
PEDIATRIC ENDOCRINE PEDIATRIC ENDOCRINE EMERGENCIESEMERGENCIES
Malcolm S. Schwartz D.O., Malcolm S. Schwartz D.O., F.A.C.O.P.F.A.C.O.P.
Congenital Adrenal HyperplasiaCongenital Adrenal Hyperplasia
Congenital HypothyroidismCongenital Hypothyroidism
I have no Conflicts of InterestI have no Conflicts of Interest


Historical perspectiveHistorical perspective
30 BCE Vitruvius described the occurrence of 30 BCE Vitruvius described the occurrence of goiter in the Alpsgoiter in the Alps
1527 Paracelsus described relationship 1527 Paracelsus described relationship between hypothyroidism and mental between hypothyroidism and mental retardationretardation
Congenital Hypothyroidism
retardationretardation
1850 Curling described sporadic congenital 1850 Curling described sporadic congenital hypothyroidism with autopsy findingshypothyroidism with autopsy findings
1896 Pendred described goiter with deafness1896 Pendred described goiter with deafness
1897 Osler describes thyroid deficiency and 1897 Osler describes thyroid deficiency and sporadic cretinismsporadic cretinism

1891 use of thyroid extract1891 use of thyroid extract
1972 early treatment prevents MR1972 early treatment prevents MR
1972 filter paper assay1972 filter paper assay
1974 first congenital hypothyroidism 1974 first congenital hypothyroidism
Congenital Hypothyroidism
Historical perspectiveHistorical perspective
1974 first congenital hypothyroidism 1974 first congenital hypothyroidism newborn screening newborn screening

1960 1970 1980 200019902001 2002 2003 2004 2005
Timeline of Newborn Screening in New Jersey 1960s to 2005
NSARCNBS Advisory Panel
CH GAL Hgb
MS/MS
PKU
CAH
MSUD
BIO
CF
4FAO
2UCD
6OA
29 HRSA

Thyroid Embryology
The thyroid is the first endocrine gland to develop in the embryo, starting during the third week of gestation.
The thyroid derives from an epithelial proliferation of the floor of the pharynx: a thickening between the first and second pharyngo-bronchial pouches (later the foramen cecum) becomes the thyroid diverticulum.
[As we discuss this you can imagine that, at each point in the discussion, something can go wrong that would ultimately affect thyroid function in the newborn infant.]

Thyroid Embryology
By seven weeks the thyroid gland has attained its final shape and has reached its final location in the neck. The thyroglossal duct has normally degenerated and disappeared.
Thyroid Anatomic Abnormalities
Anatomic abnormalities may lead to later clinical problems if
1.the gland is missing (Athyreosis)
2.both lobes are absent (not so rare)
3.the gland is “dysgenetic” (i.e., it does not develop normally)
4.the gland is ectopic
5.it remains at the base of the tongue (lingual thyroid)5.it remains at the base of the tongue (lingual thyroid)
6.thyroid cells remain along the downward tract of the gland
7.the gland does not descend far enough, or descends too far
8.the gland is hypoplastic
9. one lobe is absent (rare)
10.the thyroglossal duct fails to degenerate and disappear
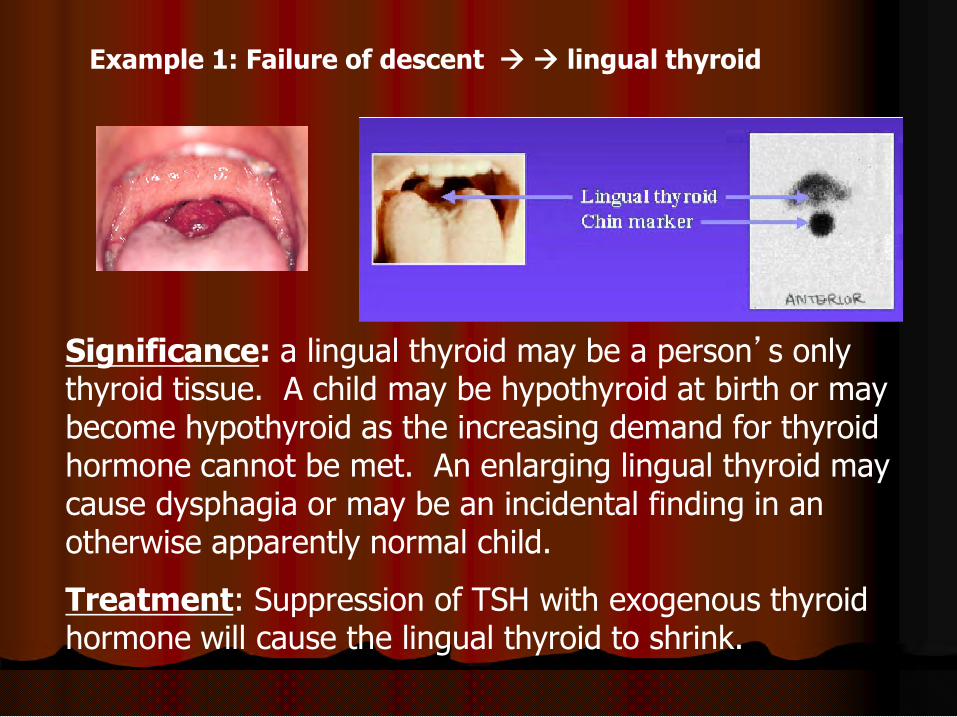
Example 1: Failure of descent lingual thyroid
Significance: a lingual thyroid may be a person’s only Significance: a lingual thyroid may be a person’s only thyroid tissue. A child may be hypothyroid at birth or may become hypothyroid as the increasing demand for thyroid hormone cannot be met. An enlarging lingual thyroid may cause dysphagia or may be an incidental finding in an otherwise apparently normal child.
Treatment: Suppression of TSH with exogenous thyroid hormone will cause the lingual thyroid to shrink.

