drug information center constipation & diarrhea and diarhea... · drug information center...
TRANSCRIPT
Drug Information Center
Constipation & Diarrhea
Constipation
What is constipation?
A medical condition characterized by : a stool frequency of less than three times per week (or) Bowel movements with stool that is
hard, dry, and small, making it painful or difficult to pass.
How it's diagnosed?
To be called constipation it must include two or more of the following criteria :
● straining during at least 25 percent of defecations
● Lumpy or hard stools in at least 25 percent of defecations
● Sensation of incomplete evacuation for at least 25 percent of defecations
● Sensation of anorectal obstruction/blockage for at least 25 percent of defecations
● Manual maneuvers to facilitate at least 25 percent of defecations
● Fewer than three defecations per week
Also we must exclude any other causes like irritable bowel syndrome
The above criteria must be fulfilled for the last three months prior the diagnosis.
What is the etiology and pathophysiology of constipation?
Constipation can be due to disorder of movement of stool in colon due to slowing of colonic transit may be idiopathic or may be
due to secondary causes.
Example of secondary causes of constipation :
Obstructing lesions of the gastrointestinal tract, including colorectal cancer, endocrine disorders such as diabetes mellitus, and
psychiatric disorders such as anorexia nervosa. Also can be due to a side effect of drugs.
Evaluation of constipation:
History from the patient, physical examination and laboratory result this entire three play major rule in evaluation of constipation.
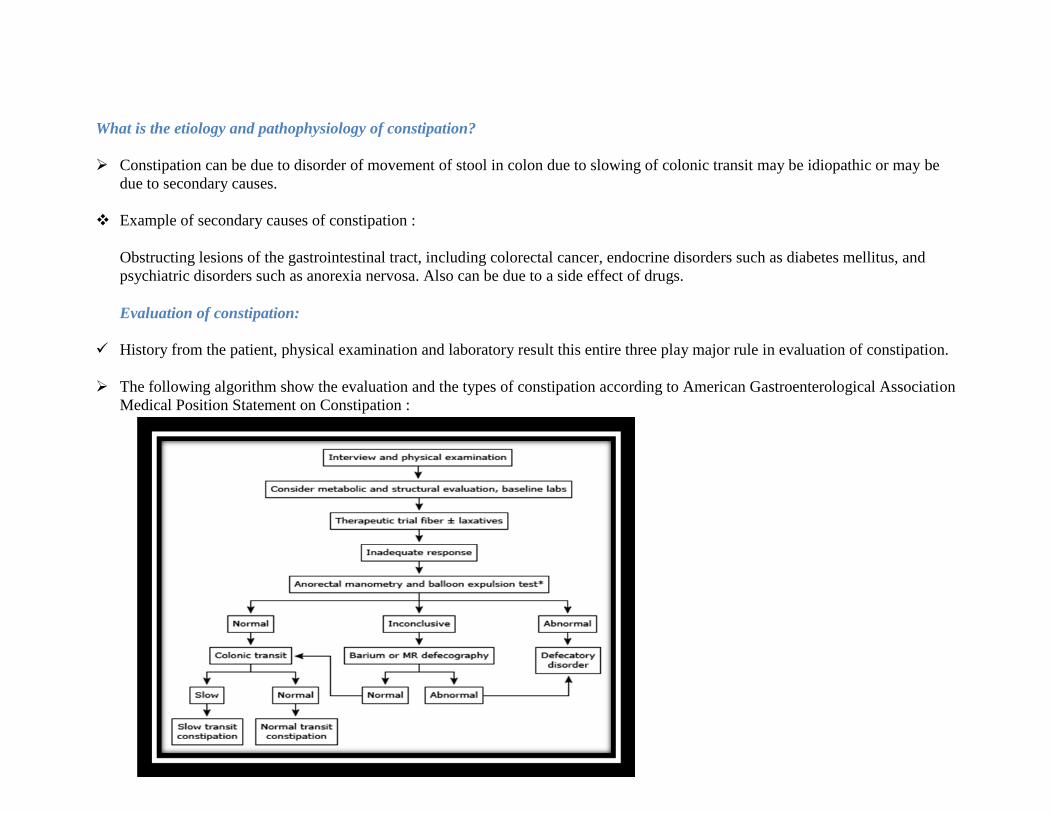
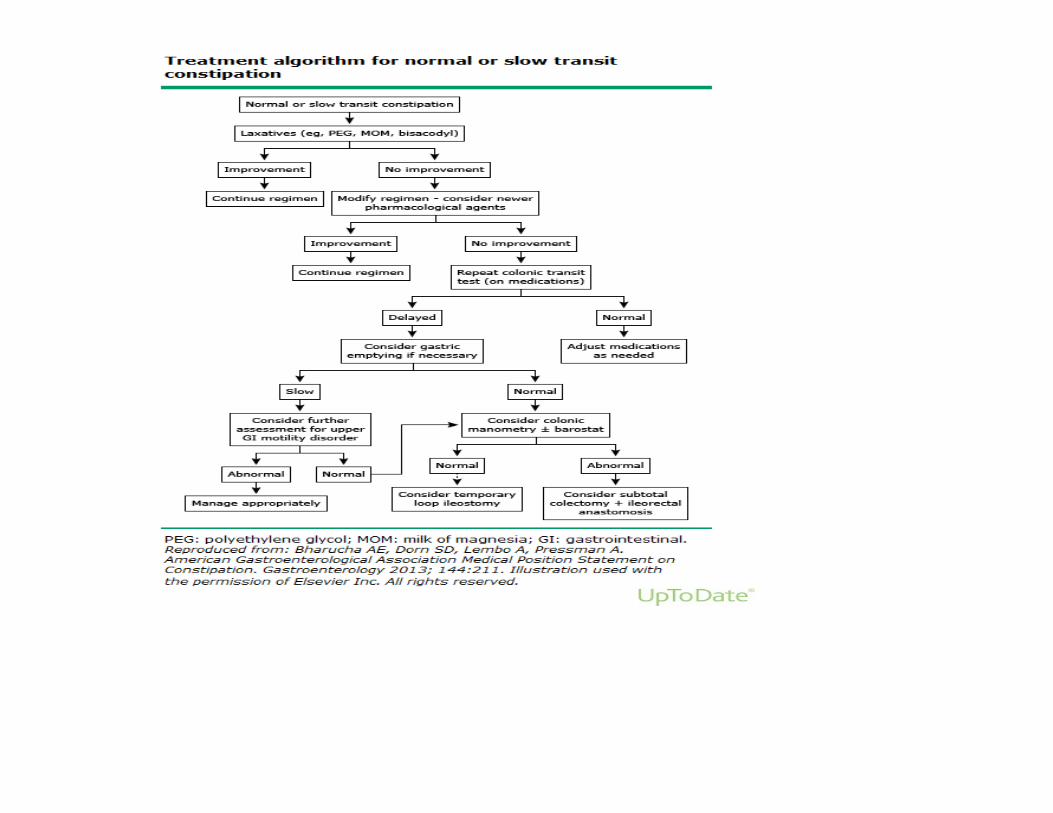
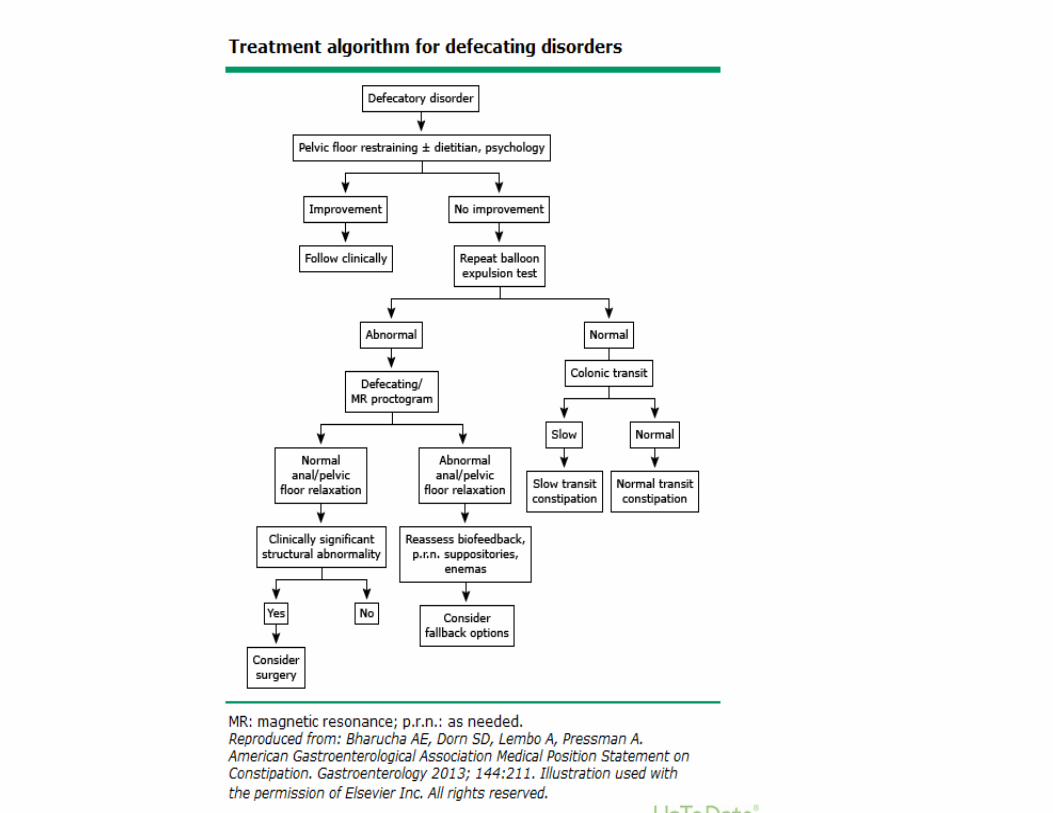
The following algorithm show the evaluation and the types of constipation according to American Gastroenterological Association
Medical Position Statement on Constipation :
Risk factors for constipation:
Female gender.
