cs 2015 neural regulation of blood pressure christian stricker associate professor for systems...
TRANSCRIPT
CS 2015
Neural Regulation ofBlood Pressure
Christian StrickerAssociate Professor for Systems Physiology
ANUMS/JCSMR - ANU
[email protected] http://stricker.jcsmr.anu.edu.au/BPControl.pptx
THE AUSTRALIAN NATIONAL UNIVERSITY
CS 2015

CS 2015
Aims
At the end of this lecture students should be able to
• locate sensors, integrators & effectors of the reflexes;
• outline the anatomy of the reflex pathways;
• contrast the nature and effect of the arterial baroreflex
(AB) and the cardiopulmonary reflexes (CP);
• explain how AB controls HR, SV and TPR, and CP
mainly venous return;
• recognise how AB establishes beat-to-beat control; and
• point out how these reflexes can be modulated by
respiration and asphyxia/shock.
CS 2015
Contents• Overview of control of blood pressure
– Principles of negative feedback
– Regulated variables
• Arterial baroreflex (AB)– Components: detectors (high pressure baroreceptors) and
afferents, efferents (sympathetic and parasympathetic
output to cardiovascular system), integrator.
• Cardiopulmonary reflexes (CP)– Low pressure baroreceptors
– Atrial stretch and release of ANP
• Respiratory and chemoreflex modulation of
baroreflex activity.

CS 2015
Topic Coverage
• In this session, we ONLY look at BP control on the
short-term (seconds).
• Long-term BP control via volume control will be done
in relation to kidney (see later “Volume regulation”).
• How vessels locally regulate resistance will be the
subject of the next lecture.
CS 2015
Overview of BP Control• In Block 1, mean arterial pressure was defined as
is mean arterial pressure (MAP), TPR total peripheral
resistance, CO cardiac output, SV stroke volume and HR
heart rate.
• controlled by 3 variables: TPR, SV and HR.
• Which system can control these parameters?– Autonomic nervous system:
• HR: sympathetic (+), parasympathetic (-; vagal) at heart
• SV: sympathetic (+), parasympathetic (-; but not muscle!) at heart;
sympathetic (+) at TPR (afterload); and others.
• TPR: sympathetic (+) ONLY at vessels (& other factors like volume, etc.).

CS 2015
Principles of Feedback Control
• Positive and negative feedback.
• Feed-forward: central command before exercise starts.
• Functional characteristic is feedback time: from few
100 ms to hours or even longer.

CS 2015
Overview of Reflex Control
Le
vick
, 5
th e
d.,
20
10
• Two feedback reflexes involved:– arterial baroreflex (AB – sympathetic and parasympathetic) and
– cardio-pulmonary reflexes (CP – at large sympathetic only).
• Modulated by respiration.
CS 2015
Arterial Baroreceptor Reflex (AB)
• Most afferent input is excitatory.
• Mostly negative feedback to brainstem, sympathetic
nervous system and heart: Depressor reflex.• If BP↑ → HR↓, SV↓, TPR↓ and vice versa if BP↓.
• Most important contributor to short-term homeostatic
control of BP (s - min).

CS 2015
Locations of AB Sensors
• Pressoreceptors in aortic arch and carotid sinus.
• Afferent nerves: IX (carotid sinus) & X (aortic arch).
