computerized physician order entry in critical care
TRANSCRIPT
Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38
Contents lists available at ScienceDirect
Best Practice & Research ClinicalAnaesthesiology
journal homepage: www.elsevier .com/locate/bean
3
Computerized physician order entry in critical care
Kirsten Colpaert, MD, Medical Doctor, Intensivist *, Johan Decruyenaere, MD,PhD, Professor of Medicine, Head of DepartmentDepartment of Intensive Care Medicine, Ghent University Hospital, De Pintelaan 185, B-9000 Ghent, Belgium
Keywords:computerized physician order entrymedication erroradverse drug eventcritical care medicine
* Corresponding author. Tel.: þ32 9 332 63 17; FE-mail address: [email protected] (K. C
1521-6896/$ – see front matter � 2008 Elsevier Ltdoi:10.1016/j.bpa.2008.07.002
Computerized physician order entry means prescribing of medi-cation and ordering laboratory tests or radiology examinations inan electronic way instead of using paper forms. In itself, it offersadvantages such as legible orders, faster order completion,inventory management and automatic billing. If combined withclinical decision support, the real benefits of CPOE becomeapparent in the first place by prevention of medication errors andadverse drug events. On the contrary, if CPOE configuration is notdone carefully, adverse drug events can be facilitated. Therefore,and for reasons of end-user acceptance, implementation is chal-lenging. CPOE has the potential for significant economic saving.However, the initial implementation cost is high.
� 2008 Elsevier Ltd. All rights reserved.
Introduction
Computerized Physician Order Entry (CPOE) refers to the entry process of physician instructions inan electronic way, and in that way replaces verbal or written paper-based orders. Besides the termComputerized Physician Order Entry, the terms Computerized Provider Order Entry or ComputerizedPrescriber Order Entry are sometimes used, because physicians are not the only ones to order on CPOE.Nurse practitioners and physician assistants order on CPOE as well.
Using information and communication technology (ICT) for entry of medical orders offers theo-retically many advantages: less delay in order completion, reduced errors related to handwriting,transcription or verbal communication, potential to do the order entry at the point-of-care and evenoff-site, possibility of error checking, inventory management support, potential for automatic billingand decision support at the moment of electronic order entry.
ax: þ32 9 332 50 21.olpaert).
d. All rights reserved.

K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3828
CPOE refers to a variety of orders including medication orders, laboratory and radiology orders.The most important area with the highest possible benefits involves the medication prescriptionprocess and this is also the focus of this review. According to the important report ‘‘To Err is Human’’by the Institute of Medicine, 7000 deaths occur annually in the United States due to medication errors(MEs).1 This report suggests widespread implementation of hospital-based CPOE to improve thesafety and quality of healthcare delivery. CPOE is also one out of three safety initiatives with thegreatest potential to reduce deaths due to medical errors, recommended by the Leapfrog Group,a large consortium of private and public purchasers.2 For various reasons, especially the ICU is a highrisk environment, where patients experience, on average, 1.7 errors per day3, and suffer during theirICU stay at least one potential life-threatening error. Most errors are not due to individual mistakesand the best prevention strategies therefore target systems by optimalizing work processes, and thisis where CPOE comes in.4
It is important to realize that not all CPOE systems have the same features. Standard CPOE onlyallows for standardized order entry, which means that only electronic orders are accepted in a standardand complete format, thereby also ensuring legibility. Nowadays, almost all CPOE systems includefacilities for ‘‘Clinical Decision Support (CDS)’’ of varying sophistication. Basic CDS may includesuggestions or default values for drug doses, routes, and frequencies. More sophisticated CDS canperform drug-allergy checks, drug-laboratory value checks, drug-drug interaction checks, in additionto providing reminders about corollary orders (e.g. prompting the user to order glucose checks afterordering insulin or prompting osmolality checks after ordering mannitol). The most advanced CDSincludes the integration of guidelines to assist the physician at the time of drug prescription.5 Thesemore sophisticated systems provide physicians with an environment that is more appropriate for thecomplexities of today’s medicine than a paper-based setting6 (See Table 1).
Especially the critical care patient is vulnerable to safety challenges and particulary MEs, and in thatway finds himself in the most perfect environment to benefit from the potential advantages of CPOE.
Table 1Advantages of CPOE systems.
Advantages of CPOE Systems in Comparison with the Paper-Based Setting
CPOE without CDSFaster to the pharmacy resulting in less delay in order completionFree of handwriting identification problemsPossibility to do the order at the point-of-care or even off-siteSupport for inventory managementPotential for automatic billingPotential to identify the prescribing physician
CPOE with basic CDSDefault values for drug doses, routes and frequenciesLess subject to error associated with similar drug namesAble to avoid specification errors, such as trailing zeros
CPOE with advanced CDSDrug allergy checksDrug-laboratory value checksDrug-drug interaction checksAble to generate reminders for corollary ordersAble to integrate with drug guidelinesAble to avoid incorrect drug choices f.e. for antibiotic therapyAble to suggest dose adaptations according to evolutions in renal functionPotential for significant economic savings
Suggest enteral route over parenteral routeReduce overprescribingSuggest more cost-effective alternativesSuggest appropriate duration of drug therapies
CPOE¼ computerized physician order entry.
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38 29
Intensive Care Units (ICUs) are typically extremely data-rich environments with around the clockincoming physiologic and test result data.7 There is an increasing amount of up-do-date therapeuticoptions, new medications, and an overwhelming amount of, more or less important, interactions,together with an increased vulnerability of the critical care patient to delayed or suboptimal care.8
In this review, we discuss the potential benefits, risks, costs and implementation barriers of CPOE incritical care.
