disorders of calcium metabolism sophia ish-shalom rambam medical center haifa
TRANSCRIPT

calcium
40-45 % ionized
40-45 %albuminbound
10%10% complexedcomplexed
citrate, sulphatecitrate, sulphate
8.5–10.5 8.5–10.5 mg/dlmg/dl
ECFECF
FiltrationFiltration5-7gr5-7gr
ReabsorptionReabsorption4.9-6.7gr4.9-6.7gr98%98%
Diet 0.5-1.5 grDiet 0.5-1.5 gr
AbsorptionAbsorption0.25-0.5gr0.25-0.5gr
SecretionSecretion0.1-0.2gr0.1-0.2gr
FecesFeces0.35-0.6gr0.35-0.6gr
ResorptionResorption0.3-0.5 g0.3-0.5 g
FormationFormation0.3-0.5 g0.3-0.5 g
BoneBone1000 g1000 g
0.15-0.3 g/24h0.15-0.3 g/24h
• Total body Ca Total body Ca 1 to 1.5 kg1 to 1.5 kg• 99%- skeleton99%- skeleton• 0.1% ECF0.1% ECF• rest intracellularrest intracellular

CalciumCalcium
• An essential intracellular and extracellular cationAn essential intracellular and extracellular cation
• Extracellular calcium is required to maintain normal Extracellular calcium is required to maintain normal biological function of nervous system, the biological function of nervous system, the musculoskeletal system, and blood coagulationmusculoskeletal system, and blood coagulation
• Intracellular calcium is needed for normal activity of many Intracellular calcium is needed for normal activity of many enzymesenzymes
• Preservation of the integrity of cellular membranePreservation of the integrity of cellular membrane
• Regulation of endocrine and exocrine secretory activitiesRegulation of endocrine and exocrine secretory activities
• Activation of compliment systemActivation of compliment system
• Bone metabolismBone metabolism

Calcium (Ionized) - RolesCalcium (Ionized) - Roles
• In bone: calcium salts provide structural In bone: calcium salts provide structural integrity of the skeleton ( mineralization)integrity of the skeleton ( mineralization)
• Regulation of neuromuscular contractilityRegulation of neuromuscular contractility
• Regulation of activity of many enzymesRegulation of activity of many enzymes
• Cofactor in coagulation process ( factors Cofactor in coagulation process ( factors VII, IX, XVII, IX, X and prothrombin)and prothrombin)
• Cellular activities: second messenger, mediating Cellular activities: second messenger, mediating the effects of membrane signals on release or the effects of membrane signals on release or secretory products (neurotransmitters, amylase, secretory products (neurotransmitters, amylase, insulin, aldosteron)insulin, aldosteron)

Calcium and Albumin Calcium and Albumin
• 40-45% of circulating calcium is bound to albumin40-45% of circulating calcium is bound to albumin
• Change in serum Change in serum albuminalbumin change in change in measured measured total serum calciumtotal serum calcium concentration concentration
• Calcium is bound to carboxyl groups in albumin, this Calcium is bound to carboxyl groups in albumin, this binding is highly pH dependent binding is highly pH dependent
• Acute Acute acidosisacidosis binding ionized calcium binding ionized calcium
• Acute Acute alkalosisalkalosis binding ionized calcium binding ionized calcium
• A shift of 0.1 pH unit produces a change in ionized A shift of 0.1 pH unit produces a change in ionized calcium of 0.04 to 0.05 mmol/L ( 0.16-0.2 mg/dl)calcium of 0.04 to 0.05 mmol/L ( 0.16-0.2 mg/dl)
• These changes are not reflected at the total calciumThese changes are not reflected at the total calcium
Calcium and AlbuminCalcium and Albumin
• At pH 7.4 At pH 7.4 each g/dleach g/dl of serum albumin binds of serum albumin binds 0.8 mg/dl of 0.8 mg/dl of calcium calcium
• Serum calcium should be “corrected” according to Serum calcium should be “corrected” according to serum albumin levelserum albumin level
• Normal level of serum albumin is Normal level of serum albumin is 4 g/dl4 g/dl
• Change ofChange of 1 g/dl in serum albumin 0.8 mg/dl in total 1 g/dl in serum albumin 0.8 mg/dl in total serum calciumserum calcium
• Example: A patient with total serum calcium Example: A patient with total serum calcium 7.5 mg/dl7.5 mg/dl albumin albumin 2 mg/dl2 mg/dl, has corrected serum calcium of , has corrected serum calcium of 9.1 9.1 mg/dlmg/dl
Disorders of Calcium MetabolismDisorders of Calcium Metabolism
• Hypercalcemia Serum Calcium >10.4 mg/dlHypercalcemia Serum Calcium >10.4 mg/dl
• Hypocalcemia Serum Calcium < 8.5 mg/dlHypocalcemia Serum Calcium < 8.5 mg/dl

