dr zainuri_embriologi dan topografi trac respiratorius
TRANSCRIPT

Tractus Respiratorius
dr. Zainuri Sabta Dep. Anatomi FK UII


Paranasal Sinuses
• Four bones of the skull contain paired air spaces called the paranasal sinuses - frontal, ethmoidal, sphenoidal, maxillary
• Decrease skull bone weight• Warm, moisten and filter incoming air • Add resonance to voice.• Communicate with the nasal cavity by
ducts.• Lined by pseudostratified ciliated
columnar epithelium.
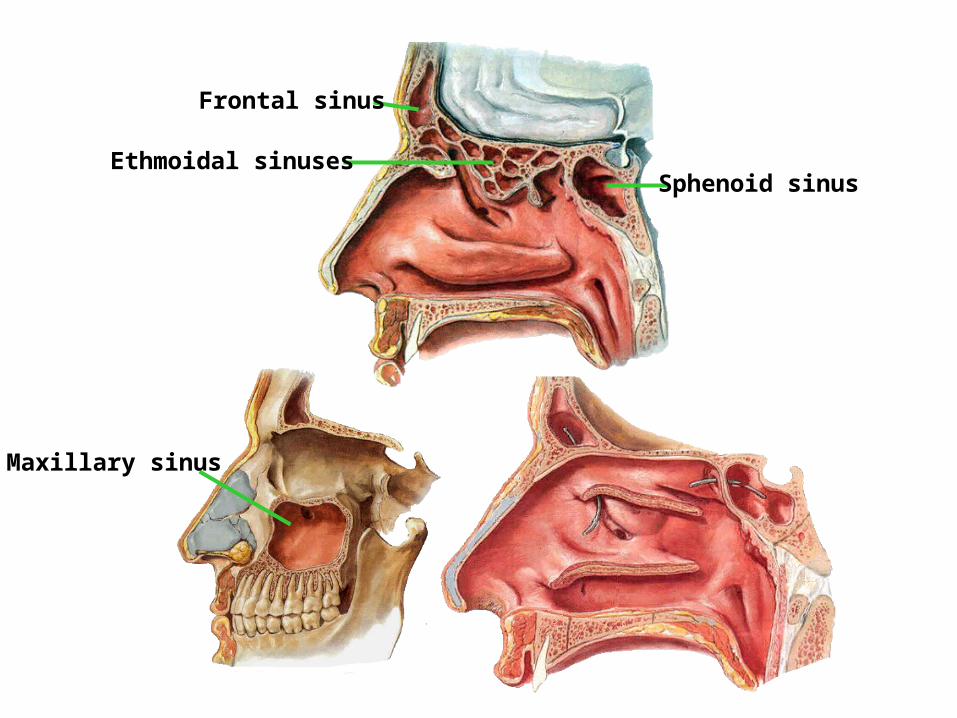
Frontal sinus
Ethmoidal sinusesSphenoid sinus
Maxillary sinus





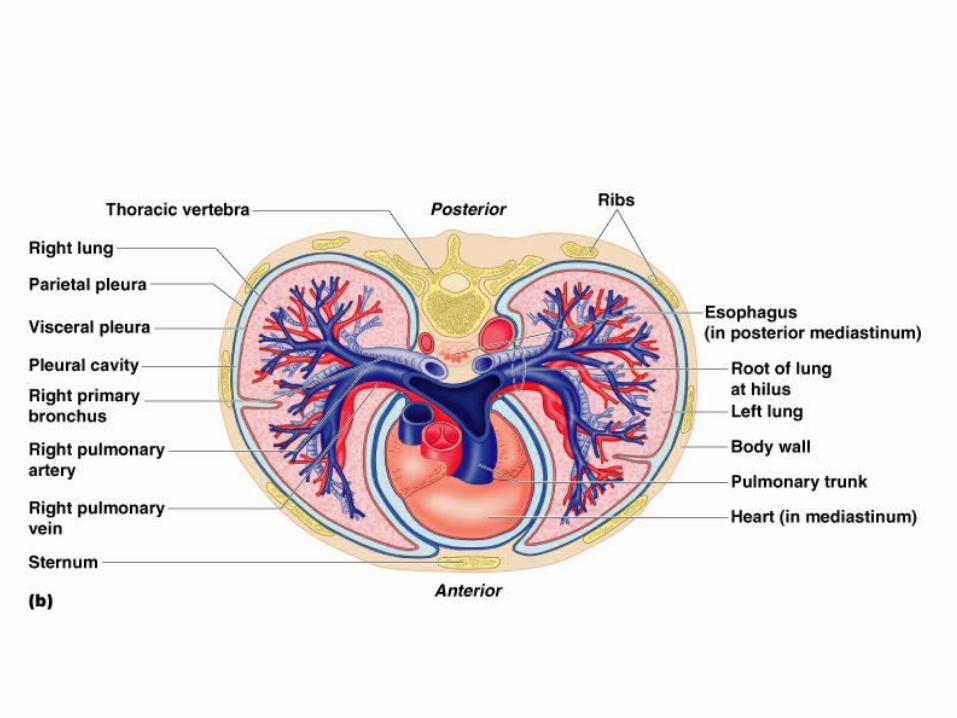
Right and Left Pleural Cavities Parietal Pleura Visceral (Pulmonary) Pleura Parietal
Costal Mediastinal Diaphragmatic Cupola
Connecting Pleura







