comprehensive multi year plan - uip in india
DESCRIPTION
Multi-Year Strategic 2013-17 Plan Universal Immunization Program REACHING EVERY CHILDIndia’s Universal Immunization Programme is one of the largest of its kind in the world, in terms of quantity of vaccine used, number of beneficiaries reached out to, number of immunization sessions organized and the geographical spread and diversity of areas covered. It caters to nearly 27 million infants and 30 million pregnant women annually free of cost. Routine Immunization Program in India, Immunization Technical Support, routine immunization services in India, Ministry of Health and Family Welfare, Adverse Event Following Immunization Secretariat, Vaccine logistics and supply chain,Universal Immunization Program in IndiaTRANSCRIPT

Multi-Year Strategic 2013-17
Plan
Universal Immunization ProgramREACHING EVERY CHILD

Contents
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1. INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.1 UIP as a component of Reproductive, Maternal, Newborn, Child and Adolescent
health (RMNCH+A) in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.2 Purpose of cYMP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.3 Planning Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.4 Immunization global priorities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2. NATIONAL CONTEXT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.1 History of immunization program in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.2 National Rural Health Mission (NRHM) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.3 Burden of vaccine preventable diseases (VPDs) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.4 Status of vaccine coverage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.4.1 Vaccine coverage and equity issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.5 Current structure for service delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.5.1 Other stakeholders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.5.2 Current UIP Schedule in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.6 UIP successes as a child survival strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.7 Barriers for effective programming . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. GUIDING PRINCIPLES OF UIP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. UIP STRATEGIC PLAN: 2013-17 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.1 UIP strategic plan framework . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.2 Impact indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.3 Target population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Acknowledgment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
i
iii
v
vii
1
1223
555678
1011121314
19
21212222
M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
5. NATIONAL MONITORING AND EVALUATION PLAN FOR UIP . . . . . . . . . . . . . . . . . . . 5.1 Rationale . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.2 Objective . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.3 Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.4 Components of National M & E Plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 5.5 Process for National M & E Plan development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6. ANNEXURES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ANNEX 1: List of states showing good performance on immunization coverage and other
parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ANNEX 2: List of States showing poor performance on immunization coverage and other
parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ANNEX 3: NCCVMRC concept approved by MoHFW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ANNEX 4: Key Recommendations from Effective Vaccine Management Assessment Report
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ANNEX 5: National Open Vial Policy 2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ANNEX 6: Monitoring Framework . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ANNEX 7: Emergency Preparedness and Response Plan 2011 . . . . . . . . . . . . . . . . . . . . . . . . . .
7. COSTING AND FINANCIAL SUSTAINABILITY OF THE UNIVERSAL IMMUNIZATION PROGRAM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2. Summary of Findings on Baseline Expenditures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3. Details of Baseline Program Cost and Financing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4. Recurrent Costs - Structure and Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.1 Demographic projections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.2 Vaccine and injection supplies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.3 Personnel Costs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.4 Training, Program Management, Disease Surveillance, Social Mobilization, Advocacy
and Communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4.5 Cold Chain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.0. Future Resource Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6.0. Future Financing and funding gap analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
515151515252
53
55
5657
59626574
8385858690909194
94979899


iii

Acknowledgment
The comprehensive Multi Year plan (2013-17) was commissioned by the Ministry of Health and Family Welfare and its development was carried out under the leadership of Ms. Anuradha Gupta, Additional Secretary and Mission Director NRHM and Dr Rakesh Kumar, Joint Secretary.
We wish to acknowledge the contribution of the following from National Immunization Division, MoHFW for providing regular guidance and inputs into the document – Dr Ajay Khera, Deputy Commissioner Child Health and Immunization; Dr M.K. Agarwal, Deputy Commissioner UIP and Immunization; and Dr Pradeep Haldar, Deputy Commissioner Immunization.
Immunization Technical Support Unit (ITSU) maintained an oversight and coordinated the development of the plan by a team comprising of Dr Manish Pant, Dr Susmita Chatterjee, Dr Rajeev Gera, Ms Susmita Roy. Dr Shrihari Dutta from UNICEF India office provided technical inputs on a regular basis to this team.
Professor Ramanan Laxminarayan, Public Health Foundation of India and Dr Vijay Moses, Director ITSU were a constant source of support for the ITSU team while drafting the plan.
We are grateful to the following individuals for contributing their time and inputs in preparing this document.
Dr Brighu Kapuria ITSU
Dr Jyoti Joshi Jain ITSU
Ms. Monica Chaturvedi ITSU
Ms Chaitali Mukherjee ITSU
Dr Prem Singh ITSU
Ms. Amruta Bahulekar ITSU
Mr Nithiyananthan Muthusamy ITSU
Ms Apoorva Sharan ITSU
Mr Arup Deb Roy ITSU
Mr Rajat Jain ITSU
Dr Raveesha R. Mugali, UNICEF India
Dr Satish Gupta UNICEF India
Dr Chandrakant Lahariya WHO India
Dr Pankaj Bhatnagar WHO India
Dr Balwinder Singh WHO India
Dr Satyabrata Routray WHO India
v

Abbreviations
AEFI
AES
AFP
ASHA
AVD
AWW
BCG
bOPV
CBHI
CCE
CCL
CFC
cMYP
CRM
CSO
CSSM
DF
DIR
DPT
DTFI
EPC
EPRP
eVIN
EVM
FHW
FIR
FMG
Adverse Events Following Immunization
Acute Encephalitis Syndrome
Acute Flaccid Paralysis
Accredited Social Health Activist
Alternate Vaccine Delivery
Anganwadi Worker
Bacillus Calmette–Guérin
Bivalent Oral Polio Vaccine
Central Bureau of Health Intelligence
Cold Chain Equipment
Cold Chain and Logistics
Chloroflurocarbon
Comprehensive Multi-year Plan
Common Review Mission
Civil Society Organization
Child Survival and Safe Motherhood
Deep Freezer
Detailed Investigation Report
Diphtheria Pertussis Tetanus
District Task Force on Immunization
Evidence to Policy
Empowered Program Committee
Emergency Preparedness and Response Plan
electronic Vaccine Intelligence Network
Effective Vaccine Management
Frontline Health Worker
First Information Report
Financial Management Group
E2P
................................ v i i
M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7 v i i i
GMSD
GoI
HepB
HiB
HMIS
HR
ICDS
IDH
IEC
ILR
IMNCI
IMR
IPC
IPC
IPHS
ISP
ITSU
IUCD
JE
JRM
JSSK
JSY
KO
LHV
MCTS
MCV
MDG
MDVP
MIS
MMR
MoHFW
MSG
NBSU
NCCA
NCCMIS
NCCTC
NCCVMRC
Government Medical Store Depot
Government of India
Hepatitis B
Haemophilus influenzae B
Health Management Information system
Human Resources
Integrated Child Development Services
Infectious Diseases Hospital
Information, Education and Communication
Ice-Lined Refrigerator
Integrated Management of Neonatal and Childhood Illnesses
Infant Mortality Rate
Inter-personal Communication
Indian Pharmacopoeia Commission
Indian Public Health Standards
Immunization Strengthening Project
Immunization Technical Support Unit
Intra-Uterine Contraceptive Device
Japanese Encephalitis
Joint Review Mission
Janani Shishu Suraksha Karyakram
Janani SurakshaYojna
Key Objective
Lady Health Visitor
Mother and Child Tracking System
Measles Containing Vaccine
Millennium Development Goal
Multi Dose Vial Policy
Management Information System
Maternal Mortality Rate
Ministry of Health and Family Welfare
Mission Steering Group
Newborn Stabilization Unit
National Cold Chain Assessment
National Cold Chain Management Information System
National Cold Chain Training Center
National Cold Chain Vaccine Management Resource Center
................................
NGO
NIHFW
NNT
NRC
NRHM
NTAGI
OCP
OPV
ORS
OVP
PIP
PIR
RCH
RI
RMNCH+A
RRT
RTI
SBHI
SHTO
SIA
SMS
SNCU
STI
STSC
TFR
tOPV
TT
UIP
UNICEF
UT
VHND
VLM
VMAT
VPD
WHO
WIC
WIF
Non-Governmental Organization
National Institute of Health and Family Welfare
Neonatal Tetanus
Nutrition Rehabilitation Center
National Rural Health Mission
National Technical Advisory Group on Immunization
Oral Contraceptive Pill
Oral Polio Vaccine
Oral Rehydration Salt
Open Vial Policy
Program Implementation Plan
Preliminary Investigation Report
Reproductive and Child Health
Routine Immunization
Reproductive, Maternal, Newborn, Child & Adolescent Health
Rapid Response Team
Reproductive Tract Infection
State Bureau of Health Intelligence
State Health Transport Organization
Supplementary Immunization Activity
Short Message Text
Sick Newborn Care Unit
Sexually Transmitted Infection
Standing Technical Sub-Committee
Total Fertility Rate
Trivalent Oral Polio Vaccine
Tetanus Toxoid
Universal Immunization Program
United Nations Children's Fund
Union Territory
Village Health and Nutrition Day
Vaccines Logistics Management
Vaccine Management Assessment Tool
Vaccine Preventable Disease
World Health Organization
Walk-in Cooler
Walk-in Freezer
i x
A B B R E V I A T I O N S

Introduction
1.1 UIP as a component of Reproductive, Maternal, Newborn, Child and Adolescent Health in India
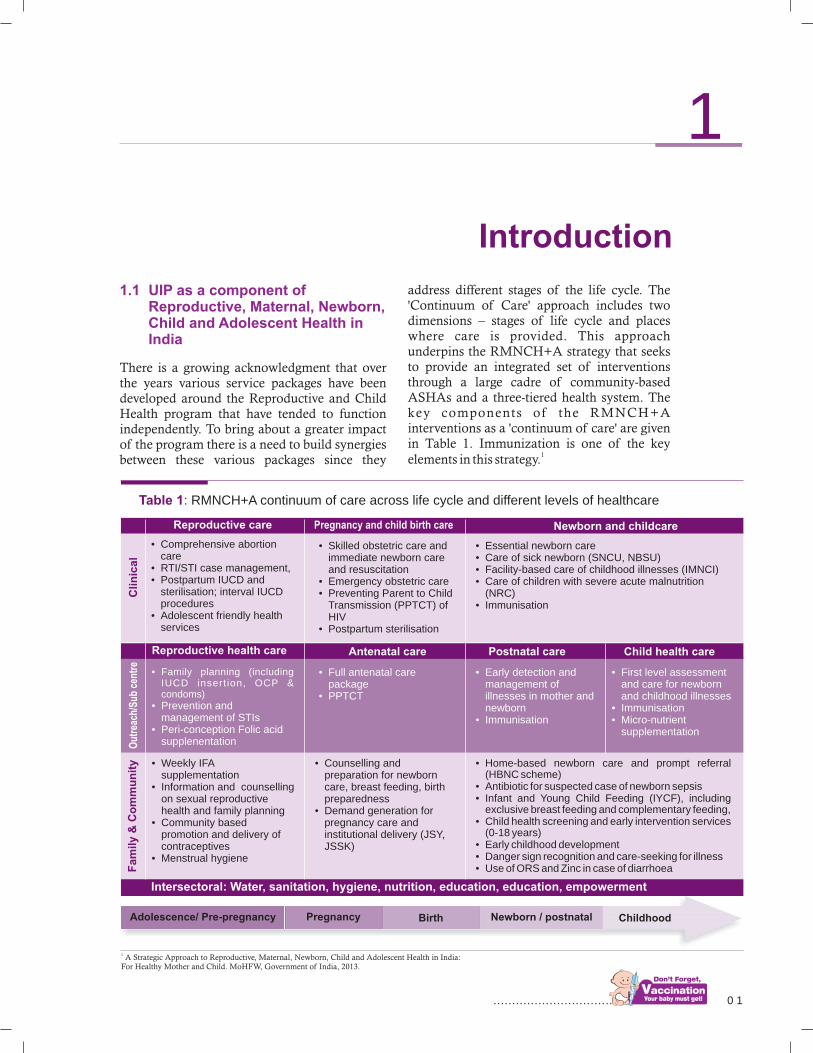
There is a growing acknowledgment that over the years various service packages have been developed around the Reproductive and Child Health program that have tended to function independently. To bring about a greater impact of the program there is a need to build synergies between these various packages since they
address different stages of the life cycle. The 'Continuum of Care' approach includes two dimensions – stages of life cycle and places where care is provided. This approach underpins the RMNCH+A strategy that seeks to provide an integrated set of interventions through a large cadre of community-based ASHAs and a three-tiered health system. The key components of the RMNCH+A interventions as a 'continuum of care' are given in Table 1. Immunization is one of the key
1elements in this strategy.
Table 1: RMNCH+A continuum of care across life cycle and different levels of healthcare
Reproductive care Newborn and childcarePregnancy and child birth care
• Comprehensive abortion care
• RTI/STI case management,• Postpartum IUCD and
sterilisation; interval IUCDprocedures
• Adolescent friendly health services
• Skilled obstetric care andimmediate newborn care and resuscitation
• Emergency obstetric care• Preventing Parent to Child
Transmission (PPTCT) of HIV
• Postpartum sterilisation
• Essential newborn care• Care of sick newborn (SNCU, NBSU)• Facility-based care of childhood illnesses (IMNCI)• Care of children with severe acute malnutrition
(NRC)• Immunisation
Cli
nic
al
• Family planning (including IUCD insert ion, OCP & condoms)
• Prevention and management of STIs
• Peri-conception Folic acid supplenentation
• Full antenatal care package
• PPTCT
• Early detection and management of illnesses in mother and newborn
• Immunisation
• First level assessment and care for newborn and childhood illnesses
• Immunisation• Micro-nutrient
supplementation
• Weekly IFA supplementation
• Information and counselling on sexual reproductive health and family planning
• Community based promotion and delivery of contraceptives
• Menstrual hygiene
• Counselling and preparation for newborn care, breast feeding, birth preparedness
• Demand generation for pregnancy care and institutional delivery (JSY,JSSK)
Antenatal care Postnatal careReproductive health care
• Home-based newborn care and prompt referral (HBNC scheme)
• Antibiotic for suspected case of newborn sepsis• Infant and Young Child Feeding (IYCF), including
exclusive breast feeding and complementary feeding,• Child health screening and early intervention services
(0-18 years)• Early childhood development• Danger sign recognition and care-seeking for illness• Use of ORS and Zinc in case of diarrhoea
Intersectoral: Water, sanitation, hygiene, nutrition, education, education, empowerment
Out
reac
h/S
ub c
entr
eF
am
ily &
Co
mm
un
ity
Child health care
1 A Strategic Approach to Reproductive, Maternal, Newborn, Child and Adolescent Health in India: For Healthy Mother and Child. MoHFW, Government of India, 2013.
Adolescence/ Pre-pregnancy Pregnancy Birth Newborn / postnatal Childhood
1
0 1................................

0 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Immunization is one of the most cost-effective interventions that prevent needless suffering through sickness, disability and death. The benefits of immunization are not restricted to improvement in health and life expectancy but also have social and economic impact at both community and national levels. Moreover, an effective, equitable immunization program and its impact on reducing the burden of vaccine-preventable diseases will greatly contribute to achieving the Millennium Development Goal 4 (MDG4) that envisages a two-third reduction in child mortality by 2015.
In the last three decades, India has made significant progress on sustainable and inclusive growth. There is now a greater sense of awareness and expectations from the people as the country makes further social and economic progress. Investments on the social determinants of health have improved availability and access to health services though there still remain challenges of inequity and affordability.
This multi-year strategic plan (2013–17) has evolved from its first iteration (cMYP 2005–10) and is underpinned by the Government of India RMNCH+A 2013 strategy and the National Vaccine Policy, 2011. The document mainly seeks to:
a. Provide a broad framework of objectives, expected results and strategies that cover the different aspects of Routine Immunization – program ser v ice de l iver y, sys tem strengthening, social mobilization and demand generation, newer vaccines and technology, epidemiology of vaccine-preventable diseases and management of adverse events following immunization.
b. Identify costing and financing requirement as part of the planning cycle.
c. Propose monitoring and accountability tracking mechanisms that should lead to improved program efficiency
d. Explore and expand opportunities to
1.2 Purpose of cMYP
integrate other maternal and child health interventions such as breast feeding, Vitamin A supplementation and ORS through UIP.
The strategic plan had been prepared through a close collaborative and iterative process involving national program managers, state o f f i c ia l s, p ro fess iona l assoc ia t ions, development partners and implementing agencies, which provide the goals, objectives, indicators, strategies and costs. As cMYP (2005–10) was completing its life in March 2010, a supplement to extend it till March 2012 was prepared. Initially, a framework for revised cMYP was agreed upon by a working group of national immunization program managers and development partners where attention was paid to new developments and initiatives that had taken place since 2005. These initiatives included those that have been enacted under the National Rural Health Mission (NRHM) and the recommendations of NTAGI in the recent years. Two regional consultations were held in New Delhi and Kolkata. These consultations were attended by senior officials in the Ministry of Health and Family Welfare (MoHFW), program managers from the national immunization division; state, district and block level immunization officials, and by representatives of development partners and other professional organizations and Non-Government Organizations.
In April 2013, under the guidance of national immunization division, ITSU facilitated the process of drafting the next cMYP (2013–17) and set up a core committee to draft the plan, comprising of representatives from ITSU, WHO and UNICEF. The members of the core committee met and communicated on a regular basis among themselves to continually refine the draft plan. Inputs on key objectives and strategies came through the national immunization division through regular meetings with the drafting team. The current cMYP document went through several iterations before it was sent to NTAGI for comments, which were subsequently
1.3 Planning process

................................
0 3 I N T R O D U C T I O N
to reducing approximately 25 percent to the 2reduction in child mortality.
WHO has identified priority areas in immunization for the future to sustain the
3momentum on immunization. These priorities, which are also reflected in the national cMYP, include the following:
lstrengthening the Routine Immunization program,
laccelerating measles control activities,
lintroducing newer vaccines through evidence-based policies,
lincreasing access to immunization services through system strengthening.
As the current set of MDGs reach their end in 2015, new global health paradigms will emerge that will focus on universal health coverage and sustainable development. A well-functioning UIP that aims to reach out to every child will contribute to universal health coverage and healthier future generation. To achieve this, UIP will need strong underpinning of good governance and accountability at all levels. This will necessarily lead to improved program efficiency and more children will get immunized.
incorporated. In addition to the main strategic component of cMYP, the core committee also worked on the detailed costing of the program under the guidance of national immunization division.
Accord ing to WHO, immuniza t ion interventions have proven to be a success across the globe and today reach out to over 100 million children and prevent 2.5 million deaths per year. As new global health paradigms emerge, fresh perspectives and priorities are emerging in immunization as well. Universal immunization coverage is an important element of universal health coverage to achieve the MDGs by 2015. Despite improved vaccination coverage there are rising inequities among different population groups that need to be addressed for a more meaningful success. There are at least ten new antigens now available that can be added to the traditional EPI interventions including vaccines against Hepatitis B, Rota virus, Japanese Encephalitis, and Human Papilloma Virus. Several countries are now moving beyond the traditional target population of infants and pregnant women to include adolescents and adults. WHO expects that by 2015 immunization should contribute
1.4 Global Priorities on immunization
2 WHO Strategic Plan 2010–15. Department of Immunization, Vaccines and Biologicals3 Global Action Vaccine Plan 2011–2020. World Health Organization
................................ 0 5
2.1 History of immunization program in India
The success of smallpox eradication in the 70s brought attention to the immunization program globally as well as in India. The Expanded Program on Immunization (EPI), a national policy of immunizing all children during the first year of life with DPT, OPV, BCG and typhoid–paratyphoid fever vaccines was launched in 1978. Immunization of pregnant mothers with TT vaccine was introduced in 1983. In 1985, the name of EPI was changed to the Universal Immunization Program (UIP) with activities phased in to the entire country by 1990. The stated objectives of UIP are:
lTo rapidly increase immunization coverage
lTo improve the quality of services
lTo establish a reliable cold chain system to the health facility level
lTo introduce a district-wise system for monitoring of performance
lTo achieve self-sufficiency in vaccine production
UIP was given the status of a one of the five 'National Technology Missions' in 1986. Subsequently in 1992, UIP became a part of Child Survival and Safe Motherhood (CSSM) program and then of Reproductive and Child Health (RCH) program in 1997. A specific Immunization Strengthening Project (ISP) was designed to run from 2000 to 2003, which included the following main components:
lpolio eradication
lstrengthening routine immunization
lstrategic framework for development.
Immunization is a critical component of the Government of India's child survival strategy. In 1997 the MoHFW launched a Reproductive and Child Health (RCH) program to reduce IMR, MMR, TFR and to increase immunization coverage, especially in rural areas. The second phase of the RCH program (2005–10) focused on minimizing regional variations through provision of assured, equitable, and responsive quality services. With a view to strengthen public health system in rural areas, the Government of India launched the National Rural Health Mission in 2005. The NRHM was established as a single platform to bring together all of the national
4health efforts, including RCH. The goal of the NRHM is to address gaps in the provision of effective health care to rural population with a special focus on 18 states, which have weak
5public health infrastructure. To achieve this goal the NRHM envisions a shift away from the vertical health and family welfare programs to a new architecture in which societies under different programs are merged and resources pooled at the district level. NRHM also provides states with flexibility in making their own plans in delivering RI interventions. It also seeks to strengthen local public health provision with infrastructure and manpower and facilitate the participation of the not-for-profit and for-profit sectors in achieving
2.2 National Rural Health Mission (NRHM)
National Context
2
4Ministry of Health and Family Welfare (2005): “National Rural Health Mission, Framework for Implementation (2005-12)”
5The 18 states are Arunachal Pradesh, Assam, Bihar, Chhattisgarh, Himachal Pradesh, Jharkhand, Jammu & Kashmir, Manipur, Mizoram, Meghalaya, Madhya Pradesh, Nagaland, Odisha, Rajasthan, Sikkim, Tripura, Uttaranchal and Uttar Pradesh.

