dehydration
TRANSCRIPT


Dehydration:-
It mean volume depletion and occurs when fluid loss from the extracellular space at a rate that exceeds intake.

Body fluid distribution
• The body contains 2 major fluid compartments: the intracellular fluid (ICF) and the extracellular fluid (ECF). The ICF comprises of two thirds of the total body water (TBW), while the ECF accounts for the remaining third. The ECF is further divided into the interstitial fluid (75%) and plasma (25%). The TBW comprises approximately 70% of body weight in infants, 65% in children, and 60% in adults.
• Infants' and children’s higher body water content, along with their higher metabolic rates and increased body surface area to mass index, contribute to their higher turnover of fluids and solute. Therefore, infants and children require proportionally greater volumes of water than adults to maintain their fluid equilibrium and are more susceptible to volume depletion. Significant fluid losses may occur rapidly, leading to depletion of the intravascular volume.
•
Causes of dehydration in
children
1. Dehydration is most often caused by a viral infection that causes fever, diarrhoea, vomiting and a decreased ability to drink or eat.Common viral infections causing vomiting and diarrhoeainclude rotavirus.
2. Sometimes sores in a child's mouth caused by a virus make it painful to eat or drink, helping to cause or worsen dehydration.
3. More serious bacterial infections can make a child less likely to eat and may cause vomiting and diarrhoea. Common bacterial infections include Salmonella, E coli, CampylobacterandC.difficile.
4. Parasitic infections such as Giardia lamblia cause the condition known as giardiasis.
5. Increased sweating from a very hot environment can cause dehydration.
6. Excessive urination caused by unrecognised or poorly treated diabetes (not taking insulin) and Diabetes insipidus.

7-Third-space extravasation of intravascular fluid (eg, pancreatitis, peritonitis, sepsis, heart failure)
8-Hemorrhage
9-burn

Signs &Symptoms of dehydration in children
You should be concerned if your child has an excessive loss of fluid from vomiting or diarrhoea, or if the child refuses to eat or drink.
Signs of dehydration:1. Sunken eyes2. Decreased frequency of urination or dry nappies3. Sunken soft spot on the top of the head in babies (called the
fontanelle)4. No tears when the child cries5. Dry or sticky mucous membranes (the lining of the mouth
or tongue)6. Lethargy (less activity than normal)7. Irritability (more crying, fussiness)8. Abnormal capillary refill time9. Abnormal skin turgor10 .Abnormal respiratory pattern



investigation
• A full blood count may identify seriousness or type of infection.
• Blood cultures may identify the type of bacterial infection.
• Blood chemistry may identify any electrolyte abnormality caused by vomiting and diarrhoea, and may identify serious imbalances in body chemistry caused by illness.
• Urinalysis may identify bladder infection, give evidence of severity of dehydration and may identify sugar and ketones in urine (evidence of uncontrolled diabetes).
• Stool examination

Evaluation the degree of dehydration

CALCULATION OF THE DEFICIT:-Determining the fluid deficit necessitates clinically determining the
percent dehydration and multiplying this percentage by the patient's weight; a child who weighs 10 kg and is 10% dehydrated has a fluid deficit of 1 L.
10kg x 10/100= 1L. .
CALCULATION OF MAINTENANCE:-100 ml/kg for the first 10 kg body wt. = 1000 ml.50 ml/kg for the second 10 kg body wt. = 500 ml.25 ml/kg for the third 10 kg body wt. = 250 ml.
TOTAL FLUID REQUIRMENT:- equal to
Fluid deficit + maintenance within 24 hrs.

Treatment
Mild Volume Depletion
• Patients with minimal to mild volume depletion should be encouraged to continue an age-appropriate diet and adequate intake of oral fluids. Oral rehydration solution (ORS) should be used. Children should be given sips of ORS (5 mL or 1 teaspoon) every 2 minutes . the goal should be to drink 10 mL/kg body weight for each watery stool and estimate volume of emesis for each episode of vomiting .

• If commercially prepared ORS is not available, the following recipe may be used:
• In 1 L of water, add 2 level tablespoons of sugar or honey, a quarter teaspoon of table salt (NaCl), and a quarter teaspoon of baking soda (bicarbonate of soda)
• If baking soda is not available, use another quarter teaspoon of salt instead
• If available, add one-half cup of orange juice.
• The water is safer if boiled, but do not lose time doing this if the child is very ill
• Inpatient therapy generally is not indicated for mild volume depletion. However, it is prudent to arrange outpatient follow-up evaluation within 48 hours, with instructions to return sooner if symptoms worsen.