Proyeksi external paru
Lungs
Light, soft, spongy Conical in shape, apex, base, costal
surface, medial surface, hilus. Note various impressions
Right lung Three lobes; superior, middle and inferior Oblique and horizontal fissure
Left Lung Two lobes; superior and inferior also Lingula
and Cardiac notch, horizontal fissure

Struktur yang keluar/masuk hilus pulmonis:
1.Bronchi2.a. & v. pulmonalis3.a. & v. bronchialis4.Vasa dan nodi lymphatici5.nervus

• Lungs formed by progressive branching, first 16 generations of airways = conducting zone, generations 16-23 = gas exchange zone
• 300 million alveoli (0.3 mm in diameter), total surface area 85 m2, 0.4 m2 if lung a sphere
• Change in intrathoracic pressure moves air inspiratory muscles (diaphragm, external intercostals, accessory = SCM, scalene) ↑ size of thorax ↓ intrathoracic pressure relative to atmospheric pressure bulk flow into airways (flow = pressure gradient / resistance)


Inervasi diaphargma



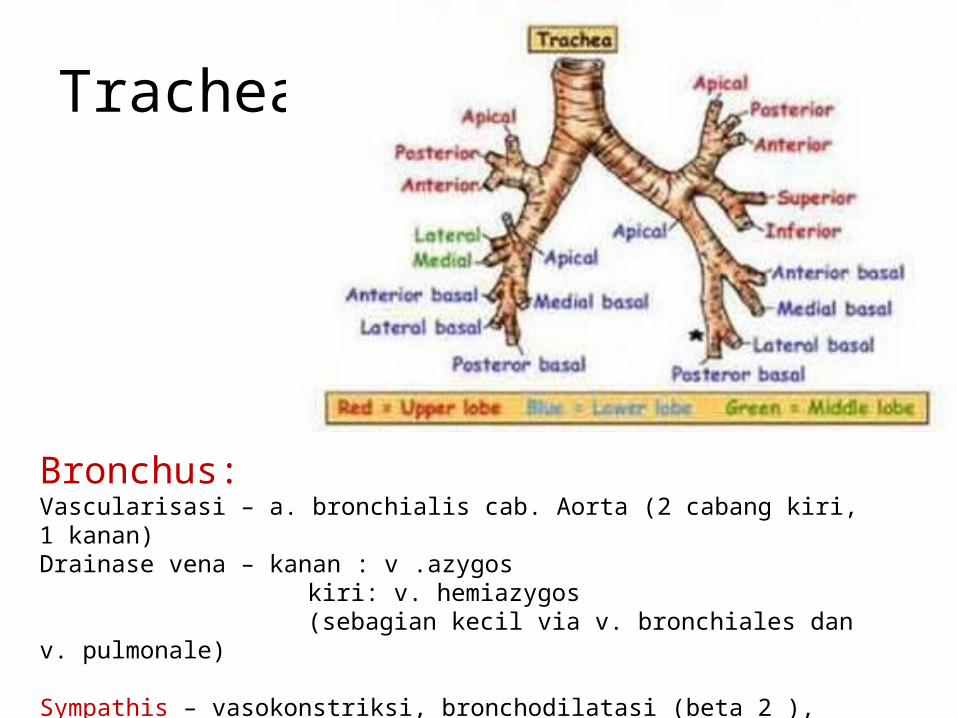
Trachea
Bronchus:Vascularisasi – a. bronchialis cab. Aorta (2 cabang kiri, 1 kanan)Drainase vena – kanan : v .azygos
kiri: v. hemiazygos (sebagian kecil via v. bronchiales dan v. pulmonale)
Sympathis – vasokonstriksi, bronchodilatasi (beta 2 ), supresi sekresi kelenjar (alpha)Parasympathis – vasodilatasi, bronchokonstriksi, peningkatan sekresi kelenjar , sensasi
Lungs have large surface area & thin membrane for gas exchange, formed by progressive branching (vascular and air spaces brought close together), first 16 generations of airways = conducting zone, generations 16-23 = gas exchange zone
300 million alveoli (0.3 mm in diameter), total surface area 85 m2, 0.4 m2 if lung a sphere
Change in intrathoracic pressure moves air inspiratory muscles (diaphragm, external intercostals, accessory = SCM, scalene) ↑ size of thorax ↓ intrathoracic pressure relative to atmospheric pressure bulk flow into airways (flow = pressure gradient / resistance)

