dr chris turner consultant neurologist - treat- · pdf file2 i) cardiology investigation 0 2 4...
TRANSCRIPT
Queen Square Centre for Neuromuscular Diseases
Standards of Care in Myotonic DystrophyDr Chris Turner
Consultant Neurologist

LONDON’S GLOBAL UNIVERSITY
MRC Centre for Neuromuscular
Diseases
Myotonic Dystrophy Workshop
1st December 2010
UCL Institute of NeurologyBox 102, Queen Square
London WC1N 3BGwww.cnmd.ac.uk
Standards of Care in DM1-what do we know?•Cynthia Gagnon, Luc Noreau, Richard T Moxley, Luc Laberge, Stéphane Jean. Louis Richer, Michel Perron, Suzanne Veillette and Jean Mathieu, Towards an integrative approach to the management of myotonic dystrophy type 1. J. Neurol. Neurosurg. Psychiatry 2007;78;800-806.
•Management of Adults with Myotonic Dystrophy ”A Guide for Professionals” July 2009. Scottish Muscle Network
•Gagnon C, Chouinard MC, Laberge L, Veillette S, Bégin P, Breton R, Jean S, Brisson D, Gaudet D, Mathieu J; DMI Expert Panel. Health supervision and anticipatory guidance in adult myotonic dystrophy type 1. Neuromuscul Disord. 2010 Dec;20(12):847-51.
Queen Square Centre for Neuromuscular Diseases

Online DM1 questionnaire
•Dr Chris Turner Queen Square Centre for NMD
•Professor Hanns Lochmüller-Newcastle
•Michael Hails (online design)-Newcastle
•Karen Rafferty-Newcastle
•11 “spines of care”
•20 requests-11 respondents from a wide geography


1 iii) What is the average outpatient waiting time for a new appointment?
0
2
4
6
8
10
12
Less than 1 week Less than 1 month Less than 6 months Over 6 months
Queen Square Centre for Neuromuscular Diseases

1 iii) What is the average outpatient waiting time for a followup appointment?
0
1
2
3
4
5
6
Less than 1 week Less than 1 month Less than 6 months Over 6 months
Queen Square Centre for Neuromuscular Diseases

