declaration - suyajna incidence of cs...declaration statutory warning! the contents of this lecture...
TRANSCRIPT

DECLARATION STATUTORY WARNING!
THE CONTENTS OF THIS LECTURE ARE NEITHER MY PERSONAL OPINIONS NOR CRITISISM OF ANY INDIVIDUAL, HOSPITAL, INSTITUTION, STATE OR COUNTRY.
REDUCING INCIDENCE OF CS MYTH or REALITY
SUYAJNA

INTRODUCTION
C SECTION

CLASSIFICATION OF CS
Ø 1. INDICATED CS
Ø 2. NON-INDICATED CS: Ø a. CSMD Ø b. Lack of FACILITY Ø c. Lack of obstetrical skill Ø Ø d. NON MEDICAL REASONS

HISTORY OF C SECTION
Bindusara, 320 BC, his mother – wife of Chandragupta Maurya accidentally consumed poison during labor, operated by CHANAKYA.
Etymology of the name of Julius Caesar ?? His mother AURELIA lived through his
childbirth and his DEATH 1500..Jakob Nufer of Switzerland , pig gelder

Who is primitive ?
Ø Successful Caesarean section by indigenous healers in Kahura, Uganda.
As observed by R. W. Felkin in 1879.

LANDMARKS in Modern CS
Ø 1876.. Eduardo Porro Ø 1881..Ferdinand Adolf Kehrer Ø 1882.. Max Saumlnger of Leippzig Ø 1912.. Kronig… Munro Kerr

NORMAL DELIVERY ?
NORMAL DELIVERY ??
VAGINAL C S
IS HUMAN PELVIS FIT FOR VD

Humankind has been delivering babies for millions of years…
Homo Habilis “Handy man”
walked the earth - 1,750,000 years ago
NO CS

Homo Erectus
BIPED The female pelvis became adaptively narrower in the region of the vaginal canal, making labor anatomically
more difficult. The narrow birth canal, and the greater size of the head
of the human fetus when compared to other mammals, made human labor the most painful among primates.

PELVIS OF ‘LUCY’
"Lucy" skeleton 3-million-year old Australopithicus afarensis, 1974, has a
much narrower pelvic opening. In comparison to H. Erectus

Homo Erectus – Gona - 2008
birth canal and brain size were co-evolving, to give birth to larger babies - to adapt to the pressure of external
environmental factors.

Homo Sapiens – ‘WISE MAN’
a new anatomical adaptation compensated the narrowing of the pelvis
Homo sapiens in relation to the greater relative size of the brain of NB:
greater immaturity of the central nervous system (CNS)

WHY C S ?
Ø Up to 1850 : to save the baby
Ø Up to 1950 : to save the mother
Ø Up to 2000 : to save the baby
Ø Beyond 2000 : to save the DOCTOR

IS THE TOPIC RELEVANT ?
C. Section Rise Not evolution

Cesarean Delivery: ‘Epidemic’ DISEASE ?
0
5
10
15
20
25
%
1970 1975 1980 1985 1990 1995 1998
C/SPrimary C/SRepeat C/S
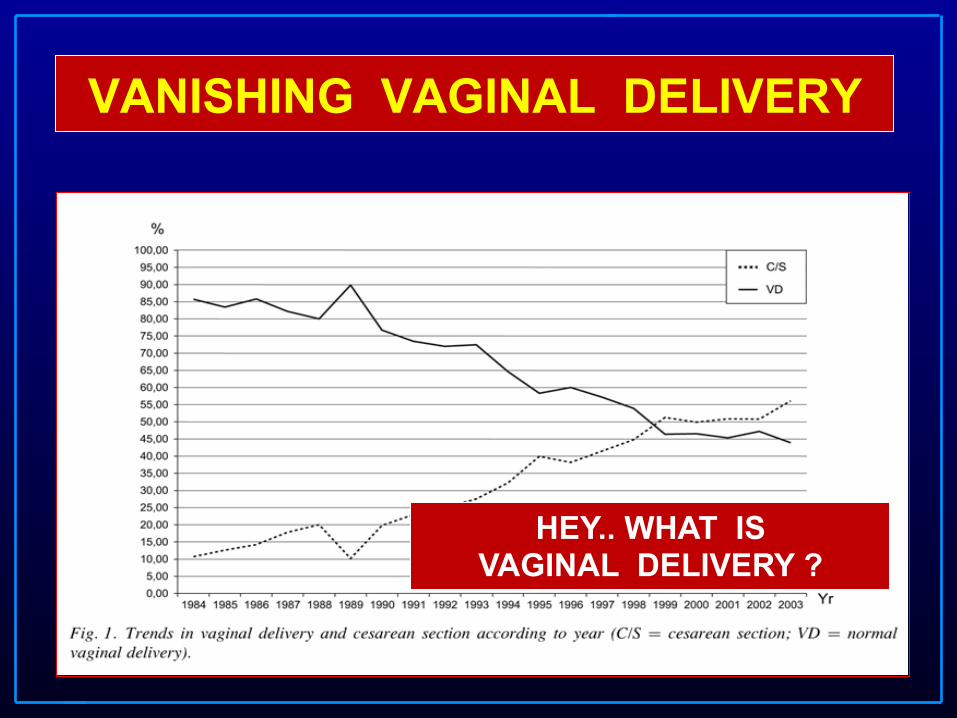
VANISHING VAGINAL DELIVERY
HEY.. WHAT IS VAGINAL DELIVERY ?

