continuing medical education article implementation...
TRANSCRIPT

Continuing Medical Education Article
Implementation of a medical emergency team in a large pediatricteaching hospital prevents respiratory and cardiopulmonary arrestsoutside the intensive care unitRichard J. Brilli, MD, FCCM, FAAP; Rosemary Gibson, RN, MSN; Joseph W. Luria, MD, FAAP;T. Arthur Wheeler, MS, MBA; Julie Shaw, MSN, MBA, RN; Matt Linam, MD; John Kheir, MD;Patricia McLain, RN; Tammy Lingsch, RN, BSN; Amy Hall-Haering, RN, MSN; Mary McBride, MD
LEARNING OBJECTIVESOn completion of this article, the reader should be able to:1. Define the potential barriers to the implementation of a medical emergency team (MET) in pediatric teaching hospitals.2. Describe the criteria that are appropriate for the activation of MET in a pediatric teaching hospital.3. Identify the situations in which MET can and cannot be effective in preventing codes.All authors have disclosed that they have no financial relationships with or interests in any commercial companies pertainingto this educational activity.Lippincott CME Institute, Inc., has identified and resolved all faculty conflicts of interest regarding this educational activity.Visit the Pediatric Critical Care Medicine Web site (www.pccmjournal.org) for information on obtaining continuing medicaleducation credit.
Objective: We implemented a medical emergency team (MET)in our free-standing children’s hospital. The specific aim was toreduce the rate of codes (respiratory and cardiopulmonary ar-rests) outside the intensive care units by 50% for >6 monthsfollowing MET implementation.
Design: Retrospective chart review and program implementation.Setting: A children’s hospital.Patients: None.Interventions: The records of patients who required cardiore-
spiratory resuscitation outside the critical care areas were re-viewed before MET implementation to determine activation crite-ria for the MET. Codes were prospectively defined as respiratoryarrests or cardiopulmonary arrests. MET-preventable codes wereprospectively defined. The incidence of codes before and afterMET implementation was recorded.
Measurements and Main Results: Twenty-five codes occurredduring the pre-MET baseline compared with six following MET im-plementation. The code rate (respiratory arrests � cardiopulmonaryarrests) post-MET was 0.11 per 1,000 patient days compared with
baseline of 0.27 (risk ratio, 0.42; 95% confidence interval, 0–0.89;p � .03). The code rate per 1,000 admissions decreased from 1.54(baseline) to 0.62 (post-MET) (risk ratio, 0.41; 95% confidence inter-val, 0–0.86; p � .02). For MET-preventable codes, the code ratepost-MET was 0.04 per 1,000 patient days compared with a baselineof 0.14 (risk ratio, 0.27; 95% confidence interval, 0–0.94; p � .04).There was no difference in the incidence of cardiopulmonary arrestsbefore and after MET. For codes outside the intensive care unit, thepre-MET mortality rate was 0.12 per 1,000 days compared with 0.06post-MET (risk ratio, 0.48; 95% confidence interval, 0–1.4, p � .13).The overall mortality rate for outside the intensive care unit codeswas 42% (15 of 36 patients).
Conclusions: Implementation of a MET is associated with areduction in the risk of respiratory and cardiopulmonary arrestoutside of critical care areas in a large tertiary children’s hospital.(Pediatr Crit Care Med 2007; 8:236–246)
KEY WORDS: cardiopulmonary arrest; respiratory arrest; pediat-rics; children; rapid response system; medical emergency team
*See also p. 297.Associate Chief of Staff, Medical Director, Pediatric
Intensive Care Unit, Professor, Pediatrics, Division ofCritical Care Medicine, Cincinnati College of Medicine,Cincinnati, OH (RJB); Clinical Nurse Specialist (RG),Associate Professor of Clinical Pediatrics (JWL), SeniorDecision Support Analyst (TAW), Senior Clinical Direc-tor (JS), Pediatric Infectious Disease Fellow (ML), Reg-istered Nurse II (PM), Care Manager, Heart Center (TL),
Clinical Director Manager of Patient Services (AH),Cincinnati Childrens’ Hospital Medical Center, Cincin-nati, OH; Clinical Fellow in Critical Care Medicine,Department of Anesthesia, Perioperative and PainMedicine, Childrens’ Hospital of Boston, Boston, MA(JK); Pediatric Cardiology Fellow, Washington Univer-sity, St. Louis, MO (MM).
The authors have not disclosed any potential con-flicts of interest.
For information regarding this article, E-mail:[email protected]
Copyright © 2007 by the Society of Critical CareMedicine and the World Federation of Pediatric Inten-sive and Critical Care Societies
DOI: 10.1097/01.PCC.0000262947.72442.EA
236 Pediatr Crit Care Med 2007 Vol. 8, No. 3

I n response to the United StatesCongress’ mandate that U.S. hos-pitals develop a culture of safety,the Agency for Healthcare Re-
search and Quality developed national pa-tient safety indicators (1). Failure to res-cue, defined as a death resulting from acomplication rather than the primary di-agnosis, is one of these indicators (2).In-hospital cardiopulmonary arrests thatoccur outside the intensive care unit(ICU) represent failure-to-rescue events.The Institute for Healthcare Improve-ment’s Saving 100,000 Lives Campaignhas advocated the deployment of in-hospital medical emergency teams(METs) as a means to rescue patients andreduce hospital mortality rates (3). Re-cent reports in adult hospitals haveshown that METs decrease the number ofcardiopulmonary arrests that occur out-side the ICU and can decrease postoper-ative mortality, mean duration of hospitallength of stay, and overall hospital mor-tality (4–9).
Recently, more information has be-come available about in-hospital cardio-pulmonary arrests in children. The inci-dence of in-hospital cardiopulmonaryarrests in pediatric patients (includingthose occurring in the ICU) varies be-tween 0.7% and 3% of all hospital admis-sions (10, 11). The survival-to-dischargerate for such patients is poor and variesbetween 15% and 27% (11, 12). Cardio-pulmonary arrests that occur outside thecritical care units in pediatric hospitalsare uncommon but also have a poor sur-vival rate. Suominen et al. (10) reported12 cardiopulmonary arrests outside theICU from among 32,400 hospital admis-sions (0.03%). Outside the ICU, cardio-pulmonary arrests accounted for 10.1%of in-hospital cardiopulmonary arrests,and the discharge survival rate for thesepatients was 33%. Others report that8.5% to 14% of all in-hospital cardiopul-monary arrests in children occur outsidethe ICU, and the mortality rate for thesepatients is 50% to 67% (10 –13). Thishigh mortality rate in children makesprevention of in-hospital, out-of-ICUcardiopulmonary arrest particularlyimportant.