Oral Rehydration SolutionComposition:
NaCl: 3.5 gm, NaHCO3: 2.5 gm, KCl: 1.5 gm, Glucose: 20 gm, In 1000ml (1 litre) of water.
Some replace NaHCOs by 2 gm Tri-sodium Citrate Di-hydrate which lessens vomiting, is tastier and more stable in humid and hot areas.
Advantages of ORS:
Cheap, effective and easy to give at home by the mother. This is why 95% of the cases are treated by ORS, as children will not develop dehydration, when they get diarrhoea.
Limitations to oral rehydration therapy include shock, an ileus, intussusception, carbohydrate intolerance (rare), severe emesis, and high stool output (>10 mL/kg/hr).

Preparation of ORS:
The water should be boiled and cooled before the powder is added to avoid the loss of bicarbonate, and changes of concentration. In winter, warm the solution to 40°C to increase acceptability, increase the rate of absorption, decrease vomiting & decrease the risk of a drop in the body temperature when large volumes are consumed.
Diarrhoea case fatality rate has decreased a lot after the introduction of the ORS, due to the prevention of dehydration.
Moderate Volume Depletion
• The literature supports use of oral rehydration for the moderately dehydrated child. Similar outcomes have been achieved in randomized studies comparing ORS with intravenous fluid therapy with fewer complications and higher parent satisfaction in the ORS groups. Moreover, ORS can typically be initiated sooner than IV fluid therapy .
• With ORS, patients should receive approximately 50-100 mL/kg body weight over 2-4 hours, again starting with 5 mL every 5 minutes. If the child can tolerate this amount and asks for more fluids, the amount given can gradually be increased. Once the fluid deficit has been corrected, parents should be instructed on how to replace volume losses at home if the child continues to have vomiting or diarrhea.
• Children in whom ORS fails should be given a bolus (20 mL/kg) of isotonic fluid intravenously. This may be followed by maintenance therapy. Over the next few hours, the patient may be transitioned to oral rehydration as tolerated, at which point the intravenous therapy may be discontinued.
• Children with moderate volume depletion may require inpatient treatment if they are unable to tolerate oral fluids despite rehydration. Hospitalization may also be required for treatment of the underlying cause of the fluid deficit.
Severe Volume Depletion
• Patients with severe volume depletion should receive intravenous isotonic fluid boluses (20-60 mL/kg). In children with difficult peripheral access, perform intraosseous or central access promptly. Fluid boluses should be repeated until vital signs, perfusion, and capillary refill have normalized.
• If a patient reaches 60-80 mL/kg in isotonic crystalloid boluses and is not significantly improved, consider other causes of shock (eg, sepsis, hemorrhage, cardiac disease). In addition, consider administering vasopressors and instituting advanced monitoring, such as a bladder catheter, central venous pressure, and measuring mixed venous oxygen saturation.
• Although physicians typically give normal saline for these initial boluses, it is important to remember to check a bedside glucose level for patients who appear lethargic or altered. Treat hypoglycemia promptly. The appropriate dose is 0.25 g/kg IV (2.5 mL/kg of 10% dextrose or 1 mL/kg of 25% dextrose).

• Once vital sign abnormalities are corrected, initiate maintenance fluid therapy plus additional fluid to make up for any continued losses.
• Daily fluid requirements may be met using dextrose 5% in half-normal saline solution.
• The emergency physician also should consider daily sodium and potassium requirements as follows:
• Sodium 2-3 mEq/kg/d
• Potassium 2-3 mEq/kg/d
Fluid management of dehydration

During Therapy Monitor:1- Vital sign :
pulse , blood pressure
2- Intake and output:
fluid balance and urine output
3-Physical examination:
weight
sign of volume depletion or overload
4-Electrolytes

