diffuse ventricular fibrosis is a la te outcome of...
TRANSCRIPT

DOI: 10.1161/CIRCEP.113.000515
1
Diffuse Ventricular Fibrosis is a Late Outcome of Tachycardia-Mediated
Cardiomyopathy Following Successful Ablation
Running title: Ling et al.; Diffuse Ventricular Fibrosis Post-TMC
Liang-han Ling, MBBS1,2; Jonathan Kalman, MBBS, PhD2; Andris Ellims, MBBS1; Leah Iles,
MBBS1; Caroline Medi, MBBS, PhD1,2; Craig Sherratt, BAppSc1; David Kaye, MBBS, PhD1,2;
James Hare, MBBS, PhD1; Peter Kistler, MBBS, PhD1; Andrew Taylor MBBS PhD1
1Alfred Hospital and Baker IDI Heart and Diabetes Institute; 2Royal Melbourne Hospital and
Faculty of Medicine, Dentistry, and Health Sciences, University of Melbourne, Australia
Correspondence:
Prof Jonathan Kalman
Royal Melbourne Hospital
Victoria, 3050
Australia
Tel: +61 3 9349 5400
Fax: +61 3 9349 5411
E-mail: [email protected]
Journal Subject Codes: [5] Arrhythmias, clinical electrophysiology, drugs, [104] Structure, [105] Contractile function, [30] CT and MRI
Ellims, MBBS ; LeLeahaa
avid KaKaKaKayeyeyeye,, MBMBMBMBBSBSBSBS, , ,, PPPhPh
es Hare MBBS PhD1 P t Ki tl MBBS PhD1 A d T l MBBS PhD1
H l
y l
es HaaHarerere,, MBMBMBBSSSBS, PhD1; Peter Kistler, MBBBBSBSBS, PhD1; Andrewwww Taylor MBBS PhD1
Hosssspipipipitatataal l anananandd dd BaBaBakekek r rrr IDIDIDI I HeHeHeHearrarart ttt andddd DiDiDiDiabababbetetetteseses IIInsnsnsnstititiitututututetetete; ;;; 2222RoRoRoRoyayayay ll MeMeMelblblblbouououournrnrnr eeee HoHoHospspsppittittalaa
y offff MMMedededediciciccinininne,e,e,, DDDDenenentititiistststryryry, ananana d HeHHeHealalalalthththh Sciciciienenencececees,ss UUUUnininin veveveersrsrr itititityy y ofofoff MMMMelelee bobobobourururnenenene, AuAuAuAusssts ral
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
2
Abstract
Background - Successful arrhythmia ablation normalizes ejection fraction (EF) in tachycardia-
mediated cardiomyopathy (TMC), but recurrent heart failure and late sudden death have been
reported. The aim of this study was to characterize the left ventricle (LV) of TMC patients long
after definitive arrhythmia cure.
Methods and Results - Thirty-three patients with a history of successfully ablated incessant focal
atrial tachycardia 64±36 months prior, and 20 healthy controls were recruited. At ablation, 18
patients had EF<50% (AT-Low EF) that recovered within 3 months from 37±12 to 56±4%
(p<0.001), while 15 patients had EF>55% (AT-Normal EF). No subjects had EF of 50% to 55%.
Subjects underwent echocardiography with speckle tracking and contrast-enhanced cardiac
magnetic resonance imaging (CMR) with ventricular T1 mapping as an index of diffuse fibrosis.
CMR was performed using a clinical 1.5-T scanner and 0.2 mmol/kg gadolinium-DTPA for
contrast. Subject characteristics were similar across the 3 groups. Compared to AT-Normal EF
patients and controls, AT-Low EF patients had lower EF (60±6 vs 64±4 and 65±4%, p<0.05),
greater indexed LV end-diastolic volume (102±34 vs 84±14 and 85±16 ml/m2, p<0.05), and
greater indexed LV end-systolic volume (41±11 vs 31±7 and 30±8 ml/m2, p<0.01) on CMR.
Compared to controls, AT-Low EF patients had reduced global LV corrected T1 time (442±53 vs
529±61, p<0.05) consistent with diffuse fibrosis.
Conclusions - TMC patients exhibit differences in LV structure and function including diffuse
fibrosis long after arrhythmia cure, indicating that recovery is incomplete.
Key words: tachyarrhythmia, ablation, magnetic resonance imaging, T1 mapping, cardiomyopathy
aaaastststst-eee-enhnhnhnhanananancecececed d d d cacacacardrdddiaiaiaiacccc
n indexexexe oooof f f f didididiffffffffususususe e e e fififf br
p o
u l
d 0
e d
e R
to controls, p g 1 (442±
perfrfrfrforororormememeed dd d uusininingg g a clinical 1.5-T scannerrr aaandn 0.2 mmol/ll kg ggggadaa olinium-DTPA fo
uuubbbjb ect characccteteterristststiciici s ss s wewewewerererer simimimimililillarr accroooss thhe 3333 grouououo psss. CoCoCompmpm arrrredededed to oo ATATATAT-N-N-NNorororrmmamm l
d cccononontrols,,, AAATT-Lowww EFFFF pppataa ieeentnnn s hhhah d loooweer EFFFF (6(6(60±00±0 6 vsvsvss 64±±44 anananand ddd 6555±4±4±4± %,%, p<0<0<0.0
exed dd LVLV endndndn -diasasastott lic vovovovolume (1(( 02±3±±± 4 4 vsvsvsvs 84±141414 and 85±5±5±±16 ml///l/mmmm2,, p<p<p<p 0.05),),, and
exedd d LVLVLV enddd---sysysys stt llolicii v lollume (4(4(4( 11±1 1111111 vs 313131±7±77 a ddndd 30±0±0±0 8888 mlll/m/m/mm2222,,, p<pp 00.00 0101011)))) onononon CCCCMR
ttoo cocontntrorolslsls, , ATATATAT-LoLLoL w w EFEFEFE papattttieiiei nttntntss hahhah d dd d rereduddud ceced dd d glgllloboboboballall LLLLV VV V cocorrrrecectetett d dd d TTTT111 titititimeme (4(44242± by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000515
3
Introduction
Tachycardia-mediated cardiomyopathy (TMC) is an important cause of reversible left ventricular
(LV) systolic dysfunction and may complicate supraventricular tachyarrhythmias.1, 2 Key
features include reduced global contractility, extracellular matrix remodeling, and LV chamber
dilatation. Severity of systolic impairment in TMC shows dependence on tachycardia rate and
duration.3-5 Successful rate or rhythm control results in normalization of ejection fraction (EF)
within weeks to months in the absence of concurrent causes of cardiomyopathy.1, 6-8
Despite good early outcomes, rapid deterioration of systolic function with tachycardia
recurrence and late sudden death have been reported, raising the possibility that LV myocardial
substrate remains diseased despite normalization of overall systolic function.8, 9 Large animal
models of tachypacing-induced heart failure show EF recovery following cessation of
tachypacing, but also reveal persistent LV dilatation accompanied by diffuse interstitial fibrosis,
reduced contractility, and impaired relaxation during the immediate recovery phase.10-13
Furthermore, a series of 24 TMC patients treated successfully for a variety of arrhythmias
demonstrated persistent LV dilatation up to 14 months following normalization of EF.6
Longer-term follow-up studies of TMC that characterize LV structure and function are
lacking, despite increasing availability of powerful imaging modalities such as cardiac magnetic
resonance (CMR). The long-term impact of incessant inappropriate tachycardia in subjects who
do not develop gross LV systolic dysfunction is unknown. In this study, we performed detailed
non-invasive assessment of LV function, morphology, and fibrosis, as well as clinical outcomes
in a cohort of patients with and without TMC in the setting of incessant focal atrial tachycardia at
a mean of 5 years following successful arrhythmia ablation.
nction with tachyhyycacacacardr
bilityy ttthhahah t ttt LVLVLVLV mmyoyooocccacar
e 8 9 m
t
g, but also reveal persistent LV dilatation accompanied by diffuse interstitial fibr
n
re a series of 24 Tf MC patients treated s ccessf ll for a ariet of arrh thmias
emamamamainininss didididiseseseaseeeeddd d despite normalization ofofff ovverall systolilic fuuunncnn tion.8, 9 Large anim
taaaachhhhypacing-inndduceeddd heeeararart faaaililillurrre showoww EFEFEF recccovovovovereere y fffoollowwingngg ccessaaatititt onono oof y
g, bubub tttt alalalsssso reveal lll pepersistentntntn LLLLV didididilalalalatataatititition accomomomompaaannnin edededed bbby y dididiifffff useeee ininininterstitititititiiallll ffffibiibibr
ntractilililiiti y,y,y andndndd iiimppp iaiiredd d rellal xa iition dddduriniii ggg hththhe iiimmedididid atattte recococooveryyy ppphahh se.1010101 -1313131
iri ff 2244 TTff MCMC tatiie tnt ttr ttedd fsf llll ff iiett ff hrh tthhmiia
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
4
Methods
Study Population
The study was performed at the Royal Melbourne Hospital and the Alfred Hospital in
Melbourne, Australia, and had Human Research Ethics Committee approval. Consenting patients
with a history of incessant focal atrial tachycardia (AT) and successful ablation between January
1997 and December 2011 were recruited. Patients with pre-existing LV dysfunction were
excluded. Patients were considered to have pre-existing LV dysfunction when cardiomyopathy
occurred in the context of known significant coronary artery disease, valvular heart disease,
congenital heart disease, or inherited cardiomyopathy; cardiomyopathy had been documented
before the onset of tachycardia; or the echocardiographic abnormalities were segmental or of a
pattern attributable to another cause. At the time of their ablation procedure, 18 patients had an
EF (AT-Low EF) while 15 patients an EF of 55% (AT-Normal EF), as determined by
Simpson’s biplane method on clinical echocardiography. No patients had an EF of 50% to 55%.