Currently there are limited data avail-able in pediatrics regarding METs andtheir impact on in-hospital, out-of-ICUcardiopulmonary arrests. In the only pe-diatric report to date, Tibballs et al. (14)described a trend toward reduction inrisk for out-of-ICU cardiopulmonary ar-rest after MET implementation, al-
though the risk reduction did not reachstatistical significance. In response tothe Institute for Healthcare Improve-ment imperative and the desire to elim-inate failure-to-rescue events, we imple-mented a MET. The specific aim of theinitiative, based on published adult hos-pital experience, was to reduce the rate ofcodes (respiratory arrest and cardiopul-monary arrest) outside the ICUs by 50%for �6 months following MET implemen-tation. This report describes the imple-mentation strategies and results of thisperformance improvement initiative.
METHODS
This performance improvement project re-ceived expedited review and approval by thehospital Institutional Review Board. Informedconsent was waived.
Pre-Arrest Variable Analysis. Medicalrecords of the 44 non-ICU patients hospital-ized between 2001 and 2004 who suffered ap-nea (respiratory arrest) or cardiopulmonaryarrest were retrospectively examined. The crit-ical care unit areas of the hospital were thepediatric ICU (PICU), cardiac ICU, neonatalICU, operating room, emergency department,and cardiac catheterization laboratory. Thisperformance improvement initiative was in-tended to reduce or eliminate all out-of-ICUrespiratory or cardiopulmonary arrests. Tosuccinctly name these events, we used theterm “code,” which was defined as a respira-tory arrest alone (apnea) or a cardiopulmonaryarrest (apnea � asystole or apnea � nonper-fusing heart rhythm) wherein the interven-tions provided by the hospital code alert teamincluded airway resuscitation (bag-valve maskventilation and/or tracheal intubation) and/orcardiac resuscitation (chest compressionsand/or cardioversion/defibrillation). Demo-graphic and clinical data from the 4 hrs beforethe code were recorded. This data consisted of70 precode variables including vital signs; se-lect lab values; documented physical examfindings by the bedside nurse, respiratorytherapist, or physician; and clinical narrativedescriptions of the patient.
After initial chart review, the ten most fre-quent variables that exceeded critical thresh-olds were subjected to analysis to determinewhich variables or combination of variableswere most likely to predict a code. The resultof this analysis was candidate sets of METtrigger criteria, consisting of “either/or” and“and” combinations. Each set of trigger crite-ria was ranked according to the percentage ofthe 44 cases with which it was associated. A90% confidence interval was calculated to in-dicate the percentage of future codes that thetrigger set could be associated with. The finalset of activation (trigger) criteria was chosenbased on the clinical judgment of experts, bal-ancing each trigger set’s calculated rank
against the ease of measure and detection,anticipated false alarm rate, and practical con-siderations regarding their effective use byhospital staff.
Development and Implementation of theMET. A multidisciplinary group was convenedthat consisted of bedside nurses, respiratorytherapists, physicians (residents, fellows, fac-ulty), and nursing managers from the generalcare floors and PICU. The group was chargedwith a) identifying clinical triggers to activatethe MET; b) identifying MET membership; c)implementing the MET throughout the hospi-tal; and d) establishing outcome measures,including team performance. The MET wasintroduced on pilot units over a 4-month timeperiod using small tests of change, with the“model for improvement” serving as the orga-nizing framework for the group (15).
The MET was defined as experienced clini-cians dispatched to evaluate and triage pa-tients who were perceived as having a declin-ing clinical status. A prospective decision tocreate a two-tiered hospital system response toclinical patient deterioration was made. Thefirst-tier response would continue as the codealert team, which responds immediately to allin-hospital respiratory or cardiopulmonary ar-rests and provides immediate resuscitation,stabilization, and triage to the appropriatecare unit. A new second-tier response, theMET, would be an added in-hospital responseto assess clinically deteriorating patients. Thisteam would arrive within 15 mins after acti-vation. MET functions included assessment,stabilization if necessary, and triage of generalcare floor patients to the most appropriateunit in the hospital. MET members included aPICU fellow, PICU nurse, senior pediatric res-ident, respiratory therapist, and the managerof patient services (in-hospital nursing super-visor in charge of general floor patient place-ment). The MET would be joined at the bed-side by the general care unit staff includingbut not limited to the nurse and physicianscaring for the patient and the family. The METwas activated via pagers after calling a singlephone number. Education about the new teamtook place over a 4-month implementationand education period and included presenta-tions at nursing shift changes, nursing lead-ership and shared governance meetings, phy-sician divisional and faculty meetings, andresident conferences. Education was supple-mented with posters, phone stickers, and re-source handouts for all involved units. Theposters and handouts included the team pur-pose, goals, function, and team membership;information about when to call (triggers);number to call; and instructions about how togive feedback. A simple survey tool, developedto assess team performance and staff satisfac-tion, was distributed to the 215 staff involvedin the 27 MET consults (Appendix 1). Thesurveys were available on the hospital intra-net. All MET activations were official medicalconsults, and the completed consult formserved as both medical record documentation
237Pediatr Crit Care Med 2007 Vol. 8, No. 3

of MET activity and data collection tool (Ap-pendix 2). Communication from the generalcare unit, emergency department, and operat-ing room physician staff directly to the PICUphysician staff to discuss patients requiringurgent ICU admission was not prohibited oreliminated by the MET system. These commu-nications were not categorized as MET con-sults.
Post-MET Outcome Data Analysis. Coderates were analyzed during three differenttime periods. Rates were defined using twodifferent denominators (1,000 hospital non-ICU patient days and 1,000 non-ICU hospitaladmissions). The pre-MET period (baseline)was 15 months, from October 2003 throughJanuary 2005, and included codes before anyplanning or development of the MET (Fig. 1).The implementation and education period(implementation) was from February throughMay 2005 and included codes that occurredduring the MET-related tests of change. Thepost-MET period was from June 2005 throughJanuary 2006 and reflects data after full hos-pital implementation of the MET. The imple-mentation plus post-MET periods total 12months.