Airways
• Trachea, primary bronchi, secondary bronchi, tertiary bronchi out to 25 generations
• All comprised of hyaline cartilage• Trachea
– Begins where larynx ends (about C6)– 10 cm long, half in neck, half in mediastinum– 20 U-Shaped rings of hyaline cartilage – keeps lumen
intact but not as brittle as bone– Lined with epithelium and cilia which work to keep foreign
bodies/irritants away from lungs

Airways
• Primary Brochi– One to each lung – continuation of trachea– Right bronchus is wider and shorter 2.5 cm as opposed to
5 cm and branches from the trachea at a greater angle• Secondary bronchi – one to each lobe, three in right,
two in left• Tertiary – one to each bronchopulmonary segment –
approximately 10 per lung• All of the above are hyaline cartilage with no ability
to change diameter
Bronchioles
• First level of airway surrounded by smooth muscle; therefore can change diameter as in brocho-constriction and broncho-dilation
• Bronchioles Terminal• Bronchioles Respiratory
– 3-8 orders
• alveoli


36
Conducting zone vs. respiratory zone

37
Conducting zone functions
Regulation of air flowtrachea & bronchi held open by cartilaginous ringssmooth muscle in walls of bronchioles & alveolar ductssympathetic NS & epinephrine relaxation ( receptors) air flowleukotrienes
(inflammation & allergens leukotrienes mucus & constriction)
Protectionmucus escalator (goblet cells in bronchioles & ciliated epithelium)inhibited by cigarette smoke
Warming & humidifying inspired airexpired air is 37 & 100% humidity (loss of ~400 ml pure water/day)
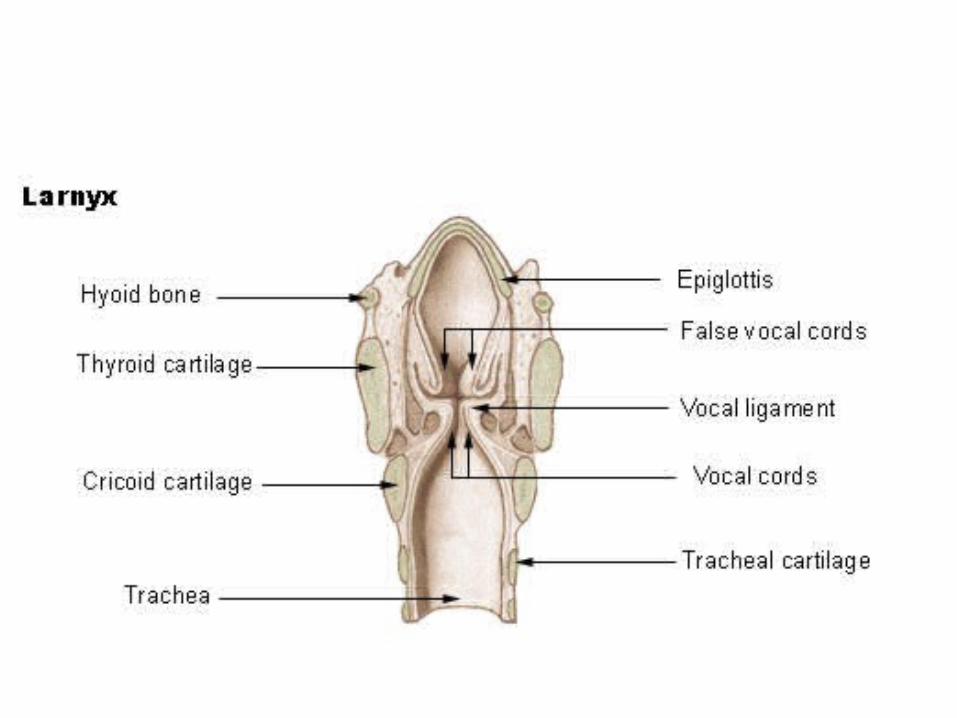
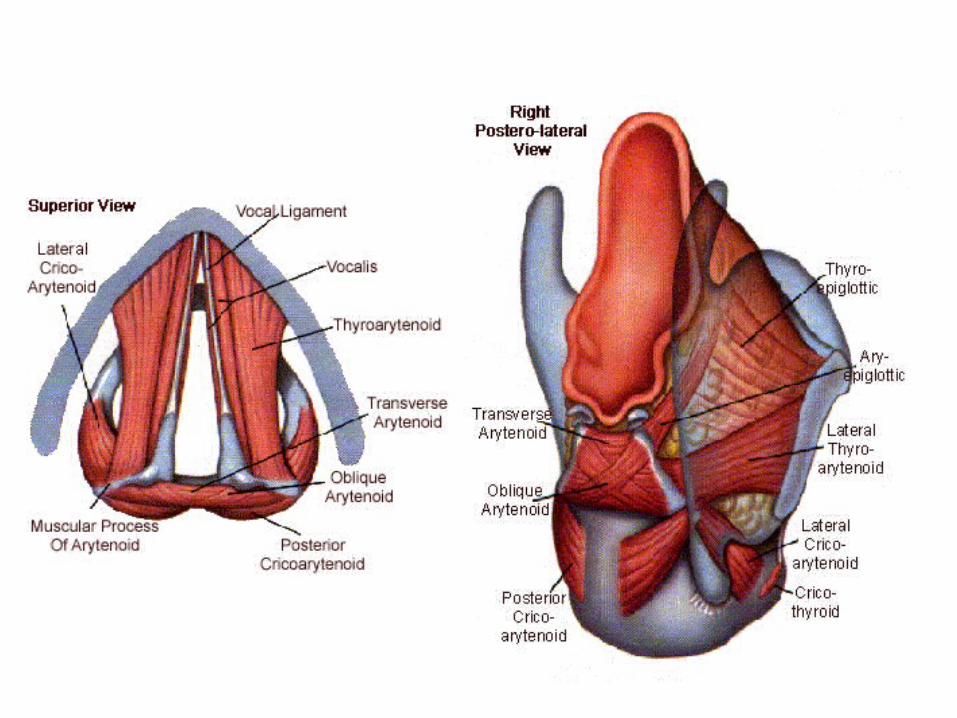
Phonationlarynx & vocal cords