Causes of HypercalcemiaCauses of Hypercalcemia
Parathyroid relatedParathyroid related
I.I. Primary Primary hyperparathyroidismhyperparathyroidism
Solitary Solitary adenomaadenoma
HyperplasiaHyperplasia MENMEN
II.II. Lithium therapyLithium therapy
III.III. Familial Hypocalciuric Familial Hypocalciuric Hypercalcemia (FHH)Hypercalcemia (FHH)
Malignancy relatedMalignancy related
I.I. Solid tumor with Solid tumor with metastasis (breast)metastasis (breast)
II.II. Solid tumor with humoral Solid tumor with humoral mediation of mediation of hypercalcemia (lung, hypercalcemia (lung, kidney)kidney)
III.III.Hematologic Hematologic malignancies (multiple malignancies (multiple myeloma, lymphoma, myeloma, lymphoma, leukemia)leukemia)

Causes of HypercalcemiaCauses of Hypercalcemia
Vitamin D relatedVitamin D related
I.I. Vitamin D intoxicationVitamin D intoxication
.II.II.. 1,25(OH)1,25(OH)22D; D;
sarcoidosis and other sarcoidosis and other granulomatous diseasesgranulomatous diseases
III.III.Idiopathic Idiopathic hypercalcemia of hypercalcemia of infancyinfancy
Associated with high Associated with high bone turnoverbone turnover
I.I. HyperthyroidismHyperthyroidism
II.II. ImmobilizationImmobilization
III.III.ThiazidesThiazides
IV.IV.Vitamin A intoxicationVitamin A intoxication
Associated with renal failureAssociated with renal failureI.I. Severe secondary Severe secondary
hyperparathyroidismhyperparathyroidismII.II. Aluminum intoxicationAluminum intoxicationIII.III. Milk- alkali syndromeMilk- alkali syndrome

Diagnosis of HypercalcemiaDiagnosis of Hypercalcemia
Serum Ca Serum Ca ..
Measure serum albuminMeasure serum albumin or ionized calciumor ionized calcium
Albumin corrected Albumin corrected calcium normalcalcium normal
Medical historyMedical history and medication use historyand medication use history
Measure PTHMeasure PTH
PTH PTH .. or N or N
Check calciuriaCheck calciuria
PTH PTH ..
MalignancyMalignancyCheck 1,25(OH)Check 1,25(OH)22DD33

Diagnosis of HypercalcemiaDiagnosis of Hypercalcemia
Check calciuriaCheck calciuria
Urine CaUrine Ca..
FHHFHH
Urine Ca Urine Ca ../ N/ N
Primary HPTPrimary HPT
Check 1,25(OH)Check 1,25(OH)22DD33
Granulomatous diseases Granulomatous diseases (Sarcoidosis), Lymphoma(Sarcoidosis), Lymphoma
1,25(OH)1,25(OH)22DD3 3 ..

