disclaimer practical molecular testing in surgical pathologylabmed.ucsf.edu/uploads/319/153... ·...
TRANSCRIPT
5/26/2011
1
1
Practical Molecular Testing in Surgical Pathology
Martin P Powers, MDUCSF Pathology and Laboratory
Medicine28 May 2011
2
Disclaimer
• I am one of the directors of the Molecular Diagnostics Lab at UCSF
• The lab and medical center may receive revenue from some of the testing hereafter described.
3
Some assumptions
• Know that DNA, RNA and protein exist• Know that DNA is transcribed into RNA,
which is then translated into protein• Know that techniques like PCR, DNA
sequencing and FISH exist– To be explained in more detail later
4
Outline (approximate)
• Oncogenes and Tumor Suppressors• Detecting clinically relevant mutations in
oncogenes and tumor suppressors– Large DNA rearrangements
• FISH, RT-PCR, LOH, etc
– Small DNA mutations• PCR, sequencing, etc.
• Technical issues• We can only scratch the surface in 45 min

5/26/2011
2
5
Introduction to oncogenes and tumor suppressors
6
Hallmarks of Cancer
• Genes that promote these hallmarks– ONCOGENES– accelerators– Mutations “switch them
on”
• Genes that inhibit these hallmarks– TUMOR
SUPPRESSORS– “brakes”– Mutations “knock them
out”
Cell. 2000 Jan 7;100(1):57-70
7
Oncogenes and tumor suppressors
• Oncogenes– Promote cell division/invasion or Inhibit
apoptosis (cell death)
– Gain of function mutation
– Dominant mutation• Only one allele mutated (usually) to promote
