diuretics
DESCRIPTION
physiology of urine formationTRANSCRIPT

KIDNEYSOME IMPORTANT FACTS:
1. About 25% of left ventricles total output of blood in each cardiac cycle is distributed through the renal arteries to the kidneys for filtration at rest.
2. WATER IS A DIURECTIC--- x ADH (Vasopressin) release. Vasopressin regulates the body's retention of water by acting to increase water reabsorption in the collecting ducts of the kidney nephron.
3. 180L of fluid is filtered/day.
4. 99% of Glomerular filtrate is reabsorbed.
5. 1.5L of urine is excreted in normal human.
6. A 1% decrease in Glomerular filtrate reabsorption will increase the output to 3L.
7. There are 1.4 Million nephron/kidney.
8. 85% of them are SUPERFICIAL NEPHRONS; occupies 2/3rd of cortex (outer) of kidney. They are
always active. Shorter in size.
9. Rest 15% of the nephron are JUXTAMEDULLARY NEPHRONS; OCCUPIES 1/3rd of cortex and major
part to Medulla (inner). They are active only under stress condition. Longer in size.
10. Afferent arterioles (shorter in size, bigger cross sectional area) brings blood about 1200ml/min.
11. Only 20% i.e. 240ml/min enters glomerulus.
12. GFR (Glomerular Filtration Rate) is 125ml/min.
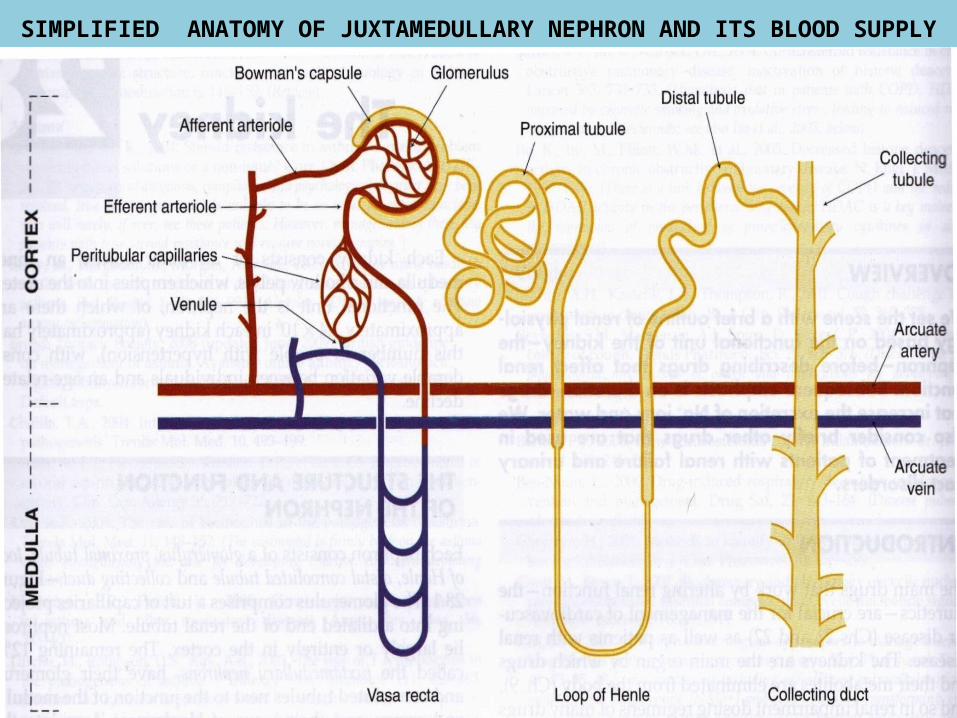
SIMPLIFIED ANATOMY OF JUXTAMEDULLARY NEPHRON AND ITS BLOOD SUPPLY

