aplas and other thrombophilias: is testing ever appropriate?
TRANSCRIPT
APLAs and Other Thrombophilias:
Is Testing Ever Appropriate?
Stephan Moll, MD
HematologyUniversity of North Carolina
Chapel Hill, NC
Anticoagulation ForumOct 30th, 2021
Q: “Is Testing Ever Appropriate?”
A: “Yes
Q: “Is Testing Ever Appropriate?”
A: “Yes, in selected patients”
Topics
Practical Take-Home Points
1 “How long to treat VTE?”
3 “How best to treat unexplained arterial thromboembolism?”
Should antithrombotic therapy be used for unexplained pregnancy loss?
Is finding a thrombophilia relevant for other family members?5
2 “What anticoagulant is best to use for VTE?”
4

Disclosures
Consultant: Bristol-Myers Squibb, Diagnostica Stago
Speaker bureau: none
2 31
DVT and PE
4 5
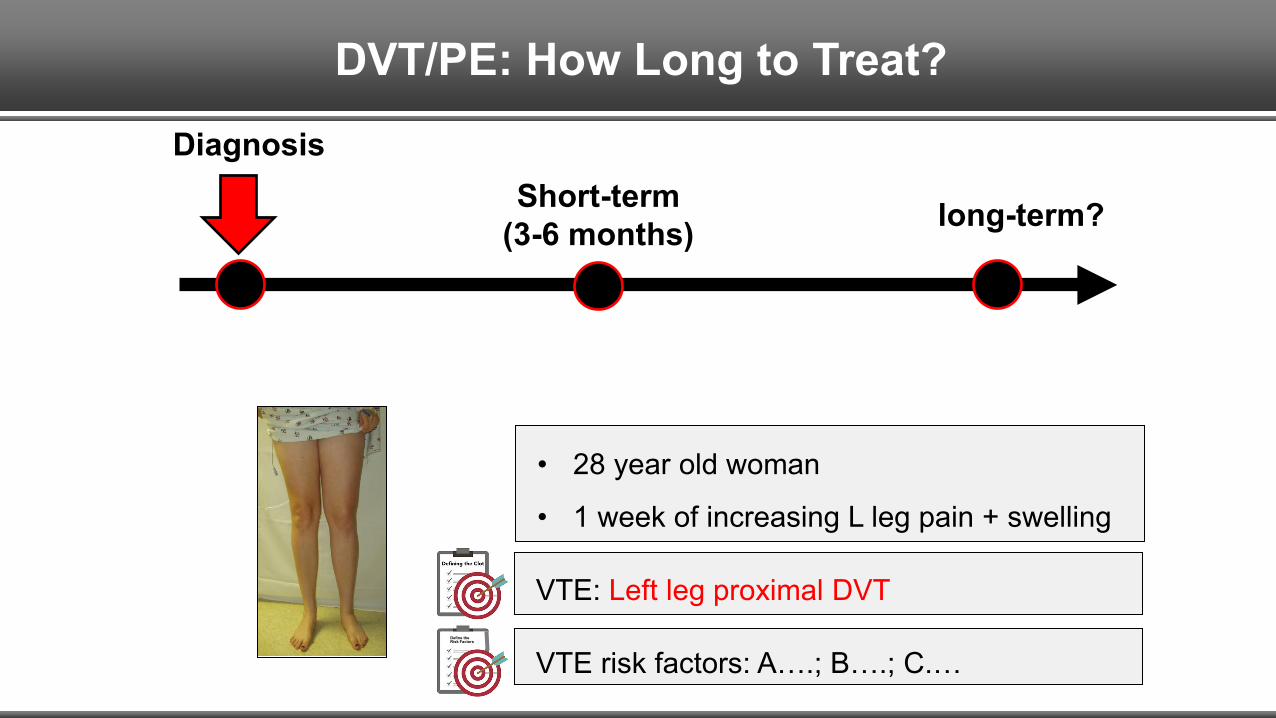
• 28 year old woman
• 1 week of increasing L leg pain + swelling
Diagnosis
DVT/PE: How Long to Treat?
VTE: Left leg proximal DVT
VTE risk factors: A….; B….; C.…Define the Risk Factors
Short-term (3-6 months) long-term?
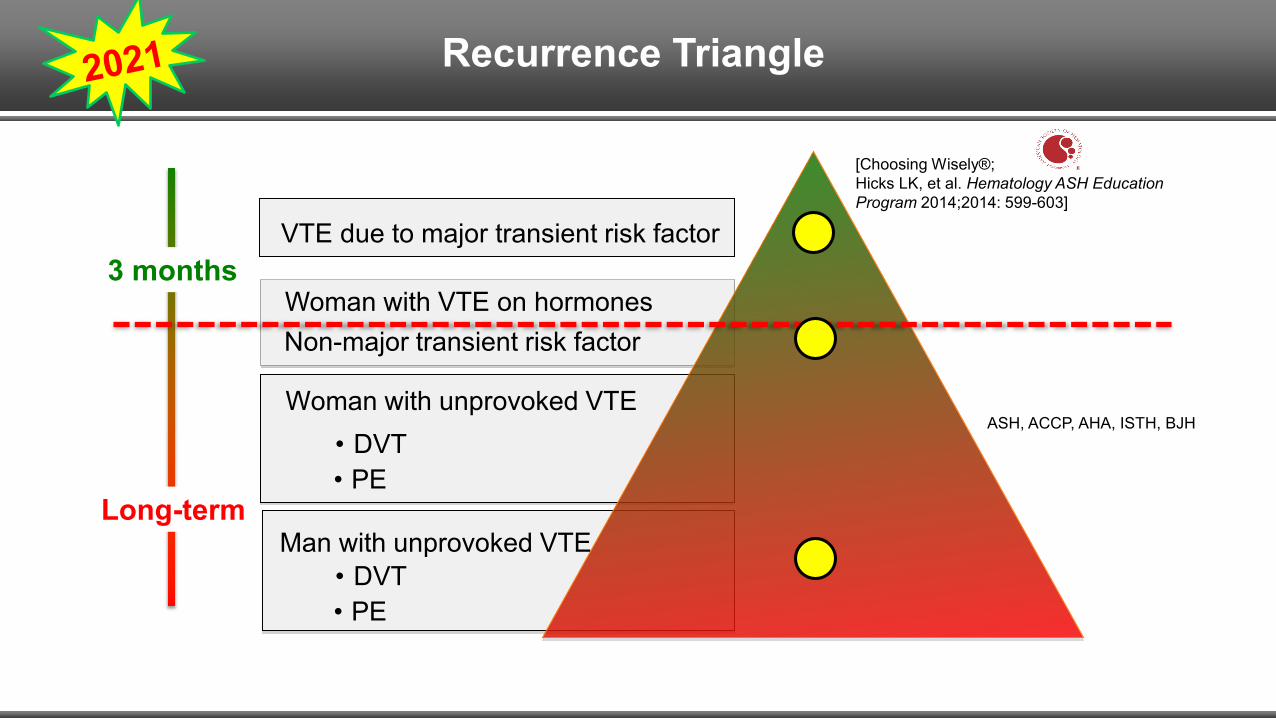
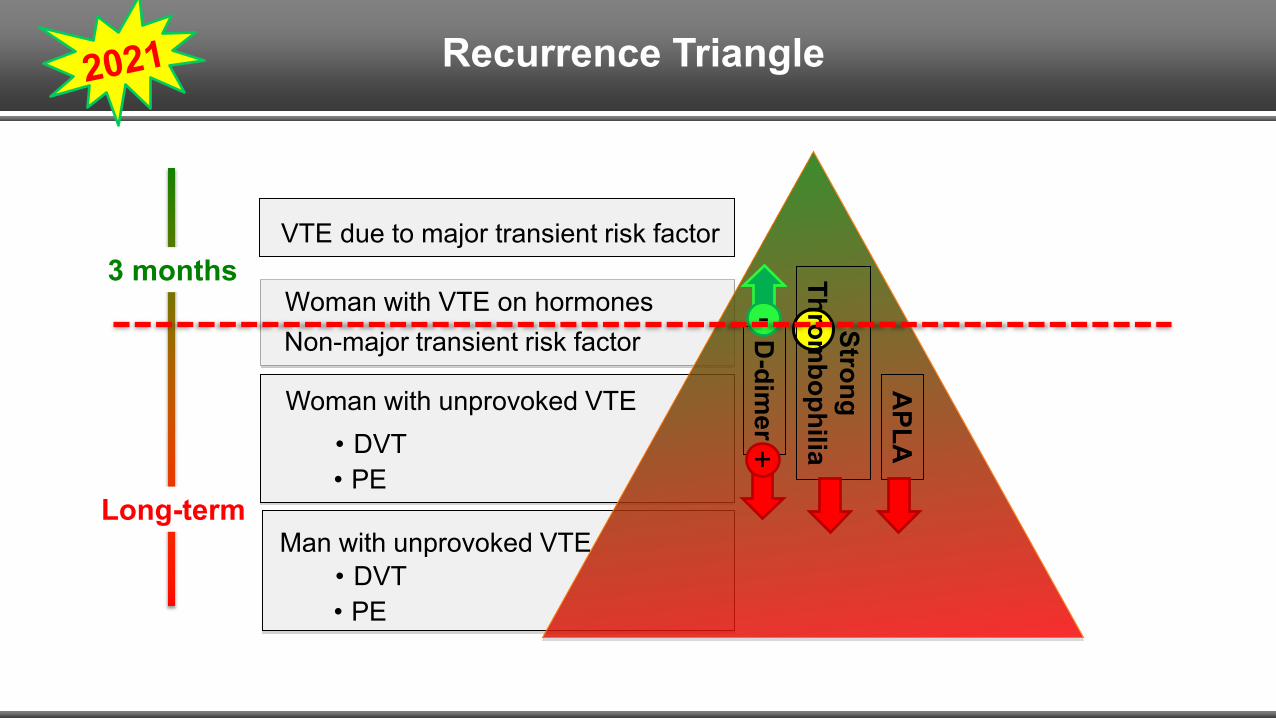
VTE due to major transient risk factor
Woman with unprovoked VTE
