diagnostic decision making: do counselors delay final judgments?
TRANSCRIPT
J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 998
ASSESSMENT & DIAGNOSIS
Spengler and his colleagues (1995) conceptualized delayed decision making within the context of a scientist–practitioner model of assessment. The model was developed to help counselors improve their clinical judgment during the assessment pro-
cess. An informed method of conducting psychological as-sessment was sorely needed because counselors commit awide array of judgmental and inferential errors during as-sessment and counseling (Dumont, 1993; Dumont &Lecomte, 1987; Faust, 1986; Spengler et al., 1995). Researchon clinical judgment has indicated that counselors fail to usebase rates (Perlick & Atkins, 1984), engage in diagnostic andtreatment overshadowing (Spengler, Blustein, & Strohmer,1990; Walker & Spengler, 1995), exhibit age (James & Haley,1995; Meeks, 1990) and health (James & Haley, 1995) bi-ases, limit themselves to confirmatory hypothesis testing(Haverkamp, 1993), form hypotheses from inferences treatedas facts (MacDonald, 1996), and retain early diagnostic im-pressions even when confronted with disconfirmatory evi-dence (Elstein, Shulman, & Sprafka, 1978).
Identifying ways that counselors err during the appraisalprocess is vital to improving assessment, treatment, andoutcome. However, generating strategies to ameliorateclinical judgment problems is equally important. Severalmethods, or “debiasing strategies,” have been offered to
encourage sound clinical decision making (Hill & Spengler,1997; Hillman, Stricker, & Zweig, 1997; Spengler et al., 1995).These strategies are theoretically linked to the nature of theirrespective judgmental biases. For example, Elstein et al.(1978) found that clinicians formed diagnostic conclusionsearly in the assessment process. These diagnostic impressionswere very resistant to change, even when contradictoryevidence emerged during subsequent clinical encounters.Spengler et al. (1995) suggested a debiasing strategy thatis directly linked to these findings: delay final judgments.This activity was recognized as a component of cogni-tive complexity almost 30 years earlier (Bieri et al., 1966).Incidentally, Elstein et al. (1978) found that the mostaccurate clinicians arrived at their final diagnoses laterthan those who were less accurate.
Although there is a theoretical, empirical rationale war-ranting the delay of diagnostic decision making, it is un-known whether this debiasing strategy is actually imple-mented in counseling practice. There are two reasons thisquestion may not be a popular subject of research. First,not all counseling researchers agree with the concept ofdiagnostic classification (Ginter, 1989; J. S. Hinkle, 1999;Ivey & Ivey, 1998). It is unlikely that delayed diagnoses areinvestigated if the investigator does not believe in assigningthem. However, diagnostic classification has become so
Carrie L. Hill is a doctoral candidate in the Department of Counseling and Educational Psychology at Indiana University in Bloomington. Charles R. Ridleyis a professor in the Department of Counseling and Educational Psychology at Indiana University in Bloomington. Correspondence regarding this article shouldbe sent to Charles R. Ridley, Department of Counseling and Educational Psychology, 201 N. Rose Avenue, Indiana University, Bloomington, IN 47405 (e-mail:[email protected]).
Diagnostic Decision Making: Do Counselors DelayFinal Judgments?
Carrie L. Hill and Charles R. Ridley
Although there is a theoretical, empirical rationale warranting the delay of diagnostic decision making, it is unknown whether thisdebiasing strategy is actually implemented in counseling practice. This study investigated whether counselors delayed theirdiagnostic decisions in a setting that allowed them the option of doing so. Clinical records were selected from a counselor trainingcenter at a large midwestern university and coded for delayed diagnostic decision making. Three pairs of chi-square analyseswere performed. Results indicated that delayed diagnostic decision making occurred to a greater extent than immediate diagnos-tic decision making across counselor–client dyads, counselors, and clients.
Delaying final judgments allows a counselor to reflect on and extend the assessment process, test alternative hypotheses, and invoke a self-correcting model open to new client data and explanations. (Spengler, Strohmer, Dixon, & Shivy, 1995, p. 524)

J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9 99
Diagnost ic Decis ion Making
widely used that it is difficult to communicate amongcolleagues or referral sources without them. In addition,the proliferation of empirically validated treatments forspecific disorders increases the use of accurate diagnos-tic decisions. Although diagnosis is only one element ofa comprehensive assessment (e.g., an assessment also in-cludes judgments about severity, prognosis, strengths, andsocial supports; Ridley, Li, & Hill, 1998), it undeniablyaffects the course of treatment. This, above any otherreason, mandates an investigation into whether counse-lors make sound diagnostic decisions using strategies suchas delayed decision making.