All 33 patients had incessant AT where tachycardia was defined by the presence of 10
consecutive tachycardia beats on 12-lead electrocardiogram or Holter monitor and incessant
tachycardia was defined as continuous tachycardia or continuous paroxysms of tachycardia
separated by 2 sinus beats.14 Following successful ablation, EF of all AT-Low EF patients (as
determined on clinical echocardiography) either recovered to >55% or made an absolute
improvement of at least 10% within 3 months, resulting in a clinical diagnosis of TMC. Success
of ablation was based on absence of recurrence on symptoms and repeated electrocardiographic
evaluation at 1, 3, 6 and 12 month follow-up visits and annually thereafter. Holter monitoring
was performed at 3, 6 and 12 month visits and thereafter if patients described symptoms. ACE-
inhibitor and -blocker therapy was not routinely prescribed following catheter ablation. A
valvular heart diseaeaeaasesess
y had ddd bebebb enen ddddococumummmeeenentt
o
r d
ents had incessant AT here tach cardia as defined b the presence of 10
onssssetetetet ooof ff tatatat chccc ycycyccaara dia; or the echocardiogrgrgrapapa hic abnormalaa itieieiess s were segmental or
ribbbbuuutu able to anottherrr ccaussseee. Atttt ttttheee ttime of tthheirr aablbllblatatata ionnn ppprocceeduuuree, 18888 ppap ttieentsss hhad
(ATATATAT-LoLoLoLow EFEFEFE )))) whhhilililile 15555 ppppaatatientttsss ananan EEEEFFFF ffoff 55555555%%% % (((ATATATAT-NoNoNoNormal EEEEFFFF)))), as ddd ttetermiiiin
biplplplane methththodododo on cllliiinicii allll echhhhocardididid ogggraphphphhyyy. NNNoN pppattieieieentnts hahahaadd d an EEEEF FF offff 55550%0%0%0% to
e tnt hhadd iin tt ATAT hhe tt hh drdiia dd fefiin ded bb thth ff 1010
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
5
control group comprising healthy volunteers having a similar age and gender distribution to the
AT patients was recruited fmor the general public through advertising within our institutions. All
subjects underwent clinical assessment, CMR, echocardiography, and the SF-36 Health Survey
as an assessment of quality of life.15 All prospective imaging acquisitions and analyses were
performed blinded to patient study group.
CMR Protocol
Subjects underwent CMR using a clinical 1.5-T MRI scanner (Signa HD 1.5-T, GE Healthcare,
Wisconsin, USA). Sequences were acquired during breath-holds of 10 to 15 s. Initial cine CMR
sequences were performed in 3 standard long-axis (4-, 3- and 2-chamber views) and short-axis
slices (basal, mid, and apical), kept identical for each subsequent sequence throughout the CMR
examination.16 From an end-diastolic, 4-chamber, long-axis view, 5 equally spaced short-axis
slices were planned, so that the 2 outer slices lined up exactly either with the tip of the apex or
the mitral annulus. The 2 outer slices were then deleted, leaving 3 slices corresponding to typical
basal, mid, and apical short-axis views. To calculate LV volume and function, a contiguous
short-axis steady state free precession stack was acquired (8 mm slice thickness, no gap),
extending from the mitral valve annulus to the LV apex.
Delayed hyperenhancement was obtained 10 min after a bolus (0.2 mmol/kg bodyweight
to a maximum of 20 mmol) of gadolinium-diethylene triamine penta-acetic acid (Magnevist,
Schering, Germany) to identify regional fibrosis using a T1 weighted inversion-recovery gradient
echo technique (repetition time: 7.1 ms, echo time: 3.1 ms, inversion time individually
determined to null the myocardial signal; range: 180 to 250 ms, slice thickness: 8 mm, matrix:
256 × 192, number of acquisitions: 2). Delayed enhancement imaging was performed using both
standard long-axis and short axis views of the LV, including a contiguous stack of slices from
to 15 s. Initial ciinenenene C
ber viviiiewews)))s) aanddndd sshohohohortrtrtrt--a
a C
o x
e x
annulus. The 2 outer slices were then deleted, leaving 3 slices corresponding to ty
and apical short a is ie s To calc late LV ol me and f nction a contig o s
al, mmmmidididi , anananand ddd appppicicici al), kept identical for eaaachchchch subsequent sssequeueueuence throughout the C
onnnn.1161 From an eennd-dididiastooolilililic, 4444-chhhammbeerrr, lonong-aaxixixis s s vviewww,,, 5 eequualllll yy y spacacaa edede sshorrrt---ax
e plannnnnenenedddd, so ththth tttat ttthhhhe 222 outututterererer slicesss s liililinenn dd d upup exaxaxaxactctctc lyyy eitttheheheer wiiithththth thehehehe ttttipipii of fff thththhe apex
annulus. ThThThe 2222 outer lsllicii es were thhhen delllet deddd, lel avinii g gg 33 lslliici esesess correspppondidididingngngn to tyyy
dd iic lal hho trt ii ii TT llc ll tat LVLV lol dd ff titi tntiig
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
6
the mitral valve annulus to the apex. For T1 mapping, all 3 standard short-axis levels were
utilized, commencing with the basal level and progressing apically.
For evaluation of diffuse interstitial fibrosis, a T1 mapping sequence described
previously17 was used to acquire images over a range of inversion times. This consisted of an
electrocardiogram-triggered, inversion-recovery prepared, 2-dimensional fast gradient echo
sequence employing variable temporal sampling of k-space (Global Applied Science Laboratory,
GE Healthcare).18 Ten images were acquired sequentially at increasing inversion times (75 to
750 ms) 15 min post-contrast over a series of 3 to 4 breath-holds using the following imaging
parameters – repetition/echo time: 3.7 ms/1.2 ms, flip angle: 20°, 256×128 acquisition matrix,
field-of-view: 36×27-cm, slice thickness: 8-mm, trigger delay: 300 ms, and views per segment:
24. Images were processed using a curve-fitting technique to generate myocardial post-contrast
T1 times as described below.
Evaluation of LV function and regional fibrosis
Volumetric analysis of the LV from which EF was derived was performed using the summation
of discs method. Left atrial volume was determined using the area-length method. Regional
fibrosis was identified by LGE within the myocardium, defined quantitatively by a myocardial
post-contrast signal intensity 5 SDs above that within a reference region of remote non-scarred
myocardium within the same slice. Myocardial delayed enhancement was considered present
only if it was identified in two orthogonal views.
Evaluation of diffuse fibrosis with T1 mapping
Following image acquisition, the 10 short-axis images of varying inversion times were analyzed
using a dedicated research software package (VizPack Version 7.2.0, Global Applied Science
Laboratory, GE Healthcare). The software enabled analysis of regions of interest (ROIs) to
g g the following g immmmagagagagi
×128 88 acacququiisisi ititititiioiion n mamamamatrtr
e m
n
s
c anal sis of the LV from hich EF as deri ed as performed sing the s mm
ew:::: 36363636×2×2×27-7-7-7 cmcmcmcm,, ,, slice thickness: 8-mm, trrrigigigiggger delay: 30000 msmsmss,, and views per segm
wwwweeere e processedd usssinng aaa ccurvvee-ffiiitttingg tttechnhniqueuue tttooo o ggeneneneratee mymyyoocardidididiaala ppoost-cococon
s descrcrccribiibibededede belllow.
of f f LVLVLVL fffunctioioionnnn and dd regigigional f f ffibibibi ro iisiis
c ll isi fof tthhe LLVV ffr hihi hch EEFF dde iri dd frf dd iin thth
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
7
determine pixel-by-pixel and mean T1 time by fitting data acquired at various preparation times
to the exponential curve Mz(t=TI) = M0(A-Be-t/T1) relating the sample magnetization Mz observed
at time t=TI to the equilibrium magnetization M0 and sample T1, where TI denotes inversion time
for an inversion recovery experiment. For each short-axis image, an ROI was drawn around the
entire LV myocardium (excluding papillary muscles) to determine post-contrast myocardial T1
time. In addition, post-contrast T1 time was determined for the LV blood pool to serve as an
internal control using ROIs traced within the LV endocardial border. This process was repeated
to obtain myocardial and blood pool T1 times at all 3 standard short-axis levels. Post-contrast T1
time is known to be dependent on several factors including time post-gadolinium infusion and
renal function.19, 20 Because post-contrast timing was progressively greater from the basal to the
apical slices for each patient, a correction was applied to raw T1 time results individually and
according to modeling proposed by Gai and co-workers, to yield corrected T1 time indexed for a
post-contrast time of 15 min and an estimated glomerular filtration rate (eGFR) of 90 ml/min.20
For each subject, a single global corrected T1 time was calculated by averaging the corrected T1
times at each of the 3 short-axis slices.
Echocardiography
Two-dimensional echocardiography was performed on the same day as CMR using a clinical
system (Vivid 7, General Electric Vingmed, Milwaukee, WI). Images were acquired using a 3.5
MHz transducer in the standard parasternal and apical views with patients in the left lateral
decubitus position. Standard M-mode and 2D images including color Doppler data for 3
consecutive heartbeats were saved in cine loop format. Analyses were performed off-line using
commercially available software (Echopac 6.1, General Electric Vingmed).
