division of - national institutes of health page thirtv-two ... for being well up on issues that...
TRANSCRIPT


division ofregionalmedical
programs
A communication devicedesigned to speed ~GWINE FMm - Regional Medical Programs To&y
the exchange of news, ~d In Historical Perspective
information and data onRegional Medical Programs
September 29, 1969 - VO1.3, No. 27
k a public service the System Development Corporation
of Santa Monica, Californi~ has devoted its entire
September, 1969 issue to Regional Medical Programs, and
a copy is attached for your review.
The lead article tells the story of the development
of Regional hledical Progrms in histori~l perspective, and
also brings their current activities and problems clearly
into focus.
The remainfig two articles detail the development and
some of the on-going activities of the Tennessee Mid-South
and Mountain States Regional Medical Programs.
U:S. I}EPARI’YIEN”I OF IIEALTI1. E1>[’CATIOX, .\XI) W“ELFARK
Puhlic ~~e:ilth Seryi{,{> ● Iiealth Services and }Ierrtal IIealth A(inlinistratiorr ● IIvil,es(la. }larylarl(l 20014

SDC MAGAZINE 7“ A,,,,.,,......,SDC
Published by System DevelopmentCorporation
= **C:..,:,

September 1969Volume 12Number 8
SDCMAGAZINESYSTEM DEVELOPMENT CORPORATION2500Colorado AvenueSanta Monica, California 90406
Editor: Virginia CarabilloMonagingEditor: Russell PaquetteProduction Monager: Mary LouDossettEditorial Stafl: Harry Bain
PeggyDobruskyKaren Profet
Art Direction: Allan WalkerPhotography: Allan Walker
CONTENTSRMP:B for Home Rule in Health Care
Page ThreeTennessee/Mid-South—Contrast,Cooperation and Quality
Page ThirteenMountain States—A Case Study inGrass-Roots Planning
Page Twenty-threeOF NOTE
Page Thirtv-two
~SystemDevelopment Corporation, 196g.Permission to reprint articles in thispublication may be obtained by writingto the editor.
Published byCorporate CommunicationsManager: Donald RamsayAssistant Manager: Virginia Carabillo
Head of Corporate Publications:Russell Paquette

A IZ-year-old 4-H Club member begins a pattern oflife in rural America much like his father beforehim, while across the country in a large urban areaa Negro boy and his brother play on a run-down citystreet, They share little in common except that theyare growing up with a better chance of beating theodds on heart disease, cancer and stroke than theirparents. Part of the story is a new federal programthat asks us grown-ups to plan and then carry outour own campaigns against these killer diseases. Thisedition of SDC Magazine describes that program,
SDC MAGAZINE . 1


RMP3forHomeRule in
HealthCareby HARRY BAIN
he has come to know Quite a few of ization, But if you’re getting someRoseville’s Z0,000citizens, He sees pa-tients every day in his office on OakRidge Drive or at the Roseville Com-munity Hospital where he’s a memberof the staff. Johnson and his five part-ners in group practice are members ofa fast disappearing physician minority—the general practitioners.
This doesn’t seem to bother John-son. He takes pride in what he’s doing.There’s no trace of the defensivenessyou sometimes sense among GPs inthis age of increasing medical special-
mellow notion that he’s- a sto-rybookcountry doctor, you’re in the wrongtown. The word for Hal Johnson isMod.
He swings in a medical and scien-tific sense because he works at it. Hereads the right journals regularly—and learns from them. He makes thetime to get to two or three continuingeducation seminars every year to keepup-to-date. You’ll usually find himdraped across a chair at classes offeredby the local hospital.
SDC MAGAZINE = 3

As a member of the Roseville CityCouncil and the local school board, healso swings in the community involve-ment sense. He’s the councilman withthe crewcut gray hair who makes it toall the meetings and has a reputationfor being well up on issues that con-cern the community. Watching himhold up his end during a clash ofviews on local taxes, you’d have toconcede that for a stripling [3g) he’spolitically hip. This applies in medicalpolitics, too, where Johnson has been
a president of his county medicalsociety.
In medicine, as in city government,Johnson likes to describe himself as aprogressive conservative. He says hewelcomes change so long as it carriesalong the positive achievements ofthe past and is based on politicallyworkable and economically soundassumptions.
Like many of his colleagues in or-ganized medicine, Hal Johnson hasharbored deep suspicions about gov-
ernment medical programs, especiallythose that have emanated from thefederal level. He has been apprehen-sive that they might eventually destroythe personal doctor-patient relation-ship or undermine the private practiceof medicine. Private medicine, he isconvinced, is both a wellspring ofmedical excellence and a powerfulwitness to individual freedom.
Knowing how Hal Johnson feels onthis score makes what he has beendoing the past 15 months all the more

remarkable. Since July 1968, he hasbeen helping set up a federally spon-sored health program in Roseville. Hebelieves it will benefit his own pa-tients and those of other Rosevillephysicians. He fought to get it. It isbeing paid for under Public Law 89-239, passed in 1965 and amended lastyear by P,L. 90-574,Johnson, and thou-sands of other physicians who havehad their thinking changed by this law,call it Regional Medical Programs, orsimply, RMP.
To capture the support of doctorslike Hal Johnson, RMP has to be aspecial program, It is. It is the firstfederal health program to insist ongrass-roots leadership in the decision-making process. Regional advisorycouncils call the shots, and the law isexplicit that the councils be represent-ative of all elements of the health com-munity, including consumers. There’sa great deal more about RMP that isdifferent from past government efforts,but first let’s talk about how the lawcame into being.
CONGRESSIONALRESPONSE
Looked at historically, RMP is dollars-and-cents Congressional recognitionthat there is much more than short-ages of physicians, other health spe-cialists and hospital beds to whatPresidents Johnson and Nixon havecalled the health crisis. Shortages maygrab the most space in our news media,but leaders in the health sciences arebeginning to talk more and moreabout a breakdown in our system fordelivering health care.
This was essentially the message ofthe President’s Commission on HeartDisease, Cancer and Stroke when itsubmitted its report in December 1964.Chaired by famed Houston heart sur-geon, Dr. Michael E, De Bakey, theCommission pointed with pride to thegreat strides made in medical researchand then viewed with alarm the slow-ness with which the results of thisresearch were being made availableto patients throughout the nation.
The following summer, Congressacted to improve the delivery of medi-cal knowledge by passing the Heart,Cancer and Stroke Amendments tothe Public Health Service Act. Thiscreated Regional Medical Programs“to afford the medical profession andthe medical institutions of the nation,through ..cooperative arrangements,
the opportunity of making available totheir patients the latest advances inthe diagnosis of heart disease, cancer,stroke, and related illnesses.” Thediseases selected were appropriatetargets. As a group, they are our mostlethal killers, accounting for 71 ofevery 100 deaths in America.
The Commission study, now knownas the De Bakey Report, had called forthe establishment of “centers of ex-cellence” for the dissemination anddemonstration of new knowledge,This concept smacked of too muchcentralism for the medical professionto swallow and was finally scrappedby Congress in favor of “cooperativearrangements” among medical schools,hospitals, medical associations and re-lated elements of the health care sys-tem, Such cooperative arrangementsare one of the most unusual RMPfeatures.
Congress went even further towardallaying the fears of many physicianswhen it declared that RMP was toaccomplish its ends “without interfer-ing with the patterns, or the methodsof financing, of patient care or profes-sional practice, or with the adminis-tration of hospitals... .“ This guarantee,along with the local autonomy dele-gated to individual regional advisorycouncils, in large measure explainswhy practicing physicians like HalJohnson have greeted RMP so warmly.
DOWN TO THEGRASS ROOTS
Physicians have been joined in theirenthusiasm by nurses, hospital admin-istrators, medical educators and repre-sentatives of voluntary health organi-zations, to name the most prominentprofessionals whose membership isrequired, along with that of physicians,on the advisory councils. Congressalso made it clear that it expected tosee some average citizens among thecouncil members.
SDC MAGAZ1h,E I 5

