nephrotic syndrome farid nakhoul m.d. deputy director dept. of nephrology rambam medical ctr....
TRANSCRIPT

Nephrotic Syndrome
Farid Nakhoul M.D.
Deputy Director
Dept. of Nephrology
Rambam Medical Ctr.
Faculty of Medicine Haifa
Tel: 04-8542590 Fax: 048542946
Email:[email protected]

Structure of the Glomerulus(1)
• One of the central function of the kidney is to excrete low molecular weight water-soluble plasma waste products into the urine. Whereas macromolecules the size of albumin and larger are retained. The filtration of plasma occurs in specialized filtration units called Glomeruli.

Structure of the Glomerulus(2)
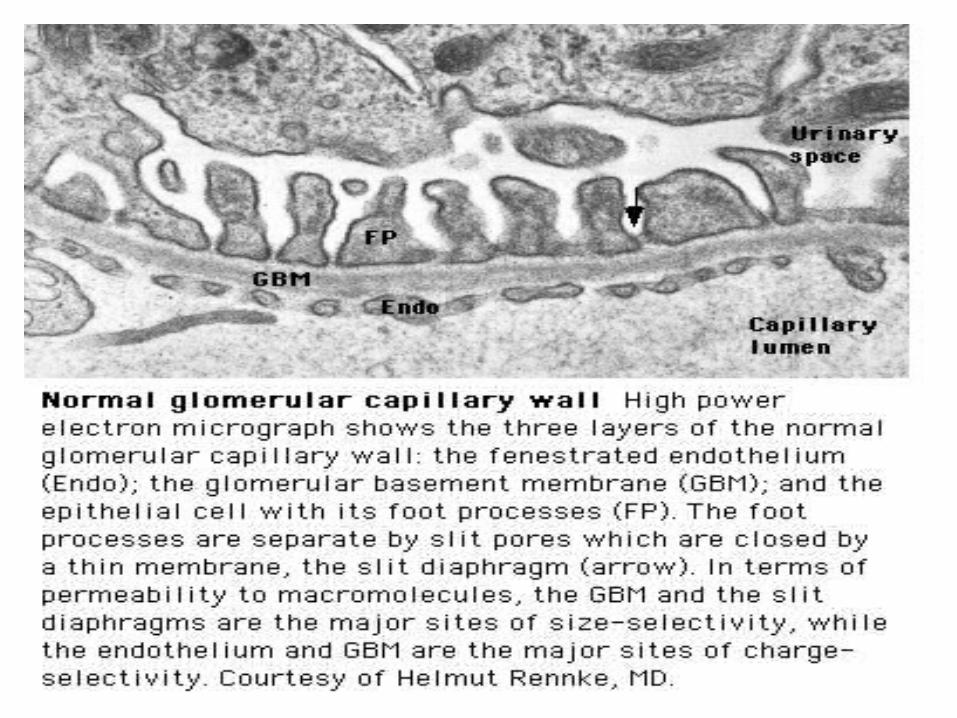
The glomerular filtration barrier consists of the three layers of the capillary wall:
1. The innermost fenestrated vascular endothelium.
2. The GBM: the GBM is regarded as a primary size and charge-selective molecular sieve of the glomerulus . The GBM contains type IV collagen, laminin, nidogen, and proteoglycans as its main components.
3. Podocyte cell layer facing the urinary space.




Proteinuria
Is the halmark of glomerular disease !!

Clinical Evaluation of Glomerular disease
1. History
2. Physical Examination
3. Laboratory Studies
4. Imaging: Ultrasound
5. Renal Biopsy ( Open, Closed, Laparoscopic).

Proteinuria
• Asymptomatic Non-nephrotic Proteinuria (<3.5 gr Protein/day).
- Glomerular
- Non-glomerular
• Nephrotic Syndrome: Pathognomonic of glomerular disease

Non-Nephrotic Proteinuria
• Defined as a urine protein excretion of less than 3.5 gr/d, and is absolutely characteristic of glomerular disease, but may occure in many non-glomerular parenchymal disease.

