Download - Managing risk in the perinatal period

Managing risk in the perinatal periodLessons from the Confidential Enquiries into Maternal Deaths
Roch [email protected]
@roch61

Risk
1. Risk of occurrence / recurrence
2. Risk of treatment / no treatment
3. Risk of self-harm / suicide
4. Risk of harm to others / harm from others
5. Risk from misattribution / misdiagnosis
6. Risk relate to systemic factors – socio-economic, race, culture, lifestyle, presence of and access to services
7. Risk for 2 individuals

Risk management

Risk minimisation not elimination

Risk in pregnancyBiological
Underlying risk
Stopping/changing medication
Pharmacodynamic effects
Kendell et al, 1987
Wesseloo et al, 2017
Viguera et al, 2000

Risk in pregnancyPsychosocial
Life event!
Contentedness with pregnancy
Planned/wanted
Stage of life
Network of support
Adaptation to pregnancyHigh expectations
Previous experiences of being parented

Postnatal risk
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
pre
_1
04
w
pre
_1
00
w
pre
_9
6w
pre
_9
2w
pre
_8
8w
pre
_8
4w
pre
_8
0w
pre
_7
6w
pre
_7
2w
pre
_6
8w
pre
_6
4w
pre
_6
0w
pre
_5
6w
pre
_5
2w
pre
_4
8w
pre
_4
4w
Pre
gnan
cy
pre
_3
6w
pre
_3
2w
pre
_2
8w
pre
_2
4w
pre
_2
0w
pre
_1
6w
pre
_1
2w
pre
_8
w
pre
_4
w
Ch
ildb
irth
po
st_
4w
po
st_
8w
po
st_
12
w
po
st_
16
w
po
st_
20
w
po
st_
24
w
po
st_
28
w
po
st_
32
w
po
st_
36
w
po
st_
40
w
po
st_
44
w
po
st_
48
w
po
st_
52
w
po
st_
56
w
po
st_
60
w
po
st_
64
w
po
st_
68
w
po
st_
72
w
po
st_
76
w
po
st_
80
w
po
st_
84
w
po
st_
88
w
po
st_
92
w
po
st_
96
w
po
st_
10
0w
po
st_
10
4w
Aad
mis
sio
n p
er
we
ek
Psychosis
Non-psychotic depression Other
Munk-Olsen et al, 2009
Langan Martin et al, 2015

Postnatal risk
Di Floria et al, 2018
Wesseloo et al, 2016

Suicide in the perinatal period
Overall rates - ↓
0.05 SMR pregnancy
0.17 SMR postnatal
(Appleby, 1991)
Small negative association between suicide and being in 1st
postnatal year (Lysell, 2017)
Women with mental illness - ↑↑
70-fold increased rate for women admitted to psychiatric hospital in 1st postnatal year (Appleby, 1998)
Significantly elevated for women with 1st presentation 0-3 months postpartum v. mothers with no psychiatric history (Johannsen, 2016)
Women with postpartum mental disorder - high rates of DSH but lower than those with other mental disorder
Risk of progression to suicide after DSH much higher than in other groups (Johannsen, 2020)

Confidential Enquiries into Maternal Deaths
Mostly qualitative methodology
Standardised reports, case note audit, data linkage
Subjects both in and not in contact
Psychiatric data from over 25 years
One of the leading causes of maternal death
Majority have mood disorders
2/3rds received sub-optimal care

Confidential Enquiries into Maternal Deaths
Older woman, no past psychiatric historyDay 7 weepy and anxiousDay 11 crisis team involved; agitated; not sleeping;
overvalued ideas of guilt and incompetence
Day 12 midwife has problems contacting psychiatristDay 13 death by violent means
Cause of
death
Past history
Yes No
Identified
Yes
No
Plan
Yes No
Suicide 19 10 9 10 4 5
Cause of death n %
Hanging
Jumping from a height
Cut throat/stabbing
Self immolation
Drowning
Carbon monoxide
Ingesting of bleach
Overdose
Total
9
9
1
3
2
1
1
3
29
31
31
3
10
7
3
3
10
100