tumorigenesis• Wild type copy can still be present
8
Somatic mutations and oncogenes
• Mutation in oncogene is only in tumor cells– (sporadic tumors)
• Surrounding stroma, inflammatory and all other cells are wild-type.
Cells of body don’t have mutation
Cells of tumor only have mutation

5/26/2011
3
9
Somatic mutations and oncogenes
Chromosome with oncogenic mutation
Wild-type (normal) chromosome
10
Oncogenes
– Mechanisms• Amplification• Overexpression by translocation• Mutation, hyperactivation
– Translocation– Point mutation
– Types of Genes• Growth Factors• Growth Factor Receptors• Signal Transducers• Transcription factors• Cyclins and Cyclin dependant kinases• Anti-apoptotic molecules
11
Growth factors, signal transduction and the cell cycle
Robbins & Cotran Pathologic Basis of Disease Online12
Tumor suppressors
• Tumor suppressors– Gatekeepers (direct)
• Inhibit cell division• Promote apoptosis
– Caretakers• Protect the genome (DNA
repair)• Indirect: Increase
mutations in oncogenes and gatekeepers
Robbins & Cotran Pathologic Basis of Disease Online

5/26/2011
4
13
Tumor suppressors• Mechanisms
– Point mutations– Deletions – silencing of gene expression (or combo for each
copy)
• Types of genes– Inhibitory growth receptors/ligands– Pro-apoptotic molecules– Cell adhesion molecules– Inhibitors of signal transduction– Cell cycle inhibitors– Sensors or enzymes for DNA repair
14
Growth factors, signal transduction and the cell cycle