At study outset and before retrospectivechart review or data analysis, the MET plan-ning group recognized that some in-hospitalcodes might not be prevented by MET imple-
mentation. Clinical conditions that occurredsuddenly or without clinical warning or eventsthat happened in an environment not accessi-ble to a MET, such as during the administra-tion of general anesthesia outside the operat-ing room, were clinical events that theplanning group prospectively identified as“codes not preventable by MET.” These in-cluded a) pulmonary embolus; b) new sei-zures; c) sudden plugged or occluded trache-otomy tube; d) code by an adult visitor; e) codeoccurring during general anesthesia adminis-tered outside the operating room (i.e., radiol-ogy suite); f) code resulting from an acutedrug overdose; and g) code in our ambulatoryclinics. Furthermore, it was recognized thatsome codes might not be prevented by a METbut might be prevented by other hospital-widesystem interventions, as described by Braith-waite et al (16). All code event records werereviewed. Each event was examined using theclinical conditions noted previously or, for thepresence of unrecognized MET triggers, othervital sign changes that might have alerted theclinician to the code event that occurred. Eachcode event was categorized as MET prevent-able, MET not preventable, or MET not pre-ventable but preventable by other means.
Final patient disposition (death or hospitaldischarge) was recorded for all outside the ICUcodes for each study time period. For all MET
consults, triage disposition (remain on gen-eral care unit or transfer to ICU) and finaldisposition (death or discharge) were re-corded. Vital signs recorded on the MET con-sult forms were used to analyze the physio-logic status of the patient at the time of METconsult. Mortality rates were adjusted to 1,000non-ICU patient days and 1,000 non-ICU ad-missions.
Statistical Analysis. Comparison of coderates and mortality for the baseline vs. theMET implementation and post-MET time pe-riods was done with an analysis of relative riskusing SAS 9.1.3 (Proc FREQ, TABLES State-ment, RELRISK Option). Statistical p valuesand associated 95% confidence intervals (CIs)are reported as both one-sided and two-sided.We believe that reporting one-sided tests isjustified by the demonstrated uniform successin cardiac arrest rate reduction by METs in theadult medical literature. That justification isaugmented by clinical consensus that imple-mentation of a MET could not realisticallymake code rates worse. Because traditionalstatistical methods suggest the use of two-tailed analysis of outcomes associated with aclinical intervention, we present our resultsusing both methods. Statistical significancewas defined as p � .05.
RESULTS
Table 1 shows the analysis of prearrestdata from codes before MET implemen-tation. After examination of 1,024 combi-nations of prearrest variables from priorcodes, no set of variables was sensitive orspecific enough for use as MET activationtriggers. The planning group combinedexpert consensus and the retrospectivechart analysis to determine the MET ac-tivation criteria (Table 2).
Outside the ICU, code rates are de-picted in Figure 1. The post-MET coderate was significantly lower comparedwith baseline (one-tailed analysis). Usingtwo-tailed analysis to compare pre- andpost-MET code rates per 1,000 patientdays revealed a risk ratio of 0.42 (95% CI0.173–1.03; p � .057). The post-METcode rate per 1,000 non-ICU admissionswas 0.62 compared with baseline of 1.54:Risk ratio (two-tailed) was 0.41 (95% CI0.167–0.99; p � .047).
Table 3 describes the clinical groupingfor all 19 code events that were not pre-ventable by MET. One code event, occur-ring during the baseline period (an acutedrug overdose), was not preventable byMET but was deemed preventable byother hospital system interventions.
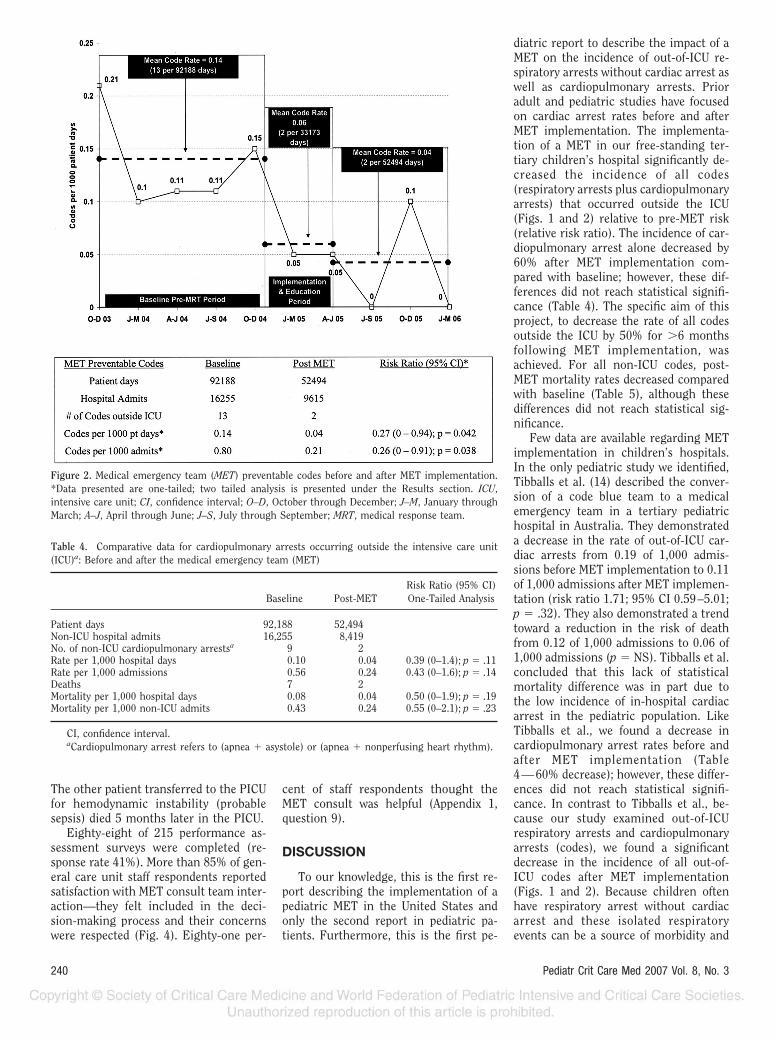
MET-preventable code rates are de-picted in Figure 2. For MET-preventablecodes, the post-MET rate was signifi-cantly lower compared with baseline
Figure 1. All codes outside the intensive care unit (ICU) before and after medical emergency team(MET) implementation. *Data presented are one-tailed; two tailed analysis is presented under theResults section. CI, confidence interval; O-D, October through December; J–M, January throughMarch; A–J, April through June; J–S, July through September; MRT, medical response team.
238 Pediatr Crit Care Med 2007 Vol. 8, No. 3

(one-tailed analysis). Using two-tailedanalysis to compare pre- and post-METpreventable code rates per 1,000 patientdays revealed a risk ratio of 0.27 (95% CI0.061–1.20; p � .085). Post-MET prevent-able code rates per 1,000 non-ICU admis-sions were 0.21 compared with baselineof 0.8: Risk ratio (two-tailed) was 0.26(95% CI 0.059–1.15; p � .076).