0 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
desirable health outcomes. In the 12th FYP the Government of India has proposed a National Health Mission for improving healthcare in rural as well as urban areas. UIP is an integral component of NRHM.
At the national level, the NRHM has a Mission Steering Group (MSG) headed by the Union Minister for Health & Family Welfare and an Empowered Program Committee (EPC) headed by the Union Secretary for Health & Family Welfare. EPC implements the Mission
6under the overall guidance of the MSG.
At the state level, the mission functions under the overall guidance of the State Health Mission headed by the Chief Minister of the
6 Source: www.nrhm.gov.in
state and provides oversight to the functioning of the health system and NRHM activities, policy inputs for health sector, conducts intersectoral coordination and advocacy. The functions under the mission are carried out through the State Health & Family Welfare Society led by the Mission Director. Under NRHM, states have set up State Health Societies to strengthen health service delivery infrastructure, financial management, coordination with NGOs/CSOs/donors and monitoring of various national programs.
The State Mission and State Society are interlinked in terms of a common secretariat as shown in Figure 1 below.
Figure 1: Composite organogram of the State Mission and the State Society
State Health Mission
Governing Body, State Health Society
Program Committees(Headed by Director/
Director General)(Optional)
SPMSU(Headed by Executive
Director/Mission Director)
Executive Committee, State Health Society
2.3 Burden of vaccine-preventable diseases (VPDs)
Over the past 20 years, the reported cases of the main VPDshave declined. However, in recent yearsthere has been an increasing trend in the number of reported measles, diphtheria and pertussis cases as shown in Figure 2. This increasing trend may be due to an actual
increase in number of cases or can be attributed to improvements in case detection and the overall surveillance system strengthening. To minimize this inconsistency and to stabilize the reporting trends, improving the surveillance of VPDs in the countryis urgently needed.It is estimated that approximately 80,000 children die annually from measles and associated complications. Although this figure has

................................
07 N A T I O N A L C O N T E X T
MCV2 six months following the completion of the campaign. Delhi, Sikkim, Goa and Puducherry took initiative themselves and introduced 2nd measles dose through MMR.In September 2013, India committed to eliminating measles and controll ing rubella/congenital rubella syndrome (CRS) by 2020 as part of the resolution that was approved by SEARO's 66th regional committee.
decreased over the years with improvements in routine vaccination coverage rates, measles mortality still remains high. In 2010, the Government of India decided to introduce a second dose of measles containing vaccine (MCV2) in UIP. In 21 states with measles 1st dose coverage more than 80 percent, MCV2 was introduced directly in their routine immunization whereas, 14 states were taken up for measles Supplementary Immunization Activity (SIA) followed by introduction of
Figure 2: Trends in the reported cases of Measles and Pertussis from 1990–2010 (Source CBHI)
120000
100000
80000
60000
40000
20000
0
19
90
19
91
19
92
19
93
19
94
19
95
19
96
19
97
19
98
19
99
20
00
20
01
20
02
20
03
20
04
20
05
20
06
20
07
20
08
20
09
20
10
Ca
se
s
PertusslsMeasles
Burden of VPDs
between geographies and population groups. These inequities represent gaps in service delivery that leaves certain groups of children at a high risk of remaining unvaccinated. As per NHFS-3 data, nine states are below the national average for vaccination coverage including Madhya Pradesh, Uttar Pradesh, Bihar and Jharkhand. Even within states there exists a difference in total coverage between
7different districts as shown in Figure 4.
2.4 Status of vaccine coverage
Though the reported vaccination coverage for all vaccines has always been higher than evaluated coverage, the average vaccination coverage has shown a consistent increase over the last two decades as shown in Figure 3 below.
However these averages mask the disparities
7 NFHS-3 data

0 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
2.4.1 Vaccine coverage and equity issues
While vaccines under UIP are provided free of cost through all the public health facilities across the countries, disparities in coverage exist for different population groups that need to be addressed. There are significant inequities in vaccination coverage in different states based on various factors related to individual (gender, birth order), family (area of residence, wealth,parental education), demography
(religion, caste) and the society (access to health care, community literacy level)
8characteristics.
There is a clear gender coverage differential as reported by different surveys. Boys generally have a higher vaccination coverage than girls as reported by most surveys conducted across the country (Figure 5).
The gap between genders also exists for individual vaccines such as BCG, DPT and measles.
Figure 3: Trends in vaccination coverage over the last twenty years as shown in different surveys
Figure 4: District level coverage of fully immunized children between 12 and 23 months of age. (Source: DLHS 2007–08)
Vaccine coverage70.0%
60.0%
50.0%
40.0%
30.0%
20.0%
10.0%
0.0%
NFHS-1(1992-93)
NFHS-2(1998-99)
NFHS-3(2005-06)
DLHS-1(1998-99)
DLHS-2(2002-04)
DLHS-3(2007-08)
CES(2009-10)
35.4%
42.0% 43.5%
54.2%
45.9%
53.5%
61.4%
Below 30
30 to 50
50 to 70
70 to 90
Above 90
8Joseph L Mathew (2012): “Inequity in Childhood Immunization in India: A Systematic Review,” Indian Pediatrics, Volume 69, March 16, 2012.
................................
0 9
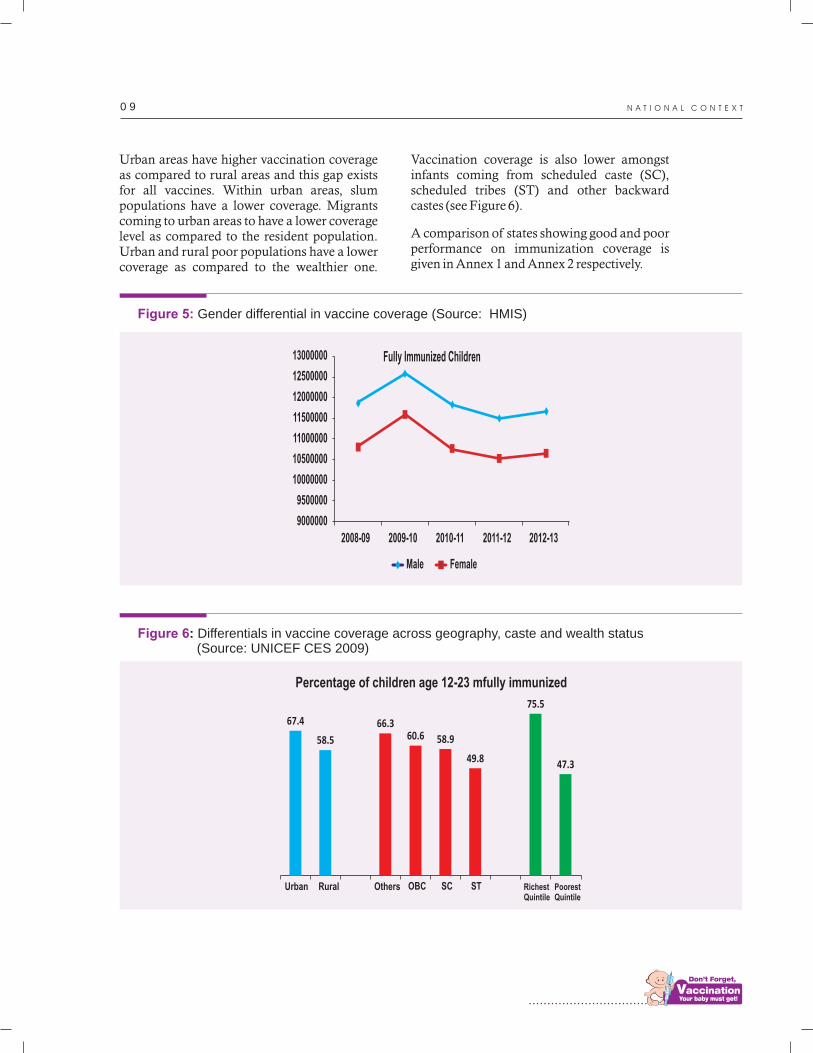
Urban areas have higher vaccination coverage as compared to rural areas and this gap exists for all vaccines. Within urban areas, slum populations have a lower coverage. Migrants coming to urban areas to have a lower coverage level as compared to the resident population. Urban and rural poor populations have a lower coverage as compared to the wealthier one.
Figure 5: Gender differential in vaccine coverage (Source: HMIS)
13000000
12500000
12000000
11500000
11000000
10500000
10000000
9500000
9000000
2008-09 2009-10 2010-11 2011-12 2012-13
Male Female
Fully Immunized Children
Figure 6: Differentials in vaccine coverage across geography, caste and wealth status (Source: UNICEF CES 2009)
Percentage of children age 12-23 mfully immunized
Urban Rural Others OBC SC ST RichestQuintile
PoorestQuintile
67.4
58.5
66.360.6 58.9
49.8 47.3
75.5
Vaccination coverage is also lower amongst infants coming from scheduled caste (SC), scheduled tribes (ST) and other backward castes (see Figure 6).
A comparison of states showing good and poor performance on immunization coverage is given in Annex 1 and Annex 2 respectively.
N A T I O N A L C O N T E X T

1 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
2.5 Current structure for immunization service delivery in the country
The implementation of the UIP is a joint responsibility of government at all levels, namely Central, State and Union Territory Districts and Sub-Districts. The relationships between central and state immunization departments and between state and district immunization officers are critical for efficient and effective service delivery.
National: The MoHFW comprises of four departments, each of which is led by a Secretary to the Government of India. These include:
lDepartment of Health & Family Welfare;
lDepartment of Ayurveda, Yoga & Naturopathy, Unani , S iddha and Homoeopathy;
lDepartment of Health Research; and
lDepartment of AIDS Control.
The MoHFW is responsible for implementing various national health programs in all states of India. The Directorate General of Health Services renders technical advice on all medical and public health matters and is involved in the monitoring of implementation of various health services. The MoHFW is responsible for funding of various national programs including immunization program, providing technical assistance and policy guidance to the states, and for monitoring and evaluation. Funding for extra staff and other health system resources at the state level is provided by the NRHM, a flexible mechanism that allows for integration of funds for all the national schemes while allowing for states to flexibly allocate funds for system improvement in a manner that is consistent with their needs and challenges. All states are required to submit in advance a Program Implementation Plan (PIP) for a financial year, along with complete projections of funds required to implement the PIP.
To augment technical and managerial support under UIP for strengthening, revitalization and successful implementation of RI, the
Immunization Division at MoHFW has set up an Immunization Technical Support Unit (ITSU). The ITSU is staffed with technical officers to support various functions of UIP under six different pillars:
lStrategic planning and system design,
lMonitoring and evaluation,
lVaccine logis t ics and cold chain management,
lAdverse events following immunization (AEFI) management and vaccine quality and safety,
lTranslation of evidence to policy, and
lStrategic communication.
Through ITSU,the ministry will facilitate to harmonize various initiatives being piloted or implemented in different states by all immunization partners and provide a single platform for discussions, development of strategies and coordination with partners for scaling up the successful models.
State: At the state level, the Secretary of Health is responsible for all health-related efforts. The State Department of Health and Family Welfare is led by a Director of Health Services under which the State Directorate of Health Services serves as the technical wing. Large states such as Bihar, Madhya Pradesh, Uttar Pradesh, Andhra Pradesh, and Karnataka have additional zonal or regional or divisions set-up between the State Directorate of Health S e r v i c e s a n d t h e D i s t r i c t H e a l t h Administration. Most of the states have a dedicated State EPI Officer; however, at places Deputy Director-HFW has additional responsibility of being EPI Officer. Additional support for UIP at the state level is provided by a cold chain officer and by data and administrative support staff. State governments are responsible for implementation and supervision of the various programs and for provision of relevant infrastructure and curative services in the states including village outreach sessions for immunization.
District: In the district, under the overall supervision of Chief Medical and Health Officer (CMHO) or Civil Surgeon (CS), the District Immunization Officer (DIO)

................................
1 1
coordinates all the immunization-related efforts. The responsibility for immunization also lies with Block Medical Officers and PHC Medical Officers. The Auxiliary Nurse Midwife (ANM) delivers the immunization services to the community.
Immunization services are provided through the following:
lsub-centers, primary health centers, and community health centers,
lsub-divisional/taluk/speciality hospitals,
ltertiary hospitals,
lurban health services provided by municipalities,
lhospitals and dispensaries run by railways, defense, and public sector undertakings,
lEmployees’ State Insurance Scheme hospitals
ldispensaries funded by the government (State and Centre).
Private health sector also provides an estimated 15–20 percent of immunization services.
The Indian Public Health Standards (IPHS) for immunization has been drafted to improve the quality of the service and NRHM supports efforts to improve the quality of service by strengthening sub-centers and primary health centers. The funding mechanism for immunization has also been simplified and made flexible along with adoption of the bottom-up planning approach through district and state Project Implementation Plans (PIPs). Immunization service delivery in many areas within a district, i.e. urban areas, especially slums and peri-urban areas, where migrant families live; areas in semi-legal situations due to weak infrastructure; areas which are managed by different local bodies such as railways and cantonment have been, and are still, a major concern.
Civil Society Civil Society Organizations (CSOs): These organizations offer a wide range of experience and knowledge essential for UIP. They can provide insight into gaps in
2.5.1 Other stakeholders
9Howard D, Roy K. Private care and public health: do vaccination and prenatal care rates differ between users of private vs. public sector care in India? Health Services Research 2004;49:2013-26
health service delivery and identify practical and political challenges that must be overcome to improve the health of citizens. CSOs therefore play a crucial role to advocate for policy changes, generate greater transparency and hold governments and other healthcare stakeholders to account. At the country level, Civil Society encompasses a diverse array of actors, including the following:
lpatient groups, health workers, medical or health unions and associations,
lfaith-based organizations,
lnon-governmental organizations,
lcommunity-based organizations,
lacademic institutions,
lmedia,
ladvocacy groups,
lmigrants, women, youth and other neglected or vulnerable groups.
Civil society groups of particular importance to ensuring that UIP achieves its intended results are those with expertise in maternal health, child health, immunizations, nutrition, health systems and services, monitoring and evaluation. The MOHFW will engage more proactively with academia, professional societies, and other national agencies and committees and networks like the development partners forum to ensure a cohesive and coordinated approach to achieving national immunization priorities.
Private hospitals and clinics: Private health sector plays an important role in providing immunization services and fill gaps in delivery of RI services through public system. Studies in India have shown that private sector does enable increased access to traditional EPI
9vaccines for those who can afford to pay. Private sector also plays a role in introducing newer and underutilized vaccines prior to their induction in the public program. Private sector also has a key role to play in supporting the surveillance system for vaccine-preventable diseases and adverse events following immunization by reporting cases that may have been missed out by the public surveillance system.
N A T I O N A L C O N T E X T

1 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
2.5.2 Current UIP Schedule in India
The current UIP vaccination schedule caters to
pregnant women, infants, children and adolescents as shown in Table 2 below.
Table 2: Vaccination schedule under UIP in India
*Give TT-2 or Booster doses before 36 weeks of pregnancy. However, give these even if more than 36 weeks have passed. Give TT to a woman in labor, if she has not previously received TT.
**Pentavalent vaccines contain a combination of DPT, HepB and HiB. In the states where it has been introduced, it will replace DPT 1,2& 3 and Hepatitis B 1, 2 & 3. Hepatitis B birth dose and booster doses of DPT will continue as before.
*** JE Vaccine (SA 14-14-2) is given in select endemic districts, after the campaign is over in that district.
****The 2nd to 9th doses of Vitamin A can be administered to children 1-5 years old during biannual rounds, in collaboration with ICDS.
Vaccine When to give Dose Route Site
0.5 ml
0.5 ml
0.5 ml
0.1ml(0.05ml until 1 month of age)
0.5 ml
2 drops
2 drops
0.5 ml
0.5 ml
0.5 ml
0.5 ml
0.5 ml
0.5 ml
2 drops
0.5 ml
0.5 ml
0.5 ml.
0.5 ml
Intra-muscular
Intra-muscular
Intra-muscular
Intra-dermal
Intra-muscular
Oral
Oral
Intra-muscular
Intra-muscular
Intra-muscular
Sub-cutaneous
Sub-cutaneous
Intra-muscular
Oral
Sub-cutaneous
Sub-cutaneous
Intra-muscular
Intra-muscular
Early in pregnancy
4 weeks after TT-1*
If received 2 TT doses in apregnancy within the last 3 years
At birth or as early as possible tillone year of age
At birth or as early as possible within 24 hours
At birth or as early as possible within the first 15 days
At 6 weeks, 10 weeks & 14 weeks
9 completed months-12 months.(give up to 5 years if not received at 9-12 months age)
9 completed months
16-24 months
16-24 months
16-24 Months
16-24 months with DPT/OPVbooster
5-6 years
10 years & 16 years
Upper Arm
Upper Arm
Upper Arm
Left Upper Arm
Antero-lateral side of mid-thigh
Oral
Oral
Antero-lateral side of mid-thigh
Antero-lateral side of mid-thigh
Antero-lateral side of mid-thigh
Right upper Arm
Left Upper Arm
Antero-lateral side of mid-thigh
Oral
Right upper Arm
Left Upper Arm
Upper Arm
Upper Arm
For Pregnant Women
TT-1
TT-2
TT- Booster
BCG
Hepatitis BBirth dose
OPV Zero dose
OPV 1,2 & 3
DPT1,2 & 3
Hepatitis B 1,2 & 3
Hi BcontainingPentavalent 1, 2 & 3**
stMeasles 1 dose
stJE 1 dose***
stDPT 1 booster
OPV Booster
Measles 2nd dose
ndJE 2 dose
DPT nd2 Booster
TT
Vitamin A****
For Infants
For Children and Adolescents
................................
1 3
2.6 UIP successes as a child survival strategy
The Universal Immunization Program (UIP) in India is one of the largest of its kind in the world, in terms of the following:
lquantity of vaccines used,
lnumber of beneficiaries reached out to,
lnumber of immunization sessions organized,
lthe geographical spread and diversity of areas covered.
It caters to nearly 27 million infants and 30 million pregnant women annually free of cost. There is a strong political commitment for achieving universal immunization coverage in the country along with the eradication and elimination of the targeted diseases.
As a key element of the national child survival strategy, UIP has contributed significantly to reducing mortality and morbidity due to vaccine-preventable diseases and the infant mortality rate over the last decade. While surveillance information for specific VPDs is limited, the steady fall of IMR from 123 to 50 deaths per 1000 live-births does in part reflect
10the impact of the UIP.
Since its launch in 1995, the Pulse Polio campaign aimed at eradicating polio from India, has begun to show results. Governments at the national and state levels are implementing strategies on a scale and intensity that is unprecedented in the history of polio eradication. These efforts have brought India closer to the goal of polio eradication and there is currently no reported case since
11January 2011. India has been declared polio non-endemic country by World Health Organization in early 2012. Neonatal Tetanus cases have declined significantly as more pregnant women received TT vaccine as part of their ante-natal care. There has been an overall reduction in the number of cases and deaths due to diphtheria, pertussis and measles as well.
Under National Rural Health Mission, MoHFW has undertaken many initiatives to improve health systems and immunization outcomes. Districts have been provided with more human as well as financial resources to improve delivery of immunization and other health services. Introduction of ASHA into the system as a community link worker has brought about a major improvement in community mobilization. Districts have strengthened their delivery systems and developed micro-plans for improved efficiency. The number of vaccine delivery points has increased along with the cold chain points. MoHFW also introduced a system for Alternate Vaccine Delivery (AVD) to provide vaccines at the outreach session sites. Innovative technology like auto-disable syringes are now in use in all states and union territories. Immunization-related trainings have led to an increased capacity of frontline health workers to deliver vaccines at the village level. Focus in the urban areas has led to an improved immunization services in slums areas, though more needs to be done in this
12area. MoHFW has also initiated Mother and Child Tracking System (MCTS) to enable the entry of mother and child data into a central database.
The year 2012–13 was declared by the Government of India as the year of Intensification of RI in India. In this context, the MoHFW had put in place a few strategic actions to improve immunization coverage. These included
limproving health systems,
lpromoting village health and nutrition day (VHND),
llaunching Immunization Weeks,
llaunching of the “Teeka Express” for delivery of vaccines to outreach sessions,
lpilot-launching of the National Cold Chain Management In for mat ion Sys tem (NCCMIS) for real-time monitoring and management of cold chain systems and
lsetting up of the Immunization Technical
10SRS 201111National Polio Surveillance Program. www.npspindia.org.12UIP Review 2004
N A T I O N A L C O N T E X T
1 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Support Unit (ITSU) to provide technical and programmatic support for successful implementation of the UIP.
India's 'Call to Action on Child Survival and Development' announced in February 2013, and led by the MoHFW, the Government of India, calls for a concerted, convergent and inter-sectorial approach to achieving the country's child survival goals by 2017. Based on composite indicators the Government of India has identified strengthening efforts in the 184 high priority districts in the country. This five-year ambitious target will heighten the importance of 'continuum of care', ensuring the tight linkage between maternal and newborn health as outlined in the new strategic
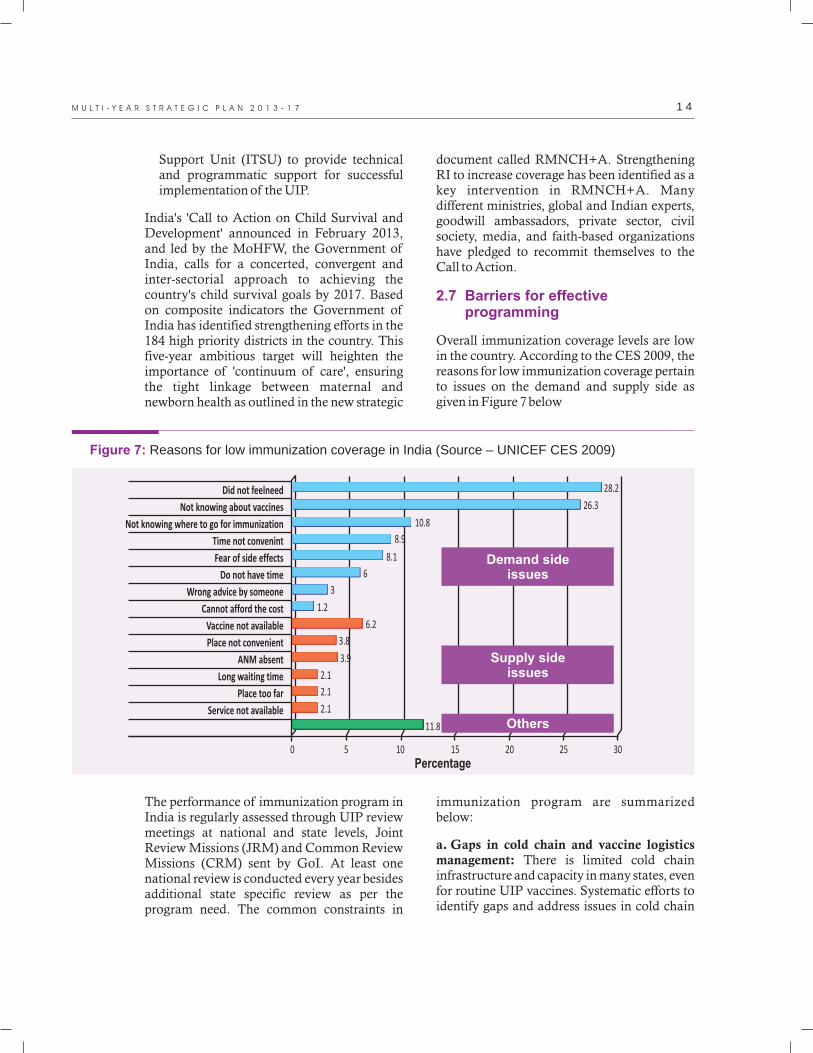
Figure 7: Reasons for low immunization coverage in India (Source – UNICEF CES 2009)
Did not feelneed
Not knowing about vaccines
Not knowing where to go for immunization
Time not convenint
Fear of side effects
Do not have time
Wrong advice by someone
Cannot afford the cost
Vaccine not available
Place not convenient
ANM absent
Long waiting time
Place too far
Service not available
28.2
26.3
10.8
8.9
8.1
6
3
1.2
6.2
3.8
3.9
2.1
2.1
2.1
11.8
0 5 10 15 20 25 30Percentage
Demand sideissues
Supply sideissues
Others
The performance of immunization program in India is regularly assessed through UIP review meetings at national and state levels, Joint Review Missions (JRM) and Common Review Missions (CRM) sent by GoI. At least one national review is conducted every year besides additional state specific review as per the program need. The common constraints in
immunization program are summarized below:
a. Gaps in cold chain and vaccine logistics management: There is limited cold chain infrastructure and capacity in many states, even for routine UIP vaccines. Systematic efforts to identify gaps and address issues in cold chain
document called RMNCH+A. Strengthening RI to increase coverage has been identified as a key intervention in RMNCH+A. Many different ministries, global and Indian experts, goodwill ambassadors, private sector, civil society, media, and faith-based organizations have pledged to recommit themselves to the Call to Action.
Overall immunization coverage levels are low in the country. According to the CES 2009, the reasons for low immunization coverage pertain to issues on the demand and supply side as given in Figure 7 below
2.7 Barriers for effective programming

