current status of hiv surveillance in children: gaps and future directions mary lou lindegren, md...
TRANSCRIPT

Current Status of Current Status of HIV Surveillance in Children: HIV Surveillance in Children: Gaps and Future DirectionsGaps and Future Directions
Mary Lou Lindegren, MDGlobal AIDS Program
Centers for Disease Control and Prevention5th IAS Conference 2009

OutlineOutline
• Current data needs, sources, and estimates– Incidence of HIV among children born to HIV-
positive mothers – HIV free survival – HIV prevalence among children– Morbidity– Mortality
• Future approaches to expanding pediatric HIV surveillance

Magnitude of the ProblemMagnitude of the Problem
• ~ 2 million children (<15 years) living with HIV; 90% of them live in sub-Saharan Africa¹
• ~ 2,086,000 million HIV+ women give birth globally (2005, UNICEF)
• An estimated 370,000 children < 15 became infected with HIV in 2007
¹From the 2008 UNAIDS report on the Global Epidemic

Births to HIV infected mothers•Estimates-UNAIDS•ANC surveillance •L&D surveillance•PMTCT program•HIV case reporting •Immunization surveys
Prevalence and morbidity•Population-based surveys with HIV testing, younger ages* •OI surveillance •HIV case reporting or advanced HIV case reporting •ART outcomes •Most at risk surveys •HIV drug resistance •ANC surveillance
HIV infection Advanced HIV Death
*In epidemics where infection is driven by the general population
Key HIV surveillance data points, Key HIV surveillance data points, 2009 and future2009 and future
Incidence•Report early infant diagnosis •Immunization surveys
Mortality•Vital registration •Verbal autopsy
HIV exposure
•HIV- free survival•Population-based surveys*

Lack of HIV surveillance data for Lack of HIV surveillance data for childrenchildren
• Population-based surveys include persons 15-49 years, few countries have included children<15
• Health facility surveys seldom include children
• Limited data on HIV-related morbidity in children
• Limited systematic measurement of PMTCT impact
• Mortality data are limited to infant mortality, neonatal mortality and peri-natal mortality and AIDS is seldom reported

Missed Opportunities for Missed Opportunities for Prevention, Diagnosis, and Prevention, Diagnosis, and
Treatment for ChildrenTreatment for Children• Globally, inadequate scale-up of effective PMTCT
– Poor coverage HIV testing in ANC - 18% in 2008– Few pregnant women with HIV get ARVs- 34%
• Poor linkage and lost to follow-up from PMTCT• Lack of identification of HIV-infected children• Small % of those who need ART are getting it• Majority starting ART at an older age• Low rates of retention in care and treatment

Children <15 as a percent of all people currently on USG supported ART treatment, FY 2008 APR
7%
8%
3%
10%
5%
8%
5%
9%
8%
9%
6%
10%
10%
0 50,000 100,000 150,000 200,000 250,000 300,000 350,000 400,000 450,000
Guyana
Vietnam
Haiti
Rwanda
Cote d'Ivoire
Mozambique
Ethiopia
Uganda
Tanzania
Zambia
Nigeria
Kenya
South Africa
Total number of adults on treatment
Total number of children on treatment

Need for Better Data Need for Better Data New WHO GuidelinesNew WHO Guidelines
• All infants should have HIV exposure status determined ideally before 6 weeks of age
• HIV-exposed infants should have viral test (HIV nucleic acid test) at 4-6 weeks of age
• Early initiation of ART for all HIV-infected infants regardless of clinical or immunologic stage significantly reduces risk of death and disease progression
• HIV testing recommended for any child presenting to health facilities with signs, symptoms or medical conditions that could indicate HIV