Primary HyperparathyroidismPrimary Hyperparathyroidism
Incidence 42/100 000Incidence 42/100 000
Age > 40 Age > 40 1/200; 1/10001/200; 1/1000
.. X 3.5X 3.5 after introduction of routine serum after introduction of routine serum calcium testingcalcium testing
80%80% single gland involvement – adenoma single gland involvement – adenoma
20%20% multiple gland involvement – hyperplasia multiple gland involvement – hyperplasia
<2%<2% carcinoma carcinoma
MENMEN


HyperparathyroidismHyperparathyroidism
Serum Serum CalciumCalcium
Serum Serum PhosphorusPhosphorus Plasma PTHPlasma PTH
PrimaryPrimary .. .. / Normal/ Normal .. / Normal/ Normal
SecondarySecondary ../ Normal/ Normal .. / Normal / / Normal / .. .. / / .. ..
TertiaryTertiary .. Normal / Normal / .. .. .. ..

Clinical ManifestationsClinical Manifestations
• CNS - CNS - Cognitive difficulties, apathy, drowsiness, Cognitive difficulties, apathy, drowsiness, obtundation or even comaobtundation or even coma
• GI - GI - Anorexia, nausea, vomiting, constipation and Anorexia, nausea, vomiting, constipation and rarely acute pancreatitisrarely acute pancreatitis
• CVS - CVS - Hypertension, A-V nodal delay, shortened Hypertension, A-V nodal delay, shortened QT interval, enhanced sensitivity to digitalis, QT interval, enhanced sensitivity to digitalis, compete heart block, ventricular arrhythmiascompete heart block, ventricular arrhythmias
• RENAL- RENAL- Loss of concentrating ability, polyuria, Loss of concentrating ability, polyuria, polydipsia, nephrolithiasis and occasionally polydipsia, nephrolithiasis and occasionally nephrocalcinosis, nephrocalcinosis, nocturianocturia

Bone and Joint Manifestations in Primary Bone and Joint Manifestations in Primary HyperparathyroidismHyperparathyroidism
• OsteoporosisOsteoporosis
• Diffuse bone pain without Diffuse bone pain without osteitis fibrosa cysticaosteitis fibrosa cystica
• Osteitis fibrosa cysticaOsteitis fibrosa cystica Diffuse demineralizationDiffuse demineralization Subperiostal bone Subperiostal bone
resorptionresorption PhalangesPhalanges Lamina duraLamina dura Distal claviclesDistal clavicles
Cystic lesionsCystic lesionsBrown tumors Brown tumors CystsCysts
Deformities, Fractures, Deformities, Fractures, PainPain
• Arthritic symptomsArthritic symptomsResorption of articular Resorption of articular
bonebonePeriarticular metastatic Periarticular metastatic
calcificationcalcificationPseudogoutPseudogoutGoutGout



