distribution duodenal mucosa subjects - gut.bmj.com · konturek, obtulowicz, sito, oleksy, wilkon,...
TRANSCRIPT
Gut, 1981, 22, 283-289
Distribution of prostaglandins in gastric and duodenalmucosa of healthy subjects and duodenal ulcerpatients: effects of aspirin and paracetamolS J KONTUREK,* W OBTULOWICZ, E SITO, J OLEKSY, S WILKON, ANDA KIEC-DEMBINSKA
From the Institute ofPhysiology and Pharmacology, Medical Academy and District Hospital,Krakow, Poland
SUMMARY The distribution of mucosal PGE2-like activity was determined by bioassay techniquein the body and antrum of the stomach and in the duodenum of healthy subjects and duodenalulcer patients before and after administration of aspirin, paracetamol, or histamine. In healthysubjects, the oxyntic, antral and duodenal mucosa was found to be capable of generating largeamounts ofPGE2, which were not significantly different from those found in duodenal ulcer patients.No correlation was found between the generation ofPGE2 and gastric acid secretory status or serumgastrin level. Aspirin-and to a much lesser extent, paracetamol-caused a dramatic reduction inthe ability of the gastric mucosa to biosynthesise PGE2 and this was accompanied by markedside-effects and injury to the gastric mucosa. Administration of histamine caused small but signi-ficant reduction in the biosynthesis of PGE2 but it was accompanied by marked mucosal damage.This study indicates that the gastric and duodenal mucosa is capable of generating PGE2-likeactivity which may be involved in the mechanism that protects the mucosa against the damagecaused by aspirin.
Human gastric mucosa has been shown to releaseprostaglandins under basal conditions and inresponse to secretory stimulation.'-3 It has beenpostulated that prostaglandins may play a role in thecontrol of gastric secretion4 and in the protection ofgastric mucosa against physical or chemical injury.,It has been suggested that the deficiency of mucosalprostaglandins is an important aetiological factor inpeptic ulcer disease6 7 but no information is availableregarding the generation and distribution of pro-staglandins in human gastric mucosa.
This study was undertaken to determine thedistribution of prostaglandins in gastric andduodenal mucosa of healthy subjects and duodenalulcer patients and to examine the effects of non-steroidal anti-inflammatory compounds and hista-mine administration on the generation of mucosalprostaglandins.
Address for correspondence: Professor Dr S J Konturek, Instituteof Physiology, 16 Grzegorzecka St, 31-531 Krakow, Poland.
Received for publication 18 November 1980
Methods
SUBJECTSThe study population was made up of 27 healthyvolunteers with no previous history of gastro-intestinal disease, bleeding disorders, or drug in-tolerance and 25 patients with active duodenal ulcerconfirmed by endoscopy. Their average age was 28years (range 20-34 years). They were not taking H2-blockers or anticholinergic drugs and had dis-continued antacids for at least 24 hours before theexamination. The study was approved by theHuman Research Review Committee and informedconsent was obtained from all participants after thenature of study has been fully explained.The examination started in early morning after a
12 hour fast, and a venous blood sample was takenfrom all subjects for serum gastrin and salicylatedetermination. Then intravenous diazepam wasgiven as premedication and gastro-duodenal endo-scopy was performed with the Olympus GIF-D2(Japan) endoscope. Four or five biopsy samples wereobtained from the stomach body and antrum and the
283
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from

Konturek, Obtulowicz, Sito, Oleksy, Wilkon, and Kiec-Dembinska
duodenal bulb. The mucosal samples were im-mediately plunged in ice-cold 005 M Tris buffer,pH 9.0, and used immediately for the bioassay ofprostaglandins as described below.
MEDICATIONThe effects of aspirin and paracetamol on gastricmucosa and the mucosal generation of prosta-glandins were examined in duodenal ulcer patientsand healthy volunteers divided into two groups,each containing six to eight subjects. Aspirin, para-
cetamol, or placebo was given orally in tablets. Eachtablet contained 0.5 g aspirin or paracetamol, whichwas administered in a total dose of 2.5 g divided intofive doses of 0.5 g each: one given before breakfast,after lunch, after supper, at bedtime the day beforeexamination, and in the early morning of the day ofexamination. In control tests, placebo tablets were
administered in the same way as aspirin or parace-tamol-that is, five times the day before and once on
the day of examination. The study was fully ran-
domised. Medications used in the study were
purchased from standard commercial sources, whileplacebo was obtained from the Upjohn Co.