CPOE and medication errors
Medication errors in health care
MEs often have tragic consequences for patients. Many serious MEs result in preventable adversedrug events (ADEs), approximately 20% of which are life-threatening. In 1999, the Institute of Medicinestated in their groundbreaking report that in the US MEs account for at least 770.000 injured, and 7000deaths annually.1,9 These drug-related errors can occur at all stages of the medication process and arecategorized into six broad stages: prescription (ordering), transcription, preparation, dispensation,administration and, if necessary, monitoring of the drug.
The earlier an error occurs in the medication process, the more chance it will be intercepted beforeit reaches the patient.10 Nurses and pharmacists are shown to intercept up to 70% of prescription errorson general wards.11 More than half of the errors occur during the administration stage, followed byprescription, preparation and transcription.12 The latter errors are mainly due to illegible handwriting,use of abbreviations, unit misinterpretation and mistakes in reading.13
Although most of these MEs are harmless, or intercepted in time, some do result in an adverse drugevent.10,14 According to Bates et al., 1/100 MEs result in an ADE, and 7/100 have the potential to do so.10
Overall, 28% to 56% of all ADEs are judged preventable, and most of these errors occur in the orderingstage of medication process.
Medication error reporting
Classification of the MEs depends on the preventability, interception, and, if not intercepted, thepotential or actual harm they cause to the patient (See Fig. 1).
The National Coordinating Council for Medication Error Reporting and Prevention15 developeda standard classification for reporting medication errors according to different types, categories andpossible causes, which is used frequently in the pharmaceutical literature. Unfortunately, this classi-fication is seldom used by clinicians evaluating the effect of CPOE on MEs, which makes comparisonbetween different studies problematic.
Irrespective of the classification ambiguities, the different types of study design make evaluation ofME or ADE even more difficult. For example, if the patient’s chart is being reviewed, the main focus ison detecting preventable MEs. But, if the clinical pharmacist is prospectively involved in the process oferror recording, especially potential and actual prescription errors, or administration errors, will beregistered.
Beside these differences in methodology, there is the issue of error reporting: some studies workwith volunteer error reporting16,17, but this has been shown to be the least efficient method fordetecting MEs, followed by chart reviewing and direct observation, the latter being the most accuratemethod.18
To conclude, it may be obvious that evaluating the influence of CPOE on MEs is not as straight-forward as one would assume.
Medication errors in the intensive care unit
In ICU settings, the rate of preventable and potential ADEs is almost twice as high as in non-ICUs.9
This can be attributed to the high number of drugs that ICU patients receive, the preference forintravenous administration and the incidence of organ failure, all of which increase the potential forerrors.9,19 Also the discharge of ICU patients poses risks, because up to three quarters of patients’
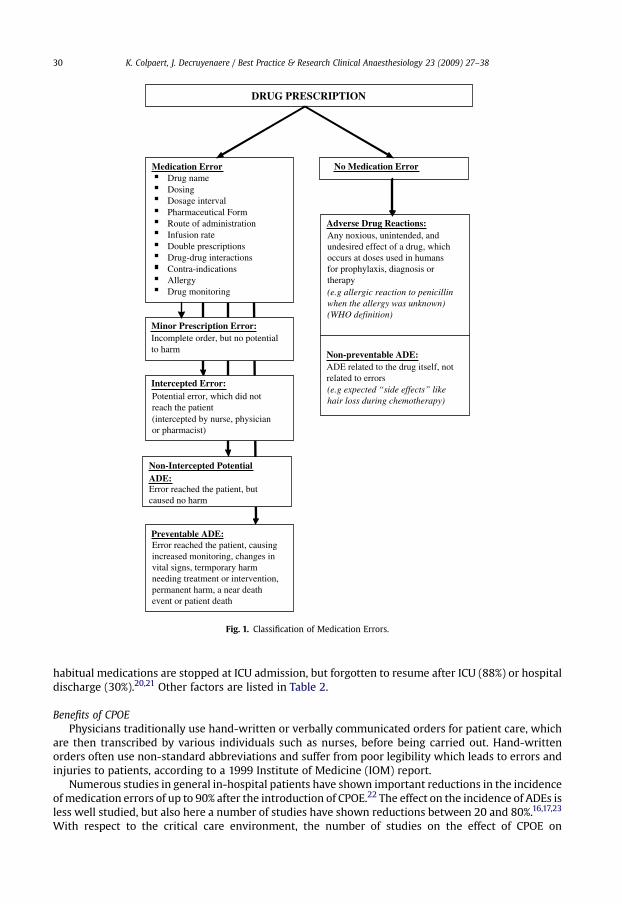
Medication ErrorDrug nameDosingDosage interval Pharmaceutical Form Route of administration Infusion rateDouble prescriptions Drug-drug interactions Contra-indications Allergy Drug monitoring
DRUG PRESCRIPTION
Minor Prescription Error:Incomplete order, but no potentialto harm
Intercepted Error:Potential error, which did notreach the patient (intercepted by nurse, physicianor pharmacist)
Non-Intercepted Potential
Error reached the patient, butcaused no harm
Preventable ADE:Error reached the patient, causingincreased monitoring, changes invital signs, termporary harmneeding treatment or intervention,permanent harm, a near deathevent or patient death
No Medication Error
Adverse Drug Reactions:Any noxious, unintended, andundesired effect of a drug, whichoccurs at doses used in humansfor prophylaxis, diagnosis ortherapy (e.g allergic reaction to penicillinwhen the allergy was unknown)(WHO definition)
Non-preventable ADE: ADE related to the drug itself, notrelated to errors (e.g expected “side effects” likehair loss during chemotherapy)
ADE:
Fig. 1. Classification of Medication Errors.
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3830
habitual medications are stopped at ICU admission, but forgotten to resume after ICU (88%) or hospitaldischarge (30%).20,21 Other factors are listed in Table 2.