TreatmentTreatment
When is surgery indicated in PHPT patients When is surgery indicated in PHPT patients
??
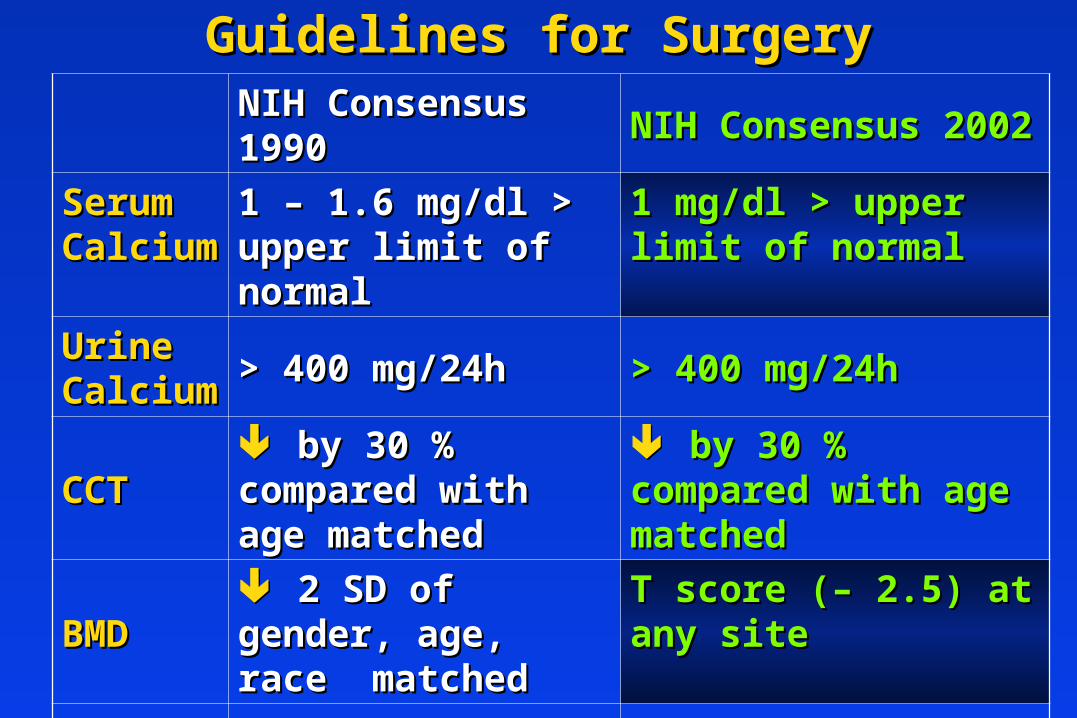
Guidelines for SurgeryGuidelines for SurgeryNIH Consensus 1990NIH Consensus 1990 NIH Consensus 2002NIH Consensus 2002
Serum Serum CalciumCalcium
1 – 1.6 mg/dl > upper 1 – 1.6 mg/dl > upper limit of normallimit of normal
1 mg/dl > upper limit of 1 mg/dl > upper limit of normalnormal
Urine Urine CalciumCalcium > 400 mg/24h> 400 mg/24h > 400 mg/24h> 400 mg/24h
CCTCCT by 30 % by 30 % compared with age compared with age matchedmatched
by 30 % compared by 30 % compared with age matchedwith age matched
BMDBMD 2 SD of gender, 2 SD of gender, age, race matchedage, race matched
T score (– 2.5) at any T score (– 2.5) at any sitesite
AgeAge < 50< 50 < 50< 50
Patients for whom medical surveillance is either not Patients for whom medical surveillance is either not desirable or not possibledesirable or not possible

Femoral Neck BMD Change in PHPT Femoral Neck BMD Change in PHPT PatientsPatients
Silverberg et al NEJM

Other ConsiderationsOther Considerations
• Neuropsychological disturbancesNeuropsychological disturbances
• Weakness and easy fatigabilityWeakness and easy fatigability
• DepressionDepression
• Intellectual wearinessIntellectual weariness
• Increased sleep requirementsIncreased sleep requirements
Improved by surgeryImproved by surgery
• Onset of MenopauseOnset of Menopause
• Increased bone lossIncreased bone loss
99m99mTc- sestamibi Parathyroid ScanTc- sestamibi Parathyroid Scan
20 min20 min 3 hours3 hours
90% sensitivity in parathyroid tissue detection90% sensitivity in parathyroid tissue detection

Patients’ MonitoringPatients’ Monitoring
Goal – early detection of:Goal – early detection of:
• Worsening of hypercalcemiaWorsening of hypercalcemia
• Renal impairmentRenal impairment
• Loss of bone massLoss of bone mass
• StonesStones
• FracturesFractures

Guidelines for MonitoringGuidelines for Monitoring
NIH Consensus 1990NIH Consensus 1990 NIH Consensus 2002NIH Consensus 2002
Serum Serum CalciumCalcium x2 yearx2 year x2 yearx2 year
Urine Urine CalciumCalcium x1 yearx1 year Not recommendedNot recommended
CCTCCT x1 yearx1 year Not recommended, s-crNot recommended, s-cr
Abdom. X-Abdom. X-Ray, US Ray, US x1 yearx1 year Not recommendedNot recommended
BMDBMD x1 year (forearm)x1 year (forearm) x1 year (3 sites: lumbar x1 year (3 sites: lumbar spine, hip, forearm)spine, hip, forearm)