Second, the influx of managed mental health care maybreed skepticism about the possibility of counselors actu-ally having the freedom to delay diagnostic judgments. Manyinsurance companies demand that counselors report diag-nostic codes as soon as possible after the first session. Itmay seem futile to research a debiasing strategy that seemsto be prohibited in many clinical settings. Nevertheless,counselors can still consciously delay their decision makingwhile complying with guidelines set by the managed carecompany. The decision simply remains tentative in thecounselor’s mind, and necessary changes are recorded as amore comprehensive and reliable decision is made over time.Although this solution is still wrought with problems, atleast it helps the counselor maintain a higher degree ofethical integrity. In addition, research on delayed decisionmaking may yield important findings that could affect man-aged care policies, such as how soon diagnostic decisions mustbe reported. This research would be especially provocativeif it indicated that counseling was more cost-effective whencounselors were not forced to make premature decisionsabout diagnosis.
Although it is becoming less common, some counselingsettings still do not require immediate diagnostic decisions.For example, counselor training sites for graduate studentsin counseling often do not have strict guidelines for diagnos-tic reporting. Counselors at these sites have the option todelay their final judgments about clients’ diagnoses. For thisreason, counselor training sites provide fertile ground forconducting research on delayed diagnostic decision making.
This study investigated whether counselors delayed theirdiagnostic decisions in a setting that allowed them the op-tion of doing so. Because no prior research guided a direc-tional hypothesis about this question, a hypothesis of nodifference was proposed. Therefore, counselors were ex-pected to exhibit no difference between the extent of theirdelayed diagnostic decision making and the extent of theirimmediate diagnostic decision making. Knowing the extentto which counselors delay their diagnostic decisions can gen-erate testable hypotheses for future research about clinicaljudgment processes during assessment. In this way, the ques-tion of this investigation seeks an answer that is essentialfor further research in this area. This study did not attemptto determine whether final diagnoses were accurate. It wasexpected that delayed decision making could sometimesresult in inaccurate diagnoses, and hasty decisions could
sometimes coincidentally result in accuracy. However, thetheoretical and empirical support undergirding delayed di-agnostic decision making warrants its regular use to achieveoverall veracity in assessment and counseling. Therefore,the study focused on an assessment process variable, diag-nostic decision making, rather than an assessment outcomevariable (e.g., diagnostic accuracy). Both Falvey (1992) andLopez (1989) emphasized the need to move away fromoutcome research and to evaluate clinical judgment activ-ity over time.
This study was conducted under the presupposition thatthe scientist–practitioner model is valuable to assessment.Pepinsky and Pepinsky (1954) introduced the scientificapproach to counseling over 40 years ago. Spengler et al.(1995) developed this fundamental approach into a sophisti-cated model of assessment. The model includes severaldebiasing strategies to be implemented throughout the as-sessment process. One of these strategies is delayed deci-sion making. It would be difficult to argue that counselorsare invoking a scientific model in their practice if they arearriving at diagnostic decisions immediately. Even the mostefficient and competent counselor would find it impossibleto gather sufficient client data, formulate tenable workinghypotheses, assess their validity through confirmatory anddisconfirmatory hypotheses testing, revise the working hy-potheses by using a self-correcting mechanism, and arrive ata valid assessment decision, all after approximately 1 hour ofclinical contact. Therefore, this study could be described as asearch for an indicator of a scientist–practitioner approachto assessment.
METHOD
This archival study used client records from a counselor train-ing center at a large midwestern university. Archival researchis “firmly established as a research tradition in the behavioralsciences” (Dane, 1990, p. 169). More specifically, the dataused in this study were particularly appropriate for clinicaljudgment research because they were not vulnerable to thetwo problems Falvey and Hebert (1992) recognized in sev-eral clinical judgment research studies. The first problem isthat the validity of data acquired about counselors’ clinicaljudgment are often threatened because the counselors mustrely on identified response options rather than exercisingclinical judgment as it naturally occurs in counseling set-tings. This study avoided the problem by examining natu-rally produced data. The second problem is ironically relatedto the first. Unfortunately, naturally occurring data areoften unstructured, making data coding less reliable. In thisinvestigation, coding was reliable despite the data’s naturalgeneration because the format of the clinical records wasalready structured for clinical purposes.