Woman with VTE on hormones
Long-term
3 months
Recurrence Triangle
• PE• DVT
Man with unprovoked VTE
Non-major transient risk factor
• PE• DVT
[Choosing Wisely®; Hicks LK, et al. Hematology ASH EducationProgram 2014;2014: 599-603]
ASH, ACCP, AHA, ISTH, BJH
VTE due to major transient risk factor
Woman with unprovoked VTE
Woman with VTE on hormones
Man with unprovoked VTE
Non-major transient risk factor
• PE• DVT
Long-term
3 months
• PE• DVTStrong
Thrombophilia
D-dim
er
+
-
APLA
Recurrence Triangle
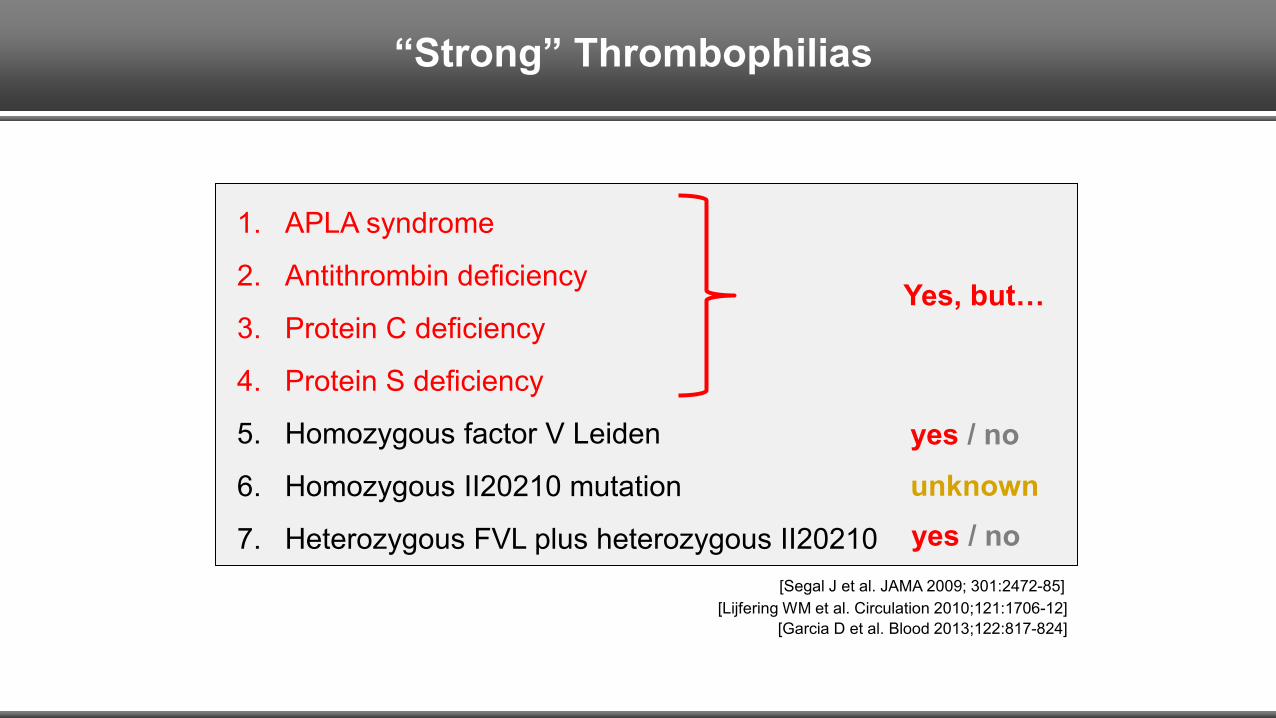
“Strong” Thrombophilias
1. APLA syndrome
2. Antithrombin deficiency
3. Protein C deficiency
4. Protein S deficiency
5. Homozygous factor V Leiden
6. Homozygous II20210 mutation
7. Heterozygous FVL plus heterozygous II20210
Yes, but…
yes / nounknownyes / no
[Segal J et al. JAMA 2009; 301:2472-85][Lijfering WM et al. Circulation 2010;121:1706-12]
[Garcia D et al. Blood 2013;122:817-824]
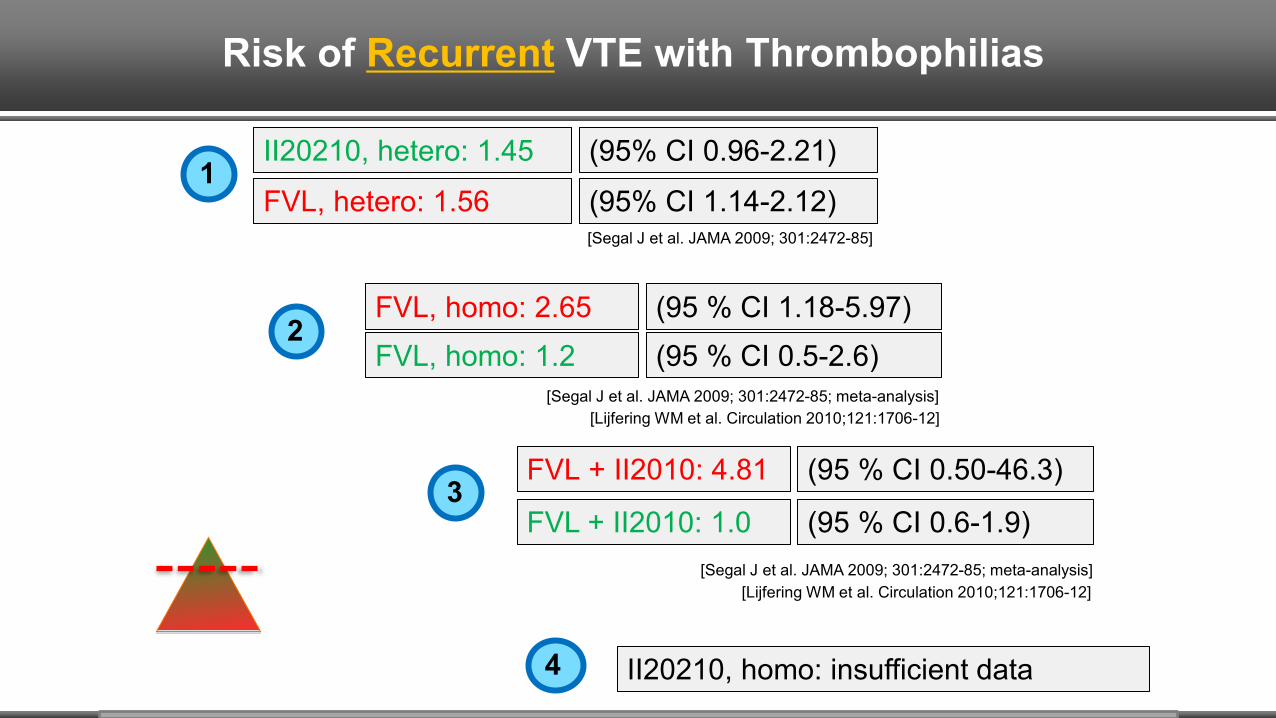
Risk of Recurrent VTE with Thrombophilias
(95% CI 0.96-2.21)II20210, hetero: 1.45
(95% CI 1.14-2.12)FVL, hetero: 1.561
[Segal J et al. JAMA 2009; 301:2472-85]