Example 2 : failure of the thyroglossal duct to degenerate
A midline mass may appear at any time anywhere from just below the base of the tongue to just above the normal location of the thyroid.
The mass may be cystic if the duct fails to atrophy, or solid if there are thyroid tissue remnants.
Since the thyroglossal duct is attached to the base of the tongue, the mass to the base of the tongue, the mass moves upward in the neck when the tongue is protruded from the mouth.
Significance: a solid mass might simulate metastases from a primary cancer site; a cystic lesion might
become infected.
Congenital Hypothyroidism
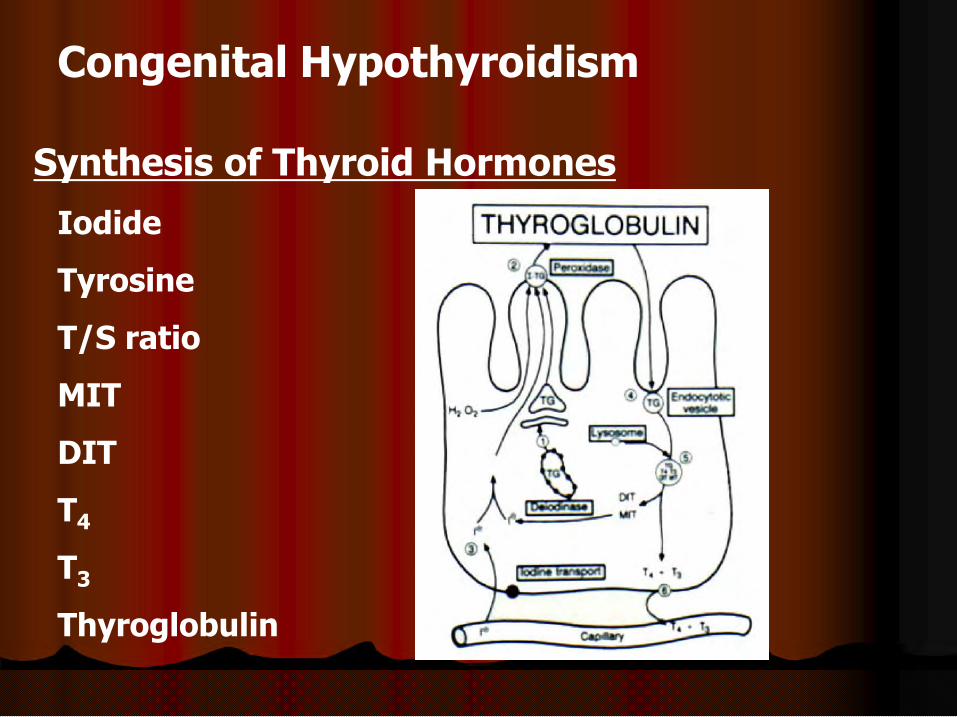
Synthesis of Thyroid Hormones
Iodide
Tyrosine
T/S ratio
MIT
DIT
T4
T3
Thyroglobulin

Once we have the anatomic thyroid gland, that gland must produce thyroid hormones. Here is the most simplistic view of
Thyroid Hormone Synthesis
Iodine (actually, iodide) is taken up by thyroid gland, attaches to tyrosine (residues) to form T3 (tri-iodo-thyronine) and T4 (thyroxine) which are released into the circulation.

Thyroid Hormone Synthesis
A little more detail … synthesis of T4
Note that the synthesis process takes place with tyrosine residues attached to thyroglobulin.
There is also mono-iodotyrosine
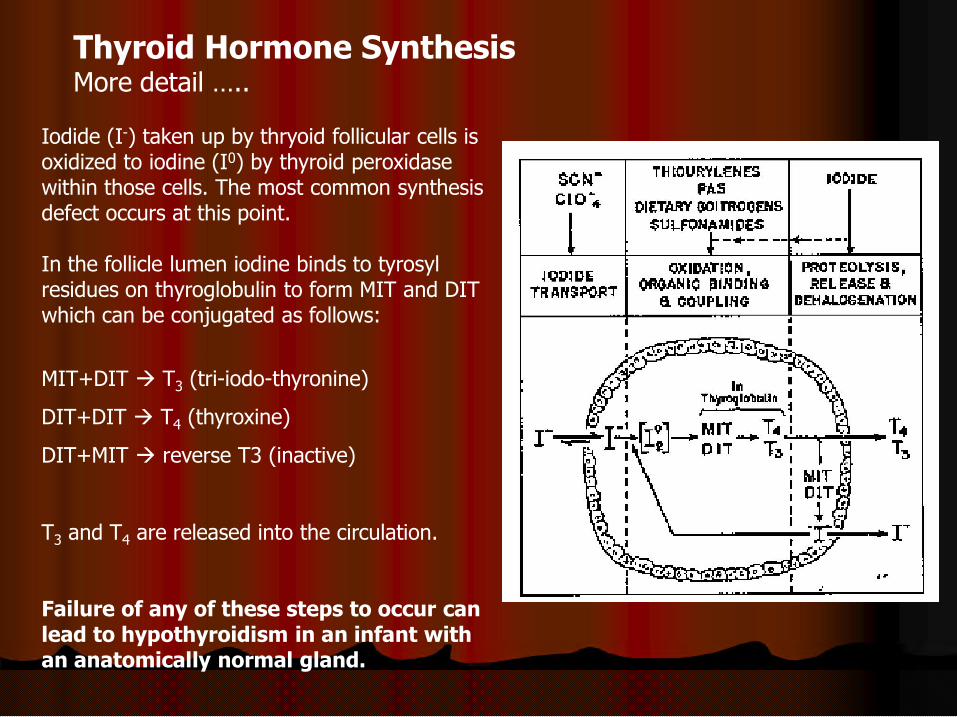
Thyroid Hormone SynthesisMore detail …..
Iodide (I-) taken up by thryoid follicular cells is oxidized to iodine (I0) by thyroid peroxidase within those cells. The most common synthesis defect occurs at this point.
In the follicle lumen iodine binds to tyrosyl residues on thyroglobulin to form MIT and DIT which can be conjugated as follows:
MIT+DIT T3 (tri-iodo-thyronine)
DIT+DIT T4 (thyroxine)
DIT+MIT reverse T3 (inactive)
T3 and T4 are released into the circulation.
Failure of any of these steps to occur can lead to hypothyroidism in an infant with an anatomically normal gland.