ADDITIONAL THERAPIES.
• Antimotility agents• are contraindicated in children with dysentery and probably have no role in
the management of acute watery diarrhea in otherwise healthy children.
• Antiemetic• ANTIBIOTIC THERAPY• Timely antibiotic therapy in select cases of diarrhea may reduce the
duration and severity of diarrhea and prevent complications
• ZINC SUPPLEMENTATION• There is strong evidence that zinc supplementation in children with
diarrhea in developing countries leads to reduced duration and severity of diarrhea WHO and UNICEF recommend that all children with acute diarrhea in at-risk areas should receive oral zinc in some form for 10–14 days during and after diarrhea (10 mg/day for infants <6 mo of age and 20 mg/day for those >6 mo).
HYPONATREMIC DEHYDRATION.
• The pathogenesis of hyponatremicdehydration is usually due to a combination of sodium and water loss and water retention to compensate for the volume depletion. The patient has a pathologic increase in fluid loss, and this fluid contains sodium. Most fluid that is lost has a lower sodium concentration, so patients with only fluid loss would have hypernatremia

• Diarrhea has, on average, a sodium concentration of 50 mEq/L. By replacing diarrheal fluid with water, which has almost no sodium, there is a reduction in the serum sodium concentration. The volume depletion stimulates synthesis of antidiuretic hormone, resulting in reduced renal water excretion. Hence, the body's usual mechanism for preventing hyponatremia, renal water excretion, is blocked. The risk of hyponatremia is further increased if the volume depletion is due to loss of fluid with a higher sodium concentration, as may occur with renal salt wasting, third space losses, or diarrhea with a high sodium content (cholera).

• Hyponatremic dehydration produces more substantial intravascular volume depletion due to the shift of water from the extracellular space into the intracellular space. In addition, some patients have symptoms, predominantly neurologic, as a result of hyponatremia .
• The initial goal in treating hyponatremia is correction of intravascular volume depletion with isotonic fluid (NS or RL). An overcorrection in the serum sodium concentration (>135 mEq/L) is associated with an increased risk of central pontinemyelinolysis (CPM). The risk of CPM also increases with overly rapid correction of the serum sodium concentration, so it is best to avoid increasing the sodium by >12 mEq/L each 24 hr. . Again, potassium delivery is adjusted based on the initial serum potassium level and the patient's renal function. Potassium is not given until the patient voids.

• The patient's sodium concentration is monitored closely to ensure appropriate correction, and the sodium concentration of the fluid is adjusted accordingly. Patients with ongoing losses require an appropriate replacement solution. Patients with neurologic symptoms (seizures) as a result of hyponatremia need to receive an acute infusion of hypertonic (3%) saline to increase the serum sodium concentration rapidly.

Treatment of hyponatremic dehydration Dehydration
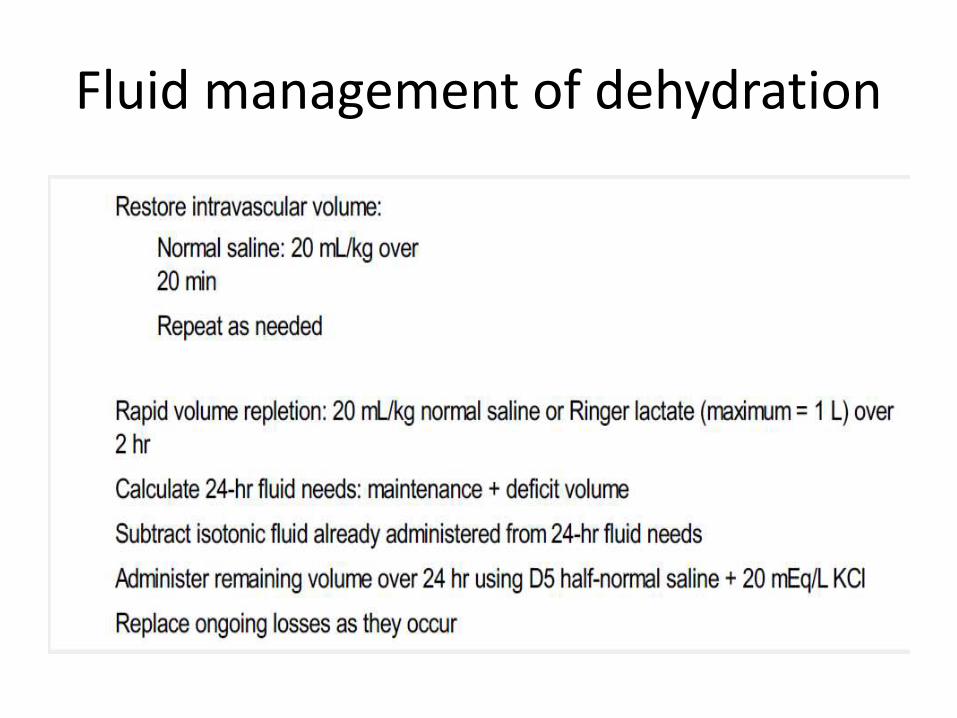
Restore intravascular volume
Normal saline: 20 mL/kg over 20 min
Repeat as needed
Rapid volume repletion: 20 mL/kg normal saline or Ringer Lactate (maximum = 1 L) over 2 hr
Calculate 24-hr fluid needs: maintenance + deficit volume
Subtract isotonic fluid already administered from 24 hr fluid needs
Administer remaining volume over 24 hr using D5 ½ normal saline + 20 mEq/L KCl
Replace ongoing losses as they occur

