drug discovery : from lead optimization to clinical ... discovery : from lead optimization to...
TRANSCRIPT

Drug Discovery : From Lead
Optimization to Clinical Candidate
and beyond
Giovanni Gaviraghi
Chief Executive Officer
Siena Biotech
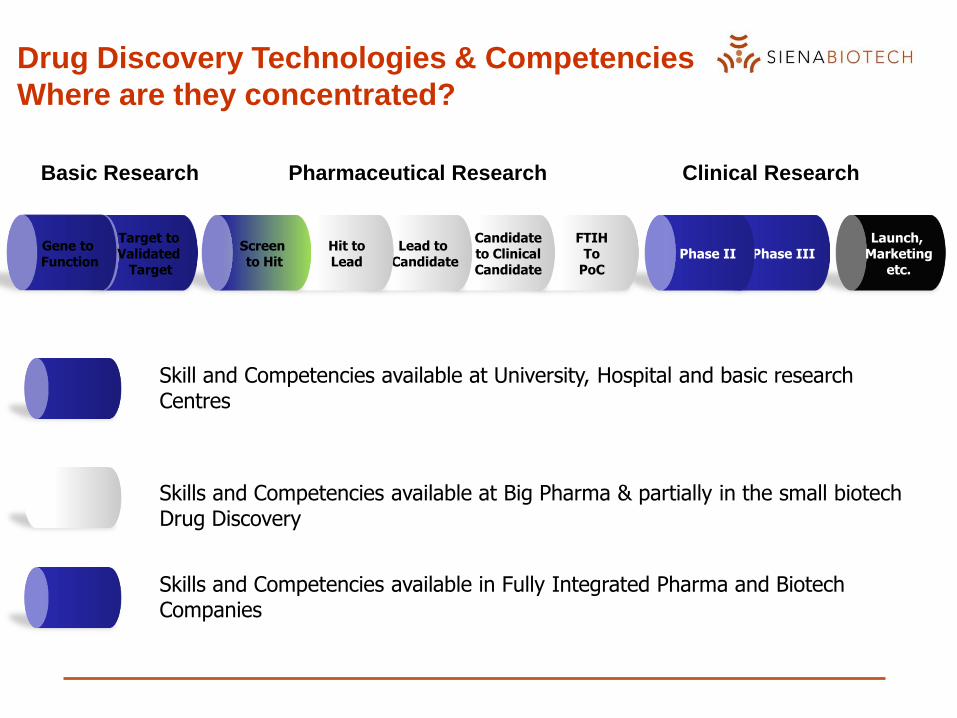
Drug Discovery Technologies & Competencies
Where are they concentrated?
Launch, Marketing
etc.Phase IIIPhase II
FTIHTo
PoC
Candidateto ClinicalCandidate
Lead to Candidate
Hit toLead
Screen to Hit
Target to Validated
Target
Gene to Function
Skill and Competencies available at University, Hospital and basic research Centres
Skills and Competencies available at Big Pharma & partially in the small biotech Drug Discovery
Skills and Competencies available in Fully Integrated Pharma and Biotech Companies
Basic Research Pharmaceutical Research Clinical Research

Studio della
malattia
Il Modello di Siena Biotech : ponte fra ricerca accademica e
clinica
Nuove cure piu’ efficaci e
sicure
Università
Grandi Aziende
Farmaceutiche
Multinazionali
Ricerca applicata per
nuovi farmaci
Ricerca di baseRicerca applicata
Clinica Mercato
Attività e competenze presenti in: Università, Ospedali, CNR ecc.
Attività e competenze presenti nelle grandi aziende farmaceutiche multinazionali
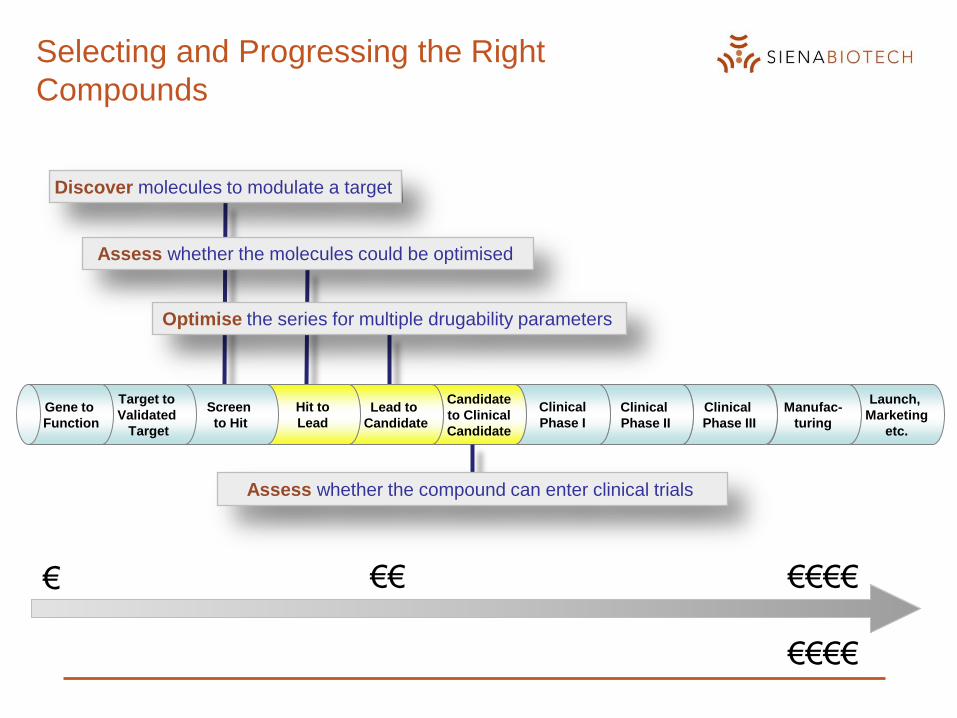
Selecting and Progressing the Right
Compounds
Launch,
Marketing
etc.
Manufac-
turing
Clinical
Phase III
Clinical
Phase II
Clinical
Phase I
Candidate
to Clinical
Candidate
Lead to
Candidate
Hit to
Lead
Screen
to Hit
Target to
Validated
Target
Gene to
Function
Discover molecules to modulate a target
Assess whether the molecules could be optimised
Optimise the series for multiple drugability parameters
Assess whether the compound can enter clinical trials
€ €€ €€€€
€€€€