Confidential Enquiries into Maternal Deaths2015 - RED FLAGS
Key messages
from the report 2015
women
It’s OK to tell
The mind changes as well as the body
during and after pregnancy.
Women who report:
•New thoughts of violent
self harm
•Sudden onset or rapidly
worsening mental
symptoms
•Persistent feelings of estrangement
from their baby
need urgent referral to a specialist
perinatal mental health team
Specialist perinatal mental
health care matters*
morewomen
Mental health matters
Almost a quarter of women who died between six
weeks and one year after pregnancy died from
mental-health related causes
1 in 7 women died by Suicide
23%
Epilepsy
Cancer
Heart disease
Sepsis
Blood clots
Stroke
9 14per 100,000 died up to six
weeks after giving birth or
the end of pregnancy in
2011 - 13
per 100,000 died between
six weeks and a year after
their pregnancy in
2011 - 13
*Mapping data from the Maternal Mental Health Alliance (http://everyonesbusiness.org.uk)
If the women who died
by suicide became ill
today:
•40% would not
be able to get any
specialist perinatal
mental health care.
•Only 25% would get
the highest standard
of care.
INDICATORS OF SUICIDE RISK
Recent significant change in mental state or emergence of
new symptoms
New thoughts or acts of violent self-harm
New and persistent expressions of incompetency as a mother or estrangement
from the infant

32 year old woman with history of depressive disorder, including
depression with suicidal ideation and self-harm after birth of 1st child.
Presented with depressive symptoms to GP 3 weeks after the birth of 2nd child. Commenced on
antidepressants. At review, described return of thoughts of self-
harm.
Referred for psychiatric assessment. DNA.
3 weeks later presented to ED following overdose. MH assessment – range of depressive symptoms but
DSH ‘impulsive’. Discharged to GP care.
6 weeks later presented to out of hours primary care service having
made cuts to wrists. MH assessment – ‘multiple suicidal ideas but no
fixed plans’; self-harm ‘impulsive’. Referred to crisis team.
5 days later note from crisis team –not severe mental illness therefore
no need for engagement.
Suicide 4 week later.
At each stage: (i) What should have been included in the
assessment? (ii) What could have been done differently? Breakout

Symptom pattern / progression
‘Anxiety’ at first presentationLack of recognition of
escalating symptom pattern
Assessments of serial presentations ‘in the
moment’
Use of terms such as ‘impulsive’ and ‘no planning’ when assessing suicide risk
behaviour
Reliance on patient reports despite evidence to the
contrary
CEMD 2015

Thoughts / acts of violent self-harm
Prior history of PND and again after this child
Found on bridge with rope few weeks after birth
A/E – ‘no ongoing suicidal intent’
Local review – ‘death completely unexpected’
Woman with prior depression in postnatal period
CEMD 2015
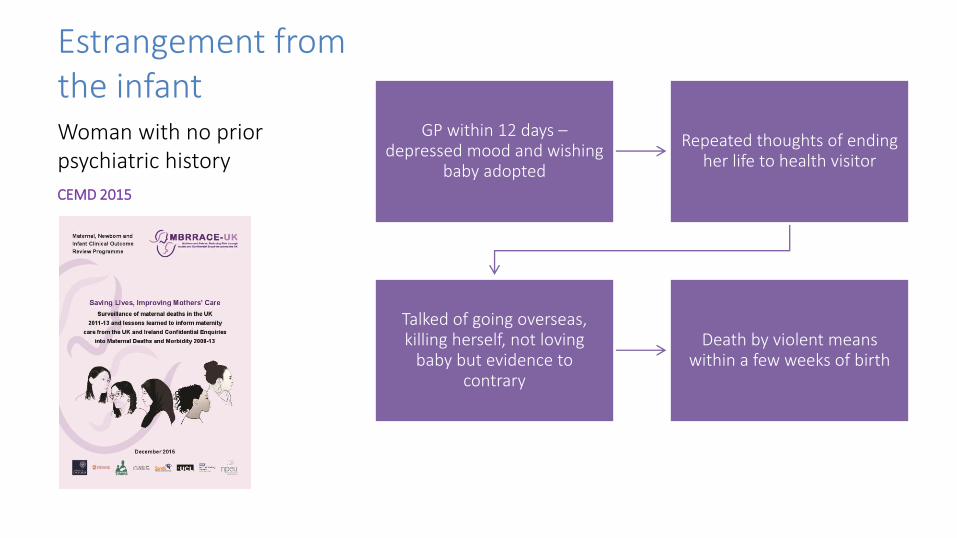
Estrangement from the infant
GP within 12 days –depressed mood and wishing
baby adopted
Repeated thoughts of ending her life to health visitor
Talked of going overseas, killing herself, not loving
baby but evidence to contrary
Death by violent means within a few weeks of birth
Woman with no prior psychiatric history
CEMD 2015