Cardiopulmonary arrest rates, whichexclude patients with only a respiratoryarrest (per 1,000 patient days and per1,000 admissions), were reduced by�60% following MET implementationcompared with baseline; however, theserates were not statistically different using
one-tailed analysis (Table 4). Similarly,the rates were not different using two-tailed analysis (data not shown).
During the baseline period, there were25 codes (respiratory arrest plus cardio-pulmonary arrest): nine cardiopulmonaryarrests (seven died) and 16 respiratoryarrests (four died). Post-MET there weresix codes: two cardiopulmonary arrests(both died) and four respiratory arrests(one died). During the implementationperiod there were five codes: four cardio-pulmonary arrests (one died) and one re-spiratory arrest (none died). The mortal-ity rate for all codes that occurred outsidethe ICU was 42% (15 of 36 patients). Themortality rates per 1,000 patient days andper 1,000 non-ICU admissions were notdifferent between the baseline period andpost-MET period (Table 5).
During the entire study period, therewere 15 cardiopulmonary arrests outsidethe ICU. The mortality rate was 67% (10 of15 patients). For patients with respiratoryarrest alone, the mortality rate was 24%(5 of 21 patients). Table 4 outlines mortalitydata for only cardiopulmonary arrest pa-tients—mortality rates were not differentbefore and after MET implementation.
Code rates in the ICUs and mean hos-pital length of stay (LOS) did not changeduring the periods of this study. Duringthe pre-MET period, the ICU code ratewas 5.1 codes per 1,000 ICU days (61codes per 12,098 days) compared with 6.6codes per 1,000 ICU days (63 codes per9,526 days) during the post-MET period(p � .13). Mean hospital LOS was 5.8days during the baseline period and 5.9days during the post-MET period (p �not significant).
The MET was activated 27 times dur-ing the 12 months of the study. The num-ber of MET consults was nearly equalacross all general care units. The mostfrequent trigger to activate the MET wasstaff concern about the patient (Fig. 3).The most frequent physiologic distur-bance cited for activating the MET wasincreased work of breathing. Vital signsfor all patients at the time of MET consultwere recorded on the MET consult form.For patients �10 yrs of age, the medianheart rate was 123 beats/min (25%, 109beats/min; 75%, 132 beats/min), medianrespiratory rate was 32 breaths/min(25%, 18 breaths/min, 75%, 56 breaths/min), and median systolic blood pressurewas 111 torr (25%, 106 torr; 75%, 120torr). For patients �2 and �10 yrs of age,the median heart rate was 150 beats/min(25%, 130 beats/min; 75%, 180 beats/min), median respiratory rate was 29breaths/min (25%, 25 breaths/min; 75%,35 breaths/min), and median systolicblood pressure was 88 torr (25%, 83 torr;75%, 111 torr). For patients �2 yrs ofage, the median heart rate was 156 beats/min (25%, 140 beats/min; 75%, 167beats/min), median respiratory rate was45 breaths/min (25%, 36 breaths/min;75%, 52 breaths/min), and median sys-tolic blood pressure was 97 torr (25%, 88torr; 75%, 107 torr). The hospital LOS forpatients before MET consult ranged from4 to 26 days, and all patients had beenappropriately triaged to the general careunit at the time of original hospital ad-mission. After MET consult, 13 patientsremained on the general care floor and 13were transferred to the ICU. One patientdeveloped increased respiratory depres-sion several hours after the MET consultdecision was to keep the child on thegeneral care unit. The child was trans-ferred to the PICU without further inci-dent. All but two patients for whom aMET consult was obtained were dis-charged home. One patient with urosep-sis was transferred to the PICU after METconsult and died 3 wks later in the PICU.
Table 1. Identifying potential medical emergency team trigger variables from retrospective chartreview: Six representative “either/or” criterion measures
90% ConfidenceInterval, %a
Clinical VariableMinimum Maximum
57.2 81.6 Increase respiratory rate and work of breathing or low oxygensaturations
54.8 79.6 Low oxygen saturations or neurological agitation52.5 77.7 Increased work of breathing or decreased consciousness47.9 73.7 Increased work of breathing or neurological agitation47.9 73.7 Low oxygen saturations or increased respiratory rate47.9 73.7 Increased oxygen requirement or decreased consciousness
aThese results indicate that a two-measure set chosen from this list identifies code situations withthe indicated success rate, when the occurrence of either one of the measures in the set is used as thecriterion for identifying a potential code.
Table 2. Medical emergency team activation cri-teria
● Increased work of breathing and any of thefollowing
y Worsening retractionsy Saturations �90% despite supplemental
oxygeny Cyanosis
● Agitation or decreased level of consciousness● Staff concern or worry about the patient● Parental concern about the child
Table 3. Number of code events not preventable by medical emergency team (MET; n � 19)
Baseline I & E Period Post-MET
Seizures 7�(A) 2�(A) 2�(A)Pulmonary embolus 0 1�(A) 0Plugged tracheotomy 2�(A) 0 0Code by adult visitor 0 0 0Code during general anesthesia outside
OR (i.e., radiology)2�(A) 0 2�(A)
Code in ambulatory clinic 0 0 0Drug overdose 1�(B) 0 0
I & E, implementation and education; A, MET not preventable; OR, operating room; B, MET notpreventable but preventable by other means.
239Pediatr Crit Care Med 2007 Vol. 8, No. 3
The other patient transferred to the PICUfor hemodynamic instability (probablesepsis) died 5 months later in the PICU.
Eighty-eight of 215 performance as-sessment surveys were completed (re-sponse rate 41%). More than 85% of gen-eral care unit staff respondents reportedsatisfaction with MET consult team inter-action—they felt included in the deci-sion-making process and their concernswere respected (Fig. 4). Eighty-one per-
cent of staff respondents thought theMET consult was helpful (Appendix 1,question 9).
DISCUSSION
To our knowledge, this is the first re-port describing the implementation of apediatric MET in the United States andonly the second report in pediatric pa-tients. Furthermore, this is the first pe-
diatric report to describe the impact of aMET on the incidence of out-of-ICU re-spiratory arrests without cardiac arrest aswell as cardiopulmonary arrests. Prioradult and pediatric studies have focusedon cardiac arrest rates before and afterMET implementation. The implementa-tion of a MET in our free-standing ter-tiary children’s hospital significantly de-creased the incidence of all codes(respiratory arrests plus cardiopulmonaryarrests) that occurred outside the ICU(Figs. 1 and 2) relative to pre-MET risk(relative risk ratio). The incidence of car-diopulmonary arrest alone decreased by60% after MET implementation com-pared with baseline; however, these dif-ferences did not reach statistical signifi-cance (Table 4). The specific aim of thisproject, to decrease the rate of all codesoutside the ICU by 50% for �6 monthsfollowing MET implementation, wasachieved. For all non-ICU codes, post-MET mortality rates decreased comparedwith baseline (Table 5), although thesedifferences did not reach statistical sig-nificance.