Non-Linear Project Progress Path
Commit to
bioassay design
and screening
Commit to lead
optimization
Commit to target
validation
Commit to lead
identification
Lead to
Candidate
PhenotypeScreening
Commit to
exploratory
biology
Target ID
ForwardChemicalGenetics
Drug DesignChemistry
Gene to Function
Hit to Lead
Target Validation
Screen to Hit
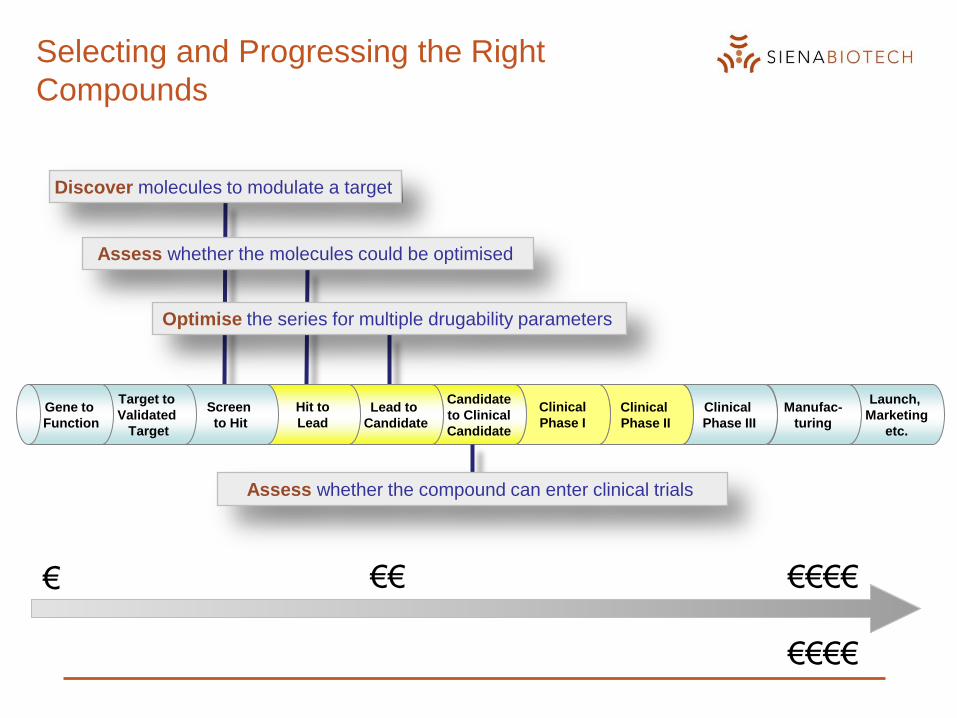
Selecting and Progressing the Right
Compounds
Launch,
Marketing
etc.
Manufac-
turing
Clinical
Phase III
Clinical
Phase II
Clinical
Phase I
Candidate
to Clinical
Candidate
Lead to
Candidate
Hit to
Lead
Screen
to Hit
Target to
Validated
Target
Gene to
Function
Discover molecules to modulate a target
Assess whether the molecules could be optimised
Optimise the series for multiple drugability parameters
Assess whether the compound can enter clinical trials
€ €€ €€€€
€€€€
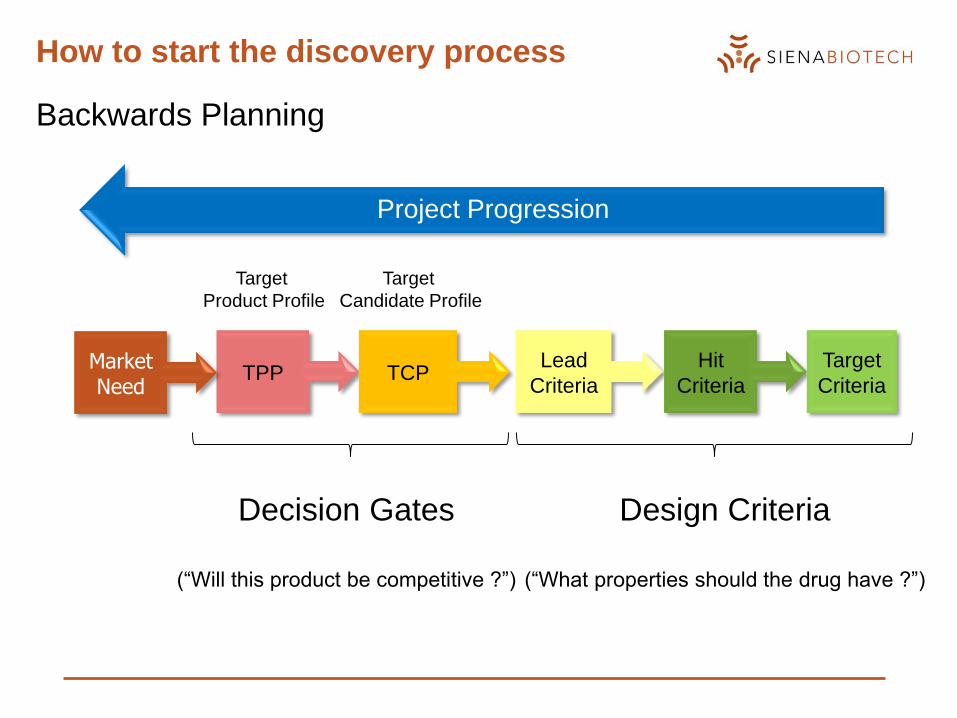
How to start the discovery process
TPP TCPLead
Criteria
Hit
Criteria
Target
Criteria
Project Progression
Market Need
Backwards Planning
Decision Gates
(“Will this product be competitive ?”)
Design Criteria
(“What properties should the drug have ?”)
Target
Product Profile
Target
Candidate Profile
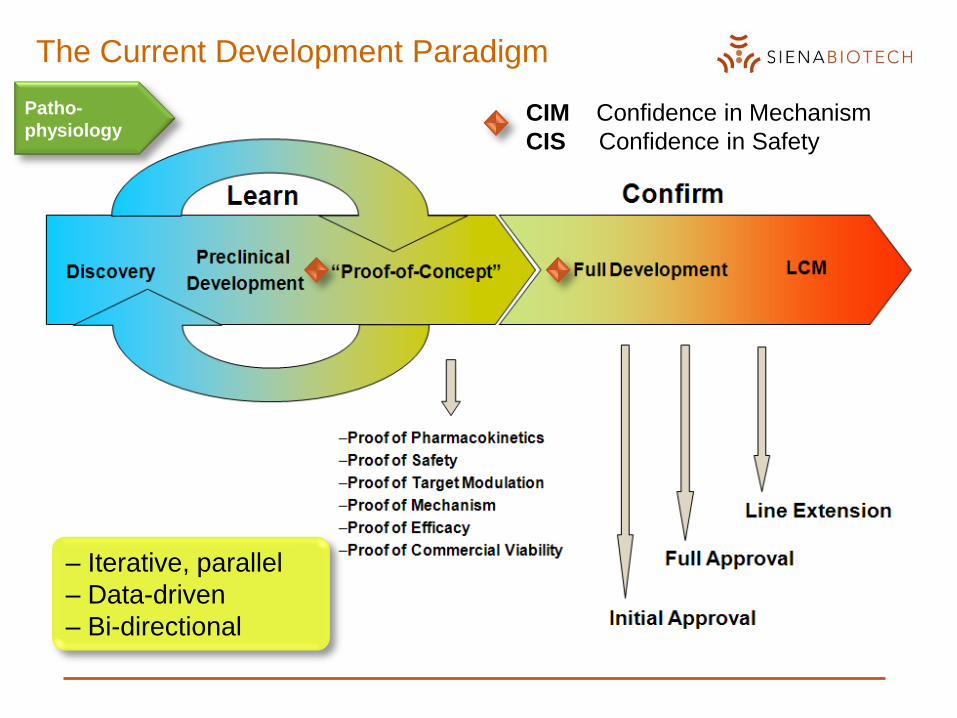
The Current Development Paradigm
Patho-
physiologyCIM Confidence in Mechanism
CIS Confidence in Safety
– Iterative, parallel
– Data-driven
– Bi-directional
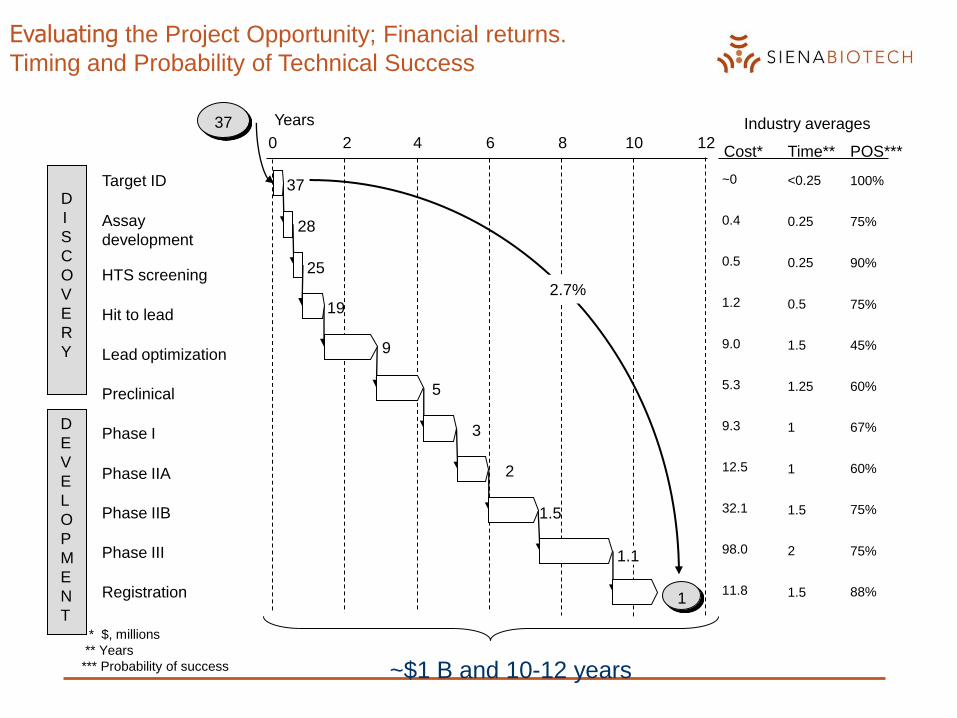
Evaluating the Project Opportunity; Financial returns.
Timing and Probability of Technical Success
0 2 4 6 8 10 12
Assay
development
Hit to lead
Lead optimization
D
I
S
C
O
V
E
R
Y
HTS screening
Target ID
Years
Preclinical
Phase I
Phase IIA
Phase IIB
Phase III
D
E
V
E
L
O
P
M
E
N
T
Registration
37
28
25
19
9
5
3
2
1.5
1.1
1
Cost*
0.4
1.2
9.0
0.5
~0
5.3
9.3
12.5
32.1
98.0
11.8
0.5
1.5
<0.25
1.25
1
Time**
0.25
0.25
1
1.5
2
1.5
37
POS***
75%
75%
45%
90%
100%
60%
67%
60%
75%
75%
88%
* $, millions
** Years
*** Probability of success
2.7%
Industry averages
~$1 B and 10-12 years
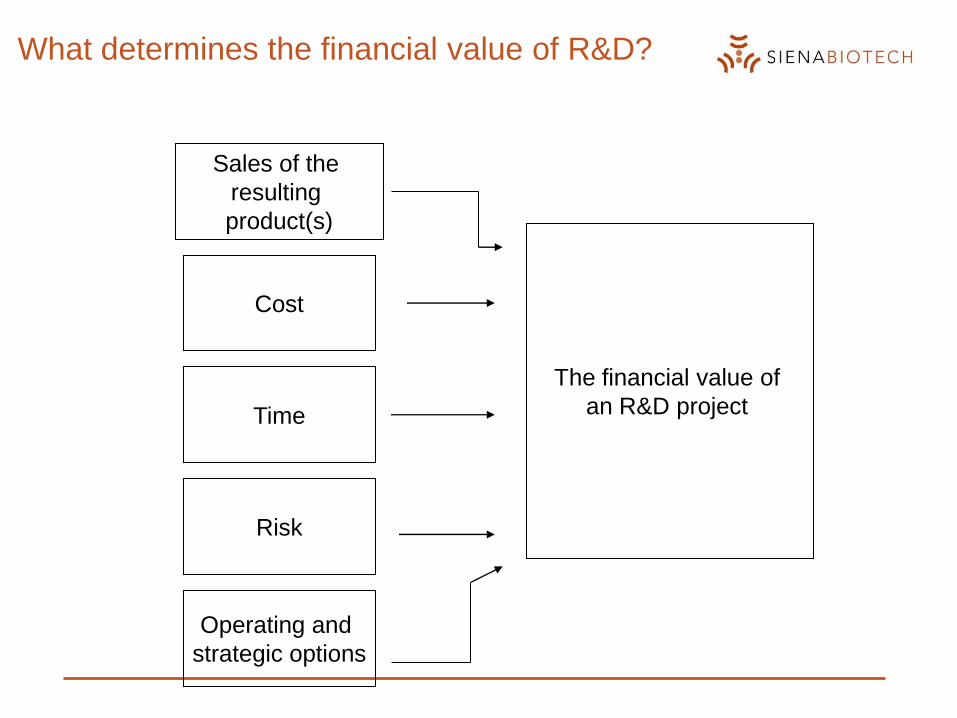
What determines the financial value of R&D?
Sales of the
resulting
product(s)
Cost
Time
Risk
Operating and
strategic options
The financial value of
an R&D project

Many Sources of Uncertainity
Technical
Timing
Market
Commercial
Efficacy
SafetyTolerability / Convenience
Manufacturing ( eg. CoG )
Annual cash flow
Order of market entry
Epidemiology / Segmentation
Healthcare
reimbursement/access
DiagnosisCompliance
Competition
Price
Resources
Development Phase is reached: Re-assessing Product Profile,
Project Potential and Market Opportunity
In other words, construction of the
final Target Product Profile starts at this point.