Other lessonsGrade of assessor
Herald symptoms | Pattern of escalation | Misattribution to
‘normal’ changes
Consideration of inpatient care
Rapidly changing mental state | Violent suicidal ideation | Pervasive guilt | Estrangement from infant |
Psychosis
Partner / family involvement
Knowledge of patient | Lack of understanding of seriousness of
illness
Care by multiple teams
CEMD 2015

Grade of assessor No past history of mental illness
Developed early onset low mood within days of delivering her first baby
Returned to hospital by midwife - appeared
perplexed, not sleeping, vivid dreams of baby being dead,
talked of jumping off a bridge
Casualty doctor found a similar presentation and
referred her for mental health assessment.
Seen by junior members of the crisis team - anxious but with no evidence of clinical
depression or psychosis
Discharged without psychiatric follow-up and died by violent means the next day
Early postpartum death
CEMD 2015

Care by multiple teams
E.g., on three consecutive days:
Day 1 (Team A)
Symptoms of psychosis
Day 2 (Team B)
‘No role’ for mental health team
Day 3 (Team C)
Admission with suicidal thoughts
Seen by at least 5 different mental health teams, each reaching different conclusions
Evidence of psychotic depression in months before death - 2 overdoses with suicidal intent
Woman who died by violent suicide in mid-pregnancy
CEMD 2015
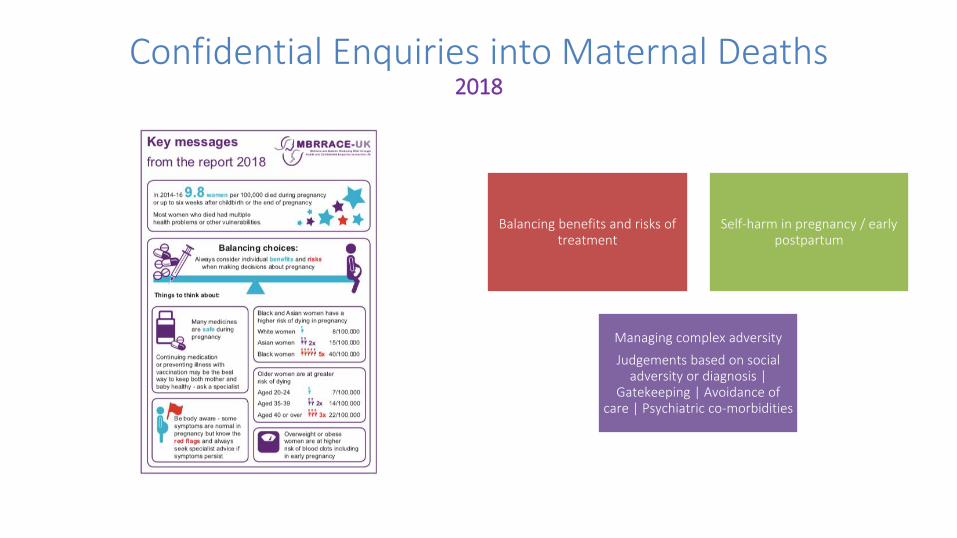
Confidential Enquiries into Maternal Deaths2018
Balancing benefits and risks of treatment
Self-harm in pregnancy / early postpartum
Managing complex adversity
Judgements based on social adversity or diagnosis |
Gatekeeping | Avoidance of care | Psychiatric co-morbidities
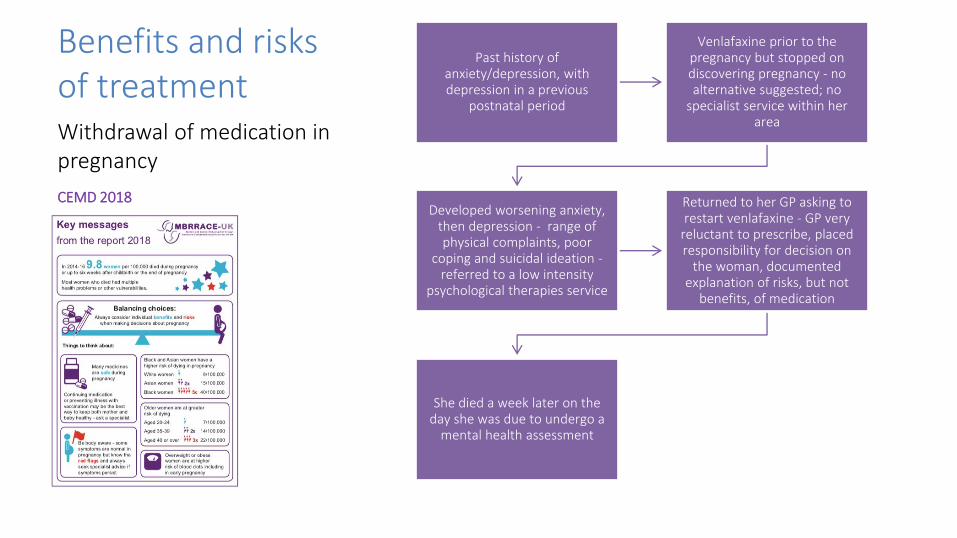
Benefits and risks of treatment
Past history of anxiety/depression, with depression in a previous
postnatal period
Venlafaxine prior to the pregnancy but stopped on discovering pregnancy - no alternative suggested; no
specialist service within her area
Developed worsening anxiety, then depression - range of physical complaints, poor
coping and suicidal ideation -referred to a low intensity
psychological therapies service
