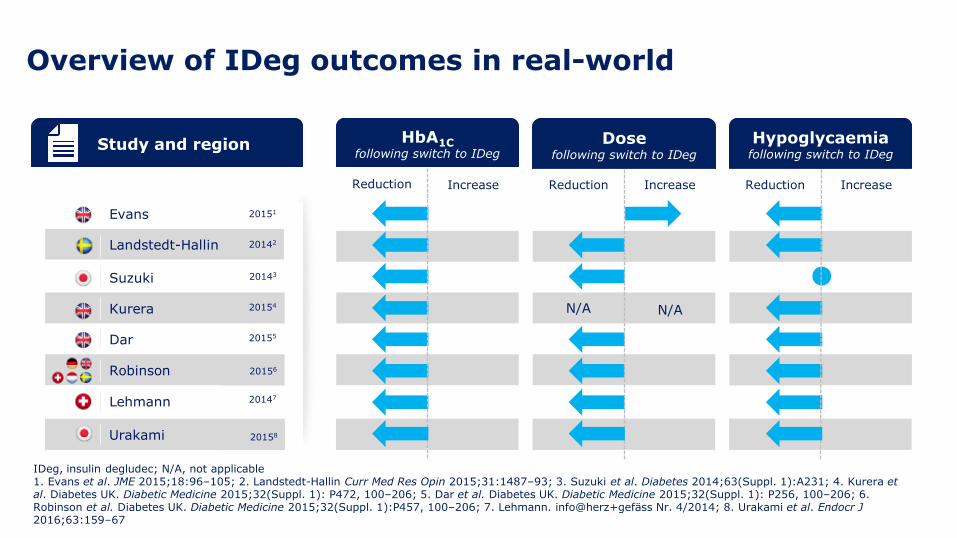
Study and region
Evans
Suzuki
Kurera
Dar
Robinson
Lehmann
Landstedt-Hallin 20142
20147
20155
20154
20143
20151
Hypoglycaemiafollowing switch to IDeg
Dosefollowing switch to IDeg
IncreaseReductionIncreaseReduction
N/A N/A
HbA1Cfollowing switch to IDeg
Reduction Increase
Urakami
20156
20158
Overview of IDeg outcomes in real-world
IDeg, insulin degludec; N/A, not applicable1. Evans et al. JME 2015;18:96–105; 2. Landstedt-Hallin Curr Med Res Opin 2015;31:1487–93; 3. Suzuki et al. Diabetes 2014;63(Suppl. 1):A231; 4. Kurera et al. Diabetes UK. Diabetic Medicine 2015;32(Suppl. 1): P472, 100–206; 5. Dar et al. Diabetes UK. Diabetic Medicine 2015;32(Suppl. 1): P256, 100–206; 6. Robinson et al. Diabetes UK. Diabetic Medicine 2015;32(Suppl. 1):P457, 100–206; 7. Lehmann. info@herz+gefäss Nr. 4/2014; 8. Urakami et al. Endocr J2016;63:159–67

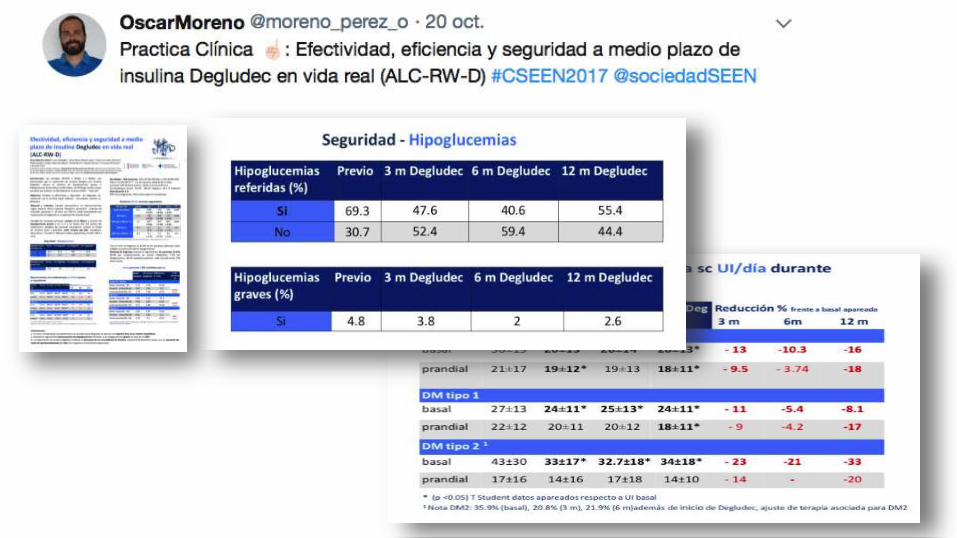
181 pacientes
70,2% hombres,29,8% mujeresEdad: 55,9 ±18,2 años Años de evolución de DM: 15,7±10,9
DM1: 33% DM2: 67%
Motivos para el cambio:
Hipoglucemias (41,7%)Variabilidad glucémica (24,1%)Dosis basal desdoblada (12,7%)Mal control metabólico (A1c > 8%) (21,5%).
EXPERIENCIA HUVM VIDA REAL UPDATE NOV16
33%
67%
DM1 DM2

EXPERIENCIA HUVM VIDA REAL update nov16
181 pacientes en los que se completó el seguimiento trimestral
A1c: 8,1±1,9%.
HBA1c :- 0.98±1,6% (*sign)
Peso: + 0,85± 2,8 kg(*sign)
No Hipos graves
Dosis de insulina total: - 7,05±23,2UI (-10,1%) (*sign)insulina basal: - 3,30±01,9UI (- 8,3%) (*sign)insulina rápida: - 4,30±2UI (- 3,9%) (*sign)
* p < 0,0001