In addition, one group of the healthy volunteerswas used for the study with histamine. The infusionof histamine was performed for 90 minutes insubjects fasted for 12 hours and gastric juice wasaspirated throughout the infusion using a standardnasogastric tube. Histamine acid phosphate wasgiven intravenously at a rate of 40 ,ug/kg/h afterblocking H,-effects with 50 mg mepyramine maleateintramuscularly. Immediately after the infusion ofhistamine, the nasogastric tube was removed andgastroduodenoscopy was performed.Duodenal ulcer subjects and volunteers involved
in the study were instructed to avoid alcohol, allmedications, and highly spiced food. They were
requested to record all side-effects, but, for thepurpose of this study, the target symptoms describedwere nausea, vomiting, epigastric pain or burning,and epigastric cramps. The overall subjectivesymptoms were characterised as minimal, moderate,or severe. About 10 days before the first dose andabout five hours after the last dose of medicationwith aspirin, paracetamol, or placebo the gastro-duodenal endoscopy was carried out and the gastricmucosa was observed and graded by the principalinvestigator, as described by Lanza et al.8 (Table).In all cases, a 0 grade was required at the initialendoscopy in order for the subject to continue in thestudy. In all cases four to five biopsy samples were
obtained from the body and antrum of the stomachand from the duodenum and immediately plunged inice-cold 0.05 M Tris buffer, pH 9 0, and used for thebioassay of prostaglandins.
Table Grading ofgastric mucosa
Grade Description
0 No evidence of submucosal haemorrhages1 + One submucosal haemorrhage2 + 1. More than one submucosal haemorrhage but not
numerous or widespread, or2. Oedema with two or more submucosal haemorrhages
3+ Numerous areas of submucosal haemorrhages4+ Large area of submucosal haehorrhage with active
bleeding or widespread involvement in the stomach
Superficial ulcers were rated as haemorrhages. Invasive ulcers of anysize were rated 4+.
GENERATION AND BIOASSAY OF MUCOSALPROSTAGLANDINSMucosal samples, which collectively weighed ap-proximately 30-50 mg, were washed from blood anddebris by shaking during five seconds with 1 ml ice-cold Tris buffer and then centrifuging at 9000 gfor 10 seconds. After the supernatant had beenremoved, a new volume of Tris buffer was added toresidual tissue in the proportion of 0 5 ml/150 mg oftissue weight. This sample was then shaken for 60seconds at room temperature using a steady speed ofa vortex stirrer and centrifuged at 9000 g for 15seconds as described by Whittle.9 Supernatant wasused for PGI,-assay immediately after centrifugationand then again after 30 minutes of storage at roomtemperature to destroy PGI2 for PGE2-assay.The concentration of PGI2 in the supernatant was
determined using its anti-aggregatory properties.10Rabbit blood was withdrawn by heart puncture to3.8% solution of sodium citrate 9 :lv/v. Plateletrich plasma (PRP) was prepared by centrifugation ofcitrated blood at 200 g for 10 minutes at roomtemperature. Platelet rich plasma was aggregated at37°C in a Born aggregometer with threshold pro-aggregatory concentrations of adenosine diphos-phate (2-5 ,uM). The anti-aggregatory potency ofstandard PGI2 was measured by addition of PGI2 atconcentrations of 0 4-10 ng/ml one minute beforeadenosine diphosphate was added. The percentage ofinhibition of the adenosine diphosphate-inducedaggregations was plotted against the effective con-centrations of PGI2 to obtain a standard curve. Tomeasure the amount of PGI2 generated by mucosa,5-50 Fl of the supernatant from incubation sampleswere added to platelet rich plasma one minute beforethe addition of ADP. The generation of a PGI2-likeactivity in tested samples was calculated by compar-ing their anti-aggregatory potency with that ofsynthetic PGI2. Results are expressed in nanogramsof the generated PGI2/g of tissue weight. The ratstomach strip and rat colon superfusion techniquewas used to determine the generation of PGE2 andPGF2a-like activity in the supernatant."1
284
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from
Distribution ofprostaglandins in gastric and duodenal mucosa
Rat stomach strip and rat colon were superfusedin cascade with pregassed (95% 02 and 5% CO2)Krebs solution containing such pharmacologicalantagonists as phenoxybenzamine (2 Fg/ml), pro-pranolol (4pg/ml), atropine sulphate (01 ,g/ml),methysergide (01 ,g/ml), diphenhydramine (0.1,ug/ml), and indomethacin (1 ,ug/ml). The tone ofrat stomach strip and rat colon was recorded withauxotonic levers (2-4 g initial load) using Harvardtransducers type 386 connected to a Watanabemultirecorder. Calibration doses of PGE2, PGF2a,or 25-50 pd of supernatant were infused alternatelyover the assay organs. Results are expressed asnonograms of the generated PGE2 per gram of tissueweight.