Le
vick
, 5
th e
d.,
20
10
CS 2015
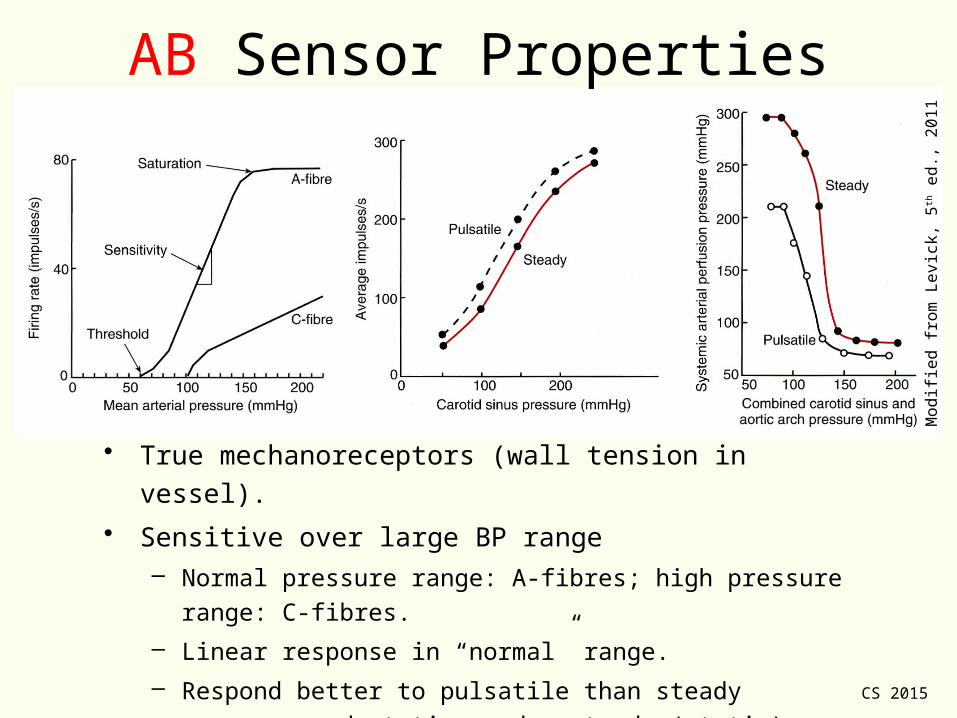
• True mechanoreceptors (wall tension in vessel).
• Sensitive over large BP range– Normal pressure range: A-fibres; high pressure range: C-fibres.
– Linear response in “normal” range.
– Respond better to pulsatile than steady pressure: adaptation
under steady (static) conditions, much less under pulsatile
(dynamic): poor at relaying absolute BP information.
AB Sensor Properties
Mo
difi
ed
fro
m L
evi
ck,
5th e
d.,
20
11
CS 2015
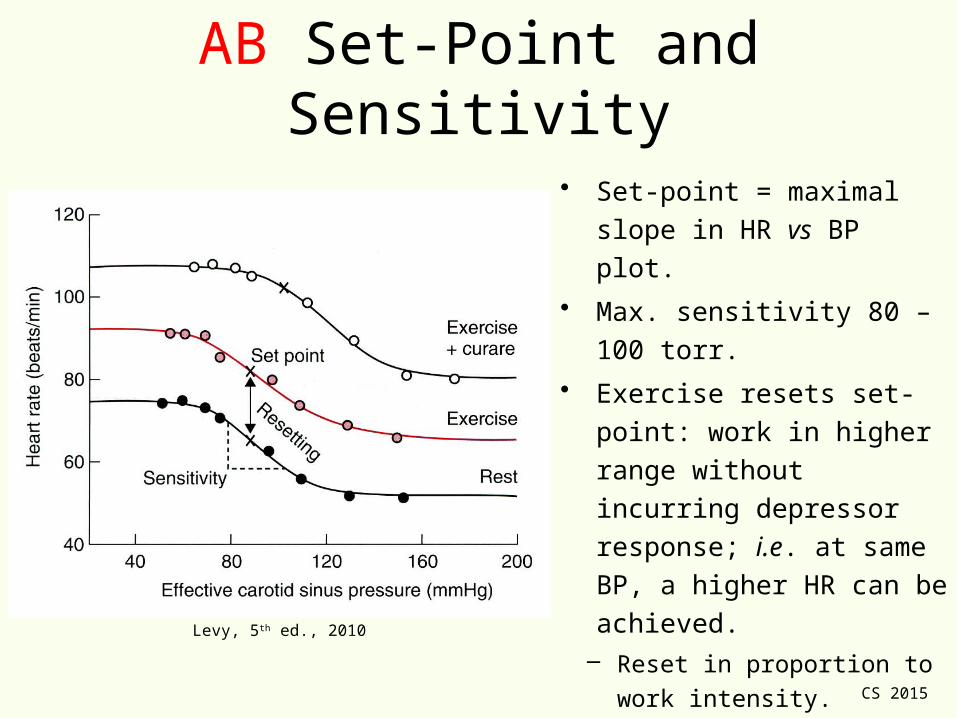
AB Set-Point and Sensitivity
• Set-point = maximal slope in
HR vs BP plot.