................................
1 5
and VLM have been conducted in recent years. In addition to the 2008 NCCA, a number of vaccine and cold chain management a s s e s s m e n t s ( Va c c i n e M a n a ge m e n t Assessment Tool (VMAT)/EVM assessments) have been conducted in 10 states and one national UIP store (Government Medical Store
13Depots (GMSD) – Karnal) between 2007–11. A recent national-level assessment of EVM conducted by the Government of India and UNICEF in 10 states and four GMSDs along with other studies including deep dive and KPMG exercises by ITSU have identified the following constraints:
lInfrastructure issues include poor infrastructure of vaccine stores and transportation systems; a lack of standards for vaccine stores at different levels and insufficient temperature monitoring system at all vaccine storage points from GMSDs to last cold chain point level, state, and regional stores. There exist difficulties in procuring the right quality of cold chain equipment on time with adequate after-sale support. There is a paucity of repair kits and spares cold chain technicians and inequitable cold chain point (last vaccine storage site) distribution. Cold chain equipment in many states in the country is old and in many cases broken. There is also a paucity of available data on Vaccine Logistics and Cold Chain to devise national plans and strategies to address them. .
lHR issues such as lack of a CCL support unit with experts on cold chain for both the immunization division of MoHFW and at the state level; lack of induction training and a regular educational program for staff inducted in the Vaccine Logistics and Cold Chain system; insufficient institutional training capacity to manage cold chain and logistics at all levels; shortage of trained manpower and relevant job-aids for managing cold chain at all levels (state, division/regional and district levels); and lack of HR with capacity for Vaccine Logistics Management (VLM) at all levels (national, GMSDs, state, district and PHCs). The shortage of HR is more acute in
the poor performing states and specifically at the field level.
lMonitoring and MIS issues such as lack of realtime vaccine stock status, consumption patterns, wastage rates, along with a continuous temperature monitoring system for cold chain, lack of cold chain inventory and real-time NCCMIS, no regular review of CCL system at the state and district level, and poor documentation and MIS for vaccine management (standardized registers, records and procedures).
lVaccine procurement issues are significant as delay in placement of procurement orders and irregular supply of vaccines have a direct impact on vaccine availability affecting immunization coverage. Moreover, certified vaccine suppliers are few, and since orders are always given to the lowest bidder, the supply of vaccines is often erratic.
These constraints have led to high breakdown rate of equipment, overstocking and stock-outs, inadequate monitoring and supervision, poor management, and the possibility of AEFIs, thus hampering improved vaccine coverage.
b. Poor social mobilization: Low levels of awareness, communication and information-sharing amongst frontline workers as well as poor HR capacity for BCC in government institutions as a whole contributes to the problem of high left-outs and dropouts. Studies have shown that insufficient and ineffective health communication along with lack of promotion or follow-up of RIs are two of the main health system constrains behind low coverage in immunization, preventing parents from initiating or following through with their child's vaccination schedule. Given that the actual rate of immunization is low, the high dropout rate reduces the number of fully immunized children in the country. Poor populations and those with lower levels of education are most vulnerable to impacts of low levels of advocacy and communication. Listed below are some of the system-related constraints in advocacy and communication
13 National Cold Chain Assessment, India. July 2008. NRHM & UNICEF
N A T I O N A L C O N T E X T
1 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
inception of UIP, India has set up a reporting mechanism from the health center to national level. In last few years, the country has also introduced electronic data systems like HMIS and MCTS to improve reporting, analysis, monitoring and planning at all levels. However, there are big gaps in quality of data being reported, its analysis and use for decision making and thus leading to inadequate information to support NTAGI and UIP to design and implement strategies to improve immunization quality and coverage. Some of the main constraints in the area of data management and evidence generation are listed below:
lPoor monitoring and evaluation for data entry, resulting in errors in data entry and inaccurate data. In recent years, partners' support and networks have contributed to increased monitoring and supportive supervision with visible positive impact in select states. However, there is a need to build the capacity of government officials and strengthen the system to improve monitoring and supervision by government officials.
lPoor monitoring and evaluation results in insufficient data quality and reporting rates. A vast majority of states have wide gaps in reported and evaluated coverage data. The factors for this variation need to be identified through regular data quality audits and necessary corrective measures should be taken.
lInadequate surveillance data quality and reporting rates result in poor surveillance of VPDs and AEFIs. While some attention has been paid to s t rengthening VPD surveillance, systemic deficiencies and bottlenecks such as insufficient laboratory capacity and limited trained manpower at the district levels to carry out surveillance, continue to exist. Inadequate VPDs reporting results in the inability of UIP to measure disease burden to make a decision on the introduction of new antigens and impact of vaccination on the disease. There is a felt need for HR capacity building in
that lead to low levels of immunization coverage.
lThere is weak capacity at the state level and inadequate HR to generate evidence-based communication strategies and effective BCC campaigns
lWe a k c o m mu n i c a t i o n c a p a c i t i e s (spokesperson system) within the government machinery at national and state levels in handling AEFIs.
lInformation dissemination is not timely and often mixed messages are received by beneficiaries
lWeak counseling and interpersonal communication (IPC) skills among health workers and community mobilizers, which adversely affects dissemination of communication of messages.
lWeak capacities and counseling skills of service providers to ensure delivery of quality care, especially in hard-to-reach areas.
There is an urgent need to strategically approach communication, aiming at behavior change both at the service delivery level and at the community level to generate demand among the caregivers. Meeting the shortfall of health professionals and building their counseling and communication skills are imperative to a sustained and holistic response to the public health concerns in the country. This requires health care to be addressed not only from the scientific perspective of what works, but also from the social and behavioral perspective of who needs it the most. One also needs to understand the social norms and barriers that prevent them from accessing the services and how to reach the unreached.
c. Poor data management and analysis for evidence generation: A robust system for data management and evidence generation is crucial to support informed decision making for the creation of realistic goals and strategies for improvement of current coverage levels and introduction of new antigens in UIP. Since the

................................
1 7
VPD surveillance, strengthening laboratory capacity by improving infrastructure and making reagents available, and building system for timely reporting and actions. Similarly surveillance of AEFI cases is poor and a structured response to reported serious cases of AEFI is lacking.
lLimited focus on operational research for immunization and finding locally suitable solutions. Good quality research is needed to provide an evidence base for a more informed decision making and improving performance.
The successful implementation of HMIS under NRHM and MCTS under Mission Mode Project provides a great opportunity to strengthen data management and evidence generation to inform decision making in UIP. With the augmentation of human resource at national level also provides an opportunity for coordination between various reporting and surveillance systems in the country as well as putting up a system for using information for decision making.
d. Weak human resource capacity: In a study of HR needs assessment in UIP by Mavlankar
14 et al (IIM Ahmedabad) the following was found:
lThere is limited technical and operational human resource capacity and quality at various levels in UIP.
lImmunization cells at both the state and the national level are small and inadequately staffed.
lKey personnel capacities are spread thin across multiple areas in day-to-day management with no focus on priorities. They are not able to focus on developing strategic solutions and to organize and coordinate activities such as introducing new vaccines, updating technology, applying for international funding and support, writing reports and analyzing data.
lThe roles and responsibilities of officials at the state immunization cells are not well defined
lState immunization officials have no financial powers and their titles are not commensurate with their responsibilities.
The lack of human resource capacity and poorly defined roles and responsibilities at various levels have a cascading effect on all other areas of program performance, including monitoring and evaluation, supply chain and logist ics management, and strategic communications. Lower quality of monitoring and supportive supervision of the program leads to reduced efficiency and effectiveness of interventions at all levels of programming and needs to be addressed seriously.
While UIP is a part of a wider RMNCH+A strategy of the government, there is a need to increase the HR capacity and numbers of immunization managers at all levels. The Government of India has set up an Immunization Technical Support Unit (ITSU) to augment human resource capacity at national level with focal persons assigned for specific functions such as cold chain and vaccine logistics, Evidence to Policy and surveillance, Strategic Communication, Monitoring and Evaluation and Adverse Events Following Immunization (AEFI). Training immunization staff on relevant topics will improve program efficiency and effectiveness as well.
e. Need for a well delineated accountability systems: A major problem is the lack of institutionalized and uniform accountability structures, focused on performance review at each administrative level i.e. central, state and district levels. The country has a Multi-Year Strategic Plan for UIP but its implementation is not monitored in absence of a monitoring and accountability structure. Though, there are review mechanisms in place at all levels, but these are not followed consistently. Moreover, in absence of a robust system for data analysis,
N A T I O N A L C O N T E X T
14Universal Immunization Program in India: A Study on HR Needs Assessment at National and State Levels. Dr D.V Mavalankar et al, IIM Ahmedabad. Study commissioned by HRD Committee on UIP constituted by GoI.

1 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
interventions and follow up, these are not very effective.
f. Evidence synthesis for informed policy making: The NTAGI was formed in 2001 and tasked with advising the MoHFW on issues related to the program, policy and implementation of the national immunization program. Since its inception the NTAGI has r e c o m m e n d e d e v i d e n c e - b a s e d recommendations to the UIP, such as the following:
lintroduction of the Hepatitis B, Pentavalent and Japanese Encephalitis vaccine
luse of VVM in government vaccine supplies
luse of AD syringes
However, there is great scope for revision and improvement in the decision-making process for the introduction of new vaccines in the UIP. In the light of the current advancements in the field and the availability of several new interventions, it is imperative to establish scientific evidence-based protocols for making immunization related decisions.
As India considers adding new antigens (e.g., rotavirus, pneumococcal, MMR, HPV, IPV/hexavalent, cholera, typhoid, and JE) as well as new immunization technologies (e.g., updated injection safety devices), the immunization program also needs to keep pace. NTAGI is an advisory body with clear terms of reference for overall guidance but not day-to-day operations. NTAGI needs a well-defined secretariat to conduct regular meetings and a clear scope of work that maintains focus on making a structured recommendation on immunization. At the same time, there is an ever increasing need to develop capacity to identify and address critical gaps in evidence base. The health system must be able to evaluate new vaccines for safety, efficacy, relevance and cost-effectiveness; accommodate
the new vaccines in its cold chain management system and vaccine logistics; assess and respond in real time to roll-out challenges; and conduct post-marketing surveillance to ensure that lessons learnt from the roll-out are incorporated back into the system.
The services provided through the UIP shall be guided by the following principles
1. Universal immunization coverage: Sustaining demand and ensuring that all pregnant mothers, children and adolescents are immunized as per national schedule in line with the principles of universal health coverage.
2. Equitable access: Ensuring that the immunizations services reach out to the under-served, needy and most vulnerable populations while addressing regional inequalities across states.
3. High quality services and innovation: Maintaining highest possible quality in vaccine
Guiding Principles of UIP
................................ 1 9
3
procurement, storage, distribution and delivery services in an innovative and safe manner.
4. Sustainability and Partnerships: Committing resources, financial, human and technical, that sustain immunization benefits to the people at all times and promoting partnerships across different sectors and organizations build synergies and expand the overall coverage of the program.
5. Governance: Decentralized planning through a bottoms up approach to improve operational efficiency
6. M a n a g e m e n t e xc e l l e n c e a n d accountability: Implementation, oversight and accountability of interventions that optimize efficient use of resources

This comprehensive multi-year strategy plan seizes on the opportunity to address geographic and social inequities in immunization coverage rates, and other immunization-related issues highlighted in earlier sections. The plan aims to strengthen immunization infrastructure within the broader RCH program and offer a platform for integrating other primary care interventions and strengthening the public health system at all levels. UIP offers universal immunization coverage to all children in the country as per the national immunization schedule.
This plan derives its essence from the National Vaccine Policy 2011 and is underpinned by the goals ascribed in the National Health Policy 2002 and National Rural Health Mission 2005. The plan framework consists of an overarching Goal and a set of six Key Objectives (KO) that
4.1 UIP strategic plan framework
Box 1: UIP Goal and Key Objectives
GOAL
KEY OBJECTIVES
Reduce mortality and morbidity due to vaccine-preventable diseases through high quality immunization services
KO 1: Improve program service delivery for equitable and efficient immunization services by all districts
KO 2: Increase demand and reduce barriers for people to access immunization services through improved advocacy at all levels and social mobilization
KO 3: Strengthen and maintain robust surveillance system for vaccine-preventable diseases (VPDs) and adverse events following immunization (AEFI)
Introduce and expand the use of new and underutilized vaccines and technology in UIP
KO 5: Strengthen health system for immunization program
KO 6: Contribute to global polio eradication, measles, maternal and neonatal tetanus elimination
KO 4:
................................ 2 1
4
cover different aspects of the immunization program including - operational efficiency, epidemiological support, health system strengthening and demand generation(See Box 1). These Key Objectives are interlinked and mutually reinforce each other, thus providing greater focus, structure and flexibility for developing context-specific strategies and interventions. Each Key Objective has a set of Expected Results to be achieved in the medium term and a set of actionable strategies that can be contextualized in the State and District implementation plans. The framework elements are designed to be simple, feasible, flexible and relevant to the needs of the people. As part of providing better governance for the program, the UIP strategic plan has a comprehensive monitoring and accountability tracking framework which consists of a key indicators, targets, source of information, assigned responsibility and information dissemination.
UIP Strategic Plan: 2013-17

2 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
4.2 Impact indicators
4.3 Target population
KEY OBJECTIVE 1: Improve program service delivery for equitable and efficient immunization services by all districts
1. Reduction in infant mortality rate
2. Reduction in cases of vaccine-preventable diseases
RI interventions will be targeted at reaching out to all eligible children and pregnant women as per the national schedule. Given the equity issues, special efforts will be made to ensure that immunization services reach out to targeted beneficiaries belonging to the lower socio-economic strata, those living in urban slums, rural areas, tribal and other hard-to-reach areas.
The following section elaborates on the strategic framework further
Vaccine logistics management is one of the critical elements in the immunization program to ensure that all vaccines are available at the last cold chain point for immunization sessions. Similarly, a reliable and adequate cold chain network is essential to ensure that vaccines are stored within the recommended temperature ranges, and safe and potent vaccines are delivered to children. Various recent studies like Effective Vaccine Management (EVM 2013), Vaccine Wastage Study (2008), ITSU deep dive study, KPMG vaccine logistics study (2013), ICMR Freezing Study etc. have pointed out issues related to the existing vaccine logistics system up to the last cold chain point, and the capacity, functionality and maintenance of cold chain equipment at all levels.
Key Performance Indicators (KPI)
1. Number of States/UTs where > 95% sessions were held as planned
2.%of d i s t r ic t s having > 80% fu l l
immunization coverage
3. Number of States/UTs having less than 10% dropout from DPT1-DPT3 (or Pentavalent)
The indicators will disaggregated by gender, geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 1.1: Strengthen the national cold chain management system:
Maintaining a strong cold chain system is critical for maximizing the operational efficiency of UIP. Strategies to achieve this will focus on capacity building, hardware management and innovative technology.
Strategies
A national plan for cold chain management is essential for improving overall UIP program efficiency. The national cold chain plan shall be based on various situation analyses on cold chain and vaccine logistics management in the country. The major components of the plan will include:
a) National Standards:
One of the major gaps in cold chain management is the absence of standards performance parameters. The national cold chain plan will include standards for the following:
lVaccine storage at all levels as per WHO standards
lCold Chain point expansion guidelines
lCold Chain equipment plan for different levels of vaccine stores
lQuality maintenance of vaccines
lTemperature monitoring of cold chain system
lHuman resource for cold chain and vaccine logistics
lCCE testing lab
1. Develop National Cold Chain Management action plan:

................................
2 3
b) Specification of equipment and accessories
A specification committee comprising technical experts from the field, the National Cold Chain Training Centre (NCCTC), engineering colleges, IITs, and program experts will be established to provide guidelines on the technical specifications of cold chain equipment and accessories.
c) Procurement guidelines for cold chain equipment and accessories
Procurement guidelines for cold chain equipment and accessories shall be developed, and reviewed periodically by a technical committee of experts convened by the MoHFW. The guidelines shall provide parameters for equipment procurement, rationale for purchase, quantity, guidelines on aging etc. The technical committee shall meet at least once a year.
Stress will be placed on promoting indigenous cold chain equipment which is contextualized and adaptable to local needs and environment. A Management Information System (MIS) for tracking the working status of cold chain equipment and spare parts will also be set up. The plan will also focus on regular retiring of old and sick cold chain equipment, regular program reviews with cold chain officers, staff trainings, maintenance and servicing of cold chain equipment, implementation of MIS, logistics and supply chain management.
d) Promote indigenous cold chain equipment for immunization
To reduce costs and improve overall program efficiency, the MOHFW will promote the use of cold chain equipment that is locally p r o d u c e d a n d s e r v i c e d b y I n d i a n manufacturers. NCCVMRC will organize consultative meetings with engineering colleges, industries, IITs, national physical laboratories, DG S&D to determine the safety standard, program need and scale of requirement required to fulfill the needs of UIP.
2. Enhance the capacity of the National Cold Chain Vaccine Management Resource Centre (NCCVMRC) and the National Cold Chain Training Center (NCCTC) to better manage the Cold Chain and Vaccine Logistics Management (VLM) system.
The NCCVMRC has been set up in National Institute of Health and Family Welfare (NIHFW) to conduct training and capacity building activities on cold chain equipment and vaccine management, including preventive maintenance and repair, at the state level. The center provides supportive supervision to states to promote smooth functioning of cold chain and vaccine management systems. The center also undertakes cold chain and vaccine management assessments and reviews jointly with the Immunization division MOHFW, UNICEF, WHO and other partners. It functions as an extended wing of the Immunization division (MoHFW) for cold chain and vaccine management. The NCCVMRC's needs enhancement in terms of human resources recruitment, infrastructure and equipment to be able to function effectively (See Annex 3).
The NCCTC, which has been set up at SHTO Pune, is the country's only cold chain training center. The NCCTC will have its capacity strengthened to perform the following:
lfunction as a testing lab of equipment performance,
lexperiment with innovative technologies,
lsupport the MoHFW for procurement by producing evidence on the specifications of equipment and their performance,
ldevelop appropriate spare parts for all types of cold chain equipment enabling local repair,
ldevelop a training module of Cold Chain Equipment (CCE) repair and maintenance,
lprovide maintenance support to GMSDs.
The center will be run as an independent body
U I P S T R A T E G I C P L A N F R A M E W O R K
2 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
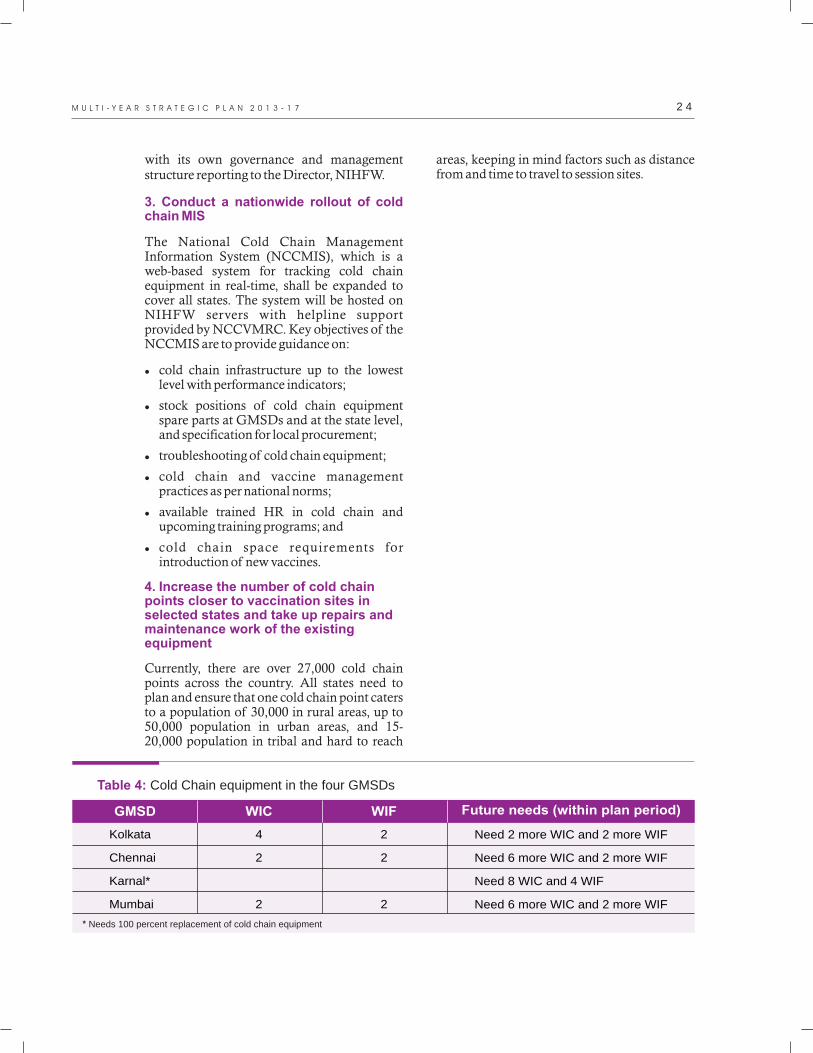
Table 4: Cold Chain equipment in the four GMSDs
* Needs 100 percent replacement of cold chain equipment
Kolkata
Chennai
Karnal*
Mumbai
Need 2 more WIC and 2
Need 6 more WIC and 2 more WIF
Need 8 WIC and 4 WIF
Need 6 more WIC and 2 more WIF
more WIF4
2
2
2
2
2
GMSD WIC WIF Future needs (within plan period)
with its own governance and management structure reporting to the Director, NIHFW.
The National Cold Chain Management Information System (NCCMIS), which is a web-based system for tracking cold chain equipment in real-time, shall be expanded to cover all states. The system will be hosted on NIHFW servers with helpline support provided by NCCVMRC. Key objectives of the NCCMIS are to provide guidance on:
lcold chain infrastructure up to the lowest level with performance indicators;
lstock positions of cold chain equipment spare parts at GMSDs and at the state level, and specification for local procurement;
ltroubleshooting of cold chain equipment;
lcold chain and vaccine management practices as per national norms;
lavailable trained HR in cold chain and upcoming training programs; and
lcold chain space requirements for introduction of new vaccines.
Currently, there are over 27,000 cold chain points across the country. All states need to plan and ensure that one cold chain point caters to a population of 30,000 in rural areas, up to 50,000 population in urban areas, and 15-20,000 population in tribal and hard to reach
3. Conduct a nationwide rollout of cold chain MIS
4. Increase the number of cold chain points closer to vaccination sites in selected states and take up repairs and maintenance work of the existing equipment
areas, keeping in mind factors such as distance from and time to travel to session sites.

