delivering serious news - garvan institute of …past experiences & attitudes to delivering...
TRANSCRIPT

Delivering Serious News

Definitions of Serious News
Includes communication regarding • Life-threatening illness
• Imminence of death
• Death of a loved one
Definition of serious news • Any information likely to alter drastically a patient’s view
of his or her future (Buckman, 1984)
• Bor et al (1993): feeling of no hope
a threat to a person’s mental or physical well-being,
a risk of upsetting an established lifestyle
fewer choices in his or her life

Types of discussion
Illness/Treatment stage ◦ Diagnosis: early vs advanced disease
◦ Progression
◦ Recurrence
◦ No further active treatment
◦ Terminal care
Factors to consider: ◦ Your relationship with the patient: new versus existing
◦ Age of the patient: older versus younger
◦ Identification within your personal life
◦ Past experiences & attitudes to delivering “bad news”

Exercise
Personal Reflection:
- Rate your average level of discomfort between 0-10
when delivering serious news
- Name 3 thoughts or feelings in relation to the idea
of delivering serious news
- Think about a situation that didn’t go well and why?
- Think about a situation that did go well and why?

Impact on Clinicians Findings from clinician surveys (Ptacek et al, 2001,
Shaw et al, 2013)
◦ Stressful
◦ Difficulties with handling own emotions: Guilt
Sorrow
Identification
Feeling like a failure
Stress can last hours, days
Little evidence that these difficulties ease with experience
Can contribute to burnout

Doctor’s Discomfort when
Delivering Bad News
Where does it come from?
• Feeling responsible for patient’s misfortune
• Perceptions of failure
• Unresolved feelings about death and dying
• Concerns about patient’s response to the
news
• Clinician’s concerns about their own
emotional response to the circumstance

Impact of Delivery on Patients
How bad news is delivered can have a
significant impact on:
◦ Patient’s understanding of their illness
◦ Treatment decisions
◦ Patient’s long-term relationship with clinicians (Rosenbaum et al., 2004)
◦ Patient’s satisfaction with care
◦ Hope and subsequent psychological
adjustment

Impact of Delivery on Patients
Patients are quite critical of how clinicians
deliver serious news
German study: (Seifart et al, 2014)
◦ Only 46% of patients were satisfied with their
clinician’s communication
◦ Inadequate in the areas of:
Addressing emotions
Providing clear explanation of diagnosis
Explaining the course of the disease

But what do patients want?
Individual differences & preferences in
WHAT they want to know
◦ 95% of patients want to be informed of their
diagnosis (Cox et al, 2006)
◦ But large variation in specific details (Cox et al.,
2006; Rutten et al., 2005; Fujimori et al., 2009)
Chances of cure
Effectiveness of cancer treatments
Specific prognosis
◦ Cross-cultural differences

How do we know what patients
want?
Difficult to predict individual preferences
therefore best to ask how much and what
type of information they want

What else do patients want?
HOW the news is delivered is critical
Doctor’s caring attitude was more important than the information provided during the clinical encounter (Siminoff et al., 1989)
Sydney Study: 100 women, early breast cancer (Lobb et
al, 2001)
◦ 91% wanted to know their prognosis, but 63% wanted the clinician to check with them first
◦ Majority wanted: Clinician to check their understanding
Opportunity to ask questions
Explain medical terms
Emotional support (79%)
Their fears & concerns listened to (97%)

What’s Important to Patients
Randell & Wearn (2005): – The manner of the doctor
– Doctor’s level of expertise
– Information needs beyond the diagnosis
– Support
Two important factors (Back, 2002) – Willingness to talk about dying
– Disclosing bad news sensitively

Impact on Patient ◦ How a patient will respond will differ
◦ The way news is conveyed can substantially
influence the impact of receiving this news
◦ Schofield et al (2003): Discussions of serious news
When doctors were willing to address patients’ feelings, patients
had significantly fewer anxiety symptoms at 4 & 13 month f/up
◦ Maguire (1999): Greater satisfaction, less anxiety, and more treatment compliance
when doctors asked about:
Patient perceptions of their problems
Patient reactions to their problems
How illness impacted their daily lives

