
Why Those Baby Blues?
Change in Strain from Child Care Arrangements and in Depression
Among Employed Mothers of Young Children
By: Rachel A. Gordon and Anna Gluzman
University of Illinois at Chicago
Prepared for the conference of the ISA Research Committee on Social Stratification and
Mobility, August 14-17, Montreal, 2007.
Contact information: Rachel A. Gordon: [email protected]; Anna Gluzman: [email protected];

2
Introduction
Depression associates with negative outcomes for both adults and their children. It refers
to an unpleasant feeling of sadness and dejection marked by difficulties in sleeping,
concentrating and acting. For adults, depression severely impairs social and physical functioning,
and is a major factor in suicide. Up to seventy percent of depressed people experience suicidal
ideation, and the lifetime risk of suicide among depressed people varies from ten to twenty
percent across studies (Milane et al., 2006). Depression also increases morbidity and mortality
from other medical illness (National Institute of Mental Health, 2004).
Not only is the individual suffering from depression affected, but also their family
members including children. Children whose mothers reported depression symptoms showed
lower cognitive-linguistic functioning, and were less cooperative (Goodman, 2007; NICHD,
1999). These negative outcomes could be caused by emotional unavailability, lack of
responsiveness and overall less sensitive and less engaged maternal care. Young children are
especially prone to these developmental problems, since they are more dependent upon their
primary caregivers’ nurturance and support of exploration than are older children.
The symptoms and consequences of depression are not evenly distributed across society.
Rates are twice as high for women as for men. For mothers of young children, the estimates of
depression rates are especially high, ranging from 12% to 47% across studies, comparing to only
9.5% in the US adult population (Heneghan et al. 1998).
Research explains depression by negative life events such as death or lay offs that require
major behavioral change (Horowits, 1999; Thoits, 1995, 1999) and chronic strains such as illness
in the family (Seifert, 2004). Higher rates of depression among women are usually explained by

3
chronic strain and distress related to social roles that they occupy (Evenson and Simon 2005;
Gove, 1972; McLanahan and Adams 1987).
This study advances prior research on this topic. We focus on one combination of roles -
mothers combining employment with parenting of infants and toddlers – and explicitly examine
the strains associated with one important aspect of their managing this role combination – child
care. Many contemporary parents work for pay and regularly turn over primary care of their
children to someone else for extended portions of each work day, potentially leading to concerns
about their children being unhappy, ignored, or even harmed. These strains may be particularly
elevated if parents cannot find the type of care that they prefer or if they believe their provider is
less than fully capable. Child care problems may also exacerbate work and family role conflict if
the arrangements fall through and parents cannot regularly be at work or if parents are often
distracted at work by worries about their child.
Measuring these strains allows us to test mechanisms assumed to underlie associations in
prior research. We distinguish the structure of child care arrangements from perceived strains,
thus identifying not only which types of care elevate depressive symptomatology but how they
do so. We also examine how these associations vary based on self-perceptions of the role
(including role salience), social support, and economic resources. And, we include important
measured controls (like life events) and use statistical models that better adjust for selection
effects than the cross-sectional approaches of prior studies.
Social Roles and Depression
Prior literature on social roles and depression finds that employment and marriage confer
mental health benefits, on average, while parenthood often does not (Evenson and Simon 2005;
McLanahan and Adams 1987). One important early line of research examined the stress of being

4
a homemaker (Gove 1972), hypothesizing that these women suffer from social isolation and lack
the buffer of multiple roles. Consistent with societal trends in women’s labor force participation,
later studies considered whether women with children benefit from employment roles as much as
do childless women (McLanahan and Adams 1987). This latter research has pointed to the
importance of fathers’ help with household tasks, including dividing routine caregiving tasks
when parents are home. Yet, only a small number of studies, reviewed below, has looked
explicitly at the strains associated with arrangements made for child care while the parents are at
work.
For employed parents of infants and toddlers, the strains associated with child care may
counterbalance any benefits associated with their roles as employees and parents (Evenson and
Simon 2005; Pearlin and Johnson 1977; Umberson and Gove 1989). Unfortunately,
interpretations of many existing studies are limited because the strains of parenthood are often
assumed rather than directly measured, for example by simply including dummy categories for
social roles like marital status, employment status, and parenthood and examining associated
average levels of distress. Some research also uses proxies for rather than direct measures of
parenting strain, such as numbers and ages of children. Yet, the strains associated with
parenthood are not uniform but vary, even for mothers with the same number and ages of
children. Some mothers can access supports within their personal social networks that avoid or
lessen the strains of parenthood. Other mothers can do so by accessing institutional supports
within their workplace or community.
In one early study, Pearlin and Johnson (1977) examined economic hardship, social
isolation and parental responsibilities as three persistent life strains differentiating unmarried
from married persons. Whereas their measures of the strains of economic hardship and social

5
isolation were explicit (e.g., How often does it happen that you do not have enough money to
afford the kind of food you should have? How many really good friends live within an hour’s
drive?), parental responsibilities was assessed simply by the number and ages of children
although more direct strains were conceptualized (e.g., self-sufficiency of older children placing
fewer time constraints on parents). More recently, although Evenson and Simon (2005) theorize
that some types of parenthood are associated with more stress and distress than others they focus
on comparing types rather than explicitly measuring the stressors. The authors conclude that
“the results provide support, albeit indirect support, for our argument that
variation in mental health among parents reflects a myriad of factors affecting
different parenting experiences. While data limitations prevented us from doing
so, future research should directly examine whether these social-psychological,
sociocultural and social-structural factors contribute to the emotional costs and
rewards associated with parenthood at different stages of the adult life course and
different types of parenthood” (Evenson and Simon 2005, p. 355).
Associations of Child Care Types and Strains with Maternal Depression
Conceptual Ideas
We expect that variation in characteristics of child care will explain some of the variation
in maternal depression among employed mothers of young children. We consider parental
perceptions of and strains associated with different types and numbers of child care
arrangements.
Child care is typically defined as any regular non-maternal care arrangements, including
care by the father, often, but not always, used to allow the mother to work at a paid job.
Arrangements can be classified into centers (care outside of a private home) and several types of

6
home-based care, including care by fathers, other relatives, or non-relatives. Prior research has
identified average differences in potential strains among different types of child care. No single
type of care setting is better across all of these characteristics, and the offsetting positive and
negative characteristics of different types of care may balance out in simple associations with
depression.
Developmental scholars have created measures of the characteristics of child care that
support school readiness, and child care centers score higher, on average, than home-based care
when observers rate them on these characteristics (Fuller et al. 2004; Li-Grining and Coley
2006). Parents seem to recognize these benefits (parents are more likely to use centers as their
children reach preschool age; Johansen, Leibowitz and Waite 1996), but it may be difficult for
parents to observe these quality characteristics. Indeed, parents often rate settings higher on such
measures of quality than do trained observers (Cryer and Burchinal 1997). Children are also less
likely to be injured or die in child care centers than private home care, likely due to the
organizational features of centers that promote strict safety procedures and the public setting and
multiple staff that deter abusive behavior (Wrigley and Dreby 2005). Yet, centers have more
rigid hours and are less likely to meet the needs of parents who work irregular, night, or weekend
shifts (Henly and Lyons 2000; Li-Grining and Coley 2006). And, centers’ size promotes
transmission of common illness and their strict illness exclusion policies mean that parents will
miss work more often due to a sick child when they use centers (Gordon, Kaestner and
Korenman 2007).
In contrast to the inputs associated with school readiness noted above, research on
caregiver sensitivity has found that fathers and relatives are more emotionally responsive than
center staff, especially with infants (NICHD Early Child Care Research Network 1996). And,

7
parents generally prefer home-based settings for infants (Johansen, Leibowitz and Waite 1996).
Still, caregiving by relatives, friends and neighbors involve social instead of or in addition to
formal business relationships. Social obligations associated with a caregiver watching the child
as a favor and conflicts between mother and caregiver over parenting strategies may produce
strains. For example, Burris (1991) and Glass (1998) found that fathers only reluctantly
provided care and working mothers often were not satisfied with fathers’ child care. Fathers’
child care has also been associated with fathers’ diminished love to mother (Crouter et al. 1987)
and higher employment turnover rates among mothers’ using this type of care (Maume and
Mullin 1993). And, qualitative research has identified similar social strains associated with care
by “kith and kin” (Henly and Lyons 2000; Lowe and Weisner 2004; Scott, London, and Hurst
2005). In addition, although home-based providers are often more flexible to parents’ work
schedules they are also more likely than centers to “fall through” (be unavailable on any given
day due to personal illness, emergency, or needs) leading mothers to miss work or scramble for
backup arrangements (Gordon, Kaestner and Korenman 2007).
Parents’ mental health may also be negatively impacted when the type of care used does
not match the type of care the parent would prefer or when they use multiple arrangements.
Research suggests that only about one-quarter of parents are able to match their desired child
care type with the type that they actually use (Gordon and Högnäs 2006; Riley and Glass 2002).
And, the type of care preferred affects the likelihood of a match. For example, Gordon and
Högnäs (2006) found that parents were most likely to achieve a match when they preferred father
care or a family day care provider. Those who preferred care in centers or by relatives were less
likely to use their preferred care type. Such mis-match may create strains for parents since they
are likely to view the arrangement they can secure less favorably than they would otherwise. A

8
substantial fraction of parents of infants and toddlers, at least one-quarter to one-third of mothers,
also use two or more child care arrangements per week (Phillips and Adams 2001). Such use of
multiple caregiving arrangements may also lead to benefits and strains that have offsetting
effects on mental health. When parents regularly use a secondary care arrangement, the provider
may be available as a backup when the primary arrangement cannot be used. On the other hand,
coordinating and transitioning among care settings may be stressful for both the parent and child.
Prior Empirical Research
A small set of studies has directly examined the association between characteristics of
child care and maternal depression (Bird 1997; Fagan 1994; Hughes and Galinsky 1994; Kontos
et al. 1995; Press, Fagan and Bernd 2006; Ross and Mirowsky 1988; Vandell, Hyde, Plant and
Essex 1997). Although important initial studies of the topic, all report cross-sectional estimates
and could examine only a limited number of mechanisms. The studies differ greatly in their
sample recruitment strategies and ages of children, although each demonstrates that some
characteristics of care are associated with maternal depression.
Two nationally-representative telephone surveys found that the husband’s greater sharing
of routine care at home and the mother’s ease of arranging regular care for the child while she
worked were associated with less maternal depression (Bird 1997; Ross and Mirowsky 1988). In
three additional studies, drawn from communities or employers, mothers reported more
symptoms of depression when their usual arrangement fell through or when problems with child
care interfered with work (Hughes and Galinsky 1994; Kontos et al. 1995; Press, Fagan, and
Bernd 2006). And, mothers in one of these community-based studies and a separate clinic-based
study were found to be less depressed when they used their preferred type of care and when they
reported being more satisfied with their arrangement (Press, Fagan and Bernd 2006; Vandell et