MEASUREMENT OF MAXIMAL ACID SECRETIONIn each subject gastric secretory test was performedusing pentagastrin in a dose 2 ,g/kg/h producingmaximal acid secretion according to the methodpreviously described.12 Peak-hour acid output wascalculated from the sum of the two highest con-secutive 15 minute outputs multiplied by 2.
SERUM GASTRIN AND SALICYLATEVenous blood obtained from the peripheral vein wasallowed to clot and serum obtained by centrifugationwas stored at -20°C until assayed. Serum gastrinconcentrations were measured by radioimmuno-assay.13 All samples were tested in duplicate in thesame assay. Antibody 4562 rabbit antiserum (kindlyprovided by Professor J F Rehfeld of Aarhus,Denmark) was used at a final dilution of 1:100 000.With this antibody all major molecular forms weremeasured on nearly equimolar basis, G-34 beingabout two-thirds as immunoreactive as G-17.Serum salicylate concentrations were measured by
the method of Saltzman.'4
STATISTICAL EVALUATION OF RESULTSResults are expressed as the means + SEM. Student'st test was used to determine the significance ofdifference between means, with differences giving aP value of less than 0.05 being consideredsignificant.'5
Results
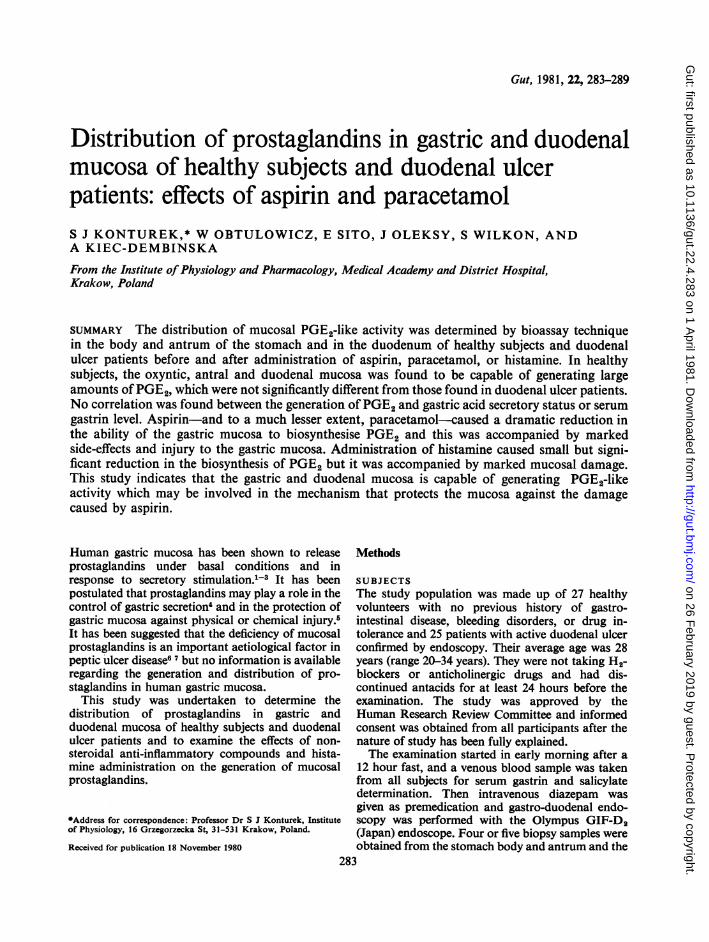
In all mucosal samples tested only the generation ofPGE2-like activity was found, whereas PGI2 andPGF2a were detected in negligible amounts andthese results are not included into the presentation.The mean (±SEM) values of the generated PGE2-like activity found in the oxyntic and antral portionsof the stomach and in the duodenum are presentedin Fig. 1. Both in normal subjects and in duodenal
NORMALSN =1L
PGE2 -activity(ng/g)
DUODENALN =13
Fig. 1 Schematic presentation of the distribution ofPGE2-like activity in the oxyntic and antral mucosa ofthe stomach and in the duodenal mucosa of healthysubjects and duodenal ulcer patients.
