customized titanium single-implant abutments: 2-year
TRANSCRIPT

Customized TitaniumSingle-Implant Abutments:
2-Year Follow-up Pilot Study Torsten ¡emt, LDS, Odont Dr'
Purpose: The aim of this study was to describe an alternative technique to fabricate single-implantrestorations by using adjustable titanium abutments with porcelain applied directly to theabutment, and to follow an early group of patients treated with these crowns. Materials andMethods: Seventeen randomly selected single crowns were consecutively placed in t4 patientsand then followed for 2 years. A protocol of using healing abutments, implant impressions, andadjustment of the final abutnient in the laboratory was used to fabricate the crowns. Results: Theclinical result revealed few clinical problems, and the mean marginal bone loss was 0.4 mm(standard deviation ± 0.57 mm) after t year in function. Conclusion: The conclusion drawn, basedin part on published literature, was that occurrence of mucosal inflammation and marginal boneloss was not related to the use ofthe present protocol. In! I Prosthodont 1998:11:312-316.
Missing single teeth have been restored withsingle implants ad modum Brânemark (Nobel
ßiocare) for more than 15 yearsJ Since the first pa-tients were treated, there has been a continuousdevelopment of the single-implant components tomeet the clinicians' and patients' mechanical andesthetic demands. The basic design of the singleabutment cylinder was first introduced in 1983.''-The cylinder was used as a template for wax-up ofthe crowns in the laboratory as well as for the finalsupport ofthe permanent crown restoration in theoral cavity.* ' The CeraOne implant system {NobelBiocarel was a modificafion of the original abut-menf to allow better control of the tightening of theabufment screw, as well as to allow the use of pre-fabricated ceramic or gold alloy cylinders."' It wasonly after the introduction of the CeraOne systemthat it became possible to use a standardized abut-ment replica in the laboratory, and thereby foavoid handling the original sterile single-implantabutment cylinder in tbe laboratory.
'Associate Professor, Head of Division of Prosthodontics. TiieErénemarii Clinic. COteborg. Sweden.
Reprint request: Or Torsten Jemt, The Brânemarii Ciinic, PubiicDental Health. Medicinarcgatan ¡2 C, S-413 90 COteborg,Sweden.
Standardized single-implant components havethe advantage that prefabricated ceramic or goldalloy cylinders can be used as a base for the finalrestoration. However, the standard single abutmentcylinder does not always allow the crown to followthe contour of the gingival margin when there is adifferent gingival level on the buccal and palatalsurface of the restoration. This may occasionallyplace some part of the crown very deep into thesoft tissue, especially on the palatal side. The re-cently introduced ceramic abutment cylinder^ isdesigned to allow preparation of the cylinder,thereby allowing a more individual placement ofthe crown margin in relation to the soft tissue.Similar techniques with individually designed tita-nium abutments for crown cementation have alsobeen described.''''' Custom-made titanium abut-ments to which ceramic has been directly appliedto avoid crown cementation have also been tested.
The aim of the present 2-year follow-up studywas to present the early clinical performance of sin-gle-implant restorations using custom-made abut-ments onto which porcelain was directly fired.
Materials and Methods
The present study was designed as a retro.spectivestudy. Tbe test group comprised Í4 patients, ran-
The Irternational Journal of Prosthcdcintii 312 il1,Number4,199B
CustomizerlTiMniiimSingie-ImplaiiLAhulmenis
domly selected at one dental clinic (BrânemarkClinic, Cöteborg, Sweden) between August 1993and October 1995. The only criteria for inclusionwas that the access hole of the implant crown wasnot placed on tbe buccal surface of tbe finalrestoration. Eleven of tbe patients were men andthree were women, with a mean age of 28 years(standard deviation ± 13.3 years) at the time of im-plant placement. Ages ranged from 20 to 72 years.
Tbe patients received 17 single-crown restora-tions altogether. Seven crowns were central in-cisors, eight were lateral incisors, and one crowneach was placed in the canine and second premo-lar area. One central incisor was placed in themandible; the remaining 16 crowns were installedin the maxilla.