In drafting P.L, 89-239, the legisla-tors recognized two distinct but re-lated phases in getting RMP into busi-ness—planning and operation, In’ thefirst, the regional advisory councildraws on all the resources in its areato identify what is needed to dealwith the problems related to heartdisease, cancer and stroke as theyexist in its own region.
Once needs are known, the counciltnust get down to the task of settingpriorities among competing needs andhammering out the cooperative arrange-ments required to develop remedialmeasures. This effort is suDDorted bvplanning funds granted unde’r the La;after approval of the National Advi-sory Council of the Division of Re-gional Medical Programs. DRMP is thecapping agency that administers theRMP program for the Department ofHealth, Education and Welfare, Plan-ning grant approval hinges on accept-ance of the region’s organizationalplan and method for proceeding.
At this point, the region is ready toenter the operational phase, which isanother way of saying it is ready tosend in an initial grant proposal tothe Division of Regional Medical Pro-grams, As required by the Law, DRMPwon’t give out money for patient treat-ment exceDt where such funds are tobe used fo; “demonstration” purposesonly, and not to set up permanent careand treatment programs. There is alsono provision in the Law for money forconstruction.
Neither Congress nor the divisionhas laid down any hard-and-fast time-table for moving from planning tooperation. It hasn’t been unusual forthe two to proceed concurrently. Afew RMP grantees—North Carolina,Kansas and Missouri, for example—had a long history of regional coopera-tion and planning and were able tomove quickly to full operational status,Others have found it necessary tomove more slowly.
DR. ALFRED M. POPMA
The real decision on the timelinessand acceptability of operational activi-ties lies with the division as expressedby the recommendations of the Re-view Committee and the National Ad-visory Council on RMP. The latter isa body of distinguished medical prac-titioners and administrators who re-view and make recommendations onall regional proposals, again as re-quired by law.
Dr. Alfred M, Popma, a Boise, Idaho,radiologist for more than a quarter-century before turning his full timeattention to RMP, knows all the anglesin the review process. He is one of the16 members of the National AdvisoryCouncil, has served on the ReviewCommittee and keeps his local per-spective sharpened as program direc-tor of the Mountain States RMP.
“At council review sessions, we areinsisting more than ever on excel-lence,” Popma says. “The successfuloperational grant must reflect the kindof solid region-wide planning that willenhance and improve patient care in
heart disease, cancer and stroke. Thecouncil makes its recommendationsto the Surgeon General who author-izes DRMP to fund approved propos-als. So far, none of sour findings hasbeen reversed, but recently some havebeen deferred because of a lack offunds,”
Perhaps the most important factorin council deliberations is the qualityand durability of the voluntary cooper-ative arrangements. Says Paul Ward,coordinator of the California RMP,“All operational proposals are basedon voluntary cooperative arrange-ments. It’s the term we’re stuck with.What does it mean? Simply plain oldverbal agreements between givenpeople to do given things, providedthey can get the resources from oneplace or another.” Once plugged intoa grant proposal and approved, how-ever, these verbal agreements take onall the legal force of a formal contract.
In form, then, RMP goes well be-yond encouraging local participation.It demands it. Moreover, the tactic oflocal control has been strengthenedthrough the philosophies of Drs.Robert Q. Marston and Stanley W.Olson, the two physicians who haveserved as directors of DRMP. (Mar-ston moved up in 1968 to becomethe first administrator of the newlycreated Health Services and MentalHealth Administration and subse-quently became director of the Na-tional Institutes of Health.) Both haveemployed the division more along thelines of a flexible staff resource thanas a heavy-handed federal directorand enforcer. In keeping with this atti-tude, the Guidelines put out by DRMPrun but 32 pages.
Refuting the notion held by somethat RMP is the beginning of a na-tional blueprint for dictating stand-ards of medical care, Dr. Olson hassaid, “Even if we knew enough todraw such blueprints—which we donot—this method of procedure is so
6 * SDC MAGAZINE

., .. . .. . ..
DR. MARC J. MUSSER
foreign to the American tradition thatit would fail if for no other reasonthan lack of acceptance.
“What in fact is intended is thatplanning shall be accomplished com-munity by community, neighborhoodby neighborhood, hospital by hospital,and doctor by doctor, not for the con-sumer but with him. . . . RegionalMedical Programs, though federallysupported, are intended to strengthenvoluntary institutions and organiza-tions of our country in their effort todevelop local resources to meet localneeds.” Olson learned this lesson onthe firing line, Before coming to Wash-ington, he was coordinator of theTennessee/Mid-South RMP,
A LEARNING PROCESS
The idea that local communitiesshould guide their own destinies hascaught hold in a number of recentlyenacted federal programs. Says IrvingLewis, deputy director of the HealthServices and Mental Health Adminis-
tration, within which DRMP now oper-ates, “We have tried to move moreand more decision making out into thefield, recognizing that coordination offederal action cannot be accomplishedin Washington alone. . . .Moving thepoint of decision to the community,we find there is no one best way ofdoing things.”
Lewis must have been listening inat some of the meetings in the 55 RMPregions funded since passage of P.L.89-239, Observers have been struckby the innovation and differentiationof approach that have distinguishedthe groups as they moved to solvetheir own health problems. Original-ity in this case is no accident. It is asintegral a part of the RMP fabric aslocal initiative.
Listen once more to Dr. Olson: “ARegional Medical Program requires awholeness that cannot be achieved byan aggregation of loosely related proj-ects. It fosters innovation and change.Change is constantly taking place, andwe can no longer accept at any stage
in our development the beliet that wehave arrived.”
Physicians, hospitals, nurses, lay-men and the rest have found it any-thing but simple to live tip to this kindof demand. To begin with, they aren’tused to sitting down together to re-solve their differences and plan a med-ical future for an entire geographicregion.
In this vein, RMP signals a new de-parture in the way decisions are madein medicine and the health sciences,Dr. Marc J. Musser, executive coordi-nator of the North Carolina RMP, says,“For the first time in the history of ourcountry, the health professionals andhealth interests are joining togetherto make our health care system morecohesive and effective, not by legisla-tion or with large sums of money, butby involvement of the right people,communications, good judgment anda challenge to local initiative. ”
California’s Paul Ward goes evenfurther: “This is a new role for themajority of our institutions and onethat is not fully understood or ac-cepted. Involving outside communityforces in planning is difficult enoughlet alone entering into operationalprojects that give responsibility tothose outside the institution.”
Adjusting prerogatives, adjudicatinglocal differences and coming up withprojects that embody both medicalexcellence and regional benefit havecaused the planning process to movedeliberately in most of the regions.Consequently, there has been someimpatience both within the programsand in Congress. The latter, alwaysstrongly in support of RMP, has haddifficulty understanding why the re-gions as a whole haven’t spent all themoney that has been appropriated.
RMP has had carry-overs of $22 mil-lion from Fiscal Year 1966,$38 millionfrom FY 1967, $36 million from FY1968 and $2o million from FY 1969.From 1966 to 1968, the fact was that
SDC MAGAZINE ■ 7

there was an insistence on qualityand compliance with the Law, an in-sistence that left some funds unobli-gated as indicated by the carry-avers.However, the most recent carry-overof $20 million from 1969 to 1970 wasan administrative decision of HEWand not the result of a shortage ofworthwhile projects, The fact remainsthat at the end of FY 1969 [June 30)there were some $25 million worth of‘approved but unfunded projects,
In a March 1968 appearance beforethe House Subcommittee on PublicHealth and Welfare, Dr. Michael DeBakey anticipated, this development.“There have been times when I havebeen guilty of impatience,” he ad-mitted, “but the fact is that this pro-gram has developed, I think, at a nor-mal pace and in a very sound way.”
He pointed out that the planningphase of RMP had stressed the design,not the implementation, of health pro-grams. This resulted in smaller ex-penditures than were projected in thebeginning, but De Bakey emphasizedthat regional planning efforts wereabout to pay off in more expensiveoperational programs that would re-quire close to $3OOmillion by lg71.He further suggested that Congress“contemplate authorization levels ofsome $5OOmillion” by lg73 to main-tain standards and momentum in theprogram.
AN EMERGING PATTERN
Through Fiscal Year 1969, the 55 re-gions had received some $145 millionin both planning and operationalgrants. In part, this paid the freightfor the nearly 2500 paid staff mem-bers (47 percent physicians) in theprograms, It did not reflect the enor-mous volunteer efforts of the nearlylo,oooprivate individuals, professionaland lay, who man the regional andnational advisory councils and serveon various subcommittees, task forcesand local action groups.
Active RMPs now blanket the Con-tinental United States and reach be-yond to take in Alaska, Puerto Ricoand Hawaii, the latter grant includingGuam, American Samoa and Micro-nesia. In land area, the regions rangefrom Washington-Alaska to Washing-ton, D.C. California leads in popula-tion with nearly 20 million; NorthernNew England, headquartered in Ver-mont, has but 425,000. All Americansnow live within at least one RMP area.Because of regional overlapping, somelive in as many as three.
Some states, like New York withfive and Ohio with four, have set upmultiple regions within their bounda-ries, The opposite has happened inthe wide open spaces of the Westwhere the Western Interstate Commis-sion for Higher Education administersa program that takes in four statesand overlaps portions of four othersthat have their own RMP activities.California, in turn, is a single regionbut has organized itself into “areas”defined by the medical service areasof the state’s eight medical schools.
Of the 55 organizations that havefiscal responsibility for the programs,25 are medical colleges or universitymedical centers. Seven others are uni-versities, while the remaining grantsare split among 17 specially charteredfoundations, commissions and associ-ations, four state medical societies,one advisory council and one stateagency.
Medical school involvement in RMPis written into the Act, since the medi-cal colleges are at once a prime locusof new knowledge through researchand because of their tradition as avehicle for disseminating such knowl-edge through established extensionteaching activities in their own medi-cal service areas. From the outsetCongress intended that RMP haveheavy educational emphasis, and it issomething of an understatement tosay that the most popular and wellsupported thrust of RMP among doc-
tors and allied health personnel hasbeen in the direction of continuingeducation courses.
In fact, Dr. Dwight Wilbur, immedi-ate past president .of the AmericanMedical Association and a staunchRMP supporter, has said: “These [RMP]programs should be primarily educa-tional, for the better educated physi-cians are, the higher the quality ofmedical care they can render.... Facili-ties and financing are important, butof prime importance is the widespreadavailability of high quality medicalcare. The key to this is more andbetter education of practicing physi-cians.” Small wonder the regionsmaintain close relations with medicalcolleges in their jurisdictions, or thatoperational grants to date have beennotable for their innovative ap-proaches to providing educational pr~-grams across a wide range of medicaland health specialties.
Few, if any, would disagree alto-gether with Dr. Wilbur’s support ofcontinuing education, but there aremany who question that such pro-grams should be the dominant themein RMP. Dr. H, Jack Geiger speaks formany of these when he argues thatRMP should devote much greater at-tention to the total health problemsof the urban and rural poor.
Now acting chairman of the depart-ment of preventive medicine at TuftsUniversity School of Medicine, Dr.Geiger holds that the categorical RMPemphasis on heart disease, cancer andstroke is too narrow and should bebroadened to include not only alldisease problems that confront thepoor, but also such pressing extra-medical issues as poverty, discrimina-tion, lack of education and unsanitaryinner city and rural housing.
Differences of opinion like thesedon’t intimidate Dr. Olson and hisstaff at DRMP. They call theirs a liv-ing program in the sense that theyexpect to see it change and grow asconditions change and new health pri-
8 I SDC MAGAZINE