................................
2 5
In addition to the GMSDs, each of the 39 State Vaccine Stores need to have 50 percent of their existing cold chain equipment replaced within the plan period. Each of these stores should have at least four WICs and two WIFs of 40 cub mt. which shall be put in place within the plan period.
Each of the 139 Divisional Vaccine Stores need to have one WIC of 40 cub mt and one WIF of 20 cub mt, which shall be put in place within the plan period.
Before the end of the plan period, each District Vaccine Store should have the following:
lone WIC and six DF in districts with a population of more than 2 million ,
leight large ILR and four large DF in districts with a population below 2 million.
Supplies of all non-electrical equipment 15(vaccine carrier, ice boxes) and accessories
shall be updated as per the needs of every cold chain point.
India is a vast country and putting a robust cold chain system in place requires a larger number of staff at all levels. As recommended in the Mavalankar report there shall be a position created for a focal point on cold chain at the national level. Each state should also make provision for a cold chain officer along with an assistant at that level. In addition, each district should have one Vaccine Logistics Manager and one Cold Chain Handler. The majority of issues and barriers related to cold chain and vaccine logistics pertain to program management rather than technical faults. All staff associated with cold chain and vaccine logistics will be provided training on various aspects of program management.
6.Enhance management capacity and numbers of cold chain and vaccine logistics staff at all levels with the district being responsible for stock distribution planning, management and repair.
7. Promote mentoring and supportive supervision to ensure that vaccines are stored within the correct temperature range
8. Scale up a system for SMS-enabled real-time temperature monitoring for cold chain as part of electronic Vaccine Intelligence Network (eVIN)
9.Enhance capacity of cold chain handlers and mechanics across the country
Various models of supportive supervision exist -using line supervisors, externally hired monitors or medical college faculty to provide mentoring and supportive supervision. A mixed approach will be applied based on state requirements to ensure that RI sessions use quality vaccines that have been stored at appropriate temperatures throughout the cold chain. Effective cold chain and vaccine management consultants will be used to review these improvement plans and vaccine store self-assessments using standard formats and local improvement plans from facilities visited
Real-time monitoring of cold chain equipment along with prompt alerts and corrective action are critical for the immunization program as all vaccines under the program are temperature-sensitive and cannot be used once damaged. As most cold chain points in the country are located in remote village settings with limited facilities, a special SMS-enabled temperature monitoring system has been developed and is being currently piloted. The technology will be further refined to prepare for its expansion to all cold chain points in the country. As part of the eVIN strategy, the possibility of unifying vaccine logistics management, temperature monitoring and cold chain equipment inventory management into one system will also be explored.
The training for vaccine and cold chain handlers shall be based on standard technical
16guidelines developed by the government. In addition to induction training, the cold chain mechanics and technicians will also be
15 Accessories include voltage stabilizer with every ILR and DF and toolkits for cold chain technicians16Handbook for Vaccine and Cold Chain Handlers 2010.Ministry of Health and Family Welfare, Government of India and UNICEF.
U I P S T R A T E G I C P L A N F R A M E W O R K

2 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
provided training on cold chain equipment – WIC, WIF, DF, ILR, cold chain accessories, solar and hybrid equipment. Refresher trainings will be held every three years to sustain capacity and ensure quality.
Expected Result 1.2: Strengthen vaccine and syringe logistics management across the c o u n t r y inc l ud in g fo r e c a s t ing a n d procurement at central level
A significant challenge in improving RI coverage is lack of visibility at every levels in the chain. Managers do not have real-time vaccine stocks status at all levels, consumption patterns, wastage rates and so on. Without such information, it is difficult to hold system functionaries responsible for lack of performance, or to generate prompt responses to breakdowns/bottlenecks in the vaccine supply chain. Data from the states where VMAT, EVMs and deep dives were conducted by UNICEF and ITSU indicate that the distribution of vaccines is uneven with some cold chain points holding excess stock levels, while others have stock-outs within the same district or division. Even when there are few stock-outs reported, there is evidence that store managers are slowing down vaccine distribution to cold chain points below them, or to session sites as a means of preventing stock-outs. This can lead to insufficient vaccines reaching immunization sessions, thus directly affecting the immunization coverage.
Strategies
Under the Universal Immunization Program, vaccines and syringes are centrally procured and supplied to States and Union Territories (UTs). The details of vaccines/syringe receipt, issue, wastage and consumption are documented in a variety of registers across the country. Some states have also started computerized documentation of stock levels, but only down to the district level. No nationwide vaccine logistics management and monitoring system currently exists that provides real-time visibility of the stock data,
1. Develop a vaccine and syringe logistics management system in the country with real-time stock visibility.
consumption patterns, wastage rates etc. In absence of such a system, a variety of ad hoc principles and processes are applied in distributing vaccines. With the potential introduction of more costly vaccines under the UIP, a robust vaccine logistics management system is a dire need.
A vaccine logistics management model is being developed that can cater to requirements at all levels i.e. from GMSD to the last vaccine storage point (last cold chain point). The product will be field tested and updated to be made ready for country-wide rollout. When fully implemented, the system will also provide better estimates for further procurement and will outline the effects on the logistics system of delays in procurement and erratic vaccine supply patterns. Based on data analysis and the vaccine supply schedule being followed, new guidelines for defining minimum and maximum stocks at different levels will also be developed.
An effective vaccine logistic management system must be supplemented by an operations team that keeps the network operational as well ensures prompt response based on data. The government will introduce a position for VLM at national, state and district levels at least in the 12 high-priority states. The district-level VLM will also oversee the functionality of cold chain equipment in the district and will ensure swift repair or replacement of cold chain equipment with support from the district refrigerator mechanic. These staff will be provided training on vaccine logistics and cold chain management.
There is substantial technology upgradation going on rapidly across the world in the field of vaccine logistics and cold chain management.
2. Strengthen HR capacity at all levels for vaccine management, including effective vaccine store management and forecasting
3. Pilot new technology for improving vaccine logistics and cold chain management with an overall objective to develop an electronic Vaccine Intelligence Network (eVIN)

................................
2 7
These interventions can be useful in ensuring the availability of safe and potent vaccines upto the last cold chain point. Such technological interventions will be field-tested for performance and will be considered for implementation with the ultimate aim of developing an electronic Vaccine Intelligence Network (eVIN).
Computer optimization models, such as HERMES, will be used for exploring means to maximize vaccine and syringe logistics efficiency.
EVMs assessments were conducted in ten priority states in 2013. These states include Jammu & Kashmir, Haryana, Rajasthan, UP, Bihar, Chattisgarh, MP, Karnataka, Kerala and
17Tripura. The key recommendations from the EVM assessments will be implemented through the PIPs of the respective states. These recommendations are included in Annex 4. A trained pool of effective cold chain and vaccine management consultants will review the progress of PIPs in states that have completed an EVM asses sment and p re pared improvement plans.
Expected Result 1.3: Ensure safer injection practices and reduced vaccine wastage
Strategies
The disposal of syringes and other waste associated with immunization sessions shall be based on the Biomedical Waste Management and Handling Rules, 1998, and Central Pollution Control Board (CPCB) Guidelines for hospital and immunization waste disposal. Under the NRHM, an Infection Management and Environment Plan (IMEP) policy framework has been formed to guide waste disposal processes. These guidelines will be widely disseminated and shared during review meetings. All health facilities will have 'waste management guidelines ' prominently
4. Implement Effective Vaccine Management (EVM) improvement plans
1. Review existing mechanisms and policies on waste management
displayed at the site of waste generation.
India had adopted the Multi-Dose Vial Policy (MDVP) for OPV during SIA campaigns. In 2011, the Multi-Dose Vial Policy was adopted for the birth dose of the Hepatitis B vaccine, and the zero dose of the Oral Polio vaccine in the UIP. Later, in the year 2011, the Multi-Dose Vial policy was adopted and implemented as part of RI for the Pentavalent vaccine in two states. The current open vial policy (OVP) applies to multi-dose vials of DPT, TT, Hepatitis B, Oral Polio and Liquid Pentavalent vaccines (where applicable). This policy does not apply to Measles, BCG, and Japanese Encephalitis (JE) vaccines (See Annex 5).
Relevant immunization trainings shall have a component on the OVP to facilitate the appropriate use and return of vials and reduce wastage. The policy of bundling shall be adopted for all vaccines, AD syringes, reconstitution syringes, diluents, disposal bags, and hub cutters to reduce wastage and improve logistics efficiency, wherever applicable. The required amount of vaccines for a session will be packed along with the needed logistics, so as to ensure that safe injection practices are adopted.
A vaccine wastage assessment carried out by UNICEF in 2010 revealed high wastage rates ranging from 61 percent (for BCG) to 27
18percent (for DPT). The main causes of wastage include vaccine expiry, discarding unused doses, poor reconstitution practices, exposure to heat, frozen vaccines, missing inventory and theft.
To reduce vaccine wastage, all categories of staff shall be trained on this aspect of the program as part of their regular training regimen and given job aids on injection safety and safe waste disposal.
2. Strengthen the implementation of Open Vial Policy (OVP) and Bundling Policy to reduce waste at session sites
3. Scale up training on injection safety and waste disposal guidelines for all categories of staff
17National Effective Vaccine Management Plan 2013: Summary Report. UNICEF and MoHFW.18Vaccine Wastage Assessment: Field assessment and observations from national stores and five selected states of India. UNICEF, April 2010.
U I P S T R A T E G I C P L A N F R A M E W O R K

2 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
4. Expand the availability and use of hub cutters in all districts and explore other technological advancements to ensure safe and appropriate bio-waste handling
1. Conduct risk analysis at state and district level
2. Provide training to and follow up with relevant staff on preparing and implementing RI micro-plans
To ensure safer injection practices, health workers will be trained on the use of hub cutters as part of their on-going trainings. In addition, technological developments in injection safety and bio-waste management will be explored and field tested. Based on performance evaluations, cost considerations, feasibility of use at the field level etc., the inclusion of these technologies in the Immunization program will be considered.
Expected Result 1.4: Ensure that regular immunization sessions are planned and held and coverage increased
Strategies
The country has identified high-priority districts for interventions under RMNCHA+A where immunization coverage has been considered a one of the key elements. States have also identified high-priority district under Emergency Preparedness and Response Plan (EPRP) to prevent wild polio virus importation. Further risk analysis will be done to identify high risk blocks and urban dwellings with low coverage.
Continuous training and skill building of health staff involved in routine immunization program is required to achieve and sustain quality and coverage of immunization. Training modules for frontline health workers, medical officers and cold chain and vaccine supply staff have been prepared and states are using them regularly to train the staff. Ministry updates these modules on regular interval and provides to states. These modules include all relevant components for preparation of plan for RI and its implementation and monitoring. However, the Government of India has
identified issues in implementation of training that varies from state to state resulting in gaps in performance. The Government of India will encourage all states to develop a time-bound schedule for training for all staffs and refresher trainings at regular intervals. These cycles will be aligned with annual PIP.
Guidelines for micro-planning and service delivery have been developed and included in the immunization handbooks for medical officers and health workers. Health workers and other relevant UIP staff will be trained on preparation of micro-plans that ensure inclusion of areas with underserved population, hard-to-reach areas and others. The efforts will be made to reach the un-reached population at least four times a year. The support of the development partners will be sought for the micro-planning efforts. The districts should ensure that micro-plans are available and being used to provide immunization services in the area.
MoHFW has recommended fixed-day, fixed-time and fixed-site strategy for outreach sessions for delivering immunization services to ensure that communities are aware of the immunization day that is now being implemented by all states. Under this strategy, the Government of India has recommended that immunization sites be fixed for each habitation, preferably at sub-centers; in villages at anganwadi centers, school and panchayat chaupal, etc. The day of the week and time of session in a particular location are also fixed. The immunization session can also be combined with Village Health and Nutrition Days (VHNDs) under NRHM to help maximize the opportunity for community mobilization and service delivery.
The Government of India is planning to strengthen health service delivery in urban areas now. This will be further strengthened with special focus to reach poor and underserved populations living especially in slums, streets and peri-urban areas.
3. Promote fixed-day, fixed time and fixed site strategy

................................
2 9
4. Fill up gaps in RI coverage through strengthening alternative vaccine delivery to provide needs-based immunization services in difficult to reach areas
5. Reduce left-outs and missed opportunities, drop-outs and ensure booster doses
To ensure improved vaccine and logistics supply and help ANM to spend more time at outreach session site and focus on improving immunizat ion ser v ice de l iver y, the Government of India has provided funds for implementing alternate vaccine delivery (AVD) system. These efforts will be further s t r e n g t h e n e d . U n d e r t h e p l a n f o r intensification of RI, the Government of India has planned to provide vaccine delivery vans to high-priority districts and blocks to strengthen vaccine supply. In this regard, the Government of India has already provided 120 vehicles in six districts of five states – Madhya Pradesh, UP, Haryana, Jammu & Kashmir and Rajasthan to implement a pilot before expansion. These vehicles have been branded “Teeka Express”. These vehicles will be used not only for vaccine delivery but carrying other logistics for immunization sessions, promoting IEC for RI, running mobile health clinic etc. depending on the need of the district.
The Government of India aims to identify all areas/populations/opportunities to reduce left-outs and to improve booster coverage beyond primary immunization schedule. This is also important in view of new antigens being introduced in UIP. To improve the access with the aim of reducing left-outs the Government of India has developed guidelines to include all high risk populations/areas, identified through polio eradication program, in the routine immunization micro-plans. The Government of India has also recommended to use polio micro-plan to identify all small areas/hamlets under each sub-center area to be reflected in micro-plan to improve reach and monitoring. It will be further strengthened by identifying all opportunities and places like OPDs and schools to enquire and vaccinate children..
a) Health facilities: Every contact of health care system with children of vaccination age will be used to enquire about the child's vaccination status. Vaccines will be administered where applicable, provided the minimum interval between doses is respected. Possible reasons for non-vaccination shall be identified and addressed.
b) Schools: School health programs will be strengthened. The LHVs will visit every school with ANMs at least once a year with vaccines to assess the immunization status of children and ensure vaccination with DPT of children aged 5–6 years, and TT vaccination for children aged 10 and 16 years.
Once a beneficiary is registered, all the efforts will be made to ensure full utilization of immunization services for completion of immunization scheduled. Special efforts will be made in the areas where immunization coverage is low and dropout rates are high.
a) Strengthen use of Due List by frontline health workers for tracking beneficiaries and improve communication with parents to reduce drop-outs:
Ensure that states and UTs make available the standardized Due List to all the FHWs with appropriate guidelines and trainings for its effective use.
b) Strengthen Mother and Child Tracking System (MCTS): The Government of India has launched Mother and Child Tracking System to improve registration of pregnant women and infants and utilization of Ante-Natal Care (ANC) and immunization services. This is being implemented as a mission mode project and all states have implemented this. The implementation and utilization of MCTS will be further strengthened to achieve the objectives.
States will utilize the NRHM framework to innovate to increase immunization coverage. The best practices and successful examples will be disseminated widely for cross learning and adoption by the states.
U I P S T R A T E G I C P L A N F R A M E W O R K

3 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
6. Strengthen the RI supervision and monitoring system
7. Involve private facilities in delivering RI services
8. Plan and conduct immunization weeks at regular intervals to improve coverage level in missed out and hard-to-reach areas, followed by integration of these areas under the district RI micro-plans.
1. Conduct bi-annual national level meetings of state EPI officers
MOHFW will focus on improving program supervision and monitoring for RI at all levels using data generated in the program and through field monitoring. RI partnership in the country is actively participating in monitoring of implementation at field level and assisted states in involving their program managers and staff in the monitoring. Haryana has developed a monitoring system by involving independent monitors using NRHM funds. Other states will also be encouraged to prepare plans for monitoring and propose in PIPs.
The involvement should be underpinned by accountability and quality standards that are regulated by the state nodal medical authority. Public and private practitioners providing vaccination will be provided free of charge vaccine and immunization cards etc. All private practitioners, offering vaccination services, will be expected to maintain appropriate institutional records, retrievable on demand. They will also be expected to report coverage, VPDs, AEFI, and wastage on a monthly basis. Private sector accountability and quality issues will be coordinated by the nodal medical authority providing the vaccines
19as per the Government of India guidelines. Necessary efforts will be made to implement the guidelines for involvement of private practitioners in immunization program.
Expected Result 1.5: Improve program coordination at all levels
Strategies
National-level half yearly meetings of all state EPI officers will be conducted regularly. State
immunization officials will be requested to conduct regular and quality quarterly review meetings with district immunization officers to strengthen the program at ground level.
The Government of India has issued directives to all states for setting up state and district-level task force on immunization for improved program coordination and monitoring. States will ensure that these task force meetings are held every month and necessary feedback is shared with national immunization division.
The ministry recognizes various efforts being done and the support provided by development p a r t n e r s i n r o u t i n e i m mu n i z a t i o n strengthening both at national and sub-national level. Efforts will be made to ensure better coordination between government and development partners through regular coordination meetings, partner's forum and other relevant platforms.
IAG, which has been setup by MoHFW, will advise and provide technical inputs to the national immunization division on ways to improve routine immunization coverage and issues around newer and underutilized vaccines.
1. % of caregivers whose child received partial or no immunization who did not feel the need for adhering to the schedule of immunization
2. % of caregivers not recalling any of routine vaccine
The indicators will be disaggregated by gender,
2. Improve coordination with development partners through regular meetings and information sharing
3. Promote immunization and related interventions through Immunization Action Group (IAG) including academia, CSOs, political representatives
KEY OBJECTIVE 2: Increase demand and reduce barriers for people to access immunization services through improved social mobilization.
Key Performance Indicators (KPI)
19 Guidelines for involvement of private practitioners in the universal immunization program (UIP). Government of India, Ministry of Health and Family Welfare, Immunization Division, 31 August 2009.
................................
3 1
geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 2.1:Develop and implement a multi-pronged national communication strategy with a focus on priority states
Strategies
A national strategic communication plan for RI will be prepared. States and districts will also be encouraged to prepare an integrated communication work plan. This plan will have focus upon components and strategies for addressing the issues related to left-outs and drop-outs, and to increase community participation in immunization.
The IRI communication guidelines have been developed by the Government of India to provide a roadmap to the immunization program managers and IEC functionaries at state, district and block level. These guidelines can be used as a reference while formulation
20state-specific communication plans.
National and state-level workshops will be conducted for immunization program managers and other staff working on communication. The trainings will focus on strengthening their communication and planning skills to better operationalize and implement IEC interventions. MOFFW will also conduct regular national and state-level meetings to monitor the progress, identify gaps and sugges t pos s ib l e so lu t ions on communication strategies. In addition, effective communication activities and best practices will be documented and shared with all the stakeholders to be used for inter-state learning.
Enhanced partnerships with CSOs and NGOs will promote greater awareness and access to
1. Develop state-specific Communication Implementation plans, advocacy and social mobilization plans
2. Strengthen national and state capacity on behavior change communication
3. Engage with partners to ensure a wider dissemination of immunization messages.
RI services. The CSO engagement strategy will focus on engaging civil society in policy and advocacy processes. The Government of India will engage the private sector to work in immunization program as part of their CSR utilizing their strengths in communication.
NRHM has provided necessary flexibility to use funds for activities related to immunization program. The available funds with districts will be utilized for health communication. The untied funds with AWW/ASHA, VHSC and ANM may a lso be used for these communication efforts, if funding from other sources is not available. States will be encouraged to prepare a detailed IEC plan for immunization and funds will allocated to this activity from NRHM PIP part A
Expected Result 2.2:Effective communication channels are set up with the community for better acceptance of vaccines
Strategies
Utilize the widespread network of over 860,000 ASHA workers to conduct social mobilization for improving immunization coverage. Interpersonal communication (IPC) with individuals and families will be strongly promoted through the frontline health workers – ASHA, ANM, Anganwadi workers and other key leaders in the communities.
The Government of India has developed a training kit to improve IPC skills of frontline health workers to improve awareness among parents about need for immunization and completion of recommended schedule and to reduce fear of AEFI to reduce drop-outs. All FHW will be trained on using this kit.
The community members, non-government organization and interest groups in
4. Ensure adequate funds are available for communication interventions
1. Use frontline health workers and community platforms like Village Health and Nutrition Day to promote RI through inter-personal communication (IPC)with families
20 Intensification of Routine Immunization: Communication Operational and Technical Guideline. 2012. Immunization Division, Ministry of Health and Family Welfare. Government of India.
U I P S T R A T E G I C P L A N F R A M E W O R K

3 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
immunization like women's self-help groups w i l l b e i nvo l ve d i n a dvo c a c y f o r implementation and increasing demand for services. Events like VHNDs will be utilized as opportunities for community mobilization. Wherever reports of mistrust towards immunization by community members are noticed, these should be studied and appropriate corrective actions need to be taken.
At the community level there is a greater scope of better social mobilization and reaching local community leaders through convergence of RI with ICDS, women self-help groups and panchayati raj institutions. The program will also seek to involve local MLAs and MPs to utilize their funds to ensure that each and every child in their community is vaccinated. Local institutions, community networks, and religious groups will also be reached out in coordinated way to reach specific groups of people for dialogue with planned messages. School children and adolescents will also be engaged as change agents to dispel myths and misconceptions related to immunization.
Expected Result 2.3: Evidence based and contextually relevant communication messages are disseminated in the community
Strategies
Targeted communication will be needed for those who have never participated before, or who are not participating consistently because of lack of knowledge, doubts and misconceptions, or frustration with the quality of health services. The issues and barriers for the immunization will be addressed in the integrated communication work plan. The focus will be on SC, ST population, migratory
2. Promote inter-sectoral synergies between organizations, communities and individuals on promoting immunization
1. Identify issues and barriers for immunization in hard-to-reach populations and address them in the communication plan
population and difficult to access areas. The reasons for low coverage and level of knowledge about immunization program will be regularly assessed. The findings from these assessments will be a base for communication and social mobilization plans.
Promote the RI branding with a new logo color coding and tagline through various media. New audiovisual communication messages for TV and radio along with print material will be developed. The government will also use social media as a parallel communication channel to increase visibility about RI with multiple target audience. The program will strengthen delivery of interpersonal communication using Polio SMNet (from UNICEF), school teachers, student networks, national-level youth networks to support social mobilization. Institutions like NSS and NCC will be mobilized to reach out of school youth and eligible children in hard-to-reach population areas
Standard Operating Procedures (SOPs) will be d eve l o p e d f o r p r o d u c t i o n o f n ew communicat ion mater ia ls and their dissemination to the states.
The Government of India will engage all categories of media – print or electronic –through regular workshops, meetings and field visits to advocate for and create an enabling environment that leads to an increasing demand for immunization services.
With newer vaccines planned for introduction in the coming years, all efforts will be made to educate people and dispel any misinformation. Communication strategies for newer vaccines including campaigns will be developed in consultation with all stakeholders.
2. Develop and disseminate widely, new communication material on immunization
3. Increase people's confidence in vaccine safety through generation and dissemination of supportive data

