
Inspection & Palpation Precordial buldge
• With the patient in the recumbent position, look tangentially while standing at the feet and the side of the patient
• Causes of precordial buldge 1. Disease since early childhood à congenital or rheumatic heart disease 2. Underlying disease as pericardial effusion and RVH
Scar
Median sternotomy (open heart surgery) • Valve replacement • Valve repair (vulvoloplasty) à Valve regurge • CABG
Lateral thoracotomy (clsed mitral vulvulotomy)
• Site: Left infra mammary • Mitral restenosis may be suspected • MR due to overcorrection may be suspected
Dilated veins
SVC obstruction • Mediastinal mass • SV thrombus
IVC obstruction
Pigmentation
Causes of pigmentation in malar area (butterfly pigmentation) • MS • SLE • Pellagra • Pregnancy
Pulsation
1. Apex 2. Left parasternal 3. Pulmonary 4. Aortic 5. Epigastric
Apex pulsation
Site
Left 5th intercostal space, midclavicular line, 3.5’’ or 9 cm from midline (normal) • LVH à outward and downward • RVH à outward • Child à 4th intercostal space • Thin and tall person à 6th intercostal space • Detrocardia à right side pulsation at 5th intercostal space • Ascites , pregnancy à above than 5th intercostal space
Extent
Localized : the maximal intensity constitute one space • LVH
Diffuse : the maximal intensity of pulsation at more than one space • RVH • LV aneurysm
Double apex (Rocking movement) à both ventricle hypertrophy, myocardial aneurysm
Character
Normal No special character
Hyperdynamic
• Forceful but non sustain • It indicates LV volume overload • Can be felt in case of
1. AR 2. Hyperdynamic circulation à pregnancy, anemia, etc
Heaving
• Forceful and sustain pulse • It indicates left ventricle pressure over load • Can be felt in case of obstruction at LV ejection à AS, coarctation of aorta, systemic
HTN Slapping • Brief apical impulse + palpable S1
• Cause by mitral stenosis
Thrill • Any abnormalities = organic murmur • Systolic thrill with the apical beat as in MR, with carotid pulsation • Diastolic thrill after the apical beat as in MS, away from carotid pulsation • Thrill at the base (aortic & pulmonary) as in AS, PS, PDA • Thrill at the parasternal à small muscular VSD • Thrill at the tricuspid area à diastolic: TS, systolic: TR
Absent apex pulse
1. Obese 2. Apex behind rib 3. Left pleural effusion or thickening or left pneumothorax 4. Emphysema 5. Pericardial effusion 6. Weak contraction or systolic retraction 7. Dextrocardia 8. Myxedema

Area Structure Anatomical location
Apex (mitral area) Apex of left ventricle Left 5th ICS, just inside MCL (below nipple)
Left parasternal 1. Right ventricle 2. Interventricular septum 3. Left atrium
Left sternal border to left MCL 3rd, 4th , 5th ICS
Tricuspid Tricuspid valve Lower end of left sternal border Right border Upper ½: ascending aorta & SVC
Lower ½: right border of right atrium Just behind or 1 cm lateral to right sternal border
Pulmonary Pulmonary artery Left 2nd ICS, in parasternal line First aortic (A1) Ascending aorta Right 2nd ICS, in parasternal line Second aortic (A2) Left ventricular outflow tract Left 3rdICS, in parasternal line
Waist
1. Left atrial appendage 2. Pulmonary artery 3. Left ventricular outflow tract
Left 3rd space and It measures from midline ½ space between midline and apex
Left infraclavicular Ductus atriosus Below medial 1/3 of left clavicle
Bare Right ventricle 4th, 5th ICS,