Clinical ClassificationClinical Classification
Isolated Hematuria Isolated Hematuria Proteinuria / Nephrotic SyndromeProteinuria / Nephrotic Syndrome Acute Nephritic SyndromeAcute Nephritic Syndrome Rapidly Progressive Glomerulonephritis Rapidly Progressive Glomerulonephritis Chronic Glomerulonephritis Chronic Glomerulonephritis

Clinical Features of Clinical Features of Glomerular DiseasesGlomerular Diseases
Proteinuria Proteinuria
HematuriaHematuria
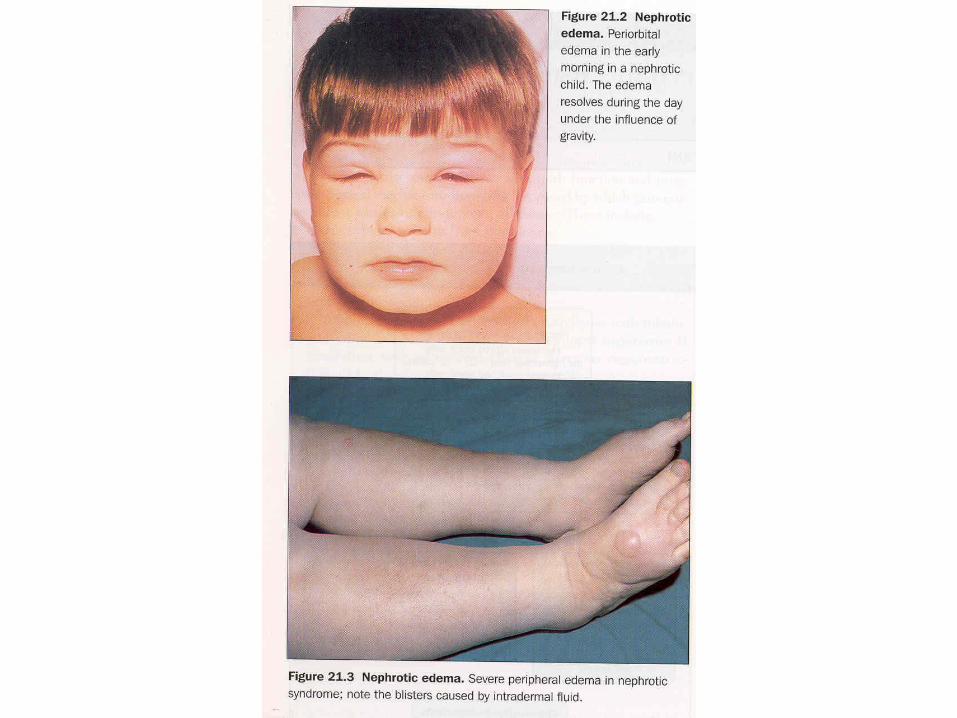
Edema Edema
HypertensionHypertension
Renal DysfunctionRenal Dysfunction

Evaluation of Proteinuria – General PracticeHistory, Physical
Examination, urinalysis
Repeat visit for qualitative proteinuria test
Positive
Measure U&E, Albumin, Quantify urine protein excretion
Negative
Transient Proteinuria; Reassure Patient


Quantifying protein excretion
Protein-to-creatinine ratio (PCR)– Simple– Validated
• Should perform quantitative measure in persistent proteinuria
24 hour urine collection– Readily quantified– Wide understanding– Cumbersome

Nephrotic SyndromeDefinition
• Urinary protein level exceeding 3.5 gr per 1.73m2 of body-surface area/day.
• Hypoalbuminemia.
• Sodium retention (Edema-State).
• Hyperlipoproteinemia. • Hypercoagulopathy