Over 65 years of age.
Low caloric intake (eating less food).
Greater number of medications used.
Sedentary lifestyle (lack of exercise).
Ignoring the urge to defecate
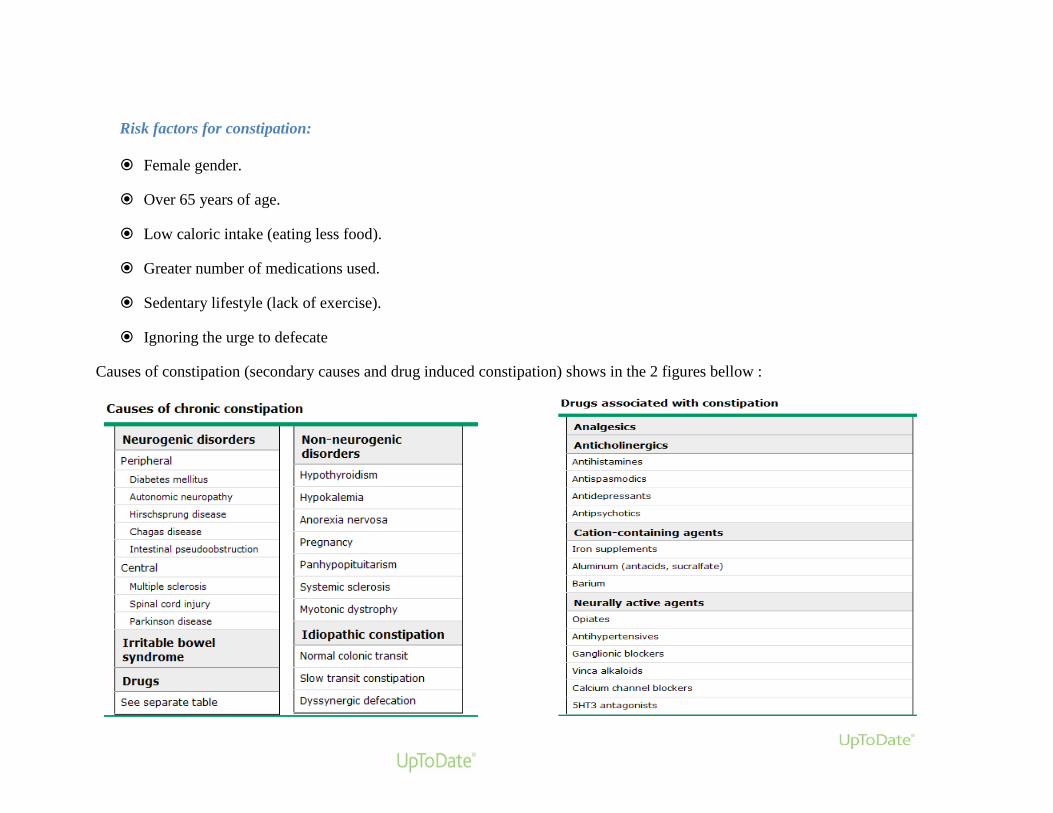
Causes of constipation (secondary causes and drug induced constipation) shows in the 2 figures bellow :
Treatment of constipation:
1- Non pharmacologic therapy.