Target Product Profile is developed on the basis of
a combination/compromise of many customers’
needs and expectations
Key Indicator Document
Key Indicator Document
– Detailed analysis of disease/condition from a clinical, marketing
and regulatory perspective
– Current and future situation; epidemiology
– Careful analysis of competitor situation
– Market dynamics and Healthcare Provider aspects
– Produced by Business and Clinical Research as starting point for
setting corporate strategy
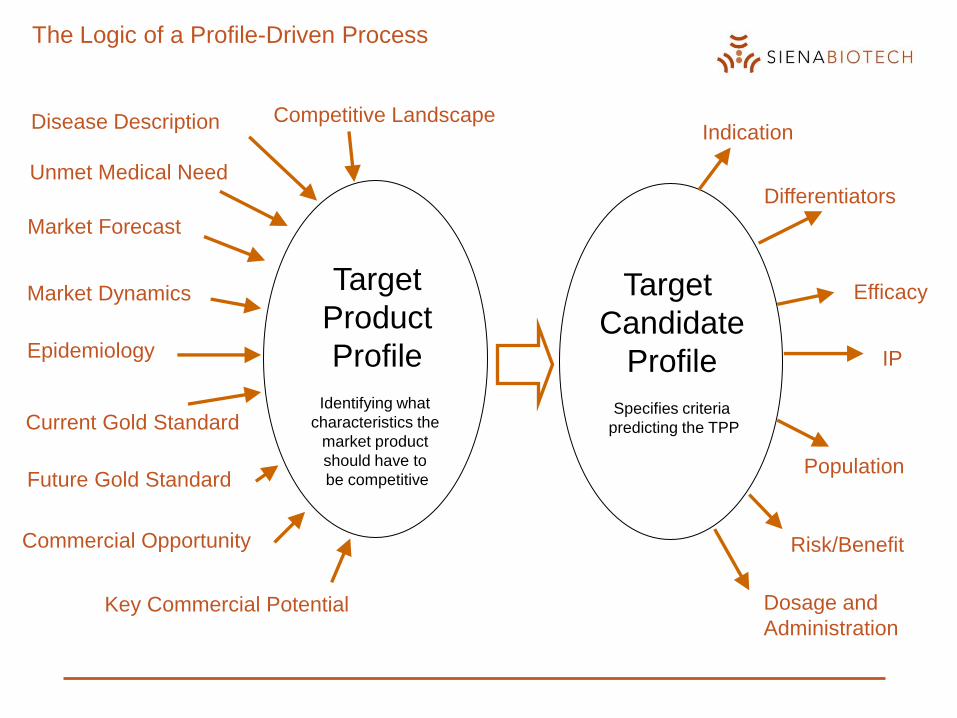
The Logic of a Profile-Driven Process
Disease Description
Commercial Opportunity
Competitive Landscape
Market Forecast
Key Commercial Potential
Market Dynamics
Unmet Medical Need
Epidemiology
Current Gold Standard
Future Gold Standard
Target
Product
Profile
Identifying what
characteristics the
market product
should have to
be competitive
Target
Candidate
Profile
Specifies criteria
predicting the TPP
Indication
Population
Efficacy
Risk/Benefit
Dosage and
Administration
IP
Differentiators
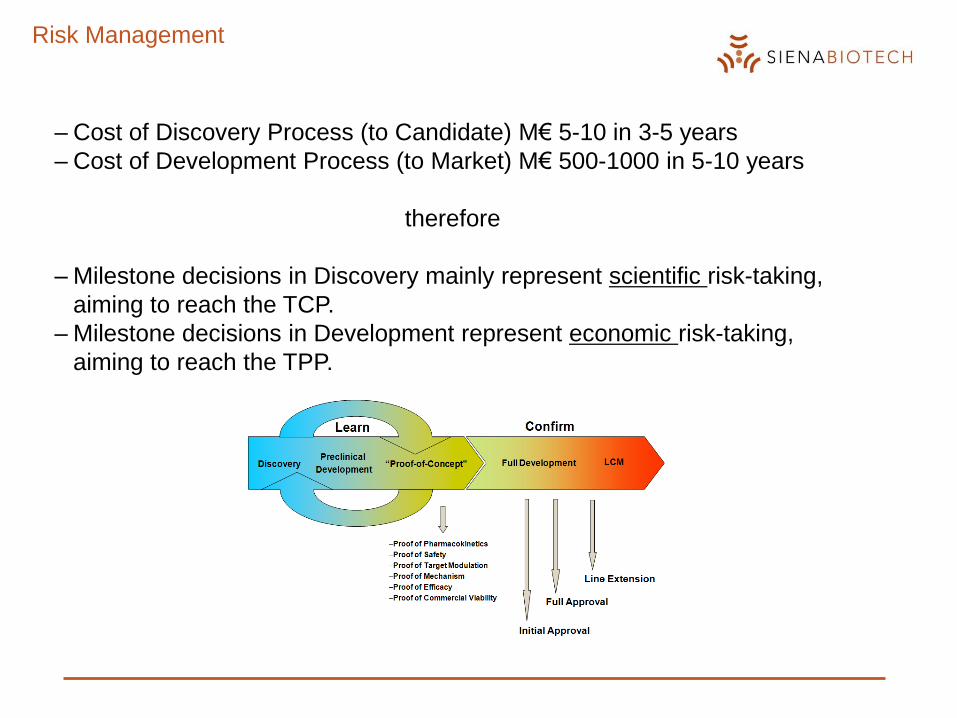
Risk Management
– Cost of Discovery Process (to Candidate) M€ 5-10 in 3-5 years
– Cost of Development Process (to Market) M€ 500-1000 in 5-10 years
therefore
– Milestone decisions in Discovery mainly represent scientific risk-taking,
aiming to reach the TCP.
– Milestone decisions in Development represent economic risk-taking,
aiming to reach the TPP.
The Lead to Candidate Phase
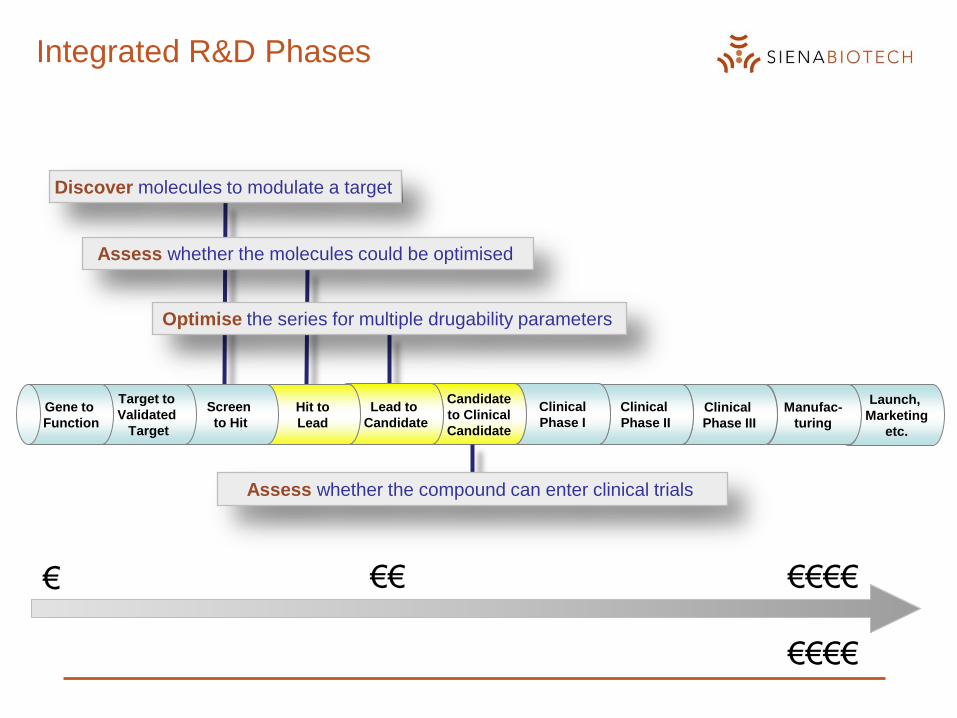
Integrated R&D Phases
Launch,
Marketing
etc.
Manufac-
turing
Clinical
Phase III
Clinical
Phase II
Clinical
Phase I
Candidate
to Clinical
Candidate
Lead to
Candidate
Hit to
Lead
Screen
to Hit
Target to
Validated
Target
Gene to
Function
Discover molecules to modulate a target
Assess whether the molecules could be optimised
Optimise the series for multiple drugability parameters
Assess whether the compound can enter clinical trials
€ €€ €€€€
€€€€
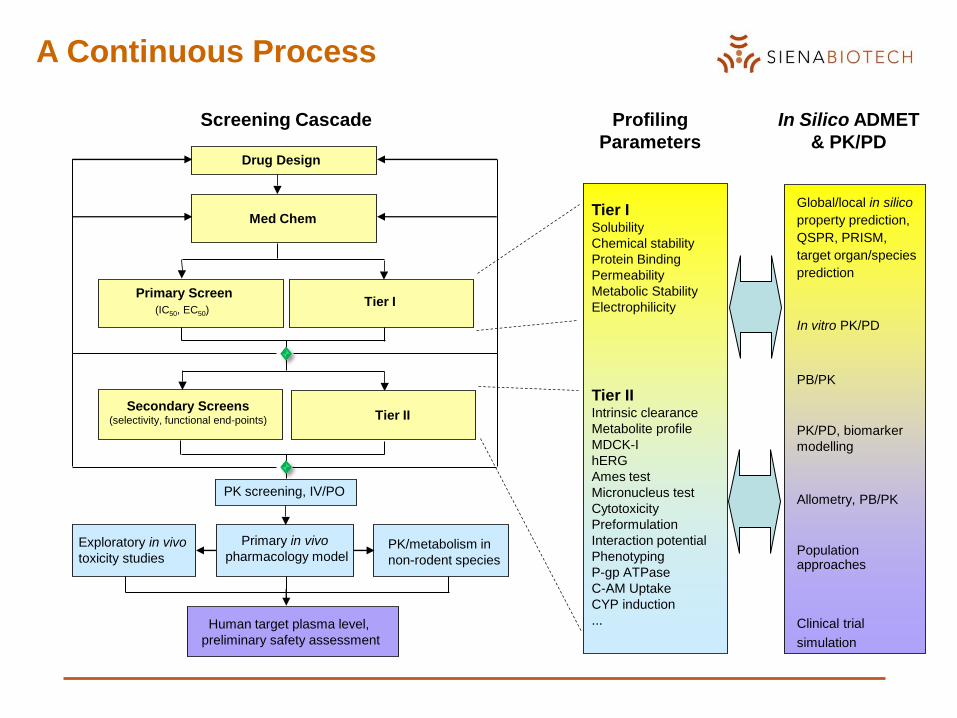
Primary Screen
(IC50, EC50)
Secondary Screens(selectivity, functional end-points)
Med ChemTier ISolubility
Chemical stability
Protein Binding
Permeability
Metabolic Stability
Electrophilicity
PK/metabolism in
non-rodent species
Human target plasma level,
preliminary safety assessment
Global/local in silico
property prediction,
QSPR, PRISM,
target organ/species
prediction
In vitro PK/PD
PB/PK
PK/PD, biomarker
modelling
Allometry, PB/PK
Population approaches
Clinical trial
simulation
Tier IIIntrinsic clearance
Metabolite profile
MDCK-I
hERG
Ames test
Micronucleus test
Cytotoxicity
Preformulation
Interaction potential
Phenotyping
P-gp ATPase
C-AM Uptake
CYP induction
...
PK screening, IV/PO
Primary in vivo
pharmacology modelExploratory in vivo
toxicity studies
Profiling
Parameters
In Silico ADMET
& PK/PD
Screening Cascade
A Continuous Process
Drug Design
Tier I
Tier II
Lead optimisation is not just about potency!
Other important parameters for a successful new medicine