(95 % CI 1.18-5.97)FVL, homo: 2.65
[Segal J et al. JAMA 2009; 301:2472-85; meta-analysis]
FVL, homo: 1.2 (95 % CI 0.5-2.6)
[Lijfering WM et al. Circulation 2010;121:1706-12]
2
(95 % CI 0.50-46.3)FVL + II2010: 4.81
[Segal J et al. JAMA 2009; 301:2472-85; meta-analysis]
FVL + II2010: 1.0 (95 % CI 0.6-1.9)
[Lijfering WM et al. Circulation 2010;121:1706-12]
3
II20210, homo: insufficient data4
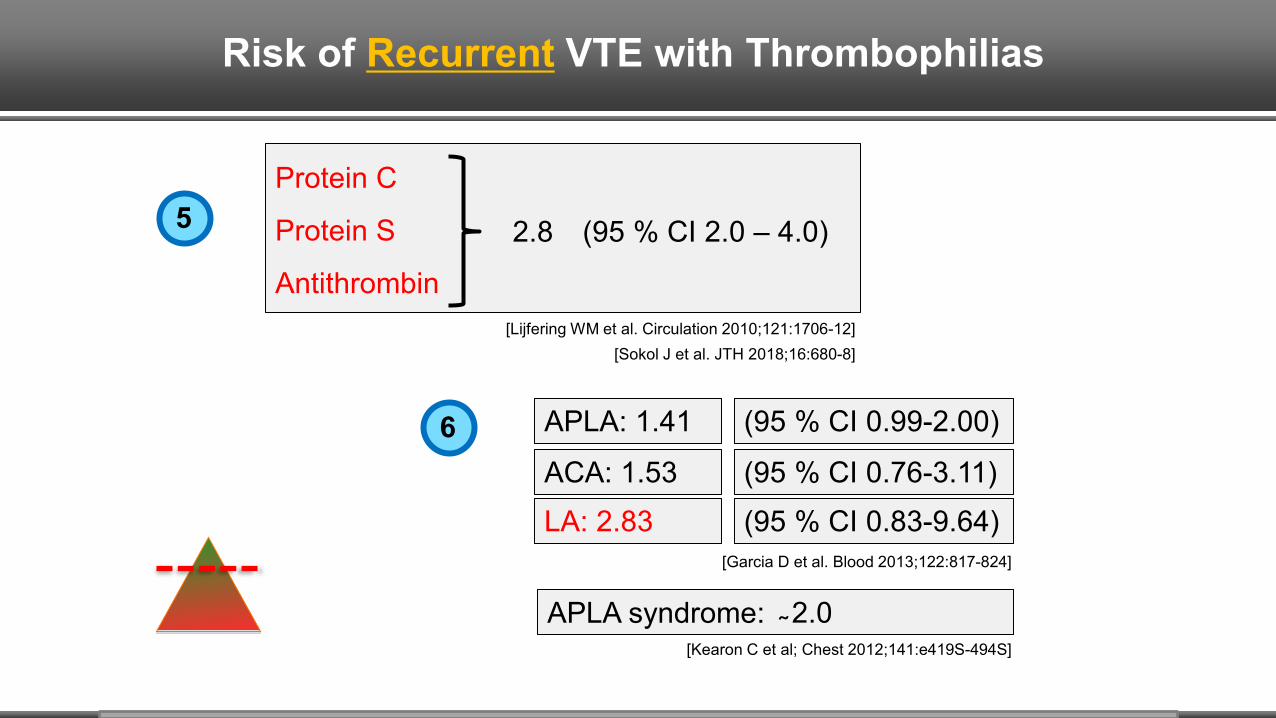
Risk of Recurrent VTE with Thrombophilias
Protein C
Protein S
Antithrombin
2.8 (95 % CI 2.0 – 4.0)
[Lijfering WM et al. Circulation 2010;121:1706-12][Sokol J et al. JTH 2018;16:680-8]
5
[Garcia D et al. Blood 2013;122:817-824]
(95 % CI 0.99-2.00)
(95 % CI 0.76-3.11)(95 % CI 0.83-9.64)
APLA: 1.41
ACA: 1.53LA: 2.83
APLA syndrome:[Kearon C et al; Chest 2012;141:e419S-494S]
2.0
6
Are APLA a Risk Factor for Recurrent VTE?
[Garcia D et al. Blood 2013;122:817-824]
• 8 eligible studies• All had important methodologic limitations.• “We judged the overall quality of the evidence as very low”.
Systematic Review
• Although it appears that pos. APLA predict ↑’d risk of VTE recurrence, the strength of this association is uncertain.