RISING TRENDS OF CS
Ø 1. INDICATED CS
Ø 2. NON-INDICATED CS: Ø a. CSMD Ø b. Lack of FACILITY Ø c. Lack of obstetrical skill Ø Ø d. NON MEDICAL REASONS

INCREASE IN INDICATED CS
1. LIE – POSITIONS – PRESENTATIONS
PREVIOUS LSCS
CPD FOETAL DISTRESS

The rise in caesarean section rate: the same indications but a lower
threshold. Leitch CR, Walker JJ.
Br J Obstet Gynaecol 1998 Jun;105(6):621-6.
Ø The results of this study show that the rate of Cesarean sections in Scotland increased by over three-
folds in the period from 1962 to 1992, with no apparent cause to justify this increase other than a lowered threshold of acceptance of the procedure in obstetric practice.

2. PREVIOUS LSCS
CAN WE VBAC
NO

0
5
10
15
20
25
30
89 91 93 95 97 99 2001Año
%
All c-sections
Primary c-section
VBAC
Frequency of cesarean section, primary cesarean and vaginal birth post-c-section between 1989 - 2001
Martin JA, et al., National Center for Health Statistics. 2002
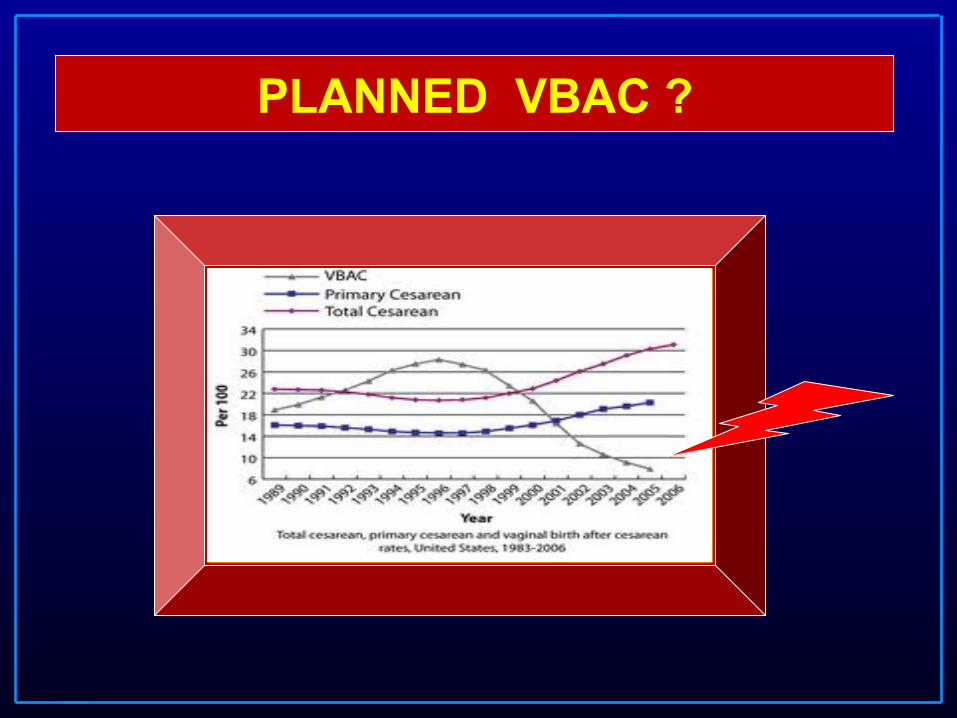
PLANNED VBAC ?