Few data are available regarding METimplementation in children’s hospitals.In the only pediatric study we identified,Tibballs et al. (14) described the conver-sion of a code blue team to a medicalemergency team in a tertiary pediatrichospital in Australia. They demonstrateda decrease in the rate of out-of-ICU car-diac arrests from 0.19 of 1,000 admis-sions before MET implementation to 0.11of 1,000 admissions after MET implemen-tation (risk ratio 1.71; 95% CI 0.59–5.01;p � .32). They also demonstrated a trendtoward a reduction in the risk of deathfrom 0.12 of 1,000 admissions to 0.06 of1,000 admissions (p � NS). Tibballs et al.concluded that this lack of statisticalmortality difference was in part due tothe low incidence of in-hospital cardiacarrest in the pediatric population. LikeTibballs et al., we found a decrease incardiopulmonary arrest rates before andafter MET implementation (Table4—60% decrease); however, these differ-ences did not reach statistical signifi-cance. In contrast to Tibballs et al., be-cause our study examined out-of-ICUrespiratory arrests and cardiopulmonaryarrests (codes), we found a significantdecrease in the incidence of all out-of-ICU codes after MET implementation(Figs. 1 and 2). Because children oftenhave respiratory arrest without cardiacarrest and these isolated respiratoryevents can be a source of morbidity and
Figure 2. Medical emergency team (MET) preventable codes before and after MET implementation.*Data presented are one-tailed; two tailed analysis is presented under the Results section. ICU,intensive care unit; CI, confidence interval; O–D, October through December; J–M, January throughMarch; A–J, April through June; J–S, July through September; MRT, medical response team.
Table 4. Comparative data for cardiopulmonary arrests occurring outside the intensive care unit(ICU)a: Before and after the medical emergency team (MET)
Baseline Post-METRisk Ratio (95% CI)One-Tailed Analysis
Patient days 92,188 52,494Non-ICU hospital admits 16,255 8,419No. of non-ICU cardiopulmonary arrestsa 9 2Rate per 1,000 hospital days 0.10 0.04 0.39 (0–1.4); p � .11Rate per 1,000 admissions 0.56 0.24 0.43 (0–1.6); p � .14Deaths 7 2Mortality per 1,000 hospital days 0.08 0.04 0.50 (0–1.9); p � .19Mortality per 1,000 non-ICU admits 0.43 0.24 0.55 (0–2.1); p � .23
CI, confidence interval.aCardiopulmonary arrest refers to (apnea � asystole) or (apnea � nonperfusing heart rhythm).
240 Pediatr Crit Care Med 2007 Vol. 8, No. 3

mortality, our study sought to look athow a MET would affect both respiratoryand cardiopulmonary arrests that occuroutside the ICU. Examining all codes, in-cluding respiratory arrests without car-diac arrest, is important in children be-cause in our study and in those of others,these patients can have significant mor-tality—24% (5 of 21) (13). To examinethe possibility that our out-of-ICU coderates decreased because either hospitalLOS increased (larger denominator) orICU codes increased (patients arrested inthe ICU instead of on the general careunit), we compared these variables dur-ing baseline and post-MET periods andfound no differences. Like Tibballs et al.,our study showed that mortality rates per1,000 non-ICU admissions for patientswho had only cardiopulmonary arrestoutside the ICU were lower—pre-MET(0.43) compared with post-MET (0.24);however, these values were not statisti-cally different (risk ratio 0.55; p � .23).Our improvement initiative was not pow-ered to determine a mortality difference;however, one reason for the lack of sta-tistical mortality difference may be that21 of the 36 code patients had only arespiratory arrest. Patients with respira-tory arrest but without cardiac arrest aremore likely to survive to hospital dis-charge, thus potentially diminishing ourability to discern a difference in mortalityrates before and after MET implementa-tion (13, 17). In our patients, the mortal-ity rate for patients with respiratory ar-rest alone was 24% (5 of 21) comparedwith 67% (10 of 15) for cardiopulmonaryarrest patients. We speculate that giventhe aforementioned mortality rates, eventhe elimination of one code outside theICU has potential impact to save lives,although that may not be evident whenexamining aggregate hospital mortalityrates.
Our findings and those of Tibballs etal. (14), which suggest a reduction incardiopulmonary arrest rates alone, aresimilar to previous reports in adult hos-pitals. Goldhill et al. (18) reported a 26%reduction in out-of-ICU cardiac arrestsover a 6-month period after the imple-mentation of a “patient at-risk team.”Bellomo et al. (4) reported a 66% relativerisk reduction in cardiac arrests outsidethe ICU among medical patients, a 63%relative risk reduction in cardiac arrestsamong surgical patients, and an overallrelative risk reduction in cardiac arrestsof 65% following implementation of aMET. These adult reports are consistent
Figure 3. Reasons for medical emergency team activation. An individual patient could havemultiple reasons. BP, blood pressure; RR, respiratory rate; MD, physician; RT, respiratorytherapist; RN, nurse; LOC, level of consciousness; Sats, saturations; WOB, work of breathing;MRT, medical response team.
Table 5. Comparative mortality data for non-intensive care unit (ICU) codesa: Before and after themedical emergency team (MET)
Baseline Post-MET Risk Ratio (95% CI)
Patient days 92,188 52,494Non-ICU hospital admits 16,255 8,419No. of non-ICU codesa 25 6Deaths 11 3Mortality per 1,000 hospital patient days 0.12 0.06 0.48 (0–1.4); p � .13Mortality per 1,000 non-ICU admits 0.67 0.36 0.53 (0–1.5); p � .16
CI, confidence interval.aCode means respiratory arrest alone or cardiopulmonary arrest.
Figure 4. Inpatient care unit staff after medical emergency team survey results. MRT, medical responseteam.