Clinical Records
The investigator (first author) obtained permission fromthe director of the counselor training center to access the

J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9100
Hi l l and Rid ley
clinical records. After interviewing the director and readingseveral editions of the center’s operating manual, it was dis-covered that the center’s policy on reporting client diag-noses had been consistent over a 2-year period. Counselorswere required to complete a case note after each counsel-ing session. A space for a multiaxial diagnosis was providedon each case note. Counselors had three options when fill-ing out a case note: (a) supply a final diagnosis, (b) report atentative decision, or (c) leave the space blank. A final diag-nosis was not required until the treatment plan was written(i.e., before the fifth session). Therefore, counselors had fouropportunities to delay and formulate their diagnostic deci-sion making about each client.
While the training center consistently conveyed its policyabout diagnostic reporting, counseling supervisors some-times advised their students differently regarding diagnos-tic decision making. For example, some supervisors preferredthat their students refrain from ever assigning diagnosesto their clients. Because supervisors’ instructions took pre-cedence over the training center’s policy, some counse-lors’ clinical records may not have accurately reflected theiractual decision-making patterns. To address this complica-tion, all of the clinical records chosen for analysis were theresponsibility of the same supervisor. This supervisor, whosupervised students over a 2-year period, did not superim-pose separate diagnostic guidelines. Rather, the supervi-sor advised counselors to follow the policy set forth bythe training center. In addition, records were only chosenif at least four sessions transpired between a particularcounselor–client dyad so that each record reflected deci-sions that were made when a maximum opportunity wasgiven to delay final judgments. Thirty-five clinical recordsmet the criteria of the study.
Procedure
Demographic data were recorded for each counselor (e.g.,age, level of graduate training, race/ethnicity, sex) and eachclient (e.g., age, race/ethnicity, sex) for the sole purpose ofdescribing the sample. The study of personal and demo-graphic variables has been a “misdirected and unfruitfuleffort that has, unfortunately, persisted in clinical judgmentresearch” (Strohmer & Spengler, 1993, p. 471). Such re-search does not inform the field about where counselors gowrong in the clinical judgment process or how judgmentscan be improved. Therefore, this study did not focus on thepersonal or demographic variables of the counselors or cli-ents. Instead, it examined the process variable of delayeddecision making.
Each clinical record received three codes. The first codewas a number assigned to the counselor. The second codewas a number assigned to the client. These codes were as-signed because counselors and clients sometimes appearedon multiple records (i.e., several counselors saw more thanone client during their training, and some clients were seenby more than one counselor if they continued services acrosssemesters). The third code reflected diagnostic decision
making. A score was assigned corresponding to the numberof times the counselor delayed a final judgment about theclient’s diagnosis (e.g., 0 = final diagnosis reached after onesession, 1 = final diagnosis reached after two sessions). Adelayed judgment was defined as one of four reportings onAxis I or II: (a) a blank, (b) a deferment, (c) a tentative orprovisional diagnosis, or (d) a rule out. In addition to thethree codes, final diagnostic decisions were noted for eachclinical record.
RESULTS
Thirteen counselors were represented among the 35 clini-cal records. Eighty-five percent of the counselors were fe-male (n = 11), whereas 15% were male (n = 2). Two coun-selors were master’s students in counseling, whereas theother 11 counselors were doctoral students in counselingpsychology. The average age of the counselors was 28. Ninecounselors were Caucasian, 3 were African American, and1 was of Hispanic background.
Thirty-one clients were represented among the 35 clini-cal records. Sixty-one percent of the clients were female (n= 19), whereas 39% were male (n = 12). The average age ofthe clients was 31. Counselors did not always report theirclients’ race or ethnicity. However, 17 clients were describedas Caucasian, 2 were described as Hispanic, 1 was describedas African American, and 1 was described as Iranian.