1 iv) How many new patients with DM1 do you see in outpatients per year?
0
1
2
3
4
5
6
Less than 10 Less than 50 Less than 100 More than 100
Queen Square Centre for Neuromuscular Diseases
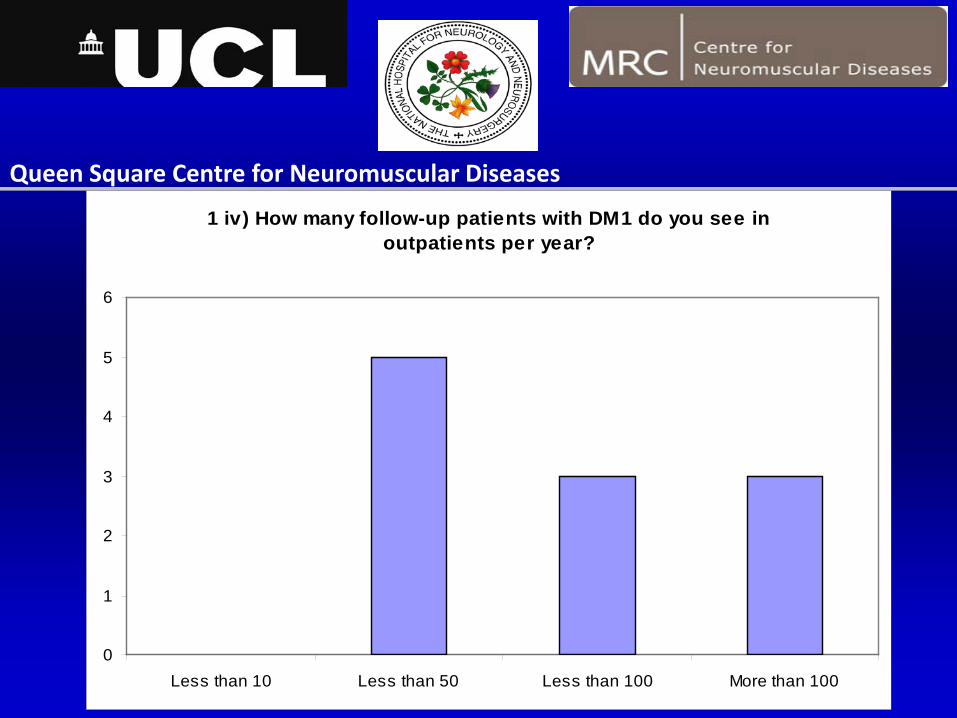
1 iv) How many follow-up patients with DM1 do you see in outpatients per year?
0
1
2
3
4
5
6
Less than 10 Less than 50 Less than 100 More than 100
Queen Square Centre for Neuromuscular Diseases
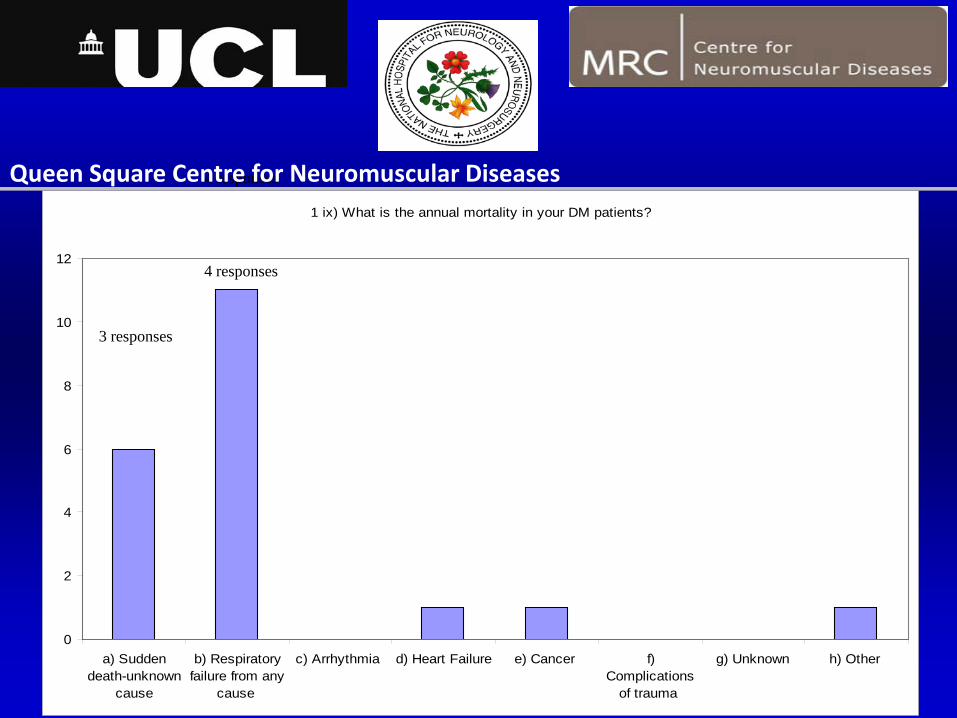
1 ix) What is the annual mortality in your DM patients?
0
2
4
6
8
10
12
a) Suddendeath-unknown
cause
b) Respiratoryfailure from any
cause
c) Arrhythmia d) Heart Failure e) Cancer f)Complications
of trauma
g) Unknown h) Other
3 responses
4 responsesQueen Square Centre for Neuromuscular Diseases
4 responses
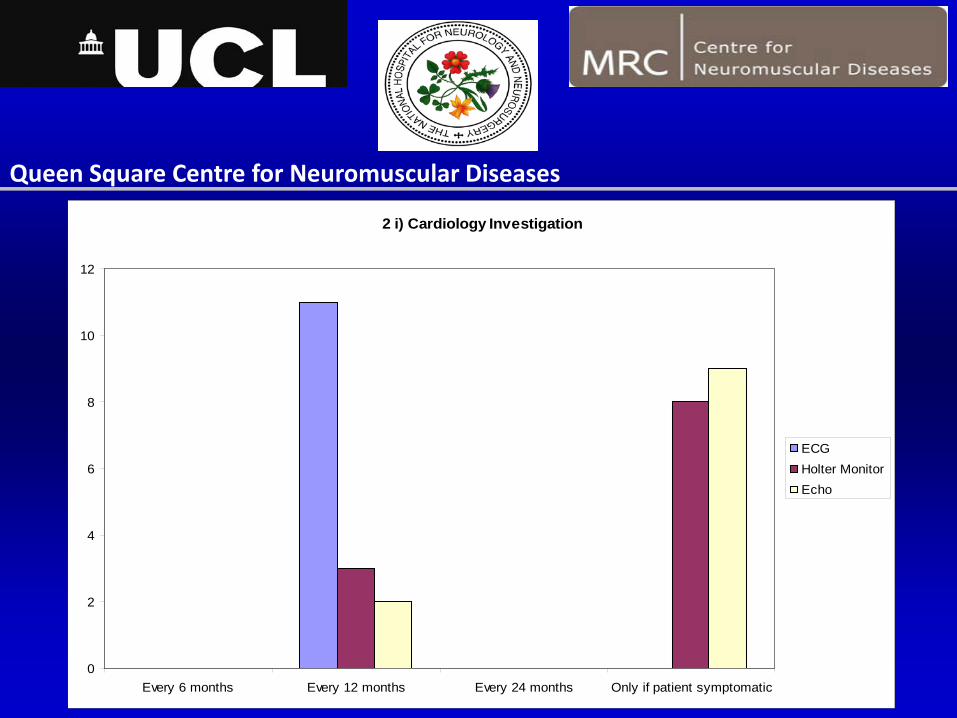
2 i) Cardiology Investigation
0
2
4
6
8
10
12
Every 6 months Every 12 months Every 24 months Only if patient symptomatic
ECGHolter Monitor Echo
Queen Square Centre for Neuromuscular Diseases