Robbins & Cotran Pathologic Basis of Disease Online
15
Tumor suppressor genes
• Must be inactive to promote tumorigenesis (lose your brakes)
• Recessive mutations• Must lose both copies in the tumor
– Knudson’s two-hit hypothesis– Inherit the first mutation in inherited cancer
syndromes• Often one of the copies is lost through a “loss of
heterozygozity” whereby the entire chromosome, or chromosome arm, or large deletion deletes one of the copies, while a point mutation (or other small mutation) was on the other copy.
16
Knudson’s two hit hypothesis
Human Molecular Genetics 2Strachan, Tom and Read, Andrew P.New York and London: Garland Science; c1999
5/26/2011
5
17
Somatic vs inherited genetics (for tumor suppressor genes)
• Inherited • Somatic (sporadic)Rb mutation
All cells of body inherit one mutation-Predisposition to RB = familial retinoblastoma- dominant inheritance
Two Mutations acquired in postnatal life in same cell;two mutations required for tumor;- Cellular recessive
Some cells get second hit (somatic)- Retinoblastoma tumor
18
Detecting clinically relevant oncogene mutations
19
Amplification
• Examples– ERBB2 (HER2/neu)
• Worse prognosis in breast cancer• Candidate for anti-ERBB2 therapy (such as
trastuzumab) for breast, GU, stomach/GE cancer
– EGFR• Worse prognosis and diagnostic for GBM
– MYC (or MYCN)• Worse prognosis in neuroblastoma and
medulloblastoma
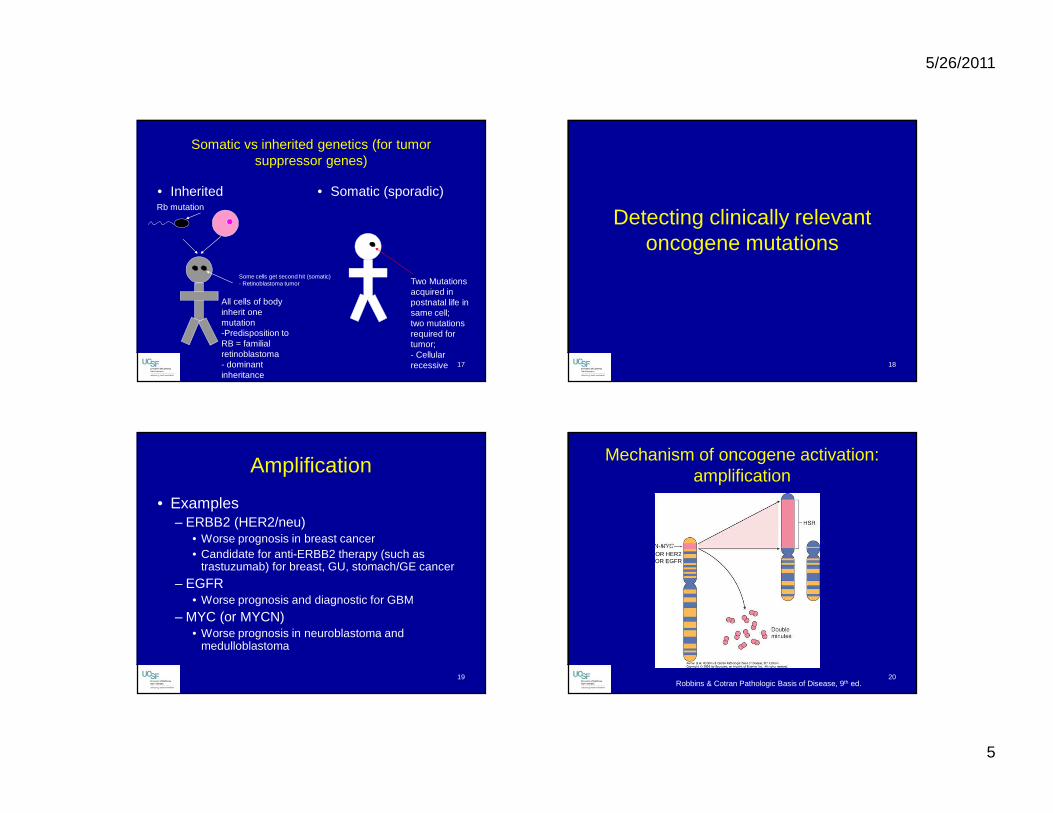
20