Three pairs of chi-square analyses were performed toexamine the nominal data in light of the following researchquestion: To what extent do counselors delay their diag-nostic decision making when given the option of doing so?The first pair of chi-square analyses investigated diagnosticdecision making across counselor–client dyads. The secondpair investigated diagnostic decision making across counse-lors. The third pair investigated diagnostic decision makingacross clients. Within each pair, the first chi-square entailedcollapsing the four degrees of delayed decision making intoone category and comparing it to immediate decision mak-ing. The second chi-square was used to investigate moresubtle differences in decision making and did not collapsethe four degrees of delayed decision making into one cat-egory. Instead, the degrees of delayed decision making werecompared with each other as well as with immediate diag-nostic decision making.
Counselor–Client Dyads
This pair of chi-square analyses investigated all 35 recordsas a total reflection of diagnostic decision making acrosscounselor–client dyads. The first chi-square of this pair com-pared cases that received immediate diagnostic decisions(i.e., code = 0) with cases that received delayed decisions(i.e., code = 1, 2, 3, or 4). In other words, records that re-ceived delayed decisions to any degree were collapsed intoa single category (see Table 1). Only two records reflectedimmediate diagnostic decision making, whereas 33 reflecteddelayed judgments to some degree. The chi-square value

J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9 101
Diagnost ic Decis ion Making
was significant, χ² = 27.46 (p < .001). Across all counselor–client dyads, the null hypothesis was rejected. The conclu-sion is that immediate and delayed decision making did notoccur to the same extent and that the increased frequencyof delayed decision making was not attributable to chancefluctuations.
The second chi-square of this pair was used to look formore subtle differences in frequency among decision-making codes (i.e., 0, 1, 2, 3, or 4). In other words, degreesof delayed decision making were not collapsed into onecategory but were compared separately along with immedi-ate diagnostic decision making (see Table 2). The chi-squarevalue was significant, χ² = 58.02 (p < .001), indicating thatacross all counselor–client dyads the null hypothesis wasrejected. The conclusion is that the five categories of deci-sion making did not occur to the same extent and that thedifferences in frequency were not attributable to chancefluctuations. To determine which categories were majorcontributors to the significant chi-square value, standard-ized residuals were calculated. When a standardized residualis greater than 2.00 (in absolute value), it can be concludedthat it is a major contributor (D. E. Hinkle, Wiersma, &Jurs, 1994). In this chi-square analysis, only the highest de-gree of delayed decision making (i.e., code = 4) was a majorcontributor to the significant finding.
Counselors
Another pair of chi-square analyses investigated the 13counselors as a reflection of diagnostic decision making
across counselors. Average codings were calculated for eachcounselor based on all of the decision-making codes assignedto the counselor. For example, Counselor 8 saw two clients,and received decision-making codes of 3 and 2 for these cli-ents, respectively. Therefore, the average decision-makingcode for Counselor 8 is the average of 3 and 2, or 2.5.