2 iv) What is the indication for PPM
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
HV interval greaterthan 70ms on EPS
Second/Third degreeHeart Block
First Degree HeartBlock
Do Not Know Other
2 iv) What is the indication for ICD
0
1
2
3
4
5
6
Inducible andsustained ventriculartachycardia (VT) on
EPS
Sustained VT onECG or Holter
monitor
VT on ECG or Holtermonitor
Do not know Other
Queen Square Centre for Neuromuscular Diseases
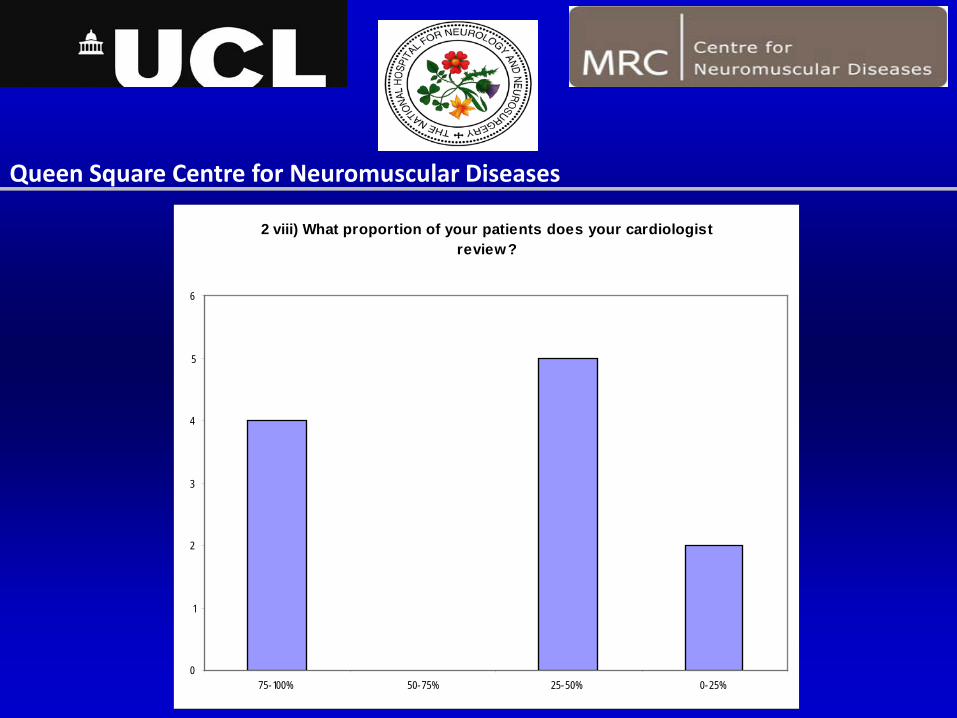
2 viii) What proportion of your patients does your cardiologist review?
0
1
2
3
4
5
6
75-100% 50-75% 25-50% 0-25%
Queen Square Centre for Neuromuscular Diseases