VBAC
Over 1000 reports:
not one RCT

VBAC..ACOG- ‘immediately available’ - practice bulletin no. 54, 2006
BECAUSE UTERINE RUPTURE MAY BE CATASTROPHIC VBAC SHOULD BE
ATTEMPTED IN INSTITUTIONS........
ACOG Practice Bulletin N° 5:1 – 8; 1999.
Less Restrictive VBAC Guidelines - 115 July 21, 2010

WHAT DECIDES VBAC ? Ø Over 1000 reports: not one RCT
Economic forces
rather than
patient well-being,
are driving the goal of
fewer cesarean
sections ? Clark S., et al., Am J Obstet Gynecol 2000;182:599-602

Conservatism in Obstetrics
“No matter how carefully the uterine incision is
sutured, we can never be certain that the cicatrized uterine wall will stand a
subsequent pregnancy and labor without rupture. This means that the usual rule is
“once a cesarean, always a cesarean”
Edwin Craigin, 1916

CRAIGIN WAS RIGHT !!
He was referring ONLY to classical cesarean scars
L.S.C.S. SCARS ?

3. Assessment of CPD
WASTE OF
TIME
CAN YOU ASSESS CPD ?
ICAN
NO

CPD ABSOLUTE RELATIVE
CPD AT THE BRIM BELOW THE BRIM

ABSOLUTE
SIZE
Ø CONTRACTED PELVIS
Ø BIG BABY 4500 Gm - BIG HEAD

RELATIVE
Ø DEFLEXION- MAL POSITION Ø SOL … INTRINSIC - EXTRINSIC HIGH INCLINATION
Ø CORD ROUND THE NECK - AXE

DO YOU ASSESS CPD ?
NO WE GUESS CPD !
VISUAL ASSESSMENT OF CPD

CPD - VIMS SCENARIO
Ø PG: WHICH UNIT …?
Ø ASSISTANT PROFESSOR: WHAT TIME ..?
Ø PROFESSOR: HEY.. GET A SCAN…
NOT SEEN ANYBODY ASSESSING
IN LAST TEN YEARS…

4. FOETAL DISTRESS
FHR
CTG
pH MSL
APGAR

CORD ROUND THE NECK
NEW INDICATION FOR CS
REPLACING CPD
JOYCE MORGAN 1948
a. INCREASE IN CSMD
MEDIA HYPE
MOST USER FRIENDLY FOR DTO

C.S. WOMAN’S BIRTH RIGHT
Ø C.S. BY CHOICE
Ø C.S. ON REQUEST
Ø C.S. ON DEMAND
"Should doctors perform an elective caesarean section on
request?" !BMJ,1998
Ø November 27, 1999 issue of the British Medical Journal, a feminist Professor of English laments "medical and social prejudices against women sidestepping their biblical sentence to painful childbirth are still with us"
Ø and a consumer advocate states "I do not believe that anyone has the right to demand women give birth vaginally."
20%

CAESAREAN BY CHOICE
Ø "With a scheduled Caesarean section, you and your doctor have agreed to a time at which you will enter the hospital in a fairly calm and leisurely fashion, and he or she will extract your baby
through a small slit at the top of your pubic hair. There are a lot of reasons to schedule a caesarean section… women elect to have a caesarean because they want to maintain the vaginal tone of a teenager, and their doctors find a medical explanation that will suit the insurance company." !
Ø Lovine V,"The Girlfriend's Guide to Pregnancy"
C.S. BIRTH RIGHT OF WOMEN
ANY TAKERS ? 0NLY 4% ITALIAN PREGNANT WOMEN OPTED FOR C.S. BY CHOICE !

b. HANDICAPPED OBSTETRICIAN
LACK OF
SKILL TRANSMISSION
PG SYNDROME CUTTING CHANCES
BUT WHOM TO CUT ?

MATHEMATICS GONE WRONG
ONE CRORE PLUS
HOW MANY CS ?
0NE THOUSAND !

c. LACK OF FACILITY
FACILITY TO CONDUCT CS AVAILABLE EVERY WHERE WITH CRASH COURSES IN CS
OPERATIVE VAGINAL DELIVERY
ALMOST VANISHED……

d. UNNECESSARY CESAREAN SECTION
true or false ?

Or..INEVITABLE CS?

Death by Medicine By Gary Null, PhD; Carolyn Dean MD, ND; Martin Feldman, MD; Debora
Rasio, MD; and Dorothy Smith, PhD
Approximately 4 million births occur annually, with 24% (960,000) delivered by cs. Netherlands, only 8% of births are delivered
by cesarean section.
This suggests 6,40,000 unnecessary cesarean sections—entailing three to four times higher mortality 20 times greater morbidity than vaginal delivery are performed annually in the US.