JUXTAGLOMERULAR APPARATUS
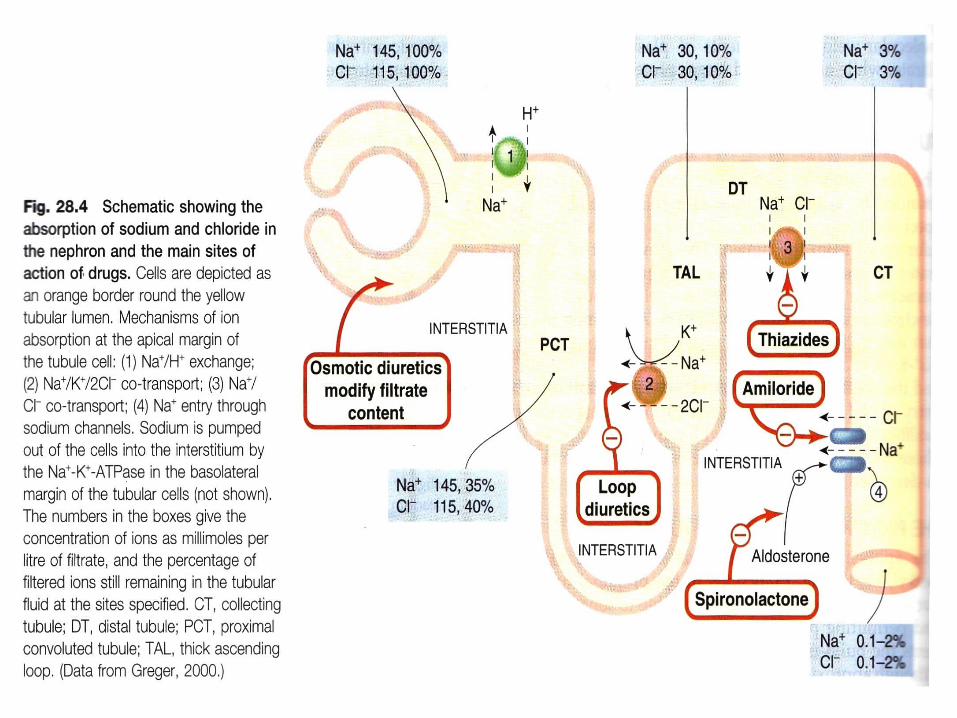
THE FOUR SITES OF SOLUTE REABSORPTION
Three cardinal processes taking place:
Glomerular Filtration- SITE-I
Selective Tubular Reabsorption SITE- I, II & III
Subsequent secretion. SITE-IV
SITE-I: Proximal convoluted tubule (PT/PCT)
SITE-II: Ascending Limb of Loop of Henle (AscLH)
SITE-III: Cortical diluting segment of Loop of Henle.
SITE-IV: Distal Tubule (DT) and Collecting Duct (DC).

SITE-I PROXIMAL TUBULE Blood supply to the nephron (from afferent to efferent arterioles) Glomerular Filtration- fluid driven from glomerulus to Bowman’s
capsule (lined by tight junction simple squamous epithelium )by hydrodynamic force opposed by oncotic pressure- permeable to LMW constituents of plasma which appear in the filtrate.
The Proximal convoluted tubule (lined by leaky junction columnar epithelium). Water and Na+ enters from capsule and diffuses passively through PT -65-70% Na+ reabsorption occurs here. The rate of entry from capsule and reabsorption from basolateral cells are so that an isotonic milieu is set.
Transport processes in PT 1. direct entry of Na+ from glomerulus to capsule-electrogenic 2. Transport of Na+ and K+ coupled with glucose, amino acids,
acetate, phosphate through specific symporter. Na+ and glucose elimination is electrogenic.