Mechanism of oncogene activation: amplification
OR HER2OR EGFR
Robbins & Cotran Pathologic Basis of Disease, 9th ed.
5/26/2011
6
21
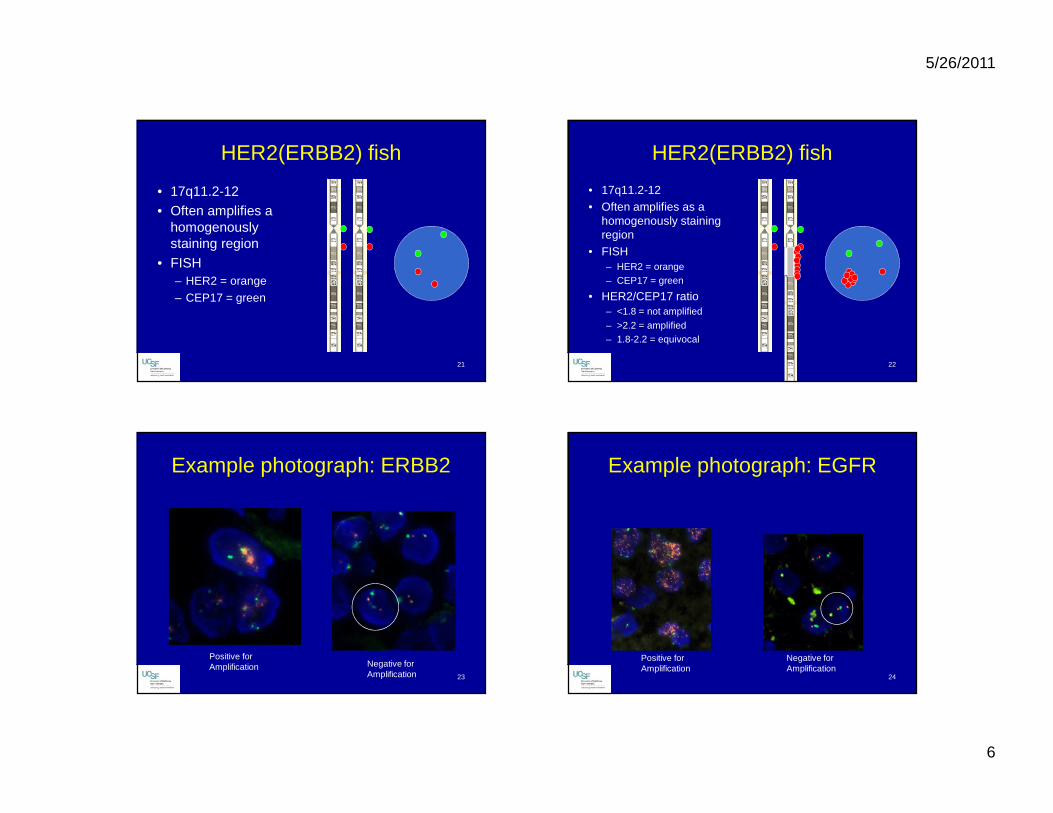
HER2(ERBB2) fish
• 17q11.2-12• Often amplifies a
homogenously staining region
• FISH– HER2 = orange
– CEP17 = green
22
HER2(ERBB2) fish
• 17q11.2-12• Often amplifies as a
homogenously staining region
• FISH– HER2 = orange– CEP17 = green
• HER2/CEP17 ratio– <1.8 = not amplified– >2.2 = amplified– 1.8-2.2 = equivocal
23
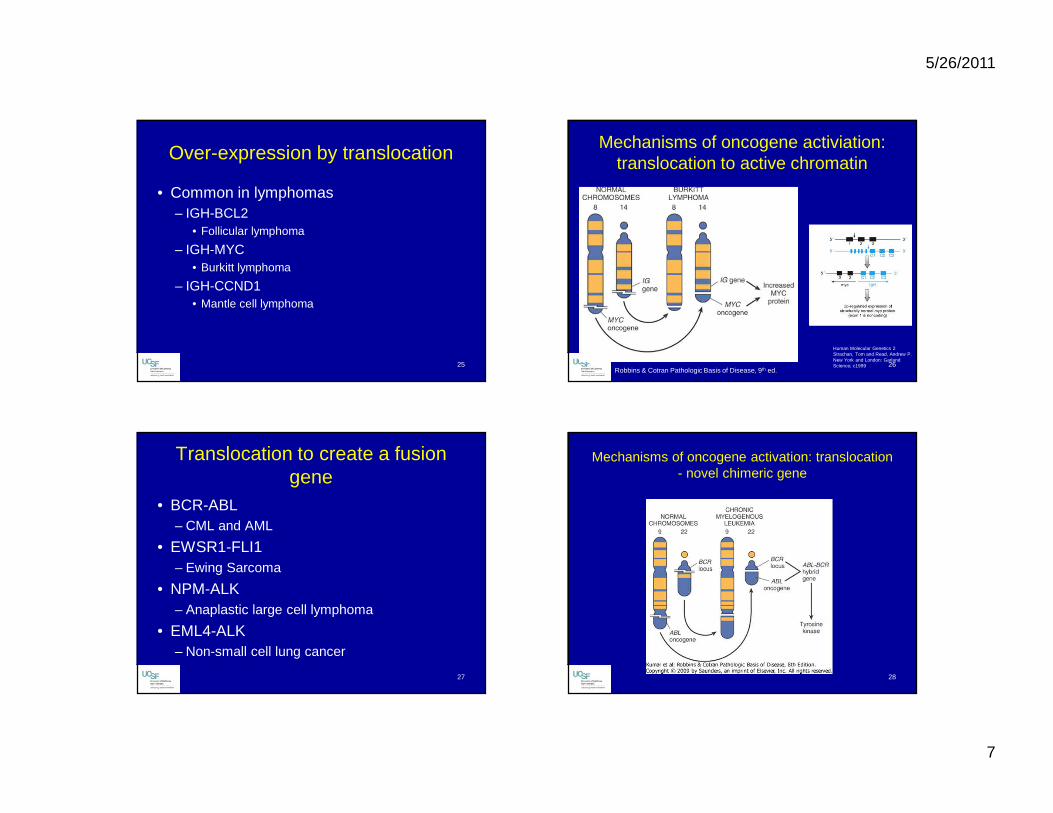
Example photograph: ERBB2
Positive for Amplification Negative for
Amplification 24
Example photograph: EGFR
Positive for Amplification
Negative for Amplification
5/26/2011
7
25
Over-expression by translocation
• Common in lymphomas– IGH-BCL2
• Follicular lymphoma
– IGH-MYC• Burkitt lymphoma
– IGH-CCND1• Mantle cell lymphoma
26
Mechanisms of oncogene activiation: translocation to active chromatin
Human Molecular Genetics 2Strachan, Tom and Read, Andrew P.New York and London: Garland Science; c1999
Robbins & Cotran Pathologic Basis of Disease, 9th ed.
27
Translocation to create a fusion gene
• BCR-ABL– CML and AML
• EWSR1-FLI1– Ewing Sarcoma
• NPM-ALK– Anaplastic large cell lymphoma
• EML4-ALK– Non-small cell lung cancer
28
Mechanisms of oncogene activation: translocation- novel chimeric gene
5/26/2011
8
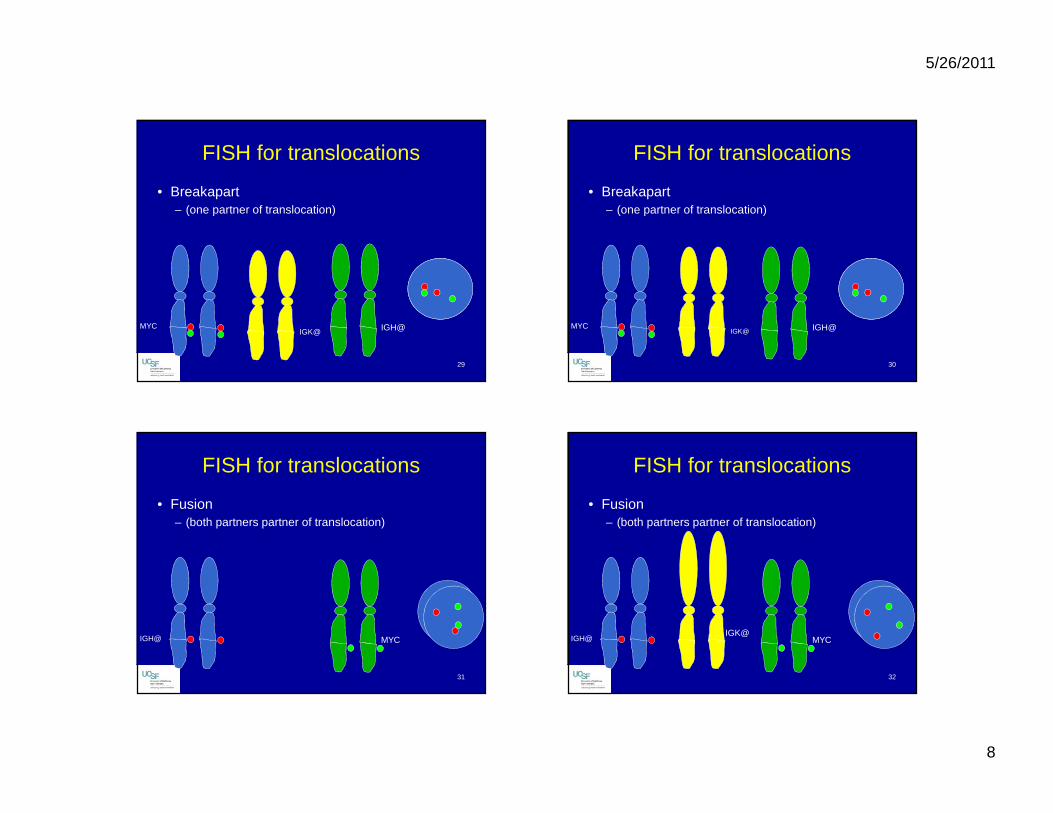
29
FISH for translocations
• Breakapart – (one partner of translocation)