HIV PrevalenceHIV Prevalence
2.5
Year
Mill
ions
0
1.5
2.0
2.5
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
0.5
1.0
This bar indicates the range around the estimate
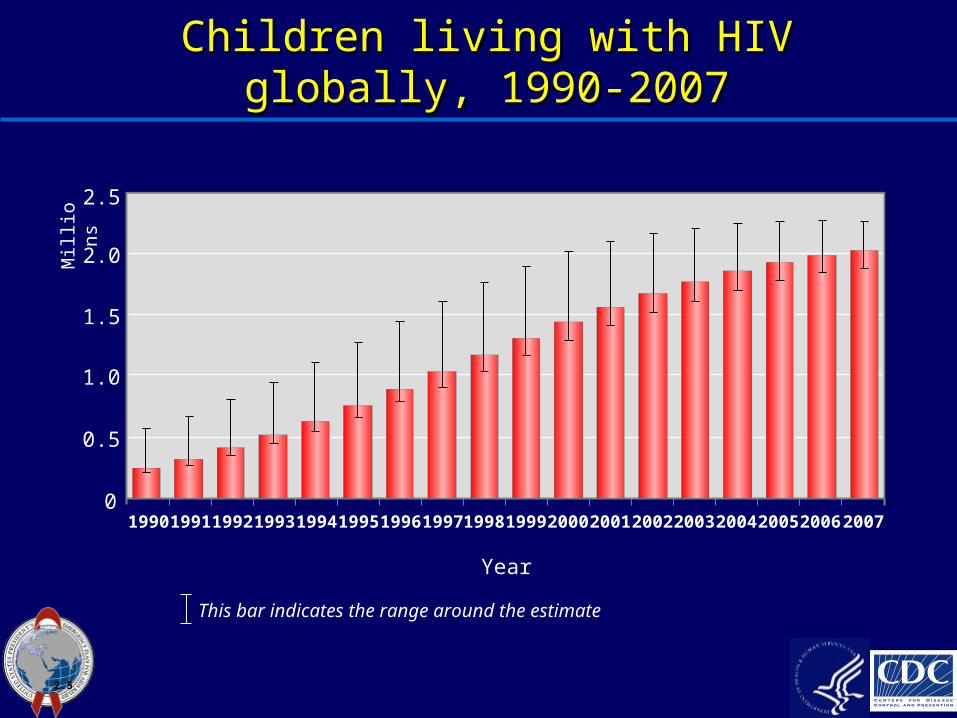
Children living with HIV globally, 1990-Children living with HIV globally, 1990-20072007

UNAIDS estimatesUNAIDS estimates
• UNAIDS estimates based on modeling of data and assumptions, including:– HIV prevalence in adult women (ages 15-49)– Fertility rates– Survival of HIV-positive women– Childhood survival
• Population-based data collected among children has not yet informed these estimates

National Population-based Surveys National Population-based Surveys With HIV testingWith HIV testing
• Conducted in 25 countries since 2000• Data used to fill in gaps and improve
estimation • Recommended for high burden, generalized
epidemics – Countries with prevalence <5% conducted surveys
• Some countries have conducted >1 survey• Only three countries- Botswana, South Africa
and Swaziland—have sampled children <15

Results Of Population-based Results Of Population-based Surveys In Three Southern African Surveys In Three Southern African
CountriesCountries• Botswana 2004
– 1.5-4 yrs 6.3%– 5-9 yrs 6.0%– 10-14 yrs 3.9%
• Swaziland 2007– 5-9 yrs 4.2%– 10-14 yrs 2.6%
• South Africa 2002, 2005– 2-14 yrs Males 3.2%
Females 3.5%• Additional risk factor data collected
– HIV status of mother and father– Receipt of PMTCT– Breast-feeding by biological mother and non-biological mother – Non MTCT risk factors, including sexual, nosocomial, etc

Population based Surveys with HIV Population based Surveys with HIV TestingTesting
ChallengesChallenges
• Should be conducted in high burden, generalized epidemics– consideration should be given to critical age
groups to include (e.g., <2, 2-9, 10-14)
• Sample Size Considerations• Logistics and expense• HIV Counseling issues• Ethical considerations
– returning HIV test results

HIV IncidenceHIV Incidence

Year
1990 19911992 1993 1994 1995 1996 199719981999 2000 2001 20022003 2004 20052006 20070
400 000
500 000
600 000
200 000
300 000
100 000
This bar indicates the range around the estimate
2.6
New HIV infections among children New HIV infections among children 1990-20071990-2007