9
al. 1997). Ross and Mirowsky (1988) also found that type of care was generally not associated
with maternal depression, although mothers who used family caregivers tended to report less
depression. The authors interpret this latter finding as potentially reflecting most mothers’
preference for relative care stating “We hope that future research measures explicitly this
preference for various types of child care, the reasons for these preferences, and the effect of
discrepancy between reality and preferences on psychological well-being” (Ross and Mirowsky
1988, p. 135).
The Current Study
The current study builds on these prior studies in several ways. First, as described in the
Methods, we are able to evaluate in a single dataset a fuller complement of child care strains that
may relate to maternal depression. In addition, we use a longitudinal fixed effects model rather
than a cross-sectional design. This means our estimates will be less biased by common causes
than the estimates in prior research. We also extend prior consideration of mothers’ job
characteristics by carefully examining how the effects of child care differ when we control for
job quality and when we focus on mothers with better and poorer jobs. We also consider the
moderating effect of self-perceptions of roles, social support, and economic resources. In
addition, we more directly acknowledge the importance of the child’s age than has prior
research. Whereas several of the prior studies included a broader age range, combining infants
and toddlers with preschool and schoolage children, we look at the youngest age groups (birth to
age three) and we test for variation in effects across the first three years of life.
Fixed-Effects Models
Prior researchers have recognized that associations between social roles and mental
health may reflect social selection as well as causation (Evenson and Simon 2005; Pearlin and

10
Johnson 1977). In our study, women who are likely to experience child care problems may also
be susceptible to depression. Common causes might include individual characteristics that are
biological (a genetic tendency toward depression) or social/environmental (experience of abuse
in childhood). They might also include family or community characteristics. For example,
marital problems at the time of the child’s birth might associate with less help from the husband
in child care and more psychological distress in the mother. Or, communities that are high in
crime might have fewer child care resources and be distressing to mothers. If we do not control
for all of the preexisting characteristics that are associated both with child care problems and
depression, then our estimates of the effect of child care problems on depression will be biased.
Fixed-effects regression models allow us to control comprehensively for time-constant
unmeasured characteristics that might bias the association. By explicitly adjusting for these
forms of selection processes, we strengthen the evidence for social causation.
Fixed-effects models do not adjust for confounds that vary across time. For example, job
characteristics and social networks may change over time and affect both child care and
depression. Women with “bad” jobs and little support at home or from family may also be more
likely to experience child care problems (women who switch to lower-paying jobs with few
benefits and little flexibility may at the same time begin using less expensive home-based care
that is lower, on average, in developmental quality; problems with child care may be more likely
to interfere with work when the husband, partner or family members becomes ill and cannot step
in to be backup caregivers, etc). Similarly, changing to use of multiple child care arrangements
may reflect parents’ work schedules becoming irregular. Our data allow us to control for many
such time varying covariates.
Moderators

11
Employment. Prior studies have mostly concentrated on the direct negative effect of
“bad” jobs on mental health. Inadequate employment - characterized by low pay, low autonomy
and high demands - increased symptoms of depression (Grzywacz and Dooley, 2003; Lennon
and Rosenfield, 1992; Rosenfield, 1989). Employment has also been found to affect parenting
styles. Parents whose jobs were less complex, challenging and stimulating exhibited parenting
styles that were harsher, less responsive and more disciplinary (Greenberger et al, 1994). As far
as we are aware, only one study has examined the moderating effect of employment on the
relationship between child care and depression. In a sample of low-income mothers from
Philadelphia, the association between preferences for a different type of care and depression was
stronger among the mothers who worked in relatively higher-paying jobs or who held only one
job (Press, Fagan and Bernd, 2006). Whether this finding would generalize to other income
groups is unknown, but we expect that in middle and higher income samples the association
between child care and depression will be stronger among mothers with poorer job
characteristics. Mothers who work longer hours, have inflexible work, have little autonomy and
high demands, and who are not in professional or managerial occupations may find it harder to
locate and secure the kind of care that they prefer. We also expect that child care strains and
depression will have a stronger association among mothers who hold bad jobs, since they could
have less work related flexibility (free time, opportunity to take child to work) to deal with the
strain.
Social Support. Prior research consistently finds that the relationship between
parenthood and depression is stronger for single than married parents (Evenson and Simon 2005;
McLanahan and Adams 1987; Pearlin and Johnson 1977). Some studies also suggest that single
parents’ greater distress may be due in large part to the fewer social and economic resources

12
available to them (Evenson and Simon 2005). We consider the presence of an adult or spouse in
the household in conjunction with perceived social support as a moderator since prior research
has found social isolation to be more important for depression in the absence of a spouse (Pearlin
and Johnson 1977). We anticipate that child care strains will be more strongly associated with
maternal depression for mothers who lack co-resident adults and perceive little social support.
Economic Resources. As Thoits (1995, p. 63) pointed out in her review, sociologists
have had a “puzzling lack of attention to an obvious coping resource: money.” This resource is
particularly important to child care strains since parents with more money can access a broader
range of child care options. They thus may be more likely to obtain a match with their preferred
care and to avoid care settings that they view as too unreliable or of insufficient quality. We
anticipate that income may moderate the association of child care strains to maternal depression
since higher-income parents can buy goods and services to lessen the stressors and their distress
(e.g., pay for sick child care, afford to stay home when their provider is unavailable, purchase
children’s activities to supplement what their provider doesn’t offer).
Self-Perceptions of Roles. Prior scholars have theorized that the association between the
stressors associated with a role and distress may be moderated by self-perceptions of the role.
Individuals are expected to be more affected by stress that occurs in the roles that are most
important to them (Thoits 1995). Empirical results have been inconsistent. Part of this
inconsistency may be due to the different ways self-perceptions of the role are defined and
measured (Marcussen, Ritter, and Safron 2004). Some researchers focus on role salience,
sometimes defined as the importance of a role or as its invocation in multiple situations. Others
focus on centrality, the relative ranking of roles. Others on additional constructs, like
13
commitment, sometimes defined as perceptions of the cost/benefit ratio associated with
employment and parenting.
We contribute to the literature by using multiple measures of self-perceptions of the two
major roles examined: employee and parent. We anticipate that some of these measures are
more likely to capture the exacerbating effect of perceptions and others the attenuating effect. In
terms of the parent role, maternal separation anxiety captures mothers’ apprehension about
leaving her child in the care of others (Hock and Lutz 1998). Problems with child care should be
particularly related to distress for mothers who score higher on separation anxiety. Role
centrality is defined by the relative ranking of roles. We consider whether employment or
parenthood is considered primary for parents. We anticipate that employed mothers will be more
affected by child care strains when they score higher on traditional gender ideology, placing their
primary role as in the home rather than the workplace. Parents may also vary in their perceptions
of the costs and benefits of parenting and employment (Barnett, Brennan and Marshall 1994).
Parenting rewards include the meaning, purpose, and enjoyment children bring to parents’ lives.
Parenting costs include the burdens of children on parents’ time, energy and finances. While the
latter may be directly influenced by child care strains, the former is conceptually similar to the
importance or salience parents’ place on parenting. We also consider job experiences as a
moderator, building on the limited prior research reviewed above which found that several job
characteristics interacted with child care strains in predicting depression (Press, Fagan and Bernd
2006).
Focus on Mothers of Infants and Toddlers
We study mothers of infants and toddlers. These mothers may be particularly anxious
about child care given their young children’s extreme dependence. In many cases, it is difficult
14
for parents to observe completely the quality of the care children receive, especially the quality
of caregiver-child interactions when parents are not present. The youngest children cannot tell
parents about problems in their care setting, parents may recognize the early years of rapid
development as a critical period, and may perceive children as particularly vulnerable to negative
caregiving experiences.
Method
Data
The National Institute of Child Health and Human Development Study of Early Child
Care is a multi-site, prospective longitudinal study of 1,364 children and their families (NICHD
Early Child Care Research Network, 1999a). The study began in 1991 when newborns were
sampled from hospital birth records at 10 sites in 9 states (Arkansas, California, Kansas,
Massachusetts, North Carolina, Pennsylvania, Virginia, Washington, and Wisconsin). The
enrollment process had three stages: (a) a hospital screening within 48 hours of birth, (b) a 2-
week phone call with a subset of screened eligibles, and (c) a 1-month interview with contacted
families who agreed to enroll in the study (NICHD Early Child Care Research Network, 1999a).
Although not based on a nationally-representative design, the SECC sample is similar to the U.S.
population on a number of characteristics (Gordon, Kaestner, and Korenman, 2007). We focus
on the first phase of the study, which followed the children to age three. Major assessments were
conducted in person when the child was 1-month, 6-months, 15-months, 24-months, and 36-
months old. Attrition was modest across waves. At 3 months 1,331 of the 1,364 children (98%)
were re-interviewed. By 36 months, 1,234 children (90%) remained. Item non-response was also
moderate. We compare results from two strategies for recovering item-level missing data: (a)
simple mean imputation and (b) multiple imputation using the ice and mim commands in Stata

15
(Acock, 2005; Royston, 2005). The current version of the paper reports only the results based on
simple mean imputation.
Measures
Descriptive statistics for the measures are found in Appendix 1.
Maternal Depression
Maternal depression was assessed using the Center for Epidemiological Studies
Depression scale (CES-D; Radloff, 1977). Respondents reported the frequency of experiencing
20 symptoms on a four-level rating scale (0=less than 1 day a week, 1=1-2 days a week, 2=3-4
days a week, 3=5-7 days a week). Example items include I felt sad, I had crying spells, and My
sleep was restless. The simple sum can range from 0 to 60. A score 16 or above suggests
clinically significant depressive symptoms (Beeghly et al. 2002, NICHD, 1999). Prior research
indicates that the scale has “high internal consistency, acceptable test re-test stability, good
concurrent and construct validity” (Roberts, 1980, p. 2) and correlates highly with other
measures of depression (Radloff, 1977; Weissman et. al. 1977).
Child Care Variables
Mother is using child care. Positive response to the question ‘Is anyone other than
yourself now caring for child on a regular basis? Please include any regular arrangement you
may have with your husband/partner’ indicated maternal usage of child care arrangement.
Type of child care currently used. Mothers provided information about up to three child
care arrangements used for the target child. The arrangement used for the most hours was coded
into four types: care in a private home by (1) fathers, (2) relatives (siblings, grandparents or
other relatives), (3) non-relatives (friends, neighbors or other unrelated adults), and (4) child care

