deep brain stimulation
TRANSCRIPT

Parkinson's disease &
Deep brain stimulation

History of PD's• In 1817 an English doctor, James Parkinson, published his essay reporting six cases of paralysis
agitans.• An Essay on the Shaking Palsy described the characteristic resting tremor, abnormal posture and
gait, paralysis and diminished muscle strength, and the way that the disease progresses over time.
• Jean-Martin Charcot studies between 1868 and 1881 were a landmark in the understanding of the disease. Among other advances, he made the distinction between rigidity, weakness and bradykinesia.
• He also championed the renaming of the disease in honor of James Parkinson.

Parkinson's disease• Parkinson's disease (PD, also known as
idiopathic or primary parkinsonism, hypokinetic rigid syndrome (HRS), or paralysis agitans) is a degenerative disorder of the central nervous system mainly affecting the motor system.
• Parkinson's disease is more common in older people, with most cases occurring after the age of 50; when it is seen in young adults, it is called young onset PD (YOPD).

Symptoms• Early in the course of the disease, the most obvious symptoms
are movement-related:• Shaking• rigidity• slowness of movement and difficulty with walking• gait. • Later thinking and behavioral problems may arise, with dementia
commonly occurring in the advanced stages of the disease• whereas depression is the most common psychiatric symptom.

Management • There is no cure for Parkinson's disease but medications, surgery and multidisciplinary
management can provide relief from the symptoms. • The Anticholinergics and surgery were the only treatments until the arrival of levodopa,
which reduced their use dramatically.• Levodopa was first synthesized in 1911 by Casimir Funk, but it received little attention
until the mid 20th century.• It entered clinical practice in 1967 and brought about a revolution in the management
of PD.• Levodopa has been the most widely used treatment for over 30 years. L-DOPA is
converted into dopamine in the dopaminergic neurons by dopa decarboxylase.• Since motor symptoms are produced by a lack of dopamine in the substantia nigra, the
administration of L-DOPA temporarily diminishes the motor symptoms.

• Dopamine agonists• MAO-B inhibitors• Other drugs• Surgery• Lesional and deep brain stimulation.• Rehabilitation • Palliative care

Future ahead
• Gene therapy• Gene therapy typically involves the use of a non-infectious virus (i.e., a viral vector such as the adeno-associated virus) to
shuttle genetic material into a part of the brain.• The gene used leads to the production of an enzyme that helps to manage PD symptoms or protects the brain from further
damage.
• Neuroprotective treatments• Several chemical compounds such as GDNF have been proposed as neuroprotectors in PD, but their effectiveness has not been
proven.
• Neural transplantation• Since early in the 1980s, fetal, porcine, carotid or retinal tissues have been used in cell transplants, in which dissociated cells
are injected into the substantia nigra in the hope that they will incorporate themselves into the brain in a way that replaces the dopamine-producing cells that have been lost.
• Stem cell transplants are a recent research target although use of fetal stem cells is controversial.It has been proposed that effective treatments may be developed in a less controversial way by use of induced pluripotent stem cells taken from adults.

The beginning of DBS
• The roots of DBS reach back to the 1960s,when Parkinson's disease was commonly treated with surgery to remove or destroy certain brain regions.
• To pinpoint which areas to target in each patient,neurosurgeons began to experiment with electrical stimulation.
• They discovered that the delivery of rapid impulses to the basal ganglia,including STN could markedly reduce the patients tremors.
• By the late 1980s,long term DBS started to emerge as an alternative treatment to surgery.

• Chronic high frequency stimulation of the VIN of the thalamus was first described in early 1990s by benavides ET AL.
• They implanted chronic stimulating electrodes in the VIN connected to a subcutaneous pulse generator positioned in the thoracic region to treat disabling tremor in 26 patients with PD and in 6 with essential tremors.
• Improvement was maintained for up to 29 months.• This new technique was reversible and led to renaissance in
functional neurosurgery.

The “Ideal” Candidate for DBS
• 1) Age: 40-70 yrs• 2) Symptomatic for 5-10 years or more• 3) Initial good response to L-dopa• 4) Severe dyskinesia• 5) Marked “on/off” phenomena• (Minimal “on-time” without dyskinesia• 6) Cognitively intact• 7) Realistic expectations• 8) Adequate social support• 9) Access to programming of stimulators
• Final decision lies with Neurologist and Neurosurgeon

Deep brain stimulation
• DBS involves placing a thin metal electrode into one of several possible brain targets and attaching it to a computerised pulse generator,which is implanted under the skin in the chest below the collarbone.