orities emerge. They’ve already seenthe categorical emphasis expandedsomewhat through greater attentionto kidney, respiratory, diabetic andother diseases that fall under the “re-lated illnesses” portion of P.L. 90-574,and they fought successfully to havedentistry included within the RMPrubric. .
Moreover, they have establishedclose liaison with social action agen-cies both in HEW [Office of EconomicOpportunity) and HUD (Model Cities)and have encouraged individual re-gions to forge cooperative arrange-ments with these and other programswherever possible. (A subsequent sec-tion in this issue touches on suchinteragency cooperation in Nashville,Tennessee.)
For all this, the program has experi-enced some disappointments. One ofthe most persistent has been the slow-ness with which RMP has moved insome of our largest and most problemridden urban areas. This has been ac-centuated by the speed and successrealized in rural and alpine regions.Much of the problem traces to hang-ups in getting RMP organized in thecore cities where, among other prob-lems, there is a plethora of healthinstitutions, people and activities, allof which are essentially autonomous.
The division has made no effort tosoft-pedal these difficulties in its testi-mony before Congress or in its publicstatements. Olson has said: “The com-plex problems of our cities pose anational crisis of the gravest order.,..We recognize that the complexitiesinvolved in developing regionalizationin urban areas have delayed the de-velopment of regions in the very areaswhere their services may be mostneeded. This is a matter to which Ihave already given a great deal of mytime and to which I am prepared todevote more of my personal efforts.”
Dr. Olson’s “complexities” are thesame bugaboos that plague most pub-lic programs in the cities—inadequate
DR. STANLEY W. OLSON
funds, social fragmentation, the diffi-culty of bringing together all the cul-turally diverse groups that must beincluded in the planning process, im-movable bureaucracies, indifference.By and large, the rural regions havehad to deal with a far less numerousbut more homogeneous population, acircumstance that goes far toward ac-counting for their rapid progress ingetting into operational status. Com-parative operational grant historiestell the story about as well as any-thing else,
Let’s consider the Kansas RMP andthe Intermountain Program based atSalt Lake City, Utah. These regions,both largely rural, have received grantfunds totaling some $3 million and$7.3 million, respectively. Anotherfast-starting group, the Albany RMPin upstate New York, has receivedalmost $2.8 million. Together, theseregions represent about eight millionpeople.
On the other side of the coin, thelatest DRMP directory of operationalgrants lists none for Chicago, Cleve-land, New York City or Pittsburgh.The New York Metropolitan RMP
alone has more people than Albany,Kansas and Intermountain combined.While awards have been made forprojects in Los Angeles, Philadelphia,St. Louis and Baltimore, they havebeen on a far less ambitious scalethan those for some of the more thinlypopulated regions.
Not that there aren’t some encour-aging urban programs. Watts-Willow-brook, a project to develop a post-graduate medical center to serve thepeople of Central Los Angeles, iswidely regarded as a possible proto-type of future community health cen-ters in ghetto areas. The Tennessee/Mid-South RMP, combining the activi-ties of predominantly black MeharryMedical School with those of tradi-tionally white Vanderbilt UniversityMedical School, is embarked on a pre-ventive medicine program that linksmultiphasic screening and an OEO-sponsored Neighborhood Health Cen-ter in a deteriorating section of NorthNashville. Similar programs are onthe drawing boards in such regions asIllinois, New Jersey, Detroit, Washing-ton and New York City.
A GLIMPSE AT~AT’S GOING ON
The working draft of a directory pre-pared by DRMP at the end of FiscalYear 1969 required nearIy 240 pagesto furnish biographical data on the 55regions and capsule descriptions ofthe projects in the 41 regions that hadachieved operational status. Most ofthe space was devoted to the lattertask.
Predictably, the individual projectsdiffer as markedly in design as the re-gions themselves differ in topography,demography, and health manpowerand facilities. Just as predictably, thereare pronounced similarities, for gapsin the armamentarium for attackingheart disease, cancer and stroke havesome characteristics that transcend re-gional boundaries.
SDC MAGAZINE * 9

For example, the best equipped andtrained personnel are found in themajor hospitals and university medi-cal centers, whether these are in ruralor urban regions. Logically, then, theseinstitutions find themselves involvedin some way in nearly all educational,training or demonstration projectsthat have won approv~l for opera-tional funding,
Commonly, RMP strategy has beentwo-fold—to build on existingstrengths wherever there is a stronglocal program and to extend knowl-edge outward from the medical centersto the smaller community hospitalswhere specialist~ and sophisticatedequipment are often nonexistent. No-where is this strategy better illustratedthan in the emphasis on coronary careprograms, an emphasis that threadsits way through RMP activities fromHawaii to Florida, from sparselypeopled Idaho to crowded New Jersey.
In the Memphis region, the Univer-sity of Tennessee Medical Centerplans to install a lz-bed “showcase”coronary care unit (CCU) that themedical staff will use to give trainingand demonstrations to health profes-sionals from throughout the area. TheMetropolitan Washington, D.C., RMPis literally putting its coronary careprogram on wheels by designing amobile CCU that will rotate amongthree hospitals in the area. The hos-pitals will provide their own nurses,who will be specially trained, and phy-sicians will be drawn from the HeartDisease Control Program of HEW.
Joint action by the Central OhioHeart Association and the Ohio StateUniversity College of Medicine char-acterizes coronary care training in theOhio State RMP, a 61-county regionin the central and southern portionsof the state, Nurses from hospitals in10 core cities come to Columbus fortwo weeks’ intensive training thatprepares them to return to their owninstitutions as “nurse educators. ” Phy-
sicians, in turn, are eligible for coro-nary care seminars right in their ownlocal hospitals,
These projects give some idea ofthe style, if not the scope, of RMPcoronary care activities. There are stillother innovations, Some of the regionshave installed 24-hour telephone hook-ups that allow small hospitals to dialregional medical centers directly forelectrocardiogram analysis and profes-sional consultation. Another twist hasbeen the development of coronarycare training programs in hospitalsother than teaching hospitals, an ap-proach that is especially relevant tothose medical personnel who livegreat distances from the large traininginstitutions. Whatever the approach,the separate regional efforts share acommon bond of helping the practic-ing physician, the nurse and others toimprove their skills in behalf of cor-onary patients.
To Marc Musser, it is this recogni-tion of the needs of patients, as muchas the recognition of the educationalneeds of health professionals, thataccounts for the RMP emphasis oncoronary care units. He says, “Coro-nary care units represent increasedawareness of the acute problems ofpatients. RMP picked up the CCUprogram at the right time, since itcombined our initial emphasis on con-tinuing education and the means toeffectively meet needs in patient care. ”
What holds for coronary care is noless true of programs in cancer andstroke. Most of the regions havemoved solidly into these areas withtumor registries, tumor boards, strokemanagement programs, and cancerand stroke screening projects. With-out exception, the regional plans dem-onstrate conscious attempts to mounta balanced attack against all thediseases identified in the legislation.(The final segment of this issue in-cludes discussion of a cancer programbeing developed in Boise, Idaho.)
TOWARD THE FUTURE
Of the many issues that will face RMPin the lg70s, none is likely to remainmore visible than the health needs ofthe urban poor. Dr. Olson believes,“Regional Medical Programs canassist in the improvement of healthservice activities through projects thatsupplement elements of both old andnew systems aimed specifically at theurban poor,
“True, we suffer from several con-straints as we attempt to deal withthese problems. Facilities are needed,but we have no authority to use fundsfor construction of facilities. Neithermay grant funds be used to pay forthe cost of medical services or hos-pitalization, Nevertheless, there aremajor contributions which RegionalMedical Programs can make....
“Regional Medical Programs arefunctioning organizations specificallydesigned to link the providers of caretogether for the purpose of collectivelyimproving services to patients,.. .Todo this, RMP must enter into coopera-tive arrangements with the many localand federal programs already address-ing themselves to health problems ofthe urban poor.
“The [RMP] programs can andshould contribute significantly in plan-ning general health services for thesepopulations, because it is only in thisfashion that we can come to gripsspecifically with the problems of heartdisease, cancer and stroke.” Clearly,the DRMP staff doesn’t intend tododge its responsibilities in the cities.
Nor, if Dr. Olson is to be believed,will RMP diminish its emphasis oncontinuing education. He is on recordas being convinced that continuingeducation is one of the most signifi-cant single components of RMP activ-ity. In years to come, however, thedivision expects to promote more com-prehensive and innovative approaches
10 ■ SDC MAGAZINE