Congenital Hypothyroidism
Metabolism of Thyroid Hormones
•T4
•T3
•TBG
•TBPA

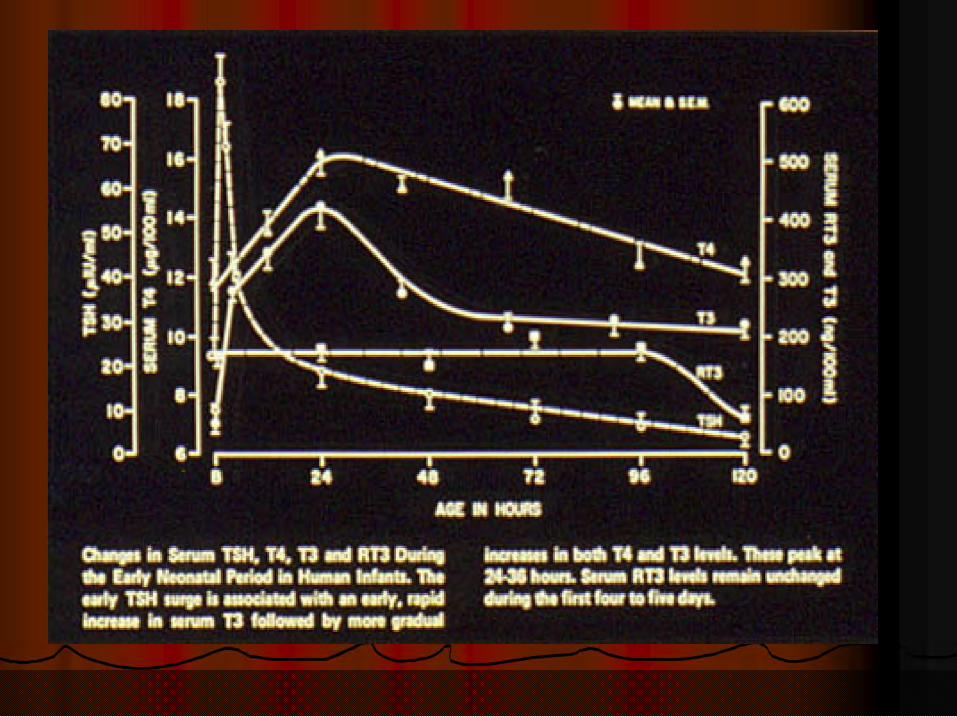
Development of Human Thyroid FunctionHormone levels throughout gestation
Note:
1. the thyroid can concentrate iodine by 10 weeks.
2. thyroid hormones begin to appear by the end of the first trimester,
3. thyroxine-binding globulin appears by 10-12 weeks, and
4. feedback control mechanisms are functioning by the end of the second trimester
Wolf-Chaikoff effect: Iodine excess causes hypothyroidism by inhibiting iodide organification and T4 and T3 synthesis. Normal people “escape” from this effect. People with abnormal thyroid glands (e.g. autoimmune thyroiditis) can become hypothyroid if given iodine for more than a few days. The excess iodine could come from OTC products, such as cough medicines, some dietary supplements, drugs such as amiodarone, or radiographic contrast.

Control of Thyroid Hormone Synthesis and Release
Negative Feedback
A classic negative feedback system controls synthesis and release of thyroid hormone:
When free T3 and T4 levels are low, their suppressive effect on the hypothalamus and pituitary is removed. Thyrotropin-Releasing Hormone (TRH) then stimulates Releasing Hormone (TRH) then stimulates release of thyrotropin (aka TSH = thyroid stimulating hormone), which in turn activates T3 and T4 synthesis and release.
Conversely, when free T3 and T4 are high, release of TRH and TSH is inhibited.
Peripheral conversion of T4 to T3 is also regulated, e.g., in response to illness.

Relation of Maternal, Placental and Fetal
Thyroid Hormones
Note:
1. Some maternal T4 and T3 are delivered to the fetus. [Delivery of T3 is especially important for brain development in the hypothyroid infant.]
2. T4 can be de-iodinated to the more 2. T4 can be de-iodinated to the more active T3 by the mother, placenta and fetus.
3. T4 can also be de-iodinated to the inactive reverse T3 by the mother, placenta and fetus.

Placental Transfer

Development of Human Thyroid FunctionMore details near birth
Note that premature infants tend to have lower levels of T4 and T3 than term infants, and may have various forms of hypothyroxinemia (low T4) without hypothyroidism (normal TSH)
This has more than academic interest.
TSH)
This fact, especially in the sick premature infant, can lead to uncertainty about whether or not these infants need thyroid replacement therapy.

And some definitions:
Problems at the level of the thyroid gland are called “primary”.
Problems at the level of the pituitary gland are called “secondary”.
Problems at the level of the hypothalamus are called “tertiary”.

Congenital Hypothyroidism

Congenital Hypothyroidism

Congenital Hypothyroidism

Congenital hypothyroidism
Differential diagnosis (with rate of occurrence)
1. Something intrinsically wrong with the thyroid “primary hypothyroidism”
Dysgenetic (ectopic, hypoplastic); usually random: 1/4,000 birthsSynthesis (enzyme) defect; autosomal recessive inheritance; 1/40,000
2. Something wrong with the pituitary (“secondary hypothyroidism”) or hypothalamus 2. Something wrong with the pituitary (“secondary hypothyroidism”) or hypothalamus (“tertiary hypothyroidism”): 1/100,000
3. Transient hypothyroidism (1/40,000) where an otherwise normal thyroid gland is temporarily suppressed, mimicking primary hypothyroidism:
drug inducedmaternal antibodies that block the infant’s TSH receptor; resolves as
antibodies disappear. These antibodies can be measured.

Congenital Hypothyroidism
Congenital Hypothyroid Causes
•Thyroid dysgenesis 1:4000
•Agenesis
•Ectopic gland
•Thyroid Dyshormonogenesis 1:30,000
•Hypothalamic-Pituitary 1:100,000
•20 or 3 0 Hypothyroidism
•Transient Hypothyroidism 1:40,000
Congenital Hypothyroidism
Clinical signs and symptoms at birth
[Why is this page blank?][Why is this page blank?]
This page is blank because most babies with congenital hypothyroidism
appear completely normal at birth. That’s why we have a screening program!
However

However, if you look very closely at babies in the nursery you might find that some babies with congenital hypothyroidism have
a large posterior fontanel (greater than 1 cm)
a goiter (in a baby with a hormone synthesis defect)
Less than 5% of babies with congenital hypothyroidism are diagnosed by clinical exam. (That’s
why we have a screening program!)
The posterior fontanel is usually almost closed in the normal term infant. A large posterior fontanel reflects delayed skeletal maturation in utero that correlates with the degree of fetal hypothyroidism. A bone age X-ray after birth has prognostic value regarding the baby’s potential for intellectual development.