Mid sternal line to left parasternal line (4cm)
Epigastric Right ventricle Abdominal aorta Liver
From xyphisternal junction & umbilicus (upper half)
Epigastric pulsation Site Between xyphisternal junction and umbilicus
Structure 1. Liver 2. Abdominal aorta 3. Right ventricle
Hepatic pulsation • TR (systolic)
• TS (presystolic) • RVF (wavy) • High vascular hepatoma (systolic)
Abdominal aorta
pulsation • Aortic aneurysm (if tender à high risk to rupture) • Causes of big pulse volume à AR and others •
Right ventricle pulsation • RVH causes • Low diaphragm in emphysema
Pulmonary area Site Left second intercostal space
Causes • Pulsation:
o Pulmonary hypertension o Pulmonary artery dilatation o Aortic aneurysm o Left atrial enlargement
• Palpable S2 = diastolic shock = pulmonary hypertension • Systolic thrill à pulmonary stenosis, AS, VSD, PDA
Left parasternal area Site Left sternal border to left midclavicular line at 3rd, 4th , 5th intercostal space
Structure Right ventricular Causes Pulsation à RVH , marked LA dilatation due to severe MR
Systolic thrill à VSD, AS, PS, TR, MR Aortic area
Site Right second intercostal space Structure Ascending aorta Causes Pulsation à aortic dilatation except post stenotic
Palpable S2 = systemic hypertension Systolic thrill à AS, PS VSD
Others area Right parasternal
pulsation • Marked right atrial dilatation • Dextrocardia
• Ascending aortic aneurysm • Huge left atrium
Suprasternal pulsation • Unfolding (or aneurysm) of aortic arch or aneurysm
• Causes of visible carotid pulsation • Hyperdynamic circulation
• High aortic arch • Short obese person • Coaractation of aorta
Percussion
Right border of heart
1. Dullness at right sternal border à normal 2. Dullness inside right sternal border à heart is shifted to the left (left fibrosis/collapse) 3. Dullness outside right sternal border
o Right atrial enlargement o Severe left atrial enlargement o Pericardial effusion o Dextrocardia o Aneurysm in aortic arch root o Giant aneurysmal dilatation of left atrium o Pushed heart by left pleural effusion or pneumothorax
Apex of the heart
Causes of dullness outside the apex 1. Ventricular aneurysm 2. Pericardial effusion 3. Lung causes
Pulmonary area
Causes of dullness at pulmonary area 1. Pulmonary artery dilatation 2. Pericardial effusion 3. Aortic aneurysm 4. Left atrial dilatation or enlargement 5. Lung causes (collapse, fibrosis, tumor, consolidation)
Aortic area
Causes of dullness at aortic area 1. Aortic dilatation 2. Lung causes
Cardiac waist
Causes of dullness of cardiac waist 1. Left atrial dilatation 2. Pulmonary dilatation 3. Pericardial effusion 4. Lung causes
Bare area of
heart
Causes of large bare are 1. Right ventricular enlargement 2. Pericardial effusion 3. Retraction of lung by collapse or fibrosis
Causes of small (or resonant) bare area 1. Emphysema 2. Left pneumothorax 3. Dextrocardia
Lower end of sternum
Causes of stony dullness 1. Marked RVH 2. Pericardial effusion 3. Right lung causes
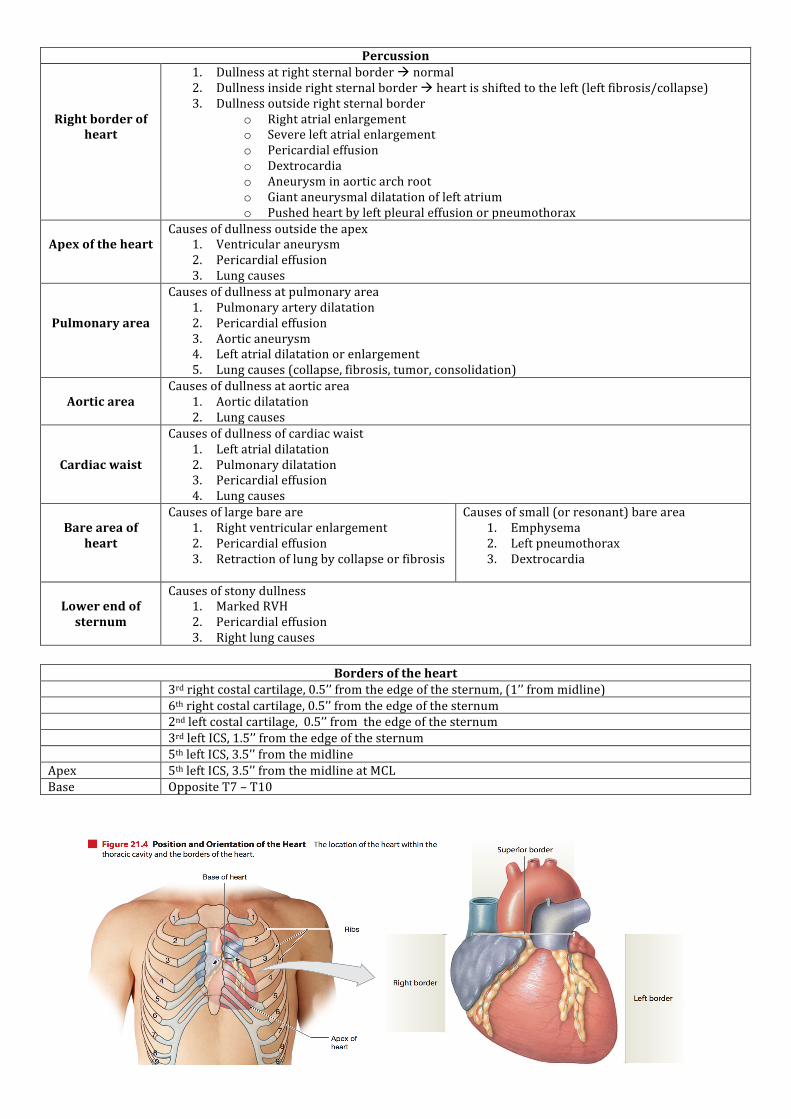
Borders of the heart
3rd right costal cartilage, 0.5’’ from the edge of the sternum, (1’’ from midline) 6th right costal cartilage, 0.5’’ from the edge of the sternum 2nd left costal cartilage, 0.5’’ from the edge of the sternum 3rd left ICS, 1.5’’ from the edge of the sternum 5th left ICS, 3.5’’ from the midline Apex 5th left ICS, 3.5’’ from the midline at MCL Base Opposite T7 – T10