Balancing act Bousquet et al (2015): Metasynthesis
Review of 40 studies, >600 oncologists, 12 countries
Communication needs to be constantly adaptive &
individualised
Differs significantly from stereotypical communication training
Describes breaking bad news as a “balancing act”:
Individual relationship with patient
Hospital system &
environment
Cultural factors
Patient’s family
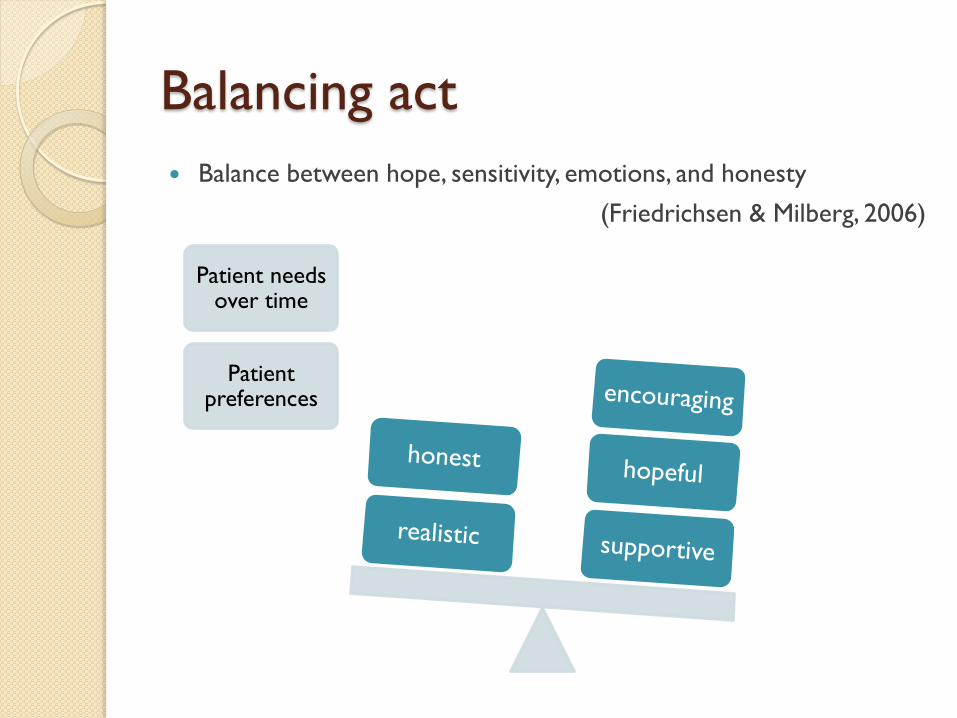
Balancing act
Balance between hope, sensitivity, emotions, and honesty
(Friedrichsen & Milberg, 2006)
Patient needs over time
Patient preferences

Effective Communication
7 important themes (Burtow et al., 2002)
1. Communication within a caring, trusting, long term relationship
2. Open and repeated discussions about patient preferences for information
3. Clear, straightforward presentation of prognosis where desired
4. Strategies to ensure patient understanding
5. Encouragement of hope and a sense of control
6. Consistency of communication within the MDT
7. Communication with other members of the family

Effective Communication
Fundamental prerequisites
◦ Information is…
Adequate
Understood
Believed
Remembered
Acted upon

Key elements in communicating
serious news
1. Preparation & setting
2. Asking patient/family what they
understand or perceive
3. Sharing the serious news
4. Attending to emotions as they arise
5. Planning & discussing next steps

1. Preparation & setting
Time to prepare & gather all medical information needed (scans, results, consult with other drs)
Quiet space
Adequate time
No distractions / pagers
Support person present Emotional support
Aids the later recall of information
Only 25% of the important facts are recalled (Dunn et al., 1993)
Interpreter

2. Asking the patient
What do they already know?
◦ Prepares you to fill in the gaps
◦ Prevents any unnecessary confusion
‘To start, I want to make sure we are on the same page. What is your
understanding of your medical situation?’
‘What have the doctors told you so far?’
‘You had a CT scan of your stomach yesterday; what did the doctors say
about why we did the CT?’