Table 1: Estimated number of pregnant women and children (0-14 years) living with HIV/AIDS in the PEPFAR focus countries
Country
Estimated number of HIV pos pregnant women, 2007, PEPFAR
Estimated number of HIV pos pregnant women, 2007, UN Estimated number of children
living with HIV/AIDS at end of 2007, UN
Botswana 15,698 11000 15,000
Cote d'Ivoire 60,192 28,000 52,000
Ethiopia 145,314 66,000 92,000
Guyana 325 <500 1500
Haiti 8,339 5,100 6,800
Kenya 101,290 76,000 155,000
Mozambique 136,960 97,000 100,000
Namibia 10,441 9,400 14,000
Nigeria 236,360 190,000 220,000
Rwanda 15,120 11,000 19,000
South Africa 352,640 220,000 280,000
Tanzania 138,243 100,000 140,000
Uganda 87,172 78,000 130,000
Vietnam 6,616 3,900 3,800
Zambia 89,300 76,000 95,000
All Countries 1,404,010 971,400 1,324,100
Estimates of the number of infants born to HIV-infected mothers are critical for determining coverage and targets for infant testing and co-trimoxazole (CTX), however, there are discrepancies that need resolution between PEPFAR estimates presented in the table above, which use annual number of births and ANC prevalence, and modeled estimates from UNAIDS, which are much lower (971,400)
Systematic MeasurementSystematic Measurement of PMTCT Impact of PMTCT Impact
• Possible Population-based Approaches– PMTCT/EID Program Data– HIV Case Reporting– Immunization Clinic Surveys– Population-based DHS Surveys
• Several Proposed Outcome Measures– HIV-transmission rate– HIV-free survival (incorporates early and late
transmission and survival benefits)

Possible Approaches to Measure Impact: Possible Approaches to Measure Impact: PMTCT/EID Program Data, BotswanaPMTCT/EID Program Data, Botswana
• High coverage (>95%) of ANC, HIV testing, and delivery in a health facility
• 90% of HIV+ women receive at least some PMTCT intervention
• Impact can be described because of high coverage of PMTCT and successful early infant diagnosis program
• Estimated transmission rate to infants at 6 weeks is 25% with no program and <5% with PMTCT program

PMTCT coverage, BotswanaPMTCT coverage, Botswana

Botswana infant HIV transmission 2007
624 (4.7%)13395Total
1819950.9%HAART starting before pregancy
158001.9%HAART starting during pregnancy
24191422.6%AZT + SD-NVP
350145824%none
HIV-positive infants
expected
# delivering women in category^
MTCT rate at 6 weeks*
PMTCT received
*Botswana Early Infant Diagnosis program, 2007)^Botswana national PMTCT program, 2007