................................
3 3
4. Develop effective communication response for AEFI crisis management
KEY OBJECTIVE 3:Strengthen and maintain a robust surveillance system for vaccine-preventable diseases (VPDs) and Adverse Events Following Immunization (AEFI)
To dispel any public misapprehension around adverse events following immunization the Gover nment of India wi l l deve lop communication guidelines to handle situations around AEFI.
The burden of diseases preventable by the vaccines is the most significant factor for making a decision on introducing relevant vaccines in the UIP. Therefore, a robust surveillance system to detect cases and deaths due to vaccine-preventable diseases is essential to generate evidence to inform the decision on introducing the vaccine as well as to measure its impact on the disease after its introduction. Besides that, the completeness and quality of VPD surveillance data is also necessary to observe the trends in disease incidence and geographical spread to help plan to strengthen the immunization program. Reporting of VPDs has been an integral part of UIP reporting system. Major challenges for UIP include the following:
lweak capacity of frontline health workers to identify cases,
llack of attention in the health system for VPD reporting,
lpoor coordination between various surveillance systems
lpoor reporting from private sectors and large institutions.
This has adversely impacted informed decision making on newer vaccine introduction and vaccine impact assessment. Therefore, it is necessary to
ldevelop the capacity of health workers for improved detection of VPDs,
lhave regular review of reports and data
limprove coordination among various surveillance systems
linclude private sectors and other institutions for improving VPD surveillance in the country.
The goal of immunization is to protect individual and the community from vaccine-preventable diseases (VPD). Although modern vaccines are safe, no vaccine is entirely without risk; adverse reactions will occasionally occur following vaccination. Some people experience adverse events after immunization ranging from mild side-effects to rare life-threatening illnesses. However, in most serious cases these events are merely coincidences. In others words, they are caused by the vaccine or by an error in the administration or handling of the vaccine. Sometimes there is no causal relationship between the vaccine and the adverse effects. Maintaining public trust in vaccine safety, therefore, is key to the success of
21all vaccination programs.
Irrespective of the cause, when adverse events following immunization (AEFI) occur, people become confused to the extent that they refuse further immunization of their children, making the children susceptible to VPDs that are more disabling and life-threatening. Surveillance of AEFIs, i.e. systematic collection of data on events following immunization,
provides valuable information to help plan and take necessary actions in order to sustain public confidence and ensure smooth functioning of the program. The national AEFI surveillance program supports the effective vaccine pharmacovigilance function for ensuring use of safe vaccines. Aggregate data for serious and non-serious AEFI are currently collected through routine monthly reporting in the HMIS but, details of serious AEFIs are also reported directly using the FIR, PIR and DIR formats.
Along with the national health programs, such as HIV and TB, that generate their own respective data through surveillance, different surveillance systems in India provide information of various diseases, including
21Immunization Safety Surveillance: Guidelines for Managers of Immunization Programs on Reporting and Investigating Adverse Events Following Immunization. WHO Regional Office for Western Pacific. 1999.
U I P S T R A T E G I C P L A N F R A M E W O R K

3 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
VPDs. These include:
Integrated Disease Surveillance Project (IDSP): This is a nationwide system that captures information on outbreaks of diseases including VPDs, such as diphtheria, pertussis, measles, AES, AFP, and Hepatitis B.
Central and State Bureaus of Health Intelligence (CBHI and SBHI):This nationwide system captures information on suspected cases through passive surveillance including that of VPDs that are under the current UIP.
Health Information Management System (HIMS): Within the NRHM framework, HMIS is an electronic data reporting system that captures data for health service delivery at health facility level every month to assist health departments, at all levels, in managing and planning health programs. HMIS also captures information on VPD disease burden from sub-block level on a monthly basis.
WHO supported AFP and Measles outbreak surveillance through NPSP network: AFP surveillance is a laboratory-based system for poliovirus detection in all states. The lab-based measles surveillance covers 15 states generating data on measles and rubella outbreaks. The laboratory assisted joint AFP-measles surveillance system is planned to cover all states and UTs by the end of 2014.
Acute Encephalitis Syndrome (AES/JE) surveillance: This is a facility-based surveillance system providing information on AES as per the guidelines under the National Vector-Borne Disease Control Program with lab support provided by ICMR.
Multicentre Pneumonia and Meningitis Surveillance: Sentinel surveillance sites are functional to identify etiologic diagnosis of pneumonia and meningitis among children below two years.
Rotavirus Surveillance Network in India: The Indian Rotavirus strain surveillance network is functional in seven regions, four hospitals and four labs. Children below five
years admitted with acute gastroenteritis and given rehydration for at least six hours are enrolled. Sites for sample collection for Rotavirus surveillance are in following cities: Delhi, Mumbai, Pune, Vellore, Jabalpur, Imphal, and Kolkata.
1. % of sentinel sites providing timely and complete reports on VPDs (including zero report) on 90% occasions
2. Increase in the number of notified serious AEFI cases above the 2012 baseline value
The indicators will be disaggregated by gender, geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 3.1:Institutionalize and strengthen surveillance mechanisms for VPDs
Strategies
There is a need to use epidemiological methods to better measure the impact of the immunization program. This will involve an initial landscaping of existing surveillance systems in the country, efforts will be made for collating, and analyzing data on VPDs generated from different surveillance systems and collate them to provide appropriate feedback. The following will be analyzed:
ldata on the VPD disease burden,
lemerging trends in the molecular epidemiology of different VPD antigens,
lseroprevalence of protective antibodies against the VPDs,
lgeographical variations in VPDs.
MoHFW will work towards developing a system that facilitates convergence of relevant data from various surveillance systems, such as IDSP and NPSP, in the country.
Key Performance Indicators (KPI)
1. Assessment of trends on VPD burden in context of reported immunization coverage

................................
3 5
2. Strengthen and improve coordination between Health information system (HMIS) and disease surveillance systems such as IDSP and NPSP to gather information on VPDs
3. Involve private sector in reporting of VPDs to further strengthen surveillance systems and inform policy making
4. Strengthen laboratories(including polio and measles lab network) and epidemiology units at medical colleges and other institutions for timely reporting, case investigation and detailed data analysis
IDSP-based surveillance system, along with other systems, need to be strengthened from district onwards to capture information on all VPDs. The model of District/Municipal Corporation-based surveillance unit for action and reporting to the state would be further strengthened. To better streamline information sharing on VPD and AEFI occurrence across the country, MoHFW will strengthen coordination and data sharing between IDSP and Immunization Division at national level to monitor and improve program performance. Similarly coordination at the state and district levels will also be promoted to strengthen DIO's role as focal person for all information on VPD and AEFI.
In view of the number of patients using private healthcare, lessons learnt from Kerala will be used to link surveillance and monitoring mechanisms with the private sector. Community reporting of VPDs will also be encouraged and specific strategies will be reviewed. Mechanisms for coverage data collection, compilation and flow from session sites/sub-centers/private clinics to the district and then to the State on uniform patterns will be highlighted. VPD surveillance mechanisms will attempt to integrate as much as possible with other surveillance mechanisms, without losing the required responsiveness for outbreak response or diluting the focus on AFP surveillance.
For improved coordination and information sharing Infectious Diseases Hospitals(IDH)
and super speciality hospitals should be integrated into IDSP. There is a network of IDH that needs to strengthen their laboratory capacity to provide updated information on outbreaks of existing or potential VPDs. India has developed a Health Management Information System (HMIS) for reporting of all health-related data from field. This tool will be used for updating VPD surveillance data in India.
Improve coordination, information sharing with existing agencies and systems such as IDSP, ICMR, CBHI and SBHI networks so as to coordinate, collate and generate robust data that will guide a more evidence-based policies a n d p r o g r a m i n t e r ve n t i o n s i n t h e immunization program future.
Expected Result 3.2: Institutionalize and strengthen surveillance mechanisms for AEFIs
Strategies
The national AEFI guidelines mandate that all states and districts in the country constitute AEFI committees at each level, to assist in streamlining AEFI reporting mechanism, investigating serious AEFI, and be involved in causality assessment at state and national level. An AEFI secretariat for the National AEFI committee has been set up at ITSU-MoHFW, New Delhi, to coordinate all AEFI related activities in India with technical support and oversight from a leading medical college (LHMC). In addition Zonal AEFI consultants are planned to be in place to provide technical support and oversight to the AEFI Secretariat in the four zones of the country and enable timely reporting, investigation and support to the states.
The National AEFI committee has been reconstituted to support the program in reviewing and updating information on tasks and responsibilities of key stakeholders in the AEFI system, including the Drug Controller
5. Strengthen sentinel surveillance for newer antigens
1. Revitalize the institutional framework and guidelines for AEFI surveillance in the country
U I P S T R A T E G I C P L A N F R A M E W O R K

3 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
G e n e r a l o f I n d i a ( D C G I ) , I n d i a n Pharmacopoeia Commission (IPC), National UIP managers and state-level UIP managers.
National AEFI Operational Guidelines, which were revised in 2010, are being revised and will
22be published in 2014. These guidelines will be distributed to all medical officers till Primary Health Centers and will be used for training the UIP staff including ASHA and ANMs. Innovative AEFI reporting models shall be piloted to enable enhanced AEFI reporting. The revised guidelines will also be utilized for trainings of AEFI committee members in the country. An abridged Standard Operating Procedure (SOP) for AEFI surveillance and case investigation version been printed and
23widely disseminated in 2011. There is well known poor reporting of minor AEFIs in India. The efforts will be made to train the field staff in collecting data on minor AEFIs and pass this information to the next level.
Since 2010, India has been participating in WHO Global network of post-marketing surveillance and the Government of India has nominated Maharashtra state for uploading AEFI data into the Uppsala Monitoring Centre vaccine safety database. The national immunization division has also started coordination with the IPC, the coordinating agency for the National Pharmacovigilance Program of India to collate and monitor vaccine safety reports in the country. The National AEFI Program already shares all data on vaccine safety with the national regulatory authority to inform all vaccine safety stakeholders.
AEFI surveillance data require detailed analysis on numerous parameters in the context of the doses distributed and children vaccinated in the UIP. Currently serious AEFIs
2. Train field level staff on new National AEFI Guidelines
3. Convergence with vaccine pharmacovigilance stakeholders and private sector for AEFI reporting and analysis
4. Electronic database and reporting system for AEFI
are reported manually on FIR/PIR and DIR formats by districts but can be transmitted electronically to the higher level (state and national). The government will pilot an electronic AEFI database and reporting system that is E2P compliant for AEFI reporting by 2015 in a phased manner.
As UIP evolves, newer antigens, such as rotavirus, JE, rubella, Pneumococcal and Pentavalent vaccines, are expected to be introduced and expanded in the schedule. This will require a strong epidemiological underpinning for estimating disease burden in the country through a robust surveillance system to be put in place. There will be a need for improving coordination among different stakeholders and experts to develop an evidence-based policy for introducing newer antigens in the program in the medium term. In addition to newer antigens, improved service delivery will require innovations in technology and approaches.
The choice of newer vaccines to be included in the UIP will be determined and periodically reviewed by the MoHFW, taking guidance from the NTAGI. Basic clinical and operational studies will be encouraged to provide inputs for NTAGI. These studies will provide evidence for decisions on the timing and selection of new vaccine introduction and provide guidelines for the use of these new vaccines. Such analysis will include the major mortality-causing diseases of children in India, namely acute diarrheal diseases and acute respiratory diseases, in anticipation of rotavirus vaccine and pneumococcal vaccine becoming available. Disease burden and health economic analyses will help assess the cost-benefit ratios of new vaccine introduction. Box 2 captures the key principles that will guide the inclusion of newer vaccine in UIP as per the national vaccine policy 2011. However, introduction of new vaccines would be as per decision of Mission Steering Group (MSG) following NTAGI recommendations.
KEY OBJECTIVE 4: Introduce and expand the use of new and underutilized vaccines and technology in UIP
22Adverse Event Following Immunization (AEFI): Surveillance and Response Operational Guidelines. MoHFW, Government of India. 2010.23Standard Operating Procedures for reporting AEFI. MoHFW, Government of India. 2011.

................................
3 7
Box 2: Principles to guide the inclusion of newer vaccines
• Disease burden (incidence/prevalence, absolute number of morbidity/mortality, epidemic/pandemic potential);
• Safety and efficacy of the vaccine under consideration;
• Affordability and financial sustainability of the vaccination program, even if the initial introduction is supported by the external funding agency;
• Program capacity to introduce a new antigen, including cold chain capacity;
• Availability of a domestic or external vaccine production capacity;
• Cost effectiveness of the vaccination program and also of the alternatives other than vaccination
Key Performance Indicators (KPI)
1. Institutionalize mechanisms to guide the introduction of newer and underutilized vaccines in the country
1. Number of newer vaccines that have been reviewed for introduction in UIP by NTAGI
2. Number of States that have introduced Pentavalent vaccine
The indicators will be disaggregated by gender, geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 4.1: Set up and strengthen institutional mechanisms, framework and policies for newer and underutilized vaccine introduction
Strategies
The introduction of new vaccines involves reviewing all licensed vaccines in different parts of the world and identifying those that would be relevant to India in the context of the burden of disease in the country and prioritization of target vaccine-preventable diseases in the country. There are several vaccines that are popular in the private market, and many of those are recommended by the Indian Academy of Pediatrics. Accurate information on which to base the decision of
introducing a new vaccine to the UIP requires periodic review and assessment on an objective scale by all agencies concerned through strong coordination and collaboration.
In this regard, the immunization decision-making process has been institutionalized by the establishment of an independent advisory body, the National Technical Advisory Group on Immunization (NTAGI) in 2001, comprising of independent experts from diverse fields such has immunology, community medicine and health economics; representatives from partner organizations like WHO, UNICEF, ICMR and DCGI as well as liaison officers from the government. The NTAGI has been reconstituted twice in 2008 and again in June 2013. The current reconstituted NTAGI comprise of a Standing Technical Sub-Committee (STSC) tasked with undertaking a detailed technical review of the issues highlighted above and a broader body with representations from all organizations mentioned above. In addition, a secretariat for this advisory body has been established by ministry under Immunization Technical Support Unit to facilitate technical and managerial support required for continuity and follow up to this body. However, the mandates of both the NTAGI and STSC are still work-in-progress. The spelling out of well-defined Standard Operating Procedures (SOPs) for the functioning and decision making of the
U I P S T R A T E G I C P L A N F R A M E W O R K

3 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
NTAGI is necessary to institutionalize the evidence-based decision-making process for the introduction of new and underutilized vaccines in the country. It is also imperative to adopt and standardize mechanisms to grade the quality of evidence available, such as burden of disease, published literature, global data, cost effectiveness data, for the NTAGI to r e v i e w a n d m a k e e v i d e n c e - b a s e d recommendations.
There are several vaccines that are already licensed and available or soon to be licensed with expanded indications for particular groups in India. Unfortunately, access to the bulk of these vaccines is available only to the privileged few who have access to private health care. The NTAGI is the highest advisory body tasked to review the available evidence on disease burden, potential impact, safety, efficacy etc. To assess these vaccines and prioritize vaccines for inclusion in the program. Vaccines that can be potentially considered for review include the Injectable Polio Vaccine(IPV), rotavirus and pneumococcal vaccines
The absence of reliable baseline estimates for the burden of VPDs in India is a major obstacle in informed policy-making process. Currently, there are multiple systems to measure different VPDs including antigen/disease specific sentinel surveillance network (Indian Rotavirus Sentinel Surveillance Network, National Polio Surveillance Program (NPSP) network and Infectious disease surveillance eProgram (IDSP). With plans to expand the range of vaccines in the UIP and improve its reach (coverage), the surveillance of VPDs will be intensified and steps will be taken to establish stronger collaboration between the already established networks and the immunization program. At the national level,
2. Identify newer vaccines that will be introduced and/or expanded to use during the plan period
3. Assess disease burden for which vaccine are becoming available or will become available in the near future
the newly formed STSC of the NTAGI has been tasked for undertaking critical review of disease burden data prior to recommending the introduction of a new vaccine in the UIP. The NTAGI secretariat at ITSU will collaborate closely with the disease surveillance centers in the country to collate the evidence for the review of the NTAGI and STSC.
Generate evidence for introducing new vaccine – including areas like vaccine safety, equity, vaccine ethics and financial sustainability, IPV as part of post-polio eradication.
Expected Result 4.2: Scale up and sustain the implementation of JE vaccination in identified endemic districts as part of Japanese Encephalitis (JE) control
Strategies
In India there are 175 districts currently identified as being endemic for JE. Most of the cases occur in UP and Assam. Though any age group can be affected by JE, children between 1 and 15 years of age bear the brunt of the disease. A study carried out in South India showed JE incidence to be 15/10,000 children between 5 and 9 years. Mortality due to JE has been estimated to be between 20 and 30 percent. Recent studies under the WHO surveillance program in India undertaken in selected centers (Bellary, Dibrugarh, Madurai and Burdwan) show that about 10 to 20 percent of the total Acute Encephalitis Syndrome (AES) cases are JE.
JE, at present like other vaccines in India's UIP, is restricted to children but there is an increasing demand for use of JE vaccine to protect the adult population in endemic districts. The NTAGI will discuss the safety and immunogenicity data of the vaccine for use in the program. Since JE is a vector-borne disease, immunizing adult populations will prove critical in breaking the transmission cycle and control of the disease.
4. Conduct operational research
1. Identify disease burden and endemic districts for prioritization
................................
3 9
2. Continue JE campaign in the endemic districts
3. Expand training and advocacy on JE vaccination
4. Introduction of JE vaccine in routine immunization program
ICMR recommends that JE vaccination program should continue for another five years in endemic areas. It was suggested, that in view of low evaluated coverage with JE vaccine, the strategy in 2010 should be to re-immunization all children up to 15 years with high vaccine coverage in a campaign mode. Thereafter coverage should be sustained by immunization of children below than 2 years through Routine
24Immunization.
Coverage survey conducted for JE vaccine suggests that overall community knowledge on JE vaccines is low. While some people are not convinced about the need for JE vaccination, others do not know where to access the vaccine from. Some pockets of communities have fear of side effects or have formed a negative opinion on the vaccine following some AEFIs
25, 26in their area.
Information about JE vaccination has been incorporated in immunization handbooks for Medical officers and health workers. Operational guidelines for JE vaccination program has been prepared and widely disseminated to ensure correct reporting and clarification on the role and responsibility of each health care provider in JE vaccination. Publicity around the JE vaccination will be made more intense prior to the campaign dates and respective states shall ensure that the IEC material reaches the target users well in in time. Adverse publicity around the vaccine will need to be countered through appropriate messages.
The planned strategy was to complete SIAs for JE vaccine and subsequent introduction of the JE vaccine routine immunization program of
endemic districts to ensure adequate vaccination coverage for new birth cohort. As from April 2013, the Government of India has already introduced a 2-dose schedule for JE vaccines in the districts implementing JE routine immunization. The 1st dose is given at 9 months of age and the 2nd dose at 16 – 24 months of age
In India, currently the SA-14-14-2 imported from China is being used in the national immunization program. Efforts will be made to ensure that JE vaccine is produced indigenously from local strains and introduced in the program.
Expected Result 4.3: Streamline and expand the use of Pentavalent vaccine to cover all the states
Strategies
As of 2012, the Haemophilus Influenzae b (HiB) vaccine has been introduced in eight states of India (Tamil Nadu, Kerala, Karnataka, Puducherry, Goa, Gujarat, Jammu and Kashmir and Haryana) in the form of the combined Pentavalent vaccine (DPT+ Hep B+ HiB). On 23 September 2013 the NTAGI endorsed the STSC's recommendation for further scale-up of the vaccine in the remaining states of India in a logistically structured manner with simultaneous strengthening of the AEFI and sentinel surveillance systems in the country. Preparations for the expansion of vaccination to the other states are planned. The operational guidelines on HiB as part of Pentavalent vaccine have been already been developed and will be useful for immunization program managers at state, district and sub-
27district level.
5. Roll out indigenously produced JE vaccine
1. Nationwide scale up of Pentavalent vaccine to introduce HiB vaccine in other states of the country
24Minutes of the Meeting of ICMR Core Committee on Vaccines. 2010
25Japanese Encephalitis Coverage Evaluation Survey Report, 2008. UNICEF and NRHM26A coverage evaluation survey of JE vaccination in two districts of Karnataka. Kumar KR et al. Journal of Communicable Diseases.Sep2010;42(3):179-84;27Operational Guidelines: Introduction of HaemophilusInfluenzae b (HiB) as Pentavalent Vaccine in Universal Immunization Program (UIP) in India. MoHFW, Government of India. 2011.
U I P S T R A T E G I C P L A N F R A M E W O R K

4 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
2. Conduct a revision of recording and reporting formats for improved surveillance and data management
3. Conduct training of FHWs and their supervisors on newer vaccine
4. Strengthen surveillance system for HiB and AEFI reporting
Introduction of newer vaccines will accompany the revision of recording and reporting formats. Vaccination cards will also be revised and updated to include newer vaccines. The reporting system in the country will also have necessary column to collect information on newer vaccines.
ANMs and their supervisors will be trained on newer vaccines and other related aspects including the vaccine administration and AEFI reporting as part of regular training. The DIOs and other Mid-level managers (MLM) will be specially trained prior to the new vaccine introduction in their respective states.
The surveillance system for newer vaccines will be further strengthened and expanded in India. Eleven sentinel sites for HiB meningitis in six different states have already started in 2013. These selected sites for bacterial meningitis surveillance (including HiB) will monitor the disease trends to measure impact trends of vaccination on the study populations. The surveillance sites for other newer vaccines are also likely to be introduced to cover additional states. Model AEFI systems are also being planned to ensure timely reporting and management of AEFIs before they snowball into a crisis.
Expected Result 4.4: Evaluate Rubella antigen for introduction in RI program
During the 66th SEARO regional committee meeting in New Delhi in 2013, India has committed to the elimination of measles and control of rubella and CRS by 2020.
Strategies
The public health importance of rubella infection stems from the fact that rubella infection in pregnancy has the potential to cause Congenital Rubella Syndrome (CRS) in the new born. The risk of development of CRS is highest when infection is in the first trimester of pregnancy. While there is no hard data on CRS, the estimated incidence in India from modelling studies gives a range of around 123 per 100,000 live births. CRS results in a cumulative burden on the health system and families of affected children on account of the chronic sequelae (such as disability of sight, hearing or cardiovascular systems) and the economic burden in diagnosis, assessment and treatment of congenital malformations and challenges to providing education in an increasingly nuclear family structure in society. There are plans at national level to establish and expand CRS surveillance through partner agencies and existing surveillance programs. The surveillance sites will be established in selected states for observing the trends in CRS, before and after vaccine introduction.
The strategy for introducing the rubella vaccine in India's UIP will be planned to fulfil the commitment the country has made to the SEARO declaration for control of rubella disease and CRS burden in the country. Since immunization program performance differs across states, expansion of rubella sentinel surveillance sites is also planned. The strategy for phase-wise implementation will be chalked out over the cMYP period. The STSC of the NTAGI shall play a crucial role in reviewing and recommending a potential strategy for implementation. The NTAGI has also recommended the establishment of a Measles
1. Expansion of Congenital Rubella Syndrome (CRS) surveillance
2. Introduction and expansion of rubella vaccine in UIP
................................
4 1
& Rubella- India Expert Advisory Group (MR-IEAG) on the same lines as polio to develop a comprehensive strategy and monitor progress for rubella control and measles elimination in the country.
Existing measles surveillance system in India frequently report rubella outbreaks or mixed measles and rubella outbreaks. The existing measles network will continue to be utilized for identifying rubella outbreaks. It is envisaged that with introduction of rubella vaccine, cases of rubella will go down and, thereafter, a possibility and need for case based surveillance will be explored.
Once CRS surveillance system is established, the information collected from surveillance network will be utilized for assessing the trends in CRS in states and the country. Studies should be carried out to estimate incidence of CRS and the social and economic burden resulting from it.
Expected Result 4.5: Evaluate Rotavirus antigen for introduction in RI program
Strategies
Diarrheal diseases are one of the largest causes of childhood (under-5 years) deaths in India
28,29and rotavirus is the leading cause. WHO estimates that 23 percent of the annual 527,000 deaths due to rotavirus occur in India. It is estimated that even with a vaccine with 50 percent effectiveness, a rotavirus vaccination program in India would prevent 44,000 deaths, 293,000 hospitalizations, and 328,000 outpatient visits annually which would avert
30$20.6 million in medical treatment costs.
3. Conduct Rubella surveillance through the existing systems
4. Conduct research on CRS and trends
1. Assess disease burden due to rotavirus and the potential impact of a preventive vaccine
2. Strengthen national level surveillance on rotavirus
3. Develop the vaccine schedule in line with EPI schedule
KEY OBJECTIVE 5: Strengthen health system for immunization program
The Indian Rotavirus Surveillance Network was set up on 2005 with four laboratories and ten hospitals in seven different parts of the
31country. The network provides valuable information on epidemiology of rotavirus that will underpin the policy decisions regarding the introduction of rotavirus vaccine in RI.
NTAGI recommends that assuming several vaccines will be licensed and recommended for use in India, it would be preferable for each child to complete all doses using the same vaccine formulation. This could be facilitated by choosing a specific vaccine for national use or by ensuring that each region or state is supplied with only one specific rotavirus
32vaccine.
A strong RI program will contribute to the overall health system strengthening both in the urban and rural areas. Four states with large populations - Uttar Pradesh, Bihar, Madhya Pradesh and Rajasthan – contribute approximately to 2/3rd of the unimmunized children in the country (CES 2009). In addition there are other states that are not performing up to the mark as shown in Annex 1. Future strategies for RI will need to be adapted and contextualized for these high-priority states to increase the vaccination coverage levels and reduce VPD mortality and morbidity. Following polio eradication the technical support structures established for polio eradication, both at the national and sub-national levels, by WHO, UNICEF and other partners are now 'transitioning' to provide support to intensification of routine immunization from 2012 onwards, based on the lessons learnt from polio. This feeds into the
28 Causes of neonatal and child mortality in India: A nationally representative mortality survey. The Million Death Study Collaborators.The Lancet.Vol 376, November 27, 201029The Global Enteric Multicenter Study (GEMS) of diarrheal disease in infants and young children in developing countries: epidemiologic and clinical methods of the case/control study.Kotloff K L, et al. Clinical Infectious Diseases. 2012 Dec;55 Suppl 4:S232-4530Projected Impact and Cost-Effectiveness of a Rotavirus Vaccination Program in India.Douglas H. Esposito et al. Clinical Infectious Diseases.2011:52 (15 January)31 Multicenter, Hospital-Based Surveillance of Rotavirus Disease and Strains among Indian Children Aged <5 Years. Gagandeep Kang et al. Journal of Infectious Diseases.2009:200 (Supplement 1)32Minutes of NTAGI meeting. 3rd August 2009.
U I P S T R A T E G I C P L A N F R A M E W O R K