General MeasuresGeneral Measures
• Hydration
• Adequate Mobility
• Diet neither restrictive nor excessive in calcium
• Adequate vitamin D status
• Prompt medical attention for the possibility of worsening of hypercalcemia (intercurrent illness accompanied by risk of dehydration)

Calcium-sensing ReceptorCalcium-sensing Receptor• A member of the G protein-coupled receptor familyA member of the G protein-coupled receptor family
• Contains seven hydrophobic helices that anchor it in the plasma Contains seven hydrophobic helices that anchor it in the plasma membrane. The large (~600 amino acids) extracellular domain - membrane. The large (~600 amino acids) extracellular domain - critical to interactions with extracellular calciumcritical to interactions with extracellular calcium
• Large (~200 amino acids) cytosolic tail. Large (~200 amino acids) cytosolic tail.

Inactivating Mutations in Calcium Inactivating Mutations in Calcium Sensing ReceptorSensing Receptor
• Inactivating mutationInactivating mutation
– Familial hypocalciuric hypercalcemia (FHHFamilial hypocalciuric hypercalcemia (FHH) - ) - heterozygousheterozygous
Calcium set point serum calcium Calcium set point serum calcium
Urinary calcium reabsorption urinaryUrinary calcium reabsorption urinary
calcium calcium
– Neonatal severe hyperparathyroidism (NSHPT) – Neonatal severe hyperparathyroidism (NSHPT) – homozygoushomozygous
מחלה קטלנית אם לא מבצעים כריתה של בלוטות ה- מחלה קטלנית אם לא מבצעים כריתה של בלוטות ה- parathyroidparathyroid
– Familial hypocalciuric hypercalcemia (FHHFamilial hypocalciuric hypercalcemia (FHH) - ) - heterozygousheterozygous
Calcium set point serum calcium Calcium set point serum calcium
Urinary calcium reabsorption urinaryUrinary calcium reabsorption urinary
calcium calcium
– Neonatal severe hyperparathyroidism (NSHPT) – Neonatal severe hyperparathyroidism (NSHPT) – homozygoushomozygous
מחלה קטלנית אם לא מבצעים כריתה של בלוטות ה- מחלה קטלנית אם לא מבצעים כריתה של בלוטות ה- parathyroidparathyroid

Hypercalcemia of MalignancyHypercalcemia of Malignancy
• Lung, breast, and prostate cancer frequently invade Lung, breast, and prostate cancer frequently invade skeleton and skeleton and destroy bone tissuedestroy bone tissue
• Breast and lung cancer also cause Breast and lung cancer also cause hypercalcemia of hypercalcemia of malignancy (HCMmalignancy (HCM), ), without invading skeletonwithout invading skeleton
• Multiple myeloma has skeletal complications in Multiple myeloma has skeletal complications in virtually 100% of casesvirtually 100% of cases
• Damage to skeleton usually late in course of diseaseDamage to skeleton usually late in course of disease
• Bone damage associated with considerable worsening Bone damage associated with considerable worsening in patient’s quality of lifein patient’s quality of life

PTHrP-PTH related peptidePTHrP-PTH related peptide 1212גן על כרומוזום גן על כרומוזום •
: סחוס, לב, זקיקי שיערות, אפיתל: סחוס, לב, זקיקי שיערות, אפיתלעובריםעובריםהגן מצוי ברקמות הגן מצוי ברקמות •
: חשוב : חשוב מבוגרמבוגר מבוטא ברקמות של מבוטא ברקמות של PTHrPPTHrPהגן ל- הגן ל- •להתפתחות רקמת שד, ריכוז גבוה בחלבלהתפתחות רקמת שד, ריכוז גבוה בחלב
מוטציה בעכברמוטציה בעכבר
הומוזיגוטים מוטציה לטלית הטרוזיגוטים תקיניםהומוזיגוטים מוטציה לטלית הטרוזיגוטים תקינים
פגמים בהתפתחות העצם והסחוספגמים בהתפתחות העצם והסחוס