• Max. sensitivity 80 – 100 torr.
• Exercise resets set-point:
work in higher range without
incurring depressor
response; i.e. at same BP, a
higher HR can be achieved.– Reset in proportion to work
intensity.
– AB active but HR is permitted
to increase (muscle spindles).Levy, 5th ed., 2010
CS 2015
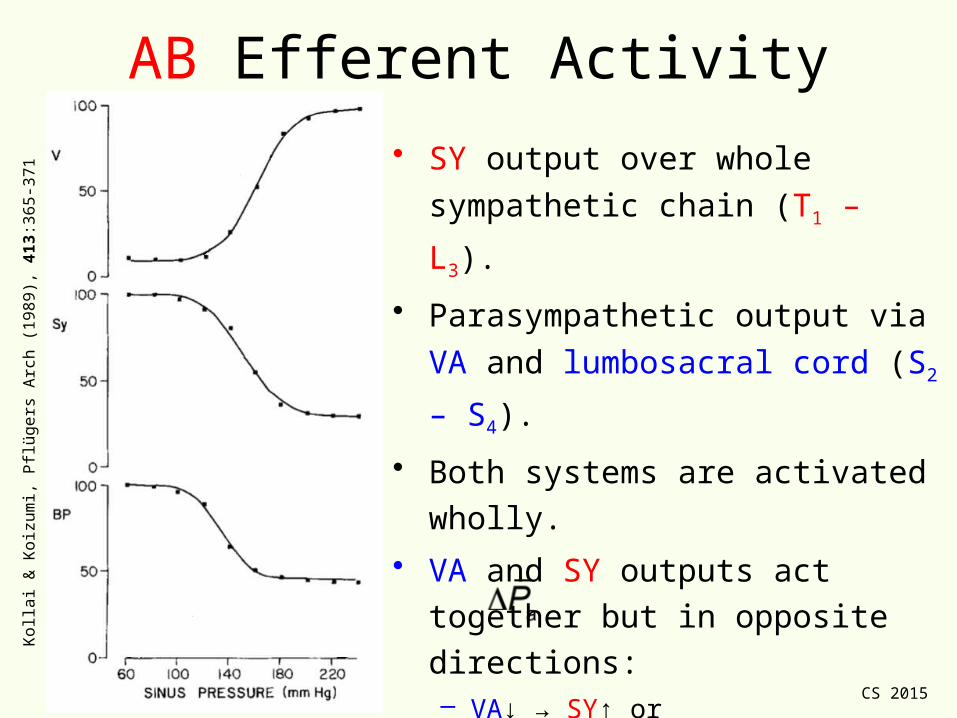
AB Efferent Activity
• SY output over whole sympathetic
chain (T1 – L3).
• Parasympathetic output via VA and
lumbosacral cord (S2 – S4).
• Both systems are activated wholly.
• VA and SY outputs act together but
in opposite directions:– VA↓ → SY↑ or
– VA↑ → SY↓.
• For > 180 torr, VA is maximised
and SY minimised.