3 ii) What indication(s) would make you request a sleep study?
0
2
4
6
8
10
12
Routine sleepstudies performed
irrespective ofsymptoms
pO2 ESS score FVC Symptomssuggestive of
Obstructive SleepApnoea (OSA)
Symptomssuggestive of type
2 respiratoryfailure
Queen Square Centre for Neuromuscular Diseases
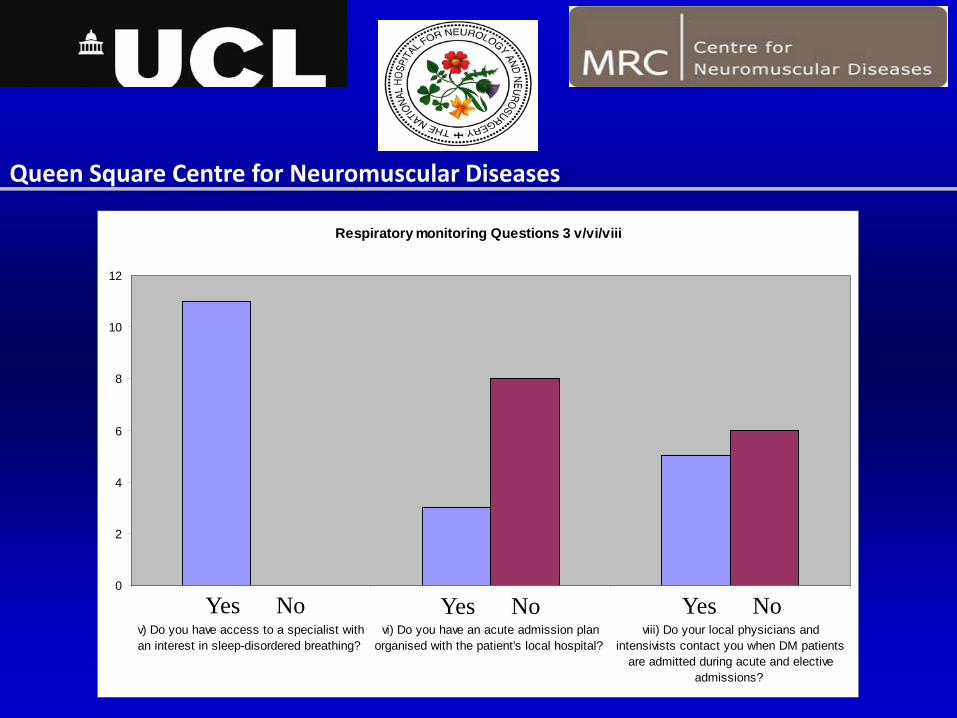
Respiratory monitoring Questions 3 v/vi/viii
0
2
4
6
8
10
12
v) Do you have access to a specialist withan interest in sleep-disordered breathing?
vi) Do you have an acute admission planorganised with the patient's local hospital?
viii) Do your local physicians andintensivists contact you when DM patients
are admitted during acute and electiveadmissions?
Yes No
Queen Square Centre for Neuromuscular Diseases
Yes No Yes No