designed to make health professionalsactive participants rather than.passivereceptacles in the educational process.
In Olson’s view there is no conflictbetween the requirement for continu-ing education and the need to do some-thing in the cities. In fact, he believesthat RMP is flexible enough to accom-modate the problems of the rural pooras well, Education and social actioncan coexist comfortably in Olson’sphilosophy, because he regards themas essential to each other.
He sees continuing education inurban areas as one sure way to achievebetter care and treat~ent for disad-vantaged patients, In the same vein,he believes that cooperative healtharrangements worked out by agenciesin the cities can be copied elsewhereto benefit the rural poor, This outlookagain reflects the importance DRMPattaches to balanced programs.
This emphasis is certain to groweven stronger throughout the 55 re-gions in coming years. The division—through its own staff, the NationalAdvisory Council, outside consultantsand the Review Committee—has tra-ditionally insisted on excellence inthe operational proposals that comebefore it for review.
In recent months, Dr. Olson hasstrengthened this policy and called onthe regions to work harder than everto improve the quality and regionalsignificance of their requests, Perhapsthe most effective means toward thisend will be the encouragement ofmore rigorous standards of reviewand criticism among the regional ad-visory councils when they evaluatetheir own operational proposals.
The quest for excellence doesn’tstop there. Today there is also moreattention than ever to the problem ofproject evaluation. All proposals mustinclude formal mechanisms for peri-odic evaluation, and the division hasinvested a great deal of effort in de-veloping sensitive tools for this task.
The object is to help the regions iden-tify weaknesses and eliminate unpro-ductive programs. It turns out to be acontinuing responsibility.
GETTING TO KNOW THEPUBLIC AND EACH OTHER
Programs like RMP recognize thattheir success is almost totally depend-ent on timely and accurate communi-cations to a wide and heterogeneousset of audiences, There’s Congress,the mass media, the general public,the medical schools, the professionalorganizations, local governments,state health agencies, voluntary asso-ciations, and on and on and on.
At another but equally importantlevel, there is the requirement foropen communications between thedivision and the regions and amongthe regions themselves. Under DRMPAssistant Director, Edward M. Fried-lander, the division has worked out aprogram to produce maximum recip-
rocal feedback. Within the separateregions, most core staffs now includea professional public informationofficer.
It’s important that he.do a good job,for as Marc Musser has said: “Mostof the problems in RMP result fromfailure to communicate at the righttime. Leave someone out and thingscan get sticky, You might think thatbusy doctors could care less, but thathas been far from the rule so far inRMP. Overlook them and they let youknow about it in a hurry.
“Frankly, getting the commitmentof local people is only the beginning,Communications exchange must bereciprocal. It must be continuous. Alesson all of us around the countryhave learned is that good communica-tions in a region don’t just happen.You must do a lot of work to makethem happen, A good core staff isessential.”
This basic lesson hasn’t been loston Ed Friedlander and his group atthe division. Early in the game theyset in motion a systematic program ofinterregional meetings designed todraw together RMP staffs from thesame geographical parts of the coun-try, Such gatherings serve several pur-poses. They allow for briefings onwhat is going on at the federal level inregard to budget and legislative policy.They also serve as a platform for inter-preting divisional guidelines and giv-ing the regions a chance to air theirgripes about what the division is doing.That way everybody has a chance tolearn some of the basic facts together.
If the meetings accomplished nomore than this, chances are both Dr.Olson and Friedlander would considerthem worthwhile. There’s anotherangle, however, that may prove evenmore useful to the regions in the longrun. Friedlander and his people areusing their get-togethers with the re-gions to encourage permanent chan-nels by which the regions can com-
SDC MAGAZINE 8 11
,
municate regularly with each other,separately and as groups.
DRMP is convinced—as are manyof the regions—that there is a many-fold pay-off in this kind of activity.For one thing, a frank exchange ofdata on operational program successesand failures can help the respectiveregions avoid expensive false starts.For another, it can provide late-start-ing regions with helpful tips on howto secure the enthusiasm of their ownpeople and how to initiate the plan-ning process, Of increasing importance,it can also help iron out jurisdictionalproblems or stimulate cooperative ar-rangements among regions whose pro-grams overlap each other.
At a February 1969 meeting inTampa, Florida, the coordinators andother staff of the 15 regions that makeup the Southeastern Region furnishedproof that interregional cooperationand exchange are gaining in apprecia-tion. Spurred by Marc Musser and Dr.J. Gordon Barrow who directs theGeorgia RMP, the Southeastern groupvoted to share the cost of an inter-regional coordinator whose taskwould be to “ride circuit” among theregions and keep everyone apprisedof what his neighbors are doing. Thenew man has already been on the jobfor several months,
BUDGET OUTLOOK
The fact that the regions are nowready to look beyond their own imme-diate interests is an indication thatthe four-year-old RMP is coming ofage. Further proof—if any is reallyneeded—lies in the rate at which pro-grams are moving out of planning intooperational status. It is at this pointthat RMP requires much higher levelsof financial support. The program isalready feeling a pinch.
Says Dr. Olson: “Clearly, we are
moving from a circumstance wherethere has been a surplus of funds—attimes an embarrassing surplus—toone in which the reverse will be thecase. Looking at applications alreadyin hand, we can predict that the aggre-gate demand for grant funds will ex-ceed our appropriations in the FiscalYear lg70, Beyond that, the amountsthat the Review Committee and theNational Advisory Council will likelyrecommend for approval from yet-to-be-received applications will also ex-ceed available funds. ”
Because RMP didn’t spend all themoney Congress made available to itin the first four years, some of thelawmakers have been dubious aboutwhether program requests do in factrepresent a reasonable estimate ofneed. Although final Congressionalappropriations for RMP grants are yetto be voted, this dubiousness, com-bined with Administrative and Con-gressional belt-tightening, resulted ina House Appropriations Committeerecommendation of $5o million ingrants for FY 1970. This is $24 millionless than the Administration askedfor and $7o million below what wasauthorized by legislation,
Many in RMP regard this as a bodyblow to the future health of the pro-gram. Both Marc Musser and PaulWard serve on the Coordinators’ Steer-ing Committee, a group of 10 coordi-nators elected by their fellows to ad-vise DRMP on national policy andprograms. Ward and Musser thinkpresent funding projections are farfrom adequate,
Musser calls the budget outlookunpromising. He warns that someprograms may have to cut back andthat the fiscal situation will almostcertainly discourage new starts. “Onthe whole,” he says, “this is occurringwith the worst possible timing, sinceso many new localities and communi-
ties are clamoring to get into RMP.”Speaking to the same point, Califor-
nia’s Ward said, “I suppose that at thepresent time you can say that the pro-gram is at its most critical stage. Yearsof planning are coming to a head, andthe projects are rolling in. Now if youdon’t get the money in a reasonabletime, the people who made the co-operative arrangements move awayor change their minds, and you haveto try to put it all together again. Well,that’s very wasteful.
“Understand me, it’s not hard tosell Congress on RMP. They werealways willing to authorize just aboutas much as the program could use, be-cause their opinion of us was alwayshigh, The only thing Congress has hadagainst us is that in the beginning weasked for too much—more than wecould realistically use. That is theproblem.”
Ward feels much the same as Dr.De Bakey did when he testified lastyear before the House—that the pro-gram must continue to grow and ex-pand. Characterizing RMP as a meansfor distributing medical knowledge,Ward draws an analogy from thebusiness world: “You know, GeneralMotors would never think of develop-ing a new automobile and then notspend some of their resources on cam-paigns to get it in the hands of cus-tomers. The same is true today inmedicine, You might just as well for-get the research unless you are willingto devote some money to distribution.
“That’s what RMP is all about, andif we are talking $100 million as aplateau for all time, we are engaged inthe wrong kind of planning. You’vegot to preserve your momentum andthe faith that people have manifestedin the future of the program. Other-wise the voluntary contributions andlocal participation will largely be lost.That is what would really hurt.”
12 = SDC MAGAZINE

TENNESSEE/MID-SContrast,Cooperationand Quality
About 120 miles east of Memphis the Tennessee River wheels north and rolls past wayne, Perry, Humphrey,Houston and Stewart Counties. The Tennessee/ Mid-south RMp begins along the river’s east bank andstretches some 400 miles farther east to the Virginia line. It takes in 74 counties in Tennesseeand a clusterof 14 more in southwestern Kentucky.
That’s room enough for a lot of contrast. The 3600 residents of rural Van Buren County follow a life-style that has its roots in the cotton and tobacco culture of the antebellum South. Over in urban DavidsonCounty, some 400,000 Tennesseans are setting a pace that’s about as hectic as you’ll find in any othermetropolitan section of the nation. Altogether, RMP is planning or providing services for some 2.75million citizens in the region.
Tennessee/ Mid-South activities hub around Nashville, probably less famous now as the educationaland cultural “Athens of the South” than as the home of the Grand Ole Opry and a burgeoning countryand western recording industry. Nashville’s importance to RMP, however, stems from the presence ofseven large hospitals and Vanderbilt and Meharry medical schools.
Both schools are committed to the success of RMP. Vanderbilt administers the RMP grant, and facultyfrom both institutions have been generous in volunteering assistance to the program. The same goes formost of the hospita!s throughout the region and for such seats of higher learning as Fisk, George Peabody,Tennessee State and the University of Tennessee.
Tennessee/ Mid-South went into business on November 1, 1966, and began operational activities 15months later. There are now 28 active operational projects, with another four approved but not yet funded.The annual budget comes to about one dollar for every resident of the region. Much of the emphasis ison training programs that give physicians and hospital personnel a chance to improve and expand theirskills in the detection, diagnosis and treatment of heart disease, cancer and stroke. The programs havegenerally started with existing strengths and built from there–more often than not with imagination anda willingness to dare something new.
SDC MAGAZINE = 13