Alveolar structure 2
Pulmonary capillariescompletely surround each alveolus; “sheet” of blood
Interstitial space diffusion distance for O2 & CO2 is less than diameter of red blood cell
Elastic fiberssecreted by fibroblasts into pulmonary interstitial spacetend to collapse lung

39
Alveolar structure 3
Type I epithelial cellsthin, flat; gas exchange
Type II epithelial cellssecrete pulmonary surfactant pulmonary compliance (later)
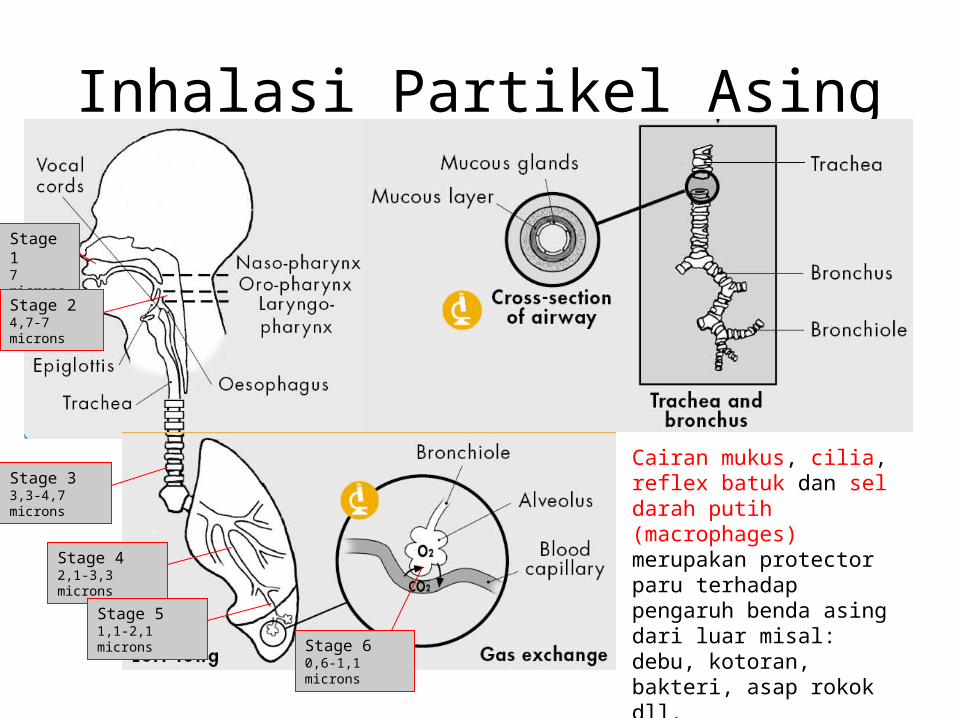
Inhalasi Partikel Asing
Stage 17 microns & above
Stage 24,7-7 microns
Stage 33,3-4,7 microns
Stage 42,1-3,3 microns
Stage 51,1-2,1 microns
Stage 60,6-1,1 microns
Cairan mukus, cilia, reflex batuk dan sel darah putih (macrophages) merupakan protector paru terhadap pengaruh benda asing dari luar misal: debu, kotoran, bakteri, asap rokok dll.
Besar-kecilnya dampak partikel yang masuk paru bergantung pada sejumlah faktor:•konsentrasi partikel di udara dengan diameter kurang dari 10 mikron,•frekuensi dan lama pemaparan, •kandungan partikel, •cuaca, dan•kondisi kesehatan seseorang.