241Pediatr Crit Care Med 2007 Vol. 8, No. 3

with the 60% reduction in cardiac arreststhat we observed after MET implementa-tion. More recently, DeVita et al. (8), in aretrospective analysis of 3,269 MET acti-vations over 6.8 yrs, reported a 17% re-duction in out-of-ICU cardiac arrest afterimplementation of a MET, but the pro-portion of fatal cardiac arrests was notdifferent when pre- and post-MET timeperiods were compared. In contrast, in-vestigators from the Medical EmergencyResponse Improvement Team (MERIT)study in Australia randomized 23 hospi-tals to either introduce the MET systemor continue functioning in their usualmanner (19). These investigators did notfind a difference in out-of-ICU cardiacarrest rates or hospital mortality betweencontrol hospitals and MET hospitals.Most recently, Winters et al. (20) summa-rized MET adult outcome data and ques-tioned the rush to implement METs.They suggested that more study is neededand that other interventions to preventout-of-ICU cardiac arrests might be justas effective as the MET.
Reliable and consistent use of a MET,which includes prompt recognition whenMET trigger criteria occur, may not besufficient to completely eliminate codes(respiratory arrests or cardiopulmonaryarrests) outside the ICU. Recognizablechanges in clinical status of patients, be-fore code events, are important determi-nants of the efficacy of a MET. Thesesigns and symptoms of clinical deteriora-tion must occur slowly enough (minutesto hours) for clinical staff to recognizethem and call for advice or help. Patientswho suffer abrupt deterioration, as a re-sult of sudden events that are not pre-ceded by clinically recognizable signs orsymptoms, are not likely to benefit from aMET. Examples of such events includebut are not limited to new-onset seizuresand sudden dysrhythmias. Similarly, codeevents that occur in areas of the hospitalnot easily accessible to MET (e.g., generalanesthesia delivered outside the operat-ing room such as in radiology) will likelynot be prevented by a MET. Among all 36codes, 19 were deemed not preventableby MET (Table 3). Four such events oc-curred during the post-MET period. Onecode occurred as a result of an acute drugoverdose, and although not preventableby MET, this event likely was potentiallypreventable by other hospital safety sys-tems. In our study (Fig. 2), two MET-preventable codes occurred during thepost-MET period. Retrospective review ofthese cases indicated that both patients
had vital sign changes before cardiopul-monary arrest, which if recognized byclinical staff should have activated theMET. These cases represent failures ofthe MET system and opportunities to ex-amine more effective MET implementa-tion strategies. Tibballs et al. (14) de-scribed four cases of sudden cardiacarrest wherein the patients did not meetMET trigger criteria because the clinicalevents were sudden. These cases weresudden dysrhythmia, vagal stimulationduring nasogastric tube placement, andintracerebral hemorrhage. These exam-ples suggest that although a MET canreduce codes outside the ICU, challengesremain to refine pediatric-specific METactivation criteria and, more important,to implement hospital systems to helpclinical staff reliably recognize triggers ina timely fashion. Education of staff aboutMET trigger criteria is not sufficient.Braithwaite et al. (16) found that METconsults could be used as markers formedical errors. Those authors found that31% of MET consults were generated be-cause a medical error had occurred and,more important, that other hospital sys-tems, other than a MET team, requiredrevision to prevent future events. Elec-tronic alarm systems generating auto-matic warning alerts could offer superiorresults compared with the system wehave described, because such a systembypasses the need for staff to rememberthe trigger criteria; however, the addi-tional cost in personnel to monitor thewarning system and to keep the falsealarm rate to a minimum could be pro-hibitive.
The clinical criteria that best suggestwhen to activate a MET have been con-troversial and include changes in respi-ratory rate, changes in blood pressure,deteriorating level of consciousness,and clinician worry or concern (21–23).Foraida et al. (24) suggested that a fo-cused organized response (MET activa-tion) to predefined abnormal physiologiccriteria can be developed and might im-prove outcome. Adult-oriented MET acti-vation criteria usually include five toeight physiologic variables (7, 25). Incontrast, MET activation triggers in pedi-atrics offer unique challenges because vi-tal sign-related triggers must be adjustedto age-specific norms, and therefore thenumber of variables for staff to rememberincreases substantially compared withthe adult population. The activation cri-teria provided by Tibballs et al. (14) in-cluded five respiratory rate criteria, ten
heart rate criteria, five blood pressurecriteria, plus any change in neurologicstatus. Similarly, the pediatric earlywarning score (PEWS), which combinesvital sign variables, perfusion, and neuro-logic assessments, has �20 signs that arecombined into an aggregate warningscore (26). Duncan et al. (27) suggestedthat using a PEWS score of 5 could iden-tify �75% of code blue calls with �1 hrwarning. We chose a MET trigger systemwith five clinical and two intuitive crite-ria (Table 2). We chose these in part be-cause our retrospective code analysis didnot reveal discriminatory vital sign orlaboratory variables that could consis-tently identify children at risk. In addi-tion, we tried to keep things simple. AfterMET rollout, we reviewed all MET con-sult forms and found a large range of vitalsigns abnormalities for each age group,but specific cutoffs that might increasethe sensitivity or specificity of our cur-rent MET triggers were lacking. The mostcommon reason for MET activation inpediatric hospitals was concern by anurse or respiratory therapist (Fig. 3)(14). This suggests that a clinician’s in-tuitive assessment of the patient may beof greater importance than any specificvital sign threshold. Despite this, we be-lieve that more work is needed to identifya simple and effective early warning trig-ger system for children at risk for respi-ratory or cardiopulmonary arrest outsidethe ICU.
There are many barriers to MET im-plementation (28). Like DeVita et al. (8),we found that a key barrier to successfulMET implementation involved changinginstitutional cultural perceptions abouttraditional professional role norms. It be-came apparent during MET implementa-tion that for physicians, the concept of aMET was equated with loss of control.For other caregivers, the MET repre-sented an opportunity and a challenge tochange the communication patterns be-tween general floor staff and the ICU.Comments from the caregiver survey re-flect these significant cultural barriers: a)“The ICU is taking over the care of pa-tients on the inpatient unit”; b) “this willtake away educational and decision mak-ing opportunities for the residents”; andc) “physicians display a lack of respon-siveness for the concerns of the nurses.”Others have reported similar concernsabout turf and control. Hodgetts et al.(29) reviewed 139 cases of avoidable adultin-hospital cardiac arrests to determineindividual and system factors that influ-
242 Pediatr Crit Care Med 2007 Vol. 8, No. 3

enced the rate of occurrence of cardiacarrests. They described multiple factorsthat contributed to in-hospital cardiac ar-rests including failure by staff to recog-nize abnormal lab values, failure bynurses to notify physicians about abnor-mal laboratory values, and reluctance byjunior doctors to seek assistance fromsenior doctors. As the MET concept wasintroduced, issues of turf and controlwere acknowledged and reassurance wasprovided that the MET was an additionalresource for clinical decision making.Caregivers were encouraged to use theMET as a supplementary resource when aclear plan about patient disposition wasin doubt and not as a mechanism to sup-plant the traditional role of the resident,fellow, or attending. Furthermore, it wasmade clear that the MET was not an ad-versarial recourse to settle disputes be-tween physicians and nurses. Generalcare unit clinical staff were encouraged tocontact the physician most familiar withthe patient before calling the MET. Directcommunication between general careunit physicians and ICU physicians aboutrapidly deteriorating patients continuedand in some instances replaced MET ac-tivation.