Desired Lead Profile
Confirmed structures and structural classes
SAR indicating potential for optimisation
What are the areas of the molecule responsible for affinity?
Which areas of the molecule can be changed without affecting affinity?
Potential for patent protection (looks promising with general searches,
identified areas to avoid)
Potent in vitro activity has been achieved for the series
e.g. <100 nM or <5 M in a phenotypic assay
Some selectivity activity versus closely related targets
Tractable chemistry - no obvious synthetic problems with class
Promising Tier 1 & 2 ADME data with an understanding of potential problems
with the lead class
An indication of activity in vivo.
Desired Preclinical Candidate Profile
The molecule(s) should have\be
Potent and selective in vitro activity
Efficacy demonstrated in appropriate in vivo models
Acceptable selectivity profile in “Cerep” and “cardiac” panels
Acceptable/manageable toxicity profile in preliminary in vivo settings
Patented/patentable
Scaleable chemistry – “fit for purpose” route available to make 50-500g
“Fit for purpose” formulation for tox and additional efficacy studies
Physicochemical properties aligned for a candidate molecule (more later)
Backup molecule(s)
Build understanding of mechanism
At Preclinical Candidate Selection
Alea iacta est
This is the end of “structural optimisation”
We are now selecting the molecule (or in some companies 2-3
molecules) to go into preclinical development.
It will succeed or fail based on its developability
The only changes to the compound that can be made to improve
chances of success are:
Drug delivery – formulation, dose regime etc
Cost of goods – improved synthesis on large scale

Typical good hits/initial leads are/have:
Potent against the cellular target (low nanomolar IC50)
Defined Structure Activity Relationship (SAR)
Synthetically accessible
Good to moderate patent position
Some indication/promise of efficacy in vivo
Moderate solubility
Selectivity vs. other enzymes/receptors not ideal
Needing improvement of in vivo potency
Unoptimised oral bioavailability or other PK parameters
Possible dose limiting toxicity
No advanced backup class should problems occur
So what are we trying to optimise?
Secondary
properties
of the
molecules
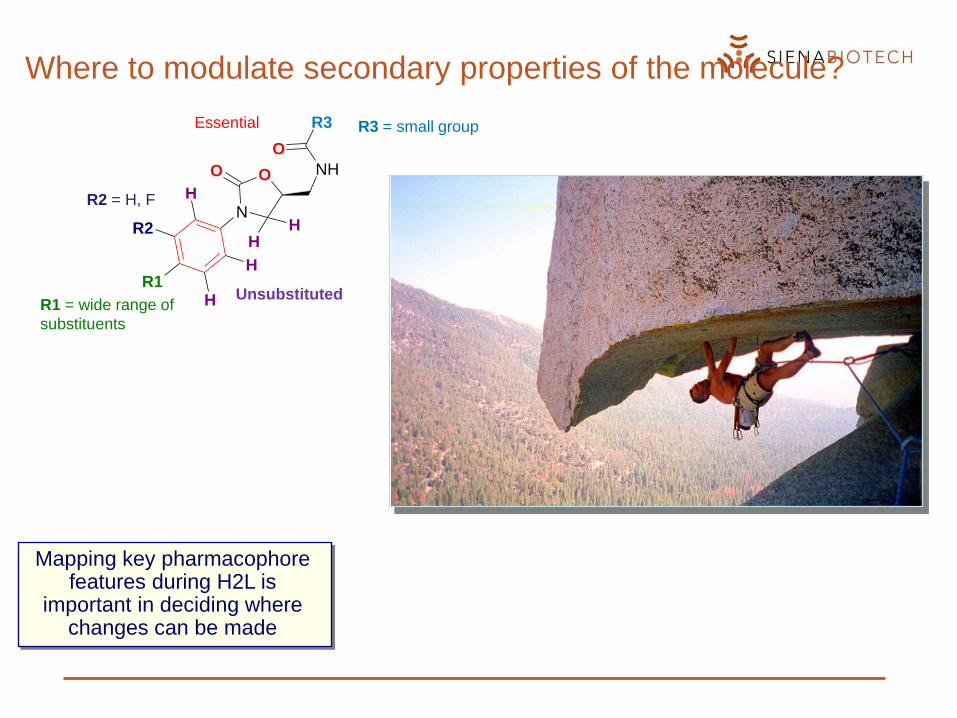
Where to modulate secondary properties of the molecule?
Mapping key pharmacophore features during H2L is
important in deciding where changes can be made
O
N
NHO
R3
O
R2
R1H
H
H
HH
R3 = small groupEssential
R1 = wide rangeof substituents
unsubstituted
R2 = H, F
R1 = wide range of
substituents
Unsubstituted
R3 = small groupEssential
R2 = H, F
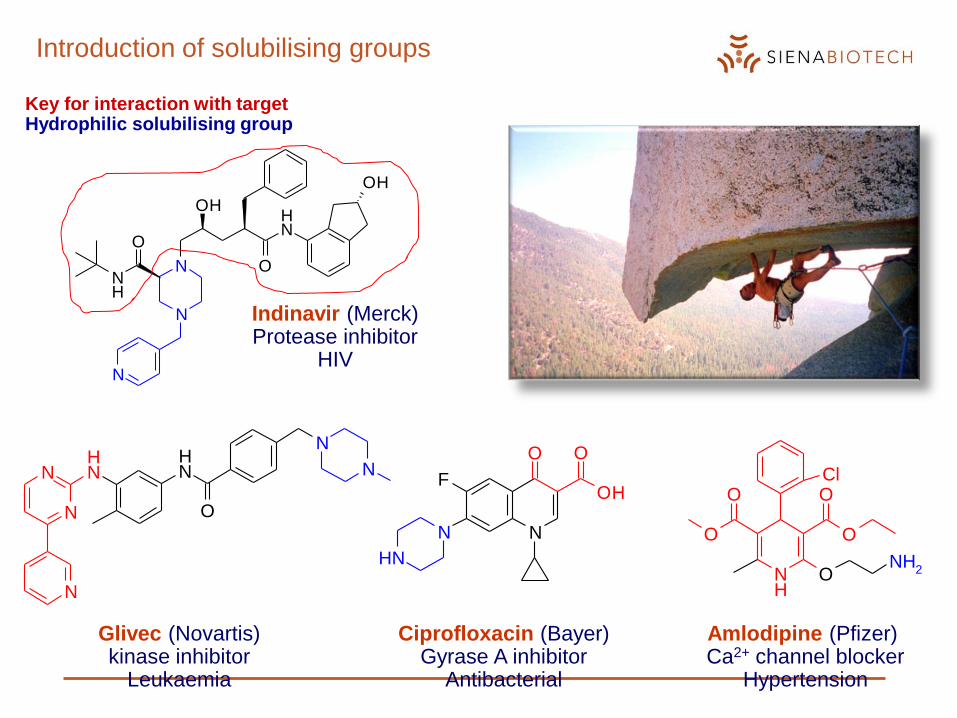
Introduction of solubilising groups
N
N NH
N
NH
O
N
N
Key for interaction with targetHydrophilic solubilising group
Glivec (Novartis)kinase inhibitor
Leukaemia
NN
O
OH
O
NH
F
NH
O
O O
O
ONH
2
Cl
Amlodipine (Pfizer)Ca2+ channel blocker
Hypertension
Indinavir (Merck)Protease inhibitor
HIV
N
N
N
NH
O
OH
O
NH
OH
Ciprofloxacin (Bayer)Gyrase A inhibitor
Antibacterial
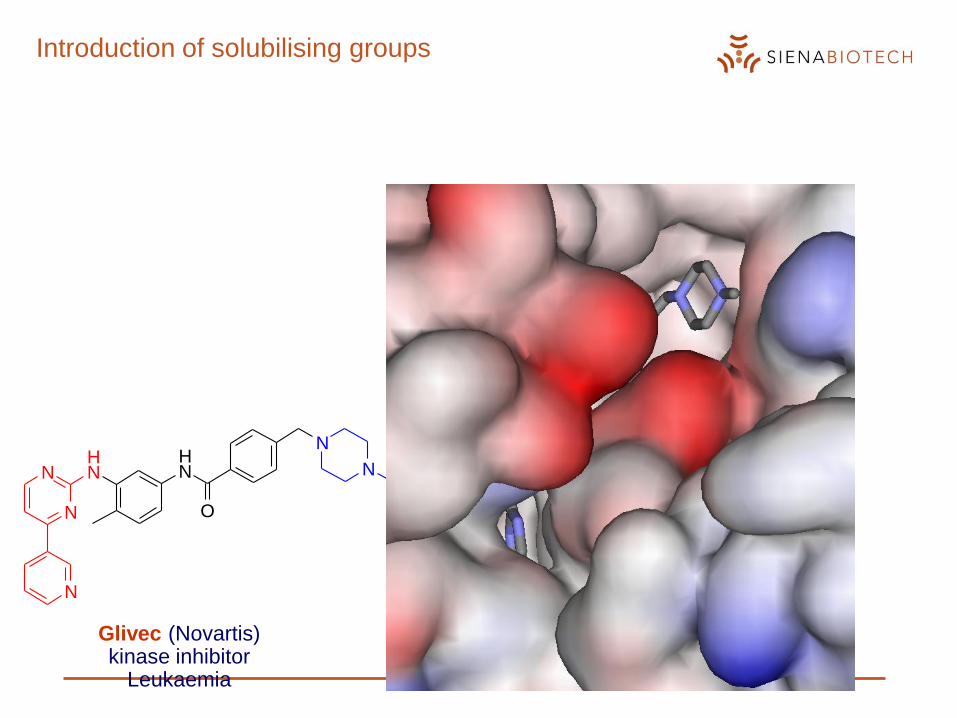
Introduction of solubilising groups
N
N NH
N
NH
O
N
N
Glivec (Novartis)kinase inhibitor
Leukaemia
Why do drugs still fail in development?
...and how optimising drug-like properties can help
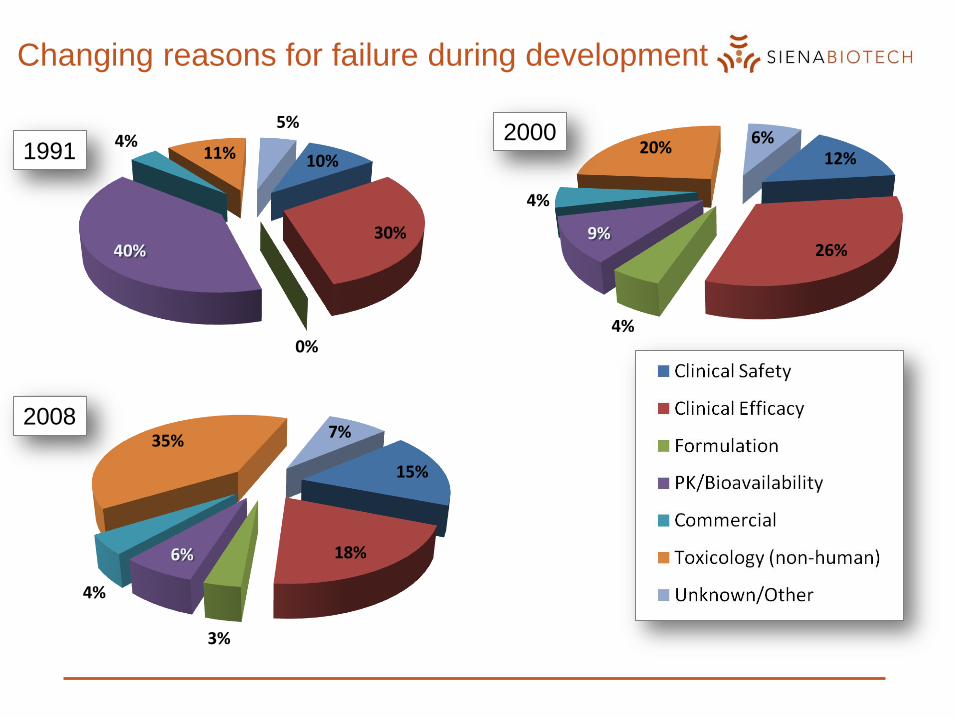
Changing reasons for failure during development
10%
30%
0%
40%
4%11%
5%
12%
26%
4%
9%
4%
20%6%
15%
18%
3%
6%
4%
35% 7%
19912000
2008
What are drug-like properties?
The compound has to dissolve, survive in and be absorbed from the
gastrointestinal tract before reaching the site of action
Poor GI absorption (oral bioavailability) will reduce the dose reaching the
target organ.
Higher initial doses required (compliance)
GI side-effects increase (e.g. antibacterials)
A goal of drug discovery is to maximise the oral bioavailability of
compounds as early in optimisation as possible.
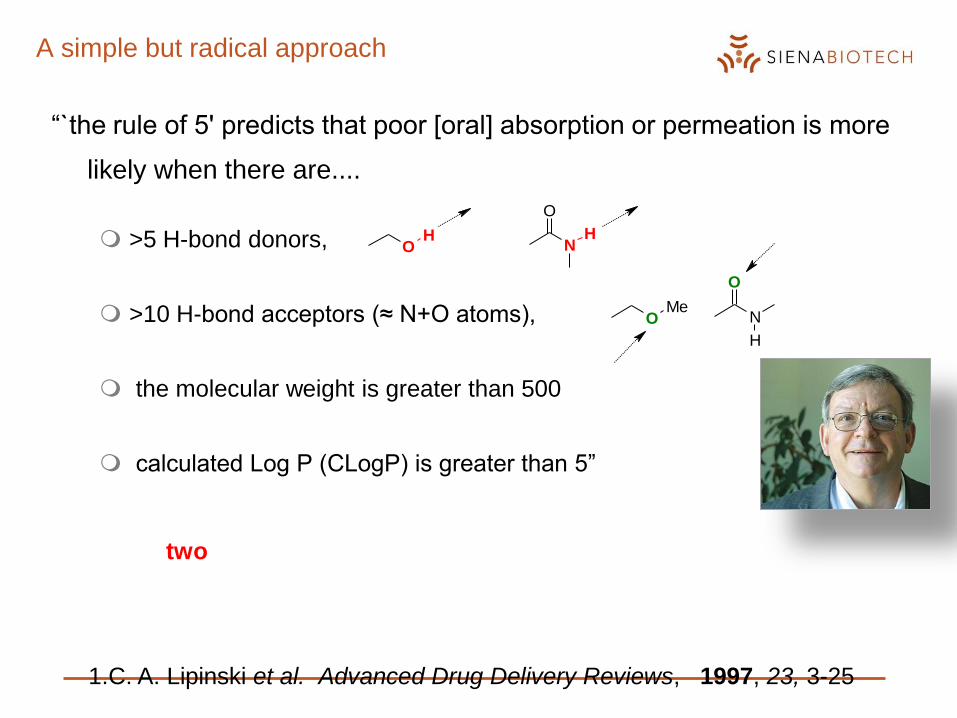
A simple but radical approach
“`the rule of 5' predicts that poor [oral] absorption or permeation is more
likely when there are....
>5 H-bond donors,
>10 H-bond acceptors (≈ N+O atoms),
the molecular weight is greater than 500
calculated Log P (CLogP) is greater than 5”
1.C. A. Lipinski et al. Advanced Drug Delivery Reviews, 1997, 23, 3-25
Breaking two of these rules is very likely to cause a major permeability problem
OH
N
O
H
OMe
N
O
H