Prognosis
• Depends upon degree of proteinuria
• 20 year follow up:– Hypertension in 50%– Renal Insufficiency in 40%

Diagnostic ApproachDiagnostic Approach
24 urine collection24 urine collection Serum electrolytes, BUN, creatinine, lipid profile, Serum electrolytes, BUN, creatinine, lipid profile,
serum albuminserum albumin Serological work up - depends upon the clinical Serological work up - depends upon the clinical
presentation - common serological tests done arepresentation - common serological tests done areANA; Anti-ds DNAANA; Anti-ds DNAComplement levelsComplement levels (C3, C4)(C3, C4)Hepatitis B and C serologiesHepatitis B and C serologiesSPEP; UPEP, ANCA, anti GBM AbsSPEP; UPEP, ANCA, anti GBM Abs
Renal UltrasoundRenal Ultrasound Renal Biopsy - IndicationsRenal Biopsy - Indications
Nephrotic SyndromeNephrotic Syndrome
Primary Primary Membranous GlomerulopathyMembranous Glomerulopathy
Focal Segmental GlomerulosclerosisFocal Segmental GlomerulosclerosisMinimal Change DiseaseMinimal Change DiseaseMembranoproliferative GNMembranoproliferative GN
Secondary Secondary Diabetic glomerulosclerosisDiabetic glomerulosclerosis
Paraproteinemia Paraproteinemia /Amyloidosis/Amyloidosis
Lupus NephritisLupus Nephritis




Nephrotic SyndromeThromboembolic Complications
• Major hazard of the nephrotic syndrome• RVT( membranous GN) in 20-30% of adult
patients, 10% are symptomatic: flank pain, gross hematuria
• Pulmonary emboli(Silent)• DVT(frequent)• Arterial thrombosis is less common• Prophylaxis : Albumin< 2 gr, Uprotein>10
gr/d. decreased level of antithrombin III, Increased fibrinogen, Hypovolemia


Nephrotic SyndromeInfections
• Decreased levels of immunoglobulin IgG
• Decreased the alternative complement factor B
• Pneumococcal peritonitis
• Recurrent Cellulitis

General ManagementGeneral Management
Edema - salt restriction, diureticsEdema - salt restriction, diuretics Hyperlipidemia - lipid lowering agentsHyperlipidemia - lipid lowering agents ACE/ARB - ACE/ARB -
– decrease Pgc and decrease proteinuriadecrease Pgc and decrease proteinuria– Renal protectiveRenal protective
Hypercoagulable - ASAHypercoagulable - ASA Specific treatment based on biopsySpecific treatment based on biopsy



Minimal Change DiseaseMCD
Introduction and Definition

Minimal Change DiseaseMinimal Change Disease
Pathogenesis - unknown, most likely Pathogenesis - unknown, most likely autoimmuneautoimmune
TreatmentTreatment– 85% respond to steroids85% respond to steroids– If resistant to steroid may require If resistant to steroid may require
cyclophosphamidecyclophosphamide

Minimal Change Nephropathy(MCD)
• Minimal change disease (MCD) :is defined by the absence of histologic glomerular abnormality, other than evidence of epithelial cell foot process fusion (EM).
Minimal Change DiseaseMCD
Pathology

Minimal Change Disease
Nephrotic SyndromeMinimal Change Disease
• Is the major cause of the nephrotic syndrome in children(85-90%) and 10% in adults
• Malignancies account for 10% of cases of idiopathic nephrotic syndrome in adults
• LM: Normal glomeruli• EM: Fusion of the epithelial cell foot
Processes ( KNB).

Minimal Change DiseaseMCD
Etiology and Pathogenesis

Minimal Change Disease
• Idiopathic
• Secondary: Malignancy
Drugs
Infections


Minimal Change DiseaseMCD
Clinical manifestations

Minimal Change NephropathyMCD
• Patients with Minimal change disease present with edema that develops over a short period of time, with fluid retention exceeding 3% of the body weight.
• Up to two-thirds of presentation and relapses follow an infection, most commonly upper respiratory tract infection.