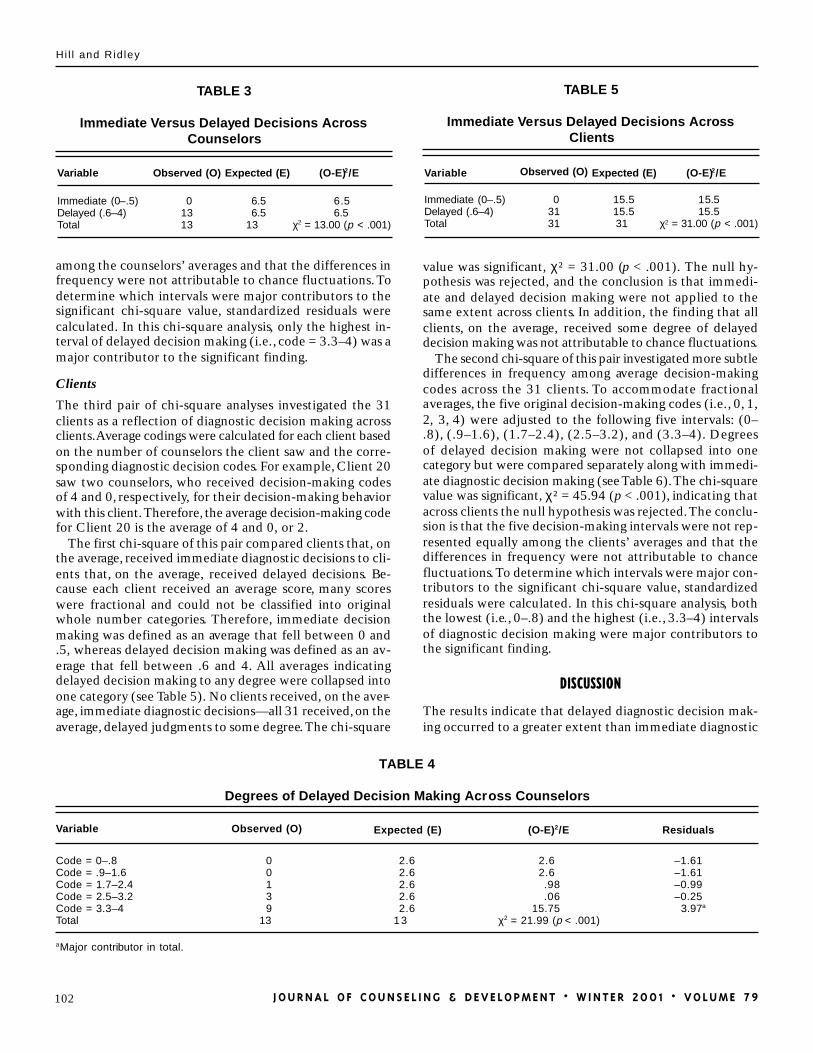
The first chi-square of this pair compared counselors that,on the average, made immediate diagnostic decisions withcounselors that, on the average, made delayed decisions.Because each counselor received an average score, manyscores were fractional (e.g., 2.5) and did not neatly fall intothe original whole number categories (e.g., 0, 1, 2). To ac-commodate these fractional averages, immediate decisionmaking was defined as an average that fell between 0 and.5, whereas delayed decision making was defined as an av-erage that fell between .6 and 4. Note that all averages indi-cating delayed decision making to any degree were collapsedinto one category (see Table 3). No counselors exhibited,on the average, immediate diagnostic decision making—all13 exhibited, on the average, delayed judgments to somedegree. The chi-square value was significant, χ² = 13.00 (p< .001). In other words, across counselors, the null hypoth-esis was rejected. The conclusion is that immediate anddelayed decision making did not occur to the same extentacross counselors’ average performance. Furthermore, thefinding that all counselors, on the average, displayed somedegree of delayed decision making was not attributable tochance fluctuations.
The second chi-square of this pair was used to searchfor more subtle differences in frequency among averagedecision-making codes across the 13 counselors. To ac-commodate fractional averages, the five original decision-making codes (i.e., 0, 1, 2, 3, 4) were adjusted to the fol-lowing five intervals: (0–.8), (.9–1.6), (1.7–2.4), (2.5–3.2),and (3.3–4). Note that degrees of delayed decision makingwere not collapsed into one category but were comparedseparately along with immediate diagnostic decision mak-ing (see Table 4). The chi-square value was significant, χ² =21.99 (p < .001), indicating that across counselors, the nullhypothesis was rejected. The conclusion is that the fivedecision-making intervals were not represented equally
TABLE 1
Immediate Versus Delayed Decisions AcrossAll Records
Variable Observed (O) Expected (E) (O-E)2/E
Immediate (0)Delayed (1, 2, 3, 4)Total
23335
17.517.535
13.7313.73
χ2 = 27.46 (p < .001)
TABLE 2
Degrees of Delayed Decision Making Across All Records
Variable Observed (O) Expected (E) (O-E)2/E Residuals
Code = 0Code = 1Code = 2Code = 3Code = 4Total
2323
2535
77777
35
3.572.293.572.29
46.30χ2 = 58.02 (p < .001)
–1.89–1.51–1.89–1.51
6.80a
aMajor contributor in total.
J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9102
Hi l l and Rid ley
among the counselors’ averages and that the differences infrequency were not attributable to chance fluctuations. Todetermine which intervals were major contributors to thesignificant chi-square value, standardized residuals werecalculated. In this chi-square analysis, only the highest in-terval of delayed decision making (i.e., code = 3.3–4) was amajor contributor to the significant finding.
Clients
The third pair of chi-square analyses investigated the 31clients as a reflection of diagnostic decision making acrossclients. Average codings were calculated for each client basedon the number of counselors the client saw and the corre-sponding diagnostic decision codes. For example, Client 20saw two counselors, who received decision-making codesof 4 and 0, respectively, for their decision-making behaviorwith this client. Therefore, the average decision-making codefor Client 20 is the average of 4 and 0, or 2.