———....—,—.-.—
They call it North Nashville. Like other inner city neigh-borhoods in other American cities, it traces a jaggedpoverty scar through broken streets where half thedwellings are either deteriorating or dilapidated. Thirtythousand people live here. Of the adults over 25 yearsof age, only one in three has made it past the eighthgrade. Three of every five families haveannual incomesof less than $3000, and women head half the house-holds. Negroes make up 80 percent of the population.
Acrossthe country, RMPhas had trouble getting startedin places like North Nashville. But health officials herethink they have come up with an approach to assuredelivery of quality health services to Nashville’s urbanpoor. The plan revolvesaround interagencycooperationbetween RMP and a new OEO-sponsoredneighborhoodhealth center that is one of the first to be constructedin the South.
Thecenter, which beganin a run-downstore on JeffersonStreet, will soon move into brand new quarters. Super-vised by faculty and staff from Meharry Medical College,it will offer comprehensive care and treatment withemphasis on the dignity of the patient. It will also beclosely tied to another Meharry project, sponsoredthrough RMPand aimed at bettering the health lot of thedisadvantaged,not only in North Nashville, but in therest of the city as well.
Called the multiphasic screening laboratory, and cen-tered in Lyttle Hall acrossfrom Hubbard Hospitalon theMeharry campus, this operational RMPproject will offerthe latest advances in the detection of heart disease,cancer and stroke and other disorders that may lead tothose illnesses
Testing for visual acuityand visual field.
I
The clinical program will utilize 21 screening stationsto provide such servicesas electrocardiography,visuaacuity testing, spirometry, blood pressure, cervicacytologyand a battery of 27 blood tests. Hourswill befrom 1 p.m. till 9 p.m. to make it easier for those whohaveto work everyday,and the patient will spendfromone to three hours on his visit to the lab.
The screeningsequencewill be automated in an effortto conservetime for the attending physiciansand maketest results availableas soonas possible.Much of thework will be carried on by nursesand technicians,withmany of the latter trained and qualified as part of aneducationalemphasisin the program.To be eligible forscreening, patients must be referred by a private physician, a public agency or the neighborhood healthcenter. Thegoal is about 25,000 examinationsannually
14 ■ SDC MAGAZINE

Surgeon Frank A. Perryof Meharry is project di-rector of the multiphasicscreening program. H;sview: “We will be able toapply preventive meas-ures on a continuingbasis as opposed to theepisodiccare that is nowthe rule in this area. Wehave good people. We’reexcited aboutour future.”
At the blood pressuresta-tion, determinations aremade on both arms.
SDC MAGAZINE . 15

“Blood chemistry screening utilizes two machines and takes one patient sample perminute. It measures electrolytes in the blood. This procedure will also be on-line.”
16 . SDC MAGAZINE