Minimal Change Nephropathy
• Clinical Feature: Heavy proteinuria, low serum albumin, edema formation and elevated serum cholesterol.
• Normal urinary sediment• Normal C3, C4• Negative ANA and Cryoglobulins• MCD patients are at risk of venous
thromboembolism.• Hypovolemia and ARF, especially patients
with diuretic therapy.

Minimal Change Disease
Natural History

Minimal Change Disease
• There is a tendency for patients with MCD to run a relapsing-remitting course and this is more frequent in children.
• Long-term remission can be expected in 75% of initial responders who do not relapse within 6 months.
• MCD does not progress to Renal Failure

Membranous GN
Definition

Membranous Nephropathy(MN)
• Membranous Nephropathy is a glomerular disease in which immune deposits of IgG and complement components develop predominantly or exclusively on the subepithelial surface of the glomerular capillary wall.
• Deposition is associated with a marked increase in glomerular permeability to protein, which manifest clinically as nephrotic syndrome.
• The pathogenesis of human MN is not known.

Membranous Nephropathy
ETIOLOGY

Membranous NephropathyMembranous Nephropathy
Most common cause of idiopathic Most common cause of idiopathic nephrotic syndrome in Caucasian nephrotic syndrome in Caucasian adults.adults.
Heavy proteinuria is common. Heavy proteinuria is common. Hypertension and azotemia develops Hypertension and azotemia develops as disease progresses.as disease progresses.
Increased incidence of renal vein Increased incidence of renal vein thrombosis.thrombosis.

Membranous nephropathy
• 2nd most common cause of nephrotic syndrome in adults (~30%)
• Usually idiopathic• Associated with
– Autoimmune diseases
– Hepatitis B– Carcinoma– Drugs (eg
penicillamine, captopril, NSAID)
• Outcome very variable– 1/3 spontaneous remission– 1/3 partial remission or very
slow progression– 1/3 progressive renal
impairment• Higher incidence of
thromboembolism• Therapy very difficult

Membranous Nephropathy
• Idiopathic• Secondary GN:• Immunological: -SLE, MCTD -Sjogren Syndrome• Rheumatoid Arthritis• Neoplasms: -Ca of lung -Ca of breast, Kidney
• Non-Hodgin Lymphoma

Membranous Nephropathy
• Infectious: -Hepatitis B
-Malaria
-Schistosomiasis
• Medications: -NSAIDs, Gold, Penicillamine
-Capoten

Pathology
• The pathologic feature of MN evolve from the initial formation of subepithelial immune complexes of IgG and complement.
• Initial stage on EM ranging from minimal change with only small deposits( stage 1) through the evolution to thickened basement membrane with resolution of deposits (stage IV).


Membranous Nephropathy

Membranous Nephropathy
Clinical manifestation

Membranous Nephropathy
• Is the most common cause of the idiopathic nephrotic syndrome in adults(30-50%)
• Nephrotic Syndrome is the common presentation
• Hypertension 30%• In children: 50% spontaneous remission,
10% to ESRD• Stage 1 >>>good prognosis• Stage 4>>>>bad Prognosis

Membranous Nephropathy
Natural History and Prognosis

Membranous GN
• The prognosis of untreated MN is somewhat worse in adults: 20% will have progressed to ESRD at 5-10 years followup.
. Bad outcome: male, age>50, HTN, Pcr high at presentation.
• Recurrence after Renal Transplantation