Changing reasons for failure during development
10%
30%
0%
40%
4%11%
5%
15%
18%
3%
6%
4%
35% 7%
1991
2008
Significant reduction in failure due to PK/Bioavailability
Current challenges
toxicity/safety (side effects)
lack of efficacy
How can we improve the situation in Lead Optimisation?
Development failure due to lack of efficacy
If related to poor links between the biological target, in vitro assays
or in vivo models to the human disease there may be little that can
be done in this phase, especially for “first in class” projects
Evidence that some alleged development failures due to lack of
efficacy are actually due to safety problems
Toxicity/Safety - a complex subject with many potential causes
Modulating the biological target may cause unwanted/ unpredicted
side effects
• Potential for improved safety if cause is tissue selectivity
• For example increased/decreased brain penetration with a new
molecule
Lack of selectivity is a significant cause of toxicity/side effects
• Selectivity improvements through increased potency for target
• Selectivity through changes to physicochemical properties.
Summary
Lead optimisation is our last chance to find the best compound in
an active series
It’s not about in vitro potency
We must reduce dose required for efficacy
Improvements to ADME/PK through physicochemical property
improvements
We must increase concentration required for toxicity
Reduce toxicity liabilities through physicochemical property
improvements
We must deliver the molecule (plus backups) for rapid progression
to the clinic
No perceived major issues for large-scale synthesis,
pharmaceutical development etc.
Therapeutic
index or
Therapeutic
window
Design Criteria for candidate to clinical candidate

From candidate to clinical candidate – Overview
Objectives
• enable Phase I Clinical Trials through the filing of an IND/CTA
Goals and activities
• Pharmacology:
– confirm efficacy in relevant animal models
– define the Minimum Active Biological Expected Level (MABEL)
• Preclinical Development:
– define safety profile
– API process development and manufacturing
• Regulatory/Clinical:
– Regulatory documents preparation and submission (IB/IMPD)
– Clinical site selection and clinical protocol definition

Project
Milestones
API/
Pharm. Dev.
Toxicology
Clinical/
Regulatory
2007 2008 2009 2010
ADME/PK
Pharmacology
H2H1
FTIMCommit
to GLPLOIIND/CTA
Submitted
2011
H2H1 H2H1 H2H1 H2H1
R6/2
EnablingR6/2
Main StudyBiomarker Development and Validation
Other HD Models
1° Non-
GMP Lot
Process
ResearchPreformulation
1° GMP Lot 2nd GMP Lot
Clinical Supply
Regulatory Stability
DRFs28-Day
GLP
Safety
Pharma-
cology
Gene
Tox
Mini-
Ames
hERG
MTD
R6/2
Enabling
2° Species
Selection
Formulation DevelopmentAnalytical Package
Formulation Development
Clinical
Supply
Bioanalytical
Method Toxicokinetics
Orphan Designation
IMPD/CTA
Phase I
Subchronic Toxicology
Segment II + III
Phase IIa
Discipline interaction

From candidate to clinical candidate: Preclinical
Development
Safety profile definition:
• Preliminary (Non GLP) studies
• Regulatory (GLP) studies
Process development and pharmaceutics need to ensure GLP/GMP
quality standard for API used for preclinical/clinical studies
Regulatory guidelines very clearly defined
Design activities to support the proposed clinical program, delaying
non-critical studies until after cPoC
Current Industry benchmark: first GLP dose to FTIM in 7 months
Safety profile definition continues in parallel with Clinical
Development, timed to coincide with requirements of clinical program
up to the NDA/MAA filing

