
Presented By: Barbara Furry, RN-BC, MS, CCRN, FAHADirector The Center of Excellence in EducationDirector of HERO
Follow me on Twitter!CEE Med Updates@BarbaraFurryRNLike me on Facebook!


Essential physiologic signs of life
Essential assessment for treatment of critical illness
Early assessment using the 10 Early Signs and intervention will: Decrease morbidity & mortality Reduce unexpected cardiac arrests

A. RespirationsB. Blood pressureC. TemperatureD. Heart rate
Resp
iratio
ns
Blood
pres
sure
Temp
erat
ure
Hea
rt rat
e
74%
11%11%5%
1. Pulse
2. Temperature
3. Blood pressure
4. Respirations
The 'Lady-in-Chief', Florence Nightingale
5. Pain – the fifth vital sign
6. Level of consciousness
7. O2 saturation / capillary refill/color
8. Urine output
9. SVO2/ScVO2
10.Base excess or lactic acid
(reflect global tissue perfusion)

Pulse: < 50 or > 90
Temperature: > 100.4
Temp < 96.8
Respiratory rate: < 8
or > 20
Blood pressure:
SBP< 90 or MAP < 60
Pain:New or sig >
Level of consciousness:
Anxiety, lethargy, stupor
Oxygen saturation: <90%
or > FIO2
Urine output: < 100ml/4hr
Capillary refill: > 3 sec
Lab: BE< 5mmol/L
LA > 2.0mml/L and or
Normal: 60 – 80 bpm at rest
Significant abnormality: < 50 or > 90/min
Pulse character and number of contraction by palpation/min

Strength of pulse reflects the difference between the systolic and diastolic pressure (stroke volume)
130/40 strong pulse andhigh stroke volume
90/75 is a weak pulse andlow stroke volume

Physiologic response to increase cardiac demand Fever
Hypovolemia
Anemia
Hypoxemia or
increased work of
breathing
− Systemic inflammatory response syndrome (SIRS)
− Sepsis
− Increase catecholamines (pain, anxiety, dopamine, dobutamine)
− Sick sinus syndrome
− Hyperthyroidism
Significant bradycardia: heart rate < 50/min in non athletes
Causes:
SINUS BRADYCARDIA
– Sick sinus syndrome common in elderly
– Hypothermia
– Beta blockers – Hyperkalemia
– Coronary ischemia – Digoxin

D/C beta blocker, digoxin, etc.
Atropine (check rhythm first!)
Dopamine/epinephrine gtt
External or internal pacing
T < 101°F low‐grade
Inflammation; i.e., surgery, pancreatitis, atelectasis
Infection
T > 101F frequently signifies infection
T > 104.5°F may need aggressive treatment to decrease delirium, seizures, insensible fluid loss

Elevated temperature is normal response to cytokines released from monocytes
Inflammation causing fever Atelectasis – Trauma Surgery – Infection Pancreatitis
Fever due to infection and atelectasisneeds to be diagnosed becauseof therapeutic implications
New fever > 38.3°C (101°F) should trigger a patient assessment focused on possible infection
Change in LOC
Lung sounds, cough, sputum production
Abdominal pain, ileus, nausea/vomiting, diarrhea
Invasive lines, drains, foley catheter
Does the patient need pan cultures,antibiotics and/or re‐assessment by MD?

Decreased blood flow/cardiac output
Decreased metabolic rate
Vasoconstriction‐can lead to peripheral ischemic tissue damage
Prolonged PT/PTT and bleeding
Used in the treatment of post‐cardiac arrest to reduce CNS injury from anoxia
Used in cardiac and neurosurgery for cardio and neuro‐protection

Most inaccurate charted vital sign Measured for 1 min
Significant differences in rates foundbetween 15 sec vs. 1 min
Approx. 500 ml of air/breath (tidal vol.)
6‐8 liters of air/min (min ventilation)

Sensitive but not specific indicator or sign of critical illness
Assessment : Rate Depth ‐ shallow, normal or deep Regularity Lung sounds
Tachypnea should be an indicator to perform assessment of other nine early signs + ABG

Significant drop in RR or a rate < 8, consider CNS depression
− Narcotics
− Sedatives
− CO2 retention/narcosis
− Brain stem compression, usually associated with dilated pupils

Appropriate cuff size and location Dynamap frequently inaccurate in seriously ill patients
Best method (in order)
Arterial line
Doppler
Stethoscope with auscultation or palpation
Dynamap

Pressure vs. Flow
Need both pressure and flow for organ perfusion
In CPR, may generate systolic pressures of 90 but very low flow (CO)
Septic shock (volume‐resuscitated) high flow state but low blood pressure
Need both adequate pressure and flow (cardiac output) in
order to have adequate organ perfusion