Membranous Nephropathy
Treatment
Treatment• Steroides
• Cyclosporine
• Imuran
• Cyclophosphamide
• Chlorambucil
Treatment of Membranous Treatment of Membranous NephropathyNephropathy Rule of 1/3Rule of 1/3 1/3 – 1/3 –
Spontaneous remissionSpontaneous remission 1/3 – 1/3 – Partial remission / slow deteriorationPartial remission / slow deterioration1/3 – Progress to ESRD1/3 – Progress to ESRD
Steroids alone are not very effectiveSteroids alone are not very effective Methylprednisolone alternating with Methylprednisolone alternating with
chlorambucil, Methylprednisolone alternating chlorambucil, Methylprednisolone alternating with cyclophosphamide.with cyclophosphamide.
CyclosporinCyclosporin

Focal Segmental Glomerulosclerosis
Introduction and Definition

Focal Segmental Glomerulosclerosis
Etiology and Pathogenesis

Focal Segmental Glomerulosclerosis (FSGS)
• Primary (Idiopathic)
• Secondary: -Sickle cell disease
-Heroin Nephropathy
-Morbid obesity
-HIV Nephropathy
-Aging Kidney
-Vesico-Ureteral Reflux
- Pamidronate

FSGS
• Most common idiopathic nephrotic syndrome in adults (33%)
• Increasing incidence
• More common in blacks
• Treatment very difficult

Focal Segmental Focal Segmental GlomerulosclerosisGlomerulosclerosis
Most common primary renal disease in Most common primary renal disease in African-AmericansAfrican-Americans
Etiology:Etiology:IdiopathicIdiopathicDrugs – Intravenous heroinDrugs – Intravenous heroinInfections – HIVInfections – HIVOthers – reflux nephropathy, obesityOthers – reflux nephropathy, obesity
Patient usually hypertensive. Usually Patient usually hypertensive. Usually progresses to ESRD over 5-20 years.progresses to ESRD over 5-20 years.

FSGS
Pathology

Focal Segmental Glomerulosclerosis (FSGS)
• FSGS is defined on histologic criteria by segmental capillary obliteration with increased mesangial matrix deposition, intracapillary hyaline deposits, and focal adhesions of the capillary tuft to Bowman’s capsule.
• Primary FSGS occur in patient with nephrotic syndrome in the absence of any of the known causes of secondary FSGS.



FSGS
Mild ModerateCollapsing
Normal
AssociationsIdiopathicMorbid obesityHeroin abuseHIV infectionNSAID(Minimal change disease)

FSGS
• In FSGS, evidence for a circulating factor is more substantial, mainly based on the high incidence of recurrence following transplantation, with heavy proteinuria developing sometimes within hours.
• Plasma exchange can lead to remission in tranplant recurrence of FSGS.

FSGS
Clinical Manifestations

FSGS
• Typically patients present with edema that develops over a short period of time.
• Very rapid onset of nephrotic syndrome• Microscopic hematuria 14-30%• Arterial Hypertension especially with
renal insufficiency.• Increased incidence pf venous
thromboembolism.
Focal Segmental Glomerulosclerosis
• Microscopic Hematuria• Proteinuria >>20-30 gram/daily• Both children and adults usually develops
ESRD 5-20 yrs from presentation.• Idiopathic FSGS may recur in the
transplanted kidney with severe proteinuria and Nephrotic Syndrome and rapid course to ESRD.

Collapsing FSGS
• Collapsing FSGS is a histologic variant of FSGS characterized by extensive focal or global glomerular capillary tuft collapse, podocyte hypertrophy and hyperplasia.
• Varying degree of tubulointerstitial injury.• African Americans• Severe nephrotic syndrome at presentation,
steroid resistance, and rapid developing ESRD (median time of 13 month).

FSGS-Treatment
• 1mg/kg Prednisone daily for 6 month
• PO Cyclosporine
• Cytotoxic Treatment (Cytoxan, Imuran)
• Symptomatic treatment with ACEI • CellCept (Mycophenolate Mofetil).