3. Sharing the serious news
Prepare the patient or not???
◦ ‘I’m sorry that the test did not show what we hoped for’ or ‘there is no easy way to say this…’
Find their starting point, be gentle, but come to the point
Use simple and direct language with attention to keeping the news brief
Use pauses to allow the patient time to process

Language
Patient confusion = major contributor to
distress
Medical terms and phrases scare and
confuse patients; they are also the biggest
source of misunderstanding
◦ E.g. 73% of patients did not understand the term
‘median’ survival (Back, 2002)
Simple language encourages patients to ask
questions

What information to give? Key principles (Randell & Wearn, 2005):
◦ Tailor the information to patient wishes & what they’re ready to hear
◦ Allow enough time
◦ Allow for silences
◦ Give information in stages
◦ Repeat information over time
◦ Avoid withholding information (even if relatives insist)
◦ Acknowledge distress and explore reasons for it
Check that the patient would like to continue the discussion
◦ Be willing to answer questions openly and honestly

What information to give? Consider providing information about…
– Diagnosis
– Prognosis
– Treatment options
– Life expectancy
– Impact of the disease on other aspects of their life (e.g. sexuality, roles)
– Fears are reduced when given enough factual information re: what is wrong + what emotional and physical symptoms to expect in the future
– Providing information about the prognosis and course of disease decreases anxiety and gives time to prepare for dying (Friedrichsen & Milberg, 2006)

Providing Reassurance and Hope
Patients fear abandonment – reassure that they will
continue to be followed up and supported
Reassurance to address fears
E.g. analgesia will be given early and at an appropriate dose
Reassurance ≠ fixing the problem
Reassurance is found in being seen & heard
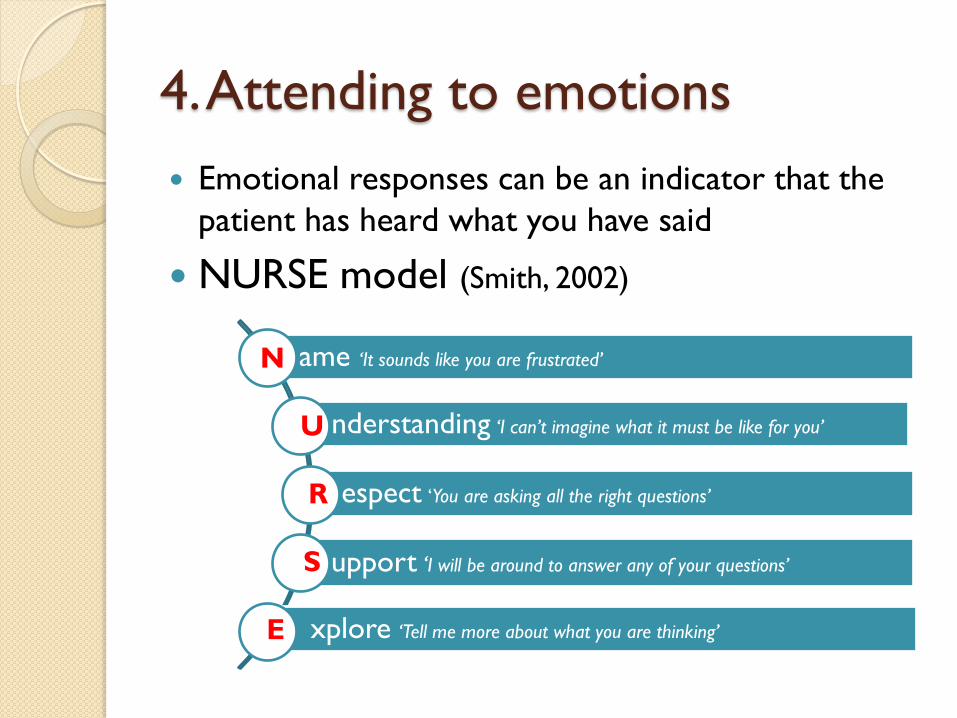
4. Attending to emotions
Emotional responses can be an indicator that the
patient has heard what you have said
NURSE model (Smith, 2002)
ame ‘It sounds like you are frustrated’
nderstanding ‘I can’t imagine what it must be like for you’
espect ‘You are asking all the right questions’
upport ‘I will be around to answer any of your questions’
xplore ‘Tell me more about what you are thinking’
N
U
R
S
E

The most important part of breaking bad
news is how well you are able to respond
to the other person’s emotions

Compassion (Kearsley, 2011)
Actively develop a deep awareness of
another person’s world
Actively attempt to understand their
suffering
Actively desire to play our part in the
person’s healing

Sackett:
“The most powerful therapeutic tool you’ll ever
have is your own personality”
(Smith, 2003)

“who you are may affect your patients as
deeply as what you know. You will often heal
with your understanding and your presence
things you cannot cure with your scientific
knowledge”
(Remen, 2001)

