Download - Thrombophilias
Hematology – Highyield Topics
Thrombophilia or hypercoagulability is the propensity to develop thrombosis (blood clots) due to an abnormality in the system of coagulation

AbnormalBlood Flow
AbnormalVessel Wall
Dr. Rudolph Virchow1821-1902
The Hypercoagulable State
AbnormalBlood

Thrombosis
Hereditarythrombophilia
Acquiredthrombophilia
SurgerytraumaImmobility
Inflammation
Malignancy
Estrogens
Atherosclerosis

Acquired InheritedMixed/unknown
Advancing age Prior Thrombosis Immobilization Major surgery Malignancy Estrogens
Antiphospholipid antibody syndrome
Myeloproliferative Disorders
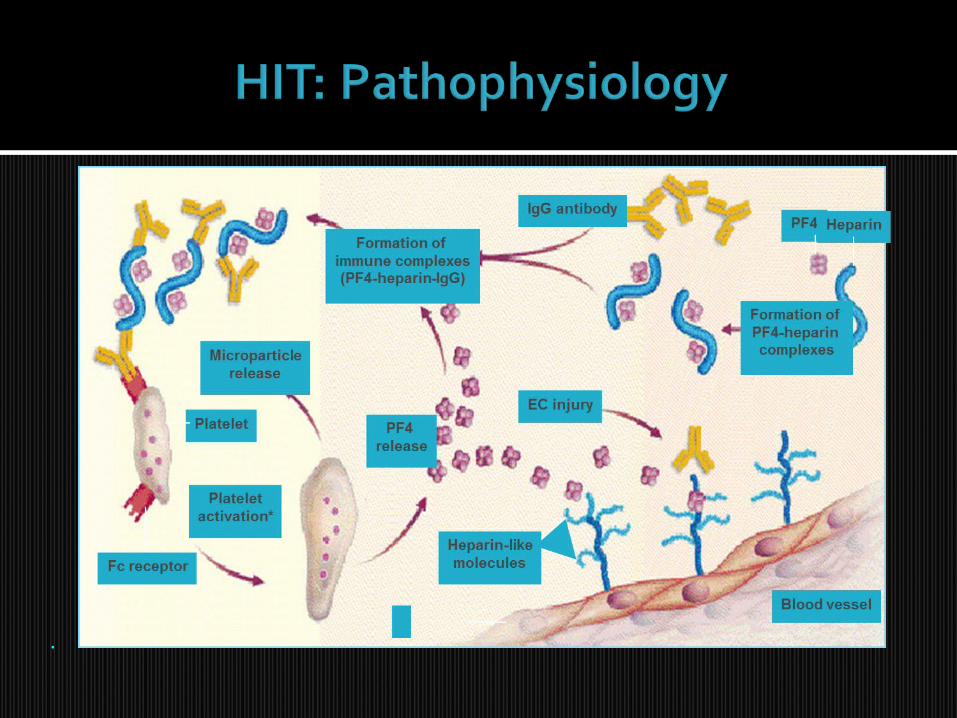
Heparin-induced thrombocytopenia (HIT)
Prolonged air travel
Antithrombin deficiency Protein C deficiency Protein S deficiency Factor V Leiden mutation (Factor V-
Arg506Gln) Prothrombin gene mutation (G A
transition at position 20210) Dysfibrinogenemias (rare)
High levels of factor VIII Acquired Protein C resistance in the
absence of Factor V Leiden High levels of Factor IX, XI
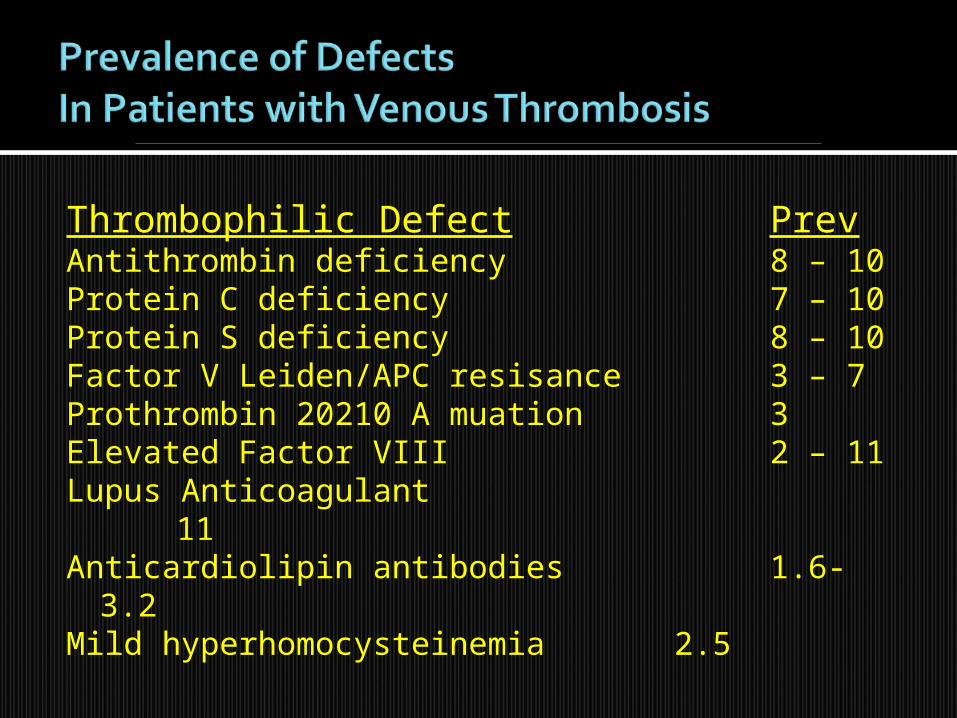
Thrombophilic Defect PrevAntithrombin deficiency 8 – 10Protein C deficiency 7 – 10 Protein S deficiency 8 – 10 Factor V Leiden/APC resisance 3 – 7 Prothrombin 20210 A muation 3Elevated Factor VIII 2 – 11 Lupus Anticoagulant 11Anticardiolipin antibodies 1.6-3.2Mild hyperhomocysteinemia 2.5
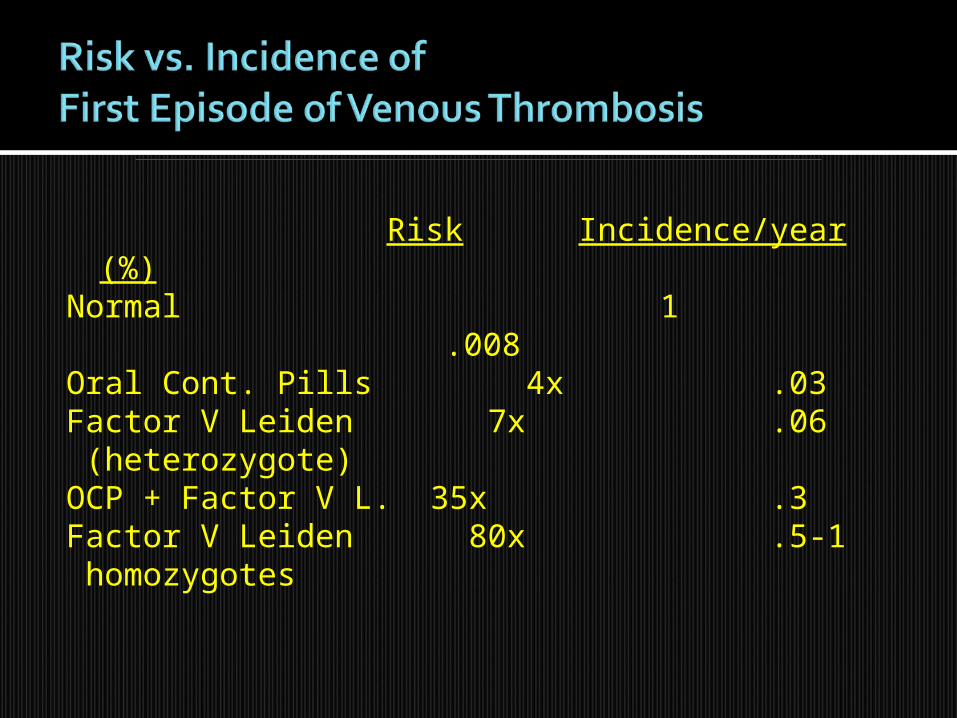
Risk Incidence/year (%)Normal 1 .008Oral Cont. Pills 4x .03Factor V Leiden 7x .06 (heterozygote)OCP + Factor V L. 35x .3Factor V Leiden 80x .5-1 homozygotes