MYCIGK@ IGH@
30
FISH for translocations
• Breakapart – (one partner of translocation)
MYCIGK@ IGH@
31
FISH for translocations
• Fusion – (both partners partner of translocation)
IGH@ MYC
32
FISH for translocations
• Fusion – (both partners partner of translocation)
IGH@IGK@
MYC
5/26/2011
9
33
FISH advantages
• Visualize tumor cells separate from normal cells
• Small tumor samples can be studied• Visualize any heterogeneity in the tumor
34
PCR for translocations
• Over-expression translocations– No fusion transcript
– Must do DNA PCR• Sensitivity depends on spacing of breakpoints
• Fusion translocations– Fusion transcript– Allows for RT-PCR
35
What is PCR
• Exponential amplification of DNA based on sequence specific primers– Amplify specific sequence between the
primers
• If you start with RNA– RT-PCR– RT (Reverse Transcription) step first converts
RNA to cDNA and then you amplify like PCR
36
5/26/2011
10
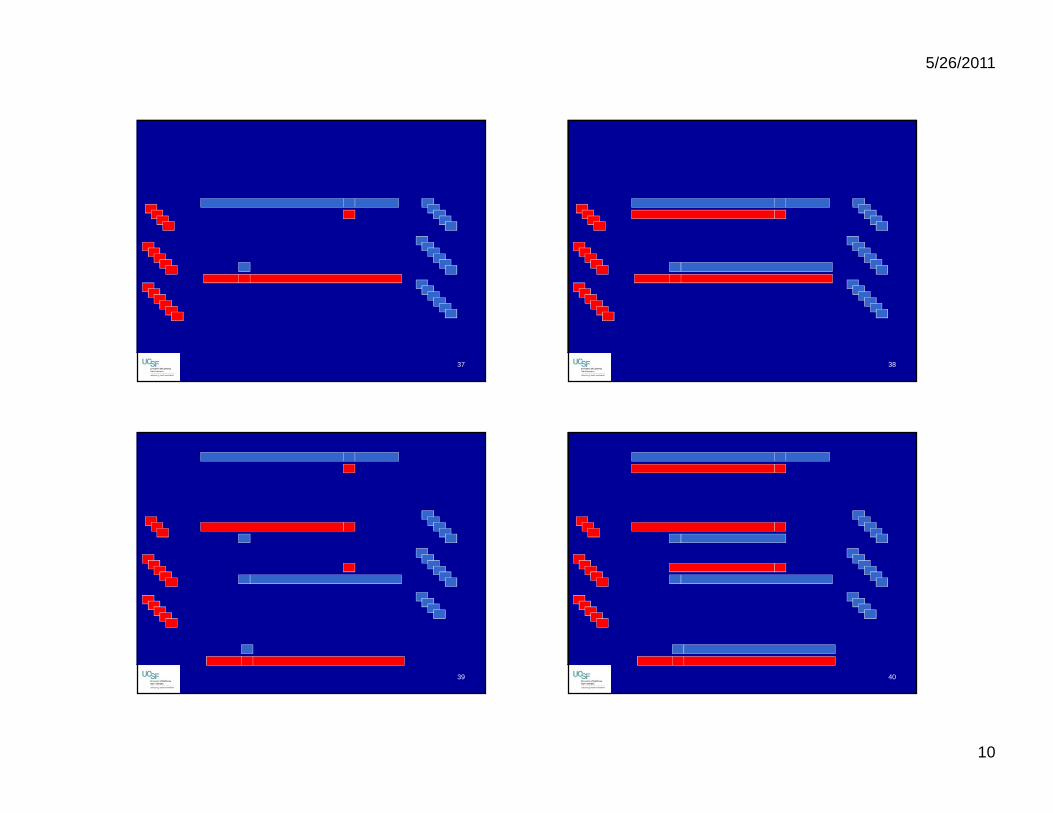
37 38
39 40
5/26/2011
11
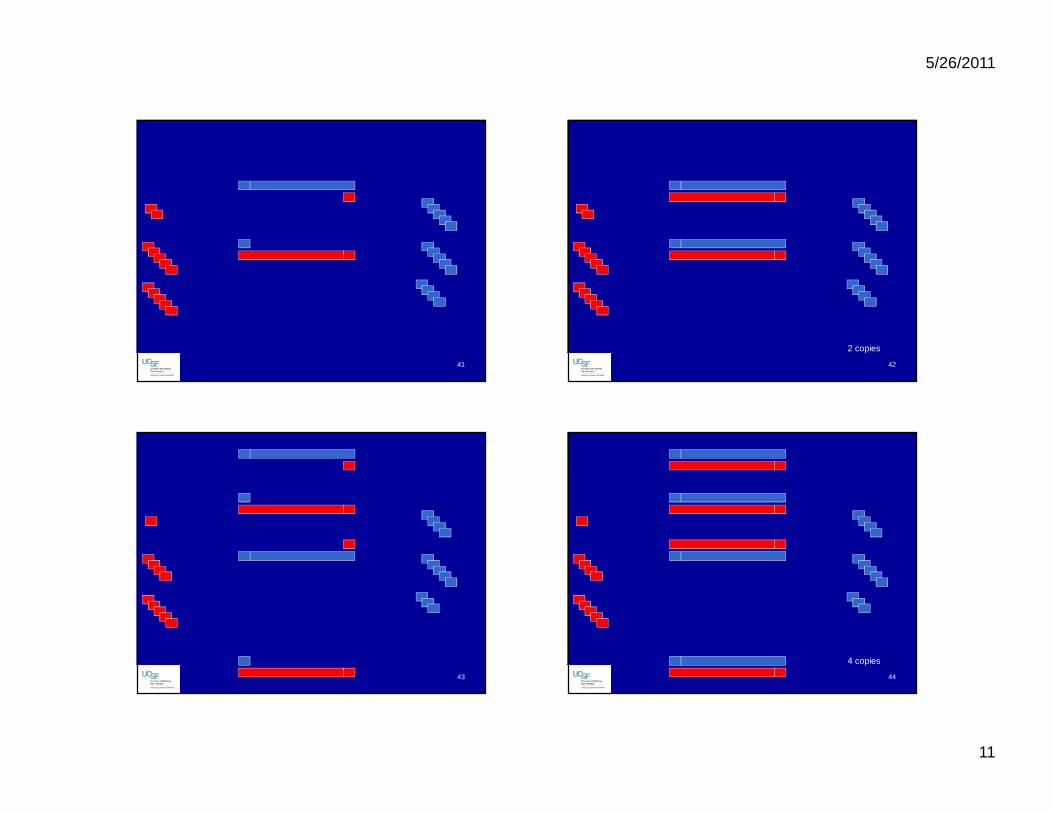
41 42
2 copies
43 44
4 copies
5/26/2011
12
45 46
8 copies
47
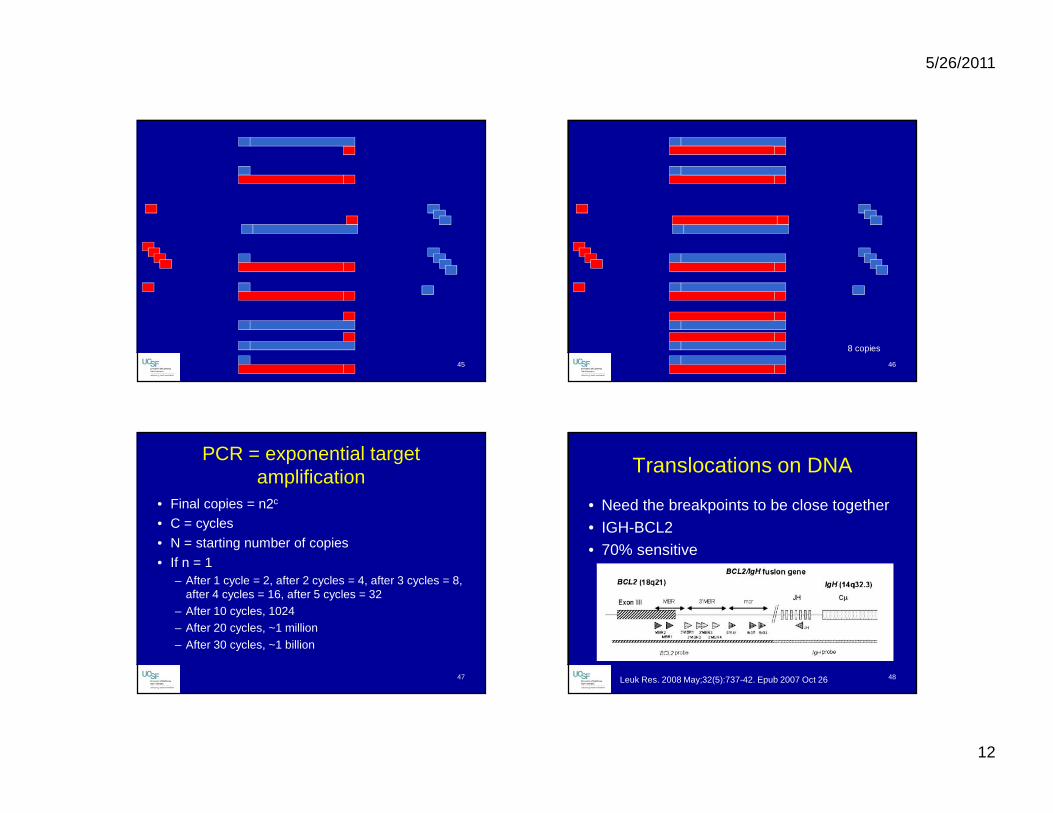
PCR = exponential target amplification
• Final copies = n2c
• C = cycles
• N = starting number of copies
• If n = 1– After 1 cycle = 2, after 2 cycles = 4, after 3 cycles = 8,
after 4 cycles = 16, after 5 cycles = 32– After 10 cycles, 1024– After 20 cycles, ~1 million
– After 30 cycles, ~1 billion
48
Translocations on DNA