Returned to her GP asking to restart venlafaxine - GP very
reluctant to prescribe, placed responsibility for decision on
the woman, documented explanation of risks, but not
benefits, of medication
She died a week later on the day she was due to undergo a
mental health assessment
Withdrawal of medication in pregnancy
CEMD 2018

Prescribing issues – de-prescribing2018

Self-harm One year history of depressive symptoms
treated in primary care; one overdose pre-
pregnancy
Overdose (incl. alcohol) and laceration to wrists in 1st trimester; attempt to
strangle self in A/E
A/E mental health assessment – no acute
mental illness but possible previous alcohol dependency – no follow
up
Booking – referred to PMHS – referral rejected
– addictions services suggested instead
GP requested specialist PMHS assessment
proceed
Further overdose and attempted self-
strangulation - A/E records note ongoing suicidal ideation – MH
assessment – ‘impulsive’
Death by violent suicide 3 weeks later
Recurrent self-harm in pregnancy
CEMD 2018

Self-harm
Self-harm in pregnancy or the early postpartum period is an unusual event, and should always prompt referral for continuing evaluation,
ideally by specialist perinatal mental health services.
CEMD 2018

Gatekeeping
Prior history of depression and family history of suicide
Engaged poorly with recommendations (for medication
and counselling) to manage low mood in pregnancy
Despite repeated assessments by maternity staff and her GP, it was
felt she did not meet the threshold for referral into
secondary care mental health services
Specifically, she did not score highly enough on standardised
assessment tools used as part of the referral criteria and not all
maternity staff could access direct referral
Violent suicide several months after birth of 2nd child
CEMD 2018

Gatekeeping
CEMD 2018
• Mental health services should work to minimise barriers to care for women in pregnancy and the postnatal period, recognising the need for lowered thresholds and direct access for maternity and primary care professionals.
• Complex care co-ordination should be led by specialist perinatal mental health services where possible and ensure continuity when key workers are absent.