Benefits of CPOEPhysicians traditionally use hand-written or verbally communicated orders for patient care, which
are then transcribed by various individuals such as nurses, before being carried out. Hand-writtenorders often use non-standard abbreviations and suffer from poor legibility which leads to errors andinjuries to patients, according to a 1999 Institute of Medicine (IOM) report.
Numerous studies in general in-hospital patients have shown important reductions in the incidenceof medication errors of up to 90% after the introduction of CPOE.22 The effect on the incidence of ADEs isless well studied, but also here a number of studies have shown reductions between 20 and 80%.16,17,23
With respect to the critical care environment, the number of studies on the effect of CPOE on

Table 2Risk Factors for Medication Errors in the ICU.
Factors Specific risk factors
Patient Severity of illnessStrongest predictor of ADEICU patients more likely to experience ADE
Extremes of ageIncreased susceptibility to ADEs
Prolonged hospitalizationIncreased exposure and susceptibility to ADEs
SedationPatients unable to participate in care and defend themselves against errors
Medications Types of medicationFrequent use of bolusses and infusionsWeight-based infusions derived from estimated weights or unreliable determinationsMathematical calculations required for medication dosagesProgramming of infusion pumps
Number of medicationsTwice as many medications prescribed as for patients in other unitsIncreased probability of ME and medication interactions
Number of interventionsIncreased risk of complications
ICU environment Complex environmentDifficult working conditions make errors more probableHigh stressHigh turnover of patients and providers
Emergency admissionsRisk of an ADE increases by approximately 6% per day
Multiple care providersChallenges the integration of different care plans
ICU: intensive care unit, ADE¼ adverse drug event, ME¼medication errors (Permission is granted by the publisher to reproducethe table from Moyen E, Camire E & Stelfox HT. Clinical review: Medication errors in critical care. Crit Care 2008 Mar 12; 12(2):208).
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38 31
medication errors is rather limited. There are 2 large studies by Bates et al.16,17, where the studypopulation consisted of a mix of general ward and ICU patients. Both studies have shown significantreductions in serious MEs (See Table 3).
Since then, 2 additional studies were performed in adult ICUs.24,25 Shulman et al. reported that thetotal proportion of MEs was significantly lower with CPOE (117 errors from 2429 prescriptions or 4.8%)than with hand-written prescription (69 errors from 1036 prescriptions or 6.7%; P< 0.04).24
In our centre25, we conducted a prospective cross-sectional trial comparing a unit with paper-basedprescription versus a unit where we implemented a commercial intensive care information systemwith incorporated CPOE and a moderate level of CDS. A total of 2,510 medication prescriptions orderedduring 160 patient days were evaluated by a clinical pharmacist. A total of 375 MEs were registered.The incidence of MEs was significantly lower in the CPOE unit compared with the paper-basedprescribing unit (44/1286 or 3.4% versus 331/1224 or 27.0%; P< 0.001). There was an almost completeelimination of minor MEs in the CPOE unit compared with the paper-based prescribing unit (9 versus225; P< 0.001). Intercepted MEs were also lower in the CPOE unit (12 versus 46; P< 0.001), as well asthe nonintercepted potential ADEs (21 versus 48; P< 0.001). There was also a statistical significantreduction of ADEs (2 in the CPOE unit versus 12 in the paper-based prescribing unit; P< 0.01).
Although these studies demonstrate that CPOE can reduce the incidence of MEs, including ADEs,more studies are needed. A recent systematic review of the effect of CPOE with clinical decision supporton the rates of ADEss identified 543 articles by MEDLINE search. However, only 10 studies met theirinclusion criteria and were included in the review analysis and only 3 of these concerned the ICU.26
Two of these ICU studies are older studies23,27 and focused only on antibiotic drug therapy. Thereforewe have not included these studies in this review.
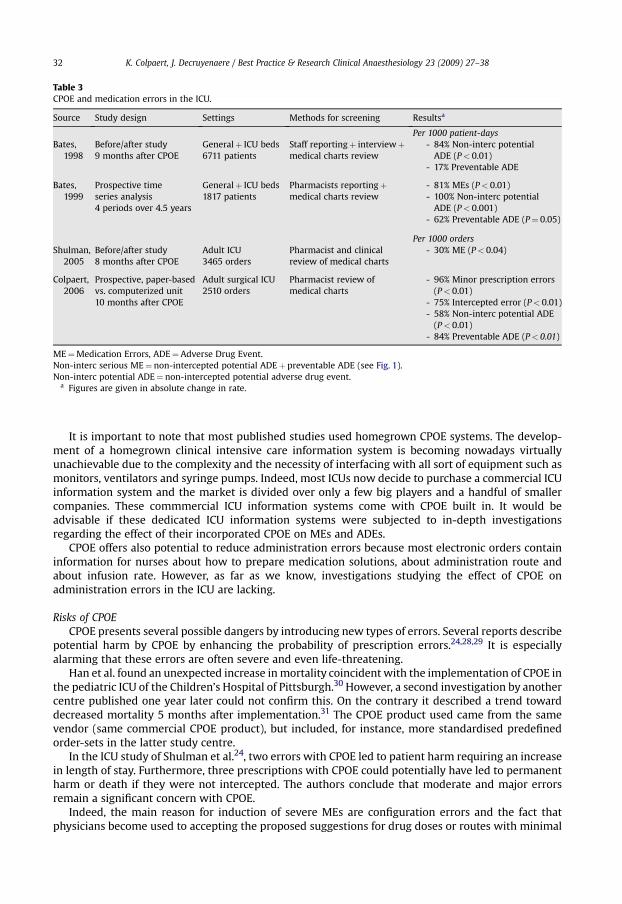
Table 3CPOE and medication errors in the ICU.