Patient education : it involves efforts to reduce dependency on laxatives and to increase fluid and fiber intake, Patients who are
dependent on laxatives should be advised to try to taper their use, as they introduce new measures to improve bowel function.
Patients should be advised to try to defecate after meals, thereby taking advantage of normal postprandial increases in colonic
motility.
Drink more water and other liquids (eight-ounce glasses a day).
A 30 minute walk every day may help keep you more regular.
Food rich in fibers like : ( fruits and vegetables , legumes, juices, breads, grains and nuts )
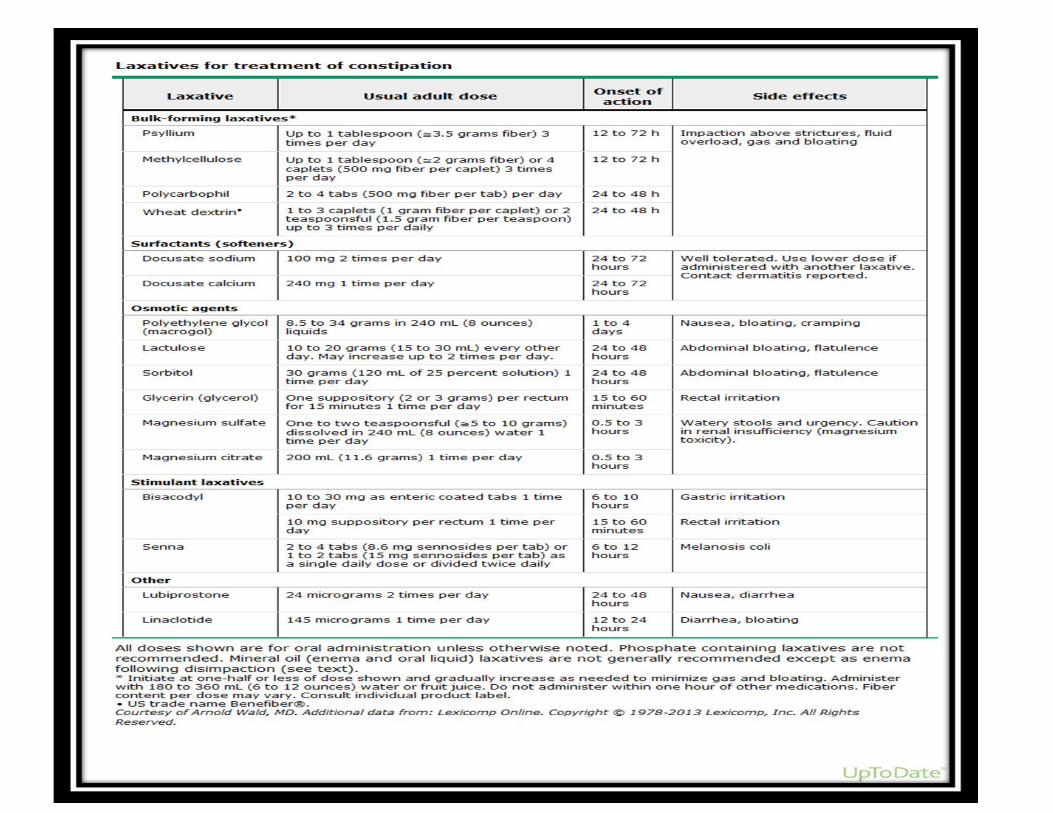
2- Pharmacological therapy.
The following two algorithms show pharmacologic treatment of constipation according to American Gastroenterological
Association Medical Position Statement on Constipation :
References
References:
http://www.uptodate.com.lib.just.edu.jo/contents/constipation-in-the-older-
adult?source=search_result&search=constipation&selectedTitle=3~150#H1058373655This topic last updated: Aug 22, 2013.
Joseph Dipiro , Robert Talbert , Gary Yee , Gary Matzke , Barbara Wells , L.Michael Posey , Pharmacotherapy: A
Pathophysiologic Approach , 8th
edition , 2011 ,627-634.
American Gastroenterological Association medical position statement on constipation, accessed in 6/4/2014,
http://www.guideline.gov/content.aspx?id=43610&search=constipatio
Diarrhea Guideline
Diarrhea is an increased frequency and decreased consistency of fecal discharge as compared with normal individuals. Frequency and
consistency are variable within and between individuals. Most cases of acute diarrhea are caused by infections with viruses, bacteria,
or protozoa.