Nephrotic Syndrome
Secondary To Systemic Disease
• Diabetes Mellitus—Type I, Type II
• Amyloidosis

Diabetes Mellitus
INTRODUCTION

Diabetic Nephropathy
Diabetic Nephropathy is a common problem that is most likely to occur in patients who have worse glycemic control, Hypertension, glomerular hyperfiltration, Blacks, Mexican, or Pima Indian.

Diabetic Nephropathy
• Diabetic nephropathy is a leading cause of end-stage renal disease (ESRD) in Western societies
• Diabetic nephropathy is a clinical syndrome characterized by persistent albuminuria(>300 mg/24hr or >200ug/min) on at least two occasions separated by 3-6 months.
• Patients invariably develop hypertension, progressive increase in proteinuria, and decline in GFR.

Diabetic Nephropathy
Major Risk Factors For DN
1 .Genetic Susceptibility
2 .Arterial Hypertension
3 .Increased glomerular filtration rate
4 .Worse Glycemic Control
5 .Blacks, Pima Indian

Microalbuminuria
. Increased protein excretion is the earlies clinical finding of diabetic nephropathy.
• The normal rate of albumin excretion is less than 20 mg/day; persistent values between 30 and 300 mg/day( 20 to 200 ug/min) in a patient with diabetes is called Microalbuminuria .

Microalbuminuria and correlation with DN
• Great attention to control of both hyperglycemia and hypertension (with ACEI) may also contribute to the apparent improvement in the course of the disease.
• Patient who progress are more likely to have higher HbA1c values and higher blood pressure than non progresses.
• The incidence of overt hypertension is approximately 15 to 25 percent in all patients with microalbuminuria and much higher as the patient progress to overt nephropathy.
Epidemiology
• Type 1 diabetic nephropathy, occur in 30-40% of patients with type 1 diabetes after 25-40 years with diabetes
• In type 2 diabetes, the cumulative incidence of nephropathy is similar to that seen in type 1 , 25% at 20 years after diagnosis.
• Since type 2 diabetes is 10-15 times more common than type 1, the prevalence of type 2 diabetic nephropathy is substantialy higher.

Renal Pathology
• The kidneys of patients with diabetes are, on average larger than those of nondiabetic control subjects(15%).
• Nodular glomerular intercapillary lesions, described by Kimmelsteil and Wilson.
• Diffuse glomerular lesion is more frequent than the nodular lesion, with an incidence of over 90% for patients with type 1 DM of over 10 years duration and an incidence of 25-50% in patients with type 2 DM.

Diabetic Nephropathy

Diabetic NephropathyDiabetic Nephropathy
Most common cause of nephrotic syndrome Most common cause of nephrotic syndrome in adults.in adults.
Leading cause of ESRD in USALeading cause of ESRD in USA 30% of patients with Type I and 20% of 30% of patients with Type I and 20% of
patients with Type II DM develop diabetic patients with Type II DM develop diabetic nephropathy.nephropathy.
Initially microalbuminuria followed by heavy Initially microalbuminuria followed by heavy proteinuria and decline in renal function.proteinuria and decline in renal function.
Diagnosis usually made on clinical grounds Diagnosis usually made on clinical grounds and biopsy not needed.and biopsy not needed.
Diabetic Nephropathy
Clinical Manifestations and Natural History


Treatment of Diabetic NephropathyTreatment of Diabetic Nephropathy
Blood glucose controlBlood glucose control Control of hypertensionControl of hypertension Use of ACE inhibitors/ARBsUse of ACE inhibitors/ARBs Control of hyperlipidemiaControl of hyperlipidemia Smoking cessationSmoking cessation Protein RestrictionProtein Restriction
Nephrotic Syndrome
Secondary To Systemic Disease: Amyloidosis
-Primary Amyloidosis
-Secondary Amyloidosis

Amyloidosis
• The Amyloidosis are a group of disorders in which soluble proteins aggregate and deposit extracellulary in tissues as insoluble fibrils, causing progressive organ dysfunction. The kidney is one of the most frequent sites of amyloid deposition in AA, AL, and several of the hereditary amyloidoses.