There are some clinical clues that appear gradually over weeks to months, and eventually will make the baby’s condition obvious:
in the newborn period
prolonged “physiologic” jaundice (more than 7 days)
gradually progressive symptoms
feeding difficulties; choking
sluggishness; lack of interest; little crying
large abdomen; umbilical hernia; constipationlarge abdomen; umbilical hernia; constipation
hypothermia; cold/mottled skin
retarded growth/development
Weight change
By the time these clinical signs lead to a diagnosis, there may have been irreversible intellectual impairment. (That’s why we have a screening program!)

Congenital Hypothyroidism
Thyroid Hormone Effects
•Metabolism
•Nutrients
•Inorganic Ions•Inorganic Ions
•Growth and Development
•Neurological Function

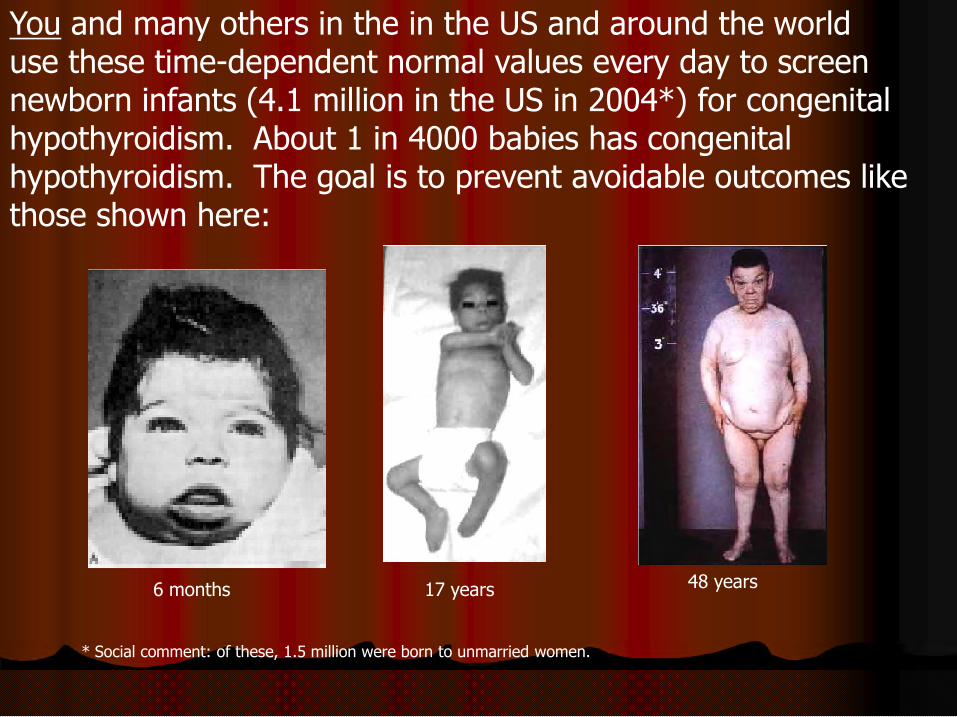
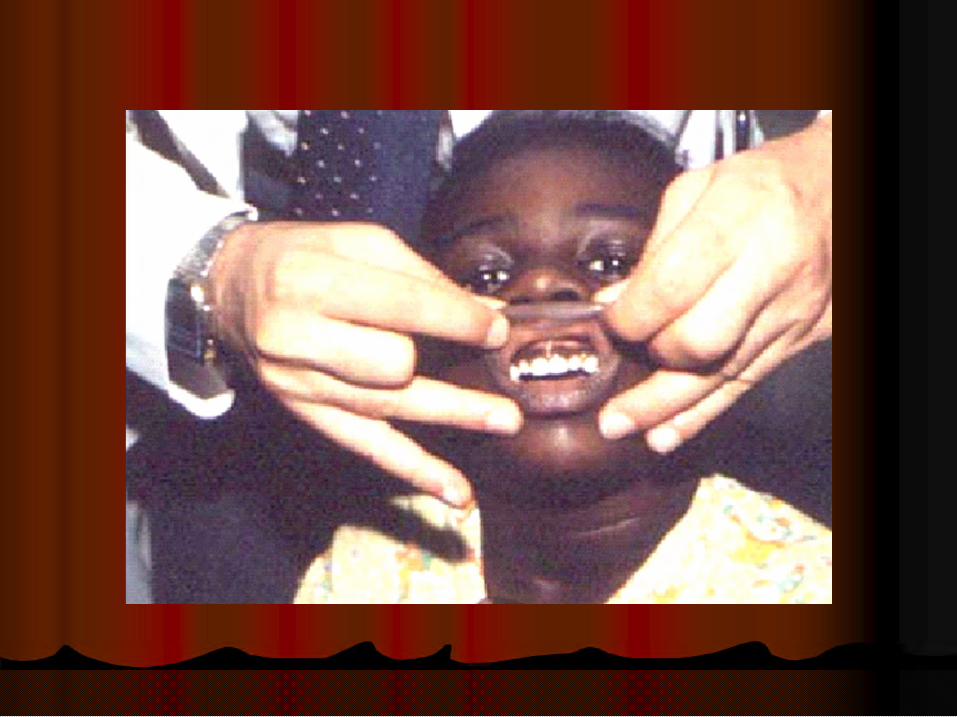
You and many others in the in the US and around the world use these time-dependent normal values every day to screen newborn infants (4.1 million in the US in 2004*) for congenital hypothyroidism. About 1 in 4000 babies has congenital hypothyroidism. The goal is to prevent avoidable outcomes like those shown here:
* Social comment: of these, 1.5 million were born to unmarried women.
6 months 17 years 48 years