mmm
.-! =,, \
/
“---- .~: ;%
‘-j *1
,,.
~~~ {1.F ‘ ‘~.,:so so ,; ‘e w, .,
-’~ ~ ~
:!$.”-.+~,,: .“..+ * :
t ?-:, ,,..; ;..;~-.,!. -. ,
‘This autoana/yzer givesus a blood chemistry profile based on 12 determi.nations. It is an economi.cal and swift way to letthephysicianknowwhichpatients have abnorma/value such as low bloodsugar content which isan indication of diabetictendency.”
“Our computer is an inte-gral part of the screeningprocess. We have a defi-nite plan for bringing thevarious screening serv-ices on-line. Our objectis to provide results tothe referring physicianor agency as fast aspossible. ”
Cooperativearrangementskeynotethe multiphasic screening program. Fisk University,adjacent to Meharry, is providing accommodationsfor the computer. SpecialistsfromVanderbilt’s computer center and school of engineering have assisted in planninghardware/software requirements and specifications, Clinicians from both Meharry andVanderbilt havevolunteeredtheir expert judgments on what and how manytests shouldbe included in the screeningbattery.
SDC MAGAZINE . f7
b P’
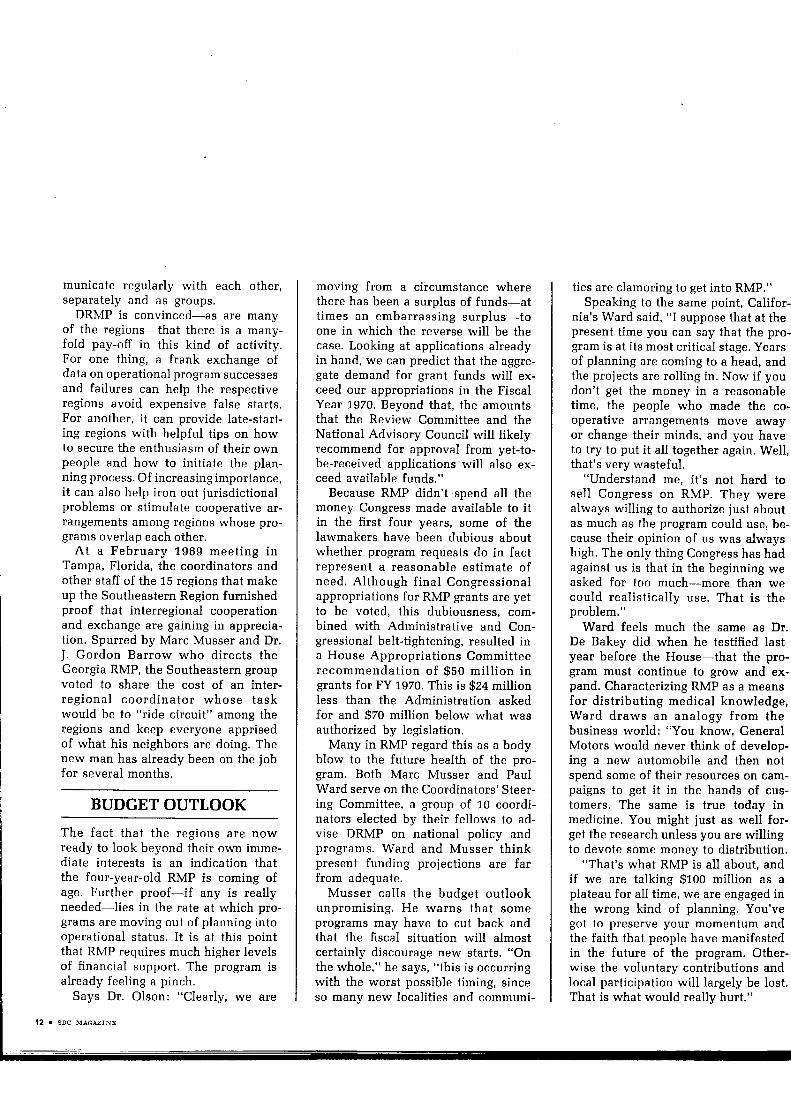
Williamson bunty Hospital is just outside Franklin, arural community of 10,000 on the L&N railroad 17 milessouth of Nashville. Last year the 100-bed hospital ad-mitted 4128 patients from its medical service area of30,000 people.About one of every 15 admissionswas acardiac patient, 22 of whom died. Physiciansand nursesat Williamson are working to lower that figure through acooperative RMP arrangement with Vanderbilt MedicalSchool’scoronary care center.
The project, under the direction of Dr. Noel Hunt ofVanderbilt and Dr. Robert Hollister of Franklin, is aneffort to find out if a small community hospital can andshould maintain a coronary care unit. Williamson hasset up a 2-bed unit and designed a 33-hour course toprepare its staff for handling the coronarypatient. it alsosent nurse Martha Miller through the rigorous coronarynursing program at Baptist Hospital in Nashville,
Through a dual monitoring system, patients at Williamson can also be monitored bythe nursing and professionalstaff at Vanderbilt. Moreover,there is a 24-hour dataphonehookupto passvital patient data betweenattending staff at the two institutionsThis arrangement allows any of the nursesor 10 physicianson the Williamson staffto have immediate accessto faculty cardiologistsand highly trained cardiac nursesat the medical school. Patients, the people for whom all this is being done, havealready benefited. Williamson administrator Cliff Gardner credits the program withsaving sevencardiac patients in its first sevenmonths of operation.
18 . SDC MAGAZINE

SDC MAGAZINE m 19
—
20 I SDC MAGAZINE

In an emergency,cardiacnurse Martha Miller ofWilliamson has nursesBonnieLandand JeanineJolly and the full re-sources of Vanderbilt’scorona ry care centerright at her fingertips.
SDC MAGAZINE * 21
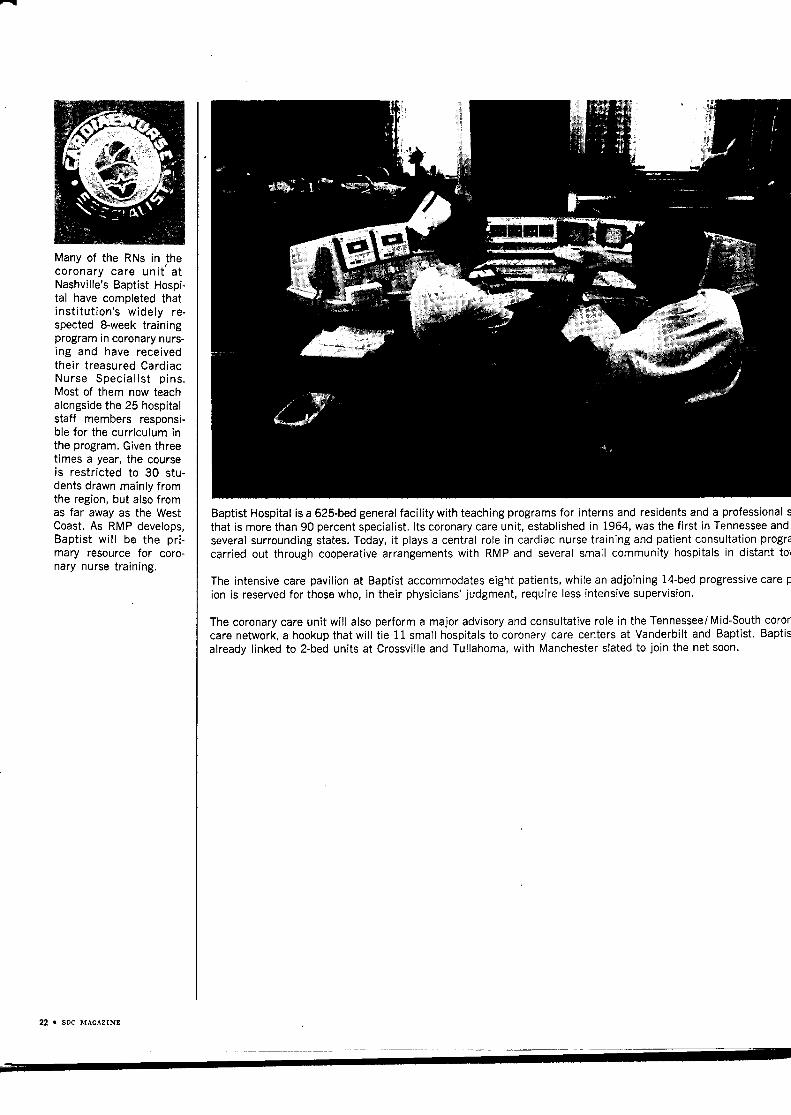
Many of the RNs in thecoronary care unit’ atNashville’sBaptist Hospi-tal have completed thatinstitution’s widely re-spected 8-week trainingprogramin coronarynurs-ing and have receivedtheir treasured CardiacNurse Specialist pins.Most of them now teachalongsidethe 25 hospitalstaff members responsi-ble for the curriculum inthe program, Giventhreetimes a year, the courseis restricted to 30 stu-dents drawn mainly fromthe region, but also fromas far away as the WestCoast, As RMP develops,Baptist will be the pri-mary resource for coro-nary nurse training.
Baptist Hospital is a 625-bedgeneralfacility with teaching programs for interns and residentsand a professionalsthat is more than 90 percent specialist. Its coronarycare unit, establishedin 1964, wasthe first in Tennesseeandseveralsurrounding states. Today, it playsa central role in cardiac nurse training and patient consultation progr?carried out through cooperative arrangements with RMP and several small community hospitals in distant to\
The intensive care pavilion at Baptist accommodateseight patients, while an adjoining 14-bedprogressivecare pion is reservedfor those who, in their physicians’judgment, require less intensivesupervision.
The coronarycare unit will also perform a major advisoryand consultative role in the Tennessee/Mid-Southcoroncare network, a hookupthat will tie 11 small hospitalsto coronary care centers at Vanderbilt and Baptist. Baptisalready linked to 2-bed units at Crossvilleand Tullahoma, with Manchesterslated to join the net soon.
22 u SDC MAGAZINE

1
MOUNTAINSTATESA Case Studyin
Grass-RootsPlanning
Al Popma and his wife, Dorothv, were born in Orange Citv, a throughout most of the western states. As a WICHE commis-little ~arming town at the nort~western tip of Iowa.-Both-ure~rom Dutch stock as are most of the people who live aroundOrange City. They came to Boise, Idaho, in 1938 when Al wasa young doctor about to begin the practice of radiology, Hekept at it until 1966 when he “retired” to take a full-time postas program director of the Mountain States RMP.
By that time Al had become one of the best known and mostrespected radiologists in his part of the country and a familiarfigure in medical circles at the state and national levels. He isa past president of the Idaho Medical Association, and whenthe American Cancer Society was reorganized in lg45, he wasone of the original board members. He later served as nationalpresident of the society.
From 1953 until 1966 he was a commissioner of the WesternInterstate Commission for Higher Education (WICHE), theorganization that administers the Mountain States RMP andis involved in the total spectrum of educational planning
sioner, Al helped draft the planning grant application thatestablished the RMP program he now directs.
He has strong convictions about RMP. “1came into this pro-gram,” he says, “because it is perhaps the first program withfederal dollars in it that has some local autonomy. For the firsttime we feel that we have an opportunity to produce projectswithout regard to state boundaries. This is truly a first in fed-eral health programs. We are also discovering that throughRMP, and again for the first time, we can develop autonomousprojects . . . that people at the grassroots can make determina-tions about their own future in health care.”
These advantages share prominence with what Popma seesas RMP’s greatest long-range contribution—the encourage-ment of permanent continuing education programs that benefitthe patient by helping physicians, nurses and other health pro-fessionals improve their skills. He discusses this and otherRMP issues in the following pages.
SDC MAGAZINE ■ ~

Al Popma has long been concerned about the lack of formalcontinuing education programs for doctors, nurses and otherhealth professionals who practice in Idaho, Montana, Nevadaand Wyoming, the four states that together compose theMountain States RMP. In his 13 years as a WICHE commis-sioner, he became convinced that one of the region’s greatestneeds was for some permanent mechanism to create and sus-tain such education and training efforts.
“WICHE undertook a ~mber of studies to assess healthtraining requirements in the four state region,” he recalls. “Anumber of years ago, for example, we made a study of healthmanpower needs and came out with very accurate predictionsof the demand for health personnel, particularly physicians,over the next couple of decades.
“And following the lead of the Faulkner Study on the needfor medical schools, in this region, WICHE set up an advisorycouncil on medical education facilities. I became chairman ofthe council, and it was largely through its work that WICHEgrew interested in the legislative hearings that led up to theestablishment of RMP. In fact, the council went to Washingtonto testify before the House committee that eventually wrotethe RMP law. ”
Popma and other council members felt at the time that agrass-roots program such as RMP would provide the spark forpermanent educational activities in the four state area. “Wewere in agreement,” Popma says, “that although we had amyriad of continuing education courses most were on a hit-and-run basis.
“Nothing was formally organized, and the professions de-pended almost entirely on volunteer agencies—the Heart As-sociation, the Cancer Society, the medical associations, thenursing societies and so on. To put it another way, the profes-sional groups themselves were entirely responsible for sustain-ing continuing education in the four states. There was little
coordination among them and quite often there was duplica-tion of course content and expenditures. ”
This was the situation as Popma remembers it in 1965 whenCongress passed P.L. 89-239 and launched RMP. From theoutset, he and other WICHE members were determined toinclude Idaho, Montana, Nevada and Wyoming in the newprogram. The first order of business was to sit down and puttogether an application for an RMP planning grant.
“This was drafted by the advisory council, working withDr. Kevin Bunnell, associate director of WICHE,” Popmarecollects. “TO assist in the effort, the council recruited threedistinguished practicing physicians from the region—Dr.Frank McPhail from Montana, Dr. Francis Barrett of Wyomingand Dr. Fred Anderson from Nevada. All were WICHEcommissioners. ”
The group got the job done, producing an application thatwas approved by the Division of Regional Medical Programs.Mountain States RMP, with Al Popma as program director,began its life in November 1966. It was—and still is—the onlyRMP region without at least one medical school, a circum-stance that some had thought would make the area ineligiblefor RMP funding.
In Popma’s view, the absence of medical schools is themajor reason there has been a lack of coordination and con-tinuity in continuing education activities in the four states.Not having medical schools also created a set of organizationalproblems for the fledgling Mountain States program.
“One of the first things we had to do to meet the require-ments of the Law,” Popma says, “was to organize a regionaladvisory group. To satisfy the requirement for medical schoolrepresentation we had to go outside our boundaries. Logically,we went to medical colleges in surrounding areas to take ad-vantage of traditional relationships to practicing physiciansin our region.
24 S SDC MAGAZINE
——

“We invited representatives from the schools in Washingtonand Oregon and chose Paul Ward to represent the severalCalifornia institutions. For representation on our southernborder, we turned to the new schools in Arizona and NewMexico. Since our physicians have always had strong ties tothe Universities of IJtah and Colorado, we added membersfrom both medical schools. Then we went a little farther awayand took in representatives from the medical college at theUnivemity of Minnesota, the medical schools in North andSouth Dakota, and from Creighton University in Omaha.”
Once medical school representation was settled, MountainStates asked for recommendations from each of its four statesto round out advisory council membership. Seventeen addi-tional people were added, including three Indian memberswho speak for the major minority group in the region. With its,advisory group selected, the program was ready to turn toother matters,
Looking back, Popma recalls that no one in the sprawling”region had accurate information on what medical facilitieswere available or what the training and educational needs ofhealth professionals were. “We recognized that we had toassess these needs,” he says, “and we decided to ask thepeople at the grass-roots level to tell us what they had to have.With this information, we could then attempt to design ade-quate programs.”