Diastolic function was assessed using the mitral inflow pattern from pulsed-wave
xis levels. Post-coontntntntrrar
gadolollliniiiniuiiiumm iinini fffufusisiiionononon a
i 19 20
e n
t d
a m
bject a single global corrected T time as calc lated b a eraging the correcte
ionnnn.191919, 202020 BeBeBeB caaaususususe post-contrast timing wawawas progressivelly grrrreaeaee ter from the basal t
essss fofofofor each patieent, aa corrrrrreeectionon wwwaas aapppplieded tooo raraaawww w T1 tiime reesuuulu ttst indididd vivv duduallylyly an
to mododododelelleliinini g g propos ddded by y GaGaGaGaiiii and ddd cocococ -woworkkkers, totototo yyieieeieldldldld ccccororre tttcted TTTT1 titiitime iii ddnddex dded
ast tiimi e offf 111555 mimimimin anddd an estimateddd glglglomer lulllar ffffilililltrattioiioi nnn n ratetete ((((eGFGFGFG R)R)R)R off ff 90909090 mmmml/m
bbjje tct isi lle llobball ttedd TT titi lal llattedd bb igi tthhe tcte
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
8
Doppler images and tissue Doppler imaging. Early (E) and late (A) diastolic filling velocities,
E/A ratio, E wave deceleration time, septal and lateral early diastolic mitral annular motion
velocity (e’), and the E/e’ ratio were assessed. The anteroposterior diameter of the left atrium
(LA) was measured at end-systole on the M-mode image obtained from the parasternal long-axis
view.
Strain Analysis
LV deformation was assessed using 2D speckle tracking strain imaging. Deformation of the LV
was determined in 3 directions: (i) radial strain, reflecting myocardial thickening/thinning in the
short-axis plane; (ii) circumferential strain, reflecting myocardial shortening/lengthening in the
short-axis plane; and (iii) longitudinal strain, reflecting myocardial shortening/lengthening in the
long-axis plane. Peak systolic radial and circumferential strain and strain rate were calculated by
averaging the peak systolic values of 18 segments, derived from the 6 segments of the 3 short-
axis views (basal, mid, and apical LV). Peak systolic longitudinal strain and strain rate were
calculated by averaging the peak systolic values of 18 segments, derived from the 6 segments of
the 3 apical views (apical long axis and 2- and 4-chamber views). Early diastolic strain rate was
calculated by averaging the values at the time of peak E for 18 segments, derived from the 6
segments of the 3 apical views. Cardiac rotation curves as mean curves of all 6 segments were
derived from basal and apical LV short-axis views. Twist and twist rate curves were generated
based on the difference between apical and basal rotation curves. Clockwise rotation was marked
as a positive value (twist) and counter-clockwise rotation as a negative value (untwist).
Statistics
All data are expressed as mean±standard deviation (SD) unless otherwise indicated.
Comparisons between 2 groups were made using Student’s t test for continuous variables and
thickening/g thinniingngngng i
teninng/g/g//lelell ngngththththeneninnnggg g iiinin
plane; and (iii) longitudinal strain, reflecting myocardial shortening/lengthening
plane. Peak systolic radial and circumferential strain and strain rate were calculat
the peak systolic values of 18 segments, derived from the 6 segments of the 3 sho
r
b a eraging the peak s stolic al es of 18 segments deri ed frof m the 6 segmen
plaaanenenene;;;; ananand dd d (i((( iiii) )) loll ngitudinal strain, reflectctctininii g myocardialaa shohohoh rtr ening/lengthening
plllal nnnen . Peak sysstooliccc rradiiialalalal andnddd ciirccumfmffeeerennttialll sstrtrtrtraaaia nn anannddd strraiin rraate wweww rrer calcuuulllat
the pepeeeakakak sysy tottt lililic valllues offf f 1881818 segmmmem ntnttnts, ddderiviii edededed ffffrorororom thththhe 666 segmmenenenenttstst of fff thththe 3333 hhsho
(((basall,l mididid, ananannd ddd apppiici alll LLLV)V)V)V . PePPP kkak sysyy tolililic llol ngggiititi udddinalal straiaiain nnn and dd sttrain rrrratatatate ee wer
bb iin thth kak ttolili ll ff 1818 tnt dd ii ded ff thth 66
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
9
Fishers Exact test for categorical variables. For comparisons across 3 groups, 1-way analysis of
variance (ANOVA) with Bonferroni correction was used for approximately normally distributed
variables and Kruskal-Wallis test with Bonferroni correction for non-normally distributed
variables. Simple and multiple linear regressions were used to assess predictors of post-contrast
ventricular T1 time. A p value of <0.05 was considered significant, and all reported p values are
2-tailed. Analyses were conducted using SPSS software (version 17, SPSS, Chicago, Illinois).
Results
Subject Characteristics
Thirty-three patients with a history of successful ablation for incessant atrial tachycardia were
recruited (Table 1): 18 with a history of TMC (AT-Low EF) and 15 without (AT-Normal EF).
AT-Low EF and AT-Normal EF patients were recruited 56±41 and 75±28 months following
successful ablation (p=ns). Two AT-Low EF patients each had one prior attempt at ablation that
was unsuccessful before the successful ablation procedure. There were no differences in mean
pre-ablation heart rate on 24-h holter monitoring, AT symptom duration, or AT cycle length
between the two AT patient groups (p=ns). AT-Normal EF patients had an index EF of 60±7%
and did not have routine follow-up echocardiography. AT-Low EF patients had an index EF of
36±12% which was significantly lower than AT-Normal EF patients (p<0.0001, unpaired t-test)
and recovered to 56±4% by 3 months post-ablation (p<0.0001, paired t-test). A further 20
healthy control subjects were recruited for study. Healthy controls, AT-Normal EF patients, and
AT-Low EF patients had a similar age and gender distribution. At follow-up, patients were
generally free of co-morbidities. Three AT-Low EF patients were prescribed both ACE-inhibitor
-blocker therapy: 2 had developed concomitant hypertension and coronary artery disease
after index presentation, and 1 remained on the combination from the time of diagnosis of TMC.
ee patients with a history of successful ablation for incessant atrial tachycardia w
T E
n
n
cessful before the successful ablation procedure. e
e patititienenentststs wwwith hhh a history of successful ablalalatitt on for incessantntntnt atrial tachycardia w
TTTTababbable 1): 18 wwiww tth aaaa hhhhisisisi totototoryryryr oof f f TMTMTMTMCC (A(A(A(AT-LLooow EFEFEFEF)))) aana dd dd 1515115 wwwitthoooutututu ((((ATATATAT-NNNNorororrmammm lll E
F aaaandndndn AAAAT-T-T-T-NNNNorororo mamamamallll EFEFEFEF patatatatieieientntntntss wewewew rereree rrrececececrururur ittedededed 5556±6±6±6±41414141 aaaandndndnd 77775±5±5±28282828 mmmmononononthththt ssss fofoolllll owowowowininiin
ablatatatatioioioi nn n (p(p(p=n=n=ns)s)s)s). TwTwTwT ooo ATATAT-L-L-L-Lowwww EFEFEF ppppataaa ieeeentntnts ss eaeaeae chchchch hhhhadadadd ooooneneee pppriririorororr aaaattttttemememmptptpt aaaatt ababablalalaation
ccesessfs ulu bbefefefforo e e ththththee susucccccesessffsffullull aablblblbl tatattioiioi n n prp ococ dededduru e.e. ThThThThere ee weweree no o didididiffffffffere ene ceces s in mee by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
10
Of AT-Normal EF patients, 2 were prescribed ACE-inhibitor therapy only for diabetes and/or
hypertension.
CMR Findings
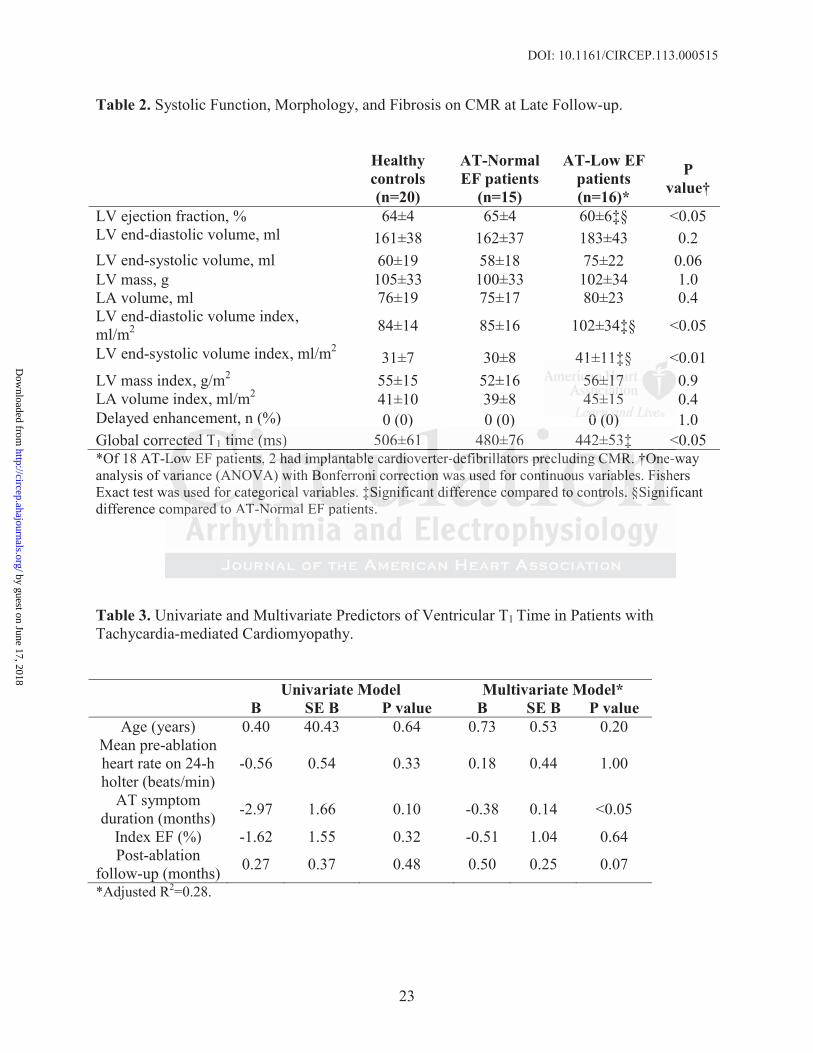
Results are detailed in Table 2. Of the 18 AT-Low EF patients, 2 had received implantable
cardioverter-defibrillators (ICDs) for primary prophylaxis prior to successful ablation of atrial
tachycardia, precluding CMR. Both devices were left in situ following normalization of EF and
at follow-up had never recorded ventricular arrhythmia. Remaining AT-Low EF patients had
larger indexed LV end-diastolic volume, larger indexed end-systolic volume, and lower LV EF
compared to healthy controls and AT-Normal EF patients. No subject had delayed regional
myocardial enhancement.