ulcer patients, antral mucosa tended to generatelarger amounts of PGE2 than oxyntic or duodenalmucosa but the difference was not significant. Nosignificant difference in the generation of PGE2 wasalso found between the oxyntic and duodenalmucosa. Healthy volunteers tended to exhibithigher PGE2 biosynthesising capability in theoxyntic and antral mucosa than duodenal ulcerpatients but, again, the difference in the generationof PGE2 between these two groups of subjects wasnot statistically significant.The mean pentagastrin-induced acid output in 14
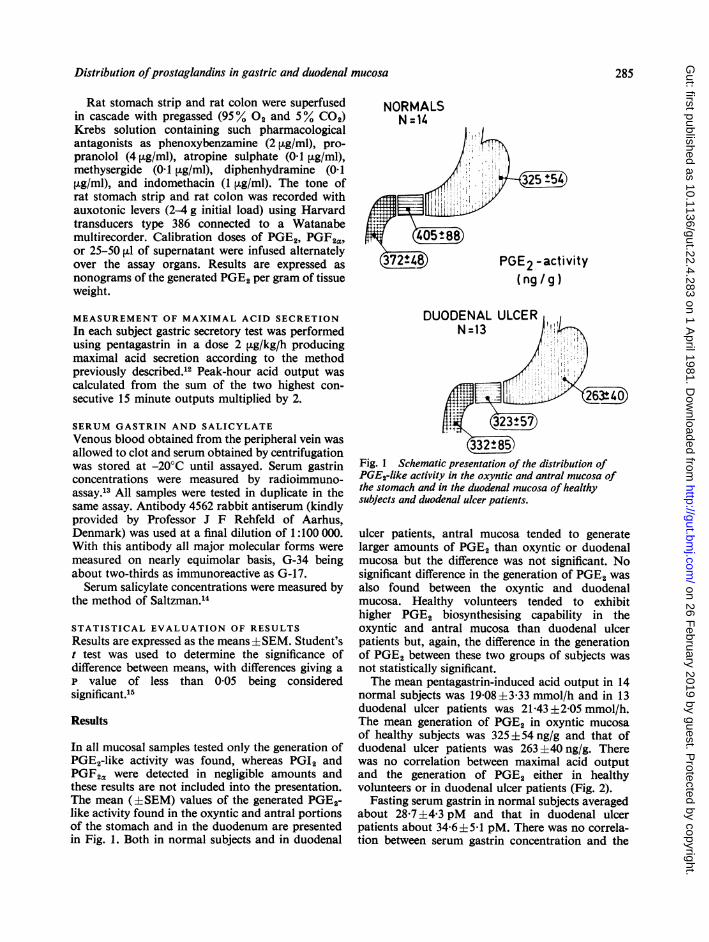
normal subjects was 19.08 ±3-33 mmol/h and in 13duodenal ulcer patients was 21.43 ±2.05 mmol/h.The mean generation of PGE2 in oxyntic mucosaof healthy subjects was 325 +54 ng/g and that ofduodenal ulcer patients was 263 ±40 ng/g. Therewas no correlation between maximal acid outputand the generation of PGE2 either in healthyvolunteers or in duodenal ulcer patients (Fig. 2).
Fasting serum gastrin in normal subjects averagedabout 28.7 ±443 pM and that in duodenal ulcerpatients about 34.6±5.1 pM. There was no correla-tion between serum gastrin concentration and the
285
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from
Konturek, Obtulowicz, Sito, Oleksy, Wilkon, and Kiec-Dembinska
60
0
.00 0
* 0° C o °
0
.
200 400PGE2 (ng/g)
Fig. 2 Relationship between maximathe generation ofPGE2 in the oxynticsubjects and duodenal ulcer patients.