Ko
llai &
Ko
izu
mi,
Pflü
ge
rs A
rch
(1
98
9),
413
:36
5-3
71
CS 2015
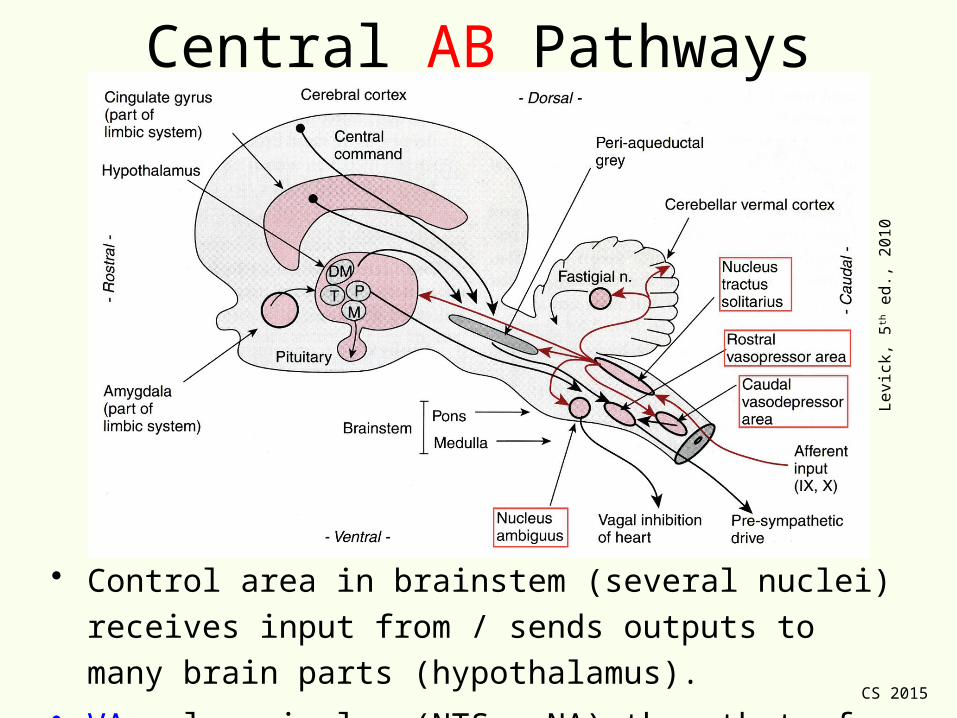
• Control area in brainstem (several nuclei) receives input
from / sends outputs to many brain parts (hypothalamus).
• VA relay simpler (NTS → NA) than that of SY pathway.
Le
vick
, 5
th e
d.,
20
10
Central AB Pathways
CS 2015
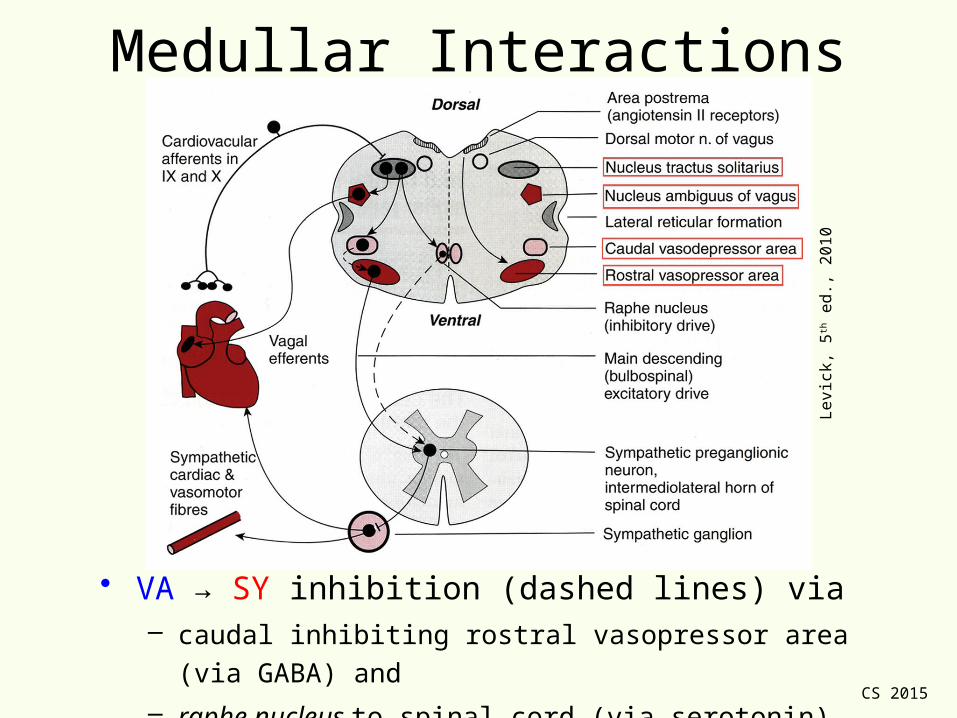
Medullar Interactions
• VA → SY inhibition (dashed lines) via – caudal inhibiting rostral vasopressor area (via GABA) and
– raphe nucleus to spinal cord (via serotonin).