Hypos Seguridad CV
VARIABILIDAD
¿QUE PODERES PEDIMOS A LAS SUPERBASALES?
Calidadde
Vida

Preferencia
Voz del paciente
Evidencia
Ensayos clínicos
LA INSULINA DEL SXXI
SUPERBASALES
@cristob_morales
Experiencia
Vida Real

Los pacientes pasan tiempo a solas con la responsabilidadautogestionar su diabetes6 horas/año con su equipo médico, 8760 Horas/año solos

DETECTANDO PERFILES
DE ALTO RIESGO
18:20-19:00
@Cristob.Morales

@Cristob_Morales
HIPOs
VARIABILIDAD
GLUCEMICA
TIEMPO EN RANGOA1
c @cristo
b_
mo
rale
s

EFICACIA_A1cEFICACIA_A1c
NO HIPOs
@cristob.morales
NUESTRAS EXIGENCIAS AUMENTAN
EFICACIA_A1cNO HIPOs ++++VARIABILIDADFLEXIBILIDAD
SEGURIDAD CARDIOVASCULAR

@Cristob_Morales
La clave del éxito es la PERSONALIZACION

+ FLEXIBILIDAD
5RAZONES
PARA ELEGIR
1 INSULINA
SUPERBASAL
@Cristob.Morales

LA MEJOR INSULINA ES:
-La que el paciente se pone y la que se adapte a su vida
“adherirme al tratamiento sin
desadherime a mi vida”
-La que le de SEGURIDAD al paciente
- Hipos- Variabilidad- Dosis- Pinchazos

@CRISTOB_MORALES
DIABETESHIPOs
VARIAB



Fuente: www.doctablet.com
Fuente: www.doctablet.com

Fuente: www.doctablet.com

RESERVAS PARA DEBATE: CLAMPS

Day-to-day and within-day variability in glucose-lowering effect between
I.Deg and Gla-300
Heise T, Kaplan K, Haahr HL
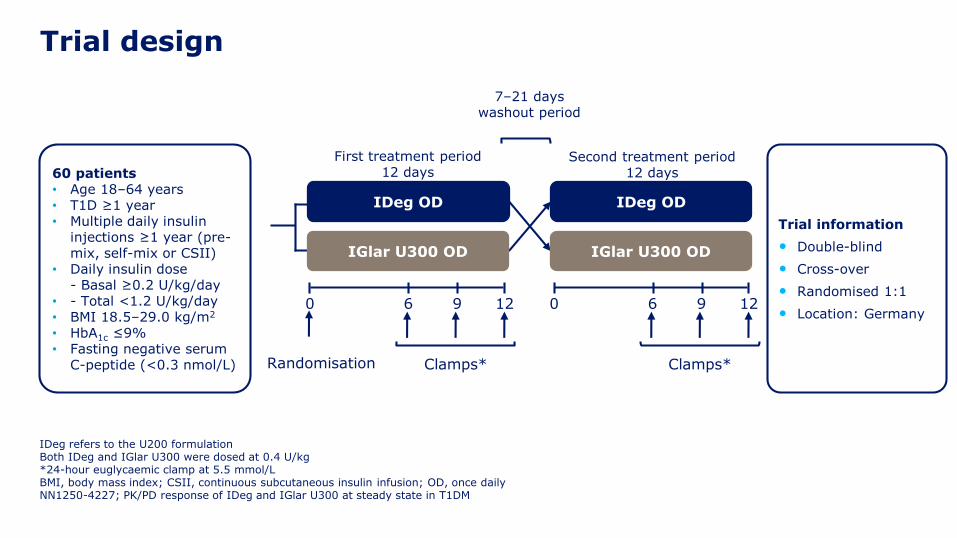
Trial design
Trial information
• Double-blind
• Cross-over
• Randomised 1:1
• Location: Germany
60 patients• Age 18–64 years• T1D ≥1 year• Multiple daily insulin
injections ≥1 year (pre-mix, self-mix or CSII)
• Daily insulin dose- Basal ≥0.2 U/kg/day
• - Total <1.2 U/kg/day • BMI 18.5–29.0 kg/m2
• HbA1c ≤9%• Fasting negative serum
C-peptide (<0.3 nmol/L)
First treatment period12 days
Second treatment period12 days
IGlar U300 OD
IDeg OD
IGlar U300 OD
IDeg OD
7–21 days washout period
Clamps*
0 6 9 12
Clamps*
0 6 9 12
Randomisation
IDeg refers to the U200 formulationBoth IDeg and IGlar U300 were dosed at 0.4 U/kg*24-hour euglycaemic clamp at 5.5 mmol/LBMI, body mass index; CSII, continuous subcutaneous insulin infusion; OD, once dailyNN1250-4227; PK/PD response of IDeg and IGlar U300 at steady state in T1DM




Fuente: www.doctablet.com
RESERVAS PARA DEBATE: PRECIO

IDEG 100U5 plumas x 3ml
IGLAR 300U3 plumas x 1,5ml
PVP IVA * 82,57 € 51,94€
U / Pack 1500 1350
Coste unitario 0,0550 € 0,0385 €
Coste tratamiento/día **
1,76 € (32 U) 1,54 € (40 U)
Coste tratamiento/año 642,91 € 561,72 €
Coste incremental anual Ideg vs Iglar300 +81,19 €
* Aplicación de la deducción del 7,5% conforme al Real Decreto-ley 8/2010 en insulina degludec
** Se debe considerar una reducción de la dosis del 20% en base a la dosis de insulina basal previa seguida de ajustes de dosis individuales cuando se cambia a I.Deg desde I.Glar300

Fuente: www.doctablet.com



DUELO DE SUPERBASALES