EFEK TERHADAP KESEHATAN
Inhalasi debu mineral secara umum disebut Pneumoconiosis.
Silicosis adalah penyakit paru akibat inhalasi debu yang mengandung cristal silica (alpha-quartz or silicon dioxide), atau silica tipe polymorphs (tridymite or cristobalite), yang secara alami terdapat pada dan memiliki toksisitas sangat tinggi terhadap paru.Gejala silikosis umumnya muncul beberapa tahun setelah terkena paparan. Sebagai contoh pekerja terpapar silica selama 30 tahun, dimana terjadi fibrosisasi jaringan paru hebat.

EFEK TERHADAP KESEHATAN
Mekanisme Kerusakan paru
Partikel < 1 mikron
Permukaan partikel merangsang terbentuknya radikal bebas (hydroxyl, hydrogen peroxide, and other oxygen radicals)
Terjadi kerusakan membran sel epitel alveoli melalui mekanisme peroksidasi lipid dan dan inaktivasi protein esensial sel
Macrophag alveoli memakan partikel, teraktivasi dan merangsang pengeluaran cytokines, termasuk tumor necrosis factor, interleukin-1, and leukotriene B-4, dan terjadilah proses radang (inflamasi) yang menyebabkan kerusakan sel dan matrik alveoli. Pada tahap selanjutnya merubah growth factor–alpha induces proliferation of type 2 pneumocytes, and other cytokines (eg, platelet-derived growth factor, insulin - like growth factor) dan merangsang sel fibroblas berproliferasi memproduksi collagen dan akhirnya terjadi fibrosis paru.

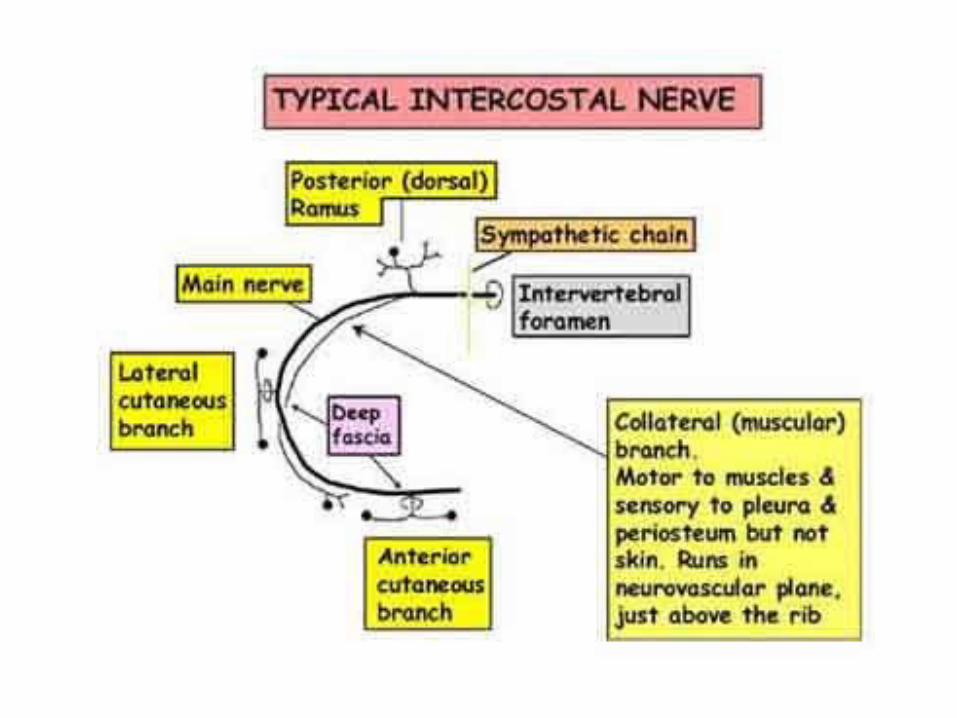
Innervation
• Pleura via intercostal (thoracic) nerves• Tracheobronchial tree• Parasympathetic via CN X efferent function =
broncho-constriction via smooth mm., also to epithelial cells in trachea; afferent = responsible for cough reflex
• Sympathetic from T1-T5 efferent = brocho-dilation