Source Study design Settings Methods for screening Resultsa
Per 1000 patient-daysBates,
1998Before/after study9 months after CPOE
Generalþ ICU beds6711 patients
Staff reportingþ interviewþmedical charts review
- 84% Non-interc potentialADE (P< 0.01)
- 17% Preventable ADE
Bates,1999
Prospective timeseries analysis4 periods over 4.5 years
Generalþ ICU beds1817 patients
Pharmacists reportingþmedical charts review
- 81% MEs (P< 0.01)- 100% Non-interc potential
ADE (P< 0.001)- 62% Preventable ADE (P¼ 0.05)
Per 1000 ordersShulman,
2005Before/after study8 months after CPOE
Adult ICU3465 orders
Pharmacist and clinicalreview of medical charts
- 30% ME (P< 0.04)
Colpaert,2006
Prospective, paper-basedvs. computerized unit10 months after CPOE
Adult surgical ICU2510 orders
Pharmacist review ofmedical charts
- 96% Minor prescription errors(P< 0.01)
- 75% Intercepted error (P< 0.01)- 58% Non-interc potential ADE
(P< 0.01)- 84% Preventable ADE (P< 0.01)
ME¼Medication Errors, ADE¼Adverse Drug Event.Non-interc serious ME¼ non-intercepted potential ADEþ preventable ADE (see Fig. 1).Non-interc potential ADE¼ non-intercepted potential adverse drug event.
a Figures are given in absolute change in rate.
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3832
It is important to note that most published studies used homegrown CPOE systems. The develop-ment of a homegrown clinical intensive care information system is becoming nowadays virtuallyunachievable due to the complexity and the necessity of interfacing with all sort of equipment such asmonitors, ventilators and syringe pumps. Indeed, most ICUs now decide to purchase a commercial ICUinformation system and the market is divided over only a few big players and a handful of smallercompanies. These commmercial ICU information systems come with CPOE built in. It would beadvisable if these dedicated ICU information systems were subjected to in-depth investigationsregarding the effect of their incorporated CPOE on MEs and ADEs.
CPOE offers also potential to reduce administration errors because most electronic orders containinformation for nurses about how to prepare medication solutions, about administration route andabout infusion rate. However, as far as we know, investigations studying the effect of CPOE onadministration errors in the ICU are lacking.
Risks of CPOECPOE presents several possible dangers by introducing new types of errors. Several reports describe
potential harm by CPOE by enhancing the probability of prescription errors.24,28,29 It is especiallyalarming that these errors are often severe and even life-threatening.
Han et al. found an unexpected increase in mortality coincident with the implementation of CPOE inthe pediatric ICU of the Children’s Hospital of Pittsburgh.30 However, a second investigation by anothercentre published one year later could not confirm this. On the contrary it described a trend towarddecreased mortality 5 months after implementation.31 The CPOE product used came from the samevendor (same commercial CPOE product), but included, for instance, more standardised predefinedorder-sets in the latter study centre.
In the ICU study of Shulman et al.24, two errors with CPOE led to patient harm requiring an increasein length of stay. Furthermore, three prescriptions with CPOE could potentially have led to permanentharm or death if they were not intercepted. The authors conclude that moderate and major errorsremain a significant concern with CPOE.
Indeed, the main reason for induction of severe MEs are configuration errors and the fact thatphysicians become used to accepting the proposed suggestions for drug doses or routes with minimal
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38 33
reflection.32 Computerization induces a false sense of security, a misconception that when technologysuggests a course of action, errors are avoided.
Advanced CDS has other potential pittfalls because frequent alerts and warnings can interrupt workflow, causing these messages to be ignored or overridden.
Therefore, the importance of evaluating a newly installed CPOE system in-depth cannot beunderestimated. In our centre, every new drug configuration or a change in an existing one, is first sentby e-mail to a core group of ICU physicians for evaluation and even double-checked by clinical phar-macists before implementing.
Another substantial problem of introducing CPOE in the ICU is the potential breakdown incommunication between physicians and nurses. Physician to nurse communication can indeedworsen if each group works alone at their workstations. Indeed, recent studies have shown that CPOEmay undermine the efficiency and safety of the medication process by impeding nurse-physiciancollaboration.33
Other beneficial effects of CPOE
Computerized alerts have an important potential to improve the quality of care. CPOE can be anessential component – when combined with other sources of clinical electronic information – ingenerating relevant electronic clinical alerts.
A recent study showed that integration of two data sources (CPOE data on blood productprescription and blood gas values from the laboratory) can screen for post-transfusion acute respira-tory lung injury (TRALI).34 The computer alert system detected the patients not only faster, but alsomore efficiently than did the clinicians’.
Timeliness of service is another important dimension for quality of care.35 This may be especiallytrue in the ICU setting because of the rapid course of organ failure which can occur in critically illpatients. Thompsom has shown that the introduction of CPOE is associated with a shorter time fromordering to reporting of results for diagnostic laboratory tests and imaging tests, with net saving ofaround 60 minutes.36
Implementing guidelines and achieving good compliance is a real challenge. CPOE may bea powerful tool to increase compliance with evidence-based guidelines in critical care.7 An exampleis the evidence-based red cell transfusion in critically ill patients. Anemia is a very common problemin ICU patients, and patients admitted to the ICU for more than 1 week are almost certainlytransfused.37 However, transfusion of blood is still associated with a number of serious complica-tions, the most important being TRALI. Moreover, a multicenter controlled clinical trial of trans-fusion requirements in critical care has shown that a liberal transfusion strategy is associated witha trend to increased mortality and increased costs.38 The ‘‘Transfusion in the ICU Interest Group’’ hasshown that the implementation of an institutional protocol and decision support through CPOEcould effectively decrease inappropriate red cell transfusion, and the associated rate of transfusioncomplications.39
Another example of a successful guideline adherence with CPOE is the study by Boord et al.40, whohas shown that a computer-based insulin infusion protocol in a surgical ICU improved glycaemiacontrol compared to the previous manual protocol, and reduced time to insulin therapy initiation.