Thrombophilic Defect Rel. RiskAntithrombin, protein C, 2.5or protein S deficiencyFactor V Leiden mutation 1.4Prothrombin 20210A mutation 1.4Elevated Factor VIII:c 6 – 11 Antiphospholipid antibodies 2 – 9

Idiopathic VTE Residual DVT Elevated D-dimer levels Age
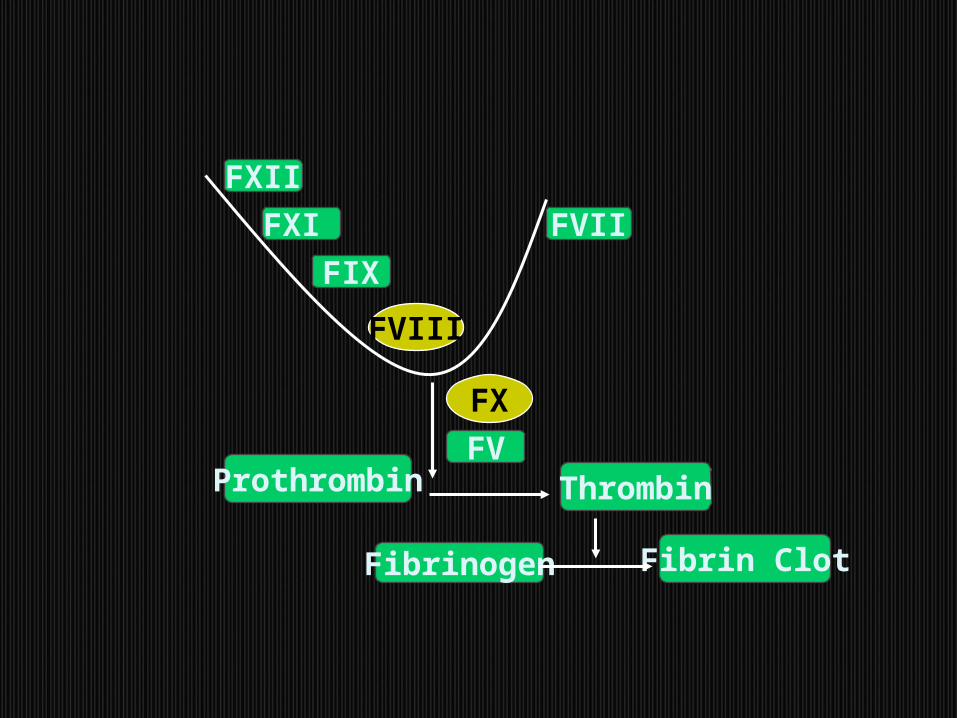
FXI
FIX
FXII
FV
FVII
Prothrombin Thrombin
Fibrinogen Fibrin Clot
FVIII
FX