The US cesarean rate rose from just 4.5% in 1965 to 24.1% in 1986.
Sakala contends that an “uncontrolled pandemic of
medically unnecessary cesarean births is occurring.”

Estimating the proportion of unnecessary Cesarean sections in Ohio using birth certificate data. Koroukian SM, Trisel B, Rimm AA. J Clin Epidemiol 1998 Dec;51(12):1327-34. The results of this study show that approximately
40% of Cesarean sections performed in Ohio have no medical indication that justifies their use and are therefore, unnecessary.

WHO IS BENEFITTED ?
WHO reports: "In the United States the profit motive explained hospital-specific cesarean section rates that
were high even by United States standards."

WHY INCREASE IS NOT WELCOME
Ø U.S. there is a four fold risk of death compared to vaginal birth.
Ø England, emergency cesarean birth has a nine fold risk of death when compared to vaginal and elective
cesareans have a threefold risk.
Ø Women are twice as likely to be re-hospitalized within 60 days of birth when compared with women who have a vaginal birth.

IS IT EVIDENCE BASED ?
NO
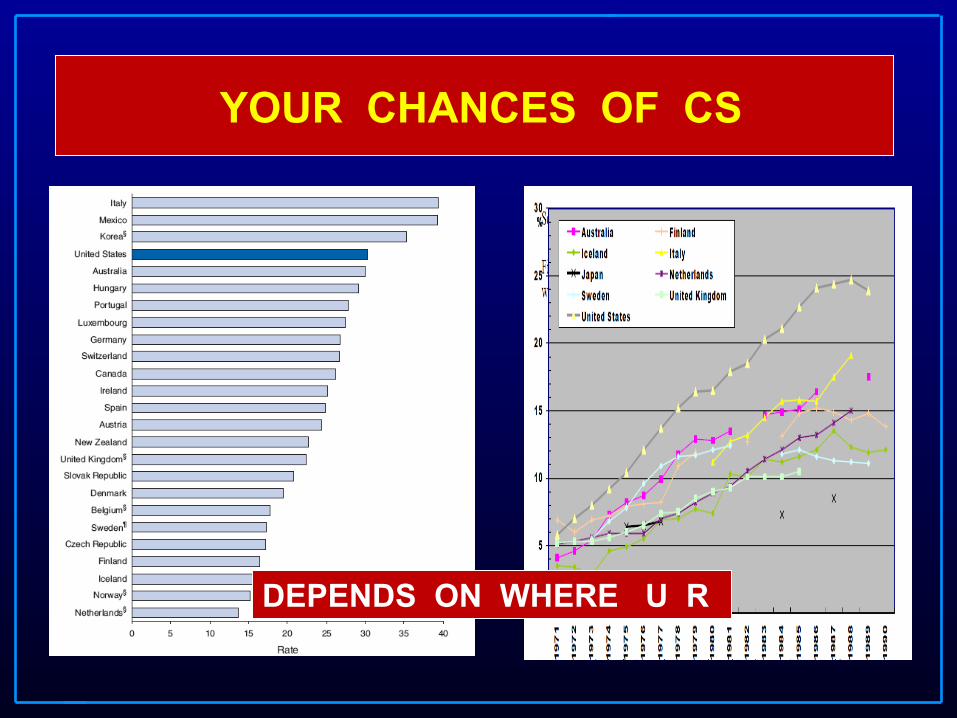
YOUR CHANCES OF CS
DEPENDS ON WHERE U R

R U LUCKY ?
SELECT YOUR PLACE OF DELIVERY

WORLD MAP OF CORRUPTION

Why has the rate of cesarean delivery climbed so dramatically in the past 25 years?
1. Lower tolerance for taking risks
2. Fear of malpractice litigation
3. Increased use of epidural anesthesia ?
4. Increased use of electronic fetal monitoring
5. The convenience of physicians
Sachs BP et al., NEJM ;340:54 – 57
Reasons for Couples choose C-Section
Ø Concern for safety of infant Ø Fear of pain and pushing the baby Ø Perception that a C-section is safer than
vaginal delivery. Ø Social convenience Ø Damage to perineal floor Ø Prior complicated/traumatic births Ø Stress & anxiety TRUE /
FALSE

CEREBRAL PALSY

Reasons for Couples choose C-Section
Ø Concern for safety of infant Ø Fear of pain and pushing the baby Ø Perception that a C-section is safer than
vaginal delivery. Ø Social convenience Ø Damage to perineal floor Ø Prior complicated/traumatic births Ø StrTRUE / FALSE

Risk of maternal death “...the presumed increased risk of maternal death with
elective cesarean delivery traditionally has been the most compelling reason to reject a policy of universal cesarean delivery or "cesarean on demand." However, good evidence is accumulating that this is no longer true; the maternal morbidity and mortality from elective cesarean delivery at term before the onset of labor appear to be similar to those associated with vaginal birth....”
Hannah ME, Lancet 2000;356:1375-83.