From candidate to clinical candidate: Interaction among
disciplines
Toxicology
Single and repeated dose,
Genotox, Reprotox, Local
tolerance, etc.
Safety Pharmacology
core battery studies (CNS, CV,
Resp), special studies.
ADME
Bioanalysis, (PK/TK),
protein binding,
biotransformation
Process Development &
Pharmaceutics
Formulation supply and
conc. checksQuality Assurance
Facility and Study Audits
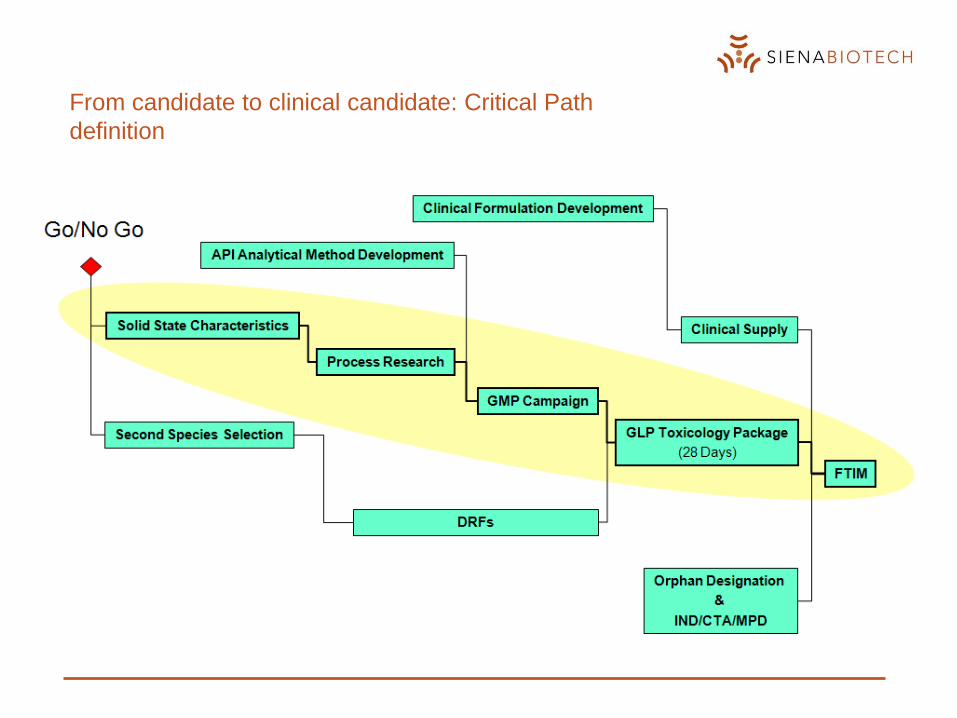
From candidate to clinical candidate: Critical Path
definition
From candidate to clinical candidate: Safety assessment (1)
Preliminary safety evaluation (non-GLP pakage)
ADME• Single dose PK (rodents and non rodents)
• Met profile invivo
Toxicology • Single/repeared dose DRF: in parallel (rat) or escalating (dog or monkey)
• Repeated MTD tox + TK (2wk), rat and dog or monkey
Safety Pharmacology• CV: cardiac panel, purkinjie fibers, isolated heart, single dose ECG, telemetry
• CNS: Irwin test/FOB – rat
Genotox studies• In vitro mutagenicity in bacteria – Miniames
• In vitro chorm abs in mammalian cells - COMET or µnucleous
09/02/2011
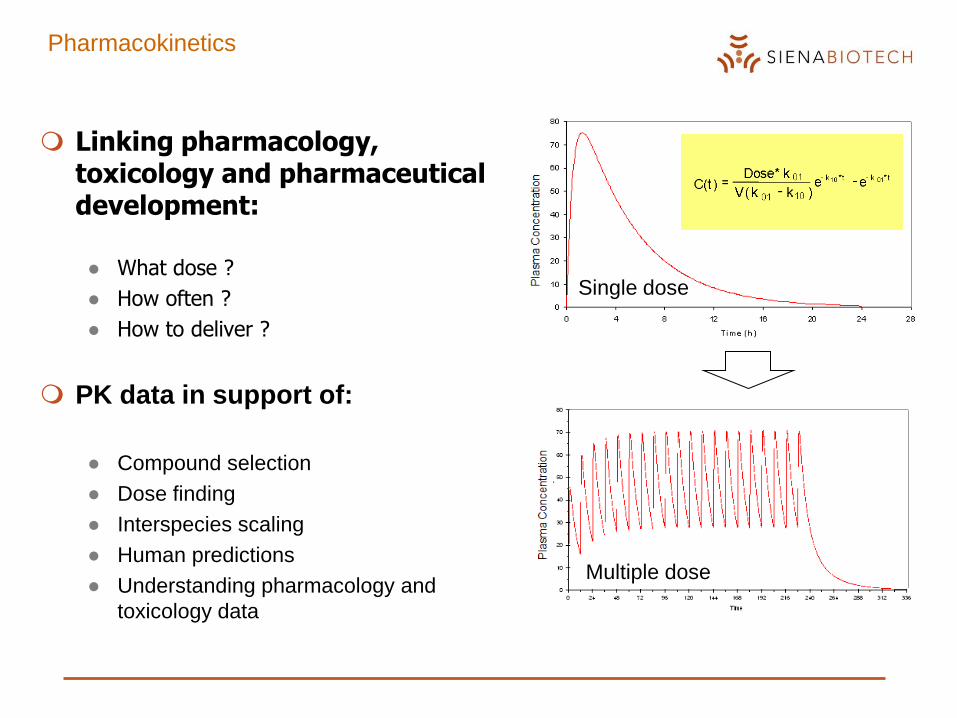
Pharmacokinetics
Single dose
Multiple dose
Linking pharmacology, toxicology and pharmaceutical development:
● What dose ?
● How often ?
● How to deliver ?
PK data in support of:
● Compound selection
● Dose finding
● Interspecies scaling
● Human predictions
● Understanding pharmacology and
toxicology data
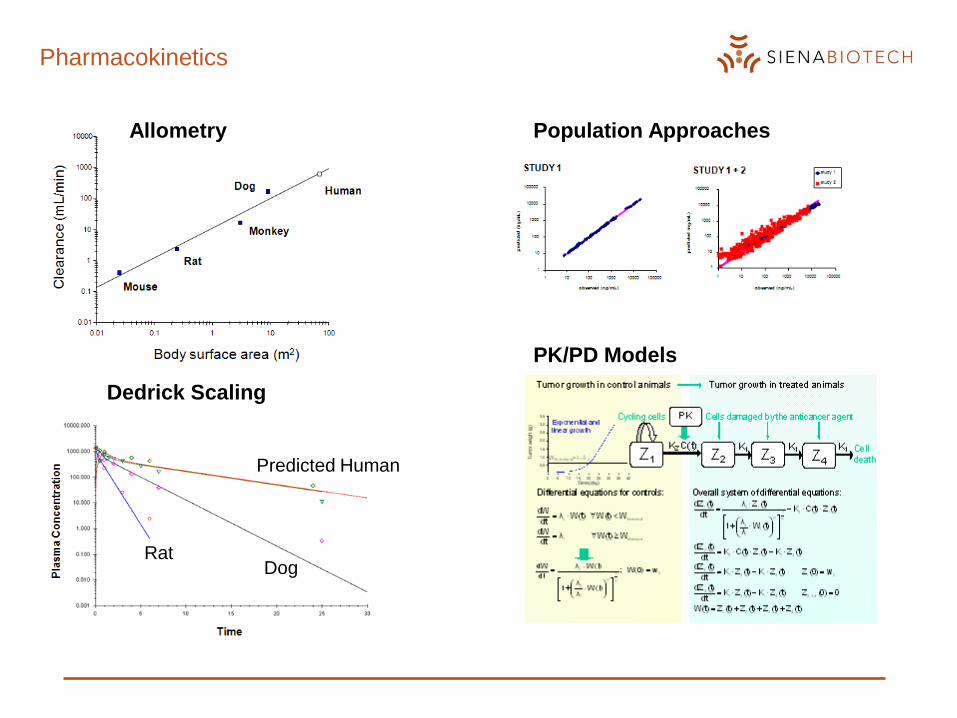
Pharmacokinetics
Dedrick Scaling
RatDog
Predicted Human
Allometry
PK/PD Models
Population Approaches
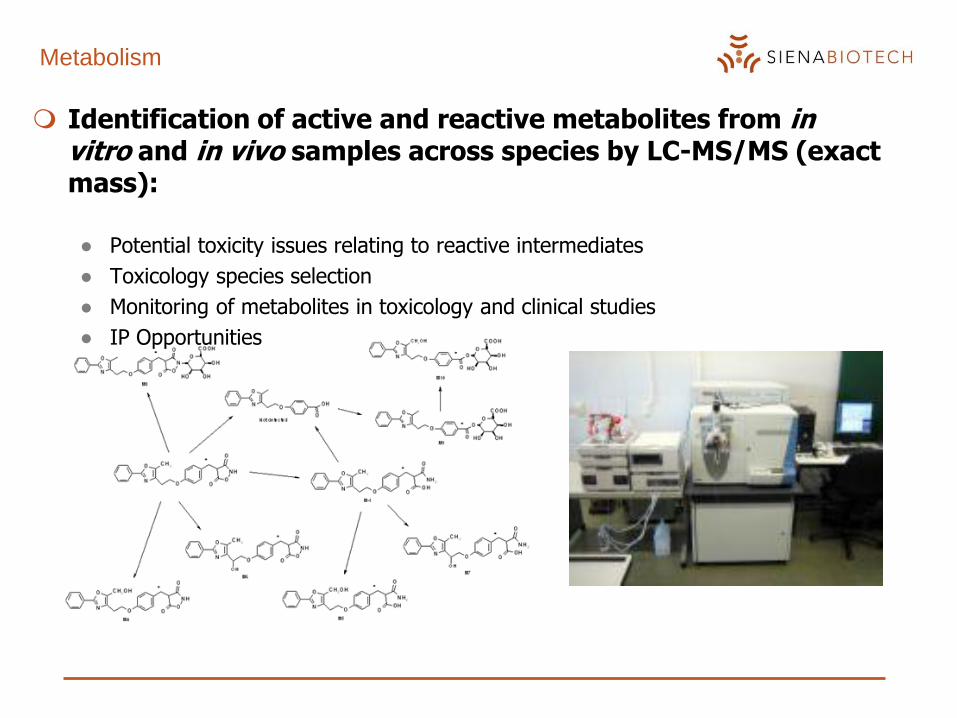
Metabolism
Identification of active and reactive metabolites from in vitro and in vivo samples across species by LC-MS/MS (exact mass):
● Potential toxicity issues relating to reactive intermediates
● Toxicology species selection
● Monitoring of metabolites in toxicology and clinical studies
● IP Opportunities
From candidate to clinical candidate: Safety assessment (2)
Regulatory safety evaluation (GLP pakage)
Toxicology – repeated dose studies
• Repeated dose + TK in rodents (mouse, rat)
• Repeated dose + TK in non rodents (dog, monkey, minipig)
Safety Pharmacology – single dose studies
• CV: telemetry (dog, monkey, ferret, guineapig)
• CNS: Irwin test /FOB (rat, mouse)
• Respiratory: Plethismographic system (rat, dog, monkey)
• Other studies based on specific issues (e.g. GI, kidney, etc.)
Genotox studies
• In vitro mutagenicity in bacteria – Ames
• In vitro chorm abs in mammalian cells – HPLA
• In vivo: rat µnucleous
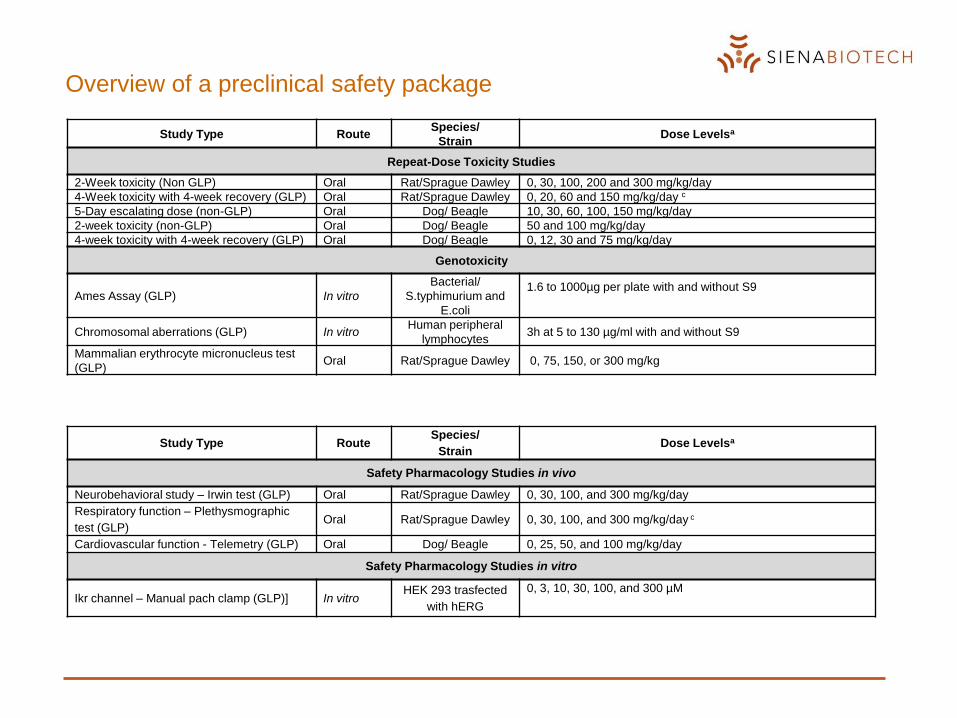
Study Type RouteSpecies/
StrainDose Levelsa
Repeat-Dose Toxicity Studies
2-Week toxicity (Non GLP) Oral Rat/Sprague Dawley 0, 30, 100, 200 and 300 mg/kg/day
4-Week toxicity with 4-week recovery (GLP) Oral Rat/Sprague Dawley 0, 20, 60 and 150 mg/kg/day c
5-Day escalating dose (non-GLP) Oral Dog/ Beagle 10, 30, 60, 100, 150 mg/kg/day
2-week toxicity (non-GLP) Oral Dog/ Beagle 50 and 100 mg/kg/day
4-week toxicity with 4-week recovery (GLP) Oral Dog/ Beagle 0, 12, 30 and 75 mg/kg/day
Genotoxicity
Ames Assay (GLP) In vitro
Bacterial/
S.typhimurium and
E.coli
1.6 to 1000µg per plate with and without S9
Chromosomal aberrations (GLP) In vitroHuman peripheral
lymphocytes3h at 5 to 130 µg/ml with and without S9
Mammalian erythrocyte micronucleus test
(GLP) Oral Rat/Sprague Dawley 0, 75, 150, or 300 mg/kg
Study Type RouteSpecies/
StrainDose Levelsa
Safety Pharmacology Studies in vivo
Neurobehavioral study – Irwin test (GLP) Oral Rat/Sprague Dawley 0, 30, 100, and 300 mg/kg/day
Respiratory function – Plethysmographic
test (GLP) Oral Rat/Sprague Dawley 0, 30, 100, and 300 mg/kg/day c
Cardiovascular function - Telemetry (GLP) Oral Dog/ Beagle 0, 25, 50, and 100 mg/kg/day
Safety Pharmacology Studies in vitro
Ikr channel – Manual pach clamp (GLP)] In vitroHEK 293 trasfected
with hERG
0, 3, 10, 30, 100, and 300 µM
Overview of a preclinical safety package