J Thromb. Haem.1.525, 2003
Also known as Antithrombin III Inhibits coagulation by irreversibly binding
the thrombogenic proteins thrombin (IIa), IXa, Xa, XIa and XIIa
Antithrombin’s binding reaction is amplified 1000-fold by heparin, which binds to antithrombin to cause a conformational change which more avidly binds thrombin and the other serine proteases

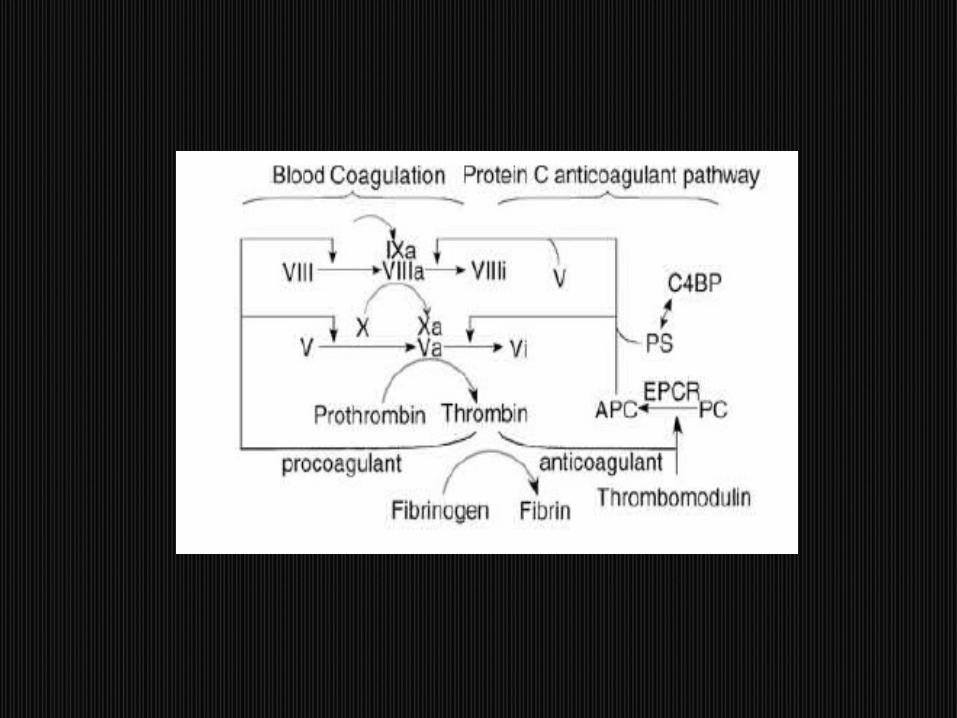
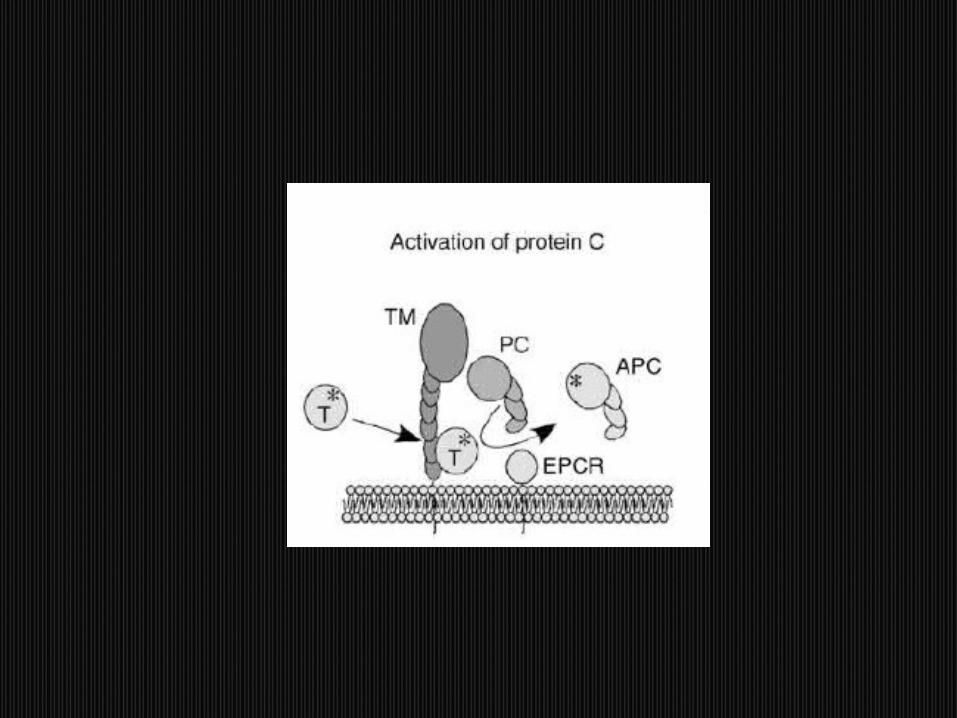
Protein C is a vitamin K dependent glycoprotein produced in the liver
In the activation of protein C, thrombin binds to thrombomodulin, a structural protein on the endothelial cell surface
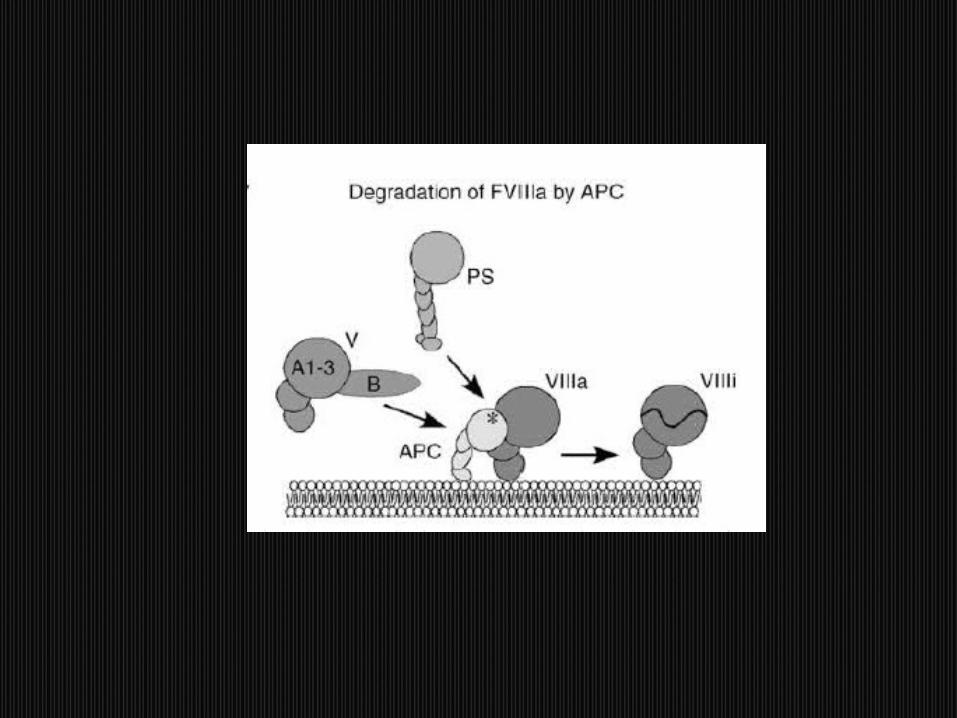
This complex then converts protein C to activated protein C (APC), which degrades factors Va and VIIIa, limiting thrombin production
For protein C to bind, cleave and degrade factors Va and VIIIa, protein S must be available
Protein C deficiency, whether inherited or acquired, may cause thrombosis when levels drop to 50% or below
Protein C deficiency also occurs with surgery, trauma, pregnancy, OCP, liver or renal failure, DIC,or warfarin