Local unit managers and hospitalleaders were important for the success ofthe project. Senior hospital leaders wereneeded to provide clear authority that theMET initiative was an important hospitalpriority. Similarly, local unit leaders werekey—they determined the most appropri-ate methods to introduce the MET intheir respective areas (slides, posters, pre-sentations) and provided sustainabilitythrough feedback to staff about each METconsult. Spread and sustainability of theMET system were enhanced by spontane-ous communication among clinical staffdescribing nonconfrontational collabora-tion between the MET and the caregiverswho activated the team. Galhotra et al.(30) reported that nurses caring for adultpatients who had activated a MET consultvalued the experience, and the confidencethey gained made them likely to use thesystem a second time. Figure 4 quantifiesgeneral floor staff satisfaction with theimplemented system. Providing clinicalstaff with a mechanism for feedback andcomment about the MET process was an-other important aspect of implementa-tion. Debriefings and discussions afterMET consult helped to build enthusiasmfor the project and emphasized the role ofteam in improving patient mortality. Ap-pendix 1 describes the performance as-
sessment feedback survey, and Figure 4 isa sample of the survey data. This real-time feedback allowed MET implementa-tion to occur without the process beingperfect before rollout. Feedback could beanalyzed quickly and the MET systemrapidly adjusted in response.
This report has several limitations andpresents some controversial issues. First,the MET activation criteria used in ourhospital were effective and may serve as aframework for others, but these criteriahave not been validated across multiplecenters. The success using these criteriain our hospital may relate as much toimplementation strategies as to specificactivation criteria. Second, some will notagree with our definitions of “MET-preventable” codes. The definitions wereprospectively determined, and the chartof each patient was reviewed to determinewhether MET triggers were present be-fore the code. We believe that by present-ing all code rates and preventable coderates, the reader can fully evaluate thepotential impact of a MET. Third, this isthe first pediatric report to include bothrespiratory arrest and cardiopulmonaryarrest data, whereas prior studies havefocused only on cardiopulmonary arrests.This makes comparison with other stud-ies more difficult. Because respiratory ar-rest alone was common in our study andsome of these patients died, we would beremiss to exclude these patients from re-view. To facilitate comparison, we haveincluded data about only cardiopulmo-nary arrests in Table 4. Fourth, previousreports and a recent consensus confer-ence normalized cardiac arrest data orcode data to 1,000 admissions (28). Wechose to adjust our data to 1,000 patientdays, because we believe that the risk fora code is much more dependent on thedays of exposure to the risk (i.e., totalhospital days) than on total admissions,which does not take into account varyinglength of stay. Using the 1,000 admissiondenominator, our results and conclu-sions did not change; however, so thereader can compare our data with priorreports, we present both denominators inthe text, figures, and tables. Fifth, asmentioned in the methods, our analysisuses both one-tailed and two-tailed statis-tical tests. Most clinical studies that ana-lyze outcome differences before and afteran intervention (drug treatment, diag-nostic intervention) use two-tailed anal-ysis because the outcome after the inter-vention could be either worse or better.Because there is no reasonable concern
that implementing a MET will worsenoutcome, we believe that one-tailed anal-ysis is most appropriate. For complete-ness we have presented data using bothanalytic approaches.
This improvement initiative has pro-vided a template for how to implement aMET team in a large tertiary teachingchildren’s facility. More important, thisstudy demonstrates that implementationof a MET can reduce the incidence ofrespiratory and cardiopulmonary arrestsoutside the critical care areas in a singlechildren’s hospital. More long-range dataare needed to fully examine the effect ofMETs on pediatric hospital mortality.
REFERENCES
1. University of California, San Francisco, Stan-ford University Evidence-Based Practice Cen-ter: Evidence Research Measures of PatientSafety Based on Hospital AdministrativeData: The Patient Safety Indicators. Rock-ville, MD, Agency for Healthcare Researchand Quality, 2002
2. Sedman A, Harris M, Schulz K, et al: Rele-vance of the Agency for Healthcare Researchand Quality Patient Safety Indicators for Chil-dren’s Hospitals. Pediatrics 2005; 115:135–145
3. 100K Lives Campaign—Getting Started Kit:Rapid Response Teams. Available at: http://www.ihi.org/IHI/Programs/Campaign/Campaign.htm?TabId�1.Accessed February 6, 2006