All patients were treated with Brânemark im-plants and standard abutments (Nobel Biocare) ac-cording to routine surgical procedures presentedelsewhere.•''^ Two patients had removable partialdentures after the second surgical procedure. Theremaining 12 patients were provided with provi-sional acrylic crowns, cured to temporary plasticcylinders (DCA 159, Nobel Biocare). These crownswere connected to the abutments. The final impres-sion of tbe implant was performed at a mean of 55days (SD ± 19 days) after the second surgical stage.
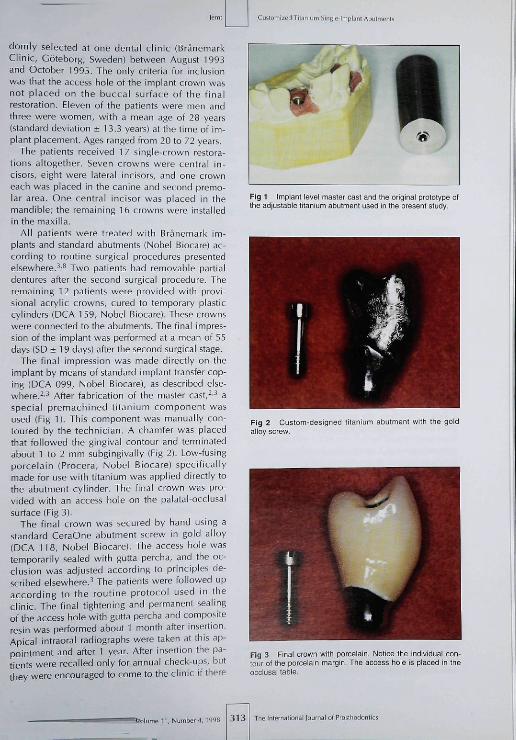
The final impression was made directly on theimplant by means of standard implant transfer cop-ing (DCA 099, Nobel Biocare), as described else-where.''^ After fabrication of the master cast,'-^ aspecial premachined titanium component wasused (Fig 1). This component was manually con-toured by tbe technician. A chamfer was placedthat followed the gingival contour and terminatedabout 1 to 2 mm subgingivally (Fig 2). Low-fusingporcelain (Procera, Nobel Biocare) specificallymade for use with titanium was applied directly tothe abutment cylinder. The final crown was pro-vided with an access hole on the palatal-occlusalsurface (Fig 3).
The final crown was secured by hand using astandard CeraOne abutment screw in gold alloy(DCA 118, Nobel Biocare). The access hole wastemporarily sealed witb gutta percha, and the oc-clusion was adjusted according to principles de-scribed elsewhere.^ The patients were followed upaccording to the routine protocol used in theclinic. The final tightening and permanent sealingof tbe access bole with gutta percha and compositeresin was performed about 1 month after insertion.Apical intraoral radiographs were taken at this ap-pointment and after 1 year. After insertion the pa-tients were recalled only for annual check-ups, butthey were encouraged to come to the clinic if there
Fig 1 impiant levei master cast and tine originai protetype ofthe adjustabie titanium abutment used in the present study.
Fig 2 Custom-designed titanium abutment with the goldalioy screw
Fig 3 Final crown with porcelain. Notice the individual con-tour ot the porcelain margin. The access hoie is placed in theocclusai table.
, Number4, 1998 313 The Intern aliona i i oí Prost il odont i es

Cu Storni zed Tiianium Singie-lmpiani Abuimt-nts
were any problems with their implant restorations.Careful examination was performed annually to as-sess clinical stability, oral maintenance, soft tissuecondition, and occlusion. The radiographs wereanalyzed with regard to osseointegration and mar-ginal bone loss. Bone loss was measured to theclosest 0.3 mm in relation to the reference point oftbe implant, as described elsewhere.''^
One patient, provided with one central incisor,was lost to follow-up after insertion and final tight-ening of the crown. This patient moved to anothercity. The remaining 13 patients were followed for 2years.