16
centers (care in centers, nurseries, and other locations). On average over 95% percent of the
time children spent in non-maternal care, took place in this primary arrangement.
Match of child care type used with ideal type of care. At the one-month interview,
mothers responded to the question: “If you could choose any kind of child care, other than caring
for your baby yourself, what would you choose?” Mothers could report up to three ideal types of
care, although most mothers (78%) reported only one ideal type of child care. The first type of
ideal care that the mother reported was coded into the same categories as type of care used. For
each wave, a dummy variable indicated whether the type of care currently used for the most
hours matched the type reported as ideal at one month.
Maternal perceptions of child care arrangements. At each wave, mothers reported the
most important reason for choosing each child care arrangement and whether they would
recommend the setting to a friend. We used responses about their primary arrangement.
Dummy variables indicated whether the mother reported choosing the setting for accessibility
reasons (cost, location, or availability), because of her perceptions of the quality of the provider,
environment, or program, due to preference for the selected kind of care, or for other reasons.
Few mothers reported that they would have doubts or advise against a friend using the care
setting (fewer than 150 mothers at each wave). Consequently, a single dummy variable indicated
whether the mother would strongly recommend the arrangement versus recommend, have doubts
about recommending or advise against. Two additional items measured mothers’ perception of
child care as good and as affordable care. The former is measured by the item ‘I am working
right now because I have good child care’; its values could range from 1-not true to 5- very true.
The latter is a scale combined from the two items of ‘I am working right now because I have
17
child care I can afford’ and ‘I am working right now because I earn enough to make it
worthwhile even after paying for child care’, with possible range of 2 to 10.
Strain associated with child care. At each interview, the mother reported about work
absences that were associated with child care. Missing work due to child care problems captured
whether the mother reported that she or her spouse/partner had stayed home from work because
the child care provider was not available, including the provider being ill, the provider’s family
member being ill or the setting being closed for a scheduled or unscheduled reason. Separate
dummy variables indicated whether the child had been sick on a work day since the last
interview and (a) the mother had to stay home with the baby or take baby to work (b) the mother
was able to use her regular child care or (c) the mother used other arrangements (including
partner, relative, friend, hired sitter, other child or arrangement for sick kids) versus (d) the child
had not been sick. We also include a dummy indicator of whether the mother used multiple
arrangements and the percentage of time spent in the primary arrangement, anticipating that
juggling multiple arrangements and transitioning among them would be stressful.
A final item measuring the strain connected to child care was taken from the Work-
Family Strains and Gains Scale (Marshall and Barnett, 1993): ‘Thinking about your children
interferes with your performance at work.’ The item ranged from 1=Not at all true to 4=Very
true. The remaining Work-Family Strains and Gains Scale items included 13 strains (e.g.
working leaves you with too little time to be the kind parent you want to be; during work time
you feel resentful not spending time with your family) and 8 benefits (e.g. having work and
family responsibilities challenges you to be the best you can; working makes you a better
parent). The scale for each item ranged from 1= Not at all true to 4= Very true. Following the

18
standard scoring procedures, the averaged gains item were subtracted from averaged strain items
and the scale had possible range from -3 to 3.
Moderators
Employment. Measures of mother’s employment include her current work hours from up
to four jobs, her work shifts, and her report of the flexibility of her work arrangements. An
adaptation of the Job Role Quality Scale captured the mother’s concerns about advancement,
respect, lack of appreciation, too much to do, lack of support, lower than deserved earnings as
well as rewards, including recognition, important work, team work, and sense of accomplishment
(Marshall and Barnett, 1993). Following the standard scoring procedures, the averaged positive
job characteristics items were subtracted from averaged negative job characteristics items and the
scale had possible range from -3 to 3. A higher score indicates a more negative job experience.
We also included a dummy variable that measures maternal occupation – being professional or
managerial occupation versus other.
Potential social support. Dummy variables indicated the presence of a spouse or partner
and of other adults in the household. Emotional and instrumental support were measured using a
modified version of the Social Support Scale (Marshall and Barnett, 1993). Each item ranged
from 1=none of the time to 6=all of the time. The emotional support sub-scale included 7 items,
such as People who are important encourage me when I feel discouraged or down, and had
possible range from 7 to 42. Instrumental support sub-scale included 3 items, such as When I
need someone to help me out, I can usually find someone and could range from 3 to 18.
Income. Mothers’ earnings, fathers’ income and other sources of income were adjusted
to 2005 dollars. Total household income summed these separated items. A dummy variable of

19
public assistance indicated mothers’ report of receiving food stamps, Aid to Families with
Dependent Children or WIC.
Role salience. We use several time-constant measures of role salience. Mothers
responded to a question about the salience of their current role depending on their current work
and school status. The item was worded “Because [being a mother/my work/going to school] is
important to the way I see myself” and responses ranged from 1=definitely false to 5=Very true.
Dummy variables also indicated whether the mother felt her ideal situation was (a) working or
studying full time or (b) working or studying part time versus (c) staying home full time. And,
the Maternal Separation Anxiety Scale (DeMeis et.al., 1986) measured mothers’ level of worry,
sadness and guilt when separated from the baby, including items such as I like to have my child
close to me most of the time and could range from 21 to 105. From the scale above we pulled out
one item that represents parental role salience concretely “When away from my child, I often
wonder if his/her physical needs (dry diapers, enough to eat, etc) are being met”.
Employment role salience included the measure of Attitude toward Maternal
Employment (Greenberger et al, 1988) that relates to central issues of maternal employment and
children development. The standard scale captures perceived employment costs. Each item
ranges from 1=disagree very strongly to 6= agree very strongly. The scale score ranged from 11
to 66. Positive and Negative Attitudes toward Maternal Employment are two constructs that
summarized from items of the standard scale described above. Positive employment attitudes
measure constructed from 5 items like ‘For children, working mothers are good role models for
leading busy and productive life.’ and ranges from 5 to 30. Negative employment attitudes
constructed from 6 items such as ‘Working mothers more likely to have children with
psychological problems than mothers who do not work outside the home’, and ranges from 6 to

20
36. Mothers also filled out the Work Commitment Scale (Grinberger and Goldberg, 1989),
higher work commitment relates to higher role salience. The scale was constructed from 8 items,
each ranges from 1=strongly disagree to 6=strongly agree, the scale ranges from 8 to 48. We
pulled out one item that especially reflects the commitment toward work role-‘career is central
to my self-esteem’.
We sum additional parent role salience related item from three available subscales of the
Parental Stress Index: Attachment, Restrictions of Role and Sense of Competence (Abidin,
1982) with the resulting score ranging from 25 to 125. Additionally, we use a 20-item revised
version of Parental Locus of Control Scale that measures a total internal vs. external locus of
control, parental efficacy, parental responsibility, child control of parent’s life, parental belief in
fate/chance, and parental control of the child behavior (Campis, Lyman and Prentice-Dunn,
1986). The scale ranges from 20 to 100. Finally, Parenting Experience measure adopted from
Marshal and Barnet (1991) Parent-Role Scale and consists of 10 concern and 10 reward items.
Each item ranges from 1=Not at all a concern to 4=Extreme concern. The standard scale score’s
theoretical range is from -3 to 3, the higher score indicates higher parenting stress.
Control Variables
In our analysis, we adjusted for several time-varying and time-constant characteristics,
which prior theory and research suggests may correlate with child care characteristics and
depression.
We adjusted for time-varying indicators of life events, including family members’ lay
offs, death, or illness or the mother’s report of a “big difference” happening in family and the
mother’s reports of her own, the baby’s and, where applicable, her partner’s health.

21
Time-constant covariates included mothers’ age at the time of the child’s birth, her
educational level, mother’s income before the child was born, mother’s race, whether the child
was female and the number of days the child spent in the hospital. We also adjusted for the
baby’s temperament, the scale consists of 14 items, each ranges from 1=Almost never (occur) to
6=Almost always (occur), the higher score indicates difficult child temperament. A separate item
specifically measures difficult child temperament versus above average temperament or easier
than average temperament. Additionally, we adjusted for the quality of the marital relationship as
reported by mothers at the 1 month interview, the higher average score of 6 items indicates better
mother/partner relationship. Lastly, benefits – parental, sick, and vacation leave with or without
the pay – were assessed from the mothers’ report of her employment in the year before the child
was born.
Results
Social Roles and Mental Health
We begin by replicating the well-documented result from prior research that women’s
employment is associated with better mental health. We run four regression models, two OLS
models without fixed effects and two fixed effects models, one of each with minimal measured
controls (site and wave dummies and an indicator for the number of variables with a missing
value) and the other with extensive measured controls (with the covariate results provided in
Appendixes).
First looking at the model without fixed effects and minimal measured controls we find
that within our sample of mothers of young children, mothers who are employed are significantly
less depressed than those who are not (see Table 1, Model 1). The difference is over two points
on the CES-D, nearly one-quarter of the measure’s standard deviation. Specifically, women who