4. Bellomo R, Goldsmith D, Uchino S, et al: Aprospective before-and-after trial of a medi-cal emergency team. Med J Aust 2003; 179:283–287
5. Bristow PJ, Hillman KM, Chey T, et al: Ratesof in-hospital arrests, deaths and intensivecare admission: The effect of a medical emer-gency team. Med J Aust 2000; 173:236–240
6. Buist M, Moore G, Bernard S, et al: Effects ofa medical emergency team on reduction ofincidence of and mortality from unexpectedcardiac arrests in hospital: Preliminarystudy. BMJ 2002; 324:387–389
7. Bellomo R, Goldsmith D, Uchino S, et al:Prospective controlled trial of effect of med-ical emergency team on postoperative mor-bidity and mortality rates. Crit Care Med2004; 32:916–921
8. DeVita M, Braithwaite R, Mahidhara R, et al:Use of medical emergency team responses toreduce hospital cardiopulmonary arrests.Qual Saf Health Care 2004; 13:251–254
9. Kenward G, Castle N, Hodgetts T, et al: Eval-uation of a Medical Emergency Team oneyear after implementation. Resuscitation2004; 61:257–263
10. Suominen P, Olkkola K, Voipio V, et al: Ut-stein style reporting of in-hospital paediatriccardiopulmonary resuscitation. Resuscita-tion 2000; 45:17–25
11. Reis A, Nadkarni V, Perondi M, et al: A pro-spective investigation into the epidemiology
243Pediatr Crit Care Med 2007 Vol. 8, No. 3

of in-hospital pediatric cardiopulmonary re-suscitation using the international Utsteinreporting style. Pediatrics 2002; 109:200–209
12. Nadkarni V, Larkin G, Peberdy M, et al: Firstdocumented rhythm and clinical outcomefrom in-hospital cardiac arrest among chil-dren and adults. JAMA 2006; 295:50–57
13. Lopez-Herce J, Garcia C, Dominquez P, et al:Characteristics and outcome of cardiorespi-ratory arrest in children. Resuscitation 2004;63:311–320
14. Tibballs J, Kinney S, Duke T, et al: Reductionof paediatric in-patient cardiac arrest anddeath with a medical emergency team: Pre-liminary results. Arch Dis Child 2005; 90:1148–1152
15. Langley G, Nolan K, Nolan T, et al: TheImprovement Guide: A Practical Approachto Enhancing Organizational Performance.1st ed. San Francisco, CA, Jossey-Bass,1996
16. Braithwaite R, DeVita M, Mahidhara R, et al:Use of medical emergency team (MET) re-sponses to detect medical errors. Qual SafHealth Care 2004; 13:255–259
17. López-Herce J, García C, Rodriquez-NunezA, et al: Long-term outcome of paediatric
cardiorespiratory arrest in Spain. Resuscita-tion 2005; 64:79–85
18. Goldhill DR, Worthington L, Mulcahy A, etal: The patient-at-risk team: Identifying andmanaging seriously ill ward patients. Anaes-thesia 1999; 54:853–860
19. MERIT study investigators: Introduction ofthe medical emergency team (MET) system:A cluster-randomized controlled trial. Lan-cet 2005; 365:2091–2097
20. Winters B, Pham J, Pronovost P: Rapid re-sponse teams—Walk, don’t run. JAMA 2006;296:1645–1647
21. Hodgetts T, Kenward G, Vlachonikolis I, etal: The identification of risk factors for car-diac arrest and formulation of activation cri-teria to alert a medical emergency team. Re-suscitation 2002; 54:125–131
22. Buist M, Bernard S, Nguyen TV, et al: Asso-ciation between clinically abnormal observa-tions and subsequent in-hospital mortality: Aprospective study. Resuscitation 2004; 62:137–141
23. Oggioni R, Bandini F, Fradella G, et al: Bed-side clinical severity score to assess patientsat risk and to prevent in-hospital cardiacarrest. Crit Care Med 2004; 32:A65
24. Foraida M, DeVita M, Braithwaite S, et al:
Improving the utilization of medical crisisteams (condition C) at an urban tertiary carehospital. J Crit Care 2003; 18:87–94
25. Subbe C, Williams E, Gemmell L, et al: Aremedical emergency teams picking up enoughpatients with increased respiratory rate? CritCare Med 2004; 32:1983–1984
26. Monaghan A: Detecting and managing dete-rioration in children. Paediatr Nurs 2005;17:32–35
27. Duncan H, Hutchison J, Parshuram C: Thepediatric early warning system score: A se-verity of illness score to predict urgent med-ical need in hospitalized children. J Crit Care2006; 21:271–279
28. DeVita M, Bellomo R, Hillman K, et al: Find-ings of the First Consensus Conference onMedical Emergency Teams. Crit Care Med2006; 34:2463–2478
29. Hodgetts T, Kenward G, Vlachonikolis I, etal: Incidence, location, and reasons for avoid-able in-hospital cardiac arrest in a districtgeneral hospital. Resuscitation 2002; 54:115–123
30. Galhotra S, Scholle C, Dew M, et al: Medicalemergency teams: A strategy for improvingpatient care and nursing work environments.J Adv Nurs 2006; 55:180–187
244 Pediatr Crit Care Med 2007 Vol. 8, No. 3

Appendix 1. Medical Emergency Team (MET) Responder Evaluation Form
245Pediatr Crit Care Med 2007 Vol. 8, No. 3
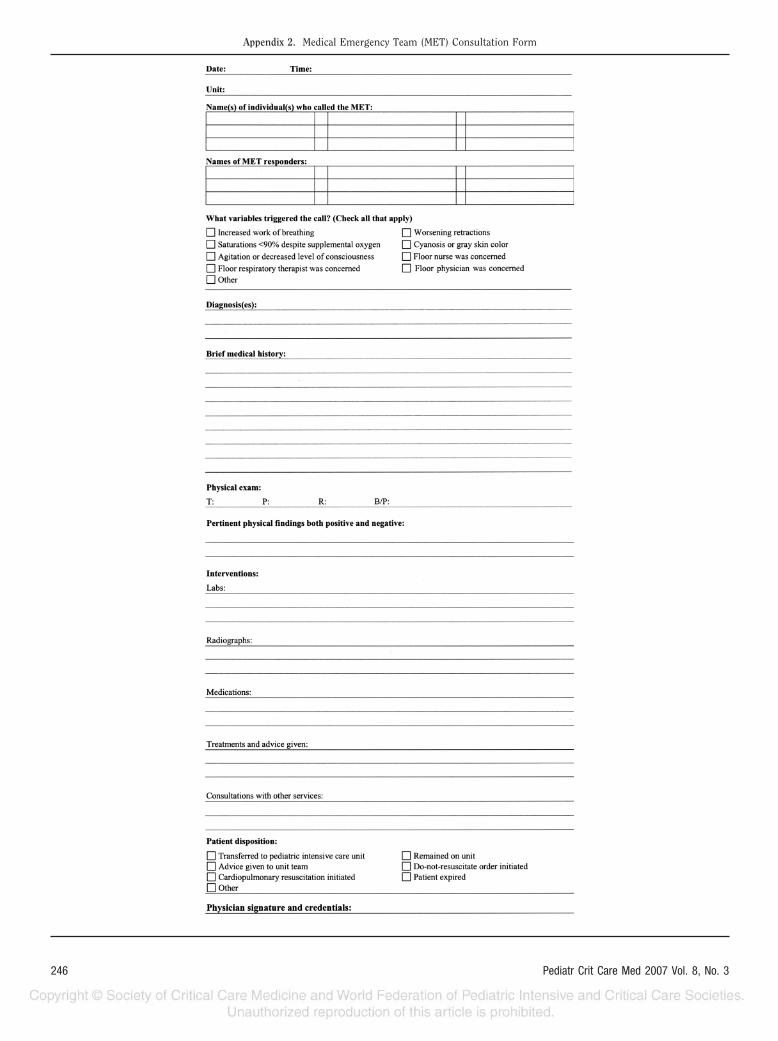
Appendix 2. Medical Emergency Team (MET) Consultation Form
246 Pediatr Crit Care Med 2007 Vol. 8, No. 3