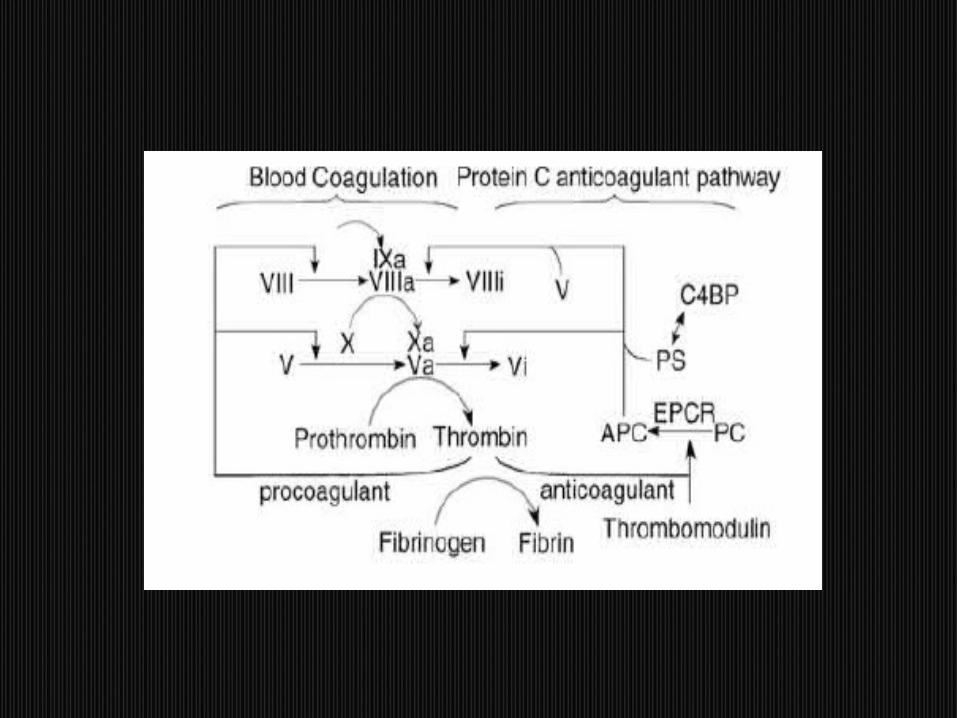
Protein S is an essential cofactor in the protein C pathway
Protein S exists in a free and bound state 60-70% of protein S circulates bound to
C4b binding proten The remaining protein S, called free PS, is
the functionally active form of protein S Inherited PS deficiency is an autosomal
dominant disorder, causing thrombosis when levels drop to 50% or lower
May be due to elevated C4bBP, decreased PS synthesis, or increased PS consumption
C4bBP is an acute phase reactant and may be elevated in inflammation, pregnancy, SLE, causing a drop in free PS
Functional PS activity may be decreased in vitamin K deficiency, warfarin, liver disease
Increased PS consumption occurs in acute thrombosis, DIC, MPD, sickle cell disease
Activated protein C (APC) is the functional form of the naturally occurring, vitamin K dependent anticoagulant, protein C
APC is an anticoagulant which inactivates factors Va and VIIIa in the presence of its cofactor, protein S
Alterations of the factor V molecule at APC binding sites (such as amino acid 506 in Factor V Leiden) impair, or resist APC’s ability to degrade or inactivate factor Va

A G-to-A substitution in nucleotide position 20210 is responsible for a factor II polymorphism
The presence of one allele (heterozygosity) is associated with a 3-6 fold increased for all ages and both genders
The mutation causes a 30% increase in prothrombin levels.