Limitations of Facility-based Limitations of Facility-based Program DataProgram Data
• Difficult to obtain standard, representative data – Miss those who do not access services (ANC, L/D, etc)– Varying coverage of PMTCT and EID – Limited information on those who are lost to follow-up
• Data on PMTCT ARV regimens not generally available (new indicator)
• Misses women who seroconvert post-natally• Sites may differ significantly in data quality and
program performance• Potential for duplicate counting• National program data are difficult to obtain for
surveillance use
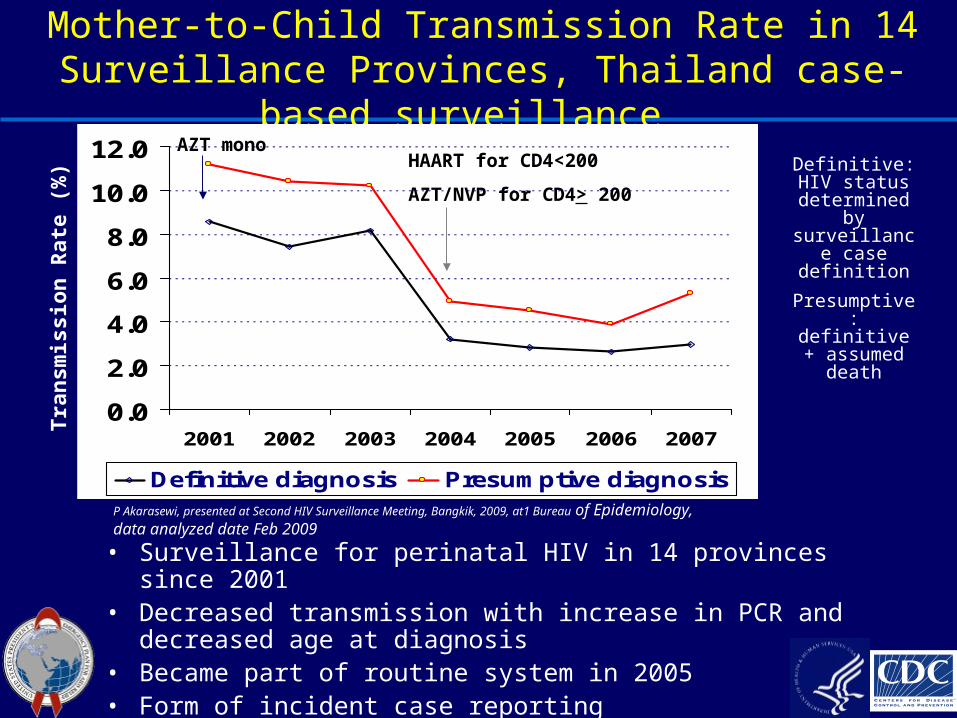
Mother-to-Child Transmission Rate in 14 Surveillance Provinces, Thailand case-based
surveillance
P Akarasewi, presented at Second HIV Surveillance Meeting, Bangkik, 2009, at1 Bureau of Epidemiology, data analyzed date Feb 2009
Tra
nsm
issio
n R
ate
(%
)
NVP
0.0
2.0
4.0
6.0
8.0
10.0
12.0
2001 2002 2003 2004 2005 2006 2007
Definitive diagnosis Presumptive diagnosis
AZT monoHAART for CD4<200
AZT/NVP for CD4> 200
Definitive: HIV status
determined by
surveillance case
definition
Presumptive: definitive +
assumed death
• Surveillance for perinatal HIV in 14 provinces since 2001• Decreased transmission with increase in PCR and
decreased age at diagnosis • Became part of routine system in 2005 • Form of incident case reporting

Possible ApproachesPossible ApproachesImmunization Clinic SurveysImmunization Clinic Surveys
• Measure “Incidence” of HIV among infants attending PHC for immunization services (EID) (cumulative effectiveness of PMTCT)
• Anonymous, unlinked testing survey conducted on infants attending immunization clinics at 6 weeks of age in 3 urban and 4 rural clinics in SA; mothers were asked for written informed consent and offered linked PCR testing for HIV for their infants
• HIV antibody testing (infant exposure status) with subsequent PCR testing-qualitative RNA assay (early infection rate)
• Mothers were asked outcomes of previous pregnancies to estimate infant and child mortality rates
• Estimated transmission rate was 20.2%, 7.5% of all 6 week old infants were HIV infected
• Subsequent survey had testing with informed consent, post-test counseling, and linkage to care and treatment for mother and baby
• Uptake 91%, acceptable and feasible in three clinics in South Africa
•Rollins, AIDS 2007; Rollins AIDS 2009

Possible Approaches: Modification ofPossible Approaches: Modification ofPopulation-based surveys to Measure Population-based surveys to Measure
ImpactImpact• More detailed questions on PMTCT enrollment,
interventions, infant feeding, and household child mortality
• Collected DBS from all children < 2 years (HIV exposure and infection status)
• Estimate HIV free survival= #born in last 2 yrs-(#infected +# died)/#born in last 2 yrs and transmission rate
• Consider addition of “verbal autopsy” interview for recent child deaths to approximate HIV-attributable infant mortality
• Use of adults in these surveys as index cases to identify infants for inclusion
Stringer E, et al Bulletin of WHO; January 2008, 86 (1)