From candidate to clinical candidate: to do list (1)
Before GLP Tox pakage starting
explore toxicity in a broad dose range in vivo
define MTD and possible target organs
define PK profile at different dose levels and schedule (single and repeated)
identify relevant metabolites in vitro and in vivo in different species
define study design for Regulatory studies
• animal species
• dose level and schedule
• formulation schedule.
prepare GLP/GMP API batch for the following regulatory studies
set up and validate analitical and Bioanalitical methods
verify stability of API and dosing solutions
define API specs and release GLP/GMP batch(es)
From candidate to clinical candidate: to do list (2)
During GLP Tox pakage
investigate in deep the toxicity in a well defined (non lethal) dose range
• accomodation to toxic effects and/or recovery
• gender differences
• target organs and the reversibility of lesions
• systemic exposure
compare toxicity findings across species
define NOAEL /NOEL for each in vivo study
Identify potential risk for humans and possible monitoring strategies
confirm metabolite profile in vivo
prepare regulatory documents to support IND/CTA
select clinical site for Ph1 study and book study slot
prepare formulation for clinical use based on escalation rules
From candidate to clinical candidate: Decision to be
taken
At the end of preliminary Tox pakage
Evaluate the overall potential for harm on acute and repeated administration
Evaluate the relevance of lesions for humans
Identify unacceptable risks
Evaluate preliminary safety margins
Understand mechanism of toxicity and the possibility to monitoring tox effect in man
Decide whether or not progressing in the Regulatory phase
At the end of GLP Tox pakage
Confirm the overall safety profile of the compound
Confirm that changes are reversible and monitorable
Calculate the starting dose for clinical studies
Commit the beginning of clinical study and regulatory submission (IB/IMPD)
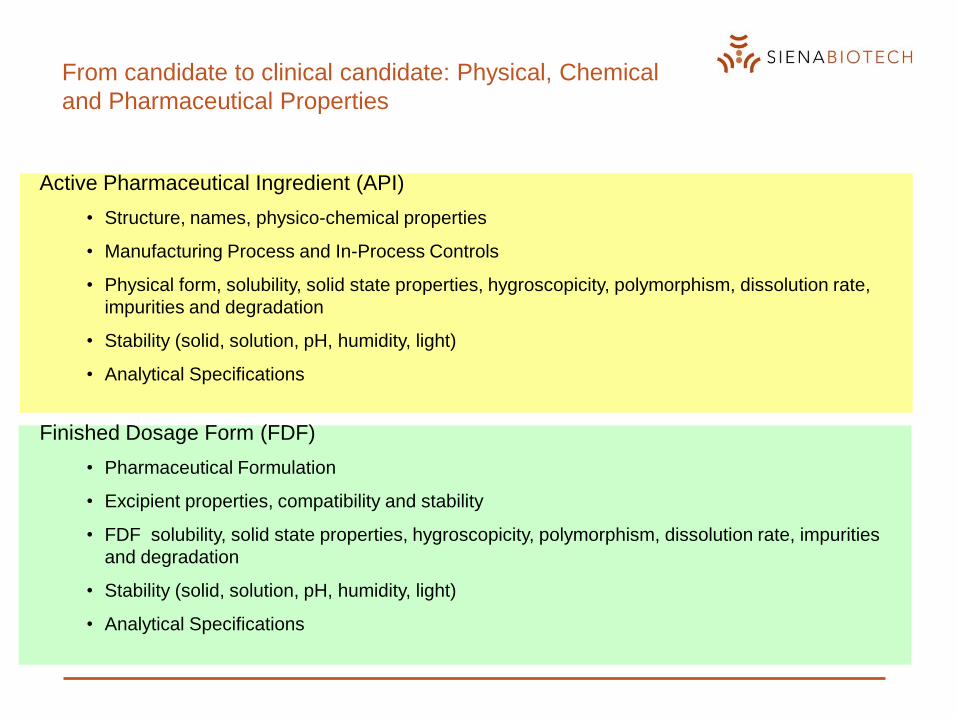
Active Pharmaceutical Ingredient (API)
• Structure, names, physico-chemical properties
• Manufacturing Process and In-Process Controls
• Physical form, solubility, solid state properties, hygroscopicity, polymorphism, dissolution rate,
impurities and degradation
• Stability (solid, solution, pH, humidity, light)
• Analytical Specifications
Finished Dosage Form (FDF)
• Pharmaceutical Formulation
• Excipient properties, compatibility and stability
• FDF solubility, solid state properties, hygroscopicity, polymorphism, dissolution rate, impurities
and degradation
• Stability (solid, solution, pH, humidity, light)
• Analytical Specifications
From candidate to clinical candidate: Physical, Chemical
and Pharmaceutical Properties
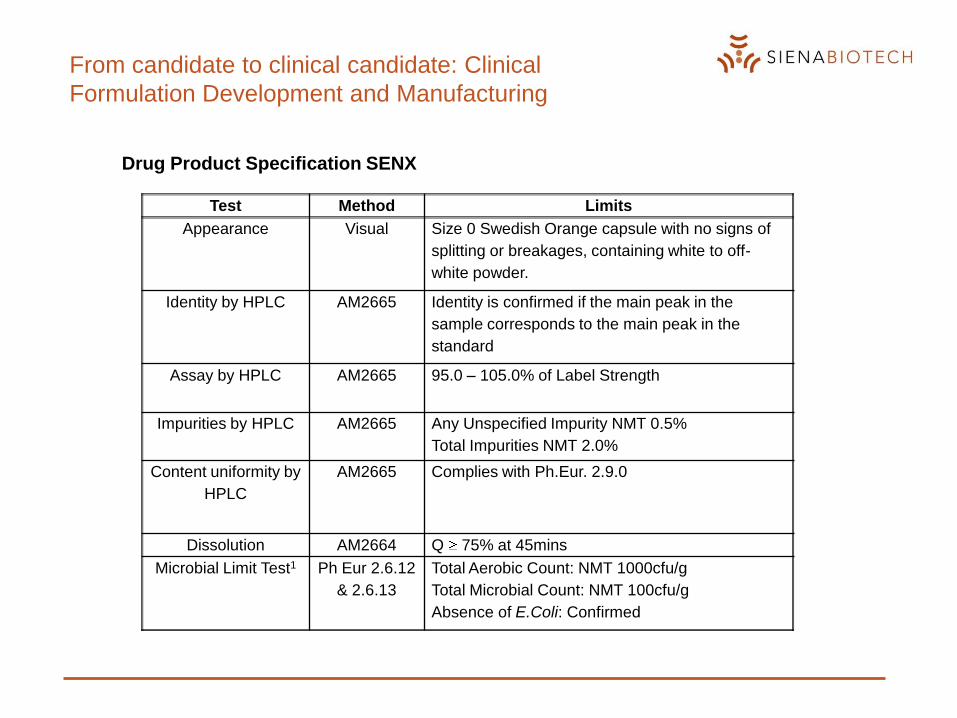
Drug Product Specification SENX
Test Method Limits
Appearance Visual Size 0 Swedish Orange capsule with no signs of
splitting or breakages, containing white to off-
white powder.
Identity by HPLC AM2665 Identity is confirmed if the main peak in the
sample corresponds to the main peak in the
standard
Assay by HPLC AM2665 95.0 – 105.0% of Label Strength
Impurities by HPLC AM2665 Any Unspecified Impurity NMT 0.5%
Total Impurities NMT 2.0%
Content uniformity by
HPLC
AM2665 Complies with Ph.Eur. 2.9.0
Dissolution AM2664 Q 75% at 45mins
Microbial Limit Test1 Ph Eur 2.6.12
& 2.6.13
Total Aerobic Count: NMT 1000cfu/g
Total Microbial Count: NMT 100cfu/g
Absence of E.Coli: Confirmed
From candidate to clinical candidate: Clinical
Formulation Development and Manufacturing
Clinical and Regulatory Development
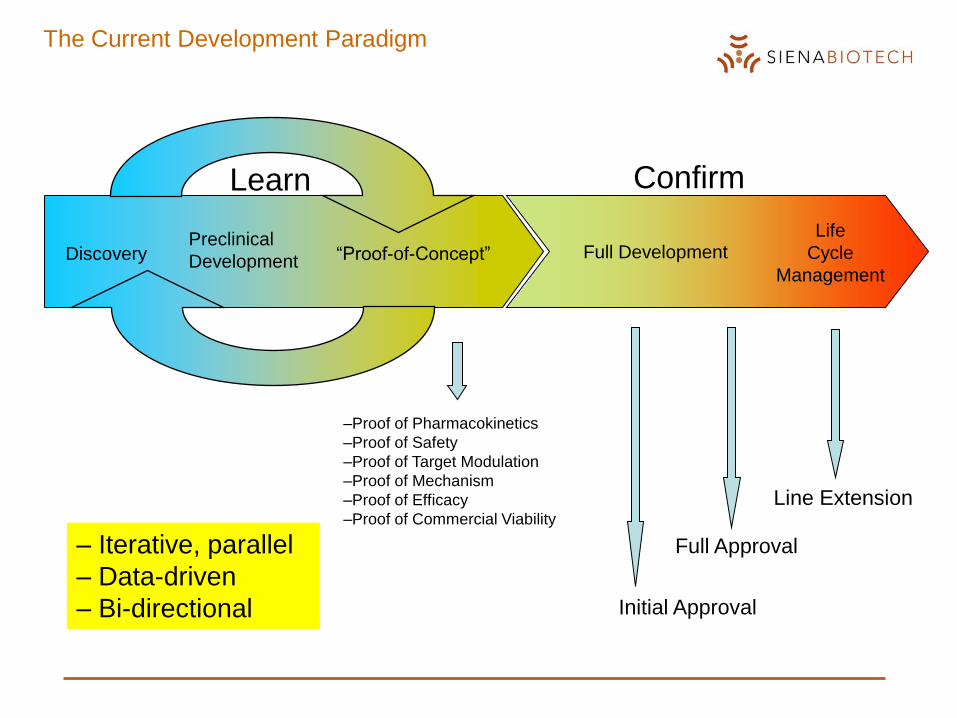
The Current Development Paradigm
Full DevelopmentLife
Cycle
Management
Initial Approval
DiscoveryPreclinical
Development “Proof-of-Concept”
Confirm
Full Approval
Line Extension
Learn
–Proof of Pharmacokinetics
–Proof of Safety
–Proof of Target Modulation
–Proof of Mechanism
–Proof of Efficacy
–Proof of Commercial Viability
– Iterative, parallel
– Data-driven
– Bi-directional
Clinical Development
– Clinical Development strives to achieve registration according to the TPP
– The Clinical Development process is strongly dependent on Health Authority
regulations
– Guidelines relating to clinical studies define minimal criteria for Manufacturing,
Pharmaceutical form, Preclinical Safety and Quality. Such activities are
conducted according to GxP:
o Good Clinical Practice (GCP)
o Good Manufacturing Practice (GMP)
o Good Laboratory Practice (GLP)
– Clinical studies for use in regulatory submissions need to have a defined study
design – typically, registrational studies are conducted with a double-blind,
placebo-controlled design
“Do only what is required to get to the next decision point”
– Process-driven rather than science-driven
– Clear definition of “need-to-have” vs. “nice-to-have” and decision trees
– Delay non-critical activities as far as possible
– Continuous focus on the critical path
– Guidelines aim to ascertain safety and ethics of clinical trials
– Guidelines establish minimal criteria for risk/benefit assessments
– Usually, competitor activities force Sponsors to conduct studies not required by
guidelines
– Guidelines enforced by regular Inspections, especially as regards manufacturing and
documentation
“Development
Mind-Set”
Regulatory Affairs and the Development Process