PATHOPHYSIOLOGY
Diarrhea is an imbalance in absorption and secretion of water and electrolytes, and occure by 4 mechanism :
(1) A change in active ion transport by either decreased Na absorption or increased CL secretion
(2) Change in intestinal motility.
(3) Increase in luminal osmolarity.
(4) Increase in tissue hydrostatic pressure.
*These mechanisms have been related to 4 clinical diarrheal groups: secretory, osmotic, exudative, and altered intestinal transit.
Groups of diarrhea:
(1) Secretory diarrhea:
Occurs when a stimulating substance (e.g., vasoactive intestinal peptide [VIP], laxatives, or bacterial toxin) increases secretion or
decreases absorption of large amounts of water and electrolytes.
(2) Osmotic diarrhea:
Poorly absorbed substances retain intestinal fluids.
(3) Inflammatory diseases of the GI tract can cause exudative diarrhea by discharge of mucus, proteins, or blood into the gut.
(4) Altered Intestinal motility can be by reduced contact time in the small intestine, premature emptying of the colon, and by bacterial
overgrowth
Clinical Presentation of Diarrhea
Usually, acute diarrheal episodes subside within 72 hours of onset, whereas chronic diarrhea involves frequent attacks over extended
time periods more than 14 days.
Signs and symptoms
1- Abrupt onset of nausea, vomiting, abdominal pain, headache, fever, chills, and malaise.
2- Bowel movements are frequent and never bloody, and diarrhea lasts 12–60 hours.
3- Intermittent periumbilical or lower right quadrant pain with cramps and audible bowel sounds is characteristic of small
intestinal disease.
4- When pain is present in large intestinal diarrhea, it is a gripping, aching sensation with tenesmus (straining, ineffective and
painful stooling). Pain localizes to the hypogastric region, right or left lower quadrant, or sacral region.
5- In chronic diarrhea, a history of previous bouts, weight loss, anorexia, and chronic weakness are important findings.
Laboratory tests
Stool analysis include examination for microorganisms, blood, mucus, fat, osmolality, pH, electrolyte and mineral
concentration, and cultures.
Stool test kits are useful for detecting GI viruses, particularly rotavirus.
Determine total daily stool volume.
Endoscopic visualization and biopsy of the colon may be undertaken to assess for the presence of conditions such as colitis or