Blood Supply
• Lungs do not receive any vascular supply from the pulmonary vessels (pulmonary aa. Or veins)
• Blood delivered to lung tissue via the bronchiole arteries
• Vessels evolve from aortic arch• Travel along the bronchial tree

Pharyngeal Arches (Brachial Arches)
• General:– develop during 4th week of gestation– lateral swellings on either side of head; result from
local proliferation of NCC – give rise to specific cartilages and bones– pharyngeal grooves—external delineations between
brachial arches; ectoderm covered– pharyngeal pouches—internal deliniation between
brachial arches; endoderm lined– closing membranes—ectoderm/endoderm contact
points ensuring non-mixing between brachial arches

• Aortic Arch Arteries– blood vessel development follows path of least resistance
(thru mesenchyme) => many run through brachial arches during early embryogenesis
• Cranial Nerves—each is associated with a specific pharyngeal arch & innervates all its muscles, etc
• Muscles—each pharyngeal arch differentiates into a specific set of muscles which are innervated by the CN in that arch

Pharyngeal ArchesArch Artery Nerve Skeletal Elements Muscles
1 MaxillaryV(V2 & V3
only)
(NCCs) Maxilla, mandible, zygomatic portions of temporal,
mm. of mastication (temporalis, masseter, pterygoids) myelohyoid,
ant. belly of digastric, tensor tympani, & veli palatini
2Stapedial
(practically degenerates)
VII(NCCs) Stapes, styloid process, part of hyoid
muscles of facial expression, post. belly of digastric, stylohyoid,
stapedius
3 Carotid IX (NCCs) Part of hyoid Stylopharyngeus
4
Right: subclavian, Left: arch of
the aorta
X (superior laryngeal
br)
(LPM) Laryngeal cartilages
Cricothyroid, levator veli palatine, pharynx constrictors
5 - - - -
6 Pulmonary
X (recurrent laryngeal
br)
(LPM) Laryngeal cartilages
Intrinsic larynx mm.
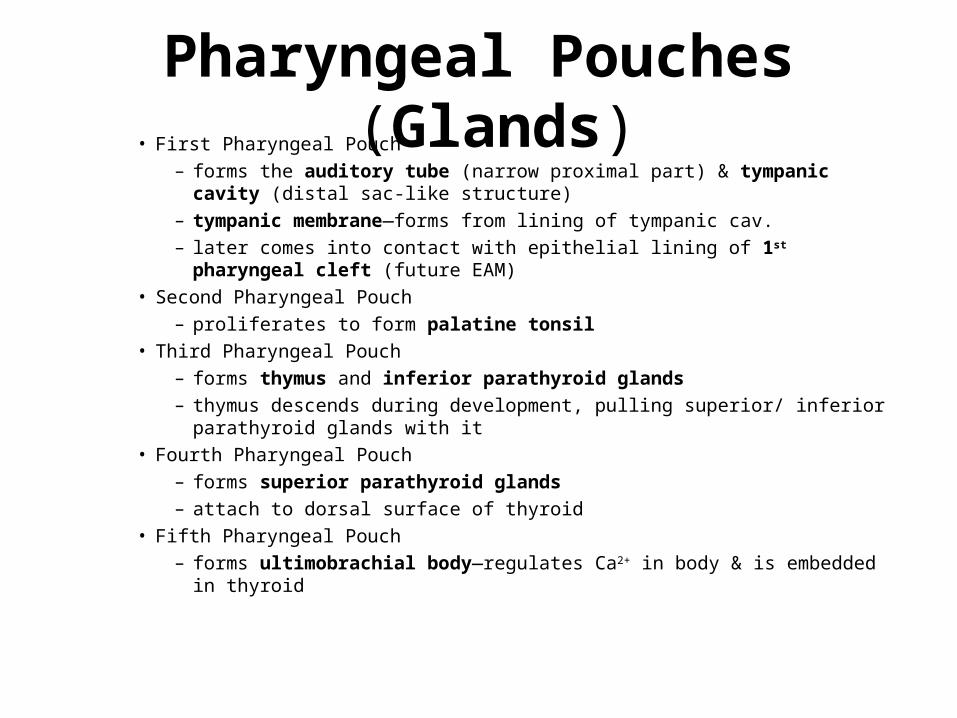
Pharyngeal Pouches (Glands)• First Pharyngeal Pouch
– forms the auditory tube (narrow proximal part) & tympanic cavity (distal sac-like structure)
– tympanic membrane—forms from lining of tympanic cav. – later comes into contact with epithelial lining of 1st pharyngeal cleft (future EAM)
• Second Pharyngeal Pouch– proliferates to form palatine tonsil
• Third Pharyngeal Pouch– forms thymus and inferior parathyroid glands– thymus descends during development, pulling superior/ inferior parathyroid glands
with it• Fourth Pharyngeal Pouch
– forms superior parathyroid glands– attach to dorsal surface of thyroid
• Fifth Pharyngeal Pouch– forms ultimobrachial body—regulates Ca2+ in body & is embedded in thyroid