Congenital Hypothyroidism


Congenital Hypothyroidism
Thyroid Function Tests
Serum Thyroid and pituitary Hormones
•TSH
•T4
•T3
•Free T4
•Free T3
•TRH Stimulation
•T3 UptakeX
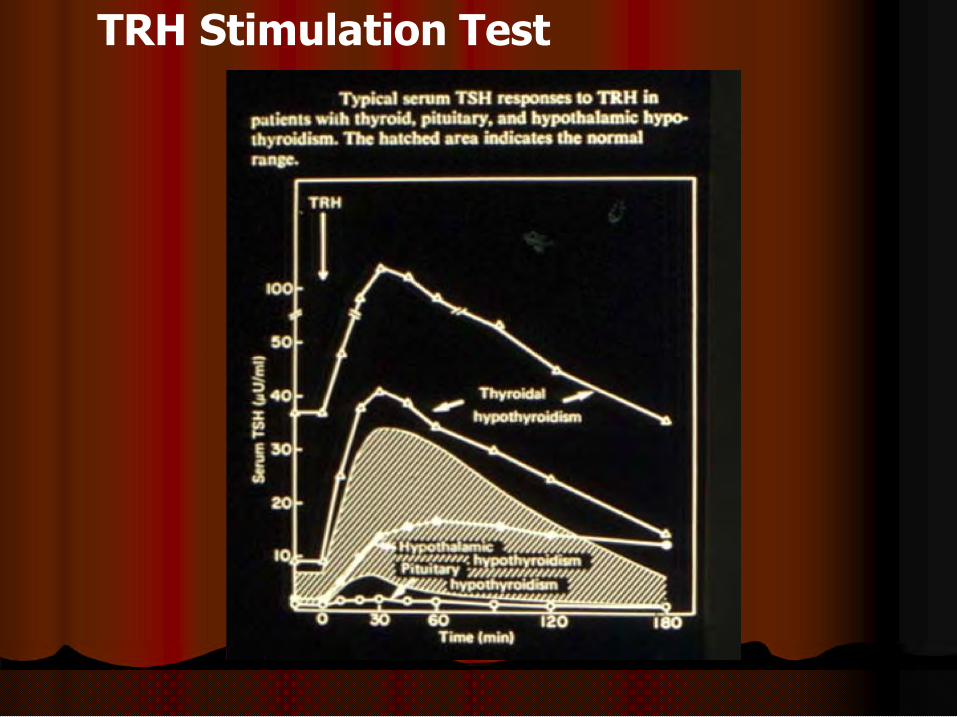
TRH Stimulation Test

Congenital Hypothyroidism
Radiologic Studies
•Bone age
Thyroid Imaging
•Ultrasound
•Radioisotope Scanning and Uptake•Radioisotope Scanning and Uptake
•TC99M
•I123
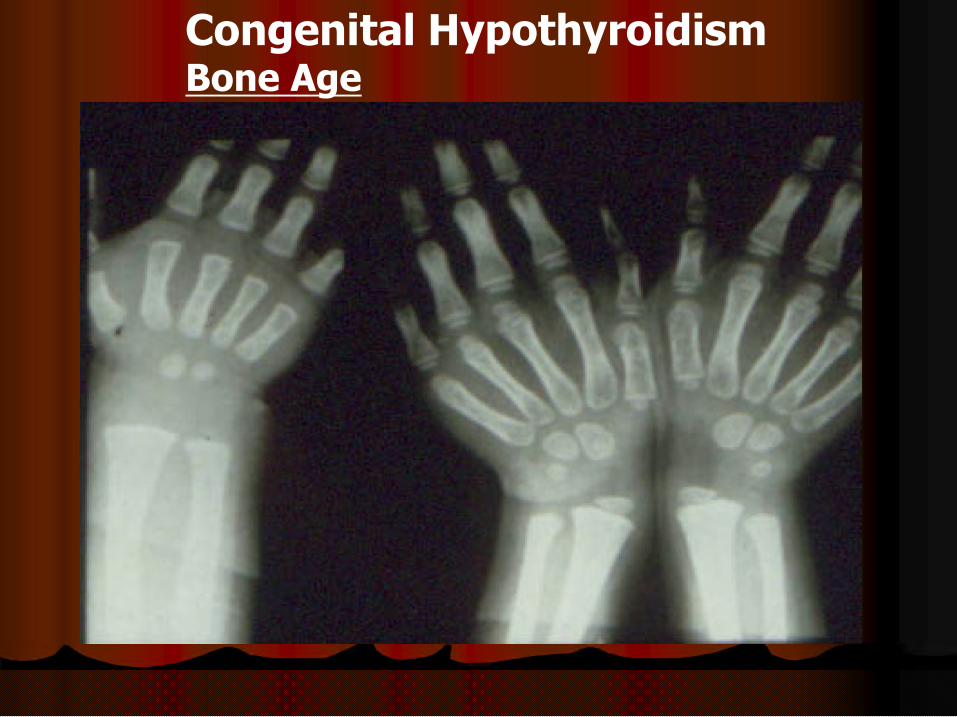
Congenital HypothyroidismBone Age

Congenital HypothyroidismBone Age

Congenital Hypothyroidism
Tests for Underlying Etiology
•Serum Antithyroid Antibodies
•Anti-Thyroglobulin•Anti-Thyroglobulin
•Anti-Thyroid Peroxidsase (TPO)
•Perchlorate Discharge

THYROID DISORDERS OF CHILDHOOD
FrFree Tee T4 4 0.3 ng/dl0.3 ng/dl 0.5 ng/dl0.5 ng/dl 0.8 ng/dl0.8 ng/dl
Why screen ?Why screen ?
Most cases are asymptomaticMost cases are asymptomatic When symptoms develop, damage may have When symptoms develop, damage may have
already occurredalready occurred
Early treatment can prevent mental retardationEarly treatment can prevent mental retardation
As early as possibleAs early as possible
Congenital Hypothyroidism
As early as possibleAs early as possible
Subsequent normal growthSubsequent normal growth
Severe in utero hypothyroidism is more likely Severe in utero hypothyroidism is more likely associated with mild developmental problems associated with mild developmental problems despite adequate treatmentdespite adequate treatment