Conclusion
[Ortel TL et al. J Thromb Haemost 2020;18:2274-86]
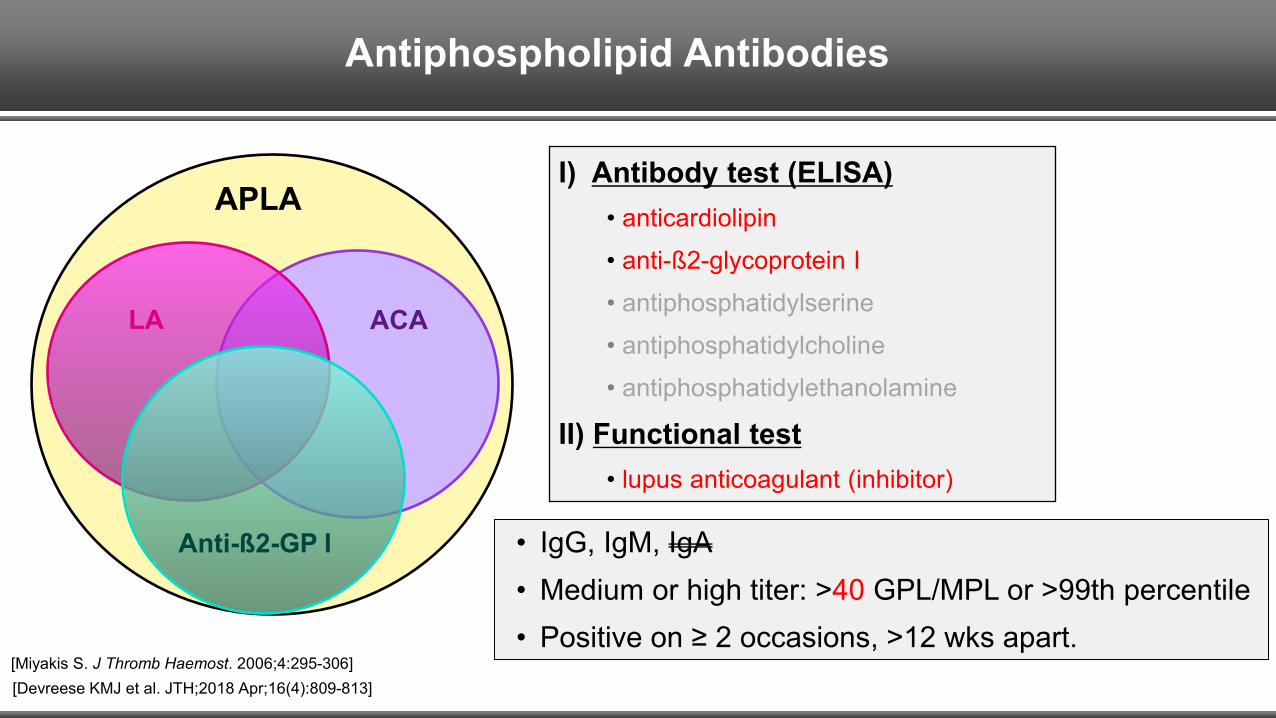
Antiphospholipid Antibodies
APLA
ACALA
Anti-ß2-GP I
I) Antibody test (ELISA)• anticardiolipin• anti-ß2-glycoprotein I• antiphosphatidylserine• antiphosphatidylcholine• antiphosphatidylethanolamine
II) Functional test• lupus anticoagulant (inhibitor)
[Miyakis S. J Thromb Haemost. 2006;4:295-306][Devreese KMJ et al. JTH;2018 Apr;16(4):809-813]
• IgG, IgM, IgA• Medium or high titer: >40 GPL/MPL or >99th percentile• Positive on ≥ 2 occasions, >12 wks apart.
Elevated FVIII is a risk factor for:• 1st VTE event• Recurrent VTE 1-3
Limitations:• Acute phase protein• Increases with age 4
• Results vary from lab to lab• Clinician does not know what “upper 10th or 25th percentile” is.
1 [Kyrle PE et al. NEJM 2000;343(7):457-62. AUREC study]2 [Timp JF et al. JTH 2015 Oct;13(10):1823-32. MEGA study]
3 [Cosmi B et al. Thromb Res. 2008;122(5):610-7][Shrivastava S et al. JTH 2006 Jun;4(6):1208-14]
Factor VIII NOT really a useful routine clinical tool to predict recurrent VTE.
Factor VIII
4 [Albanez S et al. JTH 2016,14: 953–963]
DVT/PE
Pt with VTE and intermediate risk for recurrence… and I don’t quite know whether to stop or continue anticoagulation: I consider thrombophilia w/u, particularly APLA (in addition to D-dimer).
Take-home point
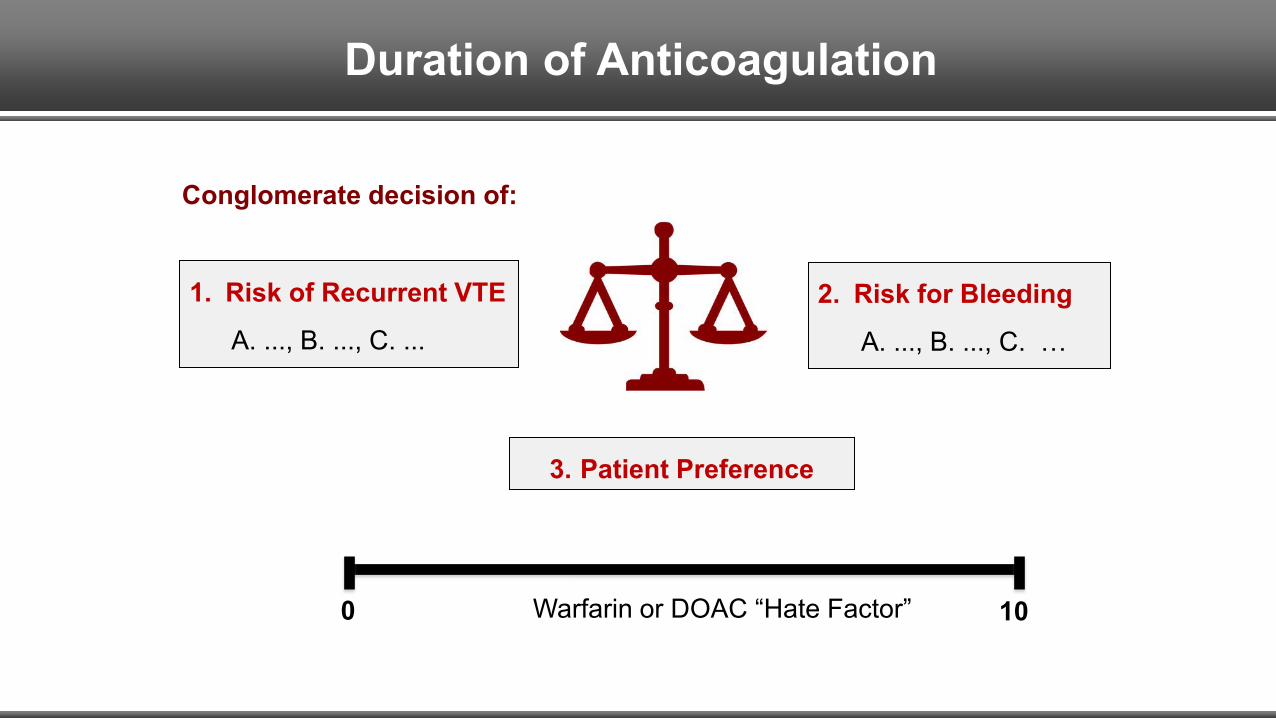
Duration of Anticoagulation
3. Patient Preference
2. Risk for Bleeding
A. ..., B. ..., C. …
1. Risk of Recurrent VTE
A. ..., B. ..., C. ...
Conglomerate decision of:
0 10Warfarin or DOAC “Hate Factor”
1 3
What Anticoagulant is Best to Use?
