dr harald böhm oth di h ti florthopaedic hospital for ... · oth di h ti florthopaedic hospital...
TRANSCRIPT

Muscles structure andMuscles structure and function in children with cerebral palsy
Dr Harald BöhmDr Harald Böhm
O th di H it l fOrthopaedic Hospital forChildren, Aschau
Germany

Agendag
• Clinical picture of Cerebral Palsy
T t t f l t t d th• Treatment of muscle contractures and the implication for gait analysis
• Muscle structure and function
• Muscle modelling
2

Agendag
• Clinical picture of Cerebral Palsy
T t t f l t t d th• Treatment of muscle contractures and the implication for gait analysis
• Muscle structure and function
• Muscle modelling
3

Cerebral Palsy:
Is defined as a nonprogressive insult p gto the immature brain, to areas that affect motor function
Is characterized by motor incoordination that impairs most notably ambulation
2 of 1000 children are affected [1][ ]
[1] Hagberg et al Acta Paediatr. 2001;90:271–277
4

Development over time
• Although the brain lesion is static, the effects on the ,musculoskeletal system are not
• Spasticity increases the muscle tone
• Soft tissue contractions develop pover time
• Without therapeutic intervention the level of ambulation cannot b i t i dbe maintained

Equinus gaitq g
6

Crouch gait
7

Hemiplegia unilateral involvementp g
8

muscle atrophy in Hemiplegiap y p gInvolved, dynamic equinus healthy
9

Muscle contracture in Hemiplegiap gInvolved side fixed equinus
10

SummarySummary
• Cerebral palsy is a brain damage which cannot b d d d lif l thbe cured and needs lifelong therapy
• Muscle tone is increased by spasticityy p y
• Muscles develop contractures (high muscle tiff ) hi h d ROM d t blstiffness) which reduces ROM and notably
affects gait performance
11

Agendag
• Clinical picture of Cerebral Palsy
T t t f l t t d th• Treatment of muscle contractures and the implication for gait analysis
• Muscle structure and function
• Muscle modelling
12

Equinus gaitq g
13

Instrumented gait analysisg y
left right norm
Spatio-temporalparameters
left right norm
step length [cm] 44 52 66
G h i di k it [k /h] 3 6 4 5Geschwindigkeit [km/h] 3,6 4,5
Generation
Power ankle
Generation
Absorption
14

Relevance of PlantarflexorsPlantarflexors
• PF generate 40 % of thePF generate 40 % of the total propulsive work Sawicki J Exp Biol 2008
er
Sawicki J. Exp. Biol. 2008
eP
owe
Ank
le
1515

Conservative therapies
16

Orthoses that restrict ankle plantarflexion have good short time effects [1]have good short time effects [1]
8 weeks
[1] Autti-Ramö et al. Literature reviewLiterature review Am. J. Phys. Med. Rehabil.Vol. 85, No. 1
17

Equinus: Therapy outcome after 8 weeks wearing orthoses
Passive Dorsiflexion improved from 10° to 20°
Post PreAnkle power at push off PreAnkle power at push-off increased Premature power burstPremature power burst decreased
18

Surgical procedures, achilles tendon lengtheningachilles tendon lengthening
19

Auswirkungen der Ganganalyse auf OperationsentscheidungenOperationsentscheidungen
52 89 % of descisions based on clinical examination were52 - 89 % of descisions based on clinical examination were changed after gait analysis [1-6]
f th 37 39 % i t ti ll dof those 37 - 39 % interventions were cancelled
28 - 40 % were added
[1] Cook et al. J Pediatr Orthop 2003; 23:292-5 [2] DeLuca et al. J Pediatr Orthop 1997; 17:608-14[3] Fuller et al. Foot & Ankle 2002; 23:738-43 [4] Kay et al. Clin Orthop Relat Res 2000; 217-22[5] Lofterod et al. Acta Orthop 2007; 78:74-80[6] Wren et al. Gait & Posture 2011 in press (randomisiert mit Kontrollgruppe)
20