22
are not employed score a 10.56 on the CES-D whereas women who are employed score a 8.55,
on average. This difference is reduced substantially in magnitude and becomes nonsignificant
when we add numerous measured controls (Model 2) and the difference is smaller still when we
introduce fixed effects into the model (Models 3 and 4; The full models including covariates are
in Appendix 2). Predictions based on Model 3 illustrate the similar depression levels of women
who are and are not employed, once fixed effects are adjusted: Mothers who are not employed
score a 9.25 on the CES-D whereas women who are employed score a 9.06. These results reveal
that the descriptive association between maternal employment and better mental health is evident
in our sample, consistent with prior research, but that adjustment for measured and unmeasured
controls is important as we interpret this association. Specifically, our findings suggest that the
descriptive association is a result of selective sorting of mothers into social roles, rather than a
causal effect of those roles on mental health. We continue to control for these confounds as we
examine variation in depression among the mothers who are employed.
Strains in Employed Mothers’ Roles
We next consider whether strains associated with employed mothers’ roles explains
variation in their depression levels. To allow for a larger sample size, and continue to contrast
employed with non-employed mothers, we utilize the full sample. Similar results are evident
when we restrict the model to mothers who are employed and using child care at all four waves
(details available from the authors). We tested for, but did not find, interactions by child’s age
(wave), by maternal employment status, and by use of child care.
We begin by examining the association between each of the main child care
characteristics and maternal depression in models with minimal controls (site and wave dummies
and an indicator for the number of variables with a missing value) both with and without fixed
23
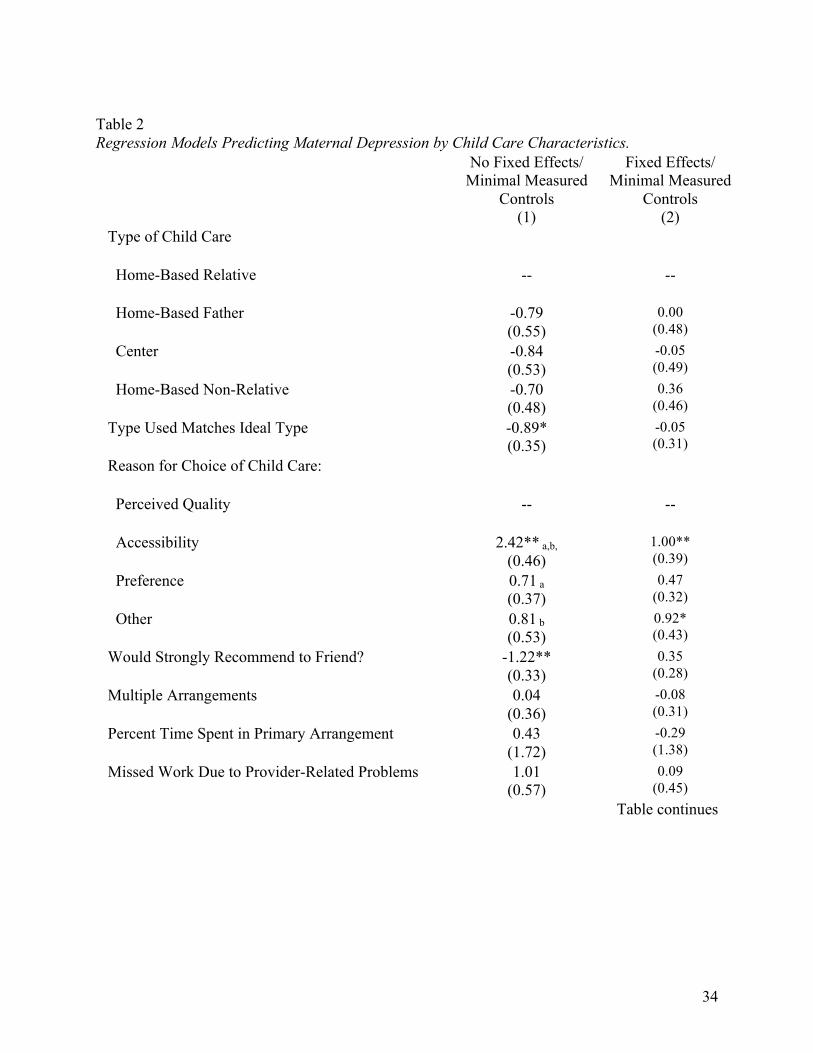
effects. The results, presented in Table 2, partially replicate prior cross-sectional research and
again demonstrate the importance of controlling for confounds through fixed effects. Consistent
with our expectation and prior studies reviewed above, mothers are less depressed when the type
of care they use matches their ideal type of care, when they would strongly recommend their care
setting to a friend, and when they chose their care setting for quality reasons (see Model 1, Table
2). Similarly, missing work due to provider-related problems tends to associate with higher
depression scores (b = 1.01, p < .08). But, most of these coefficients becomes small and
nonsignificant in the fixed effects model. The exception is the reason for choosing care, which
we will discuss further below. As noted above, the direction of association between type of care
and depression is ambiguous, and results from prior research are inconsistent. We find no
significant variation by type of care (Whereas prior to the introduction of fixed effects there is a
trend toward mothers having lower depression levels when they do not use home-based relative
care, these associations become close to zero and nonsignificant in the fixed effects model).
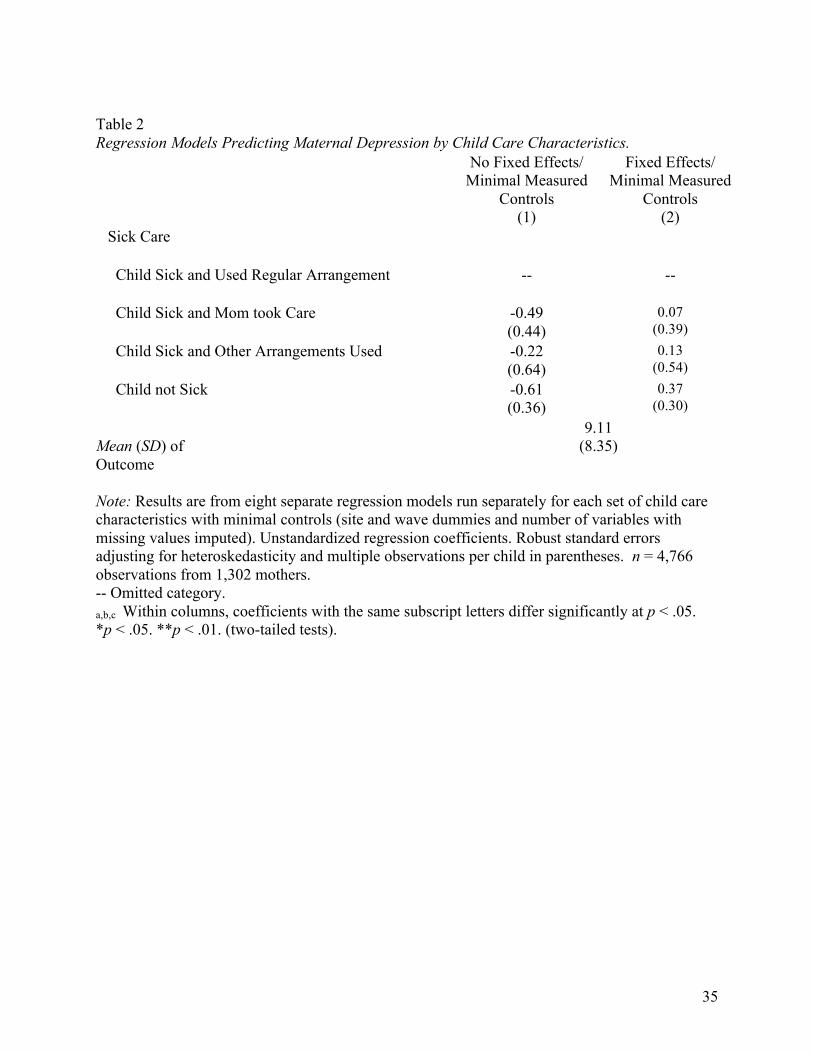
Likewise, use of multiple arrangements, percentage time spent in the primary arrangement, and
needing to arrange for sick care are not associated with maternal depression before or after the
introduction of fixed effects.
We next include all the child care characteristics together in a single model and include
extensive measured controls, both with and without fixed effects. We focus our discussion on
the fixed-effects results. Table 3 provides results for the only child care characteristic that is
significantly associated with maternal depression: the reason for choosing the child care setting
(The full models with all child care characteristics and covariates are in Appendix 3). In the
fixed-effects model, mothers who chose their child’s care setting for accessibility or other
reasons are significantly more depressed than those who chose the setting for quality reasons.

24
The difference between choosing because of preference and because of quality is nearly
significant as well, at p < .052. Average maternal depression levels are not significantly different
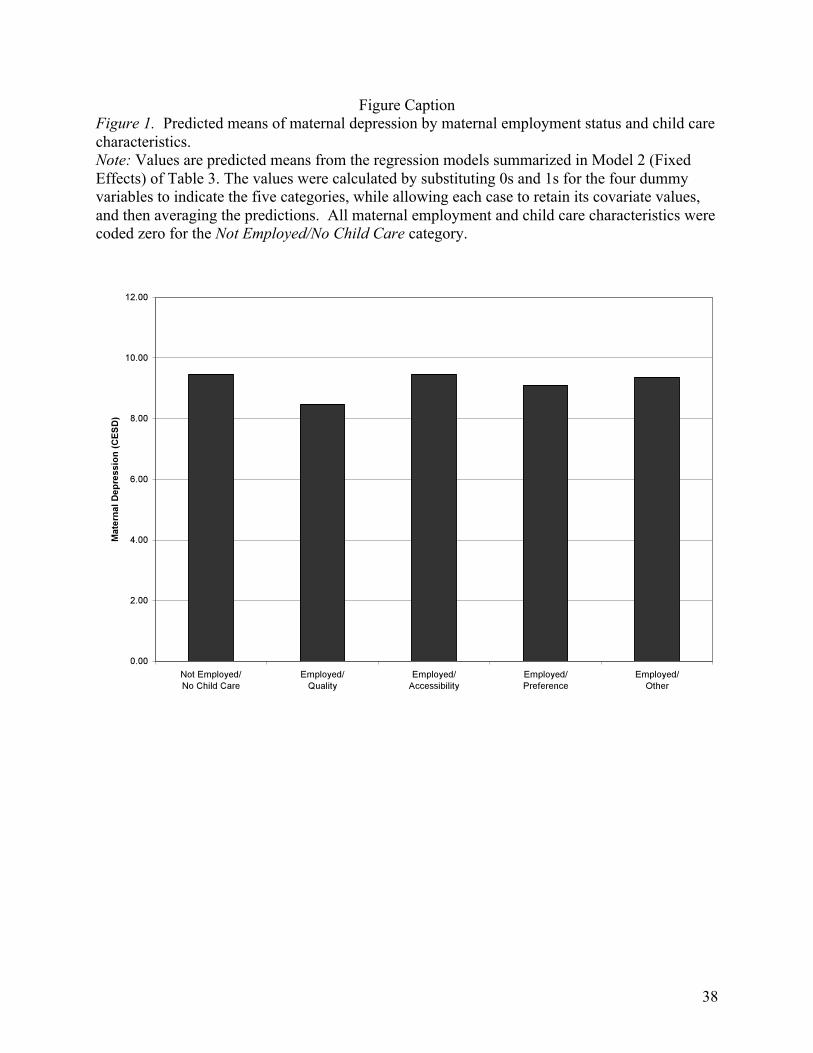
among the three non-quality reasons. To illustrate the substantive significance of these
significant contrasts, Figure 1 plots the predicted means based on the fixed-effects model. The
plot shows that employed mothers who chose the child’s care setting for quality reasons have the
lowest average depression scores – nearly one point lower than the other groups (a difference of
over 10% of the standard deviation of CES-D).
We did not find an interaction between child care characteristics and maternal
employment status in our initial models (not shown). Still, we ran an alternative specification
that cross-classified employment status, child care use and the reason for choosing a child care
setting to provide a more direct comparison of the groups. The results are found in Table 4
(Appendix 4 contains the full models). The fixed-effects results confirm that mothers who are
employed and chose their care setting for quality reasons are less depressed than those who are
either not employed and not using child care (first row of Table 4) or are employed but chose
care for reasons other than quality (fifth row of Table 4). Average depression levels are
statistically equivalent in the two contrast groups – Not Employed/No Child Care and
Employed/Not Chosen for Quality. The three groups Not Employed/No Child Care,
Employed/Not Chosen for Quality, Employed/ Chosen for Quality have the largest sample sizes.
Yet, in the fixed-effects model, the smallest group – women who are not employed and using
child care that they chose for quality reasons – score significantly lower on the CES-D than
several other groups. Further, although this Not Employed/Chosen for Quality group scores
lower on depression than the Employed/Chosen for Quality group, the difference between these
two groups is not significant.