Nutrition (majority perform SALT referral or Video fluoroscopy “if clinically indicated”)
x) What clinical indication(s) do you use to start parenteral nutrition?
0
1
2
3
4
5
6
7
8
a) Following first episodeof aspiration pneumonia
b) Recurrent aspirationpneumonia
c) Reduction in BodyMass Index. To what
level? Please state below
d) On the advice of otherprofessionals such as
SALT
e) Recurrent episodes ofchoking following oral
liquid and/or solid intake
ix) How many of your DM patients receive parenteral nutrition?
0
1
2
3
4
5
6
7
Less than 5 5-20 20-40 Greater than 40
Queen Square Centre for Neuromuscular Diseases

Which sleepiness test? (9/11 respondants)
0
1
2
3
4
5
6
7
8
9
10
a) Epworth SleepinessScale
b) Multiple Sleep LatencyTest (MSLT)
c) Stanford SleepinessScale
d) Maintenance ofwakefulness test (MWT)
Routinely
Occasionally
Rarely
Queen Square Centre for Neuromuscular Diseases

5 iv) What proportion of your DM patients take modafinil?(10/11 respondants)
0
1
2
3
4
5
6
Less than 10% 10-25% 25-50% More than 50%
Queen Square Centre for Neuromuscular Diseases

6 ii) What rating scale(s) do you use to assess patient's power?(7/11 respondants)
0
1
2
3
4
5
a) MRC rating scale ofmajor muscle groups
b) MRC Sum Score c) Muscular DisabilityRating Score (MDRS)
d) Muscular ImpairmentRating Scale (MIRS)
e) Other - please statebelow
Queen Square Centre for Neuromuscular Diseases

Treatment of myotonia Question 6 vi)(7/11 respondants)
0
1
2
3
4
5
6
a) Mexiletine b) Phenytoin c) Tricyclicantidepressants
d) Other class 1 anti-arrhythmic
e) Otheranticonvulsants
FrequentlySometimesRarely Never
Queen Square Centre for Neuromuscular Diseases