HYPERNATREMIC DEHYDRATION.
• Hypernatremic dehydration is the most dangerous form of dehydration due to complications of hypernatremia and of therapy. Hypernatremia can cause serious neurologic damage, including central nervous system hemorrhages and thrombosis. This appears to be secondary to the movement of water from the brain cells into the hypertonic extracellular fluid, causing brain cell shrinkage and tearing blood vessels within the brain .

• The movement of water from the intracellular space to the extracellular space during hypernatremicdehydration partially protects the intravascular volume. Thus, children with hypernatremia often appear less ill than children with a similar degree of isotonic dehydration. Urine output may be preserved longer, and there may be less tachycardia. Unfortunately, because the initial manifestations are milder, children with hypernatremic dehydration are often brought for medical attention with more profound dehydration.
• Children with hypernatremic dehydration are often lethargic, and they may be irritable when touched. Hypernatremia may cause fever, hypertonicity, and hyperreflexia. More severe neurologic symptoms may develop if cerebral bleeding or thrombosis occurs.

• Overly rapid treatment of hypernatremic dehydration may cause significant morbidity and mortality. Idiogenic osmolesare generated within the brain during the development of hypernatremia. These idiogenic osmoles increase the osmolality within the cells of the brain, providing protection against brain cell shrinkage caused by movement of water out of the cells and into the hypertonic extracellular fluid. They dissipate slowly during the correction of hypernatremia. With overly rapid lowering of the extracellular osmolality during the correction of hypernatremia, there may be an osmotic gradient created that causes water movement from the extracellular space into the cells of the brain, producing cerebral edema. Symptoms of the resultant cerebral edema can range from seizures to brain herniation and death.