CPOE and health care costs
Although most agree with the potential benefits of CPOE, some still wonder whether it is worth thecost. The truth is that implementation of CPOE is a very expensive and complex undertaking. This totalcost of ownership (TCO) of an ICT system can be defined as the total cost of acquiring, installing, using,maintaining, changing, upgrading and disposing of an information technology system over its pre-dicted useful lifespan. Typically, most people only consider the costs for hardware and software,thereby underestimating considerably the total cost because hard- and software represent onlya quarter to a third of the TCO (Table 4).
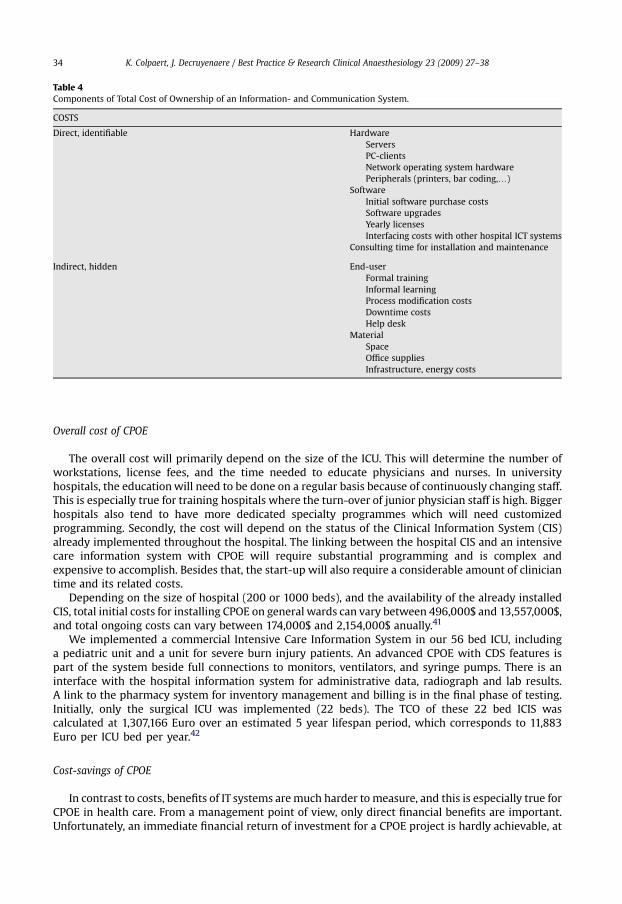
Table 4Components of Total Cost of Ownership of an Information- and Communication System.
COSTS
Direct, identifiable HardwareServersPC-clientsNetwork operating system hardwarePeripherals (printers, bar coding,.)
SoftwareInitial software purchase costsSoftware upgradesYearly licensesInterfacing costs with other hospital ICT systems
Consulting time for installation and maintenance
Indirect, hidden End-userFormal trainingInformal learningProcess modification costsDowntime costsHelp desk
MaterialSpaceOffice suppliesInfrastructure, energy costs
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3834
Overall cost of CPOE
The overall cost will primarily depend on the size of the ICU. This will determine the number ofworkstations, license fees, and the time needed to educate physicians and nurses. In universityhospitals, the education will need to be done on a regular basis because of continuously changing staff.This is especially true for training hospitals where the turn-over of junior physician staff is high. Biggerhospitals also tend to have more dedicated specialty programmes which will need customizedprogramming. Secondly, the cost will depend on the status of the Clinical Information System (CIS)already implemented throughout the hospital. The linking between the hospital CIS and an intensivecare information system with CPOE will require substantial programming and is complex andexpensive to accomplish. Besides that, the start-up will also require a considerable amount of cliniciantime and its related costs.
Depending on the size of hospital (200 or 1000 beds), and the availability of the already installedCIS, total initial costs for installing CPOE on general wards can vary between 496,000$ and 13,557,000$,and total ongoing costs can vary between 174,000$ and 2,154,000$ anually.41
We implemented a commercial Intensive Care Information System in our 56 bed ICU, includinga pediatric unit and a unit for severe burn injury patients. An advanced CPOE with CDS features ispart of the system beside full connections to monitors, ventilators, and syringe pumps. There is aninterface with the hospital information system for administrative data, radiograph and lab results.A link to the pharmacy system for inventory management and billing is in the final phase of testing.Initially, only the surgical ICU was implemented (22 beds). The TCO of these 22 bed ICIS wascalculated at 1,307,166 Euro over an estimated 5 year lifespan period, which corresponds to 11,883Euro per ICU bed per year.42
Cost-savings of CPOE
In contrast to costs, benefits of IT systems are much harder to measure, and this is especially true forCPOE in health care. From a management point of view, only direct financial benefits are important.Unfortunately, an immediate financial return of investment for a CPOE project is hardly achievable, at
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38 35
least for now. Several benefits are not easily amenable to measurement such as improved interde-partmental communication, strategic positioning, enhanced quality of care by reducing errors andadverse events or improved guideline adherence. Eventually some of these improvements could leadto a decrease in length of stay, and maybe a decrease in mortality.