What is an Indication ?
– A drug can only be prescribed for the indication(s) for which it has been approved
– A drug is approved only for a specific indication(s), for which safety and efficacy data have
been collected
– “Indication” is a precise regulatory term, with a precise meaning and is NOT the same as
“disease”
Disease Indication
Small Cell Lung Cancer Second-line treatment of patients with locally advanced or metastatic non-small cell lung cancer after failure of both platinum-based and docetaxel chemotherapy.
Glioblastoma Multiformae First line treatment of adult patients with newly diagnosed glioblastoma multiforme concomitantly with radiotherapy and then as main-tenance treatment. Second-line treatment of adult patients with refractory anaplastic astro-cytoma, i.e. patients who have experienced disease progression on a drug regimen containing nitrosourea and procarbazine.
Depression Clinically manifest bipolar disorder as adjunctive to lithium or valproate in pediatric patients aged 10 to 17 years
What is a Label Claim ?
– The Label Claim comprises the Safety and Efficacy chapters of the TPP and forms the
basis for NDA/MAA approval
– A Label Claim is often written in the form of Clinical and Commercial Objectives, e.g.
“Compound X is indicated for the first-line treatment of Y, with efficacy not inferior to Gold
Standard, and associated with a frequency of adverse events lower than Gold Standard.”
– Approvable label claims are defined in dialogue with regulatory agencies and must be
reached to achieve registration
– Selection of label claims depends on data from exploratory clinical trials and positioning
vs. competitor products
– Each label claim has to be associated with a unique study
Clinical Development
Prior to Starting a Clinical Trial
1. Approved IND (US, Japan); CTA/IMPD (EU)
2. Local Ethics Committee Approval (IEC/IRB)
3. Signed Clinical Study Protocol
4. Clinical Site Defined (Academic ? CRO ? Investigators ?)
5. Import/Export Licenses
6. Clinical Supply and related documentation
IND: Investigational New Drug application
CTA: Clinical Trial Application
IMPD: Investigational Medical Product Dossier
IEC: Independent Ethical Committee
IRB: Institutional Review Board
CRO: Contract Research Organisation

Phase I
Clinical Phase I Studies
Study Population
Male and female healthy volunteers, 6+2 per cohort
Study Design
Randomized, double-blind single ascending dose (SAD) and
a multiple ascending dose (MAD) element with placebo control
Primary Objective
To determine the safety and tolerability
of single oral escalating doses of SEN0012345
Secondary Objectives
To determine the pharmacokinetic profile of single oral escalating doses of SEN0012345. To determine
expression of XXX in blood/plasma/urine/CSF/tumour/bone marrow
Primary Endpoints
– Safety (laboratory safety test results, telemetry and 12-lead ECG including QTc intervals, vital signs
and physical examination findings.
– Tolerability (type and frequency of adverse events)
Secondary Endpoints
Genotyping for expression of YYY, phenotyping of functional expression of YYY, food effects,
pharmacokinetic interactions etc
0 12 24 36 48
Time (h)
0.01
0.1
1
PH
A-6
83
42
5 C
on
ce
ntr
ati
on
(n
g/m
L)
P H A -683425 P las m a C onc en t ra t ion A f t e r 0 .5 m g P H A -690509 in f us ion (1 h )
1
23456
789101112
Not all “Phase I studies” are conducted during “Phase I”
– Food Interactions
Single dose level w/ and w/o standard meal to assess impact on absorption. Patients or volunteers.
– Thorough QT Study
Required in new ICH S7 guidelines if compounds demonstrates potential for QT prolongation, even if
no in-life findings in pre-clinical studies.
– Drug-drug Interactions
Required if compound demonstrates potential for DDIs at the levels of CYPs or transporters
– Impaired Renal Function
Required if drug is predominantly cleared via renal excretion.
– Impaired Hepatic Function
Required if drug is predominantly cleared via hepatic clearance.
– Bioequivalence Studies
Required if formulation has been changed and Sponsor wants to make use of “old” data. Can be
onerous and expensive.
Other Phase I Studies

“Phase II”
Proof-of-Concept
What is meant by cPoC ?
– May not be a single study, but the accumulated and integrated evidence from Discovery and early clinical
studies
Not an official term, no guidelines; represents what the Sponsor considers sufficient evidence to progress
to Full Development. Based on Pharmacokinetics, Safety, target modulation, MoA.......
– Phase IIa vs. IIb
Phase IIa often small, open-label studies aimed at establishing response in a relevant population. Read-
out based on a small set of clinical end-points and/or biomarkers. Phase IIb confirmatory studies with
double-blind design, often using the intended clinical end-point.
– Learn Process !
Both positive and negative data fed back to Discovery for back-up and/or second-generation compounds.
CONCLUSION
Preclinical drug development is a complex, long and risky
process
To achieve the success you may need:
Top science
A clear objective (product profile)
Accurate planning of activities
Integrated development competences
Financial resources
Customer focus
Capability to predict the market value of the drug
Luck