SCREENINGSCREENING
US, Canada, western Europe, Israel, US, Canada, western Europe, Israel, Japan, Australia and New Zealand have Japan, Australia and New Zealand have developed programsdeveloped programs
Latin and South America, Eastern Europe, Latin and South America, Eastern Europe, Latin and South America, Eastern Europe, Latin and South America, Eastern Europe, Africa and Asia in processAfrica and Asia in process
Approximately 1250 cases in US & 7000 Approximately 1250 cases in US & 7000 cases worldwide detectedcases worldwide detected

ScreeningScreening
States vary in their use of T4, TSH or both States vary in their use of T4, TSH or both as primary screenas primary screen
After 24 hours of lifeAfter 24 hours of life
Statistical detection of lowest 10% T4Statistical detection of lowest 10% T4 Statistical detection of lowest 10% T4Statistical detection of lowest 10% T4
Secondary TSHSecondary TSH
TSH >20 mciu/ml needs secondary TSH >20 mciu/ml needs secondary confirmation with venous bloodconfirmation with venous blood
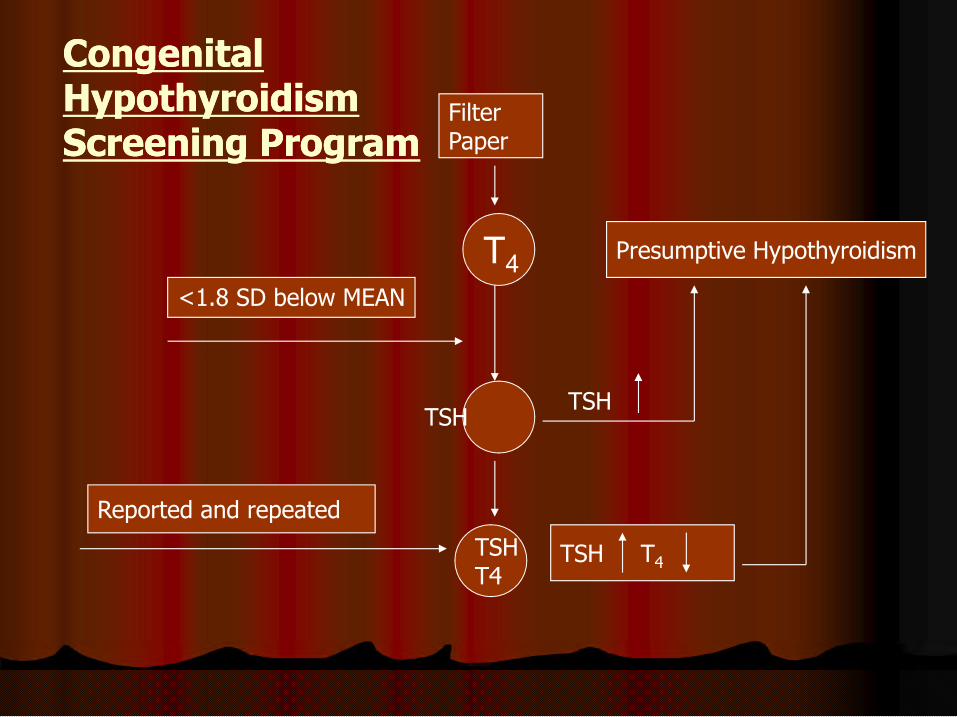
Presumptive HypothyroidismT4
<1.8 SD below MEAN
FilterPaper
Congenital Congenital HypothyroidismHypothyroidismScreening ProgramScreening Program
Reported and repeated
TSHT4
TSHTSH
TSH T4
Most common Most common presentationpresentation
Telephone call from the state newborn Telephone call from the state newborn screening follow up programscreening follow up program
FT baby born 5 days ago had a FT baby born 5 days ago had a presumptive positive for congenital presumptive positive for congenital
Congenital Hypothyroidism
presumptive positive for congenital presumptive positive for congenital hypothyroidism:hypothyroidism:
T4 T4 ““lowlow””
TSH > 100TSH > 100
What do I do? What do I do?
(even if it is Friday before Memorial Day)(even if it is Friday before Memorial Day)

Initial Steps for a Presumptive Initial Steps for a Presumptive PositivePositive
Immediate consultation with a pediatric Immediate consultation with a pediatric endocrinologistendocrinologist
Send serum for free T4, and TSH as Send serum for free T4, and TSH as directed by endocrinologistdirected by endocrinologistdirected by endocrinologistdirected by endocrinologist
If treatment is needed it should be If treatment is needed it should be initiated immediately in discussion with initiated immediately in discussion with consultantconsultant