PthrP Induced HypercalcemiaPthrP Induced Hypercalcemia
Squamous cell carcinoma
Islet cell tumor (pancreas)
Adult T cell leukemia
Renal cell carcinoma
Breast carcinoma

Paracrine Effect of Bone Resorbing Paracrine Effect of Bone Resorbing SubstancesSubstances
Malignant cells travel through Malignant cells travel through bloodstream & invade bonebloodstream & invade bone
Release substances into immediate area:Release substances into immediate area:
• PTHrPPTHrP
• TGF-TGF- (transforming growth factor- (transforming growth factor-alpha)alpha)
• IL-1 (interleukin-1)IL-1 (interleukin-1)
• TNF (tumor necrosis factor)TNF (tumor necrosis factor)
• IL-6 (interleukin-6)IL-6 (interleukin-6)
Cause osteoclast activation andlocal Cause osteoclast activation andlocal bone destruction & can lead to bone destruction & can lead to hypercalcemiahypercalcemia


Plasma Cell MyelomaPlasma Cell Myeloma

Skeletal MetastasisSkeletal Metastasis

TreatmentTreatment
HydrationHydration
FurosemideFurosemide
BisphosphonatesBisphosphonates
CalcitoninCalcitonin
GlucocorticoidsGlucocorticoids
DialysisDialysis

HydrationHydration
• First step in the management of severe First step in the management of severe hypercalcemia - Isotonic salinehypercalcemia - Isotonic saline
• Usually Usually .. serum calcium by 1.6-2.4mg/dl serum calcium by 1.6-2.4mg/dl
• Hydration alone rarely leads to Hydration alone rarely leads to normalization in severe hypercalcemianormalization in severe hypercalcemia
• Rate of IV saline based on severity of Rate of IV saline based on severity of hypercalcemia and tolerance of CVS for hypercalcemia and tolerance of CVS for volume expansion, if possible achieve volume expansion, if possible achieve urine output of 300 ml/hrurine output of 300 ml/hr

Loop DiureticsLoop Diuretics
• Facilitate urinary excretion of calcium
– By inhibiting calcium reabsorption in the By inhibiting calcium reabsorption in the thick ascending limb of the loop of Henle. thick ascending limb of the loop of Henle.
• Guard against volume overload
– Volume expansion must precede the Volume expansion must precede the administration of furosemide, because the administration of furosemide, because the drug’s effect depends on delivery of calcium drug’s effect depends on delivery of calcium to the ascending limb. Needs frequent to the ascending limb. Needs frequent measurement of electrolytes and watermeasurement of electrolytes and water

BisphosphonatesBisphosphonates
• Structurally related to pyrophosphate
• Bind to hydroxyapatite in bone and inhibit the dessolution of crystals
• Great affinity for bone and their resistance to degradation
• Extremely long half life in bone
• Poor GI absorption < 1%

PamidronatePamidronate
• Inhibits osteoclast functionInhibits osteoclast function
• 60mg to 90 mg IV over 24hr60mg to 90 mg IV over 24hr
• 70% to 100% of patients had 70% to 100% of patients had .. serum serum calcium within 24 hrs, 2/3rd of this group calcium within 24 hrs, 2/3rd of this group had normal serum calcium within 7 dayshad normal serum calcium within 7 days
• Adverse effects:Adverse effects:
– mild transient mild transient .. in temp (<2deg C) in temp (<2deg C)
– transient leukopeniatransient leukopenia
– small small .. in s phosphate level in s phosphate level
• Excreted by kidney Excreted by kidney .. dose adjustment dose adjustment