• Need the breakpoints to be close together• IGH-BCL2• 70% sensitive
Leuk Res. 2008 May;32(5):737-42. Epub 2007 Oct 26

5/26/2011
13
49
Translocations on RNA
• Advantage of exon specific primers• BCR-ABL
Adapted from Genes Chromosomes Cancer. 2001 Oct;32(2):97-111 50
Activating point mutations in oncogenes
• KRAS– Resistance to EGFR therapy in colorectal
carcinoma
• BRAF– Resistance to EGFR therapy (colon),
candidate for BRAF therapy (melanoma)
• EGFR– Response to EGFR therapy in lung cancer
51
How many mutations are there
• COSMIC– Catalogue of somatic mutations in cancer
– Database of literature reported mutations in cancer in different genes
– http://www.sanger.ac.uk/genetics/CGP/cosmic/
52
BRAF in COSMIC
5/26/2011
14
53
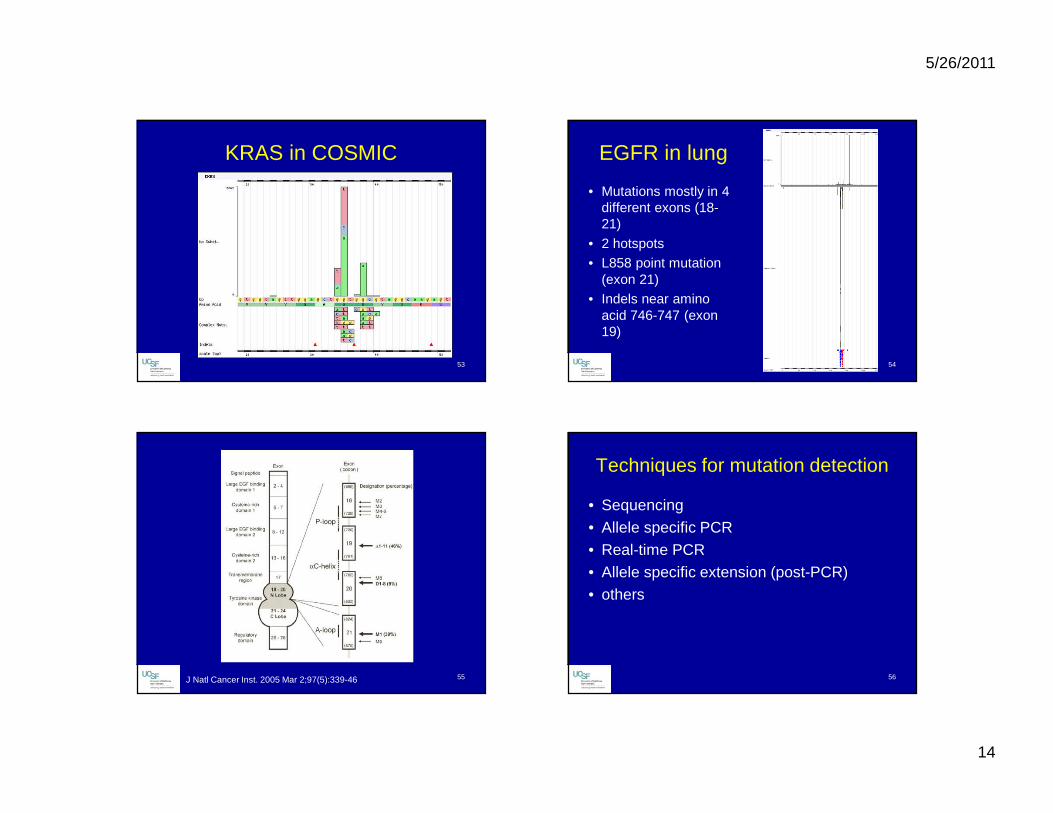
KRAS in COSMIC
54
EGFR in lung
• Mutations mostly in 4 different exons (18-21)
• 2 hotspots• L858 point mutation
(exon 21)• Indels near amino
acid 746-747 (exon 19)
55J Natl Cancer Inst. 2005 Mar 2;97(5):339-46 56
Techniques for mutation detection
• Sequencing• Allele specific PCR• Real-time PCR• Allele specific extension (post-PCR)• others

5/26/2011
15
57
Issues to consider for mutation testing
• Analytical sensitivity– How much DNA is needed?
• Total amount of DNA, and therefore specimen required
• 1ng of DNA represents about 330 diploid cells• 1 diploid genome is about 6.6 pg of DNA
– How many % mutant copies need to be present to detect a mutant signal?