Amyloidosis
• Amyloidosis is defined by the ability of a variety of proteins to form B-pleated sheets. These fibrils can be identified on biopsy specimens both by their characteristic appearance on electron microscopy and by their ability to bind Congo Red(leading to green birefringence under polarized light) and thioflavine-T (producing an intense yellow-green fluorescence).


Amyloidosis
• Amyloid A in secondary amyloidosis
• Immunoglobulin light chains in primary amyloidosis
• B2-microglobulin in dialysis-patients associated arthropathy
• Amyloid beta protein in Alzheimer’s disease

Amyloidosis
• Renal involvement occurs in over 90% of patients with either primary or secondary amyloidosis.
• Primary forms(> 90%) is a plasma cell dyscrasia and may be associated with MM.
• Light Chain Deposition Disease (LCDD) is a disorder of similar pathogenesis. The abnormal protein do not form the B-pleated amyloid fibrils.
• Secondary amyloidosis is a consequence of chronic inflammatory diseases such as : Rheumatoid arthritis, FMF, Osteomyelitis, Hypernephroma, PID.

Amyloidosis-Secondary
• Clinically evident renal involvement occurs only in primary or secondary amyloidosis
• Secondary amyloidosis is associated with increased hepatocyte production of the acute phase reactant serum amyloidosis A (SAA); this process may be stimulated by the release of cytokines ( Interleukin-1) from activated macrophages. Cleavage in circulating monocyte/macrophages results in the generation of smaller fragments, called AA protein, that can then deposit in the tissue.

Primary Amyloidosis (AL)
• The fibrils in AL consist of segments of the variable portions of monoclonal light chains
• AL Amyloidosis is a plasma cell dyscrasia in which the malignant characteristic of M.M are usually absent and circulating light chains are frequently demonstrated .
• Only a minority of patients who produce an excessive amounts of light-chains (as M.M) develop amyloidosis.
• Lambda light-chains are much more likely to produce amyloidosis than Kappa light chains.

DysproteinemiaDysproteinemia
Myeloma Cast NephropathyMyeloma Cast Nephropathy– Path shows multiple intraluminal Path shows multiple intraluminal
proteinaceous castsproteinaceous casts– PathogenesisPathogenesis
Disorder of plasma cells with overproduction Disorder of plasma cells with overproduction the antibody light chain the antibody light chain
– TreatmentTreatment Hydration, plasmapheresis to remove the Hydration, plasmapheresis to remove the
abnormal protein and chemotherapy to abnormal protein and chemotherapy to suppress plasma cellssuppress plasma cells

Myeloma Cast NephropathyMyeloma Cast Nephropathy

Light Chain Deposition DiseaseLight Chain Deposition Disease
Amyloid protein produced in plasma Amyloid protein produced in plasma cell dyscrasias is preferentially lamda cell dyscrasias is preferentially lamda light chainslight chains
Kappa chain can occur and termed Kappa chain can occur and termed light chain deposition diseaselight chain deposition disease
Kappa chain deposits tend to deposit Kappa chain deposits tend to deposit in tubules and glomeruli, spare vesselsin tubules and glomeruli, spare vessels
Kappa more aggressive than lambdaKappa more aggressive than lambda
Diagnosis
• Documentation of tissue deposition of amyloid fibrils.
• Kidney biopsy> 90% of patients• Abdominal fat pad> 80-90%• Rectal> 50-80%• Gingival>60%• Once the DX of primary amyloidosis is made,
the patient should be evaluated for M.M ! ! !