42 5
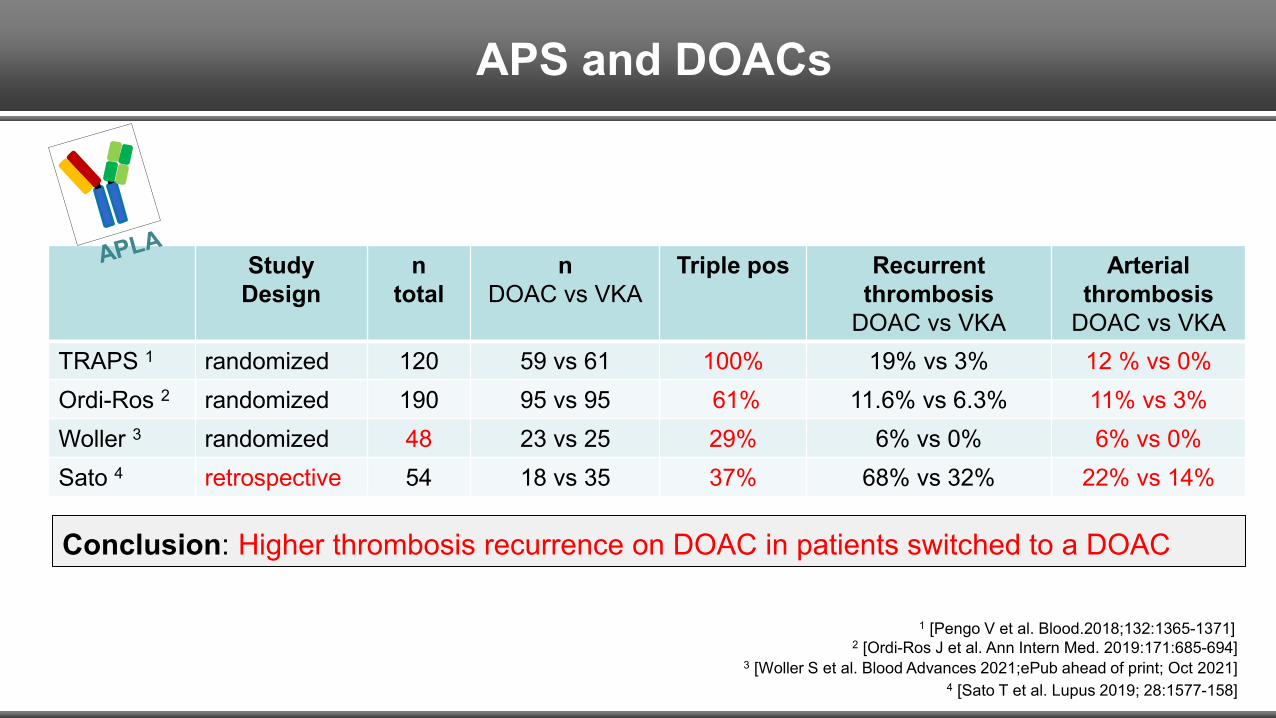
APS and DOACs
Study Design
n total
nDOAC vs VKA
Triple pos Recurrent thrombosis
DOAC vs VKA
Arterial thrombosis
DOAC vs VKATRAPS 1 randomized 120 59 vs 61 100% 19% vs 3% 12 % vs 0%Ordi-Ros 2 randomized 190 95 vs 95 61% 11.6% vs 6.3% 11% vs 3%Woller 3 randomized 48 23 vs 25 29% 6% vs 0% 6% vs 0%Sato 4 retrospective 54 18 vs 35 37% 68% vs 32% 22% vs 14%
4 [Sato T et al. Lupus 2019; 28:1577-158]
2 [Ordi-Ros J et al. Ann Intern Med. 2019:171:685-694]
Conclusion: Higher thrombosis recurrence on DOAC in patients switched to a DOAC
1 [Pengo V et al. Blood.2018;132:1365-1371]
3 [Woller S et al. Blood Advances 2021;ePub ahead of print; Oct 2021]
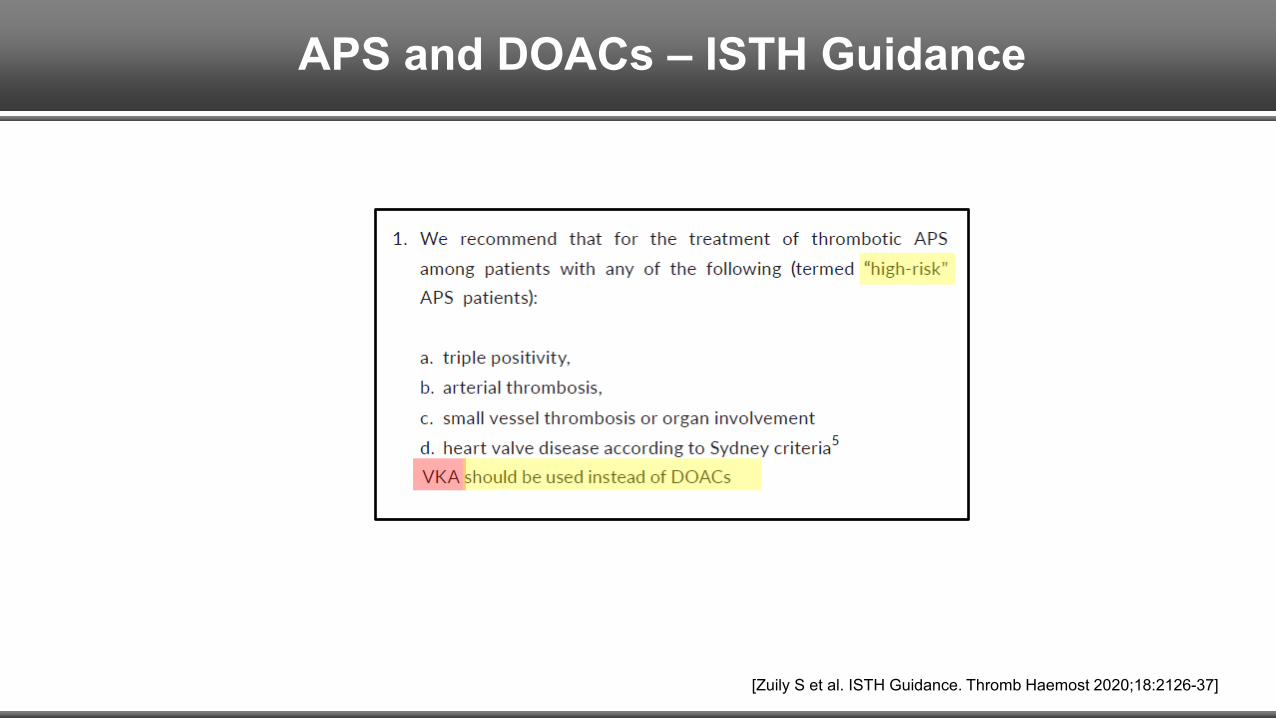
APS and DOACs – ISTH Guidance
[Zuily S et al. ISTH Guidance. Thromb Haemost 2020;18:2126-37]
APS and DOACs
1. In general, I prefer warfarin2. If patient with APS has done well on a DOAC for ≥ 2 years: I don’t switch to a VKA.3. In the de novo dx’d APS patient: unclear what is the best anticoagulant.4. High “Warfarin-hate factor”: Dabigatran an option? LMWH? Fondaparinux?