58
% mutant burden
• DNA Sequencing• Analytic Sensitivity ~20%
•50% mutant alleles•20% mutant allele
59
To dissect or not to dissect
12 tumor cells, 8 lymphocytes: 30% mutant allele burden 60
To dissect or not to dissect
12 tumor cells, 8 lymphocytes, 50 fibroblasts and endothelial cells: 8.5% mutant burden, but can dissect a discreet tumor mass with less normal cells

5/26/2011
16
61
To dissect or not to dissect
12 tumor cells, 8 lymphocytes, 50 fibroblasts and endothelial cells: 8.5% mutant burden, but no discreet tumor mass
62
Important things to think about
• Analytical sensitivity and whether or not your lab dissects
• Choice of mutations that will be tested for– Is the panel comprehensive enough for your
clinicians need
• Fixative
63
Effects of Fixative on DNA
• Buffered formalin– Damages DNA, but not as bad as unbuffered formalin
which will nearly totatlly degrade DNA
• Alcohol based fixatives– Good preservation of DNA
• B5, Bouin, Zenkers– Very bad for DNA
• Decalcification– Strong acids are very bad for DNA
64
Testing for tumor suppressors
• DNA sequencing• Loss of functions mutations• May be anywhere in gene

5/26/2011
17
65
Test for loss of other copy of gene
• Deletion/Absence of other copy by FISH• LOH of polymorphic markers in
neighborhood of gene
66
Deletion testing by FISH: 1p/19q
• Good prognosis and prediction of chemotherapeutic response
• Actual tumor suppressors not cloned yet• Tend to delete the entire 1p and 19q
chromosome arms
67
1p/19q FISH
68
1p/19q FISH
5/26/2011
18
69
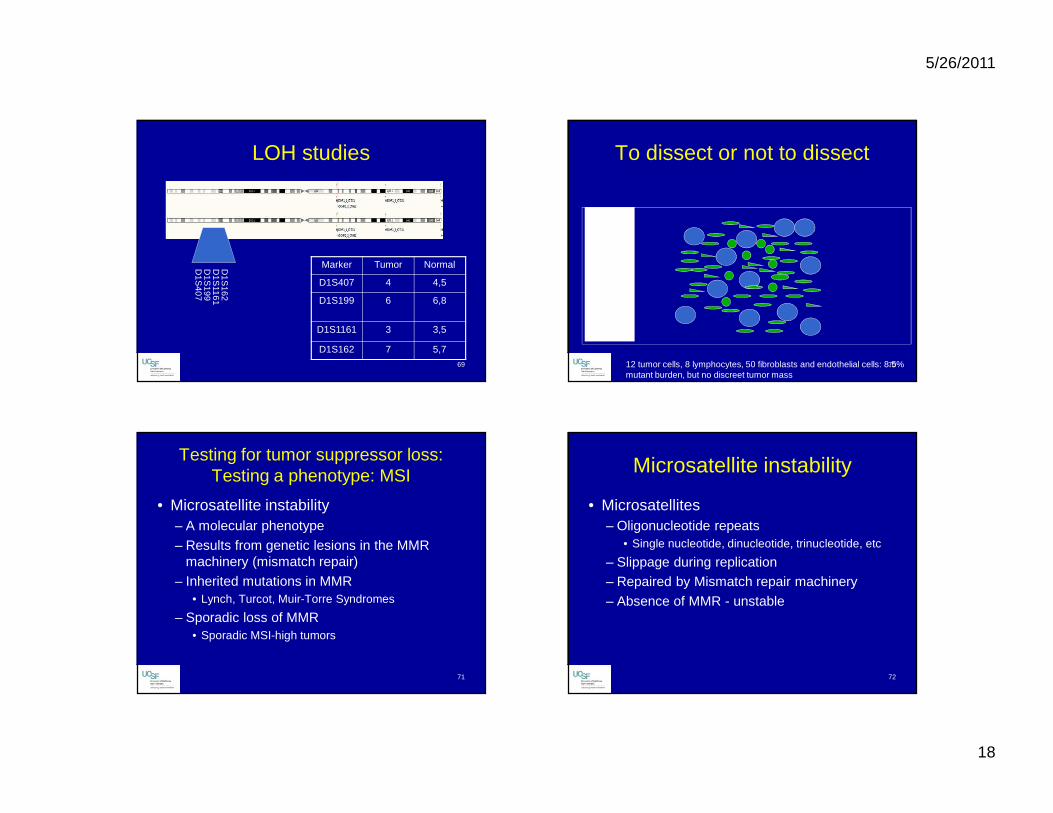
LOH studies
D1S
407D
1S199
D1S
1161D
1S162
Marker Tumor Normal
D1S407 4 4,5
D1S199 6 6,8
D1S1161 3 3,5
D1S162 7 5,7
70
To dissect or not to dissect
12 tumor cells, 8 lymphocytes, 50 fibroblasts and endothelial cells: 8.5% mutant burden, but no discreet tumor mass
71
Testing for tumor suppressor loss: Testing a phenotype: MSI
• Microsatellite instability– A molecular phenotype
– Results from genetic lesions in the MMR machinery (mismatch repair)
– Inherited mutations in MMR• Lynch, Turcot, Muir-Torre Syndromes
– Sporadic loss of MMR• Sporadic MSI-high tumors
72
Microsatellite instability