MorbidityMorbidity

HIV prevalence and HIV testing in TB HIV prevalence and HIV testing in TB patients, worldwide, 2006: patients, worldwide, 2006: What about data What about data
for children?for children?
WHO. Global Tuberculosis Control 2008. Surveillance, Planning, Financing.
% of notified TB patients tested for HIV:
America – 32%
Europe – 46%
Africa – 22%

Incidence of Selected AIDS-Defining Incidence of Selected AIDS-Defining Condition, 1Condition, 1992-2001, USA*
0
0.8
1.6
2.4
3.2
4
'92 '93 '94 '95 '96 '97 '98 '99' 2000 2001
Incid
en
ce P
er
100 C
hil
dre
n a
t R
isk
PCP LIP HIV EncephWasting Bacterial Infect
Year
HAART eraHAART era
1992 Overall 13% 2001 Overall 2%
*Pediatric spectrum of Disease project

MortalityMortality

Year
1990 19911992 1993 1994 1995 1996 199719981999 20002001 20022003 2004 20052006 20070
300 000
400 000
500 000
100 000
200 000
This bar indicates the range around the estimate
2.7
Child Deaths due to AIDS, Globally, Child Deaths due to AIDS, Globally, 1990-20071990-2007

Estimated impact of AIDS on under-5 child Estimated impact of AIDS on under-5 child mortality ratesmortality rates – – Selected African countries, 2010Selected African countries, 2010
Source: US Bureau of the Census
250
200
150
100
50
0
per 1000 live births with AIDS
Botswana Kenya Malawi Tanzania Zambia Zimbabwe
without AIDS

Vital registration in AfricaVital registration in Africa
Mathers CD, Ma Fat D, Inoue M, Rao C, Lopez AD. Counting the dead and what they died from: an assessment of the global status of cause of death data. Bull World Health Org 2005;83:171-7.

MortalityMortalityFuture DirectionsFuture Directions
• Lack of reliable cause of death information in vital registration systems contributes to significant gaps in mortality data– Need for improvement in overall vital registration
• Emerging models to measure cause of death– Verbal autopsy with strengthening of vital
registration (SAVVY: sample vital registration with verbal autopsy-Zambia)
– Morgue/burial surveillance– Hospital surveillance

Future DirectionsFuture Directionsfor HIV Surveillance in Childrenfor HIV Surveillance in Children
• Need for Improved Pediatric surveillance– Burden of the epidemic in children to assess care & treatment
needs, guide program planning– Impact of PMTCT programs on incidence, HIV free survival– Impact of care and treatment programs on mortality
• Expanded surveillance should include:– Sampling children in population-based surveys for high burden
countries with generalized epidemics – HIV surveillance in health facilities (e.g. HIV testing during
immunization visits)– Case-based surveillance registry (e.g. Thailand) – Improve HIV/AIDS mortality surveillance to more active efforts and
improve overall vital registration– Improved OI surveillance (TB at a minimum)– ART outcomes and drug resistance monitoring among children– Linking surveillance data to risk behavior data (increased
understanding of HIV risk exposure)

Future DirectionsFuture Directionsfor HIV Surveillance in Childrenfor HIV Surveillance in Children
• Consider Regional Approaches– Harmonize approach at country level– Different approaches depending on burden of disease in
children and phase of implementation of the program
• Understand ethical and other barriers to including children in these broader population-based surveys
• Use expansion of HIV surveillance to improve surveillance capacity for other child health programs
• Address gaps and needs for adolescent populations (population-based and most-at-risk populations-in and out of school youth)
• Strengthen use of surveillance data
Thank youThank you
• O Shisana, HRSC• T Rehle, HRSC• S Patel, CDC• E Kim, CDC• T Goldman, CDC SA• T Creek, CDC• E Rivadeneira, CDC• T Dinh, CDC SA• N Rollins, WHO