4 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
overall goal of strengthening health systems in the country.
The indicators will be disaggregated by gender, geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 5.1: Increase the pool of skilled human resources to provide quality immunization services in an integrated manner
Lack of adequate numbers of trained and skilled human resources has been a major barrier in improving the overall quality and outreach of UIP. The Immunization Division at MoHFW is small with few technical officers to manage such a large program. The Government of India has addressed this capacity gap by setting up an Immunization Technical Support Unit (ITSU) in year 2012 with technical officers to support various components of UIP. In addition to the national level, the HR capacity on UIP in the states need to expand. It is important to identify key functions within the UIP at state level also that would need full time positions to ensure a smoother functioning, improve institutional memory and enhance the overall coverage of immunization in the state. Under NRHM PIP, the Government of India has given the flexibility to the states to propose human resource augmentation plans at state and district level.
Strategies
The strength and capacity of the national immunization division has been enhanced
Key Performance Indicators (KPI)
1. Number of districts with full immunization coverage rate of >80%
1. Increase the number of technical managers for immunization at national and state level and strengthen organizational capacity to adequately perform strategic and technical functions under UIP
with the setting up of ITSU at MoHFW with recruitment of technical officers for key functions of UIP such as strategic planning and system designs, monitoring and evaluation, cold chain and vaccine logistics, strategic communication, vaccine safety and AEFI, and evidence to policy. This unit will help in the development of policies, procedures and guidelines to improve program management at national level. This setup will be further strengthened to augment the capacity for operational research and use of more technology in UIP. Similarly, a state-level structure is also proposed that includes recruiting focal points for the program management, Cold Chain, Vaccine Logistics, Management Information System (MIS), and Technology and research etc.
Relevant trainings will be carried out for new staff working in the immunization cell at all levels based on the existing training norms and guidelines under NRHM. Immunization-specific training norms will also be used, e.g. cold chain training norms. The training material for both medical officers and health workers in routine immunization has been updated, printed and widely disseminated. This material is being utilized for conducting need-based training.
National Institute of Health and Family Welfare (NIHFW) is the national nodal agency for training activities including Immunization. The NIHFW, in coordinat ion with Immunization and Training Divisions within MoHFW, will review the training plans from all states; conduct Training of Trainers courses, as well as monitor and evaluate the quality of trainings. The State Institute of Health and Family Welfare (SIHFW) is nodal agency at state level to plan, implement, monitor and evaluate the immunization training activities.
2. Conduct relevant training and induction programs and develop need-based immunization training materials
3. Strengthen training infrastructure

................................
4 3
A plan is being instituted to conduct induction training for new State Immunization Officers as per the need and refresher trainings on regular interval.
There is need for strengthening the existing training infrastructure and also starting new facilities. The issues of shortage of health workers and their training needs can be addressed by institutionalizing training mechanism for this category of staff. This can be achieved by:
lOn-the-job refresher training every two years for every health functionary.
lEach state will identify core district training teams for each district. This team will move to each block identifying gaps in knowledge and train appropriately,
lMonthly block meetings will provide an opportunity for supervisors to help identify gaps in knowledge and provide some training.
NRHM provides for hiring staff on contract basis. All staff members (medical officers, staff nurses, health workers including ANMs) hired on contract basis will also be trained. ANM and ASHA vacancies will be filled up by the states on urgent basis.
A stronger immunization program will also be used as a platform to deliver other child health services in an integrated manner. Preventive child health interventions like Vitamin A, deworming, ORS, growth monitoring can also be given along with immunization. A well-functioning RI program will act as a catalyst in getting more people to use the health facility and contribute to overall demand generation and better address equity issues.
4. Hire and train more field level staff under NRHM
5. Promote integrated delivery of different health interventions through UIP
Expected Result 5.2: Ensure that adequate financial resources are available for UIP.
Strategies
A core team for immunization financing named Financial Management Group (FMG) has been established within the MoHFW. Using tools that are already available, this team wil l analyze cur rent and projected immunization costs factoring in the plan for scale up and introduction of newer vaccines in the coming years. These will be compared to projected finances available and funding gaps will be highlighted.
The country will be expanding the VPD and AEFI surveillance, which will require a well-functioning laboratory network. A mechanism for the separate budgeting mechanism will be devised for the strengthening of the laboratory and surveillance mechanism in the country
Expected Result 5.3: Improve program accountability, monitoring and reporting at all levels.
Strategies
Quarterly review meetings will be held at national and state level; and monthly meetings at district and block levels to track the progress in immunization program, to identify problems, analyze the issues and address them. State-level meetings will be chaired by State Secretary/MD-NRHM and district-level meetings will be chaired by the DM.
1. Prepare a national financial sustainability plan
2. Provide funding for laboratory strengthening and surveillance
3. Explore the possibility of setting up a Vaccine Fund through innovative financing mechanisms
1. Hold regular program reviews at all levels
U I P S T R A T E G I C P L A N F R A M E W O R K
4 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Comprehensive EPI reviews will be held in the good and poor performing states to help prepare state specific action plan.
MoHFW will develop a monitoring and accountability tracking framework for UIP that will identify key program indicators and assign responsibility of delivering results on specific individual or organizations
At the service-delivery level, more formal, institutionalized systems for complaint and redressal should be put in place. They must be supported by timely emergency response systems, such as telephone helplines, and proper managerial authority should be granted so that structures are in place to rectify acute cha l l enges r e l a t ed to r e f e r ra l and transpor tation or the mistreatment/ exploitation of patients at the facilities. A formal system to lodge complaints and seek redress should also provide oversight to help protect women who register complaints, from future re pr i sa l s. The demonst ra ted initiatives/innovation for accountability, for instance call center for integrated grievance handling system, can be considered.
The Mother and Child Tracking System (MCTS) is designed to collate information of all pregnant women and infants into a central database to ensure that all pregnant women and children receive full maternal and immunization services. This centralized database will enable functions like data analysis, report generation, and therefore contribute to greater strategic decision-making and need-based allocation of resources. It will act as a feedback system for health workers like
2. Develop national monitoring and evaluation plan for immunization
3. Formalize and make accountability mechanisms system-led as part of community participation
4. Expand the usage of Mother and Child Tracking System (MCTS) to all districts to help reduce the gap between reported and evaluated coverage
Auxiliary Nurse Midwives and ASHAs and will enable better health service delivery by drawing out action plans for health workers for ante-natal care, pre-natal care and child immunization. MCTS will also generate reports such as facility service statistics and Auxiliary Nurse Midwife monthly action plans. Currently the states aggregate the relevant data in a Microsoft Excel template available on the HMIS portal. MCTS has been fully operational since April 2010 and has picked up speed in terms of usage by states and union territories as of 1 April 2011. Under this system, SMS alerts are sent to pregnant women who are nearing the delivery date to remind them of the need to visit the PHC for pre-natal check-up and delivery. Women are also reminded over the cell phone on the due dates for immunization of their children to ensure follow through with RI. Bring out annual reports on UIP as part of a strengthened HMIS at state and district level.
The scope of the Quality Assurance (QA) system is now enhanced to include the full range of RMNCH+A services. For rolling out QA system, organizational arrangements will be set up at various levels with clearly defined roles and responsibilities for each level. These will include
(1) Central Quality Supervisory Committee;
(2) (2a) State Quality Assurance Committees, (2b) Quality Assurance Cell and
(2c) Full time quality assessors;
(3) District Quality Assurance Committees; and
(4) Quality Circles at the District Hospital level.
The central QA team will comprise technical officers from the program divisions of the Ministry of Health and Family Welfare and
5. Introduce the Quality Assurance (QA) system for immunization services as part of RMCH+A

................................
4 5
counterparts working with technical support partners. The QA standards will be defined for each technical theme, categorized by the level of health facilities.
Expected Result 5.4: Strengthen RI program management and service delivery through field level supportive supervision in high priority states
To achieve immediate and sustainable improvement in RI coverage at national level, the Government of India needs to focus on high priority states, Rajasthan, Madhya Pradesh, Uttar Pradesh and Bihar, which have the maximum number of unimmunized and par t ia l ly immunized ch i ldren . The RMNCH+A strategic approach recognizes the need to strengthen supportive supervision of frontline workers (ASHAs and ANMs) and service providers (Staff Nurses and Medical Officers) in order to bring about integration of primary care services, improve quality, enhance skills and skill application.
Strategies
To support the implementation and monitor the activities at the district level, there will be a State Level Supportive Supervision Team consisting of officers from the state health department, partners and students and Staff of Medical Colleges (Department of Community Medicine). Each state officers or medical college team will support and monitor 4 to 5 districts for implementation through regular visits, and help establish a link between districts and the state. It will establish State and district RI supportive supervision team. The mobility support will come from NRHM.
At the district level the supportive supervision team will consist of selected medical officers, senior supervisors, medical college staff to support PHC/planning unit. Each member of supportive supervision team including medical college staff will be responsible for two PHC or
1. Augment HR for supportive supervision and program management
planning units, and would visit each unit twice a month (total four visits in a month). S/he will provide regular supportive supervision services to the unit as well as the vaccinators in the area.
Skill building of ANMs is required for ensuring supportive supervision of ASHAs (and AWWs). While ANMs do perform supervisory functions informally, their skills in supportive supervision are limited and need to be enhanced on this specific issue.
The supportive supervision by Institute of Child Health in Tamil Nadu has led to significant improvement in quality of maternal-newborn care in eight districts. A similar engagement of Medical College faculty in other districts and states would be a useful strategy. The technical expertise available with the partners will be utilized to impart knowledge to the state and district level staff.
State-level mechanisms will be strengthened to monitor the program, and guide the districts to improve, implement and monitor the program.
a) Quarterly review meeting will be held at the state for all DIOs and District RI managers
b) Monthly meetings will be held between State and District Task Force meeting
c) Monthly review meetings will be held at the district for all block and PHC medical officers in charge and RI coordinators
d) All supportive supervision checklists will be collected at the district level, and entered into software. This data will be sent to the state for compilation and subsequently the state will send the data sheets to the national
2. Leverage expertise and experience of development partners and medical colleges
3. Establish an institutional mechanism for program oversight and monitoring the implementation of supportive supervision model
U I P S T R A T E G I C P L A N F R A M E W O R K
4 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
immunization division.
e) Data will be presented and feedback provided at all the levels (state, division, district and block level) for appropriate action.
State RI cell/RRT members will be trained through Training of Trainer (ToT) by a national team once in a year. District RI team will be trained once a year by the state core team. District RI team shall be responsible for training, providing supportive supervision and implementation of RI activities at the block and PHC level. On-job regular capacity building will take during the visits of Support Team members from the state. District-level immunization off icers f rom par tner organizations will also contribute to the capacity building process.
Block and PHC team members will be trained annually by the team comprising of members of the district team and one of the facilitators from the state. They will also receive on-job training on a regular basis by district immunization facilitators during their visits and review meetings.
These guidelines will be developed as part of the RMNCH+A strategy to further augment the supportive supervision mechanisms.
Result 5.5: Build institutional capacity to promote operational and translational research for successful implementation of UIP
4. Carry out capacity building and on-job training of staff for strengthening RI supervision all level
5. Prepare integrated guidelines and checklists for supportive supervision linking UIP-MNCH (Universal Immunization Program and Maternal, Newborn And Child Health) supervisory mechanism
Strategies:
Areas for OR could include, but not be limited to, HR training in immunization, operational aspects of cold chain system, vaccine freezing, vaccine wastage, injection safety, barriers to service access and utilization.
A leading research organization may be identified to work in collaboration with immunization division and other stakeholders
Funds will be ear-marked and sufficient amount will be ensured for operational research and implementation in UIP.
National immunization cell will seek to avoid long time lag between conducting research and translating the findings for advocacy, communication and UIP interventions. Technical expertise of partners working on immunization shall be availed as and when required.
Key Performance Indicators (KPI)
1. No wild polio virus detected in the country
2. Non Polio AFP rate is maintained or
1. Define areas for Operational Research and mechanisms for translating evidence-based approaches into program service delivery
2. Evolve institutional mechanism for operational research
3. Ensure sufficient funding for operational research
4. Ensure adequate knowledge management and translation for greater public good
KEY OBJECTIVE 6: Contribute to global polio eradication, measles and maternal and neonatal tetanus elimination and rubella control

................................
4 7
exceeds 2 per 100,000 children under 15 years
3. Reported AFP cases have two adequate stool specimens collected within 14 days of onset of paralysis in > 80% cases
4. Number of States with MCV 1 coverage of > 90%
5. Number of States with MCV-2 coverage of> 90%
6. % of districts with >80% TT2 coverage for pregnant women
The indicators will be disaggregated by gender, geography (urban slum, urban, rural) and socio-economic parameters, where relevant.
Expected Result 6.1: Achieve country-wide certification of polio eradication by 2014
Strategies
The polio eradication program and the polio endgame strategy shall continue to be guided by India Expert Advisory Group constituted by
33the Government of India.
Conduct regular supplementary immunization activities (SIAs), ensure that the SIAs maintain good qua l i t y and conduc t r egu la r seroprevalence surveys to detect immunity levels. The plans for SIAs to be conducted in the coming two years are as below
SIAs for the remainder of 2013
As per current national plans, three large scale SNIDs with bOPV, targeting all of UP, Bihar, Delhi and associated high risk areas of Haryana, Rajasthan, and Uttarakhand, and migrant/high risk areas in Maharashtra, Punjab, Gujarat, Jharkhand, and West Bengal.
1. Maintain high level of population immunity
Polio SIAs in 2014
lTwo NIDs with tOPV in all areas in 1st quarter of 2014
lThree SNIDs with bOPV, ideally one in each of quarters 2, 3, and 4 of 2014 targeting all of UP, Bihar, Delhi, and associated high risk areas of Haryana, Rajasthan, and Uttarakhand, and migrant/high risk areas in Maharashtra, Punjab, Gujarat, Jharkhand, and West Bengal.
Polio SIAs in 2015
lTwo NIDs with tOPV in all areas in 1st quarter of 2014
lTwo to three SNIDs with bOPV (depending on global epidemiology) targeting all of UP, Bihar, Delhi, and associated high risk areas of Haryana, Rajasthan, and Uttarakhand, and migrant/high risk areas in Maharashtra, Punjab, Gujarat, Jharkhand, and West Bengal.
The timing of sub-national rounds should be at the discretion of the national program and based on operational and epidemiological considerations
An extremely high level of vigilance will be maintained through to global certification of eradication, and through to cessation of use of oral poliovirus vaccines; this requires ensuring that adequate financial and human resources and attention are devoted to the surveillance and laboratory systems by the Government of India and partners.
Regular field reviews of surveillance would continue to be conducted on a rotational basis and with particular attention to high risk areas as determined by epidemiological, surveillance or immunization indicators.
2. Maintain the quality and effectiveness of the existing surveillance and laboratory systems to detect and respond to outbreaks
33http://www.npspindia.org/advisory.asp
U I P S T R A T E G I C P L A N F R A M E W O R K

4 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Environmental surveillance for detection of polioviruses in the sewage would be expanded in other states of the country. All detected VDPVs would continue to be thoroughly investigated to determine any risk of circulation, and appropriate actions taken based on investigation findings.
The Emergency Preparedness and Response Plans (EPRPs) at national and state-levels will be updated annually; the update will include a full new risk analysis to inform risk mitigation measures. See Annex 7 for EPRP details.
A simulation exercise ('table top exercise') for the emergency response plans at national and selected state levels will be conducted annually to maintain readiness and sharpness of response. Government of India will ensure a rolling stock of 40 million doses of bOPV and 10 million doses of tOPV to enable response to any wild poliovirus or vaccine derived poliovirus detection.
Immunization of travelers at land border crossing points from neighboring countries is the most significant risk reduction strategy and will continue until there is no longer an epidemiological risk. Particular attention should continue to be paid to border populations to ensure that they are effectively covered by SIAs and routine immunization.
The Government of India will strongly promote implementation of the current WHO p o l i o i m m u n i z a t i o n a d v i s o r y
3. Augment the current response capacity by developing a national and state-level emergency response preparedness plan and maintain a rolling stock of bOPV and tOPV
4. Reduce risks of polio importation based on WHO recommendations for travelers coming to or from endemic or infected areas
/recommendations for travelers to and from endemic or infected areas.
The Government of India will develop the inventory of all labs holding polio virus(phase 1) and securing the WPV (phase 2).
This includes planning for tOPV/bOPV shift, IPV introduction process, and operational assessments of the cold chain system.
These sero-surveys will be conducted in the traditionally high risk areas of UP and Bihar and other regions with potential risk of wild poliovirus importation or emergence of circulating vaccine derived poliovirus. This will provide an epidemiological description of the trends on population immunity and possible reasons for these trends.
Expected Result 6.2:Achieve measles elimination and control for rubella/congenital rubella syndrome (CRS) by 2020
Strategies
The first-dose Measles Containing Vaccine (MCV1) at 9-12 months is delivered through Routine Immunization. Efforts will be made to improve coverage with MCV1 by strengthening RI services with a target to reach all children. In addition follow-up campaigns will be conducted in low coverage areas. It will be ensured that the coverage in every district is more than 90 percent and progress is sustained.
5. Work towards the certification process
6. Develop post-eradication policy in preparation for the polio endgame
7. Conduct periodic seroprevalence studies in high priority areas.
1. Increase coverage with the first dose of measles vaccine for infants (9-12 months)

34A Guide to Introducing a Second Dose of Measles Vaccine into Routine Immunization Schedules. 2013. World Health Organization, Measles and Rubella Initiative.
................................
4 9
2. Increase the coverage of second dose of measles vaccine (at 16–24 months of age) based on global guidelines
3. Strengthen and expand the laboratory surveillance for measles and rubella
1. Strengthen service delivery and improve institutional deliveries
34
Conduct measles SIAs in 14 states where MCV 1 coverage is below 80 percent vaccinating all children in age group of 9 months to 9 years. All states where MCV1 coverage was more than 80 percent have already introduced MCV2 in routine immunization at the time of DPT booster 1.
Twice yearly state-by-state review of all measles data will be conducted. The laboratory-based measles and rubella surveillance has started in eight states, namely Andhra Pradesh, Gujarat, Karnataka, Kerala, Tamil Nadu, West Bengal, Rajasthan, Madhya Pradesh, Bihar and Assam. The surveillance laboratory network will be further expanded with priority being given to the states with measles morbidity and mortality. In addition, surveillance data on measles outbreak from IDSP will also be collated and analyzed for action.
Expected Result 6.3: Eliminate maternal and neonatal tetanus by 2015
Strategies
Promote institutional delivery and safe delivery by skilled birth attendants (SBA) under NRHM and ensure that TT is offered at all ante-natal clinics and routine immunization sessions. Provide twoTT doses for the first pregnancy (with immunization card) and further doses according to the national schedule. The tetanus vaccine for pregnant
mothers will also be ensured in all outreach sessions being conducted.
Establish MNT as a reportable disease and report MNT cases from every health facility. MNT will be included with weekly AFP in active surveillance and zero reporting. Case investigations for hospital-based cases and the cases from low-risk areas are regularly done.
Improve TT coverage through quality RI in all areas. SIAs may be considered for those areas where coverage with 2 doses of TT is poor. The Government of India will take need-based decision to conduct targeted SIA for elimination of MNT. The mode and time for these SIAs will be decided by an expert group.
A national MNT database will be established with regular review of indicators, identifying high-risk districts within states. The high-risk districts within states will be validated for elimination of MNNT by Lot Quality Assurance Surveys (LQAS) and districts prioritized on the basis of this for targeted corrective action.
In states where MNT has been validated to have been eliminated, efforts will be made to maintain the high coverage with TT2, and safe delivery practices to ensure the elimination status in those states.
15 states have validated MNT till 2008, and four more states have conducted MNT validation exercise in 2013. The remaining states and UTs will be assessed in 2014–2015.
2. Increased surveillance for tetanus cases
3. Conduct targeted SIAs
4. Establish national MNT database
5. Maintaining the elimination status
U I P S T R A T E G I C P L A N F R A M E W O R K

5.1 Rationale
lThe Universal Immunization Program (UIP) in India uses a set of indicators to measure the performance at national as well as other levels of program implementation. For this purpose, the country uses various data sources that include:
lRoutine administrative reporting,
lReports from various disease surveillance systems and field level monitoring by partners,
lPeriodic Coverage Evaluation Surveys (CESs) at national and sub-national level,
lVarious assessment studies conducted from time-to-time by different organizations.
Despite the availability of multiple sources of data, there is no comprehensive independent UIP Monitoring & Evaluation (M&E) Plan in the country to
lsystematically identify data needs as well as data sources to meet dynamic program requirements,
lreview the process of data gathering,
lconduct Data Quality Assessments (DQAs).
In the absence of this plan, there is also no mechanism to identify information gaps, especially to measure process indicators, and plan targeted studies to inform the program. Though there are provisions for immunization program reviews at all levels, these are not regular and are not effective in the absence of a real-time quality data.
................................ 5 1
5
5.2 Objective
5.3 Methodology
I. Strengthen routine data reporting
The overall objective of this National Monitoring and Evaluation (M&E) Plan is to systematically generate, capture and disseminate knowledge to guide UIP implementation monitoring and UIP impact evaluation.
This monitoring and evaluation plan will work at three levels:
Currently UIP does not have its own electronic data management system. The Health Management Information System (HMIS) captures immunization data from the health facility-level and the Mother & Child Tracking System (MCTS) tracks ante-natal and immunization services at the individual pregnant woman and child level. The National Monitoring and Evaluation Plan will aim to strengthen these existing data reporting systems through the following mechanisms:
a) Structured Review Mechanism
There is currently limited use of HMIS and MCTS data sets for analyzing and reviewing program implementation and for providing feedback to the concerned districts or blocks. The proposed monitoring and evaluation plan will establish a structured review mechanism in the country to enhance the use of immunization data and to further improve data quality.
National Monitoring And Evaluation Plan For UIP