Question 7 i) How often do you check for diabetes mellitus in your patients?
0
1
2
3
4
5
6
a) If clinical suspected only b) 6 monthly c) Yearly d) Two Yearly
Queen Square Centre for Neuromuscular Diseases
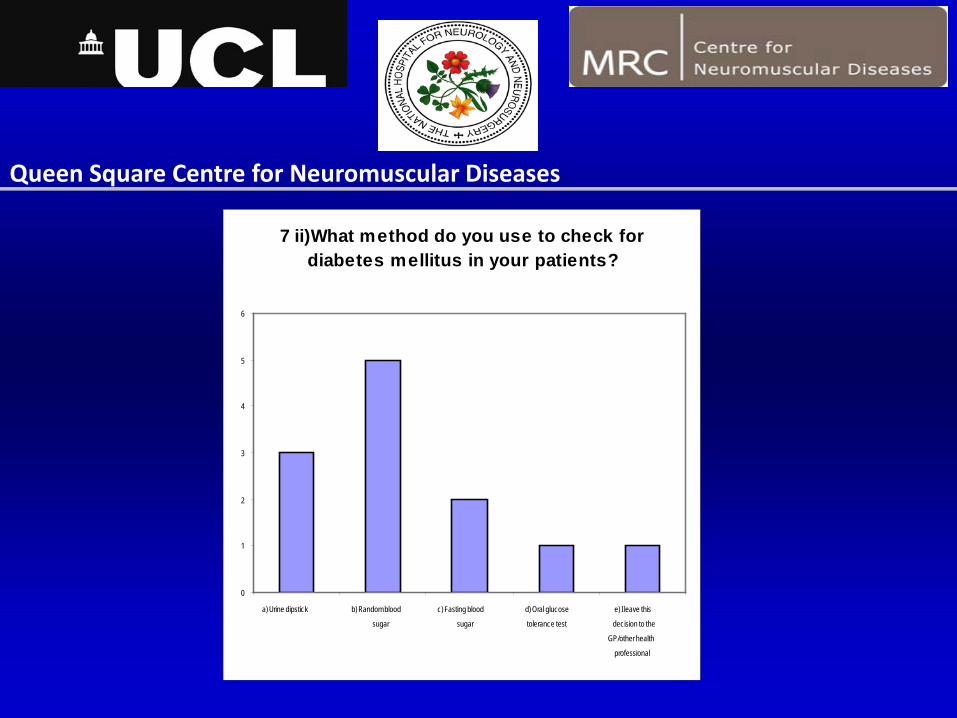
7 ii)What method do you use to check for diabetes mellitus in your patients?
0
1
2
3
4
5
6
a) Urine dipstick b) Random blood
sugar
c) Fasting blood
sugar
d) Oral glucose
tolerance test
e) I leave this
decision to the
GP/other health
professional
Queen Square Centre for Neuromuscular Diseases
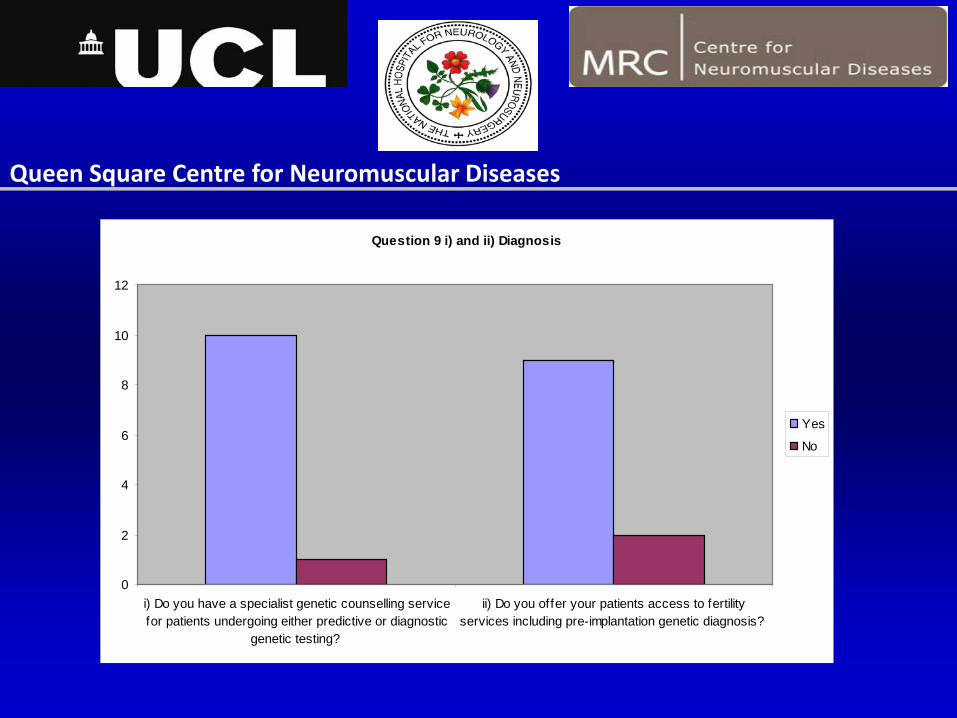
Question 9 i) and ii) Diagnosis
0
2
4
6
8
10
12
i) Do you have a specialist genetic counselling servicefor patients undergoing either predictive or diagnostic
genetic testing?
ii) Do you offer your patients access to fertilityservices including pre-implantation genetic diagnosis?
Yes
No
Queen Square Centre for Neuromuscular Diseases
DM1 Online Questionnaire June 2011-Summary of Important Questions
1 Outpatient Experience-Frequency of follow-up?-DM specialist clinics only?-Joint Clinics? With cardiology/respiratory/CNS/therapies-Mortality data
2 Cardiology-ECHO/Holter/EPS-How often and when?-Indications for referral to cardiology?-Indications for PPM/ICD
Queen Square Centre for Neuromuscular Diseases