Defined by the occurrence of at least one clinical feature and the presence of at least one type of autoantibody known as an antiphospholipid antibody (aPL).
Clinical Criteria-Arterial or venous thrombosis-Pregnancy morbidity
Laboratory Criteria – confirmed on 2 or more occassions at least 12 weeks apart -IgG or IgM anticardiolipin antibody-medium or high titer-Lupus Anticoagulant
- Anti-Beta2 Glycoprotein antibodies

Thrombosis—arterial or venous Pregnancy loss Thrombocytopenia CNS syndromes—stroke, chorea Cardiac valve disease Livedo Reticularis Catastrophic APLS – thromboses,
thrombocytopenia, MAHA, Widepread organ damage. D/D – TTP, DIC

DRVVT- venom activates F. X directly;prolonged by LAC’s
APTT- Usually prolonged, does not correct in 1:1 mix
Prothrombin Time- seldom very prolonged
ACAs are antibodies directed at a protein-phosholipid complex
Detected in an ELISA assay using plates coated with cardiolipin and B2-glycoprotein

Patients with thrombosis- anticoagulation, INR 3
Anticoagulation is long-term—risk of thrombosis is 50% at 2 years after discontinuation
Women with recurrent fetal loss and APS require LMW heparin and low-dose heparin during their pregnancies

Abnormality Arterial VenousFactor V Leiden - +Prothrombin G20210A - +Antithrombin deficiency - +Protein C deficiency - +Protein S deficiency - +Lupus Anticoagulant +
+
A case of VT where no evidence of underlying obvious cause such as surgery, trauma or known malignancy is present.
Search for a hypercoagulable state in such conditions
APPROACH

Clinical History “Weakly” “Strongly”Age of onset <50 - +Recurrent thrombosis - +Positive family history - +
ProImprove understanding of pathogenesis of
thrombosisIdentify and counsel affected family membersObviate expensive diagnostic testing (e.g. CT
scans) looking for a malignancyConInfrequent identification of patients with defects
whose management would changePotential for overaggressive managementInsurance implicationsCost of testing
Routine screening of patients with VTE for an underlying thrombophilic defect “is not justified”
However, the risk of subsequent thrombosis over 5 years in men with idiopathic VTE is 30%
Any additional defect adds to risk and to possible need for prolongation of anticoagulation
Furthermore, women with a history of VTE who wish to become pregnant will be treated differently if a defect were found

Test for Factor V Leiden Genetic test for prothrombin gene mutation
20210A Functional assay of antithrombin III Functional assay of protein C Functional assay of protein S Testing for Anti-phospholipid antibody syndrome : Clotting test for lupus anticoagulant ( mixing
studies, DRVVT, STACLOT-LA) /ELISA for cardiolipin antibodies.
A complete hypercoagulability work – up as above is recommended in strongly thrombophilic patients.

Test for Factor V Leiden Genetic test for prothrombin gene mutation
G20210A Clotting assay for lupus anticoagulant/ELISA for
cardiolipin antibodies
LIMITED THROMBOPHILIA W/U AS ABOVE IN “Weakly” thrombophilic patients.
Eg. for a “weakly” thrombophilic case : one time spontaneous thrombosis in a patient age > 50 years with no family history of thrombophilia.

Hyperhomocystinemia in Thrombophilia In the past, homocysteine levels were recommended in
thrombophilic patients. Measurement of fasting total plasma homocysteine is no
longer recommended There are no data supporting a change in the duration or type
of therapy for a patient with hyperhomocysteinemia and a past history of VTE, since hyperhomocysteinemia may be a marker of thrombotic disease rather than a cause.
Results from the Leiden MEGA study indicate that the presence of methylenetetrahydrofolate reductase (MTHFR) mutation which mildly increases homocysteine levels, is not associated with an increased risk for venous thrombosis.
Hence, there is no clinical rationale for measurement of plasma homocysteine levels or for assaying for presence of the MTHFR mutation when screening for the risk of VTE.

Clues –
Bilateral DVTs, Arterial and venous thrombosis and Warfarin refractory thrombosis.
Follow age – specific screening recommendations and clinical history to select appropriate investigations when cancer associated thromboses are suscpected.

Heparin Controversial AT-III (heparin vs acute event) Most coagulation based test for APLA
▪ Hexagonal phospholipid not affected
Warfarin Protein C and protein S Need to wait 3 weeks before testing protein S Most coagulation based APLA tests

?
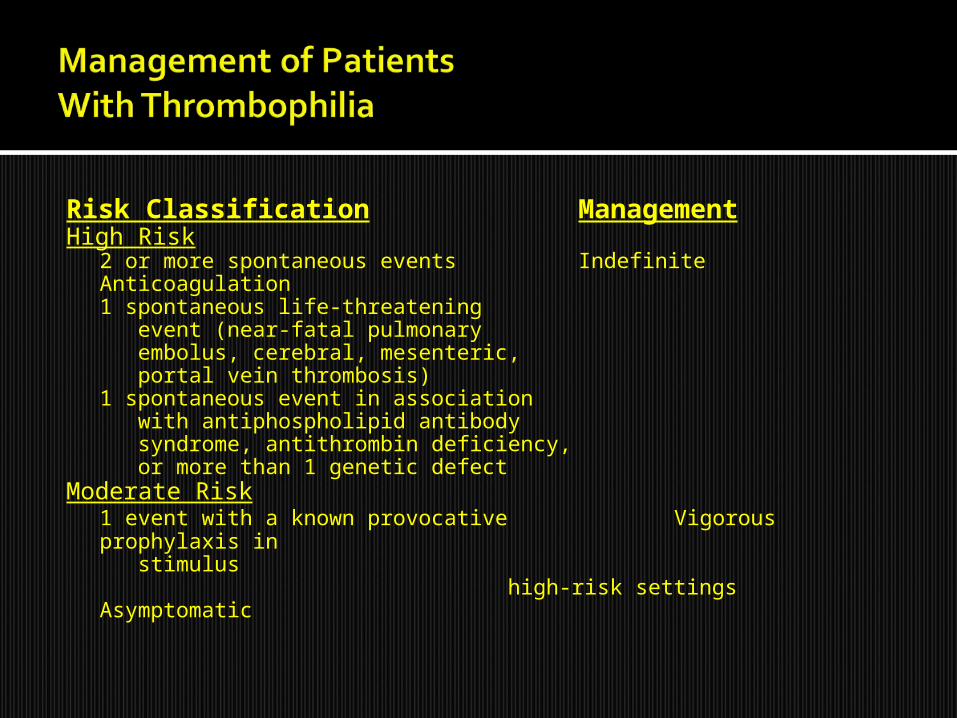
Risk Classification ManagementHigh Risk
2 or more spontaneous events Indefinite Anticoagulation1 spontaneous life-threatening event (near-fatal pulmonary embolus, cerebral, mesenteric, portal vein thrombosis)1 spontaneous event in association with antiphospholipid antibody syndrome, antithrombin deficiency, or more than 1 genetic defect
Moderate Risk1 event with a known provocative Vigorous prophylaxis in stimulus high-risk settingsAsymptomatic