5 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
b) Human Resource & Capacity Building
A core part of the plan is to improve monitoring and evaluation human resource capacity through trainings, supportive supervision, mentoring, and providing guidelines and tools.
c) Data Quality Assessments (DQA)
DQAs will be conducted regularly in coordination with state governments and with the support of technical and development partners. State Immunization Managers will also be trained in conducting these DQAs by using WHO DQA tools.
d)Feedback to program managers
Data quality will be improved by examining the immunization information system in operation at all administrative levels– from data collection at the point of vaccination, to the periodic compilation of data at the national level. Practical feedback will be provided to managers on how to improve the quality of their administrative immunization reporting systems.
Knowledge gaps identified through routine program monitoring and reporting will be filled by targeted studies and operational research. The results from these research activities can help the UIP in taking ongoing corrective measures for better outcomes. The monitoring and evaluation plan will also include regular audit at facility and service level using WHO tools and provide feedback to program managers for strengthening the facilities and services.
Currently, evaluation surveys conducted in the country address all MCH services, and the immunization component is limited only to antigen-wise and full immunization coverage. Moreover, these surveys are done every three to
I. Conduct targeted studies and field assessments to fill knowledge gaps in the program
II. Plan and conduct coverage evaluation studies
four years, and do not provide latest coverage numbers on a yearly basis. The monitoring and evaluation plan will propose a yearly evaluation survey for routine immunization, focusing on outcome and impact indicators of all RI components. This can be done through external agencies, in line with NFHS and DLHS surveys.
MOHFW will guide the development of the national monitoring and evaluation plan. The Monitoring and Evaluation division of Immunization Technical Support Unit (ITSU) will coordinate the development of the plan. ITSU will hire a consultant to work on the plan after consultation with ministry and technical partners for the scope. The consultant will work closely with ITSU team and, in consultation with all stakeholders including states, with the aim of creating a realistic, expedient and effective national monitoring and evaluation plan for the UIP.
The National Monitoring and Evaluation plan will be developed in line with the cMYP and five-year plan of the country. The proposed national monitoring and evaluation plan will cover all major areas for establishing and running an effective monitoring and evaluation system in the country. These include:
lOrganizational structure along with roles and responsibilities for monitoring and evaluation at various levels
lPlan for capacity building of monitoring and evaluation staff on transmission, analysis and use of data at all levels
lKey coordination mechanisms for the country
lImmunization monitoring and evaluation performance and accountability tracking framework and implementation plan at national and state level (see Annex 6)
5.4 Process for national M & E Plan development
5.5 Components of National Monitoring and Evaluation Plan

................................ 5 3
ANNEXURES
6


................................
5 5
ANNEX 1: List of states showing good performance on immunization coverage and other parameters
States
Andhra Pradesh
Delhi
Goa
Haryana
Himachal Pradesh
Jammu & Kashmir
Karnataka
Kerala
Maharashtra
Punjab
Tamil Nadu
Mizoram
Sikkim
Tripura
Uttarakhand
West Bengal
Full immunization coverage (%)
68.0
71.5
87.9
71.7
75.8
66.6
78.0
81.5
78.6
83.6
77.3
73.7
85.3
66.0
71.5
64.9
No. of sub-centers without
ANM/HW*
0
0
0
N/A
178
N/A
N/A
0
N/A
N/A
140
N/A
0
0
34
N/A
Mos trained
(%)
93.7
55.5
93.7
72.8
4.0
7.3
44.8
50.5
51.8
95.8
82.2
48.3
75.0
30.0
19.5
19.7
Sessions held vs. planned
(%)**
N/A
92.8
99.2
93.9
98.2
90.5
95.4
N/A
80.2
95.1
99.1
66.7
N/A
92.9
91.8
91.6
Dropout rates in age
group12-23 months for
BCG- measles (%)
8.3
6.5
1.4
5.3
2.2
9.4
7.4
8.3
3.7
9.6
0.6
7.3
0.1
7.3
14.2
13.6
No. of severe AEFI cases reported***
21
12
4
10
3
N/A
9
1
71
4
5
N/A
N/A
4
1
28
Children aged 12-23 months
having an immunization
card (%)
64.9
50.7
60.6
42.7
60.3
60
52
78.9
58.8
53.2
44.8
77.9
85.2
75.9
41.1
77.8
* Collated data from state review meetings on immunization obtained from MoHFW, GoI.* * Data from the HMIS web portal April to October, 2011; ** *Severe AEFI cases reported to the Government of India by the states till mid-December, 2011;
A N N E X U R E S

5 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
States
Arunachal Pradesh
Manipur
Meghalaya
Nagaland
Assam
Bihar
Madhya Pradesh
Orissa
Rajasthan
Uttar Pradesh
Chhattisgarh
Gujarat
Jharkhand
Full immunization coverage (%)
24.8
51.9
60.8
27.8
59.1
49.0
42.9
59.5
53.8
40.9
57.3
56.6
59.7
No. of sub-centers without
ANM/HW*
N/A
N/A
0
0
0
200
119
535
392
1,776
458
488
0
MOs trained
(%)
43.8
49.4
93.4
40.1
84.7
18.3
32.5
44.9
33.4
32.1
8.7
24.7
36.3
Sessions held vs. planned
(%)**
81.5
89.6
80.8
93.7
97.4
95.1
96.1
96.0
113.9
89.8
90.3
97.2
94.4
Dropout rates in age group 12-23 months
for BCG- measles (%)
27
12.9%
9.4
11.5
7.2
29.3
24
17.6
20.6
30.9
13.8
8.1
22.8
No. of severe AEFI cases reported ***
N/A
N/A
3
N/A
7
19
8
5
3
21
N/A
3
11
Children aged 12-23 months
having an immunization
card (%)
41.9
55.6
63.8
45
66.9
43.1
45.8
58.3
24
35.9
46.3
49.5
63.1
ANNEX 2: List of States showing poor performance on immunization coverage and other parameters
*Collated data from state review meetings on immunization obtained from MoHFW, GoI. **Data from the HMIS web portal April to October, 2011;***Severe AEFI cases reported to the Government of India by the states till mid-December, 2011

adequate space in the unused portion of the Animal House for the establishment of NCCVMRC. UNICEF has supported the establishment by hiring an architect to prepare the plans and estimates for remodeling of the existing building of the Animal House. Immunization Division has provided five tool kits for the training center. NIHFW has already conducted a six days pilot Training for Cold Chain Technicians in Repair and Maintenance of ILRs and DFs from 17-22 October 2011 using alternate temporary space made specifically available for the training.
The Resource Centre will be set up to train cold chain mechanics in repair and maintenance of all electrical cold chain equipment (ILRs, DFs, WICs, WIFs and voltage stabilizers). In addition, it will also conduct trainings related to vaccine and logistics management for vaccine and logistics managers in the country. It is expected to make it a cold chain training center for other countries in South-east Asia. In addition to trainings, NCCVMRC will be a repository of documents such as guidelines, government orders/notifications and other resource materials related to cold chain and
Brief about resource centre
Establishment of national cold chain and vaccine management resource centre and nihfw, new delhi
BACKGROUND
The Immunization Division, MOHFW, New Delhi has proposed to establish a National Cold Chain and Vaccine Management Resource Centre (NCCVMRC) at NIHFW, New Delhi and it has been approved by the competent authority of MoHFW, Government of India (Annexure A). Further it has been intimated that NIHFW may utilize any MOHFW, GoI funds available or the proposal estimates be provided for necessary approvals from the competent authority. MOHFW, GoI shal l suppor t the es tabl i shment of NCCVMRC, trainings of officials from Central/state Governments related to cold chain equipment, vaccine and logistics management, etc. and the human resources needed for the trainings on regular and /or contractual staff and all other expenses related to the Training Centre. The necessary technical support will be provided by UNICEF.
National Institute of Health and Family Welfare, New Delhi has on its part demarcated
................................
5 7
ANNEX 3: NCCVMRC concept approved by MoHFW
ESTABLISHMENT OF
NATIONAL COLD CHAIN AND VACCINE MANAGEMENT
RESOURCE CENTRE (NCCVMRC)
PROPOSAL ESTIMATES
IMMUNIZATION DIVISION,
MINISTRY OF HEALTH AND FAMILY WELFARE, NEW DELHI
AT NATIONAL INSTITUTE OF HEALTH AND FAMILY WELFARE, NEW DELHI
(With blueprint)
Submitted to
By
National Institute of Health and Family Welfare, New Delhi
A N N E X U R E S
5 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
vaccine management. The soft copies will be on the resource centre website and hard copies will be maintained in a small library in the centre.
The resource center will be set in the unused portion (earlier Primate Section) of the Animal House. There will be a Lecture Room, a work lab (for repair of ILRs and DFs) and a room for housing a Walk in Cooler and a Walk in Freezer. In addition, there will be an administrator's room and a facilitator's room as well as a store room. The ingress will be separate from the animal House with adequate accessibility for heavy vehicles (for loading and unloading of cold chain equipment).
A training coordinator, an assistant and a support staff are the human resources needed for the resource center. MoHFW has agreed to support in hiring of the training coordinator and support staff from NIHFW can be deputed to work in the resource center. UNICEF may also initially support the hiring of technical staff.
The following are the different types of trainings to be undertaken at the NCCVMRC, New Delhi:
1. Training for Cold Chain Technicians in Repair and Maintenance of ILRs and DFs
2. Training for Cold Chain Technicians in Repair and Maintenance of WICs and WIFs
3. Training on repair and maintenance of voltage stabilizers
4. Training on installation and repair of Solar cold chain equipment.
5. Training for Vaccine and Cold Chain Handlers
6. Training on Vaccine Management
There are more than 500 cold chain technicians and vaccine logistics managers in the country. Some of these are newly inducted have had no induction training. Many of the older refrigerator mechanics need refresher trainings for which such a course will be designed separately. Therefore the establishment of the NCCVMRC is justified.

................................
5 9
– Procurement Policy for CCE
– Institutional Capacity Building of NCCTC and NCCVMRC
– Greater role of NCCTC and NCCVMRC for CCVLM
– Review Mechanism of CCVLM
l Induction Training of HR engaged for Cold Chain and VM
l Improvement of management skills of program managers
lDedicated staffs for CCL at all level (at least up to district)
lEach GMSD and SVSs need to have VLM and CCT
lSome of the existing staffs of GMSD can be profiled for Data management
lCold rooms should have some semiskilled helpers
lDevelop Training package for the VLMs and also for the Immunization program managers and house them in the institution to overcome attrition
lReview of Knowledge (Training) to skills transformation barriers
lRegular orientation, at least every 3 years for all staffs
A.Building
lDedicated stores for State, Division, District
2. Human Resource and capacity building
3. Infrastructure
The recommendations are categorized in to five broad categories “Management Policy, Human Resource and capacity building, Infrastructure, Planning and Documentation and improvement in practice and development of an improvement plan to implement these recommendations through NRHM state PIPs.
lIntroduce VAR for Vaccine stores up to Sub National level
lDevelop and implement real time MIS for Vaccine Logistic Management for 5 levels of supply chain.
lIntegrate vaccine management MIS with NCCMIS
lAccelerate NCCMIS implementation for GMSDs
lSegregate all SVSs attached to RVS and RVSs attached to DVS: Building, equipment, documents and Staff.
lDevelop National Cold Chain action Plan
– Develop National standards for:
lVaccine store at all levels as per WHO standards
lCold Chain point expansion guidelines
lCold Chain Equipment plan for different level of vaccine stores
lQuality maintenance of vaccine
lTemperature Monitoring of cold chain system
lHuman resource for Cold Chain and VM
lCCE Testing Lab
1. Management Policy
ANNEX 4: Key Recommendations from Effective Vaccine Management Assessment Report 2013
A N N E X U R E S

6 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
and Health Facilities(PHC),
lConsider the future need, national standard
lGreater collaboration with PWD, Electricity and Municipal corporation/bodies for regular maintenance
B.Equipment
lEquipment specification as per global standards
lMinimize variety of equipment to reduce number of spare parts
lAll WIC/WIF with working hooters
lMapping of spare parts and ensuring availability to make non-functioning equipment (Solar, Haier, Blue star, others)functional
lDefine realistic stock level in months at five supply chain level
lDefine, print and distribute standard vaccine stock registers
lVaccine indent and distribution plans based on the required peak stocks.
lPreventive maintenance plan for technicians
lRegular data uploading in NCCMIS for performance assessment of CC at all level
lEstablish a system for recording wastage in vaccine registers
lManual temperature monitoring and recording to be carried out 2 times daily, for all 7 days including holidays
lMaintain a service log sheet for each equipment. This can be done as part of the
4. Planning and Documentation
5. Improvement in Practice
Temperature monitoring booklet.
lDiluents MUST be marked in supply voucher and should be recorded just like the vaccines in stock registers.
lAt CHC and PHC the DF must be used exclusively to prepare ice packs. Vaccines must never be stored in the same unit. All vaccines should be kept in ILRs at the CHC and PHC.
lAlways use standardized Ice Packs after conditioning
EVM is a diagnostic tool and it assess, 3 Ps like Process, Practices and Policies of health system requires for efficient cold chain and vaccine management.
Improvement Plan(IP )is the intervention for Strengthening of existing Cold Chain and Vaccine Logistics System to make it Reliable ,Affordable and Efficient. Issues identified through EVM needs to be fixed and to be sustained success of the EVM initiatives lies in developing an implementable improvement plan and then actually implementing the IP and reviewing the IP on the regular basis for strengthening the Cold chain logistics system. While EVM is a diagnostic tool, IP lay down the treatment strategies for the gaps in the CCL system. Development of an improvement plan is the key output that comes from the EVM assessment and its recommendations. While a skilled facilitation is needed to make sure that the plan does indeed address key deficiencies, it should be possible to provide a menu of innovative approaches and technologies for consideration, guided by country realities. A menu of innovations approaches is included in the Improvement Plan to guide planning for future system design and to enhance monitoring of the implementation of the plan. While planning, guiding principles that need to be considered for an ef fect ive and implementable IP are:
6. Improvement Plan (IP)
................................
6 1 A N N E X U R E S
lIntegration with other planning processes
lIP template should be adapted by government to align with existing planning and budgeting documents
o IP should be consistent with and input into other planning documents such as cMYP, national and sub-national annual work plans, etc.
lDynamic and living document
lPlan that needs regular review and monitoring for implementations of recommendations IP need to be prepared through consultative process and it should be integrated annual health PIP.
lGovernment ownership
lPlan which need to be reviewed regularly for progress of implementation
lEngagement of all levels
lDisseminate widely , leveraging existing mechanisms
lMake IP foundational plan for improving immunization supply chain performance
o Identifies priority action areas and establishes accountability for improving performance
o Takes longer-term view and reflects future needs (NVI, population growth, etc.)
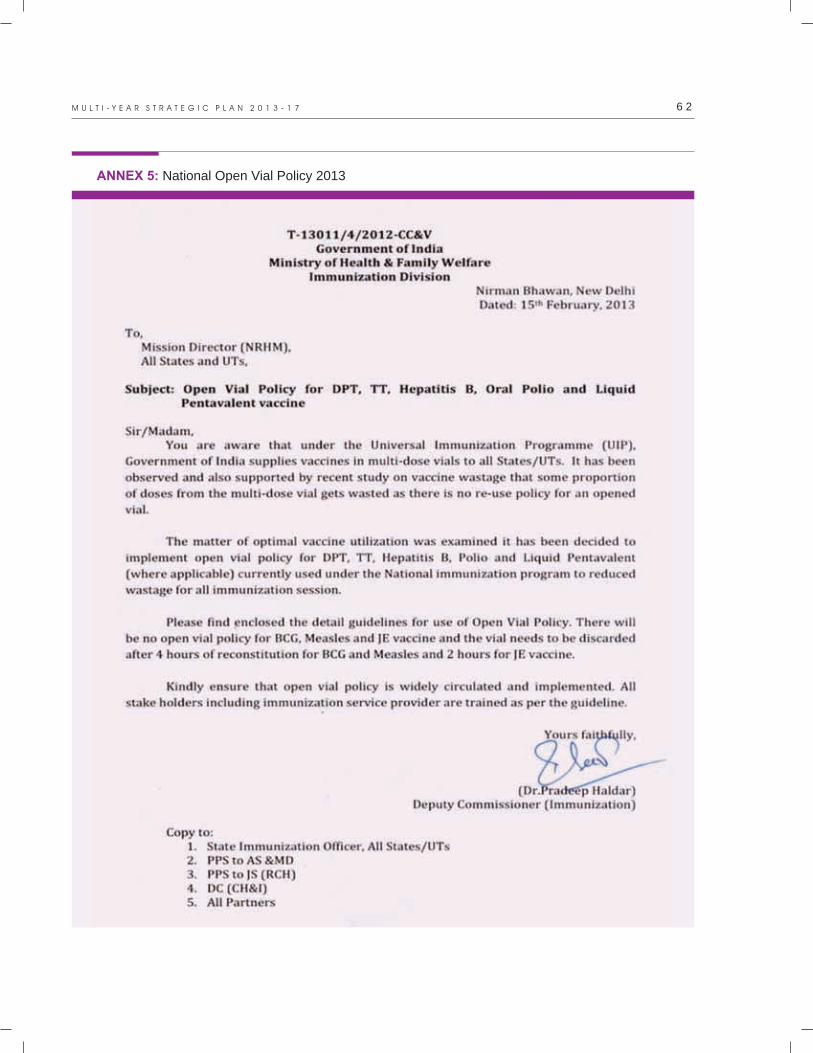
6 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
ANNEX 5: National Open Vial Policy 2013

................................
6 3 A N N E X U R E S
Guidelines for use of open vial in immunization program
Conditions that must be fulfilled for the use of open vial policy:
1. This opened vial policy applies to multi-dose vials of the DPT, TT, Hepatitis B, Oral Polio Vaccine (OPV) and Liquid Pentavalent (where applicable). This policy does not apply to Measles, BCG, Japanese Encephalitis (JE) vaccines.
2. Use the DPT, TT, Hepatitis B, Oral Polio vaccine (OPV) and Liquid Pentavalent (DPT + HepB + HiB) where applicable) vaccines opened in a fixed or outreach session can be used at more than one immunization session up to four weeks provided that:
a. The expiry date has not passed.
b. The vaccines are stored under appropriate cold chain conditions both during transportation and storage in cold chain storage point.
c. The vaccine vial septum has not been submerged in water or contaminated in any way.
d. Aseptic technique has been used to withdraw all doses.
e. The vaccine vial monitor (VVM), has not reached the discard point.
3. Discard vaccine vial in case any one of the following conditions is met:
a. If expiry date has passed.
b. VVM reached discard point (for freeze dried vaccine, before reconstitution only) or Vaccine vials without VVM or disfigured VVM.
c. No label or partially torn label or writing on label is not legible.
d. Any vial thought to be exposed to non-sterile procedure for withdrawal.
e. Open vials that have been under water or
vials removed from a vaccine carrier that has water.
f. If vaccine vial is frozen or contains floccules.
4. Health workers must be able to distinguish between vials that can be used in subsequent sessions and vials that must be discarded. Training and supervision materials should be revised to reflect the policy change.
5. Maintain temperature of ILR between 20 to 80C for storage of vaccines & diluents and monitor temperature twice daily regularly.
6. Note the manufacturer, batch and expiry date of the vaccine and diluent in the stock register.
7. Proper recording and reporting of vaccine distribution and usage has to be ensured.
8. Keep stock up to date, don't over-stock or under-stock vaccines and diluents.
9. Multi-dose vials from which at least one dose has been removed may be at risk of contamination of the vial septum. These vials should therefore, never be allowed to be submerged in water (from melted ice for example) and the septum should remain clean and dry. NOTE: Well-sealed conditioned ice packs should be used in vaccine carriers and water should not be allowed to accumulate where the vials are stored. Vaccine vials must be transported in a plastic zipper bag.
10. Keep the “returned, partially used” vials in a separate box, and label it accordingly.
11.Observe earliest expiry first out (EEFO) policy for issuing vaccines. If the vaccines are of same expiry date, the partially used vaccine vials should be re-issued. The vial opened earlier, as recorded on the vial label, should be issued first.
12. Contingency plan has to be in place in case
Cold chain maintenance and vaccine distribution