The first chi-square of this pair compared clients that, onthe average, received immediate diagnostic decisions to cli-ents that, on the average, received delayed decisions. Be-cause each client received an average score, many scoreswere fractional and could not be classified into originalwhole number categories. Therefore, immediate decisionmaking was defined as an average that fell between 0 and.5, whereas delayed decision making was defined as an av-erage that fell between .6 and 4. All averages indicatingdelayed decision making to any degree were collapsed intoone category (see Table 5). No clients received, on the aver-age, immediate diagnostic decisions—all 31 received, on theaverage, delayed judgments to some degree. The chi-square
value was significant, χ² = 31.00 (p < .001). The null hy-pothesis was rejected, and the conclusion is that immedi-ate and delayed decision making were not applied to thesame extent across clients. In addition, the finding that allclients, on the average, received some degree of delayeddecision making was not attributable to chance fluctuations.
The second chi-square of this pair investigated more subtledifferences in frequency among average decision-makingcodes across the 31 clients. To accommodate fractionalaverages, the five original decision-making codes (i.e., 0, 1,2, 3, 4) were adjusted to the following five intervals: (0–.8), (.9–1.6), (1.7–2.4), (2.5–3.2), and (3.3–4). Degreesof delayed decision making were not collapsed into onecategory but were compared separately along with immedi-ate diagnostic decision making (see Table 6). The chi-squarevalue was significant, χ² = 45.94 (p < .001), indicating thatacross clients the null hypothesis was rejected. The conclu-sion is that the five decision-making intervals were not rep-resented equally among the clients’ averages and that thedifferences in frequency were not attributable to chancefluctuations. To determine which intervals were major con-tributors to the significant chi-square value, standardizedresiduals were calculated. In this chi-square analysis, boththe lowest (i.e., 0–.8) and the highest (i.e., 3.3–4) intervalsof diagnostic decision making were major contributors tothe significant finding.
DISCUSSION
The results indicate that delayed diagnostic decision mak-ing occurred to a greater extent than immediate diagnostic
TABLE 3
Immediate Versus Delayed Decisions AcrossCounselors
Variable Observed (O) Expected (E) (O-E)2/E
Immediate (0–.5)Delayed (.6–4)Total
01313
6.56.5
13
6.56.5
χ2 = 13.00 (p < .001)
TABLE 5
Immediate Versus Delayed Decisions AcrossClients
Variable Observed (O) Expected (E) (O-E)2/E
Immediate (0–.5)Delayed (.6–4)Total
03131
15.515.531
15.515.5
χ2 = 31.00 (p < .001)
TABLE 4
Degrees of Delayed Decision Making Across Counselors
Variable Observed (O) Expected (E) (O-E)2/E Residuals
Code = 0–.8Code = .9–1.6Code = 1.7–2.4Code = 2.5–3.2Code = 3.3–4Total
00139
13
2.62.62.62.62.6
13
2.62.6.98.06
15.75 χ2 = 21.99 (p < .001)
–1.61–1.61–0.99–0.25
3.97a
aMajor contributor in total.

J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9 103
Diagnost ic Decis ion Making
decision making across counselor–client dyads, counselors,and clients. The highest level of delayed decision makingwas a major contributor to the significant findings forcounselor–client dyads and counselors. In other words,across counselor–client dyads and across counselors, thephenomenon of delaying diagnostic decisions for as long aspossible occurred significantly more often than expected.Both the lowest and highest levels of diagnostic decisionmaking were major contributors to the significant findingfor clients. In other words, across clients, the phenomenonof reaching immediate diagnostic decisions occurred sig-nificantly less often than expected, whereas the phenom-enon of delaying diagnostic decisions for as long as possibleoccurred significantly more often than expected.