The time delay from gadolinium infusion to image acquisition increased overall across
the 3 short-axis planes from 22.6±2.9 min (basal LV) to 27.0±3.7 min (mid LV) and 31.4±4.6
min (apical LV) (p<0.001). However, the time delay from gadolinium infusion to image
acquisition was not significantly different between the 3 groups at each of the 3 LV short-axis
planes (p=ns for all comparisons). Following correction of T1 time for post-contrast time delay
and eGFR, there were no significant differences in post-contrast T1 time between the 3 LV short-
axis planes within each of the 3 groups (p=ns for all comparisons). Global corrected T1 time was
shorter in AT-Low EF patients compared with controls (442±53 vs 506±61 ms, p<0.05). This
difference remained significant after exclusion of apical T1 time measurements, a potential
source of error due to their smaller size and the influence of noise and patient specific delays
(440±54 vs 492±70, p<0.05).
Predictors of Ventricular T1 Time in AT-Low EF Patients
Simple and multiple linear regressions were performed to assess predictors of fibrosis as
olume, and lowerr LLLLVV
had dedded lalall yeyedddd reregigiigiononononalal
l
e r
- 4
l
n as not significantl different b t the 3 gro ps at each of the 3 LV short a
l enhnhhnhananana ceceeemmem ntntntt....
e timmmem delay frromm gaggadolililinninn umm infuusioonnn to immagegege aaaacqccqc uiisiiitionn iincccreeasedd dd ovovo errall l aacr
-axisi ppplalalalannnnes frfff om 222222.6±66 2.22 999 9 mmmin (b(b(b(baasasa alallal LLLV)V)V)V tttto 27272727 0.000±3±3±3±3.7777 mimimimin (((midddd LLLLV)V)VV anddd 33331.111 4±4±4±4±4
l LVVVV))) (p(p(p<000 0.000101011).).). HHHowever, the iitime dddellayyy fffrom gagg ddod lililil ninininium iiinfnfnfnfusiiion to iiimamamamagegegege
tt isi ififiic tltl didiffff tt bb t tthhe 33 tat hh fof tthhe 33 LLVV hsh tt
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
11
measured by ventricular T1 time, using the following known and putative predictors of diffuse
fibrosis: age, mean heart rate on 24-h holter monitoring, AT symptom duration, index EF, and
post-ablation follow-up duration (Table 3). Simple linear regression revealed a potential
relationship between AT symptom duration and ventricular T1 time (F=3.19, R2=0.24, p=0.1). A
significant inverse relationship between AT symptom duration and ventricular T1 time was
confirmed in the multivariate model ( =-0.79, p<0.05; adjusted R2=0.28).
Echocardiographic Findings
There were no significant differences in diastolic parameters across the 3 groups (Table 4).
Speckle tracking analysis revealed subtle differences in LV systolic and diastolic function (Table
5). Despite having recovered EF within the normal range, AT-Low EF patients showed
attenuated global circumferential strain, global longitudinal strain, and twist rate compared with
healthy controls and AT-Normal EF patients. Global early diastolic strain rate was also reduced
compared to controls. Speckle tracking analysis showed no differences between AT-Normal EF
and control subjects.
Discussion
In this study, we characterized LV structure and function in patients with a past history of TMC
induced by incessant focal atrial tachycardia, late after successful ablation of the culprit
arrhythmia. This is a unique patient cohort as long-term arrhythmia cure is feasible. Our major
findings, 5 years following successful ablation, are as follows: (i) LV indices of TMC patients
were within normal ranges on CMR, echocardiography, and strain analysis; (ii) TMC patients
showed subtle differences in LV structure and function compared with controls, with larger LV
dimensions, lower EF, and attenuated myocardial strain and twist rate; and (iii) compared to
ee 33 ggroupps (T(( abablele 4)4)4)4).
nd diaiaststololiciic fffununctctioioioionnn (
e
n d
t a
l bj
haaaviviviinngnn rrrrececee ovvverererered EF within the normal lll rarar nnge, AT-Low www EFEFFF patients showed
ggggloooobal circummfeerentnntiial stststrrrain, globoobal looongiituudiiinanaanalll stssts raiinin, andd twwwissst ratetetet comompaaareeed
ntrolsss a ddnd ATTT-NNNorm lal EFFF patients. GlGlGlobobbalal earlyll diaii stolliici str iiain ratett was allso redd
to controls. SpSpSpeckle trackinggg analyyysis showed no differreeene cesss bbbeb tween ATTTT-NoNoNoNorma
l bj
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
12
controls, TMC patients had reduced global corrected T1 time consistent with diffuse myocardial
fibrosis.
Clinical studies of TMC consistently document good outcomes in the early recovery
phase with EF recovering to the normal range within 1 to 6 months of treatment.6, 8, 9, 21, 22
However, late adverse outcomes have been reported.8, 9 Among a cohort of 24 TMC patients (EF
26±9%) followed for a mean of 26 months after treatment, Nerheim and co-workers reported 5
cases of recurrent heart failure in which EF declined precipitously with recurrent tachycardia.9 In
addition, 3 relatively young males suffered unexpected sudden cardiac death at 6 months, 9
months, and years following recovery of normal EF. However, all 3 had recurrent and persistent
AF before death and one had undergone AV node ablation and pacing. Thus none of the 3 had
been cured of the index arrhythmia and the cause of death was uncertain. Nevertheless, these 3
patients had significantly depressed index EF compared to the rest of the cohort (16±5%).
Watanabe and co-workers reported similar findings among 12 TMC patients (EF 32±10%,
NYHA functional class 2.3±0.5): 2 patients experienced rapid return of systolic dysfunction with
tachycardia recurrence, and 1 patient died suddenly 40 months after EF recovery in the absence
of documented recurrent tachycardia and heart failure.8 These observations suggest that
persistent ultrastructural changes of the myocardium may provide an arrhythmogenic substrate
and predispose to LV deterioration in the face of repeated stress. Indeed, Dandamudi and co-
workers demonstrated persistent LV dilatation in 24 TMC patients up to 14 months after
appropriate treatment and normalization of EF.6
Our study revealed differences in LV structure and function in TMC patients compared
with controls years after definitive treatment of the culprit tachycardia. Our cohort is unique in
being composed of patients with TMC who were largely free of important confounding
c death at 6 monthhhhs,s,s,s, 99
ad rececururrerenntttt anandddd pepepeperrrsrsii
death and one had undergone AV node ablation and pacing. Thus none of the 3 h
of the index arrhythmia and the cause of death was uncertain. Nevertheless, the
d
a
nctional class 2 3±0 5): 2 patients e perienced rapid ret rn of s stolic d sf nction
deatataa h h hh ananand dd d onoo e ee hhhah d undergone AV node abababablalll tion and pacaa ing.g.g.g. Thus none of the 3 h
oooof fff the index ararrrhyyythhhmiaaa andddd tttthehehe ccausesee of f ddeatttthh h wwwaw ss uununccertaiain. NNNeverrrrthhhelleess, thhhe
d signgngngnifiifificiccicantlllly ddded prpressed ddd ininininddddex EFEFEFEF comoo papared dd totototo tthehehehe ressstttt ffof ttthhheh cohohohohorororo t (11116±6±6±±5%5%5%5%))).
andddd co-workekekersrrr reppportedd d siiiimilall r fififi ddnddiini gsgg amonggg 1111222 TMTMTMTMCC CC papapatitititients ((((EFEFEFE 33332±2±2±2±1010100%,
tctiio ll lcl 22 3±3±00 5)5) 22 titi tts iie ded idid tet fof ttolili dd fsf tctiio
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000515
13
influences. All patients presented with incessant focal atrial tachycardia with minimal
comorbidities, underwent curative ablation, and had no recurrence at follow up. In contrast, the
majority of patients in prior TMC series have had cardiomyopathy secondary to atrial
fibrillation/flutter.7-9, 21 In these series, outcomes may have been negatively biased by the
presence of conditions associated with these arrhythmias such as pre-existing hypertension and
heart failure. Cases of atrial fibrillation were generally treated with pharmacological rate-control
or cardioversion, allowing the confounding influence of arrhythmia recurrence and unrecognized
periods of poor rate-control to bias results. Evidence of a negative impact of irregular ventricular
rhythm per se on ventricular function despite “controlled” ventricular rate also exists.21, 23 In
contrast, focal atrial tachycardia is considered a sporadic arrhythmia not known to be influenced
by pre-existing ventricular cardiomyopathy. Our patients did not experience the adverse
outcomes of recurrent heart failure and sudden death described in prior series.8, 9 In 2 patients
with severely depressed index EF who received ICD implantation for primary prophylaxis, no
ventricular arrhythmias were recorded. However, our TMC cohort had less severe systolic
impairment at presentation in comparison to these previous series and this may account for
differences in observed outcomes (index EF of 36±12% vs 28±10%, p<0.05).