Case examplep
Patient
11 years, bilateral spastic CP, GMFCS II, more involved on the right side, intoeing gait
tt i htpattern right.
OP Indikation:
suprakondylar Derotation right
Clinical examination:
Hip rotation Int/ext (60/0/30) right
Normal tibial torsion
Question Gait analysis:
How much degrees should the hip be rotated?
21

22

Transversal plane j i t t tijoint rotations Hip rotation within
Normal range
Increased tibial torsion rightg
Fot internal progression
23
p og ess oright

Descision +Foot correction (Evans, NC-
Arthrodese)Arthrodese)
+Achilles tendon lengthening (Baumann)(Baumann)
+supramalleoläre External rotation Osteotomy (15°)rotation-Osteotomy (15°).
-Hip rotation not required
24

SSummary
• Plantarflexors generate about 40% of work for propulsion
• Gait analysis helps to indentify appropriate• Gait analysis helps to indentify appropriate Plantarflexor power
• Gait analysis significanty influences surgical descision making
25

Agendag
• Clinical picture of Cerebral Palsy
T t t f l t t d th• Treatment of muscle contractures and the implication for gait analysis
• Muscle structure and function
• Muscle modelling
26

Introduction
The muscle is a highly adaptive tissue, it responds p , prapidly to mechanical stress and changes in activity [1].
In hemiplegic patientsIn hemiplegic patients muscle volume was significantly reduced at the g yinvolved leg and biarticular muscles were predominantly ff t d [2]affected [2].
[1] Ponten et al. 2008, J. Neurol Sci 266:52-56 [2] Lampe et al. 2008, Brain Dev 28:500-506

purpose
Differences in the muscle tendon unit structure in the involved leg have been reportedinvolved leg have been reported.
It is unknown whether structural changes in the muscleIt is unknown whether structural changes in the muscle tendon unit are directly related to pathologic function during gait
Hypothesis:Th i l ti b t t i l t tThere is a relation between gastrocnemius muscle structure and ankle power production during gait in children with cerebral palsycerebral palsy.

MethodsPatients: • 12 children and adolescents age 12 (SD=5.2)
years 7 females with cerebral palsy (10 diplegia 2 hemiplegia with involvement in both(10 diplegia, 2 hemiplegia with involvement in both legs)
• GMFCS I+II (able to walk without walking aids)
• Exclusion: ataxia, athetosis, Botulinum-toxin injections and previous casting of the lower limbs within 6 months as well as any surgicalwithin 6 months as well as any surgical procedures.
Gait analysis: • Vicon MX Camera system, 2 forceplates• “Plug-in-Gait” model
Clinical test:Clinical test: • Passive ankle plantar and dorsiflexion (3 times,
knee extended)
• Sonography of gastrocnemius medialis both legs

Methods: sonography
2 Angle of pennation1 Tendon length 2. Angle of pennation3. Fascicle length
1. Tendon length (distance MTJ to heel marker attachment point )marker attachment point )

Method: sonograpy data evaluationg py
Common ROM of all patients was 5 -15° plantarflexionp p
10° plantarflexion was used to determine individual muscle t f th i liparameters from the regression line
Lengths were normalized to shank lengths31
Lengths were normalized to shank lengths.

Methods: gait data evaluation g
1. Push-off energy was determined as the integraldetermined as the integral of the positive ankle power in late stance phase
left side2. Muscle parameters were
correlated to the push offleft sideright side
correlated to the push-off energy for the corresponding legcorresponding leg

Predictors of ankle joint energy at push-offPredictors of ankle joint energy at push off
n=24 (legs) R p
angle of pennation [°] 0.03 0.87
fascicle length [%] 0.26 0.21
tendon length [%] ‐0.58 0.003
33