Le
vick
, 5
th e
d.,
20
10
CS 2015
AB Function
• AB helps to stabilise BP control beat by beat (fast response
– VA!) within narrow range – if taken away, BP fluctuates
widely.
• Effect via coordinated VA↑ and SY↓ activity when BP↑: HR↓,
SV↓ and TPR↓ and vice versa.
• VA and SY work together but in opposite direction.
• During exercise, set-point shifted such that BP can rise
without HR inhibition.
• Modulated via inputs from respiratory & other centres.
• Activated in orthostasis, dehydration, blood loss (shock) etc.
CS 2015
Cardiopulmonary Reflexes (CP)
• Collection of various reflexes based on
sensor types.
• Low-pressure receptor reflexes.
• Most afferent input is inhibitory.
• Work predominantly on VR – mostly SY

CS 2015
Cardiopulmonary Reflexes (CP)
1. Cardiac de-afferentiation (transplant) reveals tonic
inhibition of HR and TPR only: Inhibitory cardiac afferents– Intracoronary injection of solute causes bradycardia, vasodilation and
hypotension:• Depressor reflex: HR↓, BP↓, TPR↓.
2. Important to know some specific reflexes as some can
cause only SY↑ activity:- Activation of veno-atrial stretch receptors causes tachycardia and
diuresis.• Sympathetic only reflex on SAN/volume regulation: HR↑ and central volume.

CS 2015
Locations & Types of CP Sensors
Le
vick
, 5
th e
d.,
20
10
• Heart sends off mostly small, unmyelinated (80%) fibres from– cardiac mechano-receptors (wall tension in ventricle);
– ventricular chemosensors (mediate pain via SY fibres): SY activity↑;
– coronary artery baroreceptors (perfusion pressure); and
• Some myelinated (20%): veno-atrial mechanoreceptors (type A/B).

CS 2015
Veno-Atrial Stretch Receptors• Measure atrial blood volume, i.e. central venous
pressure/volume in low pressure part of circulation
(central veins, atria); control venous return (VR).
• Upon activation (via infusion - ‘Bainbridge effect’)– SY activity↑ to SA node (tachycardia) without change in
VA activity; and
– diuresis and natriuresis: control of blood volume via renal
vasodilation (renal Na+ excretion↑), anti-diuretic hormone
release↓ (hypothalamus) and release↑ of atrial natriuretic
peptide (ANP) by atrial cells.
• Part of long-term volume regulation response (see
volume control in kidney section, later).
CS 2015
Modulation by Respiration &
Arterial Chemoreceptors
CS 2015
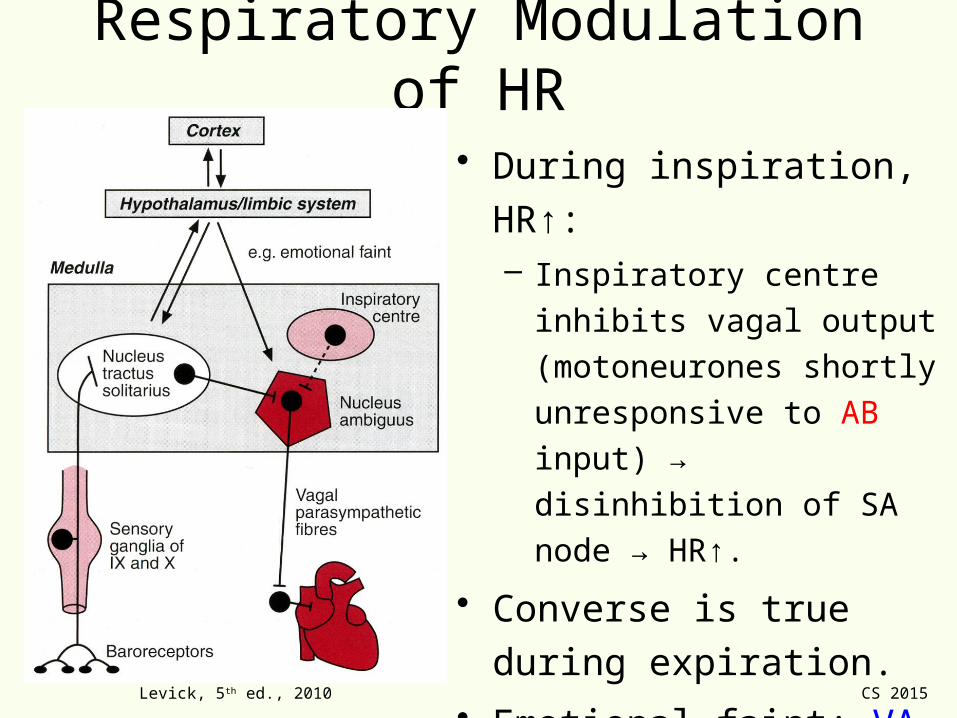
Respiratory Modulation of HR
• During inspiration, HR↑:– Inspiratory centre inhibits
vagal output (motoneurones
shortly unresponsive to AB
input) → disinhibition of SA
node → HR↑.