• The basic surgical method is called frame-based stereo taxis.• A rigid frame is attached to the patients head just before
surgery,after the skin is anesthetized with local anaesthetic.• A brain imaging study is obtained with the frame in place.• The images of the brain and frame are used to calculate the
position of the desired brain target and guide instruments to that target with minimal trauma to the brain

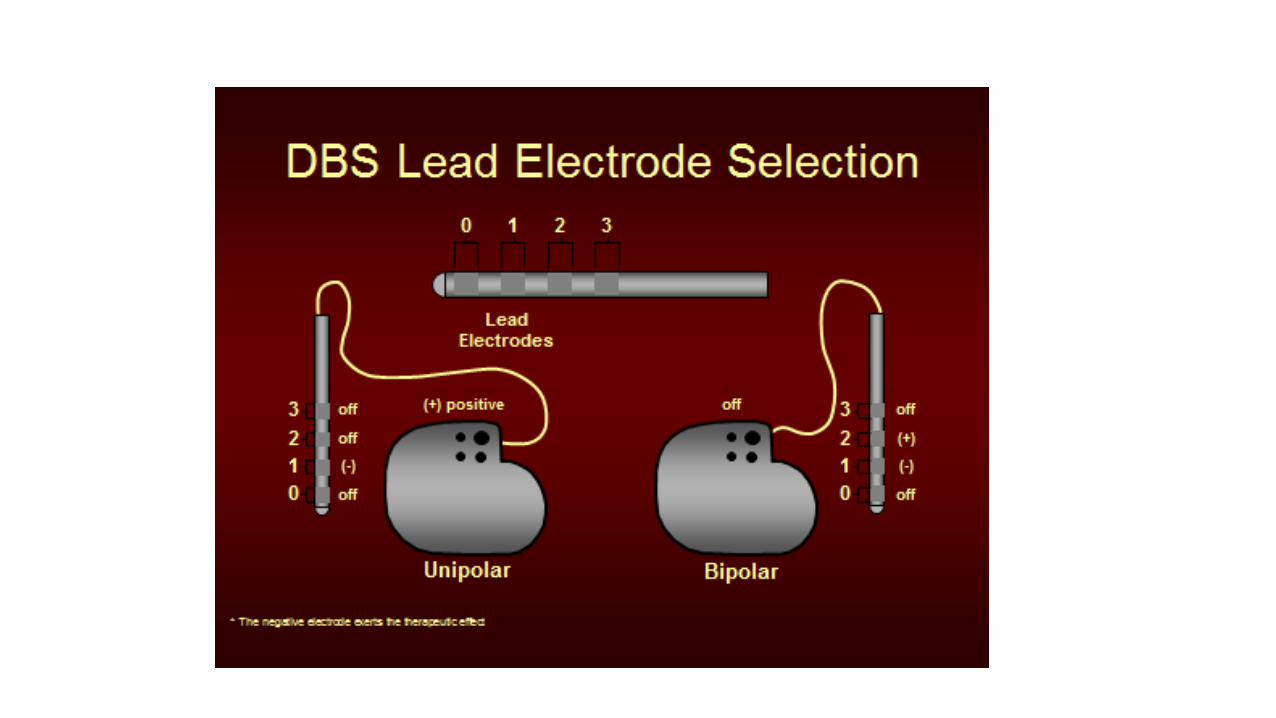
• The most commonly employed deep brain stimulation devices are quadripolar electrodes produced by Medtronic, Inc.
• The devices have an impulse generator (pacemaker), connecting wires, and a patient remote control.
• The impulse generator, whether implanted on the same day or 2 to 4 weeks later, is usually not activated until brain swelling has subsided.

• Medtronic Corporation (Minneapolis, MN, USA) provides the DBS system approved by the FDA for clinical use of Parkinson’s disease and related movement disorders.
• The most commonly used DBS electrodes have four contacts (Medtronic’s leads and electrode models 3389 and 3387).
• The voltage is often set at a value between 1-4 V, the frequency is set between 130-185 Hz, the pulse width is between 60 and 450 s.
METHODOLOGY OF SURGERY
• First,the target location is determined using anatomical landmarks identified on MR imaging.
• The target is defined by using stereotactic imaging techniques,which allow determination of coordinates relative to stereotactic frame,positioned on the patients head.
• The stereotactic target is confirmed and modified by using both micro electrode recordings and macro stimulator.
• It is possible to use MR imaging/CT fusion for anatomical localizations.