• To minimize the risk of cerebral edema during the correction of hypernatremic dehydration, the serum sodium concentration should not decrease by >12 mEq/L every 24 hr. The deficits in severe hypernatremic dehydration may need to be corrected over 2–4 days .
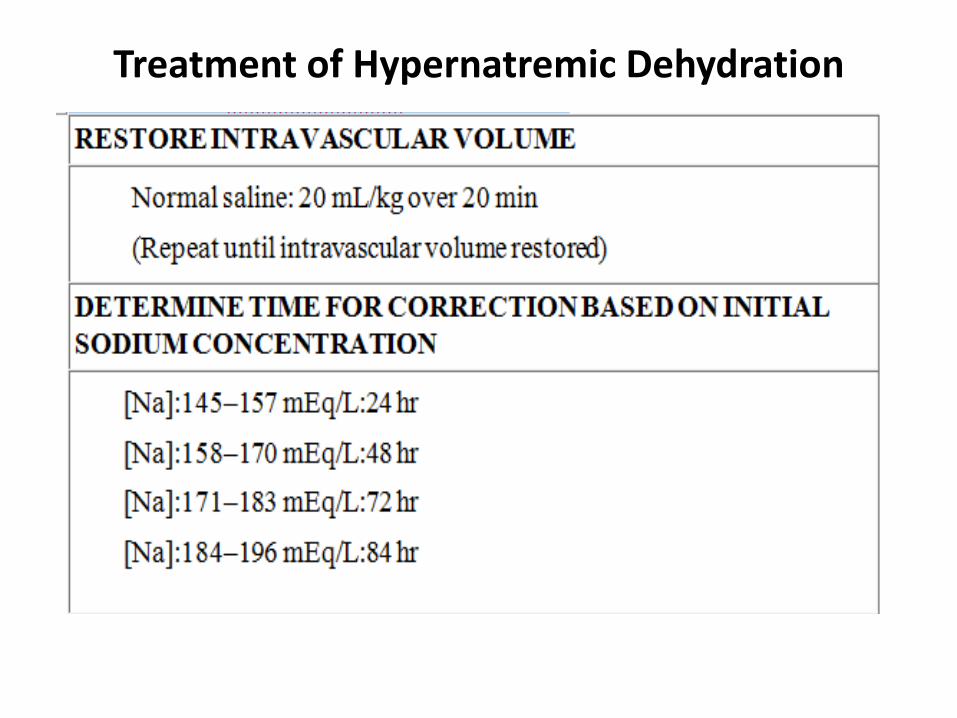
Treatment of Hypernatremic Dehydration
• The initial resuscitation of hypernatremic dehydration requires restoration of the intravascular volume with NS. LR should not be used because it is more hypotonic than NS and may cause too rapid a decrease in the serum sodium concentration, especially if multiple fluid boluses are necessary.
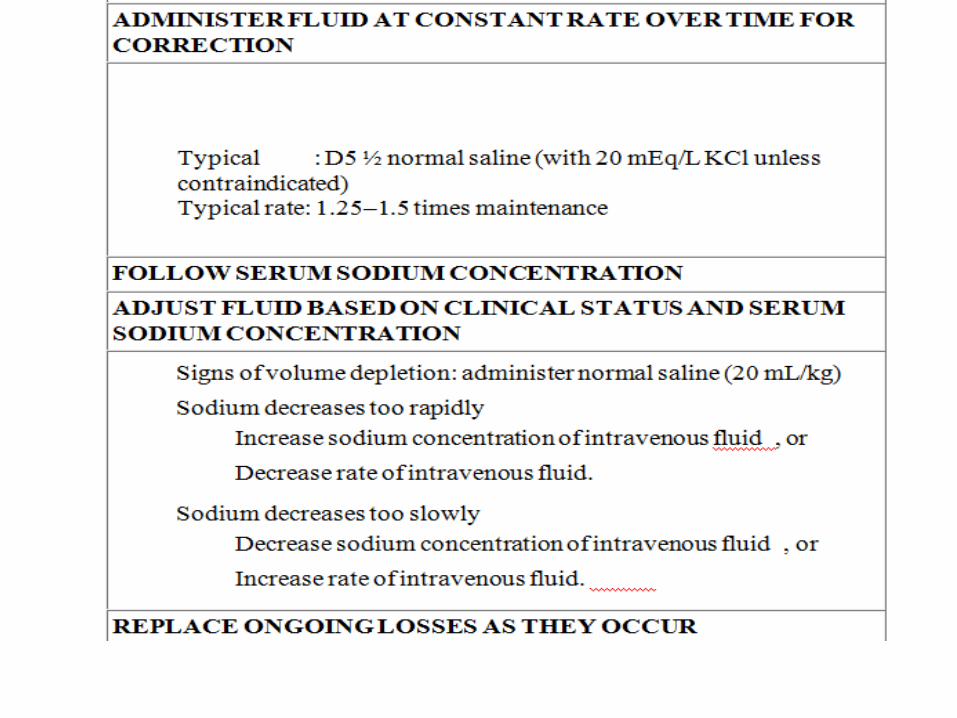
• To avoid cerebral edema when correcting hypernatremicdehydration, the fluid deficit is corrected slowly. The rate of correction depends on the initial sodium concentration .There is no general agreement on the choice or the rate of fluid for correcting hypernatremic dehydration. The choice and the rate of fluid administration are not nearly as important as vigilant monitoring of the serum sodium concentration and adjustment of the therapy based on the result .

• Seizures are the most common manifestation of cerebral edemafrom an overly rapid decrease of the serum sodium concentration during correction of hypernatremic dehydration. Acutely, increasing the serum concentration via an infusion of 3% sodium chloride can reverse the cerebral edema. Each 1 mL/kg of 3% sodium chloride increases the serum sodium concentration by approximately 1 mEq/L. An infusion of 4–6 mL/kg often results in resolution of the symptoms. This is similar to the strategy used for treating symptomatic hyponatremia .
• In patients with severe hypernatremia, oral fluids must be used cautiously. Infant formula, because of its low sodium concentration, has a high free water content, and especially if added to intravenous therapy, it may contribute to a rapid decrease in the serum sodium concentration. Less hypotonic fluid, such as an oral rehydration solution, may be more appropriate initially.