• Microsatellites– Oligonucleotide repeats
• Single nucleotide, dinucleotide, trinucleotide, etc
– Slippage during replication– Repaired by Mismatch repair machinery
– Absence of MMR - unstable
5/26/2011
19
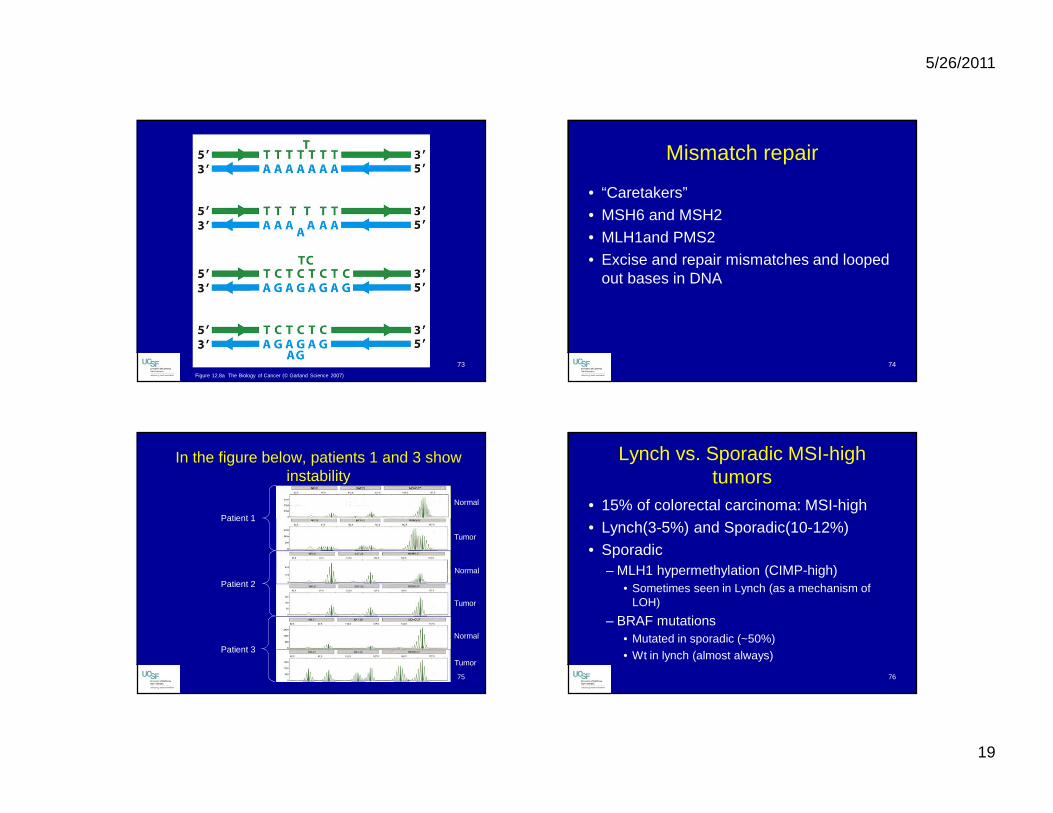
73
Figure 12.8a The Biology of Cancer (© Garland Science 2007)
74
Mismatch repair
• “Caretakers”• MSH6 and MSH2• MLH1and PMS2• Excise and repair mismatches and looped
out bases in DNA
75
In the figure below, patients 1 and 3 show instability
Patient 1
Patient 2
Patient 3
Normal
Tumor
Normal
Tumor
Normal
Tumor
76
Lynch vs. Sporadic MSI-high tumors
• 15% of colorectal carcinoma: MSI-high• Lynch(3-5%) and Sporadic(10-12%)• Sporadic
– MLH1 hypermethylation (CIMP-high)• Sometimes seen in Lynch (as a mechanism of
LOH)
– BRAF mutations• Mutated in sporadic (~50%)• Wt in lynch (almost always)
5/26/2011
20
77
Thank you for listening
Any Questions?
78
References• "Catalogue of Somatic Mutations in Cancer." Retrieved April
25, 2011, from http://www.sanger.ac.uk/genetics/CGP/cosmic/.
• Coleman, W. B. and G. J. Tsongalis (2006). Molecular diagnostics : for the clinical laboratorian. Humana Press, Totowa, N. J.
• Espinet, B., B. Bellosillo, et al. (2008). "FISH is better than BIOMED-2 PCR to detect IgH/BCL2 translocation in follicular lymphoma at diagnosis using paraffin-embedded tissue sections." Leuk Res 32(5): 737-742.
• Hanahan, D. and R. A. Weinberg (2000). "The hallmarks of cancer." Cell 100(1): 57-70.
• Hunt JL (2008) “Molecular Pathology in Anatomic Pathology Practice: A Review of Basic Principles.” Arch Pathol Lab Med 132(2): 248-260
79
References
• Kumar, V., A. K. Abbas, et al., Eds. (2010). Robbins and Cotran Pathologic Basis of Disease, Saunders Elsevier.
• Shigematsu, H., L. Lin, et al. (2005). "Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers." J Natl Cancer Inst 97(5): 339-346.
• Strachan, T. and A. P. Read (1999). Human Molecular Genetics, Wiley.
• Wang, Y. L., A. Bagg, et al. (2001). "Chronic myelogenous leukemia: laboratory diagnosis and monitoring." Genes Chromosomes Cancer 32(2): 97-111.
• Weinberg, R. A. (2007). The biology of cancer. New York, Garland Science.