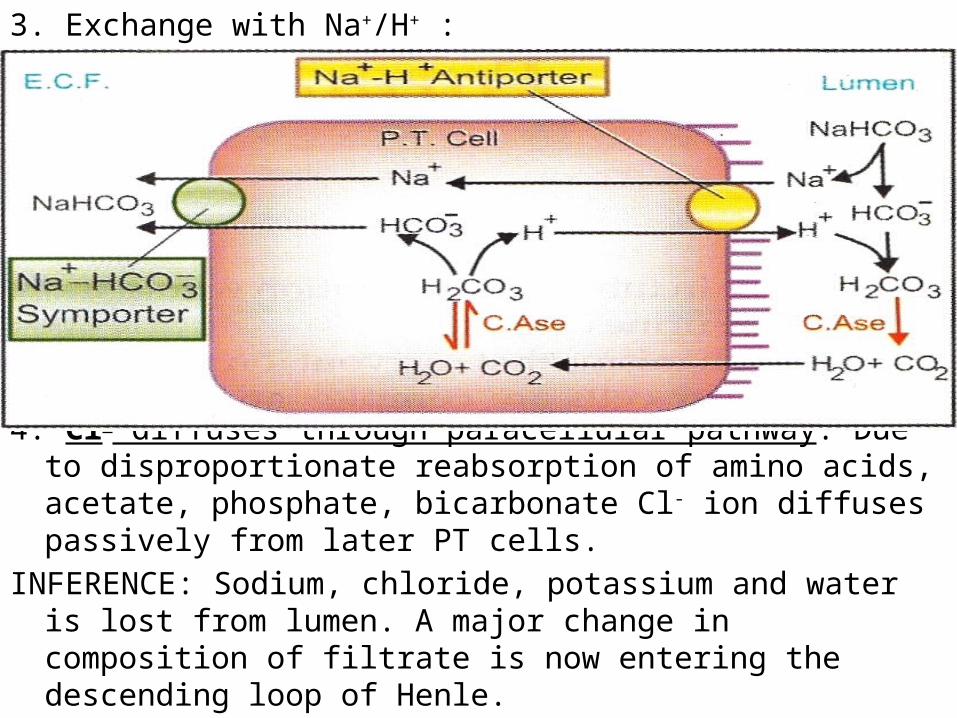
3. Exchange with Na+/H+ :
4. Cl- diffuses through paracellular pathway: Due to disproportionate reabsorption of amino acids, acetate, phosphate, bicarbonate Cl- ion diffuses passively from later PT cells.
INFERENCE: Sodium, chloride, potassium and water is lost from lumen. A major change in composition of filtrate is now entering the descending loop of Henle.
SITE-II [ASCENDING LIMB OF LOOP OF HENLE]
• Medullary part lined by cuboidal cells- Na+ - K+ -2 Cl- symporter, nonelectrogenic. In addition a Na+ - Cl- symporter moves Cl- down its electrochemical gradient into E.C.F. and carries Na+ along. As the tubular fluid traverses AscLH it progressively becomes hypotonic as this part is impermeable to water. Accumulation of NaCl in the medullary interstitium without water makes it hypertonic; a corticomedullary osmotic gradient is set up. This draws in water from descending limb of LH so that the fluid that enters AscLH becomes hypertonic.
• Cortical part lined by flattened cells.
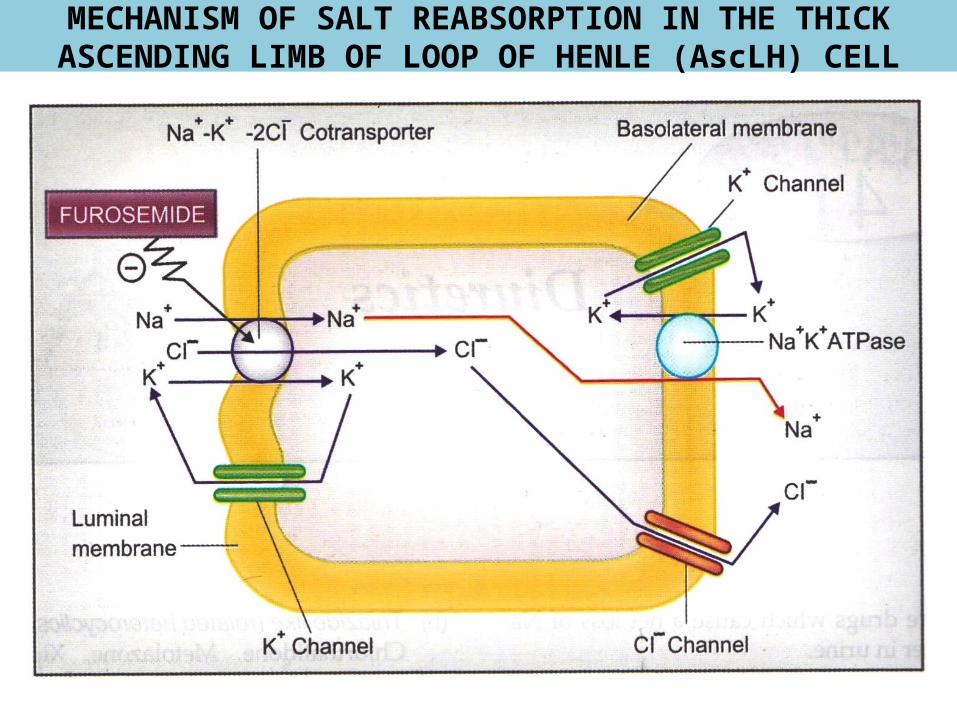
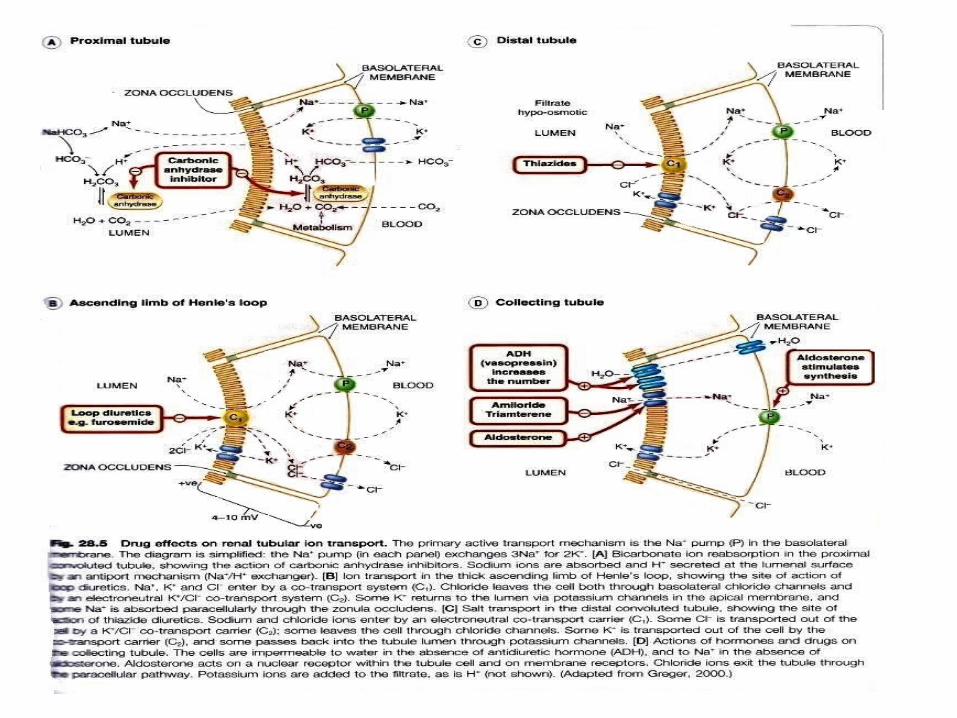