Results
All implants integrated and remained integratedduring the 2 years of follow-up. One of the crownsbecame loose and the gold alloy screw had to beretightened once during the first year of function.All crowns were clinically stable during the secondyear of follow-up.
One patient presented with a buccal fistula afterinsertion. This fistula healed after the crown wasremoved and the components and soft tissue werecarefully cleaned with 3% hydrogen peroxide solu-tion. All remaining patienis showed soft tissuehealth with no sign of severe infection, hyperpla-sia, or fistulas during the follow-up period.
The mean marginal bone level was 0,5 mm (SD± 0.46 mm] below the reference point of the im-plant at 1 month after insertion of the crowns. After1 year in function, tbe corresponding mean mar-ginal bone level was 0,9 mm (SD ± 0.66 mm). Tbebone level ranged from 0 mm to 1.7 mm below tbereference point at 1 month after insertion, and from0 mm to 1.7 mm at tbe first annual check-up. Themean marginal bone loss was 0.4 mm (SD ± 0.57mm] during tbe first year of function.
Discussion
Tbe use of custom-made titanium single abutmentsshowed favorable short-term results, Tbe result iscompletely comparable to other single-abutmentcomponents used for tbe Brânemark implant sys-tem.'''*''""^" All implants remained integrated, andtbe number and character of the few clinical prob-lems compared favorably to earlier reports.'''''"'"•^"
Tbe present technique is based on a titaniumcomponent that is contoured in the laboratory afteran implant head level impression has been made.This protocol involves both disconnection and re-connection of tbe temporary abutment cylinder, aswell as manipulation of tbe titanium cylinder in tbe
laboratory, A clinical concern could be raised tbatlhe removal and replacement of the temporaryabutment may break the seal between tbe mucosaand the titanium cylinder, thereby inducing boneloss as indicated in an experimental animalstudy.^' Handling of the titanium cylinder in thelaboratory may cause further contamination ofthetitanium surface, tbus potentially causing morebone loss as well as soft tissue inflammation. Therisks of marginai bone loss and mucosal inflamma-tion accordingly have to be evaluated in connec-tion witb the present technique,
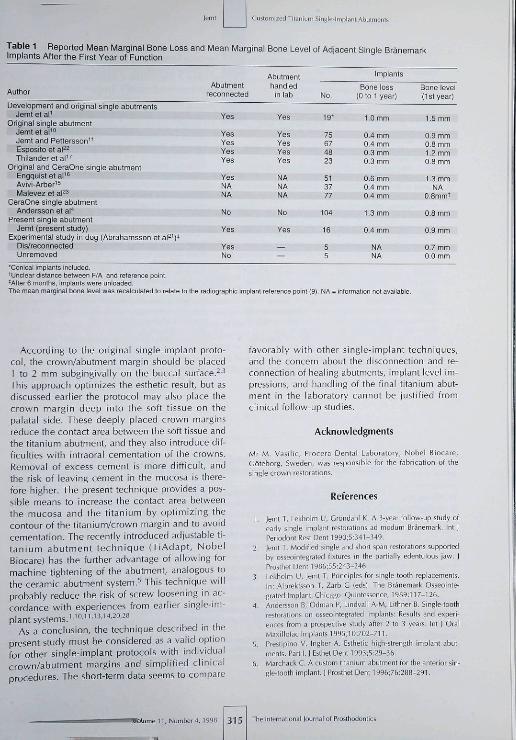
Abrahamsson et aP' bave shown in an animalstudy that tbe marginal bone level was significantlymore apical at implants where abutments bad beenrepeatedly disconnected and reconnected during ahalf-year period as compared to implants wherethe abutments bad been left undisturbed. Thesefindings may imply tbat the present techniquecaused more bone loss tban if a permanent single-implant abutment was connected and left undis-turbed at second-stage surgery. However, the pre-sent sbort-term results, witb few infection problemsand minimal bone loss, do not support the above-mentioned concern. Tbe clinical significance ofAbrahamsson's results can also be compared withclinical follow-up studies for the original single-im-plant technique with healing abutments, and theCeraOne technique where no healing abutmentswere used.