25
Figure 2 presents the predicted means based on the fixed-effects model of Table 4,
visualizing the pattern of significant differences just discussed and illustrating the magnitude of
these differences. As noted, women who are not employed and are using care they chose for
quality reasons have the lowest average depression scores – less than 8 points on average. This
level is statistically equivalent to the average depression scores of women who are employed and
using care they chose for quality (X = 8.64). The average depression scores for all of the
remaining groups are all above 9 points and do not differ significantly from one another,
although several differ significantly from one or both groups of women who chose care for
quality reasons. The largest differences are above 1 point in magnitude (e.g., between the
leftmost bar Not Employed/No Child Care and the rightmost bar Employed/Quality), which is
over 10% of the sample standard deviation of the CES-D measure.
Thus, when we take child care characteristics into account we further illuminate the
finding of prior research that isolated mothers who are not working in the paid labor force have
high levels of depression. However, the contrast with employed mothers depends on the reason
mothers chose their child’s care. It is only mothers who are employed and using care they chose
for quality reasons that are less depressed than “stay at home” mothers. Mothers who are
employed and chose care for other reasons are equally as depressed as mothers who “stay at
home.” Furthermore, although the smallest group in the sample, mothers who “stay at home” but
use child care that they chose for quality reasons have low levels of depression; they are
significantly less depressed than those who “stay at home” but do not use any child care.
Discussion
These preliminary findings add to the body of literature on social roles and depression by
demonstrating that mothers of young children benefit from employment only when their child

26
care arrangements were selected for quality reasons. When mothers chose their child care
arrangement for cost or convenience, purely for preference for the type of care, or other reasons,
they report depression levels that are equivalently as high as mothers who “stay at home.” We
also find that among mothers who “stay at home” depression levels are lower when they are
using child care arrangements that they chose for quality reasons. Although a relatively smaller
absolute number of women, they make up nearly 15% of “stay at home” mothers. Their use of
quality child care may reduce some of the isolation and stress associated with full-time
parenting.
Our final paper will also present results of tests for the possible moderation noted in the
introduction. Are the strains of child care alleviated by social support or income? Are they
accentuated if the mother is anxious about leaving the child or places great value on the
parenting role? Are mothers particularly depressed if they work for pay at a “bad” job and use
“bad” child care? Some of these models must be estimated on only the first two waves of data (6
and 15 months) because the measures (particularly perceptions of roles) were not continued at
the later waves. Also, some measures of child care characteristics were only gathered at 6 and
15 months, and we plan to examine these further in the final paper. Our final paper will also
present results based on multiple rather than simple imputation.

27
References
Abidin R.R. (1983). Parenting stress and the utilization of pediatric services. Children’s
Health Care, 11, 70-73.
Acock, A.C. (2005). Working with missing values. Journal of Marriage and
the Family, 67(4), 1012-1028.
Barnett, R.C. and Marshall, N.L. 1991. The Relationship between women’s work and
family roles and their subjective well-being and psychological distress. In M. Frankenhaeuser, U.
Lundberg and M. Chesney(Eds.), Women, work and health: Stress and opportunities.(pp.111-
136). New-York: Plenum.
Barnett, Rosalind C., Brennan, Robert T., and Marshall, Nancy L. 1994. Gender and the
relationship between parent role quality and psychological distress: A study of men and women
in dual-earner couples. Journal of Family Issues, 15(2), 229-252.
Beegly M., Weinberg M.K., Olson K.L., Hernan H. Riley J. and E.Z. Tronick. 2002.
Stability and change in level of maternal depressive symtomatology during the first postpartum
year. Journal of affective disorder 71, 169-180.
Bird, Chloe. 1997. Gender differences in the social and economic burden of parenting
and psychological distress. Journal of Marriage and the Family, 59, 809-823.
Burris, Beverly. 1991. Employed mothers: The impact of class and marital status on the
prioritizing of family and work. Social Science Quarterly, 7, 50-66.
Campis, L.K., Lyman, R.D. and Prentice-Dunn, S. (1986). The Parental Locus of control
Scale: Development and Validation. Journal of Clinical Child Psychology, 15, 260-267.

28
Crouter, Ann C., Perry-Jenkins, Maureen, Huston, Ted L., and McHale, Susan M. 1987.
Processes underlying father involvement in dual-earner and single-earner families.
Developmental Psychology, 23, 431-440.
Cryer, Debby and Burchinal, Margaret. 1997. Parents as child care consumers. Early
Childhood Research Quarterly, 12, 35-58.
DeMeis, D.K., Hock, E. and McBride, S. L. 1986. The balance of employment and
motherhood: Longitudinal study of mothers’ feelings about separation from their first-born
infants. Developmental Psychology, 22, 627-632.
Evenson, Ranae J. and Simon, Robin W. 2005. Clarifying the relationship between
parenthood and depression. Journal of Health and Social Behavior, 46, 341-358.
Fagan, Jay. 1994. Factors related to depression among higher income mothers with young
children in day care centers. Early Child Development and Care, 99, 79-92.
Fuller, Bruce, Kagan, Sharon Lynn, Loeb, Susanna, and Chang, Yueh-Wen. 2004. Child
care quality: Centers and home settings that serve poor families. Early Childhood Research
Quarterly, 19, 505-527.
Glass, Jennifer. 1998. Gender liberation, economic squeeze, or fear of strangers: Why
fathers provide infant care in dual-earner families. Journal of Marriage and the Family, 60, 821-
834.
Goodman, Sherryl H. 2007. Depression in Mothers. Annual Review of Clinical
Psychology, 3, 107-135.
Gordon, Rachel A., Robert Kaestner, and Sanders Korenman. Forthcoming. Child Care
and Work Absences: Tradeoffs by Type of Care. Journal of Marriage and Family.

29
Gordon, Rachel A. and Robin S. Högnäs. 2006. The Best Laid Plans: Expectations for
Child Care and the Stability of Care Arrangements. Journal of Marriage and Family, 68, 373-
393.
Gove, Walter R. 1972. The relationship between sex roles, marital status, and mental
illness. Social Forces, 51, 34-44.
Grenberger, E., Goldberg W.A., Crawford, T.J. and Cranger, J. (1988). Beliefs about the
consequences of maternal employment for children. Psychology of Women Quarterly, 12, 35-59.
Grenberger, E. and Goldberg, W.A. (1989). Work, parenting, and the socialization of
children . Developmental Psychology, 25, 22-35.
Hennegan Amy M., Ellen Johnson Silver, Laurie J. Bauman, Lauren E. Westbrook and
Ruth E.K. Stein (1998). Depressive Symptoms in Inner-city Mothers of Young Children: Who is
at Risk. Pediatrics, 102, 1394-1400.
Henly, J.R. & Lyons, S. (2000). The negotiation of child care and employment demands
among low_income parents. Journal of Social Issues, 56(4), 683_706.
Hock, Ellen and Wilma J. Lutz. 1998. Psychological meaning of separation anxiety in
mothers and fathers. Journal of Family Psychology, 12(1), 41-55.
Hughes, Diane L. and Galinsky, Ellen. 1994. Gender, job and family conditions and
psychological symptoms. Psychology of Women Quarterly, 18, 251-270.
Johansen, Anne S., Leibowitz, Arleen, and Waite, Linda J. 1996. The importance of
child-care characteristics to choice of care. Journal of Marriage and the Family, 58, 759-772.
Kontos, Susan, Howes, Carollee, Shinn, Marybeth, and Galinsky, Ellen. 1995. Quality in
family child care and relative care. New York: Teachers College Press.
30
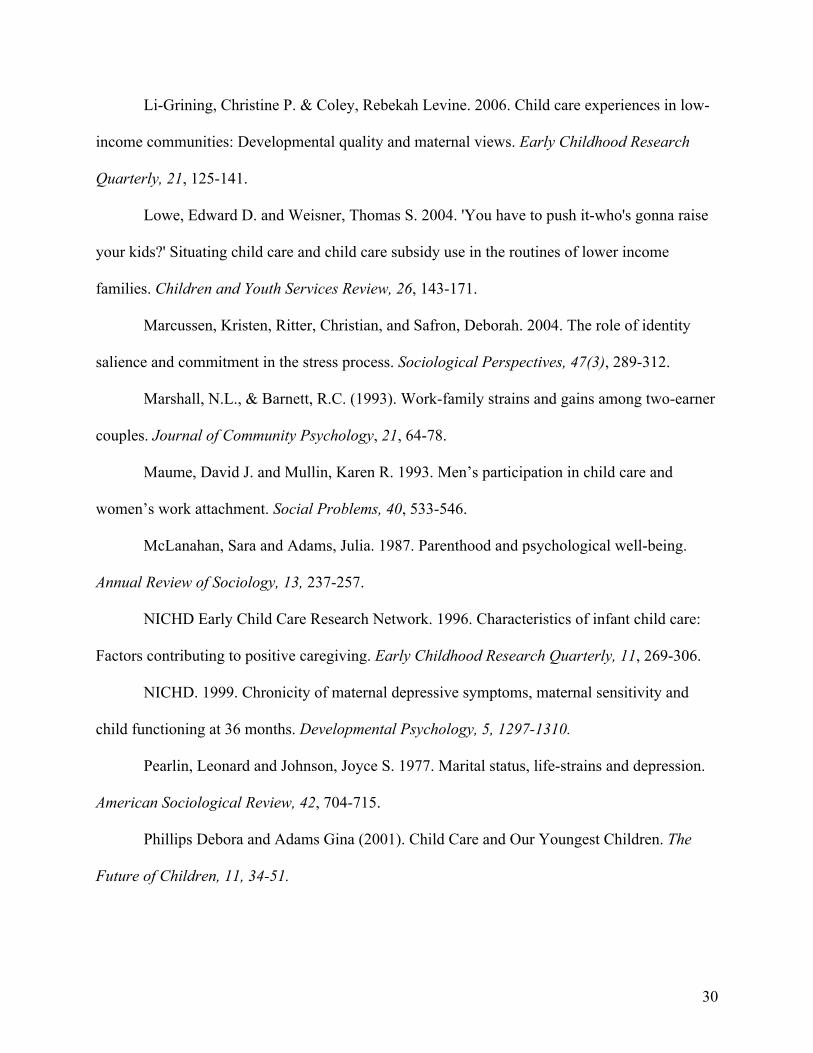
Li-Grining, Christine P. & Coley, Rebekah Levine. 2006. Child care experiences in low-
income communities: Developmental quality and maternal views. Early Childhood Research
Quarterly, 21, 125-141.
Lowe, Edward D. and Weisner, Thomas S. 2004. 'You have to push it-who's gonna raise
your kids?' Situating child care and child care subsidy use in the routines of lower income
families. Children and Youth Services Review, 26, 143-171.
Marcussen, Kristen, Ritter, Christian, and Safron, Deborah. 2004. The role of identity
salience and commitment in the stress process. Sociological Perspectives, 47(3), 289-312.
Marshall, N.L., & Barnett, R.C. (1993). Work-family strains and gains among two-earner
couples. Journal of Community Psychology, 21, 64-78.
Maume, David J. and Mullin, Karen R. 1993. Men’s participation in child care and
women’s work attachment. Social Problems, 40, 533-546.
McLanahan, Sara and Adams, Julia. 1987. Parenthood and psychological well-being.
Annual Review of Sociology, 13, 237-257.
NICHD Early Child Care Research Network. 1996. Characteristics of infant child care:
Factors contributing to positive caregiving. Early Childhood Research Quarterly, 11, 269-306.
NICHD. 1999. Chronicity of maternal depressive symptoms, maternal sensitivity and
child functioning at 36 months. Developmental Psychology, 5, 1297-1310.
Pearlin, Leonard and Johnson, Joyce S. 1977. Marital status, life-strains and depression.
American Sociological Review, 42, 704-715.
Phillips Debora and Adams Gina (2001). Child Care and Our Youngest Children. The
Future of Children, 11, 34-51.