OBSTETRIC CALAMITY
HANNAH M E
TBT
Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR.
Lancet.2000 Oct 21;356(9239):1375-83. ...

MATERNAL MORTALITY

MATERNAL MORBIDITY

CS MORBIDITY
AFTERMATH OF CS

PLACENTA ACCRETA

Reasons for Couples choose C-Section
Ø Concern for safety of infant Ø Fear of pain and pushing the baby Ø Perception that a C-section is safer than
vaginal delivery. Ø Social convenience Ø Damage to perineal floor Ø Prior complicated/traumatic births Ø Stress & anxiety TRUE /
FALSE

PELVIC FLOOR DAMAGE
NO

PERINEAL DAMAGE
YES
COSMETIC GYNAEC SURGERY

PELVIC FLOOR DISORDERS
Ø « Does caesarean section prevents from pelvic floor disorders ? »
Ø Urinary and fecal incontinence, POP, sexual dysfunction
Ø Hypothesis :
Ø - Vaginal delivery is the etiology of pelvic floor dysfunction
Ø - Caesarean section - avoid vaginal delivery
Ø - Conclusion : Cs prevents from pelvic floor dysfunction
Ø First point…
Ø Vaginal delivery is not the unique etiology of pelvic floor dysfunction
Ø BMI > 30 g/m2 = risk factor of urinary incontinence at long term follow-up
[Fritel, BJOG, 2005]

Caesarean section is unable to prevent all
urinary incontinence vaginal delivery not the only etiology of urinary incontinence
Pregnancy itself plays a major role
Deffieux et al, 2010
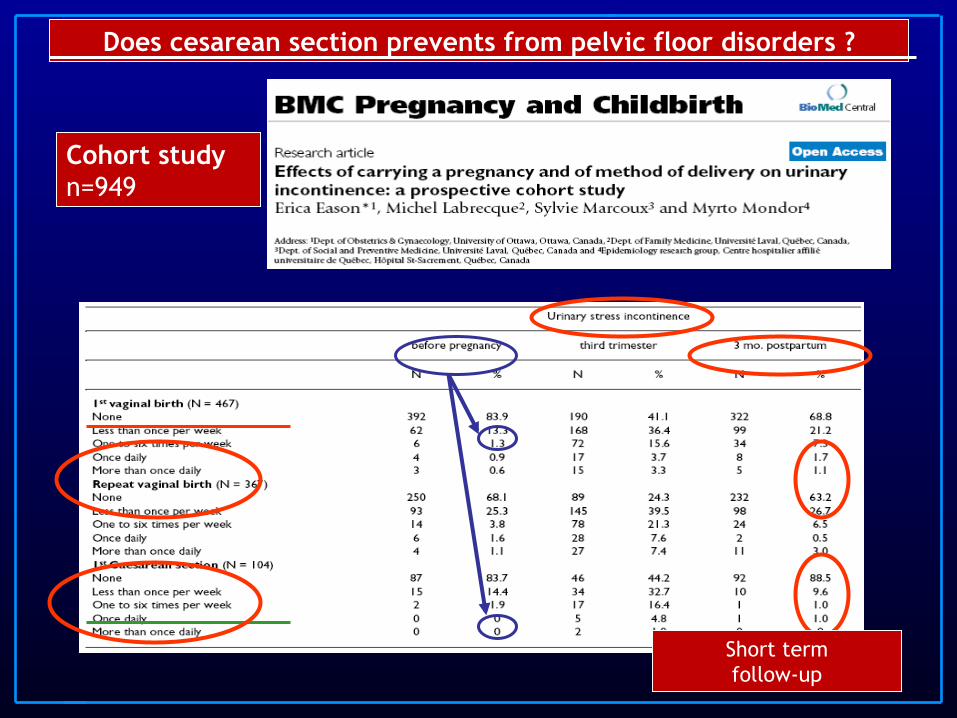
Cohort study n=949
Does cesarean section prevents from pelvic floor disorders ?
Short term follow-up

Does C-section prevents from sexual dysfunction ?
Cochrane Database
Meta-analysis
Elective C-section vs vaginal delivery
3 studies (n=2396)
At 3 months post-partum Perineal pain RR 0.32 [95% CI 0.1-0.5] ** Dyspareunia RR 0.91 [95% CI 0.7-1.1] NS At 2 years post-partum Sexual dysfunction RR 0.95 [95% CI 0.6-1.4] NS Perineal pain RR 0.65 [95% CI 0.3-1.1] NS Unhappiness with sex RR 0.87 [95% CI 0.5-1.5] NS
Does cesarean section prevents from pelvic floor disorders ?