^''''""-"'^-^"^-* From Table 1 it can be ob-served that tbe overall mean marginal bone loss forsingle-implant treatment was about 0.6 mm duringthe first year in function. The results seemed to betbe same for studies using the implant/abutmentjunct ion as the reference for their measure-ments''"""'^'^^ as for studies'''"'"'^^''^''^ using theimplant radiographie reference point''^ Bone lossamong the studies varied from 0.3 mm to 1,3 mm(Table 1). The variations were probably related tométhodologie variations such as surgical tech-niques and time of radiographs after the secondsurgery, ratber than related to components andtechniques used for restoration. The conclusiondrawn from Table 1 could be that, irrespective ofthe technique, basically ali studies presented amean marginal bone level 0.8 mm to 1.0 mmbelow the implant reference point at 1 year afterinsertion. Tbe results of the present study com-pared well with the marginal bone level reportedfrom other single-implant studies (Table 1]. Thislevel of the marginal bone after 1 year is also com-parable with tbe bone response after conventionaltwo-stage implant surgery, where abutments bavebeen left undisturbed after second surgery in par-tial and edentulous ap
The Intemalional loumal of Proilhodontics 3 1 4 Volume 11, Number 4, 199.
Custoiiiiied Tila 1 Single-Implant Abutmenls
Table 1 Reported Mean Marginal Bone Loss and Mean Marginal Bone Level of Adjacent Sinqle BrânemarkItnplants After the First Year ol Function
Author
Development and original single abutmentsJemt et aP
Original single abutmentJemt et a l ' "Jemt and Pettersson"Esposito et af^Thilander et a l "
Original and OeraOne single abutmentEngquist et al '^Avivi-Arber'^Malevez et al^^
CeraOne single abutmentAndersson et al""
Present single abutmentJemt (present study)
Experimental study in dog (Abrahamsson et al^^)*Dis/reconneotedUn removed
Abutmentreconnected
Yes
YesYesYesYes
YesNANA
No
Yes
YesNo
Abutmenthandled
in lab
Yes
YesYesYesYes
NANANA
No
Yes
——
No.
19-
75674823
513777
104
16
55
Implants
Bone loss(0 to 1 year)
1.0 mm
0.4 mm0.4 mm0.3 mm0.3 mm
0.6 mm0.4 mm0,4 mm
1.3 mm
0.4 mm
NANA
Bone level(1 st year)
1.5 mm
0.9 mm0.8 mm1.2 mmO.B mm
1.3 mmNA
0 8m mi
0.8 mm
0.9 mm
0.7 mm0 0 mm
'Conical implants included.tundear distance between F/A and reference point.'After 6 monttis, implants were unloaded.The mean marginal bone level was recalculated to relate to the adiographic implant reference point |9). NA = inlormation not available.
According to the original single-implant proto-col, the crown/abutment margin should be placed1 to 2 mm subgingivaily on tbe buccal surface,^''This approach optimizes tbe esthetic result, but asdiscussed earlier the protocoi may also place thecrown margin deep into the soft tissue on thepalatal side. These deeply placed crown marginsreduce the contact area between the soft tissue andthe titanium abutment, and they also introduce dif-ficulties with intraoral cementation of the crowns.Removal of excess cement is more difficult, andtbe risk of leaving cement in the mucosa is there-fore higher. The present technique provides a pos-sible means to increase the contact area betweenthe mucosa and the titanium by optimizing thecontour ofthe titanium/crown margin and to avoidcementation. The recently introduced adjustable ti-tanium abutment technique (TiAdapt, NobelBiocare) has the further advantage of allowing formachine tightening of the abutment, analogous tothe ceramic abutment system,^ This technique wiiiprobably reduce the risi< of screw loosening in ac-cordance with experiences from earlier single-im-plant systems.''"-'"''^''^»'^^
As a conclusion, the technique described in thepresent study must be considered as a valid optionfor other single-implant protocols with individualcrown/abutment margins and simplified clinicalprocedures. The sbort-term data seems to compare
favorably with other single-implant techniques,and the concern about the disconnection and re-connection of healing abutments, impiant level im-pressions, and handling of the final titanium abut-ment in the laboratory cannot be justified fromclinical follow-up studies.