3230
35
Severe Congenital HypothyroidismSevere Congenital HypothyroidismMental Prognosis vs. Age When Adequate Treatment Mental Prognosis vs. Age When Adequate Treatment InitiatedInitiated
32
14
21
12
2 2
4
7
2 0 2 3 1 13
2
27
11
12
00
5
10
15
20
25
30
Total Group 4 months 4-6 months 7-12 months 12 months
<50
50-69
79-89
>90
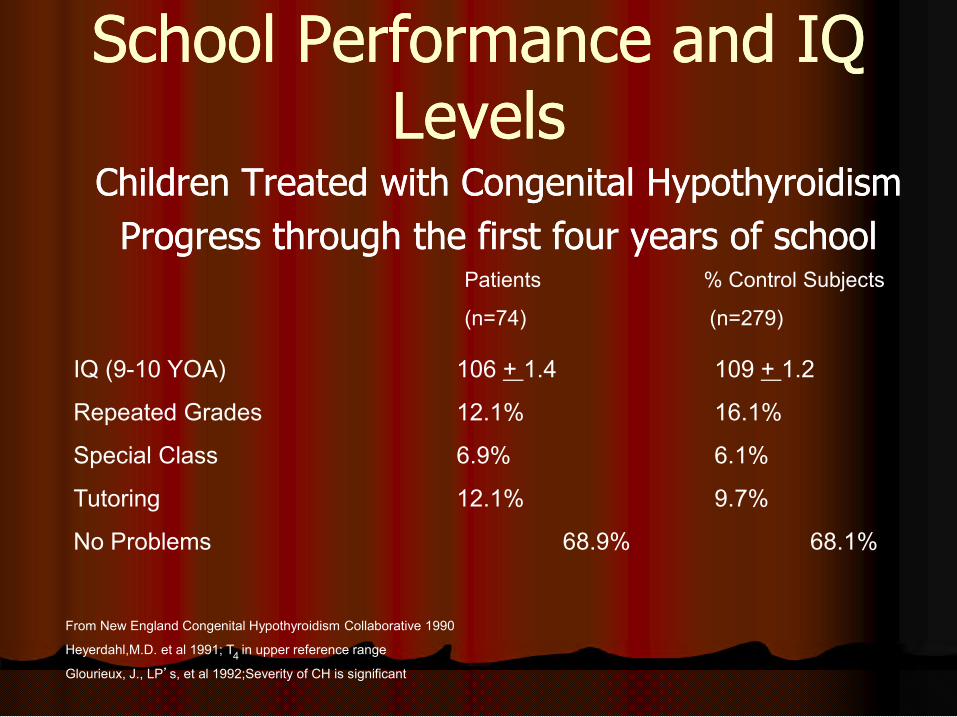
School Performance and IQ School Performance and IQ LevelsLevels
Children Treated with Congenital HypothyroidismChildren Treated with Congenital Hypothyroidism
Progress through the first four years of schoolProgress through the first four years of schoolPatients % Control Subjects
(n=74) (n=279)
IQ (9-10 YOA) 106 + 1.4 109 + 1.2
From New England Congenital Hypothyroidism Collaborative 1990
Heyerdahl,M.D. et al 1991; T in upper reference range
Glourieux, J., LP’s, et al 1992;Severity of CH is significant
IQ (9-10 YOA) 106 + 1.4 109 + 1.2
Repeated Grades 12.1% 16.1%
Special Class 6.9% 6.1%
Tutoring 12.1% 9.7%
No Problems 68.9% 68.1%
4
Rovet et. al.Rovet et. al.
80 children followed until 9 years of age80 children followed until 9 years of age
Sibling and classmate matched controlsSibling and classmate matched controls
At 6 years of age statistically significant 8 At 6 years of age statistically significant 8 point difference in McCarthypoint difference in McCarthypoint difference in McCarthypoint difference in McCarthy
At 9 and > 13 years, 9 point difference in At 9 and > 13 years, 9 point difference in WISCWISC--R and WISCR and WISC--IIIIII

Congenital Hypothyroidism TreatmentCongenital Hypothyroidism Treatment
Congenital Hypothyroidism
Age
Newborn (full term)
1-3 months
Levothyroxine (mcg/kg)
10-15 (50 mcg/day)
8-10
3-6 months
6-10 months
Maintenance
7-10
6-8
5-8
Follow clinical status monthly and thyroid function tests until stable. Then every 3-4 months

OutcomeOutcome
The earlier the treatment the betterThe earlier the treatment the better
Correlation between in utero Correlation between in utero hypothyroidism and poorer outcomehypothyroidism and poorer outcome
Complete agenesis vs. ectopic Complete agenesis vs. ectopic
Congenital Hypothyroidism
Complete agenesis vs. ectopic Complete agenesis vs. ectopic
Specific learning difficultiesSpecific learning difficulties
Visuospatial deficitsVisuospatial deficits
Memory and attention problemsMemory and attention problems

[Note: the earlier the infant is treated, the better prognosis for intellectual development. After six weeks untreated, the prognosis becomes much worse. If treatment is started in a case where the diagnosis is uncertain it should be continued for 3 years until brain development is essentially complete.]

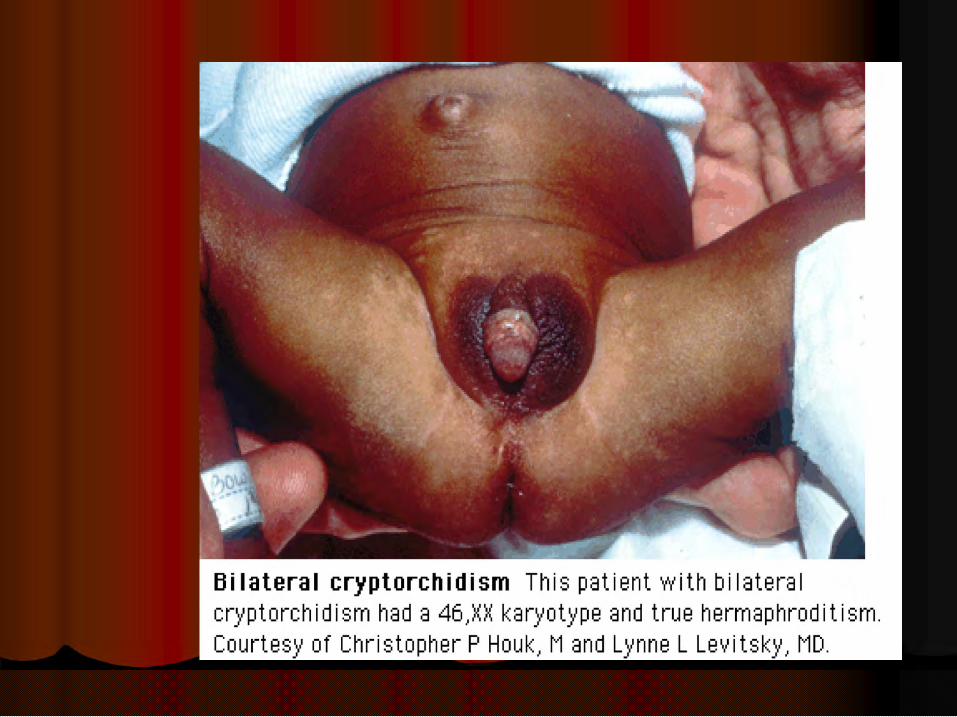
Congenital Adrenal Hyperplasia Congenital Adrenal Hyperplasia
Adrenal InsufficiencyAdrenal InsufficiencyAdrenal InsufficiencyAdrenal Insufficiency