TMC is well studied in porcine and canine tachypacing models, and is characterized by
spherical LV dilatation, systolic dysfunction, elevated filling pressures, diminished cardiac
output, reduced systemic vascular resistance, and neurohormonal activation.24 LV dilatation is
more pronounced for end-systolic than end-diastolic indices.25, 26 Systolic dysfunction results
from loss of myocardial contractility and contractile reserve reflected by whole heart and isolated
cardiomyocyte indices.10, 25 Following resumption of normal sinus rhythm, EF typically shows
dramatic recovery in the first 24 to 48 hours, subsequently normalizing in the following weeks.1,
ppact of irreggular vvenenenentrt
rate alalllsoso ee ixixiisttsts.s 2121211, , ,, 23232323 II
o e
s
o n
ely depressed index EF who received ICD implantation for primary prophylaxis,
arrh thmias ere recorded Ho e er o r TMC cohort had less se ere s stolic
ocaaaalll atatatatriririr alalalal tttaachyhyhyccac rdia is considered a sporororada ic arrhythmim a nonononot known to be influe
sttttinnnng g ventricularr caaardddiomymymyyopatttathyyy. Ouur pattieentsss dddidididd nnottt eeexpeeriiencnnce thee ee aada veverseee
of recucuccurrrrreeeent hehhh artttt fafff illililure anananndddd sudddddenenene ddddeaththth ddded scsccriririribebebeb ddd d innn ppppriiior serieieieesss.8888, 99 IIIIn 222 patiititien
ely yy deddd prpp essed dd inininindeddd x EFEFEF whohhh rec iieiveddd d ICCCCDDD iimi plplplantatiiionn fffor ppprirrr maryyy ppprophphphphylylyly axaaa is,
hrh tthhmiia ddedd HHo TTMCMC hoh tt hhadd lle tst loliic
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
14
4, 26 Nevertheless, attenuation of contractile function and relaxation remain measurable at the
cellular level 4 weeks after cessation of tachypacing, and LV volumes remain elevated.10
Development of LV hypertrophy and an increase in diffuse interstitial fibrosis are also observed,
and the resulting reduction in wall stress, rather than normalization of LV geometry or myocyte
contractility, mediates improved pump function at this stage. 10-12
With the exception of LV hypertrophy, animal model findings in the early recovery phase
bear striking resemblance to those of late follow-up in the human setting as demonstrated by our
study. We made the further observation that the degree of fibrosis correlated with arrhythmia
symptom duration but not index EF, consistent with the notion that systolic dysfunction and
fibrosis run independent courses during the induction and recovery phases of TMC as observed
in animal models.
The exact mechanism by which fibrosis is induced in this setting remains to be clearly
defined. Porcine heart failure induced by rapid atrial pacing has been associated with reduced
ventricular collagen concentration, cross-linking, and fibril diameter; while cessation of rapid
pacing resulted in recovery of systolic function accompanied by increased collagen concentration
and thickened collagen weave.11, 12 Similar findings have been replicated in dogs.27 Following
induction of heart failure by rapid pacing, LV fibroblasts isolated from failing pig hearts showed
increased formation of fibrillar collagen, increased adhesion to and migration through
extracellular matrix substrates, and differences in fibroblast associated integrins.28 In a canine
model of tachypacing-induced heart failure, isolated ventricular fibroblasts exhibited increased
proliferation rates.29 Interestingly, phenotypic changes in TMC fibroblast biology appear to
remain stable for several generations of cell culture passages.28 Collectively, these observations
point to a significant and stable transformation of fibroblast phenotype in response to
related with arrhytytytthmhmhmhm
stolicc dydydyd sfffsfununctttctioioii n nnn aaanandd
n independent courses during the induction and recovery phases of TMC as obse
m
e a
o c
collagen concentration cross linking and fibril diameter; hile cessation of rap
n indnddndepepepe enennndedededentt ccccourses during the inductioioioion and recoveryrr phahahah ses of TMC as obse
mmmom ddded ls.
e exacacacacttt mmmmechhhhaniiism bbbby whihihihichchchch fibroooosisisisis iiisi iiiinddducedededed iiinin tttthhhih s seseses ttttttt inii g remamamamainininins tottt bbbbe clllea
orcine hheh art fafafaiilili ure iini dudd ceddd d bybyby rapppidididd atriaiii lll papp cinggg hhhas bbbeeeee n asasassso icii tat dedd witittth hhh rerereeduc
llll tnt titi lili knkiin dnd ffibib irill didi tet hhilil tatiio fof
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
15
cardiomyopathy induced by rapid ventricular rates, which may explain the presence and
persistence of LV fibrosis noted in our patients.
Our finding of diffuse LV fibrosis many years after curative ablation is highly relevant,
as this may provide a substrate for late arrhythmic events proposed to account for sudden death
observed in prior series.8, 9 Extensive evidence supports the role of fibrosis in ventricular
arrhythmogenesis.30 Among sudden death autopsy series, ventricular interstitial fibrosis in the
absence of other structural abnormalities is a consistent albeit uncommon finding, affecting an
estimated 1 to 3% of cases.31-33 Murine models show a clear relationship between inducibility of
ventricular arrhythmias and degree of interstitial fibrosis.34, 35 Increased fibrosis alters tissue
electrophysiology through partial decoupling of muscle fibres, conduction slowing, zig-zag
courses of conduction propagation, localized source-sink mismatches, and conduction blocks.36-
38 Furthermore, myofibroblast coupling to cardiomyocytes through gap junction formation
imparts enhanced automaticity to cardiomyocytes when coupled to a critical number of
myofibroblasts.39
Recent whole heart studies demonstrate the role of fibrosis in modulating formation of
early afterdepolarizations (EADs) that lead to triggered activity causing ventricular fibrillation
(VF).40, 41 It is well established that oxidative stress promotes EADs and triggered activity in
isolated cardiomyocytes.42 This same stress fails to cause EADs in well-coupled, non-fibrotic
hearts due to source-to-sink mismatches arising from cell-to-cell coupling, but readily induces
ventricular tachycardia (VT) and VF in diffusely fibrotic rat and rabbit hearts.40, 41 Optical
mapping and roving glass microelectrode single cell action potential recordings revealed
triggered activity causing focal VT that degenerates within seconds to VF after the emergence of
spatially discordant action potential duration alternans leading to wavebreak, reentry and VF.30
hipp between induccibibibibili
d fibrbrbb ososisiiis aaltltltltererss titititissssssssuu
s g
m
h
lasts 39
siololologogogogyyy ththththrorrougggghhh h partial decoupling of muuuscscs le fibres, cononnduuuctctctction slowing, zig-zag
cccconnnnduction prroppagggatttationn,n localalallizedeed sououurce-sssinkkkk mmmmiiisi mamaatccches, aanddd d condddduucu tioon bbbloooc
more, myymymy fofofibroblblbllasttt coupplililiingngngng to cacaaardrdrdrdioioiomymyoc tyttteseseses tthrhrhrhrooughghghgh ggap jjjjunctctctctioioioon formatttiiiion
hanceddd autommmataaa iciii itii y yy to cardididid omyoyy cyyytes hhwhen couplplpledddd ttooo o a crrritiiti icii lall numbebebeberrr r ofofofof
ll tt 393939
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000515
16
Thus, the “first-hit” of ventricular fibrosis in this paradigm does not generate ventricular
arrhythmia alone but requires a “second-hit” of oxidative stress to do so.
Diffuse ventricular fibrosis in our TMC cohort may reflect an arrhythmogenic substrate
that has remained asymptomatic due to absence of an appropriate trigger. Sudden deaths in prior
reports potentially represent lethal ventricular arrhythmias triggered by the oxidative stress
associated with tachycardia recurrence,43, 44 or some other physiologic insult. Whether patients
with TMC would benefit from a period of anti-fibrotic or anti-failure pharmacotherapy remains
to be studied.
Study Limitations
Patient numbers were limited by the scarcity of cases with atrial tachycardia-induced TMC at our
centres. However, our study is the first to report on a group of TMC patients receiving definitive
cure for their inciting arrhythmias, and has a long follow-up duration. Retrospective study design
did not allow exclusion of ventricular abnormalities prior to development of arrhythmia.