CO x SVR70
MAP =

5L x 1200 dynes/sec 70
8L x 800 dynes/sec70
3L x 2000 dynes/sec70
MAP 85 =
MAP 91 =
MAP 85 =

When MAP < 60 perfusion is diverted to:(in order of importance)
• Coronary arteries
• Brain
• Abdomen– Kidneys– Liver– Bowel– Gallbladder
• Extremities
If intravascular volume status adequate, assess cardiac output / function:
Capillary refill
Urinary output
Multi‐lead EKG
BNP / Troponins
Echocardiogram to assess ejection fraction
Medications; beta blockers

If volume status and cardiac function adequate, assess vascular resistance
Rule out SIRS/sepsis
▪ Fever
▪ Tachypnea
▪ Tachycardia
▪ Elevated WBC or elevated bands
▪ Organ dysfunction
Medications; anti‐hypertensives, narcotics
SIRS: Fever, tachypnea, tachycardia, elevated WBCs or elevated bands
Organ dysfunction
▪ Cardiovascular; hypotension, or requiring vasopressors
▪ Renal; creatinine >2 or oliguria
▪ Pulmonary; PaO2/FiO2 (P/F ratio) <300
▪ Bilirubin > 2
▪ Hematologic; platelet count < 100,000 cell/mm

Fluid bolus of 500cc NS for hypovolemia
Withdraw of any offending medications
Narcan for narcotic induced
Ramazicon for benzodiazepine induced
Atropine or pacing for bradycardia; pressors for low SVR or cardiac causes

One of the most important symptoms Directs clinicians to where the problem exists and what the Dx may be
An important initial assessment tool If pain eliminated before assessment, incomplete clinical picture may result
Chronic pain Can lead to depression, may depress immune response, and decreases life expectancy
Normal: Awake, alert and oriented to person, place, time and situation (oriented x 4)
Abnormal LOC progression Anxiety → confusion → agitation → delirium
Anxiety → apathy → lethargy → stupor → coma
Glasgow coma scale: objective LOC assessment Eye opening
Verbal response
Motor responseBEST}

Glasgow Coma Scale
Eye Opening (E) Verbal Response (V) Motor Response (M)4=Spontaneous3=To voice2=To pain1=None
5=Oriented4=Confused3=Inappropriate words2=No words....only sounds1=None
6=Follows commands5=Localizes to pain4=Withdraws to pain3=Abnormal flexion2=Abnormal extension1=None
Total = E+V+M
GCS15 = 4+5+6

Sepsis, significant Na, BS, renal, hepatic abnormality or dysfunction
Hypoperfusion, hypercapnia, over sedation, increased ICP
Hypoxia, sedative withdraw, toxic ingestion, psychotic break
Anxiety Anxiety↓ ↓
Apathy Confusion↓ ↓
Lethargy Agitation↓ ↓
Stupor Delirium↓
Coma