Relative Potencies of BisphosphonatesRelative Potencies of Bisphosphonates
1. Green JR, Müller K, Jaeggi KA. Preclinical pharmacology of CGP 42'446, a new, potent, heterocyclic bisphosphonate compound. J Bone Miner Res. 1994;9:745-751.
0.05 1.00 2.77 7.44 35.90 43.60
847
0
100
200
300
400
500
600
700
800
900
clodronate pamidronatedisodium
olpadronate alendronate risedronate ibandronate ZOMERA®
(zoledronic acid)
Potencies of BisphosphonatesP
ote
ncy r
ela
tive t
o p
am
idro
nate
dis
od
ium
P
ote
ncy r
ela
tive t
o p
am
idro
nate
dis
od
ium
in
viv
oin
viv
o (
hyp
erc
alc
em
ic r
at)
, lin
ear
scale
(h
yp
erc
alc
em
ic r
at)
, lin
ear
scale

Zoledronic Acid (ZOMERA)Zoledronic Acid (ZOMERA)
• Zoledronic acid belongs to a new class of highly Zoledronic acid belongs to a new class of highly potent bisphosphonatespotent bisphosphonates
• Heterocyclic, nitrogen-containing bisphosphonate Heterocyclic, nitrogen-containing bisphosphonate composed of:composed of:• A core bisphosphonate moiety A core bisphosphonate moiety • An imidazole-ring side chain containing 2 critically positioned An imidazole-ring side chain containing 2 critically positioned
nitrogen atoms nitrogen atoms
NN
O
O
P
P
HO OH
OH
OH
OH

• Inhibit the growth of neoplastic lymphoid Inhibit the growth of neoplastic lymphoid tissuetissue
• Counteract the effects of vitamin DCounteract the effects of vitamin D
GlucocorticoidsGlucocorticoids

Functionally Based Classification of Functionally Based Classification of HypocalcemiaHypocalcemia
I.I. PTH absentPTH absent
A.A. Hereditary hypoparathyroidismHereditary hypoparathyroidism
B.B. Acquired hypoparathyroidismAcquired hypoparathyroidism
AutoimmuneAutoimmune
Post surgicalPost surgical
C.C. HypomagnesemiaHypomagnesemia

Functionally Based Classification of Functionally Based Classification of HypocalcemiaHypocalcemia
III.III.PTH overwhelmedPTH overwhelmed
A.A. Severe acute hyperphosphatemiaSevere acute hyperphosphatemia
1.1. Tumor lysisTumor lysis
2.2. Acute renal failureAcute renal failure
3.3. RhabdomyolysisRhabdomyolysis
B.B. ““Hungry bone syndrome” after Hungry bone syndrome” after parathyroidectomyparathyroidectomy

Functionally Based Classification of HypocalcemiaFunctionally Based Classification of Hypocalcemia
II.II. PTH ineffectivePTH ineffective
A.A. Chronic renal failureChronic renal failure
B.B. Active vitamin D lackingActive vitamin D lacking
.... ..Dietary intake or sunlightDietary intake or sunlight
2.2.Defective metabolismDefective metabolism
Anticonvulsant therapyAnticonvulsant therapy
Vitamin D dependent rickets type IVitamin D dependent rickets type I
C.C. Active vitamin D ineffectiveActive vitamin D ineffective
1.1.Intestinal malabsorptionIntestinal malabsorption
2.2.Vitamin D dependent rickets type IIVitamin D dependent rickets type II
D.D. PseudohypoparathyroidismPseudohypoparathyroidism

Differential Diagnosis of HypocalcemiaDifferential Diagnosis of Hypocalcemia
Correct calcium for albumin: Ca = measured Ca + 0.8 for Correct calcium for albumin: Ca = measured Ca + 0.8 for each mg/dl albumin below 4.0each mg/dl albumin below 4.0
Hypovitaminosis DHypovitaminosis D

Manifestations of Acute HypocalcemiaManifestations of Acute Hypocalcemia
• CNSCNS– Psychiatric disturbancesPsychiatric disturbances– SeizuresSeizures
• NeuromuscularNeuromuscular– Tremor, twitching, movement disordersTremor, twitching, movement disorders– Positive Chvostek and Trousseau signsPositive Chvostek and Trousseau signs– Carpopedal spasmCarpopedal spasm– TetanyTetany
• CardiacCardiac– Q-T prolongation on ECGQ-T prolongation on ECG– Ventricular ArrhitmiaVentricular Arrhitmia– Heart blockHeart block