31
Press, Julie, Fagan, Jay, and Bernd, Elisa. 2006. Child care, work, and depressive
symptoms among low-income mothers. Journal of Family Issues, 27, 609-632.
Radloff, L.S. 1977. The CES-D scale: A self-report depression scale for research in
general population. Applied Psychological Measurement, 1: 385-401.
Riley, Lisa A., & Glass, Jennifer L. 2002. You can't always get what you want: Infant
care preferences and use among employed mothers. Journal of Marriage and Family, 64, 2 - 15.
Roberts R.E. 1980 Reliability of CES-D scale in different ethnic contexts. Psychiatry
Research, 2. 125-134.
Ross, Catherine E. and Mirowsky, John. 1988. Child care and emotional adjustment to
wives’ employment. Journal of Health and Social Behavior, 29, 127-138.
Royston, P. (2005). Multiple imputation of missing values: Update of ice.
Stata Journal, 5(4), 527-536.
Scott, Ellen K., London, Andrew S., & Hurst, Allison. 2005. Instability in patchworks of
child care when moving from welfare to work. Journal of Marriage and the Family, 67(2), 370-
386.
Thoits, Peggy A. 1995. Identity-relevant events and psychological symptoms: A
cautionary tale. Journal of Health and Social Behavior, 36(1), 72-82.
Umberson, Debra and Gove, Walter R. 1989. Parenthood and psychological well-being.
Theory, measurement, and stage in the family life course. Journal of Family Issues, 10, 440-462.
Vandell, Deborah Lowe, Hyde, Janet, Plant, E. Ashby, and Essex, Marilyn J. 1997.
Fathers and “others” as infant-care providers: Predictors of parents’ emotional well-being and
marital satisfaction. Merrill-Palmer Quarterly, 43, 361-385.

32
Weisman M.M., Sholomskas, D., Pottenger, M., Prusoff B.A. and Locke, B.Z. Assessing
depressive symptoms in five psychiatric populations: A validation study. American Journal of
Epidemiology 106: 203-214.
Wrigley, Julia and Dreby, Joanna. 2005. Fatalities and the organization of child care in
the United States, 1985-2003. American Sociological Review, 70, 729-757.

33
Table 1 Regression Models Predicting Maternal Depression by Maternal Employment Status and Covariates
No Fixed Effects/ Minimal Measured
Controls (1)
No Fixed Effects/ Extended Measured
Controls (2)
Fixed Effects/ Minimal Measured
Controls (3)
Fixed Effects/ Extended Measured
Controls (4)
Mother is Employed
-2.01** (0.40)
-0.27 (0.33)
-0.20 (0.38)
-0.11 (0.36)
Mean (SD) of Outcome
9.11 (8.35)
Note: Unstandardized regression coefficients. Robust standard errors adjusting for heteroskedasticity and multiple observations per child in parentheses. Full models in Appendix 2. n = 4,766 observations from 1,302 mothers. *p < .05. **p < .01. (two-tailed tests).
34
Table 2 Regression Models Predicting Maternal Depression by Child Care Characteristics. No Fixed Effects/
Minimal Measured Controls
(1)
Fixed Effects/ Minimal Measured
Controls (2)
Type of Child Care
Home-Based Relative --
--
Home-Based Father -0.79 (0.55)
0.00 (0.48)
Center -0.84 (0.53)
-0.05 (0.49)
Home-Based Non-Relative -0.70 (0.48)
0.36 (0.46)
Type Used Matches Ideal Type -0.89* (0.35)
-0.05 (0.31)
Reason for Choice of Child Care:
Perceived Quality --
--
Accessibility 2.42** a,b, (0.46)
1.00** (0.39)
Preference 0.71 a (0.37)
0.47 (0.32)
Other 0.81 b (0.53)
0.92* (0.43)
Would Strongly Recommend to Friend? -1.22** (0.33)
0.35 (0.28)
Multiple Arrangements 0.04 (0.36)
-0.08 (0.31)
Percent Time Spent in Primary Arrangement 0.43 (1.72)
-0.29 (1.38)
Missed Work Due to Provider-Related Problems 1.01 (0.57)
0.09 (0.45)
Table continues
35
Table 2 Regression Models Predicting Maternal Depression by Child Care Characteristics. No Fixed Effects/
Minimal Measured Controls
(1)
Fixed Effects/ Minimal Measured
Controls (2)
Sick Care
Child Sick and Used Regular Arrangement --
--
Child Sick and Mom took Care -0.49 (0.44)
0.07 (0.39)
Child Sick and Other Arrangements Used -0.22 (0.64)
0.13 (0.54)
Child not Sick -0.61 (0.36)
0.37 (0.30)
Mean (SD) of Outcome
9.11 (8.35)
Note: Results are from eight separate regression models run separately for each set of child care characteristics with minimal controls (site and wave dummies and number of variables with missing values imputed). Unstandardized regression coefficients. Robust standard errors adjusting for heteroskedasticity and multiple observations per child in parentheses. n = 4,766 observations from 1,302 mothers. -- Omitted category. a,b,c Within columns, coefficients with the same subscript letters differ significantly at p < .05. *p < .05. **p < .01. (two-tailed tests).

36
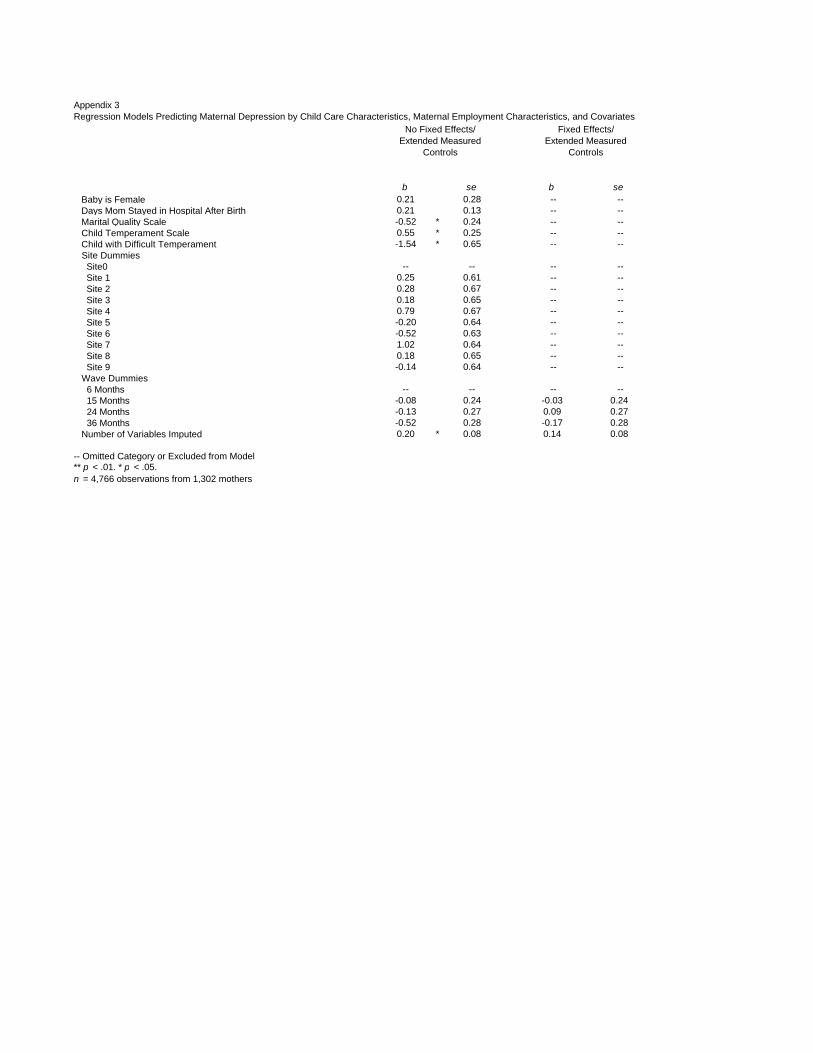
Table 3 Regression Models Predicting Maternal Depression by Child Care Characteristics, Maternal Employment Characteristics, and Covariates
No Fixed Effects/ Extended Measured
Controls (1)
Fixed Effects/ Extended Measured
Controls (2)
Reason for Choice of Child Care:
Perceived Quality -- --
Accessibility 0.81* (0.36)
0.98* (0.39)
Preference 0.56 (0.33)
0.65 (0.33)
Other
0.29 (0.44)
0.90* (0.41)
Mean (SD) of Outcome
9.11 (8.35)
Note: Unstandardized regression coefficients. Robust standard errors adjusting for heteroskedasticity and multiple observations per child in parentheses. Full models in Appendix 3. n = 4,766 observations from 1,302 mothers. -- Omitted category. *p < .05. **p < .01. (two-tailed tests).

37
Table 4 Regression Models Predicting Maternal Depression by Child Care and Maternal Employment Categories and Covariates
n
No Fixed Effects/ Extended Measured
Controls (1)
Fixed Effects/ Extended Measured
Controls (2)
Child Care and Maternal Employment Categories
Not Employed/ No Child Care
933
0.88*a (0.43)
1.05* a (0.46)
Not Employed/ Not Chosen for Quality
218
0.17 (0.58)
0.36 (0.59)
Not Employed/ Chosen for Quality
188
-0.19 a (0.53)
-0.87a,b,c (0.60)
Employed/ No Child Care
413
0.63 (0.41)
0.52 b (0.47)
Employed/ Not Chosen for Quality
1568
0.39 (0.27)
0.60* c (0.27)
Employed/ Chosen for Quality
1407
-- --
Mean (SD) of Outcome
9.11 (8.35)
Note: Unstandardized regression coefficients. Robust standard errors adjusting for heteroskedasticity and multiple observations per child in parentheses. Full models in Appendix 4. n = 4,727 observations from 1,300 mothers. -- Omitted category. a,b,c Within columns, coefficients with the same subscript letters differ significantly at p < .05. *p < .05. **p < .01. (two-tailed tests).
38
Figure Caption Figure 1. Predicted means of maternal depression by maternal employment status and child care characteristics. Note: Values are predicted means from the regression models summarized in Model 2 (Fixed Effects) of Table 3. The values were calculated by substituting 0s and 1s for the four dummy variables to indicate the five categories, while allowing each case to retain its covariate values, and then averaging the predictions. All maternal employment and child care characteristics were coded zero for the Not Employed/No Child Care category.