Does cesarean section prevents from pelvic floor disorders ?
Anal sphincter injury during vaginal delivery
Sultan et al NEJM 1993

PRIMA study 1219 primiparous women Faltain et al. Obstet Gynecol 2005
0/I II III/IV CS N=313
N=671 N=81 N=154
Fecal incontinence 8% 15% 19% 8% Urinary incontinence 10% 12% 12% 5% Perineal pain 4% 7% 7% 1% Dyspareunia 27% 41% 54% 29%
Vaginal delivery
Does cesarean section prevents from pelvic floor disorders ?
The prevalence of fecal incontinence is not different
following normal vaginal delivery and C-section

100% CS - IS IT A SOLUTION?
0
20
40
60
80
100
120
25% CS 100% CS
sphincter tear andincontinenceno sphincter tear andincontinencesphincter tear noincontinenceno sphincter tear noincontinence
250 C-section deliveries should be performed
…to prevent one case of fecal incontinence related to anal
sphincter injury

CS TO PREVENT PFD
Scientific data is insufficient to justify an
elective cesarean section in order to avoid
pelvic floor symptoms

VIMS-BELLARY
Ø 8% in 1980 Ø 38% in 2011
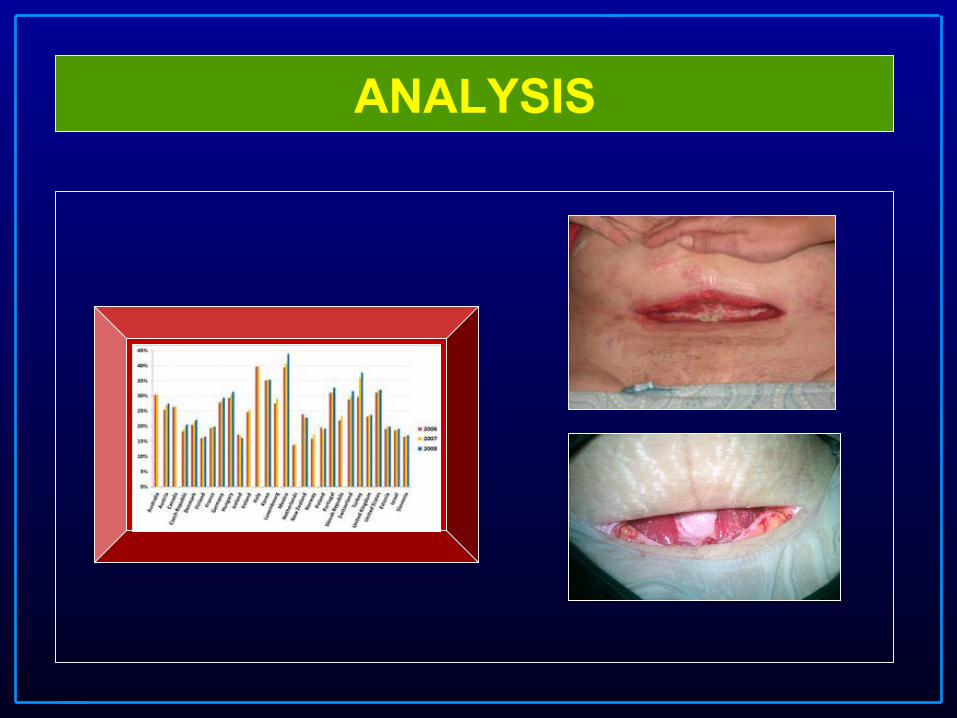
ANALYSIS

Published rates
Ø W.H.O.: – 15 %
– Maximum desirable rate of cesarean section
– No benefit for mother and the fetus for medical reasons
World Health Organisation. Appropriate technology for birth. Lancet 1985;436-7.

Sweden Ø 59 hospitals
Ø 1988 - 1992 – Perinatal mortality
– Rate of asphixia
Eckerlund I, et al., Int J Technol Asses Health Care 1999;15:123 - 35
Minimum cesarean section rate is optimal
No benefit
Outcome based study

England Ø 17 maternity units (one health region) Ø 1988 Ø 36727 singleton pregnancies
• CS rates should be 10 - 12 % • More intervensionist approach in low
birth weight infants 1 Joffe M, et al., J Epidemiol Community Health 1994;48:406 - 11
Outcome based study

Healthy People 2000
Ø Department of Health and Human Services
Ø 15 % by the year 2000
“....the advantages of a safe vaginal delivery over
a cesarean delivery are clear: a vaginal delivery is
associated with lower maternal and neonatal
morbidity and it costs less...”
Healthy People 2000; DHHS publication Nº. (PHS) 91-50212.