The results are encouraging in light of the research ques-tion: To what extent do counselors delay their diagnosticdecision making when given the option of doing so? It seemsthat the counselors in this study delayed their judgments asignificant amount of the time and often for the maximumtime possible. However, it is important to consider thethought processes underlying the behaviors exhibited inthe case notes. For example, 25 among the 35 total recordsshowed delayed diagnostic decision making for the maxi-mum amount of time (i.e., code = 4). Nineteen of these 25records included a treatment plan that was completed af-ter the fourth session. Only 9 of the 19 treatment plans(47%) included final diagnostic decisions. The 10 remain-ing treatment plans (53%) displayed delayed decisions, de-spite the requirement for a final decision. These findingsraise important questions that need further research. Werethese counselors intentionally delaying their decision mak-ing to improve their diagnoses? Were they simply not think-ing about diagnostic decisions? Were they in a quandaryabout how to make diagnostic decisions and thus possiblyavoiding decision making altogether? If the counselors wereintentionally delaying their decision making, what was thenature of their thought processes? At what point has a di-agnostic decision been delayed so long that it is no longer auseful strategy?
The generalizability of the results may be limited due tothe low number of counselors, clients, and counselor–clientdyads. In addition, all of the counselors were in training.Due to the small number of master’s students relative to
doctoral students, no attempt was made to ascertain thedifferential effects of training. It would be helpful to studydiagnostic decision making among counselors with varyinglevels of training and experience, as well as conduct studieswith a higher number of participants. A potential problemwith this suggestion is that it may be difficult to locate coun-seling sites that allow, would agree to allow, or would en-courage their counselors to exercise the option of delayingtheir diagnostic decisions. The problem is exacerbated byour current managed care environment that emphasizesbrief interventions.
The validity of using clinical case notes as indicators ofdelayed diagnostic decision making is unknown. Counse-lors may not always reflect their decision-making processesin clinical records for various reasons, such as external de-mands. However, because the counselors in this study weregiven the option to delay their diagnostic decisions, the clini-cal records may adequately reflect the phenomenon of in-terest. It would be interesting to use other methods andindicators to study diagnostic decision making, such as quali-tative methods that probe counselors’ subjective experi-ences of their clinical assessments to acquire more person-alized indicators of diagnostic decision-making processes.
Diagnostic decisions are not the only type of judgmentsmade during assessment and counseling. As previously men-tioned, a comprehensive assessment also includes decisionsabout problem severity, prognosis, strengths, and social sup-ports. Further research is needed to determine the extentto which counselors delay their decisions about these otherimportant client variables and how the timing of differenttypes of clinical decisions interact with each other and in-fluence overall clinical judgment.
Finally, delayed decision making is not the only debiasingstrategy available to counselors. Other debiasing strategiesinclude using base rates, generating alternative clinical hy-potheses, and testing hypotheses with disconfirmatorymethods (Spengler et al., 1995). The investigation of de-layed decision making is only one piece of a larger puzzle.Further research is needed on counselors’ usage of otherdebiasing strategies to obtain a comprehensive picture ofwhen and how judgmental and inferential errors occur. Thisinformation could be useful for training programs that wantto improve their ability to develop more effective counse-
TABLE 6
Degrees of Delayed Decision Making Across Clients
Variable Observed (O) Expected (E) (O-E)2/E Residuals
Code = 0–.8Code = .9–1.6Code = 1.7–2.4Code = 2.5–3.2Code = 3.3–4Total
0244
2131
6.26.26.26.26.2
31
6.22.850.780.78
35.33χ2 = 45.94 (p < .001)
–2.49a
–1.69–0.88–0.88
5.94a
aMajor contributor in total.

J O U R N A L O F C O U N S E L I N G & D E V E L O P M E N T • W I N T E R 2 0 0 1 • V O L U M E 7 9104
Hi l l and Rid ley
lors by addressing common clinical judgment pitfalls andcorresponding debiasing strategies.
In light of the study’s limitations, the results indicatedthat counselors delayed their judgments a significant amountof the time and often for the maximum time allowed. Thestudy addressed a basic question and helped establish theexistence of a clinical phenomenon. The phenomenon ofdelayed diagnostic decision making must now be exploredin greater depth, through a variety of methods, and in rela-tion to a number of other variables and strategies, to morefully understand the phenomenon’s impact on the practiceand outcome of assessment and counseling. The new re-search agenda can move beyond asking the question, “Docounselors delay final judgments?” to asking the question,“How do counselors delay final judgments?”
REFERENCE
Bieri, J., Atkins, A. L., Briar, S., Leaman, R. L., Miller, H., & Tripodi, T.(1966). Clinical and social judgment: The discrimination of behavioralinformation. New York: Wiley.
Dane, F. C. (1990). Research methods. Pacific Grove, CA: Brooks/Cole.Dumont, F. (1993). Inferential heuristics in clinical problem formula-
tion: Selective review of their strengths and weaknesses. ProfessionalPsychology: Research and Practice, 24, 196–205.