Acknowledgments
Mr M, Va.iilic, Procera Dentdl Laboiatory, Nobi-I Biocare,Göteborg, Sweden, was responsible for the fabrication of thesingle crown reçtorations.
References
1. leml T, Lekhoim U, Grúndahl K. A 3-year follow-up study ofeady single implant reslorslions ad modum Brânemark. Int JPeriodort Rest Dent 1990;5:34l-349.
2. Jemt T. Modified single and abort span restorations supportedby osseointegrated fixtures in the partiallv edentulous jaw. JProstbet Dent 1986;55:243-246,
3. Lekhoim U, Jemt T. Principles for single tooth replacements.In: Albrektüon T, Zarb G (edsl. The Brânemark Osseointe-grated Implant. Chicago: Quintessence, 1939:117-126.
4. Anderssor B, Otiman P, Lindvall A-M, Lithner B. Single-toothrestorations on OSSEO integrated implants: Results and experi-ences from a prospective study after 2 to 3 years. Int | OralMa^iillofac Implanls 1995;10:702-711,
5. Preslipino V, Ingber A. Esthetic high-strength implant abut-ments. Part ;. i Esthet Dent 1993;5:39-36,
6. Marchack C, A custom titanium abutment for the anterior sir-gle-looth implant. | Proslliet Dent 1996;7S:288-291.
Mume I I Number 4,1998 3 1 5 The Internstioral lournal of Prosthodoniics

Customiïed Tltaniurr Single-lmpl.inl Abutments
7. Schmitt S, Chance D. A custom titanium implant-retained sin-gle-tooth restoration: A clinical report. Int | Oral Maxillofaclmplants199fi:l1:7ß2-786.
8. Lekholm U. Clinical procedures for treatment with osseointe-grated dental implants. I Prosthet Dent 1983;50:n 6-120.
9. Hollendei L, RocUer B. Radiographic evaluation of osseoin-tegrated implants of the jaw, Dentomaxillofac Eadiol 19Ö0;9:91-95.
10. lemt T, Laney W, Hards D, hienry P, Krogh P, Polizzi G, eta i .Osseo in teg rated implants for single-tooth replacemenis. Aone-year report from a multicenter prospective study, Int JOral Maxillofac Implants 1991 ;6:29-36.
11. Jemt T, Pettersson P. A 3-year follow-up study on single im-plant treatment. | Dent I993;21:203-208.
12. Schmitt A, Zarb G. The longitudinal clinical effectiveness ofosseointegrated dental implants for single-tooth replacement.Int] Prosthodont 1993;6:157-202.
13. Laney W, lemt T, Harris D, Henry P, Krogh P, Poliïzi G, et al.Osseointegrated Implants lor single tooth replacements:Progress report from s rnulticeiiter prospective study after Jyears. Int | Oral Maxillofac Implants 1994;9:49-54,
14. Elifelt A, Qrlsson GE, Borjesson C. Clinical evaluation of smgle-tooth restorations supported by osseointegrated implants: A ret-rospective study. Int ] Oral Maxillofac Implants 1994;9:179-i 83.
15. Avivi-Arber L. Prosthodontic Replacement of the MissingSingle Tooth With Implant-supported Prostheses ad modumBrânemark |MSc thesis|. Toronto: University of Toronto, 1994.
16. Engquist B, Nilson H, Ästrand P. Single-tooth replacement byosseointegrated Brlnemark implants. A retrospective study of82 implants. Clin Oral Implants Res 199S;6:238-245.
17. Thiiander B, Ödman ), Cröndahi K, Friherg B. Osseointe-grated implants in adolescents. An alternative in replacingmissing leetii. Eur I Orthod 1994;! 6:84-95.
18. Cordioii G, Castagna S, Corsoiati E. Single-tooth implant re-habilitation: A retrospective study of 67 implants. Int ] Pros-thodort I9')4;7:535-531.