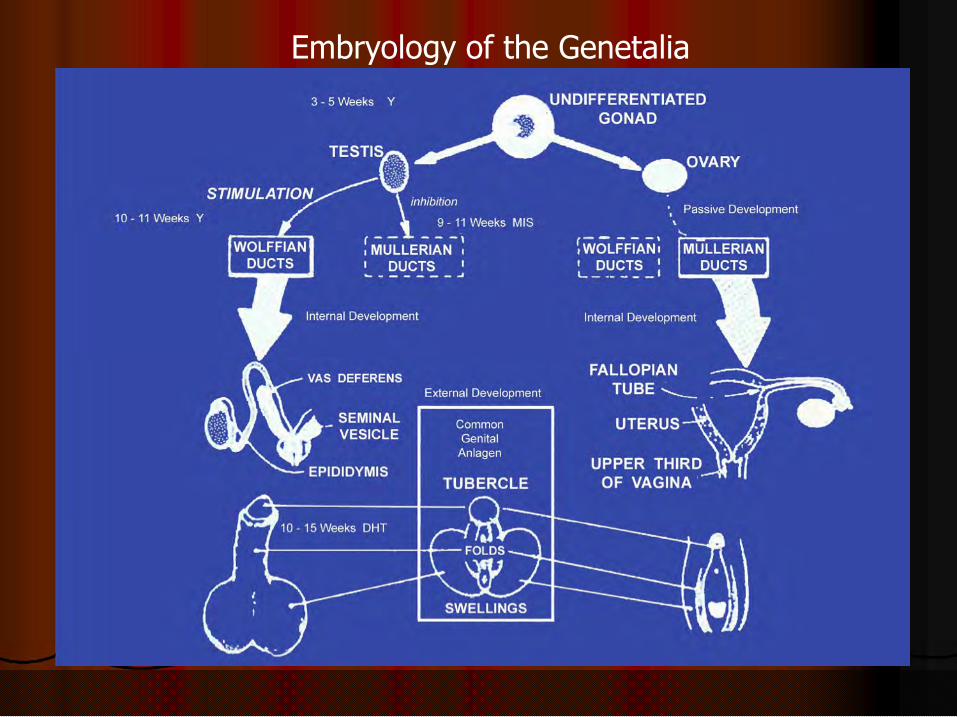
Embryology of the Genetalia






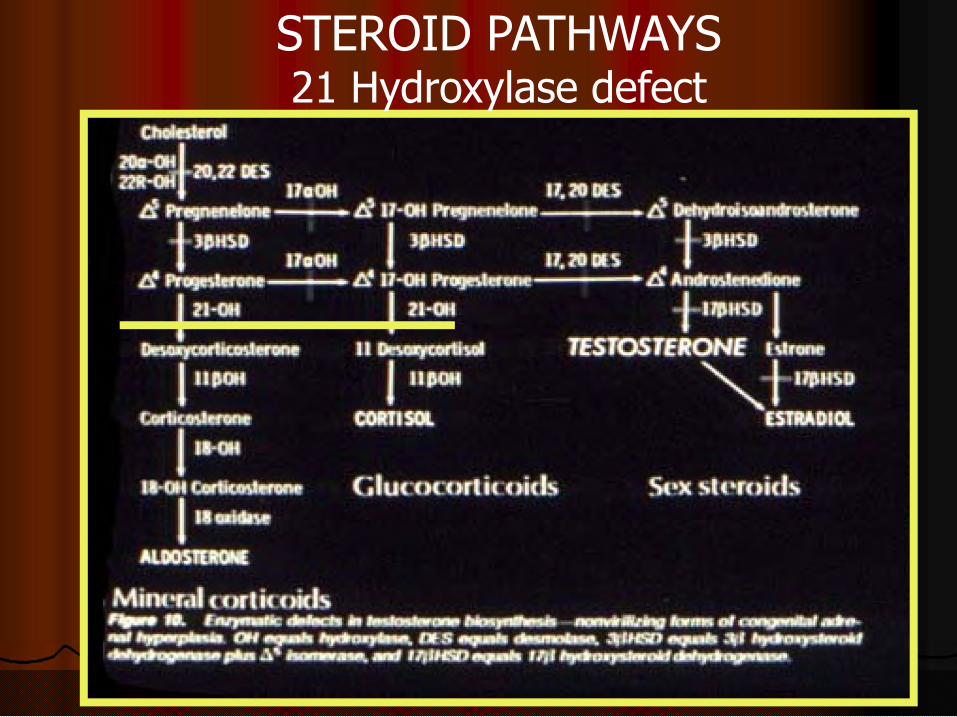
STEROID PATHWAYS21 Hydroxylase defect







17 OHP
17 OHP
FilterPaper
Congenital Adrenal HyperplasiaCongenital Adrenal HyperplasiaScreening ProgramScreening Program
Borderline Results: 17OHP ng/ml•<1250 g. - 135 to 160•>1250 to<1750 g. – 90 to 135•>1750 to 2250 g. – 65 to 90•>2250 g. – 50 to 90
Repeat
Presumptive CAH
17 OHP
17 OHP
Presumptive Positive Results: 17OHP ng/ml•<1250 g. - > 160•>1250 to<1750 g. – > 135•>1750 to 2250 g. – > 90•>2250 g. – > 90
ACTH Stimulation TestIf unclear do

GLUCOCORTICOID REPLACEMENTGLUCOCORTICOID REPLACEMENT
A. Hydrocortisone 25 mg IV bolusA. Hydrocortisone 25 mg IV bolus
B. Infusion of Hydrocortisone 50 mg / MB. Infusion of Hydrocortisone 50 mg / M22 / / 24 hours IV24 hours IV
C. Hydrocortisone 12 C. Hydrocortisone 12 -- 20 mg / M20 mg / M22 / 24 / 24 hours P.O.hours P.O.
HYPOGLYCEMIAHYPOGLYCEMIA HYPOGLYCEMIAHYPOGLYCEMIA
25 % Dextrose 1ml /kg IV followed by 25 % Dextrose 1ml /kg IV followed by 10% Dextrose IV10% Dextrose IV

MANAGEMENT OF ADRENAL INSUFFICIENCYMANAGEMENT OF ADRENAL INSUFFICIENCY
Sodium 2 Sodium 2 -- 6 meq /kg/ day6 meq /kg/ day
Hyperkalemia and acidosis rarely Hyperkalemia and acidosis rarely Hyperkalemia and acidosis rarely Hyperkalemia and acidosis rarely treatedtreated

If you are not sure or THE RESULTS ARE UNCLEAR:
• Treat• Treat• Treat• TREAT