Take-home points
“Should anybody with an acute VTE be tested for APLA?”
Unexplained Arterial Thrombosis
21 4
`
53
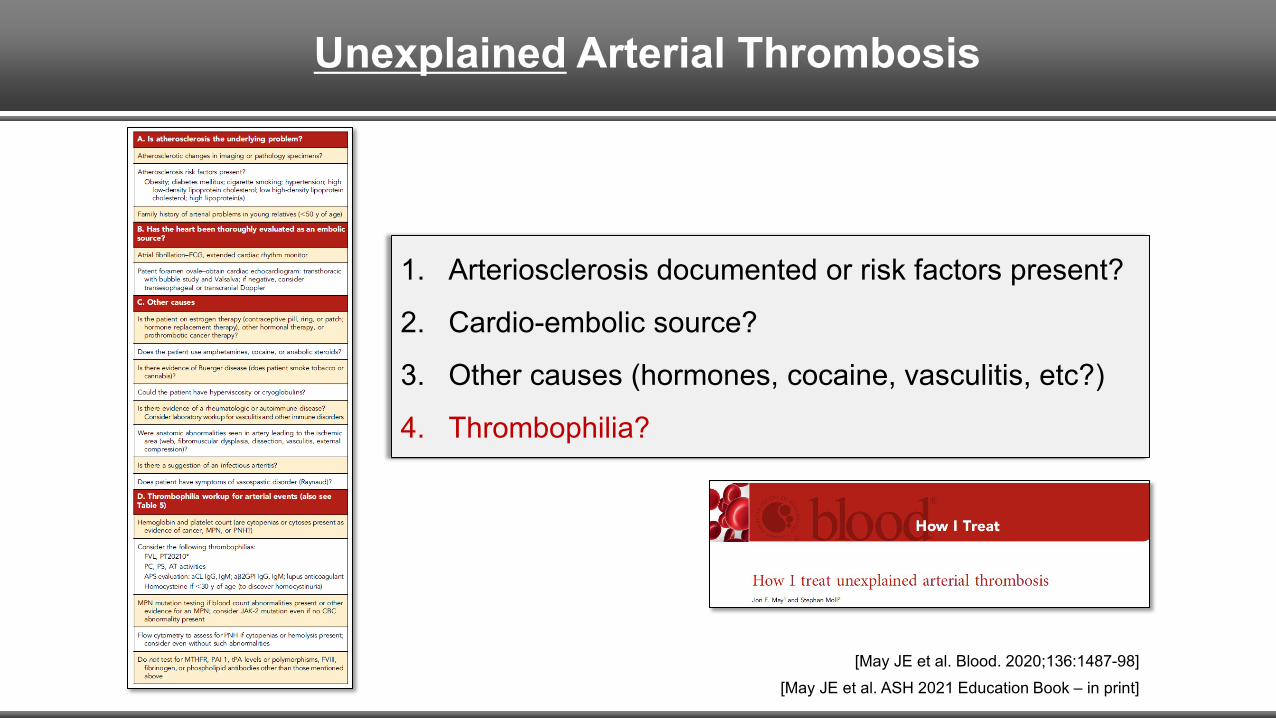
Unexplained Arterial Thrombosis
1. Arteriosclerosis documented or risk factors present?
2. Cardio-embolic source?
3. Other causes (hormones, cocaine, vasculitis, etc?)
4. Thrombophilia?
[May JE et al. Blood. 2020;136:1487-98][May JE et al. ASH 2021 Education Book – in print]
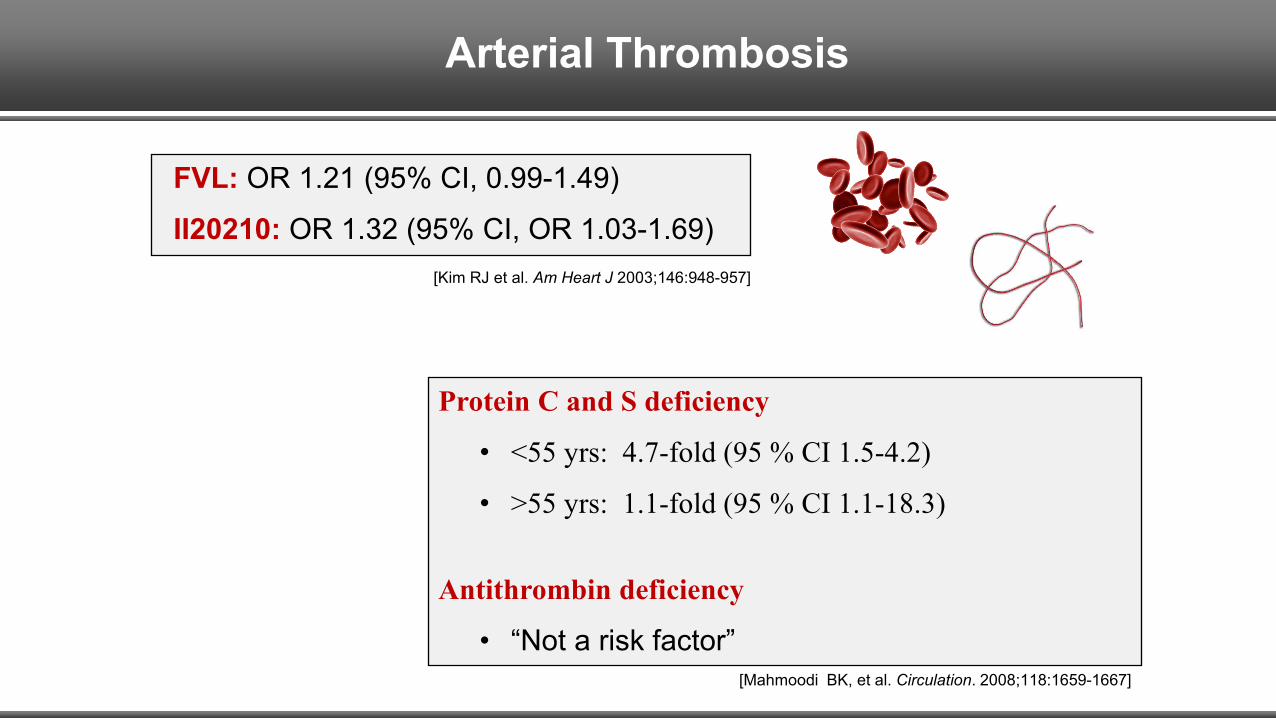
Arterial Thrombosis
FVL: OR 1.21 (95% CI, 0.99-1.49)
II20210: OR 1.32 (95% CI, OR 1.03-1.69)
Protein C and S deficiency
• <55 yrs: 4.7-fold (95 % CI 1.5-4.2)
• >55 yrs: 1.1-fold (95 % CI 1.1-18.3)
Antithrombin deficiency
• “Not a risk factor”[Mahmoodi BK, et al. Circulation. 2008;118:1659-1667]
[Kim RJ et al. Am Heart J 2003;146:948-957]
Unexplained Arterial Thrombosis
How to best treat (secondary prevention)?
1. Anti-platelet therapy?
2. Anticoagulant?
3. Both together?[May JE, Moll S. Blood. 2020;136:1487-98]
• Best treatment not known.• ASA plus an anticoagulany?