• Converse is true during
expiration.
• Emotional faint: VA output↑
→ HR↓↓.
Levick, 5th ed., 2010

CS 2015
Role of Arterial Chemoreceptors
• Carotid and aortic bodies (see respiration, later): sense
predominantly and , but also some pressure.
• Send inhibitory input to the brainstem.
• If < 80 torr (asphyxia, clinical shock, …):– Tachycardia due to resp. rate ↑ (lung stretch receptors inhibit
VA output) → SY↑.
– TPR↑ as renal, splanchnic and muscle vascular beds constrict;
– Splanchnic veins constrict → pooling↓ → SV↑ → CO↑.
– BP↑ as TPR↑ and CO↑.
CS 2015
Take-Home Messages• Under resting conditions, VA output on heart is more effective
than that of SY.
• Both, VA and SY nerves are tonically active and oppose each
other; VA effect is fast, SY effect appreciably slower.
• AB provides important short-term regulation of BP:– If BP↑, high pressure receptors in aortic arch and carotid sinus cause
HR↓, SV↓ and TPR↓ and vice versa.
• Cardiac de-afferentiation reveals tonic inhibitory effect on HR and
TPR – part of CP reflexes.
• Veno-atrial stretch receptors HR↑ and help control BP mainly via
circulating blood volume↓ → VR↓; i.e. renal vasodilation,
hypothalamic release↓ of ADH and atrial release↑ of ANP.
• When BP falls < 80 torr, peripheral chemoreceptors modulate BP
via vasoconstriction plus tachycardia.
CS 2015
MCQJack West, a 28 year-old bike rider was involved in a car accident on the
road to the snowfields. He suffered a broken femur and was immediately
transferred to Cooma Base Hospital. On admission, his HR was 112 bpm,
and his blood pressure 65 / 45 torr. Which of the following statements best
describes the state of the arterial baro- and cardiopulmonary reflex?
A. Arterial baroreceptor activity↓; sympathetic outflow↓;
parasympathetic outflow↑; low pressure mechanoreceptor activity↓.
B. Arterial baroreceptor activity↑; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↓.
C. Arterial baroreceptor activity↓; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↓.
D. Arterial baroreceptor activity↑; sympathetic outflow↓;
parasympathetic outflow↑; low pressure mechanoreceptor activity↑.
E. Arterial baroreceptor activity↑; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↑.
CS 2015
That’s it folks…

CS 2015
MCQJack West, a 28 year-old bike rider was involved in a car accident on the
road to the snowfields. He suffered a broken femur and was immediately
transferred to Cooma Base Hospital. On admission, his HR was 112 bpm,
and his blood pressure 65 / 45 torr. Which of the following statements best
describes the state of the arterial baro- and cardiopulmonary reflex?
A. Arterial baroreceptor activity↓; sympathetic outflow↓;
parasympathetic outflow↑; low pressure mechanoreceptor activity↓.
B. Arterial baroreceptor activity↑; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↓.
C. Arterial baroreceptor activity↓; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↓.
D. Arterial baroreceptor activity↑; sympathetic outflow↓;
parasympathetic outflow↑; low pressure mechanoreceptor activity↑.
E. Arterial baroreceptor activity↑; sympathetic outflow↑;
parasympathetic outflow↓; low pressure mechanoreceptor activity↑.