MECHANISM OF SALT REABSORPTION IN THE THICK ASCENDING LIMB OF LOOP OF HENLE (AscLH) CELL

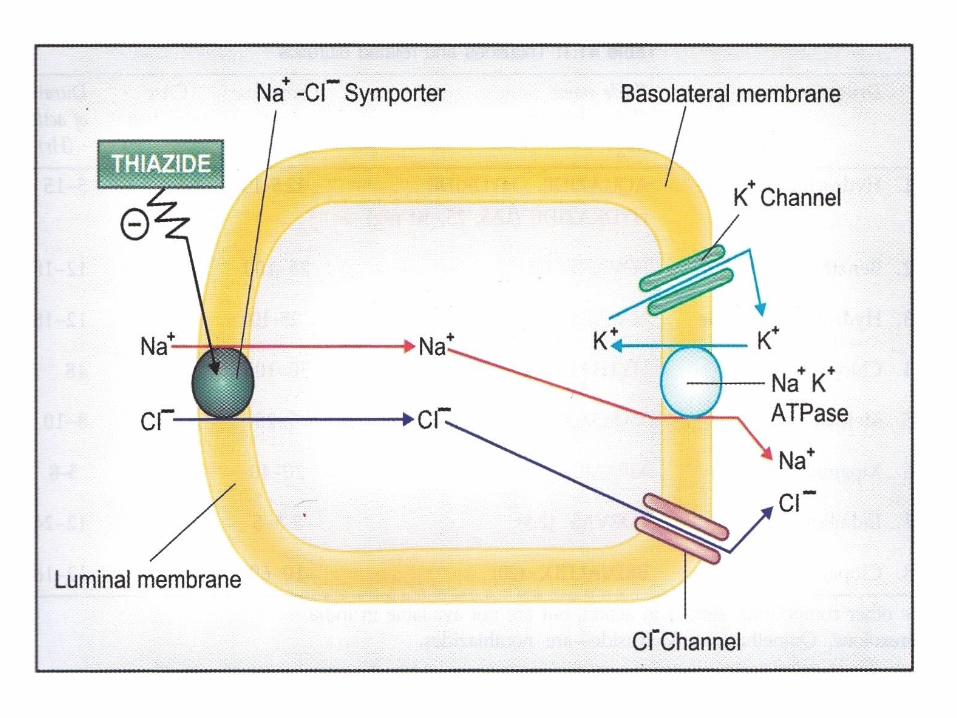
SITE-IIICORTICAL DILUTING SEGMENT OF LOOP OF HENLE
• Impermeable to water• Continues to absorb salt through Na+ - Cl-
symporter.• Tubular fluid gets further diluted.
SITE-IV DISTAL TUBULE (DT) AND COLLECTING DUCT (CD)
• In the late DT and CD, sod. Is again actively reabsorbed: the cation-anion balance being maintained by- passive chlor diffusion
and partly by pot and hydrogen. Absorption of sodium at this site occurs through a specific amiloride sensitive sod channel and by aldosterone.
DT and CD are rich in K+, a chemical gradient exists for its diffusion into tubular lumen due to transmembrane pot.difference.


DIURETICS• Drugs that promote the output of urine excreted by
kidney.• They are used for treatment of:1. Cardiac oedema related to Congestive Heart Failure (CHF).2. Nephrotic syndrome3. Diabetes insipidus4. Nutritional oedema.5. Liver cirrhosis.6. Hypertension.7. Oedema of pregnancy.8. To reduce intraocular and CSF pressure.9. Special cases: epilepsy, migraine, glaucoma, anginal
syndrome and bromide intoxication.
WHAT DIURETICS CAN DO ?• Diuretics may enhance the rate of urine
formation by :1. Increasing Glomerular Filtration. May act at
Site-I2. Depressing Tubular Reabsorption. May act at
Site-II, III, IV
THE NITTY-GRITTY
DiffusionOsmosis-isotonic, hypotonic, hypertonic, isosmoticOncotic pressure:Composition of blood:Route of urine formation:Coport- UniProt- symport- antiport• Medullary interstitium: The medullary interstitium is the tissue surrounding the
loop of Henle in the renal medulla. It functions in renal water reabsorption by building up a high hypertonicity, which draws water out of the thin descending limb of the loop of Henle and the collecting duct system. This hypertonicity, in turn, is created by an efflux of urea from the inner medullary collecting duct.
Malphigian corpuscle:Basolateral membrane:Macula densa: In the kidney, the macula densa is an area of closely packed
specialized cells lining the wall of the cortical thick ascending limb, at the transition to the distal convoluted tubule.
Interstitial fluid: ECF + plasma+ transcellular fluid. 10L