Predictors graphsg p
34
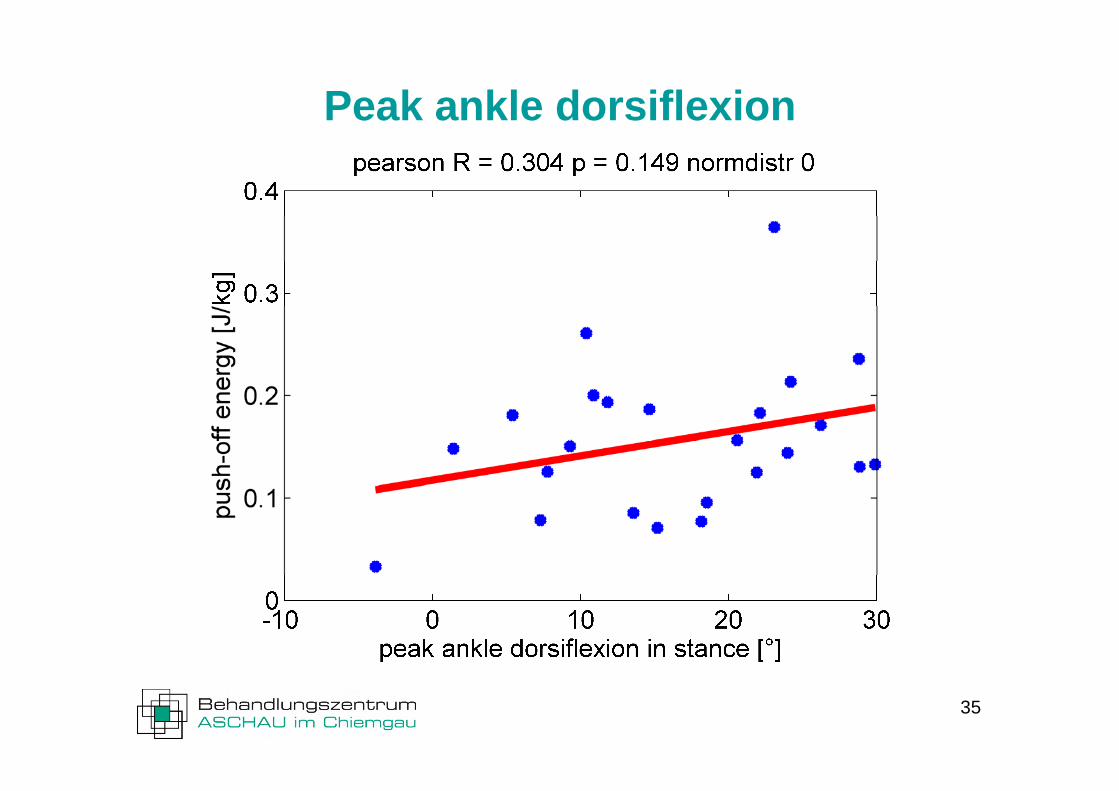
Peak ankle dorsiflexion
35

Summary results
The stronger legs with greater push-off h d h t t d denergy showed shorter tendons and
longer fascicles
Significant and excellent correlation of t d l th ith th t i h fftendon length with the concentric push-off energy

Comparison to other studies Longer tendon lengths on the weaker legs
Corresponds to shorter muscle belly lengths on the more involved side [1,2]
Shorter fascicle lengths on the weaker legs
Corresponds to [2,3] but not to [1] showing similar fascicle lengthg
[1] Malayia et al. J Electromyography and Kinesiology 2007,17, 657–63[2] Mohagheghi et al. Clin Biomech 2007, 22, 718-24 [3] Williams and Goldspink J Anat. 1978; 127: 459–68.

Discussion weakPA
Longer tendon length (TL) reduces the muscle belly length, and therefore the muscle volume which might explain a lower push-offvolume which might explain a lower push-off force
Shorter fascicle length (FL) reducesShorter fascicle length (FL) reduces contraction speed an therefore push-off power
FL
strongTL
Interpretation: On the weaker side the muscle transformed into a passive force
i i i h l d d h f i l li dtransmitting structure with longer tendon and shorter fascicles aligned along the tendon line of action. This might be useful for passive energy transmission, storage and recoil rather than active force production.