Confidential Enquiries into Maternal Deaths2020 – COVID-19 Rapid Report
Multiple referrals with mental health concerns
Lack of face to face assessments

Lack of face-to-face assessments
Referral to PMHS with low mood/difficulties coping mid-trimester
Referral declined –advised self-referral to psychological services
Referral to PMHS in late third trimester with
depressed mood
Appointment offered then cancelled due to
COVID-19
Violent suicide at 6 weeks postnatal
COVID-19 context
CEMD 2020
Breakout
(i) Who needs a face-to-face risk assessment?(ii) What precautions are required for video consultations?

Telepsychiatry Perinatal Mental Health Guidance
• High risk / severe mental state disturbance
• Privacy and confidence• Physical health concerns• Domestic violence• Mother-infant relationship
• Establish confidentiality• Encourage presence of baby• Ensure process for urgent face-to-face or
physical health assessments

Confidential Enquiries into Maternal Deaths2017 – AMBER FLAGS
INDICATORS OF RISK OF RECURRENCE
Any past history of psychotic disorder
Close monitoring if family history / refer if + current
mood disorder
Personal and familial patterns of (re)occurrence

Forward planning for future risk
A woman experienced postpartum psychosis, requiring MBU
admission, after the birth of her first child.
Her delivery had been traumatic with significant blood loss.
At the point of MBU discharge her illness was explained to her as
being due to her traumatic delivery and that she could be
seen in future pregnancy ‘should further problems arise’.
Misattributing risk
CEMD 2017

Forward planning for future risk2017
RECOMMENDATIONS
Following recovery, it is the responsibility of the treating team to ensure that all women experiencing postpartum psychosis receive a clear explanation of:
1. Future risk
2. Availability of risk minimisation strategies
3. Need for re-referral during subsequent pregnancies
Risk information
Risk reduction strategies
Referral in subsequent pregnancies

Other themes
Misdiagnosis/misattribution of physical symptoms
Communication, documentation and information sharing
•Letters (by who?)
•Late pregnancy plan
Risks associated with
•Child protection proceedings/removal
•Child loss
•Delayed/refused termination
Altered thresholds for referral and intervention
Leave and early discharge vulnerability, especially if out of area
Service provision
Substance misuse
•Specialist multidisciplinary engagement
•Drug testing
Education and training for non-specialist staff

MisdiagnosisMarried woman; 1st baby;
no previous psychiatric history
Previously diagnosed auto-immune disease
At 25/40 - increasing malaise
2 days of lethargy, withdrawal, nil by mouth, agitation - attributed to
depression, then collapse
Within 3 weeks - death from pneumonia/encephalopathy
Misattributing to mental health causes
CEMD 2011

MisdiagnosisAortic aneurysm/pulmonary
embolism - Distress/pain attributed to anxiety and
depression
Acute confusional state -Distress/agitation attributed to
postnatal depression
Lymphoma - Weight loss/cough/sweating attributed to
opiate use
TB - Weight loss/loss of appetite attributed to anorexia nervosa
Encephalopathy/SLE - Attributed to depression
Eclampsia - Agitation attributed to depression
Misattributing to mental health causes
CEMD 2011

Misdiagnosis
Misattributing to mental health causes
CEMD 2011
BACK TO BASICS

Risk assessment
• 29 year old woman, referred by health visitor 6 weeks after birth of first child; no past history.
• “Increasingly anxious about caring for her baby, not sleeping or eating, fearful baby will come to harm. Repeatedly making contacting with practice.”
• Seen by CPN – very anxious about baby’s health and development. Worried that baby may not be putting on weight properly and that she isn’t producing enough milk.
• One thought that if she crashed car, both of them would not have to suffer.
• Took extra painkillers but told no-one. Knows she ‘could not go through with it’ because of her baby.
Breakout