Furthermore, lack of baseline CMR and strain imaging precluded temporal comparisons at
follow-up. While an antecedent cardiomyopathy causing incessant focal AT is a theoretical
consideration, we are not aware of any prior description of such a relationship in the human
literature, and the prompt resolution of systolic dysfunction following successful arrhythmia
ablation points against this possibility. Nevertheless, we cannot exclude the possibility that the
structural and ultrastructural changes we observed following resolution of systolic dysfunction in
TMC patients were present prior to the development of TMC. However, this would challenge the
current paradigm of TMC that affected patients have normal hearts prior to the development of
incessant AT, suggesting that the development of TMC requires the presence of adverse cardiac
remodeling plus the advent of incessant AT. Several AT patients with hypertension, diabetes,
m C
owever, our study is the first to report on a group of TMC patients receiving defin
e d
o
re lack of baseline CMR and strain imaging precl ded temporal comparisons at
mbberererers ss s weweweerererer limmmitiii ed by the scarcity of caseseses with atrial tataachycycycycardia-induced TMC
owwwweeeve er, our stududy iiis the ffffiirst ttoo rrrepportt ooon aa grouooupppp ofoofo TMCMM ppaatieeeentntnts recececec ivvinng dededefin
eir incncncncitititininning arrhhh tttythmhhh iaiii s, andndndnd hhhas a aaa lolololongnn ffffollllllow-uuupup dddduuratatatioioioi n. RRReR trosososospepepep ctive studddy d
ow ex lcllusioii n ofoofo ventricii lullar abnormalililities pppriiiior tto dedd velolooopmpmpmenenenent t foff arrhyhyhyththththmimimim aaa.a
ll kk fof bb leliin CMCMRR dd tst iin ii igi lcl dd dd tte lal iri tt
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
17
coronary disease, and/or longstanding ACE-inhibitor/ -blocker therapy were included in our
analyses. Regardless, the key finding of shorter global corrected ventricular T1 time in TMC
patients versus controls remained significant after exclusion of these 5 patients (439±55 vs
506±61 ms, p<0.05). We did not confirm the presence of interstitial fibrosis histologically, but
relied on a histologically validated contrast-enhanced T1 mapping technique to determine its
presence. Although several T1 mapping methodologies have been described, the largest body of
data in cardiomyopathy patients using human histology as a reference standard has been acquired
with the post-contrast T1 technique utilised in this study.17, 45
Conclusion
TMC patients exhibit subtle changes in LV structure and function including diffuse fibrosis long
after arrhythmia cure and return to normal EF, indicating that recovery is incomplete.
Funding Sources: Dr Ling is supported by an Australian National Heart Foundation (NHF) Postgraduate Scholarship. Dr Iles is supported by an Australian National Health and Medical Research Council (NHMRC) Postgraduate Research Scholarship. Prof Kaye is supported by an NHMRC program grant. Dr Hare is the recipient of a Research Investigatorship from the Cardiac Society of Australia and New Zealand. A/Prof Kistler is the recipient of a Research Investigatorship from the Cardiac Society of Australia and New Zealand. Dr Ellims holds a co-funded NHMRC/NHF Postgraduate Scholarship. Dr Taylor is supported by a National Health and Medical Research Council program grant, and an Australian National Heart Foundation project grant. This research is supported in part by the Victorian Government’s Operational Infrastructure Funding.
Conflict of Interest Disclosures: None.
References:
1. Medi C, Kalman JM, Haqqani H, et al. Tachycardia-mediated cardiomyopathy secondary to focal atrial tachycardia: Long-term outcome after catheter ablation. J Am Coll Cardiol.2009;53:1791-1797.
2. Packer DL, Bardy GH, Worley SJ, et al. Tachycardia-induced cardiomyopathy: A reversible
n
s
t
S Fate Scholarship Dr Iles is s pported b an A stralian National Health and Medic
n
nnnntssss exhibit subububu ttleee chchchchanananangegegegess s inininin LLLLVVVV sstruucttturee aand d dd fuffuf ncncncn tiiiononon iiincncnc ullul dingngngn ddddififififfufuffusesese ffffibibibibrororor sis s
thmmmmiaiaia ccccurururureeee anananndd d rerereetututuurnrnnn to nononon rmrmmmal EEEEFFF,,,, inininndidididiccac tititiingngngng ttthahahahat rererer cocococ veveveveryryry iiiissss inininincocococompmpmpm lelelel teee....
Sources: DrDrDrDr LLLLininning g g g isissis sssupupupppopopop rtrtrtedededed bbbby y y y anananan AAAAusususustrtrtrralalalaliaiii n nn NaNaNaNatitiitiononono allalal HHHHeaeaeaeartrtrtrt FFFFououououndndndndatatatatioiii n (NHFtte SS hch lol hshiip DDr IIlle iis trt ded bb AA ttr laliia NNatiti lal HH ltlthh dd MMedidi
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
18
form of left ventricular dysfunction. Am J Cardiol. 1986;57:563-570.
3. Hendrick DA, Smith AC, Kratz JM, Crawford FA, Spinale FG. The pig as a model of tachycardia and dilated cardiomyopathy. Lab Anim Sci. 1990;40:495-501.
4. Moe GW, Stopps TP, Howard RJ, Armstrong PW. Early recovery from heart failure: Insights into the pathogenesis of experimental chronic pacing-induced heart failure. J Lab Clin Med.1988;112:426-432.
5. Redfield MM, Aarhus LL, Wright RS, Burnett JC, Jr. Cardiorenal and neurohumoral function in a canine model of early left ventricular dysfunction. Circulation. 1993;87:2016-2022.
6. Dandamudi G, Rampurwala AY, Mahenthiran J, Miller JM, Das MK. Persistent left ventricular dilatation in tachycardia-induced cardiomyopathy patients after appropriate treatment and normalization of ejection fraction. Heart Rhythm. 2008;5:1111-1114.
7. Chin A, Badri M, Ntusi NB, Okreglicki A. The clinical, electrocardiographic and echocardiographic characteristics and long-term outcome of patients with tachycardia-induced cardiomyopathy. Cardiovasc J Afr. 2012;23:136-142.
8. Watanabe H, Okamura K, Chinushi M, et al. Clinical characteristics, treatment, and outcome of tachycardia induced cardiomyopathy. Int Heart J. 2008;49:39-47.
9. Nerheim P, Birger-Botkin S, Piracha L, Olshansky B. Heart failure and sudden death in patients with tachycardia-induced cardiomyopathy and recurrent tachycardia. Circulation.2004;110:247-252.
10. Spinale FG, Holzgrefe HH, Mukherjee R, et al. Lv and myocyte structure and function after early recovery from tachycardia-induced cardiomyopathy. Am J Physiol. 1995;268:H836-847.
11. Spinale FG, Tomita M, Zellner JL, et al. Collagen remodeling and changes in lv function during development and recovery from supraventricular tachycardia. Am J Physiol.1991;261:H308-318.
12. Spinale FG, Zellner JL, Johnson WS, Eble DM, Munyer PD. Cellular and extracellular remodeling with the development and recovery from tachycardia-induced cardiomyopathy: Changes in fibrillar collagen, myocyte adhesion capacity and proteoglycans. J Mol Cell Cardiol.1996;28:1591-1608.
13. Spinale FG, Zellner JL, Tomita M, Crawford FA, Zile MR. Relation between ventricular and myocyte remodeling with the development and regression of supraventricular tachycardia-induced cardiomyopathy. Circ Res. 1991;69:1058-1067.
14. Saoudi N, Cosio F, Waldo A, et al. A classification of atrial flutter and regular atrial tachycardia according to electrophysiological mechanisms and anatomical bases; a statement from a joint expert group from the working group of arrhythmias of the european society of
14.
iograaphphphhiiicic aa ddndnd with taaaachchchchycycycycarararardidididiaaaa iiiindndndn u
p
be H, Okamura K, Chinushi M, et al. Clinical characteristics, treatment, and outcr
m
2
patttthyhyhy. CaCaCaardrdrdrdiooovavavavasc J Afr. 2012;23:136-1424242..
beee e HHH,H Okamuraa K, ChChChinususushi MMMM, eteet al. CCClinniccal chchchc ararararaacteeeriiisticcs,, trrreaatmeeeentntnt, anand ouououtcrdddiaiaia iiinducedededd carrdiomoomyopapapathtt y.y.y. InInInnt HeHeHeararart J.J. 220000088;8 499::3999-4447.
m P, BBBBiriririrgegegerrr-B-B-Bototototkikikikin nn S,S,S,S PPPPiririiracacacchahhh LLLL, ,, OlOlOlOlshshshhaanskskskkyyy B.B.B.B. HHHHeaeaartrtrtrt ffffaiaiaia lulululurerere aaandndndnd sssududududdededed n n n n dededeeatatath h h h in th tachhhycyy ardididiaaaa i-inddduc dedd carddid omyoyy papp thy yy and ddd recurrentt tataaa hchhycycyccardididid a. CiCiCircululululatatata ioioioion.
247-252. by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
19
cardiology and the north american society of pacing and electrophysiology. Eur Heart J.2001;22:1162-1182.
15. Ware JE, Jr., Sherbourne CD. The mos 36-item short-form health survey (sf-36). I. Conceptual framework and item selection. Med Care. 1992;30:473-483.
16. Taylor AJ, Al-Saadi N, Abdel-Aty H, et al. Detection of acutely impaired microvascular reperfusion after infarct angioplasty with magnetic resonance imaging. Circulation.2004;109:2080-2085.
17. Iles L, Pfluger H, Phrommintikul A, et al. Evaluation of diffuse myocardial fibrosis in heart failure with cardiac magnetic resonance contrast-enhanced t1 mapping. J Am Coll Cardiol.2008;52:1574-1580.
18. Saranathan M, Rochitte CE, Foo TK. Fast, three-dimensional free-breathing mr imaging of myocardial infarction: A feasibility study. Magn Reson Med. 2004;51:1055-1060.
19. Kawel N, Nacif M, Zavodni A, et al. T1 mapping of the myocardium: Intra-individual assessment of the effect of field strength, cardiac cycle and variation by myocardial region. JCardiov Magn Reson. 2012;14:27.