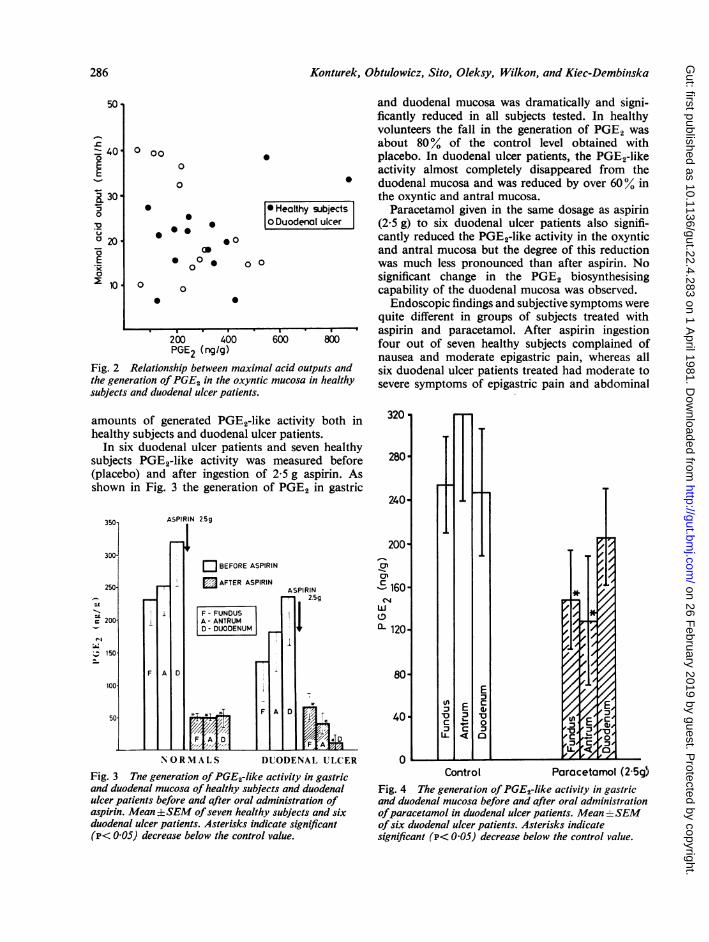
and duodenal mucosa was dramatically and signi-ficantly reduced in all subjects tested. In healthyvolunteers the fall in the generation of PGE2 wasabout 80% of the control level obtained withplacebo. In duodenal ulcer patients, the PGE2-likeactivity almost completely disappeared from theduodenal mucosa and was reduced by over 60% inthe oxyntic and antral mucosa.
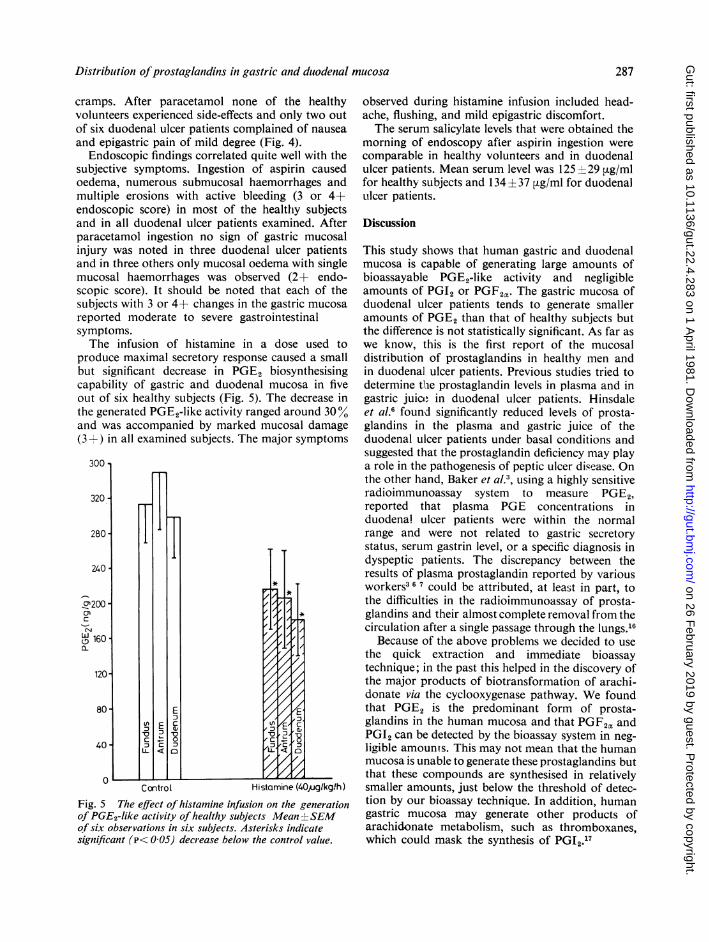
*Healthy subjects Paracetamol given in the same dosage as aspirinDuodenalulcer (25 g) to six duodenal ulcer patients also signifi-
cantly reduced the PGE2-like activity in the oxynticand antral mucosa but the degree of this reductionwas much less pronounced than after aspirin. Nosignificant change in the PGE2 biosynthesisingcapability of the duodenal mucosa was observed.