Queen Square Centre for Neuromuscular Diseases
3 Respiratory-Monitoring respiratory failure? Respiratory physician?-Non–compliance with NIV?-Acute admission plan-Vaccinations -Risks of anaesthesia
4 GI-Monitoring of dysphagia-PEG/RIG insertion?-Predicting risk of aspiration pneumonia?-Treatment of lower GI symptoms

Queen Square Centre for Neuromuscular Diseases
5 Central Nervous System-Most appropriate test for EDS?-Modafinil? Side effects and license?-Apathy/motivation/cognitive changes
6 Muscle-Appropriate test for muscle power?-Appropriate scale for physical disability -Access to Physio/OT/orthotics-Treatment of myotonia?
7 Endocrine-Diabetes/thyroid disease-which method and how often-pregnancy

Queen Square Centre for Neuromuscular Diseases
8 Ocular-who should monitor for cataracts?
9 Diagnosis-access to genetic counselling-access to PGD/antenatal screening
10 Commnunity-access to community services-access to CNS
11 Information-Care card-Charities/support services contact -End of life plan-Tissue Donation

Queen Square Centre for Neuromuscular Diseases
What’s the evidence?

Queen Square Centre for Neuromuscular Diseases

Queen Square Centre for Neuromuscular Diseases
Development of consensus statements without formal
evidence1)Areas of agreement2)Areas for discussion

Standards of Care in DM1“areas of agreement”
1) Cardiorespiratory complications account for the majority of early mortalities in DM1 and there is an imperative to improve monitoring and treatment of these complications
2) EDS is a disabling symptom for patients and families. Modafinil is effective at treating EDS in some patients and further clinical trials need to be performed to identify effective outcome measures for assessing excessive daytime sleepiness and therapeutic efficacy of modafinil
3) Further studies into the poor tolerance of NIV in DM are required
Queen Square Centre for Neuromuscular Diseases
Standards of Care in DM1“areas of agreement”
4) Improved acute admissions care planning especially for acute respiratory failure
5) Randomised intervention studies to determine the efficacy and timing of pacemakers and implantable defibrillators in DM will be important, but in the meantime a standardised National approach to monitoring cardiac complications is important
6) "Normal" electrophysiological parameters calculated with ECG and EPS monitoring
Queen Square Centre for Neuromuscular Diseases

Standards of Care in DM1“areas of agreement”
7) Improved access to specialist cardiology input-UK Cardiology DM network
8) Greater discussion and improved management of lower GI symptoms
9) A better understanding of the role of dysphagia in causing aspiration
pneumonia, malnutrition and early mortality in DM
Queen Square Centre for Neuromuscular Diseases

Standards of Care in DM1“areas of agreement”
10) Improved access and awareness of PGD/antenatal screening
11) Improved access to therapy services in the community and access to advice from specialist centres
12) Critical role of registry formation and charities
13) More open discussion and simplified pathways to obtain DM tissueneed to be generated
Queen Square Centre for Neuromuscular Diseases

Standards of Care in DM1“areas for further discussion”
•Role of joint clinics and specialist input
•Monitoring of muscle power
•Mexiletine may be an effective treatment for myotonia in some DM patients
•Monitoring of endocrine abnormalities, cataracts
Queen Square Centre for Neuromuscular Diseases

Standards of Care in DM1“publication, dissemination and funding”
Queen Square Centre for Neuromuscular Diseases
•Consensus report for publication
•Dissemination to neurologist/geneticists
•Commissioners
•NICE guidelines?