Who are involved ?
MOTHER
Childbirth
BEFORE 1950

Who are involved ?
FETUS MOTHER
Childbirth
1950 - 1980

Who are involved ?
Obstetricians
FETUS MOTHER
Health system
Obstetrical Uni-Hospital Midwives
Society
Childbirth
BEYOND 1980

Difficulties for the analysis
Ø Which is the optimun cesarean rate?
Ø Many stategies to reduce the rates
Vaginal Birth =
Quality Caserean Section
= Clasical indicaton or
failure Medical and non medical reason

Factors involved in decision
1. Fetal mortality and morbidity 2. Newborn health 3. VBAC 4. Pelvic floor damage 5. Maternal mortality
MEDICAL

ELECTIVE C.SECTION
Ø 1. A TERM SINGLETON BREECH Ø 2. A TWIN PREGNANCY WITH FIRST
TWIN BREECH Ø 3. HIV Ø 4. BOTH HIV & HEPATITIS C Ø 5. PRIMARY GENITAL HERPES IN THE
THIRD TRIMESTER Ø 6. GRADE 3 AND 4 PLACENTA PRAEVIA RCOG GUIDELINES

CATEGORISATION OF INDICATIONS C.Section
GRADE 1. IMMEDIATE THREAT TO THE LIFE OF THE WOMAN OR BABY
GRADE 2. MATERNAL OR FOETAL COMPROMISE NOT IMMEDIATELY LIFE THREATENING.
GRADE 3. NO MATERNAL OR FOETAL COMPROMISE - NEEDS EARLY DELIVERY
GRADE 4. DELIVERY TIMED TO SUIT THE WOMAN OR STAFF.
RCOG - NCEPOD

VIMS-BELLARY 2004
1350 C.S. 10 consultants
Individual c.s.-
varied from 45 to 200 !
2011…….3210

Factors involved in decision
1.Cost 2.Cultural factors 3.Autonomy - C-section on demand?
NON-MEDICAL

Beth Israel Deaconess Medical Center, Boston, USA
Ø Elective repeat cesarean delivery $ 7.700
Ø Vaginal delivery $ 6.800
Ø Intrapartum Cesarean: $ 10.000
INDIA : Vaginal Delivery- Rs. 2000 to Rs. 10000=00
C.Section - Rs. 10000 to Rs. 25000=00
GOVT. HOSPITALS – COST ??
Cost of delivery
Cultural phenomena - Brazil Ø All birth are attended by obstetricians Ø Training Ø Doctors work in the public and private health
system Ø Status of c-section: modern and technical Ø Women’s body are perceived as sexual
than maternal Ø Genitals are perceived for sexual activity
than for childbearing Nuttall C., et al., BMJ 2000;320:1072

Cesarean section on demand
Ø 31% of female obstetricians would prefer a
cesarean delivery for themselves
Ø LADY DOCTOR’S SYNDROME
Al-Muffti et al. Eur J Obstet Gynecol Reprod Biol 1997:73:1-4

Cesarean section on demand
Ø 31% of female obstetricians would prefer a cesarean
delivery for themselves 1
Ø Italian law mandates that women be given the
option of an elective cesarean, and about 4%
of pregnant women choose it. 2
1 Al-Muffti et al. Eur J Obstet Gynecol Reprod Biol 1997:73:1-4 2 Tranquilli AL, et al., Am J Obstet Gynecol 1997;177:245-246
Autonomy and informed consent
“...performing cesarean section for non medical
reasons is ethically not justified....”
Committee for the Ethical Aspects of Human Reproduction and Women’s Health of FIGO (1999)

Autonomy
Ø We respect with better eyes a woman’s
right to refuse a cesarean delivery
Ø Nobody is interested in respecting woman’s
desire to refuse vaginal delivery
Wagner M et al., Lancet 2000;356:1677-80

confusion
Ø Women’s involvement with the decision preceeding c.s. and
their degree of satisafaction. Mould TAJ et al, Br J Obstet Gynaecol 1999
Ø What is natural ? What is normal….. change it to “open concept of good” Whackerhausen S. Br J Obstet Gynaecol 1999
Ambiguity of terms
Ø Natural as desirable
Ø Natural as hazardous
Ø C-section as safe
Ø C-section as beneficial
for doctors