cancer.
Radiographic studies are helpful in neoplastic and inflammatory conditions
Drugs Causing Diarrhea
Laxatives.
Antacids containing magnesium
Antineoplastics
Antibiotics:
Clindamycin ,Tetracyclines,Sulfonamides,Any broad-spectrum antibiotic
Antihypertensives:Reserpine,Guanethidine,Methyldopa,Guanabenz,Guanadrel,Angiotensin-converting enzyme inhibitors
Cholinergics:
Bethanechol,Neostigmine
Cardiac agents:
Quinidine,Digitalis,Digoxin
Nonsteroidal antiinflammatory drugs.
Misoprostol
Colchicine
Proton pump inhibitors
H2-receptor blocker
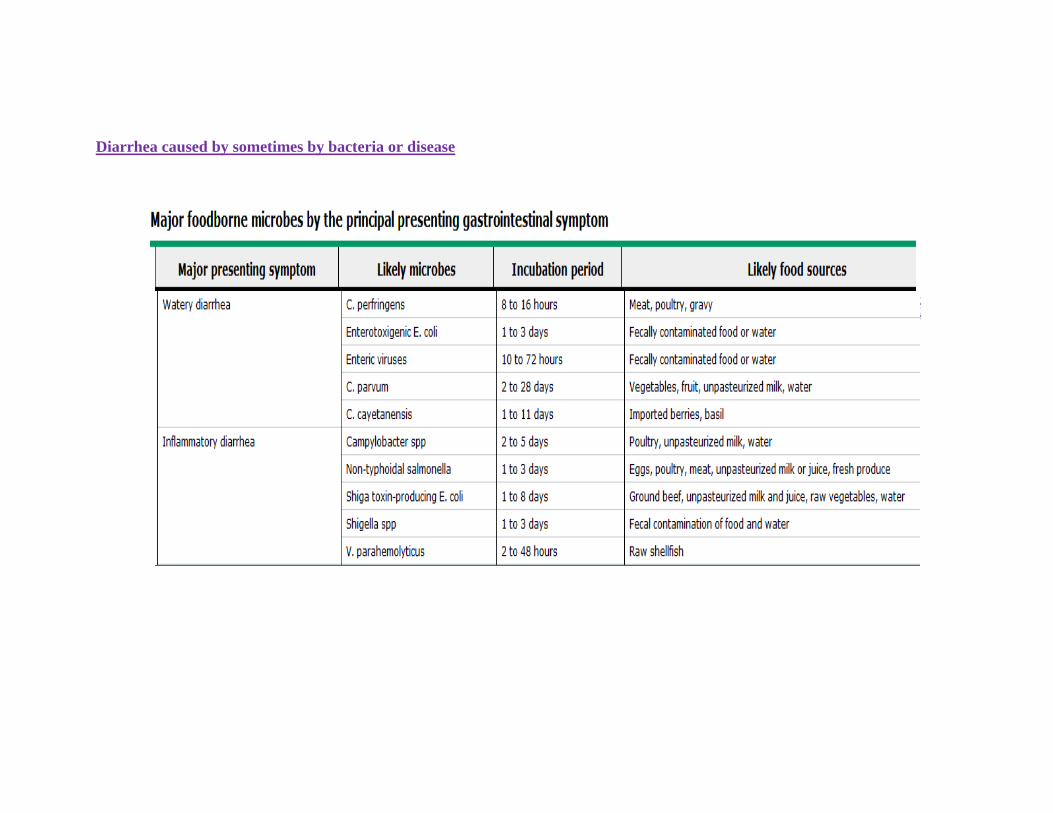
Diarrhea caused by sometimes by bacteria or disease
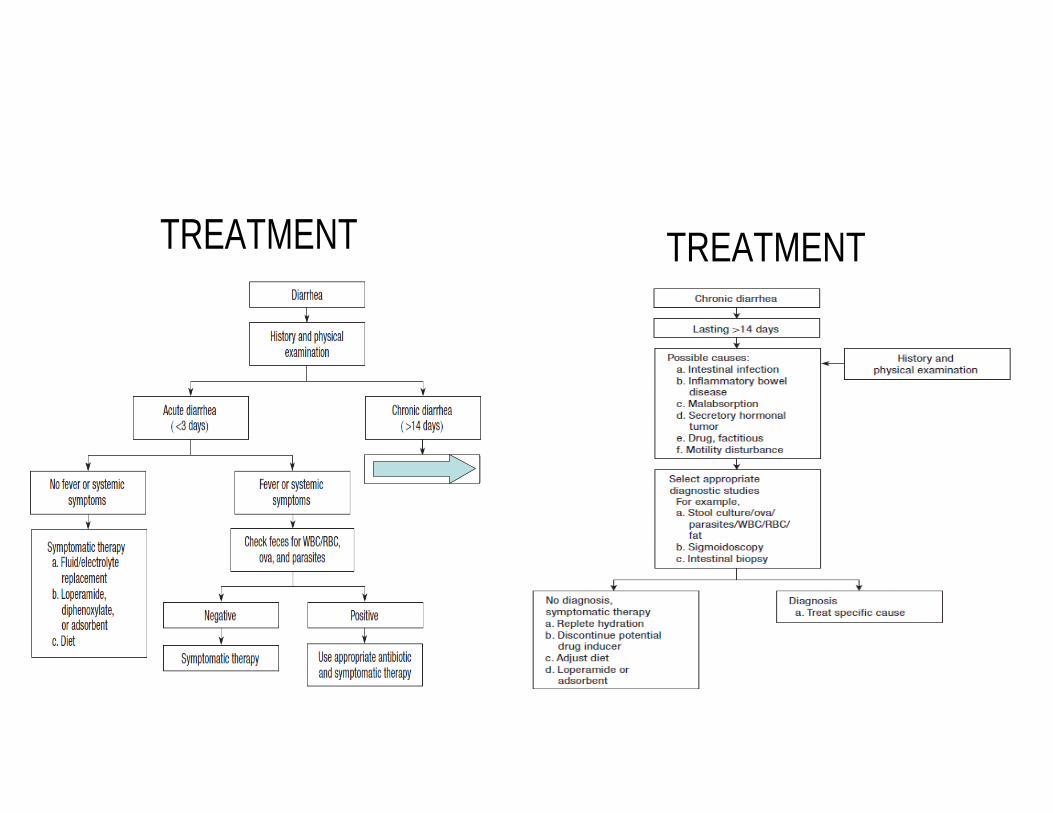
TREATMENT TREATMENT
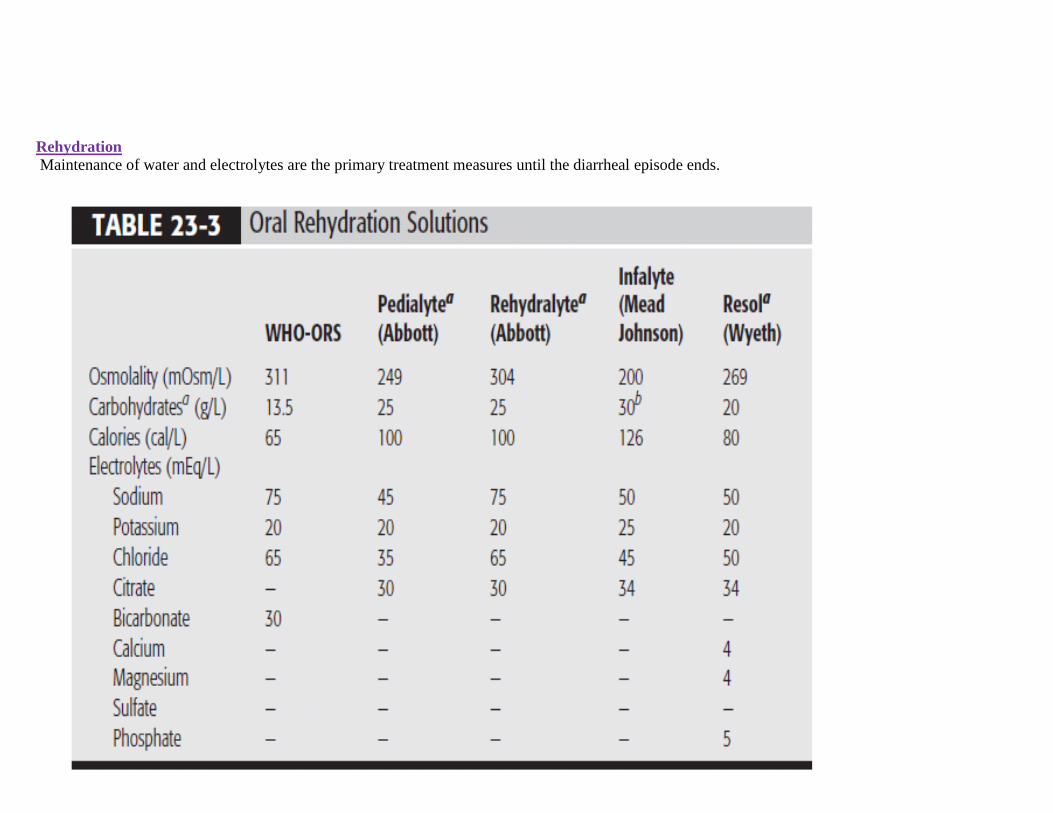
Rehydration
Maintenance of water and electrolytes are the primary treatment measures until the diarrheal episode ends.

Feeding consideration
When nausea or vomiting is mild, a digestible
Low-residue diet is administered for 24 hours.
Like eat white rice and white breads as they are lower in fiber
*If vomiting is present and is uncontrollable with antiemetics, nothing is taken by mouth. As bowel movements decrease, a bland diet is begun.