Emotions
“Am I going to die?” – recommend hearing the question as an emotion
Listen for the emotion, and stay with the emotion
Being able to sit with distress in the room ◦ “I understand that you are scared”
◦ “I see how frightened/worried/_____ you are”
When emotionally overwhelmed = cannot process information
Sitting with silence

5. Planning next steps
Patients consistently want to know what comes
next (Back et al., 2011)
◦ Why is it important?
Reduces fears about the future
Creates a sense of predictability
May involve:
◦ Treatment planning
◦ Follow-up appointments
◦ Upcoming tests

Considerations
Patients benefit from:
◦ Ongoing care; knowing that they will be seen regularly
and kept informed
◦ A consistent doctor or for their doctor to be familiar
with their case history (Randell & Wearn, 2005)
Considerations cont’d
Reasons for patients poor understanding or recall:
Primacy and recency phenomena
Emotional distress, nervousness, unrealistic expectations and the seriousness of the disease
Patients experience of shock
Disturbances in the consultation or perception of a hurried / disinterested doctor
Language
Cultural differences

SPIKES Protocol (Buckman1992)
Step Description of Task
Setting Establish rapport by creating an appropriate setting that
provides for privacy, patient comfort, uninterrupted time, setting
eye contact and inviting significant others (if desired)
Perception Elicit the patient’s perception of his or her problem
Invitation Obtain the patient’s invitation to disclose the details of the
medical condition
Knowledge Provide knowledge and information to the patient. Give
information in small chunks, check for understanding, and avoid
medical jargon
Empathize Empathize and explore emotions expressed by the patient
Summary and
Strategy
Provide a summary of what you said and negotiate a strategy
for treatment or follow up.

Alternative Protocols ABCDE (Rabow, et al, 1999)
◦ Advance
◦ Build
◦ Communicate
◦ Deal
◦ Encourage
GUIDE (Back, 2013)
◦ Get
◦ Understand
◦ Inform
◦ Deepen
◦ Equip
BREAKS (Narayanan, et al,
2010)
◦ Background
◦ Rapport
◦ Explore
◦ Announce
◦ Kindling
◦ Summarise

For another presentation….
When conflict is present
Managing angry patients/family members
Varied cultural perspectives & values
SELF MANAGEMENT

Using CBT to manage own anxieties
Cognitive Behaviour Therapy can be used to influence our
thoughts and behaviour when we have to break bad news
Personal thoughts of having “failed” or feeling “hopeless
about the future” for the patient may affect our
communication and the help we offer


‘The patient is going to get upset or angry and I don’t know how to deal with them’
Helpless
Ashamed
Worried
Guilty
Avoid the conversation / procrastinate / try to get in and out really quickly
Unhelpful Thought

‘The patient is going to get upset or angry and I don’t know how to deal with them’
Helpless
Ashamed
Worried
Guilty
Avoid the conversation / procrastinate / try to get in and out really quickly
‘I have let them down; I am a bad doctor’
Feelings intensify
Avoid or delay further consultations and follow up
Unhelpful Thought

‘The patient is likely to become distressed but this is a normal reaction and it is not a personal attack’
Helpless
Worried
Sit with the patient during their distress
Helpful Thought

‘The patient is likely to become distressed but this is a normal reaction and it is not a personal attack’
Helpless
Worried
Sit with the patient during their distress ‘That was difficult
and I feel sad for them but I managed to provide support as best I could’
Sadness Loss
Less discomfort approaching the family / patient for future consultations
Helpful Thought

Challenging Negative Thoughts
Is this a helpful thought? ◦ Not if it leads to unhelpful feelings (guilt, shame
etc) and behaviours (escape / avoidance)
Is there evidence to support this thought? Evidence against? ◦ Weigh up evidence and come up with a more
balanced thought
Is there another way of looking at it? / What are some alternative thoughts?
What would I say to a friend in this situation?