APLA and arterial thrombosis:
[Okuma H et al. Int J Med Sci 2009;7:15-18: ASA vs ASA plus warfarin in APS]
Unexplained Arterial Thrombosis
In the younger person…
… with truly unexplained thrombo-embolism:
I do consider testing for thrombophilia.
Take-home point
Pregnancy Loss
21 43
`
5
Pregnancy Loss / Complications
[Skeith L et al. Blood 2016;127:1650-5]

Pregnancy Loss / Complications
[Skeith L et al. Blood 2016;127:1650-5]
All trials
Multicenter trials only
Pregnancy Loss / Complications
Pregnancy loss + thrombophilia (other than APLA): LMWH treatmentNOT indicated.
1
Pregnancy loss: thrombophilia testing NOT indicated (other than APLA).2
Conclusions
ACOG
[Obstet Gynecol 2013 Sep;122(3):706-17]
Testing NOT recommended for recurrent pregnancy loss,
placental abruption, IUGR or preeclampsia
Inherited thrombophilias
APLA
Testing may be appropriate for women with fetal loss
1
2
Pregnancy Loss
Unexplained pregnancy loss: Test for APLA.
Take-home point

Family History
21 3
`
4 5
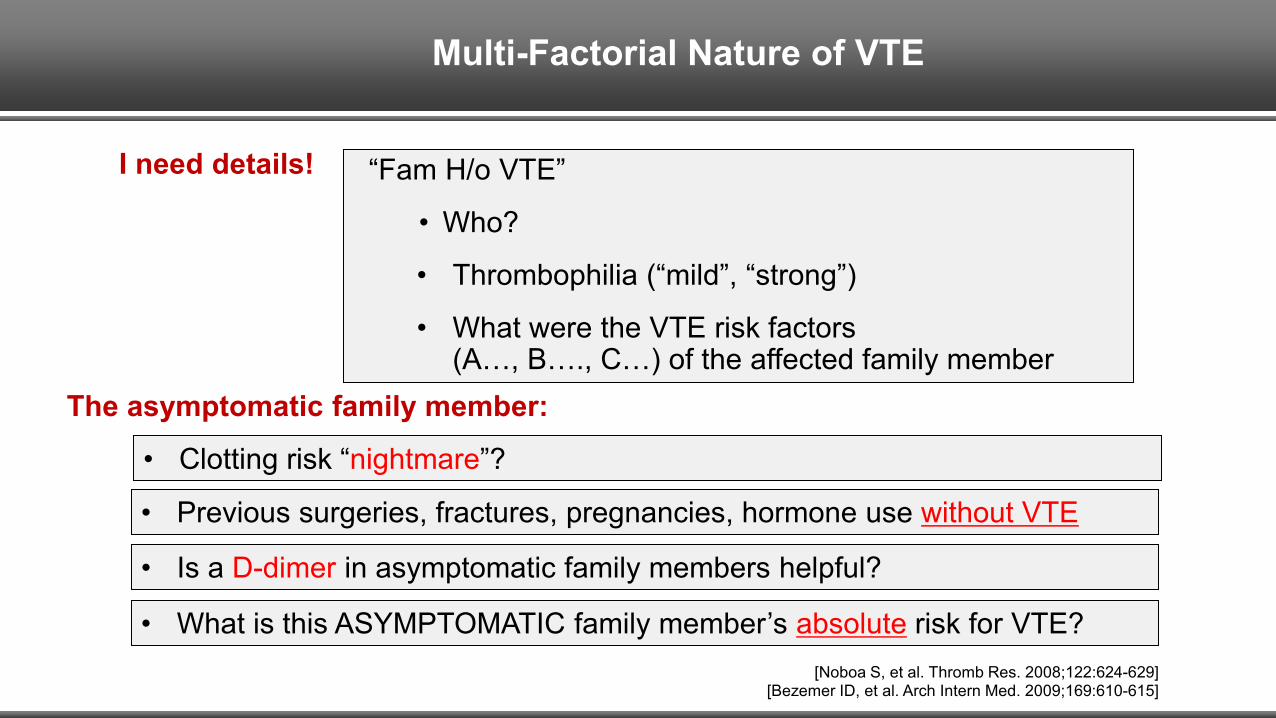
Multi-Factorial Nature of VTE
“Fam H/o VTE”
• Who?
• Thrombophilia (“mild”, “strong”)
• What were the VTE risk factors (A…, B…., C…) of the affected family member
[Noboa S, et al. Thromb Res. 2008;122:624-629]1. [Bezemer ID, et al. Arch Intern Med. 2009;169:610-615]
I need details!
• Previous surgeries, fractures, pregnancies, hormone use without VTE
• What is this ASYMPTOMATIC family member’s absolute risk for VTE?
• Is a D-dimer in asymptomatic family members helpful?
The asymptomatic family member:
• Clotting risk “nightmare”?
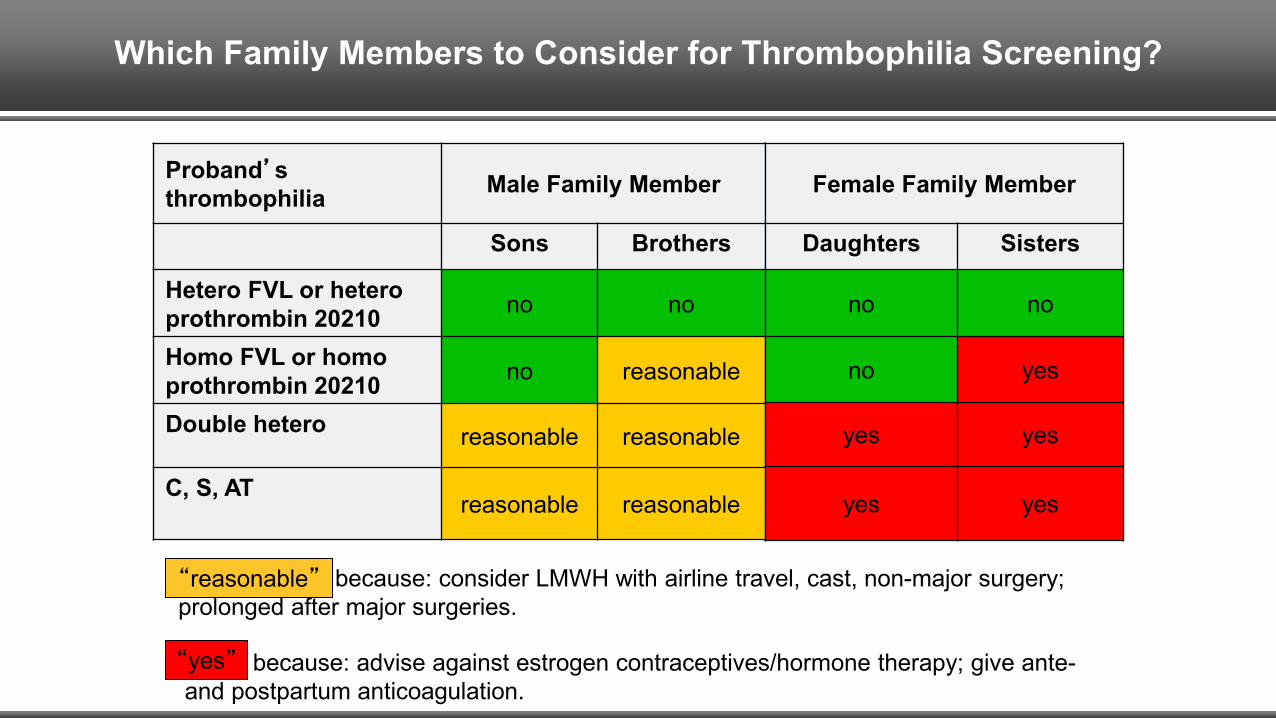
Which Family Members to Consider for Thrombophilia Screening?