39
Figure Caption Figure 2. Predicted means of maternal depression within categories of child care and maternal employment. Note: Values are predicted means from the regression models summarized in Model 2 (Fixed Effects) of Table 4. The values were calculated by substituting 0s and 1s for the five dummy variables to indicate the six categories, while allowing each case to retain its covariate values, and then averaging the predictions.

40
Appendix 1
Definition and Descriptive Statistics of Covariates Variables N M Min Max Dependent Variable Maternal Depression 4766 9.11 0 57 Child Care Variables Characteristics of Care Mom is Using Care 5053 0.71 0 1 Type of Child Care Home-Based Fatherc 5037 0.13 0 1 Home-Based Relativec 5037 0.14 0 1 Home-Based Non-Relativec 5037 0.17 0 1 Centerac Type Used Matches Ideal Typec 5037 0.29 0 1 Maternal Perceptions of Child Care Reason for Choice of Child Care: Accessibilityc 5000 0.12 0 1 Preferencec 5000 0.19 0 1 Perceived Qualityac 5000 0.33 0 1 Otherc 5000 0.07 0 1 Would Strongly Recommend to Friend?c 5015 0.53 0 1 Perceive Child Care as Goodbc 5088 3.69 1 5 Perceive Child Care as Affordable and Can Earnb 5092 7.14 2 10 Strain Associated with Child Care Percent Time Spent in Primary Arrangementc 5052 0.69 0 1 Multiple Arrangementsc 5053 0.21 0 1 Missed Work Due to Provider-Related Problemse 4951 0.05 0 1 Sick Care Child Sick and Mom took Caree 4954 0.13 0 1 Child Sick and Used Regular Arrangementae 4954 0.09 0 1 Child Sick and Other Arrangements Usede 4954 0.04 0 1 Child not Sicke 4954 0.35 0 1 Thinking About Child When at Work Interferes with Performance?d 2397 0.18 0 1 Moderators Social Support Spouse or Partner in Household 4945 0.85 0 1 Number of Other Adults in Household 4944 0.09 0 5 Perceived Emotional Support 4826 34.78 8 42 Perceived Instrumental Support 4838 14.73 3 18 Income Total Household Income 4724 70729 0 699474 Maternal Incomed 5014 19748 0 348004 Paternal Incomef 4906 41575 0 358480 Other Income 4811 8306 0 358480 Public Assistance 4830 0.20 0 1

41
Table Continues
Appendix 1 Definition and Descriptive Statistics of Covariates
Variables N M Min Max Role Salience
Employment/School Role Salienceb 5452 3.79 1 5 Parental Role Salience (Maternal Separation Anxiety Scale)b 5324 70.16 35 105 When Away From Child, Wonder if Physical Needs are Being Metb 5432 3.76 1 5 Perceptions of Ideal Work/Family Situationb Ideal Type-Work or School Full Time 5452 0.13 0 1 Ideal Type-Work or School Part Time 5452 0.53 0 1 Ideal Type-Stay Home Full Timea 5452 0.34 0 1 Attitude Toward Maternal Employment (standard scaling) 5412 34.13 11 63 Positive Employment Attitudes 5440 19.19 5 30 Negative Employment Attitudes 5420 18.33 6 36 Career Central to Self-Esteem 5448 3.64 1 6 What Employment Means to Me 5420 25.77 8 47 Feelings about Parenting 5412 53.18 27 94 Children and Their Parents (Parental Locus of Control) 5380 47.79 24 75 Parent experiences 4916 -1.59 -3 0.8 Control Variables Time-Varying Characteristics Employment Mom is Employed 5045 0.71 0 1 Occupation is Professional, Administrative, Executive, Manageriald M
4999 0.28 0 1 Job Experience Scaled 4350 -0.78 -3 2.53 Work Hoursd 5045 22.01 0 134 Shift Exclusive Day Shiftd 4724 0.45 0 1 Varying Shiftd 4724 0.07 0 1 Other Shift (Some Weeknight/Weekend)d 4724 0.16 0 1 Work Flexibility Inflexible Workd 4724 0.26 0 1 Somewhat Flexible Workd 4724 0.27 0 1 Flexible Workad 4724 0.16 0 1 Life Events Job Loss in Family 4943 0.20 0 1 Illness in family 4944 0.34 0 1 Death In Family 4943 0.24 0 1 Big Difference in Family 4943 0.43 0 1 Health Poor Health - Baby 4945 0.14 0 1 Poor Health - Mom 4943 0.15 0 1 Poor Health - Partner 4945 0.11 0 1
Table continues

42
Appendix 1 Definition and Descriptive Statistics of Covariates
Variables N M Min Max Household Composition Number of Preschool Age Children in Household 4944 0.16 0 5 Number of School Age Children in Household 4944 0.07 0 7 Time-Constant Characteristics Mom's Age 5456 28.10 18 46 Mom's Education 5452 14.23 7 21 Mom's Race Whitea 5456 0.81 0 1 Black 5456 0.13 0 1 Other 5456 0.05 0 1 Baby is Female 5456 0.48 0 1 Days Mom Stayed in Hospital After Birth 5456 2.34 0 10 Mom's Income Before the Birthg 5416 26013 0 399700 Leave Benefit with Pay 5344 0.44 0 1 Leave Benefit with No Pay 5308 0.40 0 1 Marital Quality Scale 5080 4.02 1.17 5 Child Temperament Scale 5036 3.32 1.42 5.35 Child with Difficult Temperament 5448 .004 0 1
Note: Wave and site dummies not shown. Data were distributed evenly for these variables (each site contained 9 - 11 % of the sample and each wave contained 25% of the sample). a Omitted category. b Time-constant version of the variable presented, time varying version was used for the 6,15 wave analyses. c The variable was assigned to 0 if mother did not use child care arrangements. d The variable was assigned to 0 if mother was not employed. e The variable was assigned to 0 if mother did not use child care or was not employed. f The variable was assigned to 0 if spouse or partner was absent from household. g The variable was assigned to 0 if mother was not employed in the year before baby was born.

b se b se b se b se Mom is Employed -2.01 ** 0.40 -0.27 0.33 -0.20 0.38 -0.11 0.36 Spouse or Partner in Household -- -- -1.44 ** 0.50 -- -- -1.03 0.69 Number of Other Adults in Household -- -- -0.04 0.28 -- -- -0.02 0.29 Perceived Emotional Support -- -- -0.47 ** 0.05 -- -- -0.31 ** 0.05 Perceived Instrumental Support -- -- -0.14 0.08 -- -- -0.24 ** 0.07 Paternal Income ($1000) -- -- 0.00 0.00 -- -- -0.01 0.01 Other Income ($1000) -- -- 0.00 0.00 -- -- -0.01 * 0.00 Public Assistance -- -- 1.36 ** 0.44 -- -- 0.10 0.50 Employment/School Role Salience -- -- -0.05 0.12 -- -- -- -- Perceptions of Ideal Work/Family Situation Ideal Type-Stay Home Full Time -- -- -- -- -- -- -- -- Ideal Type-Work or School Full Time -- -- 0.24 0.52 -- -- -- -- Ideal Type-Work or School Part Time -- -- 0.12 0.34 -- -- -- -- Attitude Toward Maternal Employment -- -- 0.02 0.02 -- -- -- -- Career Central to Self-Esteem -- -- 0.35 ** 0.10 -- -- -- -- Feelings about Parenting -- -- 0.09 ** 0.02 -- -- -- -- Children and Their Parents (Parental Locus of Control) -- -- 0.03 0.02 -- -- -- -- When Away From Child, Wonder if Physical Needs are Being Met -- -- 0.17 0.12 -- -- -- -- Job Loss in Family -- -- 0.81 ** 0.28 -- -- 0.17 0.27 Illness in family -- -- 0.74 ** 0.24 -- -- 0.57 ** 0.22 Death In Family -- -- 0.78 ** 0.26 -- -- 0.28 0.24 Big Difference in Family -- -- 1.36 ** 0.24 -- -- 0.84 ** 0.22 Poor Health - Baby -- -- 0.13 0.33 -- -- -0.10 0.34 Poor Health - Mom -- -- 2.67 ** 0.38 -- -- 1.15 ** 0.39 Poor Health - Partner -- -- 1.00 * 0.44 -- -- -0.54 0.40 Number of Preschool Age Children in Household -- -- 0.46 0.28 -- -- 0.43 0.25 Number of School Age Children in Household -- -- -0.02 0.30 -- -- -0.02 0.37 Mother's Age When Child Born -- -- -0.05 0.03 -- -- -- -- Mother's Education When Child Born -- -- -0.32 ** 0.08 -- -- -- -- Mother's Race White -- -- -- -- -- -- -- -- Black -- -- 0.27 0.55 -- -- -- -- Other -- -- 0.40 0.68 -- -- -- -- Baby is Female -- -- 0.21 0.28 -- -- -- -- Days Mom Stayed in Hospital After Birth -- -- 0.20 0.13 -- -- -- -- Mom's Income Before the Birth ($1000) -- -- -0.01 0.01 -- -- -- -- Job Offered Leave Benefit with Pay -- -- 0.04 0.34 -- -- -- -- Job Offered Leave Benefit with No Pay -- -- -0.61 * 0.30 -- -- -- -- Marital Quality Scale -- -- -0.55 * 0.24 -- -- -- -- Child Temperament Scale -- -- 0.57 * 0.25 -- -- -- -- Child with Difficult Temperament -- -- -1.52 * 0.64 -- -- -- -- Site Dummies Site0 -- -- -- -- -- -- -- -- Site 1 -1.58 * 0.73 0.09 0.61 -- -- -- -- Site 2 0.43 0.85 0.13 0.66 -- -- -- -- Site 3 -0.48 0.83 -0.01 0.63 -- -- -- --
Appendix 2Regression Models Predicting Maternal Depression by Maternal Employment Status and Covariates
No Fixed Effects/Minimal Measured
Controls
No Fixed Effects/Extended Measured
ControlsFixed Effects/
Minimal Measured ControlsFixed Effects/
Extended Measured Controls