After examining several alternatives, RMP and WICHE staffmembers decided that the best approach was a field surveyusing direct mail questionnaires, “There was one problem,though,” Popma remembers, “Never having devised such ques-tionnaires or formulated computer programs for this kind ofdata analysis, we came to the conclusion very quickly that werequired some rather sophisticated assistance. And so wemade an arrangement with System Development Corporationto provide us the necessary know-how.”
Even while the agreement was in negotiation, the programwas having to face up to the task of creating a regional organ-ization that could carry out the survey work and become thepermanent staff resource for long-range planning and oper-ational activities.
c’We decided to set up an office in each state and werefortunate enough to secure four outstanding practicing phy-sicians to serve as state directors, ” Popma notes. “Althoughthere have been changes, we retain excellent state leadershipin Drs, Sidney Pratt of Great Falls, Montana, Dr. ClaudeGrizzle of Cheyenne, Wyoming, David Barton of Boise, Idaho,and Lorne Phillips of Reno and Las Vegas, Nevada. The open-ing of our regional office in Boise was the final touch to givea true regional flavor to the whole program. ”
Of course, it wasn’t quite as simple as it reads today, somethree years later. Says Popma, “Compared to other programs,we had kind of a rough time getting going. Most of the othersemanated from medical schools where there were trainedpeople to write applications and get the program rolling.
“We had to start from scratch, We had absolutely nothing.We had to rent office space here in Boise and in each of thestates, and we had to recruit qualified people. To be frank,there’s a critical shortage of manpower to do this kind of job.
John Gerdes is one of those qualifiedpeople who are in such short supply inhealth programs across the country.He was on the faculty of the Schoolof Public Health at the University ofPittsburgh but came West because hepreferre~ the clean air and outdoorlife.
Al Popma says Gerdes is “one of thetop-notch young men anywhere in thecountry when it comes to developingthe kind of community supportedhealth programs required in RMP.”Among other projects, Gerdes hasbeen prominent in planning an inhala-tion therapy training program for theregion.
“It began in the fall of 1968 at ameeting in Las Vegas where we weretrying to compile a list of physicianswho might be interested in undertak-ing such a program,” Gerdes says. “Dr.Richard Browning, a Las Vegas intern-ist, had already gotten one under wayfor the state of Nevada. and our statedirectors were anxious to find a way
26 . SDC MAGAZINE

to extend it to other parts of the region.“We already knew of another inha-.
lation therapy training program just25 miles from our regional office atCaldwell Memorial Hospital, Idaho.It was being run by Charles Reed, a31-year-old internist, as part of,a two-year program at nearby Treasure Val-ley Junior College.”
Gerdes asked Reed and Browningif they would be willing to expandtheir programs to include shorter-termtraining for personnel of hospitals inthe region. Both were receptive, andthey sat down together’ to design acurriculum and draft a grant proposalto set up complementary inhalationtherapy training institutes at Caldwelland at the Southern Nevada MemorialHospital, Las Vegas. The request ispending before DRMP.
“The exciting thing about this pro-gram, ” says Gerdes, “is that two com-munity physicians, in communities1000 miles apart, are working in con-cert on a common project with a realregional emphasis and outlook. Even-tually, if we can interest other phy-sicians like Drs, Reed and Browningin becoming instructors, we hope tomake this curriculum available to hos-pitals throughout the four states.
Gerdes points out that up to nowDr. Reed’s program has been aimed atstudents going for a junior college AAdegree or expecting to transfer to afour-year school. The Mountain Statesemphasis, predictably, will be on mak-ing the training available to hospitalpersonnel or others who have the apti-tude to become inhalation technicians.
Says Gerdes: “Typical enrollees willcome from small community hospitals,They may be RNs, but we hope also toattract students who, while they haveno special medical training, do havethe aptitude to learn the material. Ourtheory is that we can upgrade theskills not only of RNs, but also oflicensed practical nurses, nurse’saides and others with the ability anddesire to acquire this training. This isconsistent with the Mountain Statesphilosophy of training its own. ”
For patients with heart and respiratory diseases, inhalation therapy can affordshort-term relief and be a significant factor toward recovery. The inhalationtherapist also comes into play in such emergency situations as cardiac arrest orserious chest injury. The latter is simulated here by students and faculty of theCaldwell Memorial Hospital Inhalation Therapy Training Program.
SDC MAGAZINE I 27

And since we were highly geared toward field research andobtaining information,. we had to find people who thoughtalong these lines. ”
Eventually the offices did get set up and staffed, at whichpoint Mountain States was ready to sit down with SDC’SHealth and Environmental Systems Department to developthe series of questionnaires that eventually would go to nearlyall health personnel in the four states.
“Our survey universe included physicians, dentists, regis-tered nurses, licensed practical nurses, hospital administrators,X-ray and lab technologists, physical therapists,,.. I thinkthere were eight categories we wanted to reach, ” Popma says,Deciding just how to reach these groups required that theBoise staff meet regularly with state offices and representa-tives from SDC to work out questionnaire logic and wording,
“It took a lot of time and a lot of wheel spinning to come upwith the proper questions,” popma recalls. “some of ourpeople had never done this, and you can imagine that therewere problems. Often there was quibbling or quarreling overthe correctness of a single word. ”
When the rough spots were ironed out to the point thateveryone could live with the results, the questionnaires wereprinted and mailed to 100 percent of all health personnelexcept RNs and licensed practical nurses. These populationswere large enough to require use of a random samplingprocedure.
“Across the region we had better than a 50 percent return, ”Popma says with satisfaction. “The data were keypunchedand put on the SDC computer in Santa Monica. So far, wehave run two analyses on this file, and the results have helpedus in devising certain operational activities. After all, provid-ing data for operational programs was the purpose and func-tion of the questionnaires, ”
At the same time the health professional survey was inprogress, Popma’s staff was also busy collecting informationon health facilities in the region, To get an accurate line onsuch things as the number of hospital beds, the number andlocation of nursing homes, and the adequacy of transportationservices, the staff designed what it now calls its Health Profiles,
“These focus down to county levels,” Popma explains, “andenable us to tell what the health facilities needs are in indi-vidual communities, I should mention that SDC didn’t assiston this effort. We devised it almost completely on our own.Naturally there were times when SDC looked at what we weredoing and made suggestions, but the work was almost all ours.”
However, SDC did have a lot to do with a third data gather-ing effort aimed at consumers of health services. This survey
28 ~ SDC MAGAZINE
-. .....

is perhaps unique to date in RMP. “As far as I know, ” Popmasays, “ours is the only RMP’that has made a systematic broad-scale effort to find out what kind of health services the ordi-nary citizen wants to have available for patients with heartdisease, cancer, stroke and the related diseases.
“This questionnaire, which we call the Survey of Consumers,went out to 10,000 people in the four states, ” Popma recaps.“We drew our random sample from telephone directories andfrom a list maintained by fhe Department of Agriculture thatshows families without telephone service. Again, our rate ofreturn was over 50 percent, ”
All told, the Mountain States RMP now has three large filesof information—health professionals, health facilities and con-sumers, “This planning data base took almost two years toassemble,” Popma sighs, “but when it is all put together itgives us a sound basis for developing operational projects.Both the professional and consumer files are stored on thecomputer in Santa Monica. ”
Part of the agreement between Mountain States and SDCwas that there would be someone from the Health SystemsDepartment full time in Boise. Speaking of the arrangement,Popma says, “we had Bob Mendenhall who did a very excel-lent job for us. He is one of the finest people we ever workedwith. No job was too great, and there was never any questionof hours, If it took till midnight, Bob would be there to do it.
“I was very interested in Bob, Our kind of program wassomething new for him since it was the first time he had beenwith a program that fundamentally and physically was at-tached to the practice of medicine, Naturally, there was a lothe didn’t know, but he learned very well and quickly andblended in with no difficulty. Bob gave us a tremendousamount of help, and I was sorry when the contract was upand he had to leave for a job elsewhere,”
(Mendenhall is now project leader for SDC on a study toassess health care requirements for residents of the ruralUpper Kennebec Valley in the state of Maine, The corporationretains its ties with Mountain States RMP, however, througha formal consulting agreement,)
Popma is quick to point out that not all the effort in Moun-tain States has been taken up with the surveys, The programhas five operational programs under way, another approvedby DRMP and four more pending DRMP review and approval.
“We did a small study in Montana to assess the needs incoronary care,” Popma says, “and we learned that 85 percentof people having heart attacks die at home. Now Montana is arural area with many small hospitals of from 15 to 50 beds,meaning that the coronary patient can’t be transported to a
nearby large medical center with facilities to care for him. Sothese people die at home.
“We recognized that if we were going to be able to take careof such patients we had to help establish facilities and trainpeople in small hospitals, ” Popma explains. ‘Our philosophyis that if a coronary care unit is good for patients in the LosAngeles metropolitan area, it is also good for those in Shelby,Montana. If we accepted the tenet that a hospital has to have300 beds before a coronary care unit is financially feasible, wewouldn’t have any coronary care programs. ”
Believing this, Popma and his associates sat down and de-vised a prototype program to prepare both physicians andnurses to provide coronary care in the small hospital, OnMarch I, 1966, thanks in large measure to the leadership ofMontana physician, Frank McPhail, Mountain States openedits first coronary training center at St. Patrick’s Hospital,Missoula, Montana. The project draws on cooperative arrange-ments among the hospital, RMP, the University of Montanaand the University of Washington Medical School whichfurnishes consultants. About 120 people went through thecourse in its first 16 months,