Dumont, F., & Lecomte, C. (1987). Inferential processes in clinical work:Inquiry into logical errors that affect diagnostic judgments. Profes-sional Psychology: Research and Practice, 18, 433–438.
Elstein, A. S., Shulman, A. S., & Sprafka, S. A. (1978). Medical problemsolving: An analysis of clinical reasoning. Cambridge, MA: HarvardUniversity Press.
Falvey, J. E. (1992). Science or serendipity? What we know about clini-cal judgment in mental health. Journal of Mental Health Counseling,14, 458–470.
Falvey, J. E., & Hebert, D. J. (1992). Psychometric study of the ClinicalTreatment Planning Simulations (CTPS) for assessing clinical judg-ment. Journal of Mental Health Counseling, 14, 490–507.
Faust, D. (1986). Research on human judgment and its application to clini-cal practice. Professional Psychology: Research and Practice, 17, 420–430.
Ginter, E. J. (1989). If you meet Moses/Jesus/Mohammed/Buddha (orassociate editors of theory) on the road, kill them! Journal of MentalHealth Counseling, 11, 335–344.
Haverkamp, B. E. (1993). Confirmatory bias in hypothesis testing forclient-identified and counselor self-generated hypotheses. Journal ofCounseling Psychology, 40, 303–315.
Hill, C. L., & Spengler, P. M. (1997). Dementia and depression: A pro-cess model for differential diagnosis. Journal of Mental Health Coun-seling, 19, 23–39.
Hillman, J. L., Stricker, G., & Zweig, R. A. (1997). Clinical psycholo-gists’ judgments of older adult patients with character pathology:Implications for practice. Professional Psychology: Research and Prac-tice, 28, 179–183.
Hinkle, D. E., Wiersma, W., & Jurs, S. G. (1994). Applied statistics for thebehavioral sciences (3rd ed.). Boston: Houghton Mifflin.
Hinkle, J. S. (1999). A voice from the trenches: A reaction to Ivey andIvey (1998). Journal of Counseling & Development, 77, 474–483.
Ivey, A. E., & Ivey, M. B. (1998). Reframing DSM-IV: Positive strategiesfrom developmental counseling and therapy. Journal of Counseling &Development, 76, 334–350.
James, J. W., & Haley, W. E. (1995). Age and health bias in practicingclinical psychologists. Psychology and Aging, 10, 610–616.
Lopez, S. R. (1989). Patient variable biases in clinical judgment: Con-ceptual overview and methodological considerations. PsychologicalBulletin, 106, 184–203.
MacDonald, G. (1996). Inferences in therapy: Processes and hazards.Professional Psychology: Research and Practice, 27, 600–603.
Meeks, S. (1990). Age bias in the diagnostic decision-making behavior ofclinicians. Professional Psychology: Research and Practice, 21, 279–284.
Pepinsky, H. B., & Pepinsky, P. N. (1954). Counseling theory and practice.New York: The Ronald Press Company.
Perlick, D., & Atkins, A. (1984). Variations in the reported age of a pa-tient: A source of bias in the diagnosis of depression and dementia.Journal of Consulting and Clinical Psychology, 52, 812–820.
Ridley, C. R., Li, L. C., & Hill, C. L. (1998). Multicultural assessment:Reexamination, reconceptualization, and practical application. TheCounseling Psychologist, 26, 827–910.
Spengler, P. M., Blustein, D. L., & Strohmer, D. C. (1990). Diagnosticand treatment overshadowing of vocational problems by personalproblems. Journal of Counseling Psychology, 37, 372–381.
Spengler, P. M., Strohmer, D. C., Dixon, D. N., & Shivy, V. A. (1995). Ascientist-practitioner model of psychological assessment: Implications fortraining, practice, and research. The Counseling Psychologist, 23, 506–534.
Strohmer, D. C., & Spengler, P. M. (1993). Studying mental health coun-selor clinical judgment: A response to Falvey and colleagues. Journalof Mental Health Counseling, 15, 465–474.
Walker, B. S., & Spengler, P. M. (1995). Clinical judgment of major depres-sion in AIDS patients: The effects of clinician complexity and stereo-typing. Professional Psychology: Research and Practice, 26, 269–273.