Physiological mapping
.
• S it1) Magnetic resonance imaging (x, y & z co-ordinates) 2) Intraoperative microelectrode recordings (neurophysiological localization of target site) 3)Microstimulation 4)Macrostimulation with DBS electrode.
(stimulation of

Target sites • Globus Pallidus (GPi) – The GPi is used as a deep brain stimulation target for dystonia.• Subthalamic Nucleus (STN) – the subthalamic nucleus is frequently used as a deep brain stimulation target
to reduce symptoms of rigidity, tremor and slowness of movement (bradykinesia). Those symptoms are generally improved by 50-70%, often with significant medication reduction.
• Ventral Intermedius Nucleus (VIM) – This area of the thalamus has been a target of choice for controlling tremor in essential tremor, Parkinson’s disease, or other movement disorders.

Selecting target site
There are 3 different ways of determining the stereotactic coordinates of the target nuclei.1.Coordinates determined in reference to the anterior and posterior commissures.2.The target nucleus can be directly visualised on MR imaging.3.It is possible to fuse MR imaging and CT data of the patient with a stereotactic atlas.

• Target coordinates are often calculated with the midcommissural point (the midpoint between AC and PC) as origin.
• Typical target coordinates in relation to the midcommissural point for DBS in movement disorders
• Target region Coordinates • STN 12 mm lateral, 2-4 mm posterior, 3 mm inferior • GPi 20-22 mm lateral, 2-3 mm anterior, 3-6 mm inferior • Thalamus 14-15 mm, lateral 3-5 mm posterior, 0-1 mm superior


Testing
• When the correct target site is confirmed with the micro electrode ,the permanent DBS electrode is inserted and tested for about 20 minutes.
• Placement of electrodes is a difficult neurosurgical procedure that demands a high degree of precision
• The testing does not focus on relief of motor symptoms but rather on unwanted stimulation induced side effects.

• This is because the beneficial effects of stimulation may take hours or days to develop whereas any unwanted effects will be present immediately.
• The device is deliberately turned up to a higher intensity than is normally used,in order to deliberately produce unwanted stimulation induced side effects such as (tingling in the arm or leg,difficulty speaking,pulling sensation in the tongue or face or flashing light skin)


• .
• DBS programming goal– Deliver the therapy to the brain target of interest with avoiding stimulation of surrounding structures
• Typically, initial programming of DBS is 2 - 4 weeks after DBS electrode implant
• Subsequent programming can be every 2-8 weeks for the first 3 months, and then every 3-6 months thereafter
• Commonly takes 6 months to obtain the best settings
• Many patients will require concurrent medication adjustments

Potential complications/risks– Hemorrhage (inherent in any stereotactic procedure);
may be silent or symptomatic
– Transient confusion
– Infection (typically occurs at neurostimulator site in chest when it does occur)
– Device related
– Stimulation related• Usually can be minimized or eliminated
by adjusting stimulation settings• Reversible paresthesia, dysarthria,
muscle contraction

Advances in DBS
• Some reported the Use of frameless stereotaxy with a skull mounted trajectory guide and an image guided workstation for DBS surgery.
• surgeons compared the precision achieved with frameless neuronavigation and conventional frame based stereotaxy.
• Electrode deviations from the target were larger using the frameless technique with a vector deviation of 2.5mm than with a frame based technique (1.2 mm vector deviation)
• Recently procedure that allows DBS electrodes to be implanted with the patient asleep in an MRI scanner instead of awake in the operating room is being done.
• Researchers are continuing to study DBS and to develop ways of improving it.
• A two part study funded by NINDS and the department of veterans affairs first compared bilateral DBS to best medical therapy,including medication adjustment and physical therapy.
• Bilateral DBS showed overall superiority to best medical therapy at improving motor symptoms and quality of life.


conclusion
• Advances in neurosciences will continue to drive the applications in DBS and innovations in biomedical engineering and technology will continue to be applied in DBS.
• The ideal platform for development of these innovations is the active collaboration between the scientist , engineers and clinicians.