b se b se b se b se
Appendix 2Regression Models Predicting Maternal Depression by Maternal Employment Status and Covariates
No Fixed Effects/Minimal Measured
Controls
No Fixed Effects/Extended Measured
ControlsFixed Effects/
Minimal Measured ControlsFixed Effects/
Extended Measured Controls
Site 4 0.39 0.89 0.60 0.67 -- -- -- -- Site 5 -1.07 0.79 -0.30 0.63 -- -- -- -- Site 6 -1.10 0.79 -0.63 0.62 -- -- -- -- Site 7 0.34 0.81 0.84 0.63 -- -- -- -- Site 8 0.84 0.87 0.08 0.65 -- -- -- -- Site 9 -0.37 0.81 -0.20 0.64 -- -- -- -- Wave Dummies 6 Months -- -- -- -- -- -- 15 Months 0.17 0.22 -0.14 0.22 0.06 0.23 -0.09 0.23 24 Months 0.49 0.26 -0.17 0.26 0.52 * 0.25 0.04 0.25 36 Months 0.29 0.26 -0.63 * 0.26 0.31 0.24 -0.29 0.26 Number of Variables Imputed 0.47 ** 0.09 0.17 * 0.07 0.13 0.07 0.09 0.07
-- Omitted Category or Excluded from Model** p < .01. * p < .05.n = 4,766 observations from 1,302 mothers

b se b se Mom is Using Care -0.32 1.51 -0.97 1.42 Type of Child Care Relative -- -- -- -- Father -0.37 0.47 0.02 0.50 Center -0.09 0.51 0.18 0.56 Non-Relative 0.22 0.42 0.65 0.47 Type Used Matches Ideal Type -0.37 0.30 -0.04 0.35 Reason for Choice of Child Care: Perceived Quality -- -- -- -- Accessibility 0.81 * 0.36 0.98 * 0.39 Preference 0.56 0.33 0.65 0.33 Other 0.29 0.44 0.90 * 0.41 Would Strongly Recommend to Friend? 0.56 0.28 0.37 0.28 Multiple Arrangements 0.02 0.33 -0.13 0.33 Percent Time Spent in Primary Arrangement -1.07 1.44 -0.79 1.30 Missed Work Due to Provider-Related Problems 0.66 0.51 0.00 0.45 Sick Care Child Sick and Used Regular Arrangement -- -- -- -- Child Sick and Mom took Care 0.44 0.37 0.17 0.39 Child Sick and Other Arrangements Used 0.58 0.55 0.17 0.57 Child not Sick 0.27 0.31 0.35 0.31 Mom is Employed -0.58 0.47 -0.54 0.53 Maternal Income ($1000) 0.00 0.01 0.00 0.01 Occupation is Professional, Administrative, Executive, Managerial 0.34 0.34 0.58 0.44 Work Hours 0.02 * 0.01 0.02 0.01 Shift Exclusive Day Shift -- -- -- -- Varying Shift 0.20 0.46 0.54 0.52 Other Shift (Some Weeknight/Weekend) -0.16 0.34 -0.36 0.37 Work Flexibility Flexible Work -- -- -- -- Inflexible Work -0.50 0.37 -0.01 0.38 Somewhat Flexible Work -0.40 0.36 -0.06 0.35 Employment/School Role Salience -0.06 0.13 -- Perceptions of Ideal Work/Family Situation Ideal Type-Stay Home Full Time -- -- -- -- Ideal Type-Work or School Full Time 0.24 0.52 -- -- Ideal Type-Work or School Part Time 0.12 0.34 -- -- Attitude Toward Maternal Employment 0.02 0.02 -- -- Career Central to Self-Esteem 0.35 ** 0.10 -- -- Feelings about Parenting 0.09 ** 0.02 -- -- Children and Their Parents (Parental Locus of Control) 0.03 0.02 -- -- When Away From Child, Wonder if Physical Needs are Being Met 0.17 0.12 -- -- Mom's Income Before the Birth ($1000) -0.01 * 0.01 -- -- Job Offered Leave Benefit with Pay 0.06 0.35 -- -- Job Offered Leave Benefit with No Pay -0.61 * 0.30 -- -- Spouse or Partner in Household -1.39 ** 0.50 -1.05 0.70 Number of Other Adults in Household -0.05 0.28 0.01 0.29 Perceived Emotional Support -0.47 ** 0.05 -0.31 ** 0.05 Perceived Instrumental Support -0.15 0.08 -0.23 ** 0.07 Paternal Income ($1000) 0.00 0.00 -0.01 0.01 Other Income ($1000) 0.00 0.00 -0.01 * 0.00 Public Assistance 1.36 ** 0.44 0.12 0.50 Job Loss in Family 0.79 ** 0.28 0.14 0.27 Illness in family 0.79 ** 0.23 0.58 ** 0.22 Death In Family 0.78 ** 0.25 0.27 0.24 Big Difference in Family 1.38 ** 0.24 0.85 ** 0.22 Poor Health - Baby 0.11 0.33 -0.09 0.34 Poor Health - Mom 2.66 ** 0.38 1.13 0.39 Poor Health - Partner 0.98 * 0.44 -0.46 0.40 Number of Preschool Age Children in Household 0.45 0.28 0.43 0.25 Number of School Age Children in Household -0.01 0.30 -0.03 0.37 Mother's Age When Child Born -0.05 0.03 -- -- Mother's Education When Child Born -0.32 ** 0.08 -- -- Mother's Race White -- -- -- -- Black 0.28 0.56 -- -- Other 0.37 0.69 -- --
Appendix 3Regression Models Predicting Maternal Depression by Child Care Characteristics, Maternal Employment Characteristics, and Covariates
No Fixed Effects/Extended Measured
Controls
Fixed Effects/Extended Measured
Controls
b se b se
Appendix 3Regression Models Predicting Maternal Depression by Child Care Characteristics, Maternal Employment Characteristics, and Covariates
No Fixed Effects/Extended Measured
Controls
Fixed Effects/Extended Measured
Controls
Baby is Female 0.21 0.28 -- -- Days Mom Stayed in Hospital After Birth 0.21 0.13 -- -- Marital Quality Scale -0.52 * 0.24 -- -- Child Temperament Scale 0.55 * 0.25 -- -- Child with Difficult Temperament -1.54 * 0.65 -- -- Site Dummies Site0 -- -- -- -- Site 1 0.25 0.61 -- -- Site 2 0.28 0.67 -- -- Site 3 0.18 0.65 -- -- Site 4 0.79 0.67 -- -- Site 5 -0.20 0.64 -- -- Site 6 -0.52 0.63 -- -- Site 7 1.02 0.64 -- -- Site 8 0.18 0.65 -- -- Site 9 -0.14 0.64 -- -- Wave Dummies 6 Months -- -- -- -- 15 Months -0.08 0.24 -0.03 0.24 24 Months -0.13 0.27 0.09 0.27 36 Months -0.52 0.28 -0.17 0.28 Number of Variables Imputed 0.20 * 0.08 0.14 0.08
-- Omitted Category or Excluded from Model** p < .01. * p < .05.n = 4,766 observations from 1,302 mothers

b se b se Maternal Employment and Child Care Not Employed/No Child Care 0.88 * 0.43 1.05 * 0.46 Not Employed/Not Chosen for Quality 0.17 0.58 0.36 0.59 Not Employed/Chosen for Quality -0.19 0.53 -0.87 0.60 Employed/No Child Care 0.63 0.41 0.52 0.47 Employed/Not Chosen for Quality 0.39 0.27 0.60 * 0.27 Employed/Chosen for Quality -- -- -- -- Employment/School Role Salience -0.04 0.13 -- -- Perceptions of Ideal Work/Family Situation Ideal Type-Stay Home Full Time -- -- -- -- Ideal Type-Work or School Full Time 0.33 0.52 -- -- Ideal Type-Work or School Part Time 0.12 0.34 -- -- Attitude Toward Maternal Employment 0.02 0.02 -- -- Career Central to Self-Esteem 0.36 ** 0.10 -- -- Feelings about Parenting 0.09 ** 0.02 -- -- Children and Their Parents (Parental Locus of Control) 0.03 0.02 -- -- When Away From Child, Wonder if Physical Needs are Being Met 0.16 0.12 -- -- Mom's Income Before the Birth ($1000) -0.01 0.01 -- -- Job Offered Leave Benefit with Pay 0.07 0.34 -- -- Job Offered Leave Benefit with No Pay -0.60 * 0.30 -- -- Spouse or Partner in Household -1.45 ** 0.50 -1.08 0.70 Number of Other Adults in Household 0.00 0.28 0.01 0.29 Perceived Emotional Support -0.46 ** 0.05 -0.31 ** 0.05 Perceived Instrumental Support -0.16 * 0.08 -0.24 ** 0.07 Paternal Income ($1000) 0.00 0.00 -0.01 0.01 Other Income ($1000) 0.00 0.00 -0.01 * 0.00 Public Assistance 1.24 ** 0.44 -0.01 0.51 Job Loss in Family 0.76 ** 0.28 0.12 0.27 Illness in family 0.77 ** 0.24 0.59 ** 0.22 Death In Family 0.83 ** 0.26 0.29 0.24 Big Difference in Family 1.36 ** 0.24 0.86 ** 0.22 Poor Health - Baby 0.16 0.33 -0.06 0.35 Poor Health - Mom 2.65 ** 0.39 1.10 ** 0.39 Poor Health - Partner 1.05 * 0.44 -0.52 0.40 Number of Preschool Age Children in Household 0.36 0.28 0.36 0.25 Number of School Age Children in Household -0.04 0.31 0.04 0.38 Mother's Age When Child Born -0.06 0.03 -- -- Mother's Education When Child Born -0.31 ** 0.08 -- -- Mother's Race White -- -- -- -- Black 0.27 0.56 -- -- Other 0.37 0.69 -- -- Baby is Female 0.17 0.28 -- -- Days Mom Stayed in Hospital After Birth 0.20 0.13 -- -- Marital Quality Scale -0.56 * 0.24 -- -- Child Temperament Scale 0.58 * 0.25 -- -- Child with Difficult Temperament -1.54 * 0.65 -- -- Site Dummies Site0 -- -- -- -- Site 1 0.12 0.61 -- -- Site 2 0.14 0.67 -- -- Site 3 -0.07 0.64 -- -- Site 4 0.60 0.68 -- -- Site 5 -0.36 0.63 -- -- Site 6 -0.63 0.63 -- -- Site 7 0.88 0.64 -- -- Site 8 0.11 0.65 -- -- Site 9 -0.21 0.65 -- -- Wave Dummies 6 Months -- -- -- -- 15 Months -0.10 0.22 -0.04 0.23 24 Months -0.15 0.26 0.09 0.25 36 Months -0.54 * 0.27 -0.16 0.26 Number of Variables Imputed 0.18 * 0.07 0.10 0.08
-- Omitted Category or Excluded from Model** p < .01. * p < .05.n = 4,727 observations from 1,300 mothers.
Appendix 4Regression Models Predicting Maternal Depression by Child Care and Maternal Employment Categories and Covariates
No Fixed Effects/Extended Measured
Controls
Fixed Effects/Extended Measured
Controls