As already discussed before, CPOE can prevent MEs and ADEs if an advanced and well-testedconfiguration is guaranteed to avoid the introduction of new types of errors. Although Bates et al. foundthat only less than 5% of MEs will lead to an adverse drug event43, the associated costs are shocking. It isestimated that attributable cost of an ADE lies between $2,262 and $5,857.44,45 In the study of Classenet al. length of hospital stay increases with 1.9 to 2.2 days and Odds ratio for mortality was 1.88 (95% CI,1,54–2,22; P< .001).44 For a 700-bed teaching hospital this could mean an attributable annual cost of$5.6 million for all ADEs occuring on general wards.45
Only 2 very recent studies evaluated the cost of ADEs in the ICU. The first study conducted in a largeacademic centre found that the attributable cost of an ADE amounts to $3,961 in a medical ICU and to$3,857 in a cardiac ICU and was associated with an increased length of ICU stay of 0.77 to 1.08 days,respectively. Total additional costs would be $1.5 million per year for both a ten-bed medical andcardiac ICU.46 The second study evaluated costs of ADEs related to intravenous drug therapy in 3academic and 2 nonacademic centres, and found that, in academic ICUs, ADEs induced an additionalcost of $6,647 and an additional 4.8 days longer hospital stay. But surprisingly, ADEs in nonacademicICUs were not related with increased cost nor length of stay. A possible explanation given by theauthors is the difference in practice pattern in response to intravenous ADEs. Academic centres, i.e.the trainee physicians, respond more inefficiently to ADEs and tend to delay ICU discharge after theoccurence of an ADE.47
CPOE can save costs by suggesting medication substitution during the prescribing process.However, hard data about the real potential savings are lacking. Even the most basic CPOE can guide
the physician when subscribing drugs. Switching from intravenous to oral drugs could lead toimportant pharmacy savings, especially for some expensive intravenous antibiotics with a high enteralbioavailability such as quinolones, antifungal azole medications or metronidazole. Even the seeminglytrivial switch from intravenous to oral paracetamol in appropriate patients could decrease coststremendously, because of high use of these agents in the ICU.
CPOE also has the potential for cost saving from reduced laboratory testing. Thierney et al. found437 redundant laboratory tests among 5,700 outpatient diagnostic tests with CPOE. Physicianscancelled almost 70% of these tests after their redundancy was flagged by the CPOE system.48
CPOE with sophisticated CDS and possibility of incorporating evidence-based guidelines can lead toincreased guideline adherence resulting in improved patient outcome, optimalisation of resource useand decreased length of stay. A study by Evans et al.28 using a antiinfectives-management electronicorder entry programme showed a decrease in average ICU costs of $9,000 per patient mainly due toa reduced average length of stay.
Finally, CPOE allows for automatic, faster and more complete billing of medication which,depending on the local reimbursement system, can have important consequences for the ICU financialmanagement.
Implementation of CPOE
Despite the considerable benefits published in the recent literature, the implementation of CPOEsystems in health care and ICUs has been slow. According to Kuperman et al.49 less than 5% of UShospitals have fully implemented CPOE systems. A recent survey about the use of ICT in 50 ICUs inCanada has shown that 46% had medication administration records, 26% physician or nursing notes,and only 22% had implemented CPOE.50 No association was found between IT availability and ICU sizeor university affiliation.
CPOE systems can take years to install and configure. Beside this, other barriers to implementationare the significant financial costs to institutions, willingness to adopt the technology and fear fortechnical malfunctions.51,52 Remarkably, one of the most prevalent barriers to successful imple-mentation is resistance from physicians. Doctors often have the fear of negative impact on productivity,and resist the idea of loosing clinical ‘‘independence’’ and unrestricted control over prescribing.53
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3836
A successful implementation needs leadership vision and commitment. Particularly thoroughcommunication of the ultimate goals of CPOE is important: improving patient safety and quality of careand optimizing work flow processes. Adequate financial resources must be guaranteed to providea sufficient number of clinical workstations or portables to facilitate order entry by physicians.50
User interfaces need to be intuitive and optimally designed to fit physicians’ workflow in order toachieve a maximal beneficial effect. Bates identified ten commandments for successful implementa-tion of CDS.54 The most important one is the speed of the information system. This parameter is mosthighly valued among physicians, even more than quality improvement aspects.55 It is also important tonote that the applications must anticipate the clinicians’ needs, and bring the information they need inreal-time. Especially in the data-rich ICU environment, crucial information can be lost or not identified,for example the presence of low-potassium level in a patient who is subscribed a diuretic.
Summary
Computerized physician order entry in critical care can improve safety of health care by reducingmedication errors and adverse drug events. Sophisticated systems have advanced facilities for clinicaldecision support included, and have therefore the greatest potential in reducing errors. Other bene-fecial effects of CPOE are improvement in quality of care by enhancing timeliness of service andincreasing compliance with guidelines. On the other hand, some reports have shown the introductionof new types of errors after the CPOE implementation, especially due to configuration errors, requiringin-depth evaluation of every newly installed system. But although the overall benefit of CPOE seemsclear, implementation in critical care has been slow. Most important barriers are resistance of thephysician end-user and the significant financial cost. On the other hand, CPOE has the potential forsignificant economic savings, in the first place by avoiding attributable costs of adverse drug events.
Practice points
� CPOE has several inherent advantages over handwritten orders such as legibility, potential formedication inventory management and automatic billing.� With the addition of CDS, CPOE systems have emerged as a key technology for reducing
medical errors in the hospital. Also for the ICU there is ample evidence that CPOE has thepotential of reducing medication prescribing orders, and this is especially true for minorerrors.� The ICU environment and the effect on more serious medication errors like ADE are less well
studied. Some studies show important ADE incidence reductions while other show a risk ofintroducing new types of even severe errors. The configuration of the CPOE here seems thecrucial factor to guarantee patients’ safety benefits and must be the subject of a constant anditerative quality improvement project.� CPOE implementation needs time and has high initial costs. Cost savings are described due to
the avoidance of attributable costs of ADEs.