Function of elastic energyFunction of elastic energy ‘storing energy at one stage in the stride and releasing it
h ’ Al d N 1977at another’ Alexander Nature 1977
‘the stored mechanical energy can be used in producing a final velocity greater than that at which the contractilea final velocity greater than that at which the contractile component itself can shorten’ Hill A.V. Proceedings of the Royal Society of London 1950.
Use of elastic energy is important during walking at push-off Ishikawa J. Appl. Physiol. 2005, Hof J. Biomech 1983Biomech. 1983
Use of elastic energy of plantarflexors increases gait effciency about 2.4 times Sawicki J. Exp. Biol. 2009y p
39

DiscussionP blProblem: fascicle length was not correlated with ankle push-off energy !
Possible reason: a passive test was used in this study. The tendon is a passive structure and not that much influenced by the muscle activation such as fascicle length or angle of pennation.

Implications for muscle modellingp g
Hill-type Muscle Model [1] Series elastic element length changes the force generation abilities of the contractile
series elastic elementelement [1-3].
contractile elementThe length should be adapted in simulation models of
[1] Hill A V Proc Royal Soc London 1950 137 273-280
in simulation models of cerebral palsy patients
[1] Hill, A.V. Proc Royal Soc London 1950, 137, 273-280.[2] Epstein & Herzog, Theoretical models of skeletal Muscle, Wiley, 1998, pp 80.[3] Böhm et al. 2006. J. Appl. Biomech. 22, 3-13.
41

SSummary
• Gastrocnemius tendon length correlates with ankle power production
• Longer tendons and shorter fascicles are• Longer tendons and shorter fascicles are associated with more impairment during gait
42

Agendag
• Clinical picture of Cerebral Palsy
T t t f l t t d th• Treatment of muscle contractures and the implication for gait analysis
• Muscle structure and function
• Muscle modelling
43

Human Models in diagnosis and gtreatment of CP
1. Inverse dynamics models
2. Kinematic models to determine muscle lengths g
3. Muscle induced acceleration method
4. Muscle driven forward dynamic simulationsimulation
44

1. Inverse dynamic models y
45Vicon Plug-in-Gait Model, . Kadaba et al. J Orthop Res 1990: 383-92.

2. Kinematic models to determine muscle lengthslengths
Application: Hamstrings in crouch gait: Allison et al. Gait & posture 2006: 273-81
Further Application: quantifyFurther Application: quantify length changes and effects of body deformities on moment arm (Arnold & Delp J Biomech
46
arm (Arnold & Delp J Biomech 2001: 437-47)

2. Muscle induced acceleration methodProcedure: forces are applied to single muscle paths and the resulting accelerations in ankle knee and hip joint are analysed (Zajac & Gordon Exerc Sport Sci Rev 1989: 187-230Exerc Sport Sci Rev 1989: 187 230
Application: Muscles can accelerate joints they do not acce e a e jo s ey do ocross, e.g. Soleus “plantarflexion knee extension” couple Kimmel pGait & Posture 2006 211-21.
47Allison et al. Gait & posture 2006 273-281

4. Muscle driven forward simulation modelsmodels
Procedure: Use mathematical optimization to find a solution for the set of muscles that drives the model to follow a specific gait pattern
Application : simulate surgical procedures. Limitation to overcome is that spastic muscle parameters and activation are not well known
48

SSummary
• Kinematic models of muscle length calculations are helpful to support clinical decision making
• Continued work is needed to ensure that the• Continued work is needed to ensure that the results generated by musculoskeletal simulations are accurate and clinically relevantsimulations are accurate and clinically relevant
49

Recommended literature
The Identification and Treatment of Gait P bl i C b l P l 2 d Edi iProblems in Cerebral Palsy 2nd Edition 2009. Edited by James R. Gage, Michael H. Schwartz, Steven E. Koop and Tom F. Novacheck, MacKeithPress.