Self Care Be aware of transference and manage
Know your own limitations
Know how to access adequate backup and
support for the patient and their family. What
other services exist?
Have support for yourself and opportunities to
debrief when you need to
Know what strategies you can put in place to
support yourself in your workplace
EAP

QUESTIONS??
St. Vincent’s Hospital The Kinghorn Cancer Centre &
Sacred Heart Rehabilitation [email protected]

References Back, A. L. (2013). Vital Talk (1.0) [Mobile Application Software] http://vitaltalk.org (Accessed
on January 13, 2015)
Back, A.L., Trinidad, S.B., Hopley, E.K, et al. (2011). What patients value when oncologists give news of cancer recurrence: commentary on specific moments in audio-recorded conversations. Oncologist, 16, 342.
Bor et al.. (1993). The meaning of bad news in HIV disease: counselling about dreaded issues revisited. Counselling Psychology, 6(1), 69-80.
Bousquet, G., Orri, M., Winterman, S. et al (2015). Breaking Bad News in Oncology: A Metasynthesis. J Clin Oncol, 33, 2437.
Buckman, R. (1984). Breaking bad news: why is it still so difficult? Br Med J (Clin Res Ed), 288, 1597.
Buckman, R. (1992). How to Break Bad News: A Guide for Health Care Professionals. Baltimore: Johns Hopkins Press.
Burtow, P. N., Dowsett, S., Hagerty, R, & Tattersall, M. H. (2002). Communicating prognosis to patients with metastatic disease: what do they really want to know? Support Care Cancer, 10, 161.
Cox, A., Jenkins, V., Catt, S., et al. (2006). Information needs and experiences: an audit of UK cancer patients. European Journal of Oncology Nursing, 10: 263.
Dunn, S.M., Patterson, P.U, Butow, P.N, Smartt, H.H., McCarthy, W.H., Tattersall, M.H. (1993) Cancer by another name: A randomized trial of the effects of euphemism and uncertainty in communicating with cancer patients. J Clin Oncol, 11, 989–996.

References Friedrichsen, M. & Milberg, A. (2006). Concerns about losing control when breaking bad news
to terminally ill patients with cancer: physicians’ perspective. J Palliat Med, 9, 673.
Fujimori, M. & Uchitomi, Y. (2009). Preferences of cancer patients regarding communication of bad news: a systematic literature review. Jpn J Clin Oncol, 39, 201.
Kearsley, 2011 (2011). In the nighttime of your fear: The anatomy of compassion in the healing of the sick. Palliative and Supportive Care, 9, 215-221
Lobb, E. A., Kenny, D. T., Butow, P. N., & Tattersall, M. H. (2001). Women’s preferences for discussion of prognosis in early breast cancer. Health Expect, 4, 48
Maguire, P. (1999). Improving communication with cancer patients. Eur J Cancer, 35, 1415.
Narayanan, V., Bista, B. & Koshy, C. (2010). ‘BREAKS’ Protocol for Breaking Bad News. Indian J Palliat Care, 16, 61.
Ptacek, J. T., Ptacek, J. J. & Ellison, N. M. (2001). “I’m sorry to tell you…” physicians’ reports of breaking bad news. J Behav Med, 24, 205.
Rabow, M. W., & McPhee, S. J. (1999). Beyond breaking bad news: how to help patients who suffer. West J Med, 171, 260.
Randell, T.C & Wearn, A.M. (2005). Receiving bad news: patients with hameatological cancer reflect upon their experience. Palliative Medicine, 19(8), 594-601
References Remen, R.N. (2001b). The power of words. Western Journal of Medicine, 175, 353–354.
Rosenbaum, M.E., Ferguson, K.J., Lobas, J.G. (2004). Teaching medical students and residents skills for delivering bad news: a review of strategies. Acad Med. 79(2), 107–117.
Rutten, L.J., Arora, N. K., Bakos, A.D., et al. (2005). Information needs and sources of information among cancer patients: a systematic review of research (1980-2003). Patient Educ Counsl, 57, 250.
Schofield, P. E., Butow, P. N., Thompson, J. F., et al (2003). Psychological responses of patients receiving a diagnosis of cancer. Ann Oncol, 14, 48.
Seifart, C., Hofmann, M. Bar, T., et al (2014). Breaking bad news – what patients want and what they get: evaluating the SPIKES protocol in Germany. Ann Oncol, 25, 707.
Shaw, J. Brown, R., Heinrich, P. & Dunn, S. (2013). Doctors’ experience of stress during simulated bad news consultations. Patient Educ Couns, 93, 203.
Siminoff LA, Fetting JH. (1989) Effects of outcome framing on treatment decisions in the real world: impact of framing on adjuvant breast cancer decisions. Med Decis Making, 9, 262-271.
Smith, R.C. (2002). Patient-Centred Interviewing: An Evidence-Based Method. Philadelphia: Lippincott Williams & Wilkins.
Smith, R. (2003). Thoughts for new medical students at a new medical school. British Medical Journal, 327, 143–1433.