Endoscopic findings and subjective symptoms werequite different in groups of subjects treated with
.o aspirin and paracetamol. After aspirin ingestion600 800 four out of seven healthy subjects complained of
nausea and moderate epigastric pain, whereas allr1 acid outputs and six duodenal ulcer patients treated had moderate tomucosa in healthy severe symptoms of epigastric pain and abdominal
amounts of generated PGE2-like activity both inhealthy subjects and duodenal ulcer patients.
In six duodenal ulcer patients and seven healthysubjects PGE2-like activity was measured before(placebo) and after ingestion of 2.5 g aspirin. Asshown in Fig. 3 the generation of PGE2 in gastric
350 ASPIRIN 25g
300-EBEFORE ASPIRIN
250 AFTER ASPIRIN
F-FUNDUS
200 1 A - ANTRUM L
D DUODENUM
150
NORMALS DIUODENAL ULCER
Fig. 3 Tne generation ofPGE2-like activity in gastricand duodenal mucosa of healthy subjects and duodenalulcer patients before and after oral administration ofaspirin. Mean ±SEM ofseven healthy subjects and sixduodenal ulcer patients. Asterisks indicate significant(P< 005) decrease below the control value.
Control Parocetomol (2 5g5Fig. 4 The generation of PGE2-like activity in gastricand duodenal mucosa before and after oral administrationofparacetamol in duodenal ulcer patients. Mean ±SEMof six duodenal ulcer patients. Asterisks indicatesignificant (P< 005) decrease below the control value.
50-
.C40.
0E-1-?I 30.0
o 20'.5E0X 10'
0 00
0
0
0
286
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from
Distribution ofprostaglandins in gastric and duodenal mucosa
cramps. After paracetamol none of the healthyvolunteers experienced side-effects and only two outof six duodenal ulcer patients complained of nauseaand epigastric pain of mild degree (Fig. 4).
Endoscopic findings correlated quite well with thesubjective symptoms. Ingestion of aspirin causedoedema, numerous submucosal haemorrhages andmultiple erosions with active bleeding (3 or 4+endoscopic score) in most of the healthly subjectsand in all duodenal ulcer patients examined. Afterparacetamol ingestion no sign of gastric mucosalinjury was noted in three duodenal ulcer patientsand in three others only mucosal oedema with singlemucosal haemorrhages was observed (2+ endo-scopic score). It should be noted that each of thesubjects with 3 or 4+ changes in the gastric mucosareported moderate to severe gastrointestinalsymptoms.The infusion of histamine in a dose used to
produce maximal secretory response caused a smallbut significant decrease in PGE2 biosynthesisingcapability of gastric and duodenal mucosa in fiveout of six healthy subjects (Fig. 5). The decrease inthe generated PGE2-like activity ranged around 30%and was accompanied by marked mucosal damage(3 +) in all examined subjects. The major symptoms
300 l
320
280-
240
'Sa200
( 160'
120-
80'
40'
Control Histamine (40pjglkg/h)Fig. 5 The effect of histamine infusion on the generationof PGE2-like activity of healthy subjects Mean +rSEMof six observations in six subjects. Asterisks indicatesignificant (P< 0O05) decrease below the control value.
observed during histamine infusion included head-ache, flushing, and mild epigastric discomfort.The serum salicylate levels that were obtained the
morning of endoscopy after aspirin ingestion werecomparable in healthy volunteers and in duodenalulcer patients. Mean serum level was 125 + 29 stg/mlfor healthy subjects and 134± 37 ,tg/ml for duodenalulcer patients.