Proband’s thrombophilia Male Family Member
Sons Brothers
Hetero FVL or hetero prothrombin 20210 no no
Homo FVL or homo prothrombin 20210 no reasonable
Double hetero reasonable reasonable
C, S, ATreasonable reasonable
Female Family Member
Daughters Sisters
no no
no yes
yes yes
yes yes
“Reasonable” because: consider LMWH with airline travel, cast, non-major surgery; prolonged after major surgeries.“reasonable”
“Yes” because: advise against estrogen contraceptives/hormone therapy; give ante-and postpartum anticoagulation.
“yes”
[Moll S. J Thromb Thrombolys 2015;39:367-378]
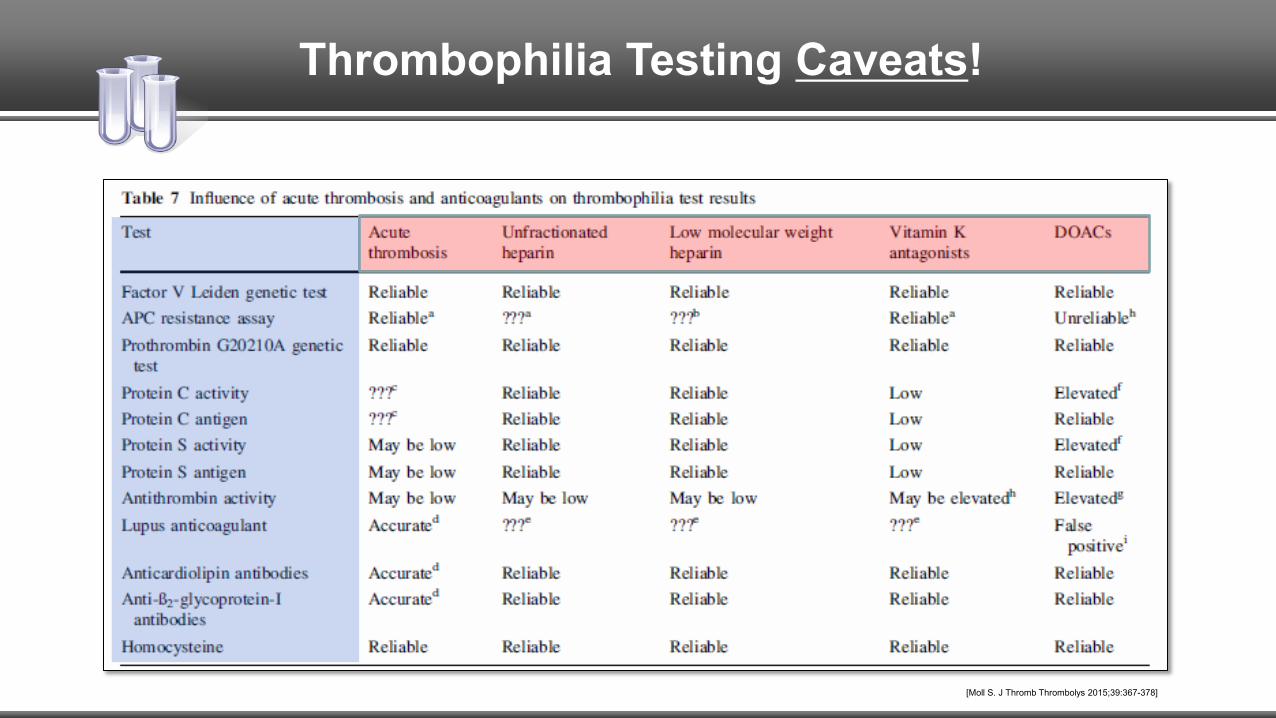
Thrombophilia Testing Caveats!
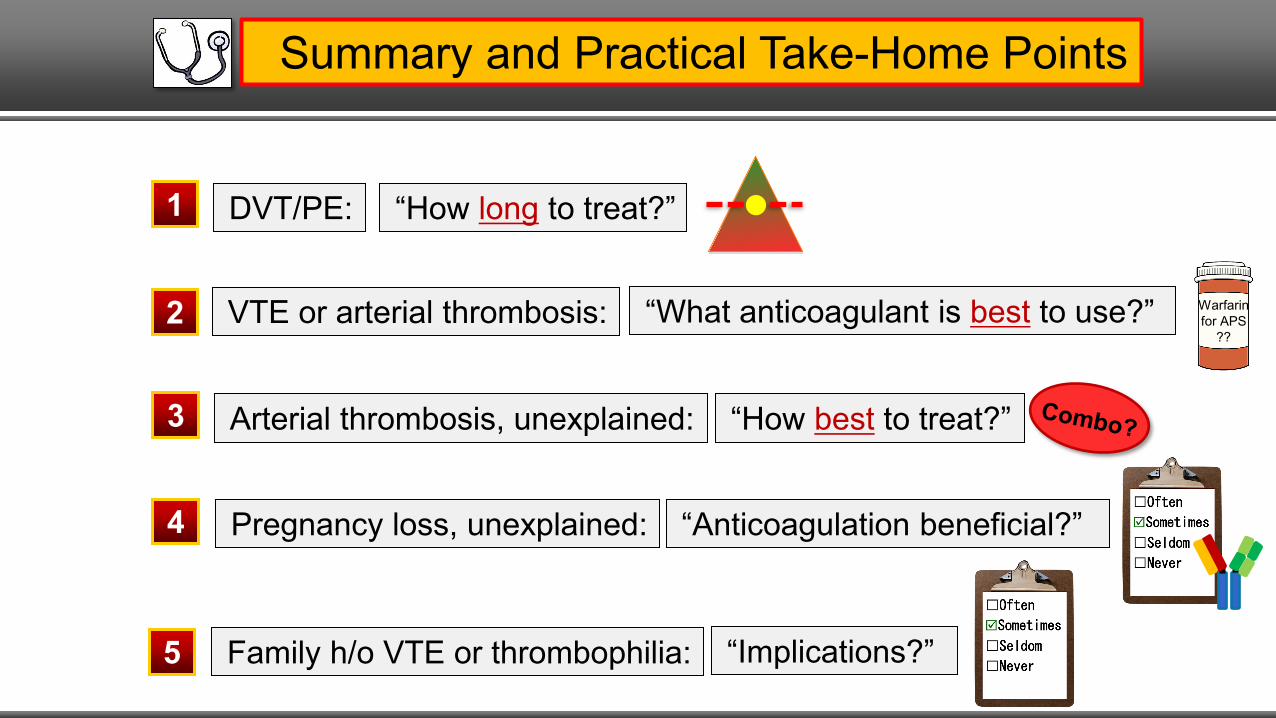
Summary and Practical Take-Home Points
Arterial thrombosis, unexplained:3 “How best to treat?”
DVT/PE:1 “How long to treat?”
2 VTE or arterial thrombosis: “What anticoagulant is best to use?” Warfarin for APS
??
Family h/o VTE or thrombophilia:5 “Implications?”
4 Pregnancy loss, unexplained: “Anticoagulation beneficial?”
Comments?
Questions?