20. Gai N, Turkbey EB, Nazarian S, et al. T1 mapping of the gadolinium-enhanced myocardium: Adjustment for factors affecting interpatient comparison. Magnet Reson Med. 2011;65:1407-1415.
21. Hsu LF, Jais P, Sanders P, et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351:2373-2383.
22. Van Gelder IC, Crijns HJ, Blanksma PK, et al. Time course of hemodynamic changes and improvement of exercise tolerance after cardioversion of chronic atrial fibrillation unassociated with cardiac valve disease. Am J Cardiol. 1993;72:560-566.
23. Clark DM, Plumb VJ, Epstein AE, Kay GN. Hemodynamic effects of an irregular sequence of ventricular cycle lengths during atrial fibrillation. J Am Coll Cardiol. 1997;30:1039-1045.
24. Shinbane JS, Wood MA, Jensen DN, et al. Tachycardia-induced cardiomyopathy: A review of animal models and clinical studies. J Am Coll Cardiol. 1997;29:709-715.
25. Shannon RP, Komamura K, Stambler BS, et al. Alterations in myocardial contractility in conscious dogs with dilated cardiomyopathy. Am J Cardiol. 1991;260:H1903-1911.
26. Howard RJ, Stopps TP, Moe GW, Gotlieb A, Armstrong PW. Recovery from heart failure: Structural and functional analysis in a canine model. Can J Physiol Pharmacol. 1988;66:1505-1512.
27. Weber KT, Pick R, Silver MA, et al. Fibrillar collagen and remodeling of dilated canine left
-breathing g mr imaagigigigingng1111050505055-5-5-5-1010101060606060. .
um: Intntntntrararara iiiindndndndivivivivididididuauauau llt of the effect of field strength, cardiac cycle and variation by myocardial region.
M
Turkb EB, Nazarian S, et al. T1 m of the dolinium-enhanced ocarn 0
F, Jais P, Sanders P, et al. Catheter ablation for atrial fibrillation in congestive heE l J M d 2004;351:2373 2383
t of f f thththheee efefefffefefefect oooof fff field strength, cardiac cyycyclcle and variatioi n bybybyb myocardial region.Maaaagngngngn Reson. 201010112;;141414:2:2:27.777
TTTurururkbkk ey EEEEB,BBB NNazaraarian S,S,S, et alalalal. T1T1T1 mmmapapppiingng oooof ff theee e gagag dododooliniiuum--e-- nhnnn annnncccedd mmyocococarnt for fafafafacttctctors affffffe tcttiiing interprprprpatientntt ccccomommpapariiison. MaMaMaMagggnetett RRRReson MMMedededed. 222011111;11 6565656 :1114040404
F, Jais P, SaSaaSandndndndererererssss P,P,PP, eeet t t alalalal. CaCaCaaththththetttterererr aaablblblb atatatatioioioion nnn fofoff r rr atatatriririialalaal fffibibibbrirririllllllllatatatatioioioion n n n ininnin ccconononongeggg stive heEE ll JJ MM dd 22000044;353511:23237373 22383833
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from
DOI: 10.1161/CIRCEP.113.000515
20
ventricle. Circulation. 1990;82:1387-1401.
28. Flack EC, Lindsey ML, Squires CE, et al. Alterations in cultured myocardial fibroblast function following the development of left ventricular failure. J Mol Cell Cardiol. 2006;40:474-483.
29. Burstein B, Libby E, Calderone A, Nattel S. Differential behaviors of atrial versus ventricular fibroblasts: A potential role for platelet-derived growth factor in atrial-ventricular remodeling differences. Circulation. 2008;117:1630-1641.
30. Karagueuzian HS. Targeting cardiac fibrosis: A new frontier in antiarrhythmic therapy? Am J Cardiovasc Dis. 2011;1:101-109.
31. John BT, Tamarappoo BK, Titus JL, et al. Global remodeling of the ventricular interstitium in idiopathic myocardial fibrosis and sudden cardiac death. Heart Rhythm. 2004;1:141-149.
32. Hookana E, Junttila MJ, Puurunen VP, et al. Causes of nonischemic sudden cardiac death in the current era. Heart Rhythm. 2011;8:1570-1575.
33. Chugh SS, Chung K, Zheng ZJ, John B, Titus JL. Cardiac pathologic findings reveal a high rate of sudden cardiac death of undetermined etiology in younger women. Am Heart J.2003;146:635-639.
34. Stein M, Noorman M, van Veen TA, et al. Dominant arrhythmia vulnerability of the right ventricle in senescent mice. Heart Rhythm. 2008;5:438-448.
35. Massare J, Berry JM, Luo X, et al. Diminished cardiac fibrosis in heart failure is associated with altered ventricular arrhythmia phenotype. J Cardiovasc Electrophysiol. 2010;21:1031-1037.
36. Ten Tusscher KH, Panfilov AV. Influence of diffuse fibrosis on wave propagation in human ventricular tissue. Europace. 2007;9 Suppl 6:vi38-45.
37. de Bakker JM, van Rijen HM. Continuous and discontinuous propagation in heart muscle. JCardiovasc Electrophysiol. 2006;17:567-573.
38. Kawara T, Derksen R, de Groot JR, et al. Activation delay after premature stimulation in chronically diseased human myocardium relates to the architecture of interstitial fibrosis. Circulation. 2001;104:3069-3075.
39. Miragoli M, Salvarani N, Rohr S. Myofibroblasts induce ectopic activity in cardiac tissue. Circ Res. 2007;101:755-758.
40. Morita N, Lee JH, Xie Y, et al. Suppression of re-entrant and multifocal ventricular fibrillation by the late sodium current blocker ranolazine. J Am Coll Cardiol. 2011;57:366-375.
41. Morita N, Sovari AA, Xie Y, et al. Increased susceptibility of aged hearts to ventricular
thm. 2004;;1:141-1414141499
ic suuddddddddenen ccarardidididiacac ddddeea
SS, Chung K, Zheng ZJ, John B, Titus JL. Cardiac pathologic findings reveal a hd6
M, Noorman M, van Veen TA, et al. Dominant arrhythmia vulnerability of the rign
re J Berr JM L o X et al Diminished cardiac fibrosis in heart fail re is associ
SSSSS , Chung ggg K,K,K ZZZZheehengngngg ZZZZJ,,, JJJJohohohohn n B,B,B, Titititususus JLL. Cararardididdiacaaca pppaataa hohohoh lolologiggg c fiindndndndininini gsggg rrreveveve eaeaeaal ll a hddddenenenen cardiac deaeath ooof ff undededeetermminnnedd ettiooologgyy innnn yyyyouououounngeeer wommennn. AAAmA HHHHeeae rtrt J.63535353 -6-6-639.
M, NNNooooooo rmrmrmananan MMMM,,,, vavavaan n n n VeVeVeVeenenen TTTTA,A,A, eeet t t t alalalal... DoDD mimimim nananaantntntnt aaaarrrrrrhyhyyhythththhmimimmiaaa vuvuvuvulnlnlnlnererere ababababililili ititity y y y ofofoff ttthehehehe rign senescent mmmicicicce. HHHeart RhRhRhhytyy hm. 222000000088;8 5:555 4343438-888 4444444888.
JJ BB JJMM LL XX tet ll DDiimiiniishhedd drdiia fifibbr iis ii hhe tt ffailil iis ii
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
21
fibrillation during oxidative stress. Am J Physiol Heart Circ Physiol. 2009;297:H1594-1605.
42. Xie LH, Chen F, Karagueuzian HS, Weiss JN. Oxidative-stress-induced afterdepolarizations and calmodulin kinase ii signaling. Circ Res. 2009;104:79-86.
43. Nakamura R, Egashira K, Machida Y, et al. Probucol attenuates left ventricular dysfunction and remodeling in tachycardia-induced heart failure: Roles of oxidative stress and inflammation. Circulation. 2002;106:362-367.
44. Shite J, Qin F, Mao W, et al. Antioxidant vitamins attenuate oxidative stress and cardiac dysfunction in tachycardia-induced cardiomyopathy. J Am Coll Cardiol. 2001;38:1734-1740.
45. Sibley CT, Noureldin RA, Gai N, et al. T1 mapping in cardiomyopathy at cardiac mr: Comparison with endomyocardial biopsy. Radiology. 2012;265:724-732.
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
22
Table 1. Subject characteristics at late-follow-up.
Healthy controls(n=20)
AT-Normal EF patients
(n=15)
AT-Low EF patients
(n=18) P value†
General characteristicsAge, years 47±17 52±14 45±19 0.7Male gender, n (%) 13 (65) 8 (53) 12 (66) 0.7Resting heart rate, beats/min 64±9 64±11 67±13 0.7Estimated GFR, ml/min 97±15 94±11 103±19 0.2Height, cm 174±11 171±8 172±9 0.8Weight, kg 73±12 75±15 75±18 0.8Body mass index, kg/m2 24±3 25±4 25±5 0.4Months post-ablation - 73±28 57±41 0.2
Co-morbidities, n (%)*Coronary artery disease 0 (0) 0 (0) 2 (11) 0.2Diabetes 0 (0) 1 (7) 0 (0) 0.3Hypertension 0 (0) 2 (13) 2 (11) 0.2
Cardiac medications, n (%)*ACE-inhibitor 0 (0) 2 (13) 3 (17) 0.1
-blocker 0 (0) 0 (0) 3 (17) 0.1AT Patient characteristics
Mean pre-abation heart rate on 24-h holter (beats/min) - 115±22 127±33 0.5
Duration of tachycardia symptoms (months) - 76±59 66±102 0.8
Tachycardia cycle length (ms) - 481±90 484±130 1.0Index EF (%) - 60±6 36±12 <0.001Early post-ablation EF (%) - - 56±6 -Late post-ablation follow-upduration (months) - 75±28 56±41 0.2
*No subjects had other cardiovascular co-morbidities or were prescribed other cardiac medications. †For comparisons across 3 groups, 1-way analysis of variance (ANOVA) with Bonferroni correction was used for continuous variables. Comparisons between 2 groups were made using Student’s t test. Fishers Exact test was used for categorical variables.