Pathology
• On light microscopy> >>Diffuse deposition of amorphous hyaline material in the mesangium and then capillary loops.
• Amyloid deposition in the glomeruli can result in the formation of nodules.
• Congo Red induces green birefringence when viewed under polarized light.
• Immunofluorescence for immunoglobulin and complement is negative.
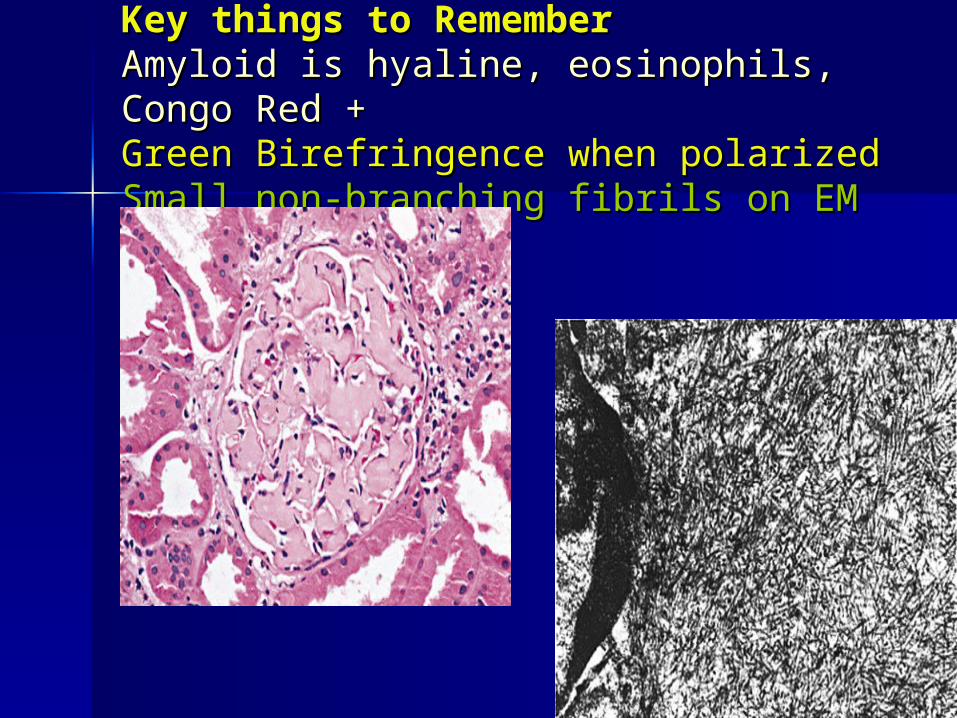
Key things to RememberKey things to RememberAmyloid is hyaline, eosinophils, Congo Red +Amyloid is hyaline, eosinophils, Congo Red +Green Birefringence when polarizedGreen Birefringence when polarizedSmall non-branching fibrils on EMSmall non-branching fibrils on EM



Amyloidosis
• More common in elderly• Two main types of renal amyloid
– AL amyloid– AA amyloid
Normal

Clinical Presentation
• Non-specific symptoms, Fatigue, Weight loss, Anemia
• Proteinuria, edema>>>Nephrotic Syndrome• Carpal tunnel syndrome• Peripheral neuropathy• Hepato-Splenomegaly, Macroglossia• Renal insufficiency• Tubular involvement : RTA, NDI, Hyperkalemia

Course and Treatment
• Prognosis depend on type of amyloidosis• MM= bad Prognosis• In primary Amyloidosis usually progress slowly
to CRF• Prednisone an Melphalan is the major mode of
therapy for primary amyloidosis• Colchicine in AL, AA amyloidosis• In AA the progression depend upon the ability to
control the underlying disease.

Asymptomatic Non-Nephrotic Proteinuria
• Overflow Proteinuria: Multiple Myeloma
-Light Chain
• Tubular Proteinuria: Tubulointerstitial dis.
< 2 gr/day
• Glomerular proteinuria

Treatment
• Steroid Treatment induces remission in almost all patients with MCD.
• Adults usually biopsied before treatment (KNB).
• Controll first volume overload (Diuretics).
Treatment
• Steroid responsive
• Steroid dependent
• Frequent relapsers