Risk of recurrence depends on type of risk factor. If 1st DVT occurred after a major risk factor, recurrence is 3% where as if it occurred after minor risk factor recurrence is 10% So, stratify pts based on risk factor and then decide duration
Major transient risk factors : Major surgery, major medical illness and leg casting.
Minor transient risk factors : OC Pills, HRT High risk thrombophilias : Homzygos Prothrombin
gene mutation, Homozygos Factor v leiden, antithrombin, protein c and protein s deficiencies and APLA Syndrome
Low risk thrombophilias : Heterozygosity for prothrobin gene mutation and Factor V leiden

Patient Patient characteristicscharacteristics
Risk of recurrence Risk of recurrence (%)(%)
- In the year after - In the year after discontinuationdiscontinuation
Duration of TherapyDuration of Therapy
a.a.Major transient risk Major transient risk factor factor
b.b.Minor risk factor, no Minor risk factor, no thrombophilia thrombophilia
c.c.Idiopathic event, no Idiopathic event, no or low risk or low risk thrombophiliathrombophilia
d.d.Idiopathic event, Idiopathic event, high risk high risk thrombophiliathrombophilia
e.e.More than one More than one idiopathic eventidiopathic event
f.f.Cancer, other Cancer, other ongoing risk factorongoing risk factor
Ref: NEJM, 2004, 351Ref: NEJM, 2004, 351
3%3%
<10% if risk factor <10% if risk factor avoided. >10% if avoided. >10% if persistentpersistent
<10%<10%
>10%>10%
>10%>10%
>10%>10%
3 months3 months
6 months6 months
Until factor resolvesUntil factor resolves
6 months6 months
IndefiniteIndefinite
IndefiniteIndefinite
Indefinite. Consider Indefinite. Consider long term Rx with long term Rx with LMWH in pts with LMWH in pts with cancercancer

DiagnosisManagement
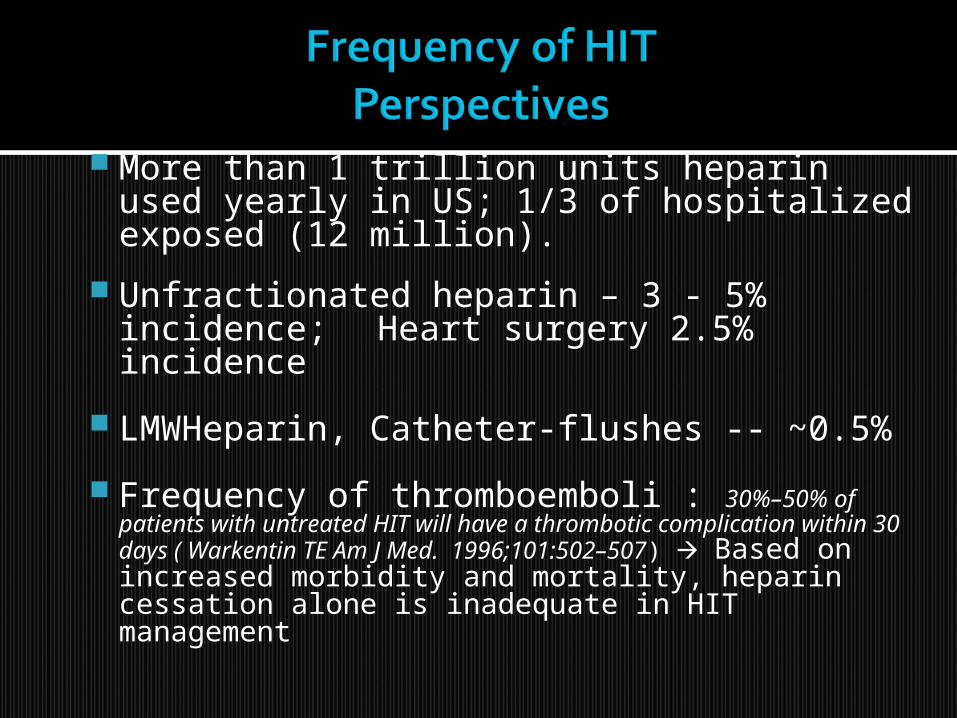
More than 1 trillion units heparin used yearly in US; 1/3 of hospitalized exposed (12 million).
Unfractionated heparin – 3 - 5% incidence;Heart surgery 2.5% incidence
LMWHeparin, Catheter-flushes -- ~0.5%
Frequency of thromboemboli : 30%–50% of patients with untreated HIT will have a thrombotic complication within 30 days ( Warkentin TE Am J Med. 1996;101:502–507) Based on increased morbidity and mortality, heparin cessation alone is inadequate in HIT management
.