– Pharyngeal Grooves (Clefts) • four recognizable clefts; all but one disappear during
development• 1st pharyngeal cleft external auditory meatus (EAM)
& part of tympanic membrane• 2nd pharangeal arch mesenchyme proliferates
overlapping arch that covers 2-4th pharangeal clefts smooth neck
• cervical sinus—temporary cavity formed during development; closes later during development
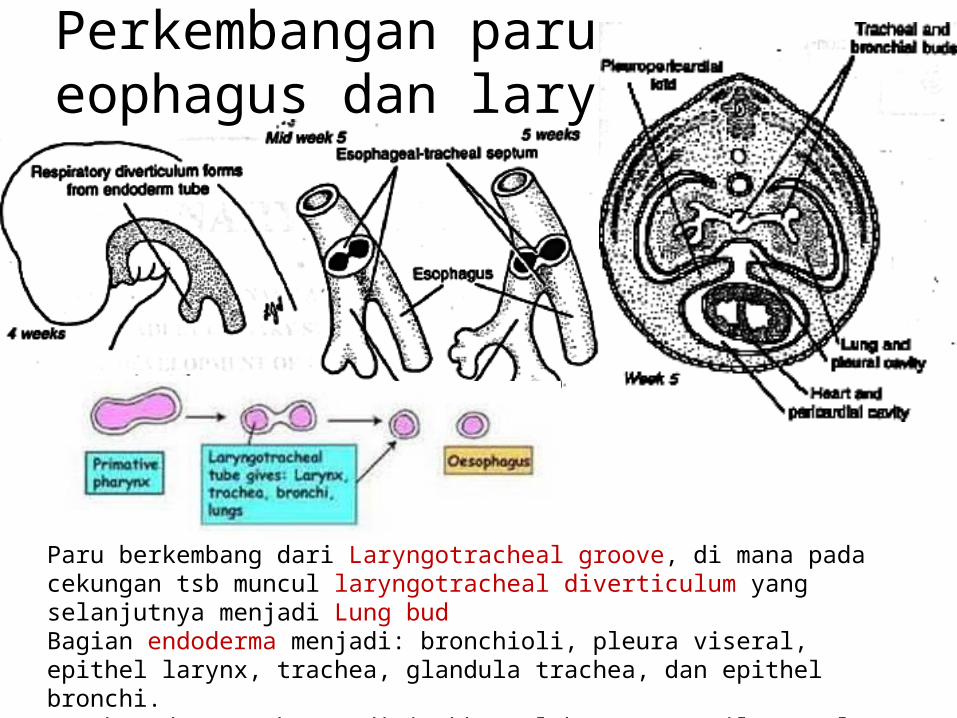
Perkembangan paru, eophagus dan larynx
Paru berkembang dari Laryngotracheal groove, di mana pada cekungan tsb muncul laryngotracheal diverticulum yang selanjutnya menjadi Lung budBagian endoderma menjadi: bronchioli, pleura viseral, epithel larynx, trachea, glandula trachea, dan epithel bronchi.Trachea dan esophagus dipisahkan oleh septum. Bila gagal memisah akan membentuk fistula.