ECG in HypocalcemiaECG in Hypocalcemia•Sinus rhythm with Sinus rhythm with diffuse T wave inversiondiffuse T wave inversion•T waves -inverted, but of relatively normal widthT waves -inverted, but of relatively normal width •QT prolongationQT prolongation (The corrected qtc is 560 ms (The corrected qtc is 560 ms ) )•Prolongation is in the Prolongation is in the ST segmentST segment rather than the rather than the T wavesT waves

Carpopedal SpasmCarpopedal Spasm

Treatment of Acute HypocalcemiaTreatment of Acute HypocalcemiaCalcium RepletionCalcium Repletion
• Promptly correct symptomatic or severe Promptly correct symptomatic or severe hypocalcemia with cardiac arrhythmias or tetany hypocalcemia with cardiac arrhythmias or tetany with parenteral administration of calcium saltswith parenteral administration of calcium salts
• Administer 1-2 ampules 10% calcium gluconate (93 Administer 1-2 ampules 10% calcium gluconate (93 mg/10 mL) in 50-100 mL of D5W over 5-10 minutes mg/10 mL) in 50-100 mL of D5W over 5-10 minutes then NS with 15 mg/kg of calciumthen NS with 15 mg/kg of calcium
• Each 10 cc ampule of 10% calcium gluconate Each 10 cc ampule of 10% calcium gluconate contains 1 gm of calcium gluconate but less than 100 contains 1 gm of calcium gluconate but less than 100 mg of calcium then therefore, if want to give 15 mg of calcium then therefore, if want to give 15 mg/kg calcium to 70 kg pt, have to give 10 ampsmg/kg calcium to 70 kg pt, have to give 10 amps
• Measure serum calcium every 4-6 hours to maintain Measure serum calcium every 4-6 hours to maintain serum calcium levels at 8-9 mg/dLserum calcium levels at 8-9 mg/dL

Treatment of Acute HypocalcemiaTreatment of Acute Hypocalcemia
• Patients with Patients with cardiac arrhythmias or patients cardiac arrhythmias or patients on digoxin therapy on digoxin therapy need continuous ECG need continuous ECG monitoringmonitoring during calcium replacement during calcium replacement because calcium potentiates digitalis toxicity.because calcium potentiates digitalis toxicity.
• In case of extreme emergency:In case of extreme emergency: Calcium Calcium chloride 10% solutionchloride 10% solution (273 mg/10-mL ampule) (273 mg/10-mL ampule) delivers higher amounts of calcium and has delivers higher amounts of calcium and has advantages when rapid correction is needed, advantages when rapid correction is needed, but it is very irritating when administered but it is very irritating when administered intravenously and probably only should be intravenously and probably only should be administered centrally. administered centrally.

Treatment of Acute HypocalcemiaTreatment of Acute Hypocalcemia
• Identify and treat the causeIdentify and treat the cause of hypocalcemia of hypocalcemia
and taper the infusion. and taper the infusion.
• Start oral calcium and vitamin D treatment Start oral calcium and vitamin D treatment
early. Patients with early. Patients with postparathyroidectomy postparathyroidectomy
hungry bone diseasehungry bone disease, especially those with , especially those with
osteitis fibrosa cysticaosteitis fibrosa cystica, can present with a , can present with a
dramatic picture of hypocalcemia. dramatic picture of hypocalcemia.

Activating MutationActivating Mutation
• Familial hypercalciuric hypocalcemia - Familial hypercalciuric hypocalcemia - the opposite of what is seen with the opposite of what is seen with inactivating mutationsinactivating mutations
Calcium set point serum calcium Calcium set point serum calcium
Urinary calcium reabsorption Urinary calcium reabsorption
Urinary calcium Urinary calcium