57±41 0.0.0.0 22
2 (1(1111111)))) 0.0.00 220 (0000)))) 0000 3
s 2mi 1r 1
e 5
( th ) 8
sionononon 0 (0) 2 (13) 2 (11) 0.2meeeedididiications,sss nnn ((((%))%)**ibbbib tttot r 000 (0) 22 2 (1(1(1133) 3 (1(1(17) 000.1r 000 (0(( ))) 00 (0(0(00))) 3 (1(1(1(17) 000.1t chhhararracacactttet riii ttstiici s-abatatatatioioionn n hehehearararrt t t rararar tetetee ooon nnner (((bebbb at /s// imiin)n)n) -- 111111115±5±5±5±2222222 121212127±7±7±7±3333333 0.5
of tachyccccarararrdidididia a a (( thh )) - 7676767 ±5±5±5± 999 9 66666666±1±1±1±102020202 0.0.88 by guest on June 17, 2018
http://circep.ahajournals.org/D
ownloaded from
DOI: 10.1161/CIRCEP.113.000515
23
Table 2. Systolic Function, Morphology, and Fibrosis on CMR at Late Follow-up.
Healthy controls (n=20)
AT-Normal EF patients
(n=15)
AT-Low EFpatients (n=16)*
Pvalue†
LV ejection fraction, % 64±4 65±4 60±6‡§ <0.05LV end-diastolic volume, ml 161±38 162±37 183±43 0.2LV end-systolic volume, ml 60±19 58±18 75±22 0.06LV mass, g 105±33 100±33 102±34 1.0LA volume, ml 76±19 75±17 80±23 0.4LV end-diastolic volume index, ml/m2 84±14 85±16 102±34‡§ <0.05
LV end-systolic volume index, ml/m231±7 30±8 41±11‡§ <0.01
LV mass index, g/m2 55±15 52±16 56±17 0.9LA volume index, ml/m2 41±10 39±8 45±15 0.4Delayed enhancement, n (%) 0 (0) 0 (0) 0 (0) 1.0Global corrected T1 time (ms) 506±61 480±76 442±53‡ <0.05*Of 18 AT-Low EF patients, 2 had implantable cardioverter-defibrillators precluding CMR. †One-way analysis of variance (ANOVA) with Bonferroni correction was used for continuous variables. Fishers Exact test was used for categorical variables. ‡Significant difference compared to controls. §Significant difference compared to AT-Normal EF patients.
Table 3. Univariate and Multivariate Predictors of Ventricular T1 Time in Patients with Tachycardia-mediated Cardiomyopathy.
Univariate Model Multivariate Model*B SE B P value B SE B P value
Age (years) 0.40 40.43 0.64 0.73 0.53 0.20Mean pre-ablation heart rate on 24-h holter (beats/min)
-0.56 0.54 0.33 0.18 0.44 1.00
AT symptom duration (months) -2.97 1.66 0.10 -0.38 0.14 <0.05
Index EF (%) -1.62 1.55 0.32 -0.51 1.04 0.64Post-ablation
follow-up (months) 0.27 0.37 0.48 0.50 0.25 0.07
*Adjusted R2=0.28.
41±11‡§ <<56565656±1±1±1±17777454545±1±1±1155550000 (0(0(0(0))))( ) ( ) ( ) ( )
r <L wvariance (ANOVA) with Bonferroni correction was used for continuous variables. Fishe
w fi
( ) ( ) ( ) ( )recccctetetetedd dd T1 titttimemee (((m( s) 506±6111 480±76777 442±53‡ <LLLLowww EF patitiiennentststs,, 2 22 hahahahad d dd imimimmplplplplanananntatatatablblblleee caardrdrdrdioiovertrter-dedededefififif brbrbrb illalalaatooorsrs ppprerreclududududinininingg g CMCMCMCMR.R.R.R ††††OnOnOnOne-wvaaaariiiiance (ANOVVA) wwith BoBoBoonferronnni corrreeectioonn was s s usususused fffororor conntiinuuuouuus vaaarirrr ababa leles. FFFissshe
was ss ususused forrr ccccategegoricaal vararariaiaiablb esesses. ‡‡‡SiSiS gngngniifi iiicannt difffff eeerennnncce cccommmmpapap reed tototot cccontrtrtrtroolo s. §§§Signgngnifiompaarerereddd tttot ATATAT-NNNorm llal EFFF papatttit ents.
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from

DOI: 10.1161/CIRCEP.113.000515
24
Table 4. Diastolic Parameters on Echocardiography at Late Follow-up.
Healthy controls(n=20)
AT-Normal EF patients
(n=15)
AT-Low EF
patients (n=18)
P value
LV ejection fraction, % 66±5 66±5 60±8*† <0.01Fractional shortening, % 36±6 41±5 32±7*† <0.01Mitral E velocity, cm/s 0.7±0.2 0.7±0.1 0.7±0.2 0.2Mitral A velocity, cm/s 0.6±0.2 0.6±0.1 0.5±0.2 0.5E/A ratio 1.4±0.5 1.5±0.6 1.5±0.6 0.9Left atrial diameter, cm 3.4±0.4 3.6±0.6 3.6±0.5 0.4Mitral E wave deceleration time, ms 193±39 199±50 206±37 0.6
Septal e’ velocity, cm/s 9.0±0.6 8.9±0.6 9.3±0.9 0.9Lateral e’ velocity, cm/s 12.0±3.9 11.4±3.6 11.5±5.0 0.9Mean e’ velocity, cm/s 10.5±3.0 10.1±2.8 10.4±4.1 1.0Septal E/e’ ratio 8.7±3.0 8.6±1.5 7.7±2.8 0.5Lateral E/e’ ratio 6.5±2.0 7.0±1.9 6.4±2.2 0.7Mean E/e’ ratio 7.4±2.3 7.6±1.6 6.8±2.1 0.6
*Significant difference compared to controls. †Significant difference compared to AT-Normal EFpatients.
Table 5. Systolic and Diastolic Indices on Speckle Tracking Analysis at Late Follow-up.
Healthy controls (n=20)
AT-Normal EF patients
(n=15)
AT-Low EFpatients (n=18)
Pvalue
Systolic functionGRS, % 44.1±11.9 41.7±13.6 38.1±14.4 0.4GRSr, 1/s 1.9±0.4 2.0±0.4 1.8±0.4 0.2GCS, % -20.8±1.5 -22.4±2.4 -17.9±3.9* <0.01GCSr, 1/s -1.5±0.3 -1.7±0.2 -1.5±0.2 0.7GLS, % -21.1±1.4 -21.4±1.9 -19.3±2.3* <0.01GLSr, 1/s -1.2±0.2 -1.2±0.2 -1.1±0.2 0.2Twist, degrees 10.8±5.5 13.1±5.2 9.2±4.3 0.6Twist rate, degrees/s 90±32 98±25 72±29*† <0.05
Diastolic functionGEDSr, 1/s 1.8±0.2 1.7±0.3 1.5±0.3* <0.05Untwist, degrees -1.8±0.9 -1.6±0.8 -2.2±1.5 0.3Untwist rate, degrees/s -88±39 -86±58 -83±40 0.9
*Significant difference compared to controls. †Significant difference compared to AT-Normal EF patients. GRS(r) – global radial strain (rate), GCS(r) – global circumferential strain (rate), GEDSr –global early diastolic strain rate, GLS(r) – global longitudinal strain (rate).
±0.9 0.9±5±5±5±5.00.00 0.0.0.0.9999±4.11 1.111 0000±2 8 0000 5555
/et
ystolic and Diastolic Indices on Speckle Tracking Analysis at Late Follow up
/e’ rrrratatatatioioioo 6.5±2.0 7.777 0±1.9 6.4±4±4±4 2.2 0.7e’ raaaatio 7.77.7 4±±4±2.22 3 77.6±±±1.1.1.6666 6.66 8±8±8±±2.1 0.0.0 6666t diffffference compmparedededd to cococontrolls. †††SSignniffficannt difffffffererererenenenencce cccooompaareed totto AT---NNoN rmrmal EEEEFFFF
systotolililicc ananddd DiDiDiasastotolililicc InIndididicecess onon SSpepe kckckllele TTrara kckckiiningg AnAn lalal sysiisis atat LLatatee FoFolllllloow upp
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from
Kaye, James Hare, Peter Kistler and Andrew TaylorLiang-han Ling, Jonathan Kalman, Andris Ellims, Leah Iles, Caroline Medi, Craig Sherratt, David
Following Successful AblationDiffuse Ventricular Fibrosis is a Late Outcome of Tachycardia-Mediated Cardiomyopathy
Print ISSN: 1941-3149. Online ISSN: 1941-3084 Copyright © 2013 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Arrhythmia and Electrophysiology
published online July 30, 2013;Circ Arrhythm Electrophysiol.
http://circep.ahajournals.org/content/early/2013/07/30/CIRCEP.113.000515World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circep.ahajournals.org//subscriptions/
is online at: Circulation: Arrhythmia and Electrophysiology Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answerinformation about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Arrhythmia and Electrophysiology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 17, 2018http://circep.ahajournals.org/
Dow
nloaded from