Kejadian Pulmo

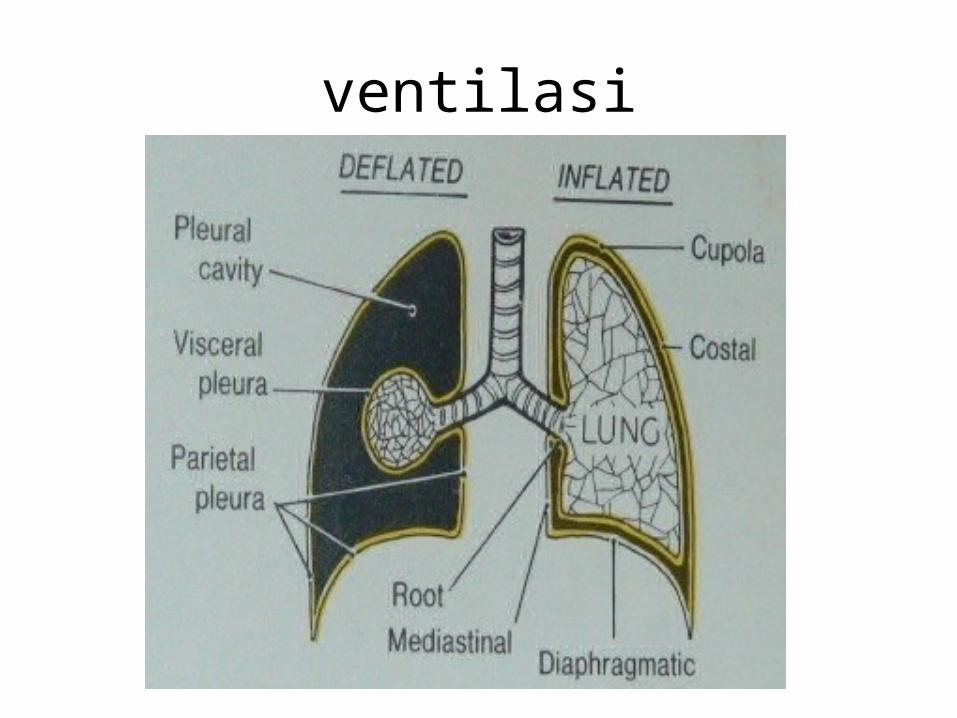
ventilasi
• Obstructive lung disease = problem w/ airflow function of lung asthma, emphysema,chronic bronchitis, cystic fibrosis
• Restrictive lung disease = problem w/ gas exchange function of lung pulmonary fibrosis,pulmonary alveolar proteinosis
• Bronchi / bronchioles have minimal effect on airflow obstruction (but contribution to COPD via enlargement of bronchial mucus glands, ↑ goblet cells, airway smooth muscle hypertrophy
• Respiratory bronchioles major cause of obstruction macrophage inflammation, mucus plugs, loss of alveolar attachments (less alveolar septae tugging on airways and keeping them open distorted / collapsed bronchioles)

• Emphysema protease imbalance destruction of alveolar tissue loss of elastic recoil hyperinflation flattening diaphragm (↑ effort) dyspnea
• Dyspnea inactivity deconditioning dyspnea inactivity deconditioning disability
• Airflow limitation during exercise no ventilatory reserve, ↑ flow only by breathing at higher volumes dynamic hyperinflation; ↑RR ↓ time to exhale hyperinflation SOB

• Emphysema– Abnormal permanent enlargement of alveolar spaces distal to
terminal bronchiole w/ wall destruction, enlargement of alveoli (overinflation)
– Centrilobular – involves respiratory bronchiles, upper lobes more involved, found inassociation w/ CB and smoking, spherical holes 1-5 mm near center of lobu
– Panlobular – all portions of lobule affected but usually alveolar ducts, both upper/lower lobes
– involved, usually in middle-aged smokers or young pt. w/ ↓antitrypsin (cotton candy lung)
• Pleuritis – painful inflammation, usually w/ viral infections, also w/ bacteria, TB, PE, tumors
• Pneumothorax – can have pleuritic pain as well, but dyspnea most common hyperresonant lung to percussion + ↓ breath sounds
• Examine pleural fluid to determine transudate or exudate (caused by infection, tumor, PE + infarct, collagen vascular disease, trauma, esophageal rupture, pancreatitis, abscess, ascites, asbestos, chylothorax, hypersensitivity)
• Exudate – damage to pleura, leakage of plasma (protein, RBC, WBC) into pleural space, meets following criteria – fluid protein / serum protein > 0.5, fluid LDH / serum LDH > 0.6, pleural fluid LDH > 2/3 of plasma (200 IU) continuum from pure transudate to exudates
• Empyema – pus in pleural space, lots of PMN, seen w/ pneumonia (esp. anaerobic), occasionally seen w/ trauma, rarely w/ surgery
• Hemothorax – blood in pleural space, due to trauma excessive blood loss hypotension
• Chylothorax – lymph fluid (milky) in pleural space, due to poor lymphatic drainage (blockage), can be due to congenital atresia of thoracic duct, trauma from esophageal surgery, or tumor
• Pneumothorax – injured chest wall (i.e. penetrating wounds, rib fracture), also due to insertion of central line, IJV or subclavian catheter, chest surgery, positive pressure ventilation air leaks in; spontaneous pneumothorax (primary – no predisposition,

Pneumothorax – injured chest wall (i.e. penetrating wounds, rib fracture), also due to insertion of central line, IJV or subclavian catheter, chest surgery, positive pressure ventilation air leaks in; spontaneous pneumothorax (primary – no predisposition,