Thorough assessment and diagnosis of cause of change in level of consciousness, including
Focused neuro exam and GCS
Assessment of other 9 early signs
Electrolytes
ABGs
Medication record
Airway and respiratory support i.e., Oxygen administration Nasal or oral airway BiPAP Intubation
Hemodynamic support treating hypoperfusion
Hold sedatives, narcotics Administer Narcan, Ramazicon etc.
Normal: 94 – 100%
Significantly abnormal: < 90%
Reflects Hg saturation i.e., % of heme binding sites saturated with oxygen
O2 content reflects sat and amount of Hb
There is 1.34 ml O2 /100 ml blood at 100% Hb saturation
O2 content = %sat x Hb x 1.34
95% O2 sat x 14 gm/Hb x 1.34 =17.8ml O2 / 100ml blood
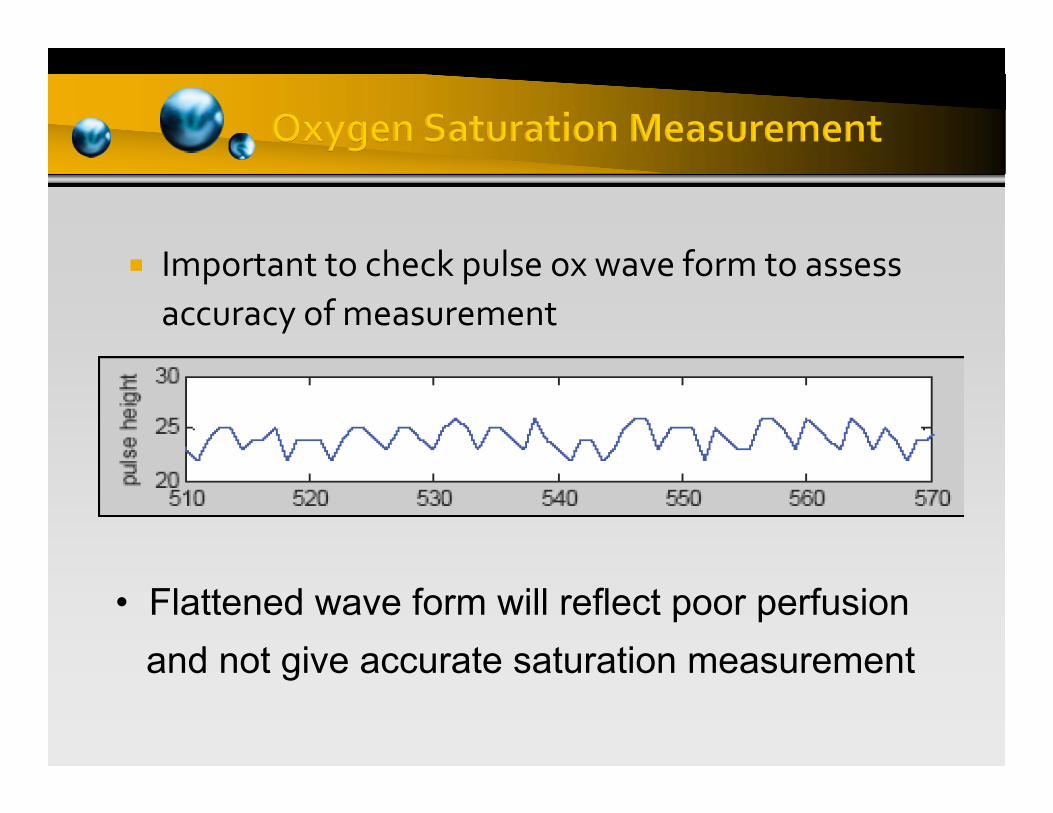
Important to check pulse ox wave form to assess accuracy of measurement
• Flattened wave form will reflect poor perfusion and not give accurate saturation measurement

Hypoxemia leads to
Anaerobic metabolism at the tissue level
Increased lactic acid production
Decreased energy production and loss of tissue energy stores (ATP)
Hypoxia leads to multi‐organdysfunction and Hypoxic Shock

Hypoxemia is an important and potentially avoidable cause of morbidity and mortality
Rapidly leads to Deteriorating LOC
Loss of respiratory and cardiovascular compensation
Cardiovascular instability
Respiratory / Cardiac Arrest

Ensure proper pulse oximeter probe placement verified by evaluating waveform on monitor
Decrease motion of extremity where probe placed
Check ABGs if needed
Nasal cannula
Ventilation mask vs. 100% non‐rebreather
High‐flow 100% mask
Bi‐pap
Intubation
A. TrueB. False
True
False
42%
58%
Our window to perfusion of the abdominal compartment
Normal: 30 ml/hr or 0.5/kg/hr
Abnormal: < 29 ml/hr for 2 consecutive hours < 400 ml/24 hours
Reflects renal arterial blood flow
Order of abdominal perfusion with low BP: Kidneys Liver Small bowel Colon Gallbladder
If kidneys are not being perfused, all other abdominal organs are at high risk for ischemia
If urine output low: Review prerenal issues
▪ Volume status
▪ Cardiac output and vascular resistance
Post‐renal: Use bladder scanner to determine if bladder emptying problem
If pre‐renal and post‐renal assessments are normal, problem is likely renal

Normal: < 2 seconds Abnormal: > 3 secondsCapillary refill time can be prolonged by:
• Low cardiac output
• Cold environment
• Vasospasm
• Arterial occlusive disease
If prolonged, indicates either
Inadequate pressure or flow to perfuse capillary bed
Cool extremities
Primary peripheral vascular problem:
▪ PVD
▪ Raynaud‘s

Increased capillary refill time is due to decreased tissue perfusion and need to assess:
Volume status
Pump status
Sepsis
Peripheral vascular disease
Hypothermia

A significant change in capillary refill time should trigger an immediate assessment of the other early signs
ANTICIPATE FLUID BOLUS
If O2 sat of venous blood is < 60% it reflects one or more of the following and requiresassessment of:
Hb
Art O2 % sat
O2 consumption at the tissues
CO / O2 delivery
If the following are unchanged:
Hemoglobin Arterial saturation O2 consumption
Temperature
Muscle activity
SVO2/ScvO2reflects
Cardiac Output
Significant abnormalities in the first five vital signs
– Temperature – Respiration– Pulse – Pain
– Blood Pressure/Color
– Level of consciousness – Base excess, lactic acid
– O2 saturation/Capillary refill
– ScvO2
– Urine output
• Should trigger the next five assessments
Proficiency in the 10 early signs will:
Decrease morbidity
Decrease mortality
Decrease codes