HIT Two types – HIT type I and Type II. In
general, the term HIT is used widely to refer HIT Type II, the immune form.
Presence of any of the following : Otherwise unexplained thrombocytopenia Venos or arterial thromboses associated
with thrombocytopenia A fall in platelet count of 50% or more from
a prior value, even if absolute Thrombocytopenia is not present.
Necrotic skin lesions at heparin injection site
Acute systemic ( anaphylactoid) reactions occuring after IV heparin bolus.
Normal platelet count before commencement of heparin therapy
Onset of thrombocytopenia typically 5–14 days after initiation of heparin therapy but can occur earlier
Exclusion of other causes of thrombocytopenia (eg, sepsis)
Occurrence of thromboembolic complications during heparin therapy

Sequelae IncidenceThrombosis 30%–50%
Amputation 20% (arterial thrombosis)
Death 22% to 28%
.

• 30%–50% of untreated patients with thrombocytopenia progress to thrombosis
4:1 Incidence Ratio Venous to Arterial
ArterialAortic/Ileofemoral ThrombosisAcute Thrombotic Stroke Myocardial Infarction, Mural thrombosis, Thrombi in upper limb, mesenteric, renal and spinal arts.
Venous Deep Vein ThrombosisPulmonary EmbolismCerebral Dural Sinus ThrombosisAdrenal Hemorrhagic Infarction
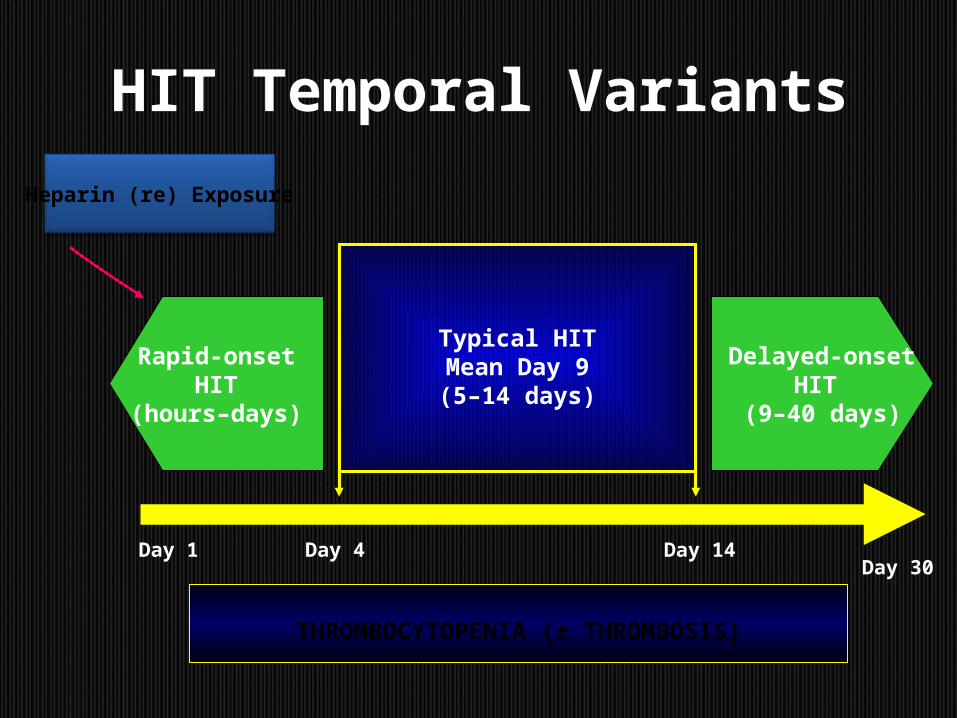
HIT Temporal Variants
Day 1 Day 4 Day 14Day 30
Delayed-onset HIT
(9–40 days)
Rapid-onset HIT
(hours–days)
Typical HITMean Day 9(5–14 days)
Heparin (re) Exposure
THROMBOCYTOPENIA (± THROMBOSIS)

Thrombocytopenia Platelet count fall > 50% and nadir greater than 20k : 2 points Platelet count fall 30 to 50% or nadir 10 to 19k : 1 point Platelet count fall < 30% or nadir < 10k : 0 points
Timing of platelet count fall Clear onset b/w days 5 to 10 or platelet count fall at ≤1 day if
prior heparin exposure within the last 30 days: 2 points Consistent with fall at 5 to 10 days but not clear (eg, missing
platelet counts) or onset after day 10 or fall ≤1 day with prior heparin exposure within the last 30 to 100 days: 1 point
Platelet count fall at <4 days without recent exposure: 0 points Thrombosis or other sequelae
Confirmed new thrombosis, skin necrosis, or acute systemic reaction after intravenous unfractionated heparin bolus: 2 points
Progressive or recurrent thrombosis, non-necrotizing (erythematous) skin lesions, or suspected thrombosis which has not been proven: 1 point
None: zero points Other causes for thrombocytopenia present —
None apparent: 2 points Possible: 1 point , Definite: zero points The 5th T : The TEST
A score is determined for each of the four above categories, resulting in a total score from zero to 8.
Pretest probabilities for HIT are, as follows:
▪ zero to 3: Low probability ▪ 4 to 5: Intermediate probability ▪ 6 to 8: High probability
Laboratory tests are ordered to confirm HIT.

Test Advantages Disadvantages
SRA Sensitivity >95%, Technically demanding
Specific > 95% Low predictive value
HIPA Rapid, available Variable sensitivity (30% – 80%);
Technique-dependent
ELISA High sensitivity High cost, less specificity,
> 95% 10% false-negative tests
There is no Gold Standard in diagnostic testing; HIT requires a clinical diagnosis .
Stop all Heparin, including heparin flushes. If dialysis, must be Heparin free.
Platelet transfusions are relatively contraindicated. ( except in those with overt bleeding).
If Intermediate or High pre-test (clinical) probability + Positive ELISA (Anti-PF4 antibody) Start alternative anticoagulant.
For low clinical probability, positive ELISA consider false positive ELISA. Obtain Serotonin Release Assay which is more specific.
If clinical probability increases over time from a prior value but if initial HIT was negative Repeat HIT antibody (ELISA) (may turn positive. ) Start alternative anticoagulant

Drug Indications
Argatroban FDA-approved for HIT (also for PCI)
Lepirudin FDA-approved for HITBivalirudin (Angiomax) PCI (including HIT patients)
Fondaparinux (Arixtra) FDA approved for DVT Prophylaxis in patients with Hip#, Hip or knee replacements. Also used in Rx of VTE. Not yet approved for HIT (Off-label use)
Danaparoid Approved for HIT in Canada, Europe, Aust.