Research agenda
� More trials are warranted preferentially about CPOE systems incorporated in commercial ICUclinical information systems with advanced CDS. An adequate design using clusterrandomization techniques and incorporating health economic evalutions is important.� Increasing collaborative research for standardization of functional CDS requirements in CPOE
systems and for development of re-usable software components is urgently needed to avoidthat every centre has to reinvent the wheel in guaranteeing patient safety benefits and insaving implementation time and money.
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–38 37
References
1. Kohn LT, Corrigan J, Donaldson MS & Institute of Medicine. To err is human: building a safer health system. Washington, DC:National Academia Press, 1999.
2. The leapfrog Group for Patient Safety. Rewarding Higher Standards. Available from: WWW.Leapfroggroup.org [accessed16.06.2008].
*3. Donchin Y, Gopher D & Olin M. A look into the nature and causes of human errors in the intensive care unit. Critical CareMedicine 1995 Feb; 23(2): 294–300.
4. Cullen DJ, Bates DW & Leape LL. Adverse Drug Event Prevention Study Group. Prevention of adverse drug events: a decadeof progress in patient safety. Journal of Clinical Anesthesia 2000 Dec; 12(8): 600–614.
5. Overhage JM, Tierney WM, Zhou XH & McDonald CJ. A randomized trial of ‘‘corollary orders’’ to prevent errors of omission.Journal of the American Medical Informatics Association 1997 Sep–Oct; 4(5): 364–375.
6. Kuperman GJ & Gibson RF. Computer physician order entry: benefits, costs, and issues. Annals of Internal Medicine 2003 Jul1; 139(1): 31–39.
*7. Rothschild J. Computerized physician order entry in the critical care and general inpatient setting: a narrative review.Journal of Critical Care 2004 Dec; 19(4): 271–278.
8. Nebeker JR, Hoffman JM & Weir CR. High rates of adverse drug events in a highly computerized hospital. Archives ofInternal Medicine 2005 May 23; 165(10): 1111–1116.
9. Cullen DJ, Sweitzer BJ, Bates DW et al. Preventable adverse drug events in hospitalized patients: a comparative study ofintensive care and general care units. Critical Care Medicine 1997 Aug; 25(8): 1289–1297.
10. Bates DW, Cullen DJ, Laird N et al. Incidence of adverse drug events and potential adverse drug events. Implicationsfor prevention. ADE prevention Study Group. JAMA: The Journal of the American Medical Association 1995 Jul 5; 274(1): 29–34.
11. Leape LL, Bates DW, Cullen DJ et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA: TheJournal of the American Medical Association 1995 Jul 5; 274(1): 35–43.
12. Krahenbuhl-Melcher A, Schlienger R, Lampert M et al. Drug-related problems in hospitals: a review of the recent liter-ature. Drug Safety 2007; 30(5): 379–407.
*13. Moyen E, Camire E & Stelfox HT. Clinical review: medication errors in critical care. Critical Care (London, England) 2008 Mar12; 12(2): 208.
14. Allan EL & Barker KN. Fundamentals of medication error research. American Journal of Hospital Pharmacy 1990 Mar; 47(3):555–571.
15. National Coordinating Council for Medication Error Reporting and Prevention NCCMERP. NCC MERP taxonomy of medi-cation errors office of the secretariat. US Pharmacopeia, 1998.
*16. Bates DW, Leape LL, Cullen DJ et al. Effect of computerized physician order entry and a team intervention on prevention ofserious medication errors. JAMA: The Journal of the American Medical Association 1998 Oct 21; 280(15): 1311–1316.
*17. Bates DW, Teich JM, Lee J et al. The impact of computerized physician order entry on medication error prevention. Journalof the American Medical Informatics Association 1999 Jul–Aug; 6(4): 313–321.
18. Flynn EA, Barker KN & Pepper GA. Comparison of methods for detecting medication errors in 36 hospitals and skillednursing facilities. American Journal of Health-system Pharmacy 2002 Mar 1; 59(5): 436–446.
19. Herout PM & Erstad BL. Medication errors involving continuously infused medications in a surgical intensive care unit.Critical Care Medicine 2004 Feb; 32(2): 428–432.
20. Campbell AJ, Bloomfield R & Noble DW. An observational study of changes to long-term medication after admission to anintensive care unit. Anaesthesia 2006 Nov; 61(11): 1087–1092.
21. Bell CM, Rahimi-Darabad P & Orner AI. Discontinuity of chronic medications in patients discharged from the intensive careunit. Journal of General Internal Medicine 2006 Sep; 21(9): 937–941.
22. Shamliyan TA, Duval S & Kane RL. Just what the doctor ordered. Review of the evidence of the impact of computerizedphysician order entry system on medication errors. Health Services Research 2008 Feb; 43(1 Pt 1): 32–53.
23. Evans RS, Pestotnik SL & Classen DC. Preventing adverse drug events in hospitalized patients. The Annals of Pharmaco-therapy 1994 Apr; 28(4): 523–527.
*24. Shulman R, Singer M, Goldstone J & Bellingan G. Medication errors: a prospective cohort study of hand-written andcomputerised physician order entry in the intensive care unit. Critical Care (London, England) 2005 Oct 5; 9(5): R516–R521.
*25. Colpaert K, Claus B, Somers A et al. Impact of computerized physician order entry on medication prescription errors in theintensive care unit: a controlled cross-sectional trial. Critical Care (London, England) 2006 Feb; 10(1): R21.
*26. Wolfstadt JI, Gurwitz JH & Field TS. The effect of computerized physician order entry with clinical decision support on therates of adverse drug events: a systematic review. Journal of General Internal Medicine 2008 Apr; 23(4): 451–458.
27. Evans RS, Pestotnik SL, Classen DC et al. A computer-assisted management program for antibiotics and other antiinfectiveagents. The New England Journal of Medicine 1998 Jan 22; 338(4): 232–238.