Bland diet (soft, low-fiber, non-spicy) may include:
low-fat milk and other lowfat dairy;
Cooked, canned, or frozen vegetables;
Cooked or canned fruit
*Feeding should continue in children with acute bacterial diarrhea
*If vomiting is present and is uncontrollable with antiemetic, nothing is taken by mouth
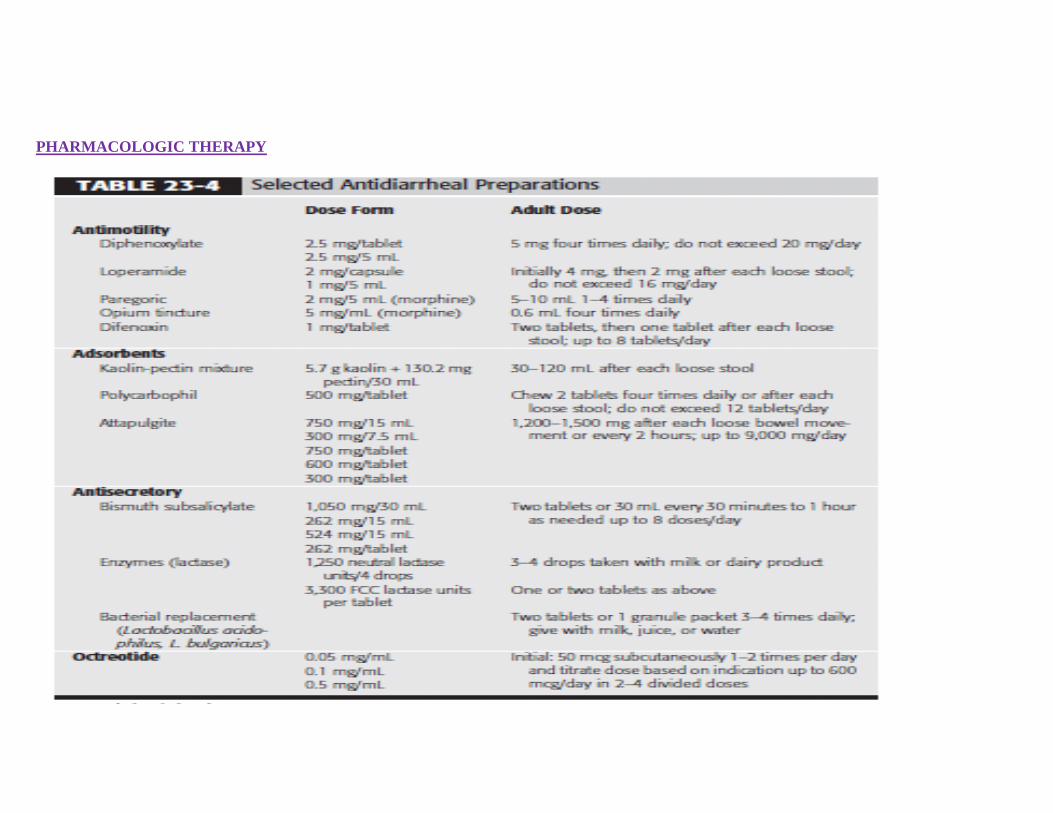
PHARMACOLOGIC THERAPY
* Usually, these drugs are not curative but palliative.
* Loperamide: is often recommended for managing acute and chronic diarrhea
*Adsorbents (such as kaolin-pectin) : are used for symptomatic relief they are nonspecific in their action; they adsorb nutrients, toxins, drugs, and
digestive juices. Coadministration with other drugs reduces their bioavailability.
*Antisecratory:
1.Bismuth subsalicylate
Is often used for treatment or prevention of diarrhea (traveler’s diarrhea) and has antisecretory, antiinflammatory, and antibacterial effects .
Bismuth subsalicylate contains multiple components that might be toxic if given in excess to prevent or treat diarrhea
2. Lactobacillus: preparation is intended to replace colonic microflora. This supposedly restores intestinal functions and suppresses the growth of
pathogenic microorganisms.
A dairy product diet containing 200 to 400 g of lactose or dextrin is equally effective in recolonization of normal flora.
*Octreotide, somatostatin
Act by reduce the intestinal secretion and slow the GIT motility
Octreotide is used in selected patients with carcinoid syndrome
Octreotide is associated with adverse effects such as cholelithiasis, nausea, diarrhea, and abdominal pain.
Evaluation of therapeutic outcome
Acute diarrhea:
In the absence of dehydration, high fever, and blood or mucous in stool, the illness self limiting within 3-7 days .Mild-moderate usually managed
on an outpatient basis with oral rehydration symptomatic treatment and diet.
Elderly with chronic illness & infants may require hospitalization for parenteral rehydration Severe diarrhea :
Restoration of patients volume status is the most important outcome .
Toxic patients (those with fever, dehydration, and hematochezia and those who are hypotensive) require hospitalization; they need IV electrolyte
solutions and empiric antibiotics while awaiting cultures.
References
1- DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM, eds, Diarrhea, Pharmacotherapy
Handbook: A Pathophysiologic Approach. 7th ed. New York, NY: McGraw-Hill; 2056-2062
2- Peter A L Bonis, MD-,J Thomas LaMont, MD, Approach to the adult with chronic diarrhea in developed countries,
http://www.uptodate.com/contents/approach-to-the-adult-with-chronic-diarrhea-in-developed-countries?source=related_link This topic last updated: Jun 7, 2011
Reviewed BY: Pharm.D: Sami kelani, Mohammad Ali . 9/4/2014