Synthetic Direct Thrombin Inhibitor indicated as a prophylactic anticoagulant or for treatment of thromboses in HIT.
MOA : Directly inhibits Thrombin, Reversibly binds to the thrombin catalytic site and Active against both free and clot-bound thrombin
Rapid Onset of Action
In healthy subjects, the pharmacokinetics and pharmacodynamics of Argatroban were NOT affected by renal impairment, age, or gender Dosage adjustment is NOT necessary in renally impaired patients
Hepatic impairment decreases Argatroban clearance; therefore, the dosage must be reduced for hepatically impaired patients
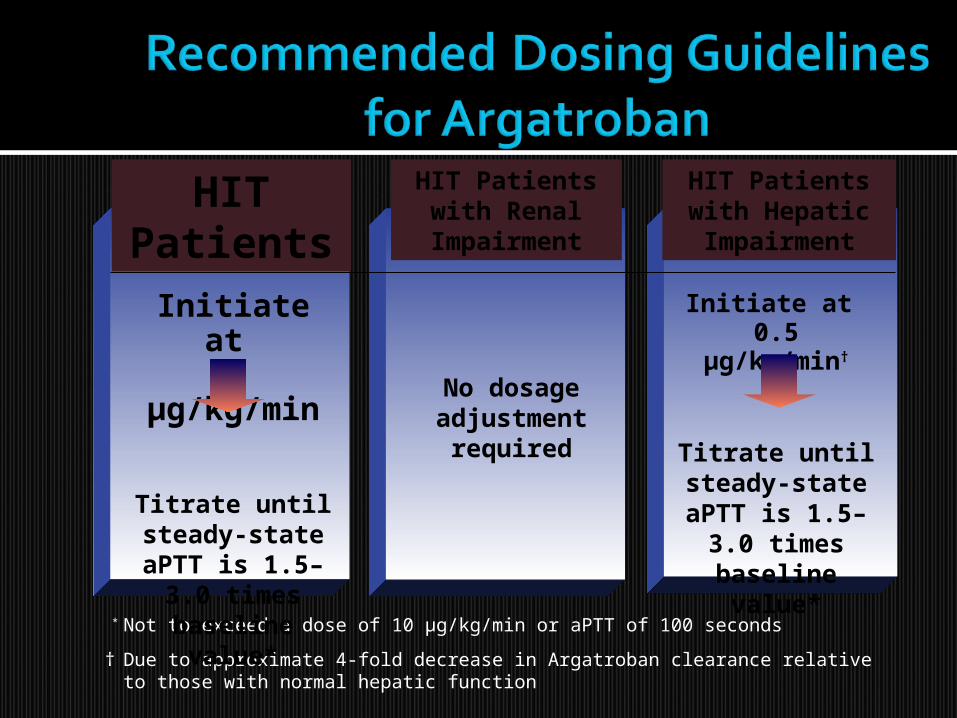
HIT Patients
HIT Patients with Renal Impairment
HIT Patients with Hepatic
Impairment
* Not to exceed a dose of 10 µg/kg/min or aPTT of 100 seconds
† Due to approximate 4-fold decrease in Argatroban clearance relative to those with normal hepatic function
Initiate at 2 µg/kg/min
Titrate until steady-state
aPTT is 1.5–3.0 times baseline
value*
No dosage adjustment
required
Initiate at 0.5 µg/kg/min†
Titrate until steady-state
aPTT is 1.5–3.0 times baseline
value*

Initiate warfarin only when platelet count increases above 100k.
All direct thrombin inhibitors, including Argatroban, may increase prothrombin time (PT); this must be taken into consideration when converting to warfarin therapy
Coadministration of Argatroban and warfarin does produce a combined effect on the laboratory measurement of the INR.
Concurrent therapy with Argatroban and warfarin does not exert an additive effect on the warfarin mechanism of action (e.g., factor Xa activity)
The previously established relationship between INR and bleeding risk is altered during combination therapy For example, an INR of 4 on co-therapy may not have the
same bleeding risk as an INR of 4 on warfarin monotherapy.
Continue anticoagulation for 2-3 months in HIT with out thromboses but continue it for 6 months if a thrombotic event occurred.

If INR is below the therapeutic range for warfarin alone, resume Argatroban
therapy
If INR is >4.0, stop Argatroban infusion
Initiate warfarin therapy using the expected daily dose of warfarin while maintaining Argatroban
infusion.* A loading dose of warfarin should not be used
If INR is within therapeutic range on warfarin alone, continue warfarin
monotherapy
If INR is 4.0, continue concomitant
therapy
Repeat INR 4-6 hours later
Measure INR daily
* For Argatroban infusion at 2 µg/kg/min, the INR on monotherapy may be estimated from the INR on cotherapy. If the dose of Argatroban >2 g/kg/min, temporarily reduce to a dose of 2 g/kg/min 4-6 hours prior to measuring the INR.
When a patient... experiences a drop in platelet counts develops thrombosis
Consider HIT during/soon after
heparin exposure*
* Heparin exposure may be through virtually any preparation (including LMWH), any dose, or any route of heparin (including flushes and coated lines)

Questions?