Inconsistencies in clinical decisions in
obstetrics. Barrett JF, Jarvis GJ, Macdonald HN, Buchan PC, Tyrrell SN,
Lilford RJ. Lancet 1990 Sep 1;336(8714):549-51.
Ø The results of this study show that 30% of Cesarean sections performed in an English teaching hospital were unnecessary.
Inconsistencies in clinical decisions in obstetrics.
Barrett JF, Jarvis GJ, Macdonald HN, Buchan PC, Tyrrell SN, Lilford RJ.
Lancet 1990 Sep 1;336(8714):549-51.
Ø Even more importantly, when physicians were presented at different times with the same information, their opinion as to whether perform or not a Cesarean section was inconsistent in
25% of cases. These data indicate that clinical decisions in obstetrics are often influenced by physicians' personal reasons rather than by medical factors
Conclusion NOT CONCENSUS
“...perhaps the time has come when the risks,
benefits and costs are so balanced between
cesarean section and vaginal delivery that the
deciding factor should simply be the
mother’s preference for how her baby is to be
delivered...” William Benson Harer

The cesarean section should not be used as
an indicator of quality of obstetrical care
C.Section will continue to stay at
Conclusion

What do we need
1. RCT: intention of labor vs elective c-section
2. To accept that is a cultural phenomena
3. Need of a medical and non medical approach
4. Informed Consent

REDUCE
The REDUCE Campaign:
Research and Education to Decrease Unnecessary
Cesarean Sections

British government urging doctors to dissuade
unnecessary Caesarean births
Women's Health News
Published: Saturday, 1-May-2004

ICAN The International
Cesarean Awareness Network, Inc. (ICAN)
is a nonprofit organization founded by Esther Booth Zorn in 1982. ICAN's mission is to improve maternal-child health
by preventing unnecessary cesareans
through education, providing support for cesarean recovery, and promoting Vaginal Birth After Cesarean (VBAC).
. CONGRATULATIONS
to ICAN Chapter Director Krista Cornish Scott on the birth of Colum David on
August 15th!
Colum is an HBAC (Home Birth After Cesarean) baby

Should Early C-Section Be Banned?
Some have accused stars such as Victoria “Posh Spice” Beckham, Claudia Schiffer, Elizabeth Hurley and Madonna of endangering their babies for vanity by choosing early C-sections over old-fashioned childbirth in order to avoid abdominal stretching. “There has been a spike in these designer C-sections

"Too Posh to Push,"
Ø MIDDLE CLASS mothers are 26% more likely to opt for a C.S. than those from the working class.
Ø Women like ‘ POSH SPICE’ VICTORIA BECKHAM are ‘ too posh to push’
DESIGNER C. SECTIONS.

Thank you
Suyajna @ yahoo.com www.suyajna.com

DISCUSSION WILL CONTINUE
And the cesarean sections…

WHAT IS GENTLEMAN DOING ?

PREPARING 3 x 6 FOR …
VAGINAL DELIVERY
PREPARING 3 x 6 FOR …
OBSTETRICIAN

NO…. FUTURE IS ….
EVD EASY VAGINAL DELIVERY
SCS SAFE CESAREAN SECTION
FUTURE
OBSTETRCIS NO LONGER AN
ART
OBSTETRICS WILL BE
SCIENCE WITH COATING OF EBM

ANC
ULTRASONOGRAM
VAGINAL DELIVERY ….
Ø CUMBERSOME Ø STRESSFULL
Ø NIGHT ORIENTED Ø UNPREDICATBLE
Ø HAUNTING UNEXPLAINED FOETAL DEATHS
Ø DIRTY…..KIRI….KIRI….

SALT TO WOUND…
CORD ROUND THE NECK
POSTDATISM HESITANT LABOR DELAY IN DESCENT UNEXPECTED FOETAL DEATHS
COMPRESSION……..OCCLUSION

2012…..
Ø INCREASE THE RATE
Ø INCREASE THE RATE

INDICATIONS FOR VD
NO EVIDECE BASED
INDICATIONS
NO RCT

MODERN OBSTETRICS
Ø WHO CONCEIVES ? Ø PATIENT.
Ø WHO DELIVERS ?
OBSTETRICIAN.
Ø SO ALLOW MIDWIVES TO DELIVER….

SOLUTION…. ANY TAKERS…
DELIVERY SHOULD BE CONDUCTED BY MIDWIVES
REDUCE INSTITUTIONAL DELIVERY

So C.s. are here to stay ….. Can we make C S SAFER ?
WHO's 'Safe Surgery Saves Lives' initiative came out with a 24-point checklist on 25-06-2008