19. Haas R, Mensdor f f -Pou i l l y N, Ma i la th C, yVatzek G.Brâremark single-tooth implants: A preliminary report of 75implants. | Pioîlhet Dent 1995:73:274-279.
20. Henry P, Laney W, Jemt T, Harris D, Krogh P, Poli^zi G, et al,Osseointegrated implants for single-tooth leplacement, Aprospective 5-year multicenter study, Int | Oral Maxillofaclmplants1996;l1:45CM55.
21. Abrahamsson I, Berglundh T, Liridhe J. The mucosal barnerfollowing ahutment d is/reconnect i on. An experimental studym dogs. J Gin Periodontoi 1997;24:56a-572.
22. Esposilo M, Ekestuhbe A, Gröndahl K, Radiological evaluationof marginal bone loss at too th surfaces fac ing singleBrinemark implants. Clin Oral Implants Res 1993:4:151-157.
23. Malevez CH, Hermans M, Daelemans PH. Marginal bonelevels at Brânemark system implants used for single toothrestoration. The influence of implant design and anatomicalregion. Clin Oral Implants Res 1996;7:162-i 69.
24. lemt T, Lekholm U. Oral implant treatment in posterior par-tially edentulous jaws: A 5-vear follow-up report, Int ] OralMaxillofac Implants 1993;8:635-640.
25. lemt T, Chai |, Harnett |, Heath R, Hutton |, |ohns R, et al. A5-year prospective multicenter follow-up report on overden-tures supported by osseointegrated implants. Inl | OralMaxillofac Implants 1996;11:29!-298.
26. van Steenberglie D, Lekholm U, Bolender C, Folmer T, HenryP, Herrmann I, el al. The applicability of osseointegrated oralimplants in the rehabi l i ta t ion of partial edentul ism: Aprospective multicenter study on 558 fixtures, Int ] OralMaxillofac implants 1990;5:272-28l,
27. Adell R, Eriksson B, Lekholm U, Brânemark P-1, |emt T. Along-term follow-up study of osseo i meg rated implants in thetreatment of totally edentulous jaws Int I Oral MaxillofacImplants 1990;5:34 7-359.
28. lornéus L, Jemt T, Carlsson L. Loads and designs of screwjoints for single crowns supported by osseointegrated im-plants, Int I Oral Maxillofac Implants 1992;7;353-359.
Literature Ai?stract
Effects of dental laboratory processing variables and in vitro testingmedium on the porcelain adherence of high-palladium aiioys.
The purpose of this study was to examine the effects of several dental laboratory process-
ing variables on the porcelain adherence of fhree representative high-palladium alloys of the
Pd-Cu-Ga and one Pd-Ga type. An Au-Pd alloy served as control Five cast plates were
cast from each of the five aiioys lor eaoh of the six experimental variables (total number of
150 specimens] and prepared and oxidated initially following the manufacturer s instruction.
Four layers cf porcelain were subsequently applied. After final glazing, the metal ceramic
specimens were subjected to fracture of the porcelain with biaxial flexure in constant strain.
The area fraction of adherent porcelain was calculated with a standardized spectrometric
technique. The effects of several processing valables en the porcelain adherence were evalu-
ated. The authors concluded, recasting without adding new metal did negatively affect one
Pd-Cu-Ga and one Pd-Ga alloy. Porcelain stnpping did not negatively affect the adherence of
the tested alloys. Altering the oxidation procedures recommended by the manufacturers
should be performed with oaution,The Au-Pd alloy exhibited the highest porcelain adherence,
Papazoglou E, Brantley WA, Johnston WM, Cair AB. J Prosthst Dent 1998:79:514-519.References: 44. Reprints: Dr ElstiatioE Papazoglou, Section of Restorative Dentistry, Prosthodonticsand Endodortics, College ol Dentistry, The Ohio State University, 305 W. 12th Avenue, Room 3001-C,Columbus, OH 43210-1241—J. Kihl
lournal of Prosthodoniics Volume 11, Number 4, 1998