Discussion
This study shows that human gastric and duodenalmucosa is capable of generating large amounts ofbioassayable PGE2-like activity and negligibleamounts of PGI2 or PGF2a. The gastric mucosa ofduodenal ulcer patients tends to generate smalleramounts of PGE2 than that of healthy subjects butthe difference is not statistically significant. As far aswe know, this is the first report of the mucosaldistribution of prostaglandins in healthy men andin duodenal ulcer patients. Previous studies tried todetermine t1he prostaglandin levels in plasma and ingastric juice in duodenal ulcer patients. Hinsdaleet al.6 found significantly reduced levels of prosta-glandins in the plasma and gastric juice of theduodenal ulcer patients under basal conditions andsuggested that the prostaglandin deficiency may playa role in the pathogenesis of peptic ulcer disease. Onthe other hand, Baker et al.3, using a highly sensitiveradioimmunoassay system to measure PGE2,reported that plasma PGE concentrations induodenal ulcer patients were within the normalrange and were not related to gastric secretorystatus, serum gastrin level, or a specific diagnosis indyspeptic patients. The discrepancy between theresults of plasma prostaglandin reported by variousworkers3 6 7 could be attributed, at least in part, tothe difficulties in the radioimmunoassay of prosta-glandins and their almost complete removal from thecirculation after a single passage through the lungs.16
Because of the above problems we decided to usethe quick extraction and immediate bioassaytechnique; in the past this helped in the discovery ofthe major products of biotransformation of arachi-donate via the cyclooxygenase pathway. We foundthat PGE2 is the predominant form of prosta-glandins in the human mucosa and that PGF2X andPGI2 can be detected by the bioassay system in neg-ligible amounts. This may not mean that the humanmucosa is unable to generate these prostaglandins butthat these compounds are synthesised in relativelysmaller amounts, just below the threshold of detec-tion by our bioassay technique. In addition, humangastric mucosa may generate other products ofarachidonate metabolism, such as thromboxanes,which could mask the synthesis of PGI2.17
287
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from
288 Konturek, Obtulowicz, Sito, Oleksy, Wilkon, and Kiec-Dembinska
Our results indicate that the generation of PGE2by the oxyntic mucosa does not show a statisticallysignificant difference between the duodenal ulcerpatients and healthy subjects and that this generationis not correlated with the gastric acid secretorycapacity or serum gastrin level. Thus, it is unlikelythat the mucosal prostaglandins play an importantrole in the pathogenesis of ulcer disease as suggestedby Hindale et al.6 or in the local feedback control ofgastric secretion as proposed by Baker and hiscolleagues.3The major finding of this study is the demonstra-
tion that aspirin, the most widely used representiveof the non-steroidal anti-inflammatory compounds,causes dramatic reduction in the capacity of thegastric and duodenal mucosa to biosynthesise pro-staglandins and that it is closely correlated with thesubjective symptoms and the marked gastricmucosal injury. The fact that aspirin inhibits thebiosynthesis of prostaglandins in other tissues byirreversible inactivation of the prostaglandin syn-thetase system'8 19 is well recognised, but our reportdemonstrates for the first time the deficiency ofgastric mucosal prostaglandins attributable toaspirin treatment in man and its relationship togastrointestinal side-effects and gastric mucosallesions. Aspirin is known to be poorly tolerated byduodenal ulcer patients20 and our study suggeststhat this intolerance is caused by severe damage tothe gastric mucosa probably attributable to thedeficiency of the mucosal generation of prosta-glandins. This is supported also by our observationthat duodenal ulcer patients receiving paracetamol,another widely used analgesic and antypyreticsalicylate-like agent,2' reported little or no intoler-ance and this was accompanied by only mildgastroscopic mucosal changes and small reduction inmucosal generation of PGE2. The study with bothaspirin and paracetamol suggests that mucosalprostaglandins play an important role in theintegrity of gastric mucosa and that the suppressionof the generation of mucosal prostaglandins by non-steroidal anti-inflammatory compounds makes themucosa more vulnerable to chemical injury andresults in visible damage.Baker et al.3 reported that the stimulated gastric
acid output is significantly correlated with the outputof PGE2 into gastric juice, suggesting that themucosal prostaglandins may play a role in the localcontrol of gastric acid secretion. To test thishypothesis, we designed experiments in which themucosal generation of prostaglandins was measuredimmediately after the infusion of histamine in a doseproducing maximal gastric acid secretion wasdiscontinued. The results of this study show thatafter secretory stimulation by histamine the genera-
tion of mucosal prostaglandins tends to decreaseand, therefore, the mucosal changes in prostaglandinsmay not be paralleled by prostaglandin changes inthe gastric juice. Thus we failed to confirm thenotion that mucosal prostaglandins may be involvedin the feedback control of gastric secretion.3 4However, our study confirms22 that histamineadministration may, cause marked endoscopicmucosal damage without marked changes in themucosal generation of prostaglandins. Thus, itappears that damage to the mucosa does notnecessarily involve a reduction in the generation ofmucosal prostaglandins and may, therefore, not bemediated by the deficiency ofmucosal prostaglandins.