“A second interesting operational program we have goingaims at providing the latest training in cancer diagnosis andtreatment,” Popma notes. “There is something for physiciansand for both the practicing and student nurse. Practicingnurses will have a chance to come to the Mountain StatesTumor Institute that we are developing in association withSt. Luke’s Hospital in Boise. Here they can study and learnthe latest techniques in cancer nursing.
“Undergraduate nurses who matriculate at the four bacca-laureate nursing schools in the region will have a chance toenter the same program on an elective basis. Since none of theschools has facilities for this kind of training, the opportunityto attend the institute should provide a new dimension inbaccalaureate nursing programs.”
Like RMP administrators in other regions, Al Popma hasgiven a lot of thought to what it takes not only to get a pro-gram started, but also to keep it moving over the long haul.“In my judgment,” he says, “the first thing that has to be doneis to sell the practicing physicians and the medical societies.You need more than their interest; you have got to have theirparticipation. This also holds true for nurses, hospital admin-istrators and other professionals. ”
Reactions to RMP have varied among physicians in the fourstate area, At the outset, there was a lot of fear and suspicionin some communities. “We tried to convince everyone thatRMP was their program and was under their control,” Popma
.
.
SDC MAGAZINE 8 Z
recalls. “We said—and we meant it—that they could take partor not take part or even drop out if they got disillusioned.”
Once physicians began to get a personal stake in the pro-gram, however, attitudes warmed considerably. “Working onthe state advisory councils, the committees, the task forcesand the surveys produced a 180-degree turnabout in many ofour physicians,” Popma says. “Feeling grew so favorable thatthe Montana State Medical Association, for example, went onrecord supporting continuing education for all health person-nel, if funded through RMP. It even set up a foundation tohelp work out cooperative arrangements and assist in healthplanning.”
Striving to maintain rapport with health professionals is atask that Mountain States shares with every other region inthe country. Another common bond is worry over where tofind enough trained people to man the respective regionalhealth care systems. Says Popma, “In my experience, the short-age of qualified people is universal. But in our area, the hos-pitals and other institutions don’t have the means to competesalary-wise with the major medical centers. That’s why ourstrategy of training our own is obvious, . . and reasonable. ”
Looking ahead, Popma doesn’t expect RMP to fade out ofthe picture any time soon. In his view there will simply be too
much community involvement at stake to let this happen. Htells a story about the Mountain States Tumor Institute :Boise to make his point.
“TO finance the Tumor Institute,” he explains, “we aldrawing on all the resources we can bring to bear, St. LukeHospital is providing the facilities—about $800,000 wor{Over the first three years, RMP has approval to provid$621,000. We’ll derive additional income from patient fe(and we expect to realize part of our operating expenses fro]philanthropic gifts.
“Take what just happened at our annual Fundsy Drive iBoise, for example. The Fundsy Drive is a community proje(in which local companies and individuals donate gifts that arauctioned off, with the proceeds going to designated charitablinstitutions. This year the Tumor Institute received $70,00for capital outlays.
“Taking all this together, I think it makes a good case studin how RMP can spark local enthusiasm and involvemerBecause of this we fully expect the institute to become pemanent and self-supporting when and if RMP money must bused elsewhere for other activities. But local support and coxmitment will remain. This is what we need. This is the geniuof the RMP approach and its most durable feature. ”
W . sDc MAGAZINE

Cancer training for nu;ses is but onefacet of the medical services MountainStates Tumor Institute is providing inthe region, Under Dr. Maurice Burk-holder, Dr. C. Ronald Koons and otherclinical specialists in the community,the institute is polishipg an ambitiousprogram to help the practicing phy-sician acquire the latest diagnosticand treatment assistance for his can-cer patients,
Koons, a young internist who wason the faculty at Johns Hopkins andstudied radiation therapy there andat the M.D. A’nderson Hospital andTumor Institute at Houston, came toBoise because he liked the challengeof developing a “first-rate” cancer pro-gram in the region.
“The purpose of the Tumor Insti-tute,” he says, “is to give this region afully staffed and equipped cancer treat-ment and education center so thatpatients and their physicians won’thave to travel the vast distances theyhave been traveling to benefit fromsuch facilities. ” It isn’t uncommon for
physicians in the four states to refercancer patients as far away as Seattle,San Francisco and Denver.
“At this institute,” Koons continues,“we’ll concentrate on outpatient treat-ment, using radiation therapy, chemo-therapy, conventional X-ray, radiumand a special unit for skin cancer [acommon medical problem in the area].We are also about to add a physicistwith experience in radiation physicsand radioisotopes. When the instituteis fully operational we expect to offerabout as much as any medium-sizedcenter in the country. ”
Physicians who staff the instituteare emphasizing an interdisciplinaryapproach. “There are no ‘stars, ’ “Koons says, “but there are a numberof qualified clinicians with sound train-ing in the various modes for treatingcancer. We will offer recommenda-tions only. The community physicianwill select the course of treatment andcontinue to care for his patient, Wewill simply provide specialized diag-nostic and treatment data. ”
I
I
.
I
At the heart of the program are theCancer Planning Conferences, heldevery Monday, Tuesday, Thursdayand Friday, at which community phy-sicians present cases to the institutestaff. Every effort is made to schedulelive patients, some of whom arebrought in from as far away as Pendle-ton, Oregon (ZOOmiles], and TwinFalls, Idaho [lZOmiles).
Initiative for the conferences re-mains with the community physicianwho decides he would like consulta-tion, a review of treatment or otherassistance from the institute staff. Thephysician contacts the institute, asksto present his patient and takes respon-sibility for sending along relevantX-rays, pathological slides, patient his-tories and records of any specialmedical treatment. If necessary, a con-ference can be arranged within threeor four days.
Says Koons: “Our aim is to encour-age the community physician to bringin any and all cancer problems, be-cause the staff is seeking the widestpossible opportunity to discuss anddemonstrate newer techniques. Inkeeping with our interdisciplinary ap-proach, we want to stress how differ-ent modes of treatment—surgery,chemotherapy, radiation therapy, forexample—can complement each otherto the ultimate benefit of the patient.
“The attending physician presentshis own patient, including pre- andpost-treatment data, and we empha-size bringing the patient in as early aspossible. The interdisciplinary ap-proach makes the institute staff bothteachers and learners. We learn fromthe community physicians and othermembers of the staff.
“Our interdisciplinary philosophyeven carries over to the design of theinstitute outpatient facilities here atSt. Luke’s Hospital. Examination andtreatment areas will be close to eachother in an attempt to maximize inter-action among the attending staff.”
SDC MAGAZINE 9

Cancer training for nurses is but onefacet of the medical services MountainStates Tumor Institute is providing inthe region. Under Dr. Maurice Burk-holder, Dr. C. Ronald Koons and otherclinical specialists in the community,the institute is polishing an ambitiousprogram to help the practicing phy-sician acquire the latest diagnosticand treatment assistance for his can-cer patients.
Koons, a young internist who wason the faculty at Johns Hopkins andstudied radiation therapy there andat the M.D. Anderson Hospital andTumor Institute at Houston, came toBoise because he liked the challengeof developing a “first-rate” cancer pro-gram in the region.
“The purpose of the Tumor Insti-tute, ” he says, “is to give this region afully staffed and equipped cancer treat-ment and education center so thatpatients and their physicians won’thave to travel the vast distances theyhave been traveling to benefit fromsuch facilities. ” It isn’t uncommon for
physicians in the four states to refercancer patients as far away as Seattle,San Francisco and Denver,
“At this institute,” Koons continues,“we’ll concentrate on outpatient treat-ment, using radiation therapy, chemo-therapy, conventional X-ray, radiumand a special unit for skin cancer [acommon medical problem in the area].We are also about to add a physicistwith experience in radiation physicsand radioisotopes. When the instituteis fully operational we expect to offerabout as much as any medium-sizedcenter in the country, ”
Physicians who staff the instituteare emphasizing an interdisciplinaryapproach. “There are no ‘stars, ’ “Koons says, “but there are a numberof qualified clinicians with sound train-ing in the various modes for treatingcancer. We will offer recommenda-tions only. The community physicianwill select the course of treatment andcontinue to care for his patient, Wewill simply provide specialized diag-nostic and treatment data, ”
DR. C. RONALD KOONS
At the heart of the program are theCancer Planning Conferences, heldevery Monday, Tuesday, Thursdayand Friday, at which community phy-sicians present cases to the institutestaff. Every effort is made to schedulelive patients, some of whom arebrought in from as far away as Pendle-ton, Oregon (ZOOmiles], and TwinFalls, Idaho [120 miles).
Initiative for the conferences re-mains with the community physicianwho decides he would like consulta-tion, a review of treatment or otherassistance from the institute staff. Thephysician contacts the institute, asksto present his patient and takes respon-sibility for sending along relevantX-rays, pathological slides, patient his-tories and records of any specialmedical treatment. If necessary, a con-ference can be arranged within threeor four days.
Says Koons: “Our aim is to encour-age the community physician to bringin any and all cancer problems, be-cause the staff is seeking the widestpossible opportunity to discuss anddemonstrate newer techniques. Inkeeping with our interdisciplinary ap-proach, we want to stress how differ-ent modes of treatment—surgery,chemotherapy, radiation therapy, forexample—can complement each otherto the ultimate benefit of the patient.
“The attending physician presentshis own patient, including pre- andpost-treatment data, and we empha-size bringing the patient in as early aspossible. The interdisciplinary ap-proach makes the institute staff bothteachers and learners. We learn fromthe community physicians and othermembers of the staff.
“Our interdisciplinary philosophyeven carries over to the design of theinstitute outpatient facilities here atSt. Luke’s Hospital. Examination andtreatment areas will be close to eachother in an attempt to maximize inter-action among the attending staff.”
SDC MAGAZINE I