28. Senholzi C & Gottlieb J. Pharmacist interventions after implementation of computerized prescriber order entry. AmericanJournal of Health-system Pharmacy 2003 Sep 15; 60(18): 1880–1882.
29. George D & Austin-Bishop N. Error rates for computerized order entry by physicians versus nonphysicians. AmericanJournal of Health-system Pharmacy 2003 Nov 1; 60(21): 2250–2252.
30. Han YY, Carcillo JA, Venkataraman ST et al. Unexpected increased mortality after implementation of a commercially soldcomputerized physician order entry system. Pediatrics 2005 Dec; 116(6): 1506–1512.
31. Del Beccaro MA, Jeffries HE, Eisenberg MA & Harry ED. Computerized provider order entry implementation: no associationwith increased mortality rates in an intensive care unit. Pediatrics 2006 Jul; 118(1): 290–295.
32. Nadzam DM & Macklis RM. Promoting patient safety: is technology the solution? The Joint Commission Journal on QualityImprovement 2001 Aug; 27(8): 430–436.
33. Pirnejad H, Niazkhani Z & Van der Sijs H. Impact of a computerized physician order entry system on nurse-physiciancollaboration in the medication process. International Journal of Medical Informatics 2008 May 29.
34. Finlay-Morreale HE, Louie C & Toy P. Computer-generated automatic alerts of respiratory distress after blood transfusion.Journal of the American Medical Informatics Association 2008 May–June; 15(3): 383–385.
K. Colpaert, J. Decruyenaere / Best Practice & Research Clinical Anaesthesiology 23 (2009) 27–3838
35. Committee on Quality of Health Care in America, Institute of Medicine. Crossing the quality chasm: a new health system forthe 21st century. Washington, DC: National Academy Press, 2001.
36. Thompson W, Dodek PM, Norena M & Dodek J. Computerized physician order entry of diagnostic tests in an intensive careunit is associated with improved timeliness of service. Critical Care Medicine 2004 Jun; 32(6): 1306–1309.
37. Corwin HL, Parsonnet KC & Gettinger A. RBC transfusion in the ICU. Is there a reason? Chest 1995 Sep; 108(3): 767–771.38. Hebert PC, Wells G & Blajchman MA. A multicenter, randomized, controlled clinical trial of transfusion requirements in
critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. The New EnglandJournal of Medicine 1999 Feb 11; 340(6): 409–417.
39. Rana R, Afessa B, Keegan MT et al. Evidence-based red cell transfusion in the critically ill: quality improvement usingcomputerized physician order entry. Critical Care Medicine 2006 Jul; 34(7): 1892–1897.
40. Boord JB, Sharifi M, Greevy RA et al. Computer-based insulin infusion protocol improves glycemia control over manualprotocol. Journal of the American Medical Informatics Association 2007 May–Jun; 14(3): 278–287.
41. Birkmeyer CM, Lee J & Bates DW. Will electronic order entry reduce health care costs? Effective Clinical Practice 2002; 5:67–74.
42. Decruyenaere J, Danneels C & Verwaeren G. Calculation of the total cost of ownership of an intensive care informationsystem. Critical Care Medicine 2004 Dec; 32(Suppl): A116.
43. Bates DW, Boyle DL, Vander Vliet MB et al. Relationship between medication errors and adverse drug events. Journal ofGeneral Internal Medicine 1995 Apr; 10(4): 199–205.
44. Classen DC, Pestotnik SL & Evans RS. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, andattributable mortality. JAMA: The Journal of the American Medical Association 1997 Jan 22–29; 277(4): 301–306.
45. Bates DW, Spell N & Cullen DJ. The costs of adverse drug events in hospitalized patients. Adverse Drug Events PreventionStudy Group. JAMA: The Journal of the American Medical Association 1997 Jan 22–29; 277(4): 307–311.
*46. Kaushal R, Bates DW & Franz C. Costs of adverse drug events in intensive care units. Critical Care Medicine 2007; 35(11):2479–2483.
47. Nuckols TK, Paddock SM & Bower AG. Costs of intravenous adverse drug events in academic and nonacademic intensivecare units. Medical Care 2008 Jan; 46(1): 17–24.
48. Tierney WM, Miller ME & McDonald CJ. The effect on test ordering of informing physicians of the charges for outpatientdiagnostic tests. The New England Journal of Medicine 1990 May 24; 322(21): 1499–1504.
49. Kuperman GJ, Bobb A, Payne TH et al. Medication-related clinical decision support in computerized provider order entrysystems: a review. Journal of the American Medical Informatics Association 2007 Jan-Feb; 14(1): 29–40.
50. Lapinsky SE, Holt D, Hallett D et al. Survey of information technology in Intensive Care Units in Ontario, Canada. BMCMedical Informatics and Decision Making 2008 Jan 24; 8: 5.
51. Weant KA, Cook AM & Armitstead JA. Medication-error reporting and pharmacy resident experience duringimplementation of computerized prescriber order entry. American Journal of Health-system Pharmacy 2007 Mar 1; 64(5):526–530.
52. Hussain E & Kao E. Medication safety and transfusion errors in the ICU and beyond. Critical Care Clinics 2005 Jan; 21(1):91–110.
53. Jones S & Moss J. Computerized provider order entry: strategies for successful implementation. The Journal of NursingAdministration 2006 Mar; 36(3): 136–139.
*54. Bates DW, Kuperman GJ, Wang S et al. Ten commandments for effective clinical decision support: making the practice ofevidence-based medicine a reality. Journal of the American Medical Informatics Association 2003 Nov–Dec; 10(6): 523–530.
55. Lee F, Teich JM & Spurr CD. Implementation of physician order entry: user satisfaction and self-reported usage patterns.Journal of the American Medical Informatics Association 1996 Jan–Feb; 3(1): 42–55.