References
1Benett A, Stamford IF, Unger WG. Prostaglandin E2and gastric acid secretion in man. J Physiol 1973; 229:349-60.2Cheung LY, Jubiz W, Moore JG. Gastric prostaglandinE2 output during basal and stimulated acid secretion innormal subjects and patients with duodenal ulcer. JSurg Res 1976; 20: 369-72.3Baker R, Jaffe BM, Venables CW. Endogenous pro-staglandins in peptic ulcer disease. Gut 1979; 20: 394-9.4Horton EW. Hypotheses on physiological roles ofprostaglandins. Physiol Rev 1969; 49: 122-61.5Robert A. Cytoprotection by prostaglandins. Gastro-enterology 1979; 77: 761-7.6Hinsdale JG, Engel JJ, Wilson DE. Prostaglandin E2in peptic ulcer disease. Prostaglandins 1974; 6: 459-500.7Baker R, Jaffe BM, Reed JD, Shaw B, Venables CW.Are prostaglandins deficient in peptic ulceration? Gut1977; 18: 950-1.8Lanza FL, Rayer GL, Nelson RS, Chen TT, SeckmanCE, Rack MF. The effects of ibuprofen, indomethacin,aspirin, naproxen and placebo on the gastric mucosaof normal volunteers. Digest Dis Sci 1979; 24: 823-8."Whittle BJR. Potential endogenous inhibitor of pro-staglandin synthetase in plasma failure to inhibitcyclooxygenase in platelets and the gastric mucosa. JPharm Pharmacol 1978; 30: 467-8.
10Gryglewski RJ, Bunting S, Moncada S, Flower RJ,Vane JR. Arterial walls are protected against depositionof platelet thrombi by a substance (prostaglandin X)which prevents platelet aggregation. Prostaglandins1976; 12: 685-9.
"Vane JR. The use of isolated organs for detecting activesubstances in the circulating blood. Br J PharmacolChemother 1964; 23: 360-73.
12Konturek SJ, Lankosz J. Pentapeptide infusion test.Scand J Gastroenterol 1967; 2: 112-7.
13Yalow RS, Berson SA. Radioimmunoassay of gastrin.Gastroenterology 1970; 58: 1-14.
14Saltzman A. Fluorophotometric method for the estima-tion of salicylate in blood. J Biol Chem 1948: 174:399-404.
16Siegel S. Nonparametric Statistics for the BehavioralSciences. New York: McGraw-Hill, 1956
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from

Distribution ofprostaglandins in gastric and duodenal mucosa 289
6Piper PJ, Vane JR, Wyllie JH. Inactivation of pro-staglandins by the lungs. Nature 1970; 225: 600-4.
17LeDuc LE, Needleman P. Regional localization ofprostacyclin and thromboxane synthesis in dog stomachand intestinal tract. J Pharmacol Exp Ther 1979; 211:181-8.
"'Vane JR. Inhibition of prostaglandin synthesis as amechanism of action for aspirin-like drugs. Nature1971; 231: 232-5.
19Smith JB, Willis AL. Aspirin selectively inhibits prosta-glandin production in human platelets. Nature 1971;231: 235-7.
20Cooke AR. Drug damage of the gastroduodenum. In:Sleisenger MH, Fordtran JS, eds. Gastrointestinaldisease. Philadelphia: Saunders, 1978: 807-26.
21Woodbury DM, Fingl E. Analgesic-antypyretics anti-inflammatory agents, and drugs employed in thetherapy of gout. In: Goodman LS, Gilman A, eds.The pharmacological basis of therapeutics. New York:MacMillan, 1975: 325-50.
22Siegel H, Harbilas E, Katz D, Glass GBJ. Gastricerosions and mucosal hemorrhage during the aug-mented histamine test. Gastroenterology 1967; 52:1120.
on 26 February 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.22.4.283 on 1 A
pril 1981. Dow
nloaded from