Risk assessment
• 29 year old woman, referred by health visitor 6 weeks after birth of first child; no past history.
• “Increasingly anxious about caring for her baby, not sleeping or eating, fearful baby will come to harm. Repeatedly making contacting with practice.”
ANXIETY V. AGITATION?• Seen by CPN – very anxious about baby’s health and development. Worried that baby
may be ill and not be putting on weight properly and that she isn’t producing enough milk.
TYPICAL ‘NEW MOTHER’ CONCERNS V. DISTORTED THINKING?• One thought that if she crashed car, both of them would not have to suffer.
OBSESSIONAL THINKING V. OVERVALUED IDEAS V. DELUSIONAL THOUGHTS• Took extra painkillers but told no-one. Knows she ‘could not go through with it’ because
of her baby.RISK V. PROTECTIVE FACTORS

Risk assessment
• 29 year old woman, referred by health visitor 6 weeks after birth of first child; no past history.
• “Increasingly anxious about caring for her baby, not sleeping or eating, fearful baby will come to harm. Repeatedly making contacting with practice.”
ANXIETY V. AGITATION?• Seen by CPN – very anxious about baby’s health and development. Worried that baby
may be ill and not be putting on weight properly and that she isn’t producing enough milk.
TYPICAL ‘NEW MOTHER’ CONCERNS V. DISTORTED THINKING?• One thought that if she crashed car, both of them would not have to suffer.
OBSESSIONAL THINKING V. OVERVALUED IDEAS V. DELUSIONAL THOUGHTS• Took extra painkillers but told no-one. Knows she ‘could not go through with it’ because
of her baby.RISK V. PROTECTIVE FACTORS

Risk assessment
• 29 year old woman, referred by health visitor 6 weeks after birth of first child; no past history.
• “Increasingly anxious about caring for her baby, not sleeping or eating, fearful baby will come to harm. Repeatedly making contacting with practice.”
ANXIETY V. AGITATION?• Seen by CPN – very anxious about baby’s health and development. Worried that baby
may be ill and not be putting on weight properly and that she isn’t producing enough milk.
TYPICAL ‘NEW MOTHER’ CONCERNS V. DISTORTED THINKING?• One thought that if she crashed car, both of them would not have to suffer.
OBSESSIONAL THINKING V. OVERVALUED IDEAS V. DELUSIONAL THOUGHTS• Took extra painkillers but told no-one. Knows she ‘could not go through with it’ because
of her baby.RISK V. PROTECTIVE FACTORS

Risk assessment
• 29 year old woman, referred by health visitor 6 weeks after birth of first child; no past history.
• “Increasingly anxious about caring for her baby, not sleeping or eating, fearful baby will come to harm. Repeatedly making contacting with practice.”
ANXIETY V. AGITATION?• Seen by CPN – very anxious about baby’s health and development. Worried that baby
may be ill and not be putting on weight properly and that she isn’t producing enough milk.
TYPICAL ‘NEW MOTHER’ CONCERNS V. DISTORTED THINKING?• One thought that if she crashed car, both of them would not have to suffer.
OBSESSIONAL THINKING V. OVERVALUED IDEAS V. DELUSIONAL THOUGHTS• Took extra painkillers but told no-one. Knows she ‘could not go through with it’ because
of her baby.RISK V. PROTECTIVE FACTORS

Interview as therapy
• Understanding the maternity context
• Creating safe space
• Seeing the ‘whole picture’
– Mental state examination is more that what the patient tells you
– Past and family history – relevant but not bound by it
– Personality and coping
• Protective factors
• Instillation of hope and expectation of recovery

Risk management
• Consult with and listen to others
• Risk is dynamic
• Institutional factors
• Recorded management plan that takes into account the maternity context

Where do we go from here?
Messages have become more complex
CEMD acts as indicator of state of health of mental health services in general
Danger of relying on previous notions of ‘distinctiveness’
Focussing only on traditional ‘high risk’ groups
Danger of forgetting old lessons
What constitutes good care
Thorough assessment and evidence of change for this woman
Need to recognise new ‘distinctiveness’ and new challenges
Continuity of care (pregnancy loss; child removal, etc.)
Mother-infant relationship and infant mental health