6 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
of any exigency like power failure, equipment breakdown, etc.
13. Inspect for and discard vaccine vial with visible contamination (i.e. checking for any change in the appearance of vaccine or any floating particles) or breaches of integrity (e.g. cracks, leaks).
14. All vaccines vials must be marked with date & time of opening at first use.
15. Note the manufacturer, batch and expiry date of the vaccine and diluent in the tally sheet.
16. Always pierce the septum with a sterile needle for drawing vaccine from the multi-dose vials used. Except oral polio vaccine which is given 2 drops orally, cap needs to be closed after each use.
17. Ensure that the vaccine vials are returned inside a vaccine carrier from the session site to cold chain point immediately after session ends, using the alternate vaccine delivery mechanism in the reverse cold chain.
18. Under no circumstance the vaccine carrier/vaccines will be kept in the field, in case of such an event, the vaccines in such vaccine carriers should be discarded and not used for subsequent sessions.
19. Storage of vaccines at any place other than a designated cold chain point will not be
At and during the immunization session
After immunization session is over
allowed. No vaccines should be stored at ANM/LHV or other health worker/ASHA house.
20.This policy is NOT applicable to opened reconstituted vials of Measles, BCG and JE vaccine, which will be used as per following instructions and discarded immediately after use:
a. Before reconstitution check that vaccine is within expiry date and the VVM has not reached the discard point. Reconstitute the vial ONLY with diluent provided by manufacturer for that batch of the vaccine.
b. Date and time of reconstitution must be mentioned on the label vial at the beginning of session.
c. Reconstituted vials will only be used for a single session; they will not be carried from one session to another, even if the session is close by.
d. BCG and Measles must be discarded within four hours of reconstitution or at end of session whichever is earlier.
e. JE to be discarded after two hours of reconstitution or at end of session whichever is earlier.
21. All vaccines are supplied with VVM. Please note that the VVM has only three status ie (i) start point (ii) end point (iii) end point exceeded. The vaccine has to be use before reaching the end
Specific attention while implementing open vial policy
End point
Square lighter than circle. If the expiry date has
not passed, USE the vaccine.
Square matches the circle. Do NOT use
the vaccine.
Square darker than the circle. Do NOT
use the vaccine.End point exceeded
Start point
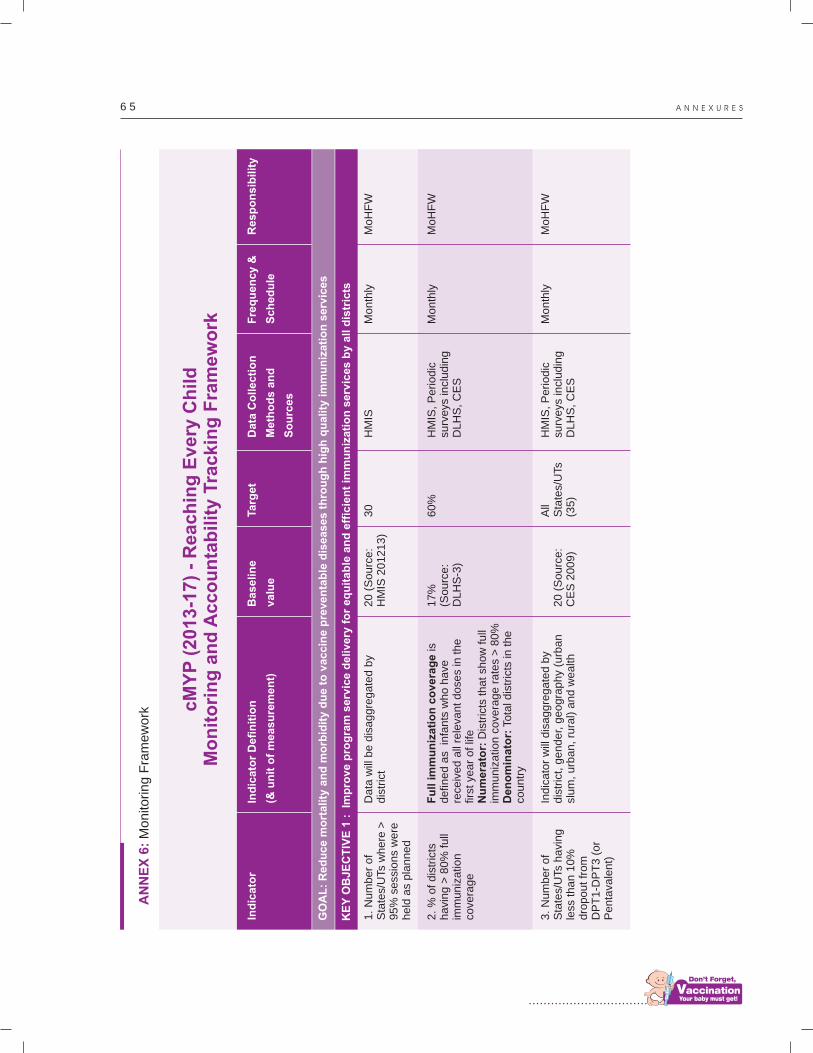
................................
6 5 A N N E X U R E S
AN
NE
X 6
: M
onito
ring F
ram
ew
ork c
MY
P (
2013-1
7)
- R
each
ing
Every
Ch
ild
M
on
ito
rin
g a
nd
Acco
un
tab
ilit
y T
rackin
g F
ram
ew
ork
Data
will
be d
isagg
reg
ate
d b
y dis
tric
t
Fu
ll i
mm
un
izati
on
co
ve
rag
e is
defin
ed a
s in
fants
wh
o h
ave
re
ceiv
ed a
ll re
leva
nt
do
ses
in t
he
fir
st y
ear
of
life
Nu
mera
tor:
Dis
tric
ts t
ha
t sh
ow
fu
ll im
muniz
atio
n c
ove
rag
e r
ate
s >
80
%D
en
om
inato
r: T
ota
l dis
tric
ts in
th
e
countr
y
Indic
ato
r w
ill d
isag
gre
ga
ted
by
dis
tric
t, g
ender,
geo
gra
ph
y (u
rba
n
slum
, urb
an,
rura
l) a
nd
we
alth
20
(S
ou
rce
: H
MIS
20
12
13
)
17
%(S
ou
rce
: D
LH
S-3
)
20
(S
ou
rce
: C
ES
20
09
)
30
60
%
All
Sta
tes/
UTs
(3
5)
HM
IS
HM
IS,
Pe
rio
dic
su
rve
ys in
clu
din
g
DL
HS
, C
ES
HM
IS,
Pe
rio
dic
su
rve
ys in
clu
din
g
DL
HS
, C
ES
Mo
nth
ly
Mo
nth
ly
Mo
nth
ly
1. N
um
ber
of
Sta
tes/
UTs
where
>
95%
se
ssio
ns
were
held
as
pla
nned
2. %
of dis
tric
ts
havi
ng >
80%
full
imm
uniz
atio
n
cove
rag
e
3. N
um
ber
of
Sta
tes/
UTs
havi
ng
less
than 1
0%
dro
pout
from
D
PT
1-D
PT
3 (
or
Penta
vale
nt)
Mo
HF
W
Mo
HF
W
Mo
HF
W
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
GO
AL
: R
ed
uce m
ort
ality
an
d m
orb
idit
y d
ue t
o v
accin
e p
reven
tab
le d
iseases t
hro
ug
h h
igh
qu
ality
im
mu
niz
ati
on
serv
ices
KE
Y O
BJE
CT
IVE
1 :
Im
pro
ve p
rog
ram
serv
ice d
elivery
fo
r eq
uit
ab
le a
nd
eff
icie
nt
imm
un
izati
on
serv
ices b
y a
ll d
istr
icts

6 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Cold
chain
sic
kness
is d
efin
ed
as
-
cold
chain
equip
me
nt
wh
ich
ou
t o
f ord
er
as
a p
erc
enta
ge
of
tota
l equip
ment
pla
ced
Self-
exp
lanato
ry
Self-
exp
lanato
ry
This
will
be im
ple
me
nte
d a
cro
ss t
he
dis
tric
ts B
ihar
and U
P
Self-
exp
lanato
ry
26
(S
ou
rce
: N
CC
MIS
2
01
3/S
tate
re
po
rts)
16
(S
ou
rce
: N
IHF
W R
I tr
ain
ing
sta
tus
rep
ort
)
0 0 0
All
Sta
tes/
UTs
(3
5)
All
Sta
tes/
UTs
(3
5)
5
Sta
tes/
UT
110
d
istr
icts
7 Sta
tes/
UT
NC
CM
IS
Sta
te t
rain
ing
re
po
rts
We
b-b
ase
d
tem
pe
ratu
re
mo
nito
rin
g r
ep
ort
We
b-b
ase
d s
tock
m
on
itorin
g
syst
em
Mo
HF
W
rep
ort
/NC
CM
IS
Mo
nth
ly
Mo
nth
ly
Mo
nth
ly
Mo
nth
ly
On
e tim
e
Mo
HF
W
SIO
SIO
/Mo
HF
W
SIO
/Mo
HF
W
Mo
HF
W
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
EX
PE
CT
ED
RE
SU
LT
1.2
: S
tren
gth
en
vaccin
e a
nd
syri
ng
e lo
gis
tics m
an
ag
em
en
t acro
ss t
he c
ou
ntr
y in
clu
din
g f
ore
casti
ng
an
d
pro
cu
rem
en
t at
cen
tral le
vel
1. N
um
ber
of
Sta
tes/
UTs
where
th
e c
old
chain
si
ckness
rate
m
eets
th
e n
atio
nal
standard
of
< 2
%
2. N
um
ber
of
Sta
tes/
UTs
where
all
cold
chain
sta
ff
are
tra
ined in
cold
ch
ain
and v
acc
ine
manage
ment
3. N
um
ber
of
Sta
tes/
UT
where
te
mpera
ture
m
onito
ring is
bein
g
done w
ith w
irele
ss
data
loggers
for
all
funct
ion
al
ele
ctrica
l co
ld c
ha
in
equip
me
nt
1. N
um
ber
of
dis
tric
ts w
here
real
time v
acc
ine s
tock
m
onito
ring s
yste
m
is im
ple
mente
d
2.N
um
ber
of
Sta
tes/
UTs
that
are
usi
ng c
om
pute
r si
mula
tion m
odel
for
vacc
ine s
upply
ch
ain
ca
paci
ty
pla
nnin
g
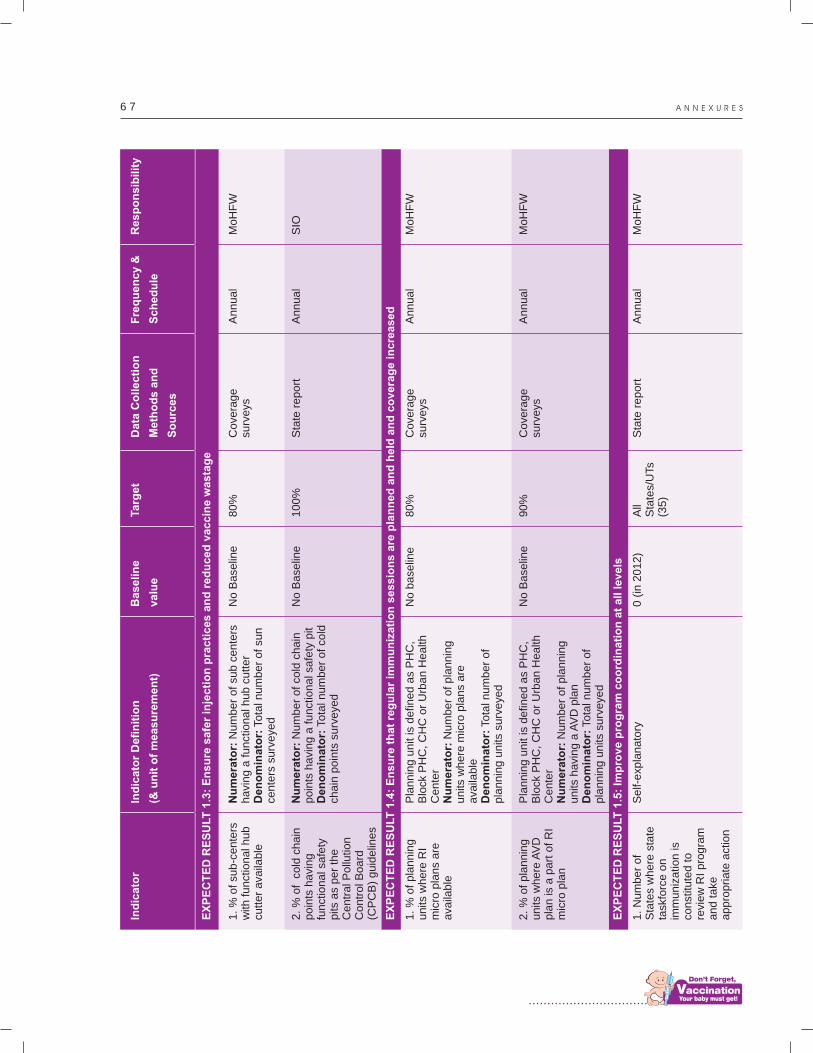
................................
6 7 A N N E X U R E S
Nu
mera
tor:
Num
be
r o
f su
b c
en
ters
havi
ng a
funct
iona
l hu
b c
utt
er
Den
om
inato
r: T
ota
l nu
mb
er
of
sun
ce
nte
rs s
urv
eye
d
Nu
mera
tor:
Num
be
r o
f co
ld c
ha
in
poin
ts h
avi
ng a
funct
ion
al s
afe
ty p
itD
en
om
inato
r: T
ota
l nu
mb
er
of
cold
ch
ain
poin
ts s
urv
eye
d
Pla
nnin
g u
nit
is d
efin
ed
as
PH
C,
Blo
ck P
HC
, C
HC
or
Urb
an
He
alth
C
ente
rN
um
era
tor:
Num
be
r o
f p
lan
nin
g
units
where
mic
ro p
lan
s a
re
ava
ilable
Den
om
inato
r: T
ota
l nu
mb
er
of
pla
nnin
g u
nits
surv
eye
d
Pla
nnin
g u
nit
is d
efin
ed
as
PH
C,
Blo
ck P
HC
, C
HC
or
Urb
an
He
alth
C
ente
rN
um
era
tor:
Num
be
r o
f p
lan
nin
g
units
havi
ng a
AV
D p
lan
Den
om
inato
r: T
ota
l nu
mb
er
of
pla
nnin
g u
nits
surv
eye
d
Self-
exp
lanato
ry
No
Ba
selin
e
No
Ba
selin
e
No
ba
selin
e
No
Ba
selin
e
0 (
in 2
01
2)
80
%
10
0%
80
%
90
%
All
Sta
tes/
UTs
(3
5)
Co
vera
ge
su
rve
ys
Sta
te r
ep
ort
Co
vera
ge
su
rve
ys
Co
vera
ge
su
rve
ys
Sta
te r
ep
ort
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
Mo
HF
W
SIO
Mo
HF
W
Mo
HF
W
Mo
HF
W
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
1. %
of
sub-c
ente
rs
with
funct
ional h
ub
cutter
ava
ilable
2. %
of c
old
chain
poin
ts h
avi
ng
funct
ional s
afe
ty
pits
as
per
the
Centr
al P
ollu
tion
Contr
ol B
oard
(C
PC
B)
guid
elin
es
1. %
of
pla
nnin
g
units
where
RI
mic
ro p
lans
are
ava
ilable
2. %
of pla
nnin
g
units
wh
ere
AV
D
pla
n is
a p
art
of
RI
mic
ro p
lan
1. N
um
ber
of
Sta
tes
where
sta
te
task
forc
e o
n
imm
uniz
atio
n is
co
nst
itute
d t
o
revi
ew
RI
pro
gra
m
and take
appro
priate
act
ion
EX
PE
CT
ED
RE
SU
LT
1.3
: E
nsu
re s
afe
r in
jecti
on
pra
cti
ces a
nd
red
uced
vaccin
e w
asta
ge
EX
PE
CT
ED
RE
SU
LT
1.4
: E
nsu
re t
hat
reg
ula
r im
mu
niz
ati
on
se
ss
ion
s a
re p
lan
ne
d a
nd
he
ld a
nd
co
ve
rag
e in
cre
as
ed
EX
PE
CT
ED
RE
SU
LT
1.5
: Im
pro
ve p
rog
ram
co
ord
ina
tio
n a
t a
ll l
ev
els
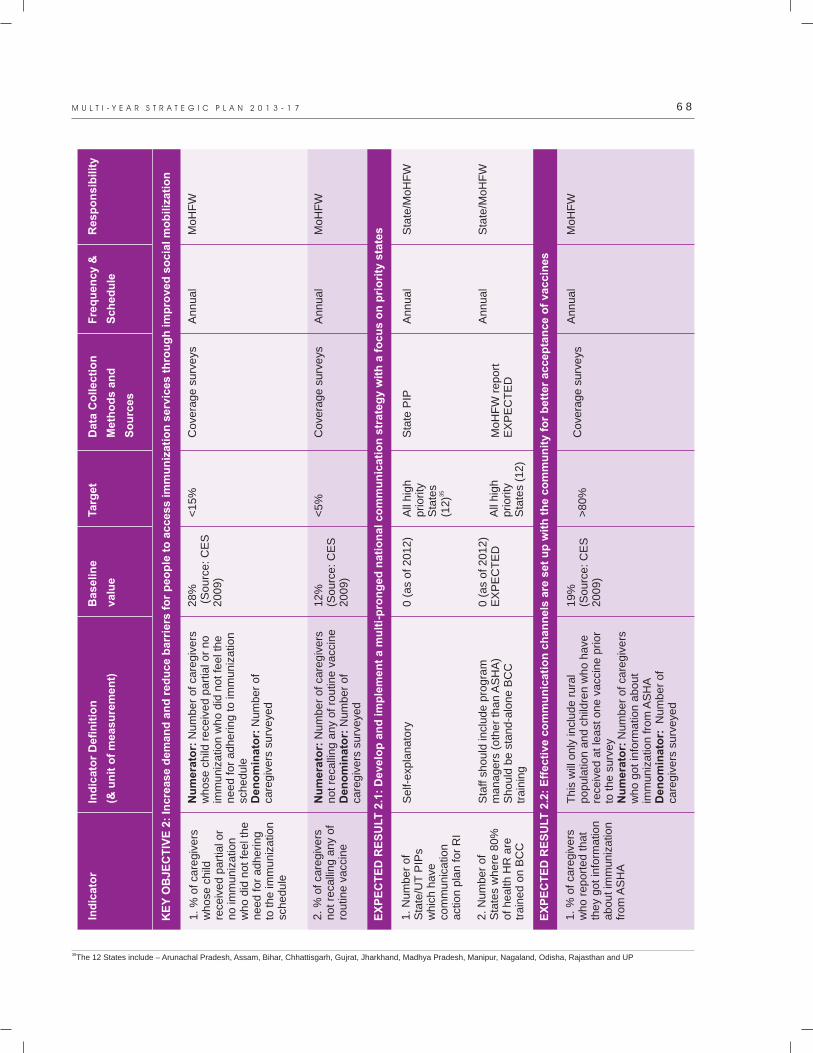
6 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Nu
mera
tor:
Num
be
r o
f ca
reg
ive
rs
whose
child
rece
ive
d p
art
ial o
r n
o
imm
uniz
atio
n w
ho d
id n
ot
fee
l th
e
need f
or
adhering t
o im
mu
niz
atio
n
schedule
Den
om
inato
r: N
um
be
r o
f ca
regiv
ers
surv
eye
d
Nu
mera
tor:
Num
be
r o
f ca
reg
ive
rs
not
reca
lling a
ny
of
rou
tine
va
ccin
eD
en
om
inato
r: N
um
be
r o
f ca
regiv
ers
surv
eye
d
Self-
exp
lanato
ry
Sta
ff s
hould
incl
ud
e p
rog
ram
m
anagers
(oth
er
tha
n A
SH
A)
Should
be s
tand-a
lon
e B
CC
tr
ain
ing
This
will
only
incl
ude
ru
ral
popula
tion a
nd c
hild
ren
wh
o h
ave
re
ceiv
ed a
t le
ast
on
e v
acc
ine
prio
r to
the s
urv
ey
Nu
mera
tor:
Num
be
r o
f ca
reg
ive
rs
who g
ot
info
rmatio
n a
bo
ut
imm
uniz
atio
n f
rom
AS
HA
Den
om
inato
r:
Num
be
r o
f ca
regiv
ers
surv
eye
d
28
% (
So
urc
e:
CE
S
20
09
)
12
%
(So
urc
e:
CE
S
20
09
)
0 (
as
of
20
12
)
0 (
as
of
20
12
)E
XP
EC
TE
D
19
%(S
ou
rce
: C
ES
2
00
9)
<1
5%
<5
%
All
hig
h
prio
rity
S
tate
s 3
5(1
2)
All
hig
h
prio
rity
S
tate
s (1
2)
>8
0%
Co
vera
ge
su
rve
ys
Co
vera
ge
su
rve
ys
Sta
te P
IP
Mo
HF
W r
ep
ort
EX
PE
CT
ED
Co
vera
ge
su
rve
ys
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
Mo
HF
W
Mo
HF
W
Sta
te/M
oH
FW
Sta
te/M
oH
FW
Mo
HF
W
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
1. %
of
care
giv
ers
w
hose
child
re
ceiv
ed p
art
ial o
r no im
muniz
atio
n
who d
id n
ot
feel t
he
need for
adhering
to the im
muniz
atio
n
schedule
2. %
of ca
regiv
ers
not re
calli
ng a
ny
of
routin
e v
acc
ine
1. N
um
ber
of
Sta
te/U
T P
IPs
whic
h h
ave
co
mm
un
icatio
n
act
ion p
lan f
or
RI
2. N
um
ber
of
Sta
tes
where
80%
of health
HR
are
tr
ain
ed o
n B
CC
1. %
of ca
regiv
ers
w
ho r
eport
ed t
hat
they
got
info
rmatio
n
about im
muniz
atio
n
from
AS
HA
KE
Y O
BJE
CT
IVE
2:
Incre
ase d
em
an
d a
nd
red
uce b
arr
iers
fo
r p
eo
ple
to
access im
mu
niz
ati
on
serv
ices t
hro
ug
h im
pro
ved
so
cia
l m
ob
iliz
ati
on
EX
PE
CT
ED
RE
SU
LT
2.1
: D
evelo
p a
nd
im
ple
men
t a m
ult
i-p
ron
ged
nati
on
al co
mm
un
icati
on
str
ate
gy w
ith
a f
ocu
s o
n p
rio
rity
sta
tes
EX
PE
CT
ED
RE
SU
LT
2.2
: E
ffecti
ve c
om
mu
nic
ati
on
ch
an
ne
ls a
re s
et
up
wit
h t
he
co
mm
un
ity
fo
r b
ett
er
ac
ce
pta
nc
e o
f v
ac
cin
es
35The 12 States include – Arunachal Pradesh, Assam, Bihar, Chhattisgarh, Gujrat, Jharkhand, Madhya Pradesh, Manipur, Nagaland, Odisha, Rajasthan and UP

................................
6 9 A N N E X U R E S
Self-
exp
lanato
ry
Mess
ages
as
rele
van
t a
t th
e t
ime
of
surv
ey
Nu
mera
tor:
Num
be
r o
f ca
reg
ive
rs
who c
an r
eca
ll new
imm
un
iza
tion
m
ess
ages/
taglin
e
Den
om
inato
r: N
um
be
r o
f ca
regiv
ers
surv
eye
d
Refe
rence
period: T
ime
ly r
ep
ort
s a
s co
mplie
d o
ver
the p
revi
ou
s o
ne
ye
ar.
Nu
mera
tor:
Num
be
r o
f se
ntin
el
site
s pro
vidin
g t
imely
an
d c
om
ple
te
report
s on 9
0%
occ
asi
on
Den
om
inato
r: A
ll se
ntin
el s
ites
Self-
exp
lanato
ry
Does
not
incl
ude P
olio
wo
rksh
op
s
0 0%
0%
(a
s o
f 2
01
2)
37
2 c
ase
s (s
ou
rce
FIR
2
01
2-1
3)
0 (
as
of
20
12
)
All
Sta
tes/
UTs
(3
5)
40
%
80
%
>1
50
0
case
s
35
(S
tate
s a
nd
UTs
)
Sta
te
com
mu
nic
atio
n
pla
n
Co
vera
ge
Su
rve
ys
Su
rve
illa
nce
re
po
rt
FIR
, P
IR,
DIR
VP
D S
urv
eill
an
ce
rep
ort
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
Sta
te/M
oH
FW
Mo
HF
W
Mo
HF
W
DIO
, S
IO
Mo
HF
W/S
IO
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
1. N
um
ber
of
Sta
tes/
UTs
that
have
a d
efin
ed
media
tra
ckin
g a
nd
ass
ess
ment
pla
n.
2. %
of
care
giv
ers
w
ho c
an r
eca
ll new
im
muniz
atio
n
mess
ages/
taglin
e
1. %
of
sentin
el
site
s pro
vidin
g
timely
and
com
ple
te r
eport
s on V
PD
s (incl
udin
g
zero
rep
ort
) on
90%
occ
asi
ons
2. Incr
ease
in t
he
num
ber
of
notif
ied
serious
AE
FI
case
s above
th
e 2
012
base
line
valu
e
1. N
um
ber
of
Sta
tes
that
have
co
nduct
ed V
PD
su
rveill
ance
w
ork
sho
ps
EX
PE
CT
ED
RE
SU
LT
2.3
: E
vid
en
ce b
ased
an
d c
on
tex
tua
lly
re
lev
an
t c
om
mu
nic
ati
on
me
ss
ag
es
are
dis
se
min
ate
d in
th
e c
om
mu
nit
y
KE
Y O
BJE
CT
IVE
3:
Str
en
gth
en
an
d m
ain
tain
ro
bu
st
su
rveilla
nce s
yste
m f
or
vaccin
e p
reven
tab
le d
iseases (
VP
Ds)
an
d
ad
vers
e e
ven
ts f
ollo
win
g im
mu
niz
ati
on
(A
EF
I)
EX
PE
CT
ED
RE
SU
L3.1
: In
sti
tuti
on
alize a
nd
str
en
gth
en
su
rveilla
nce m
ech
an
ism
s f
or
VP
Ds
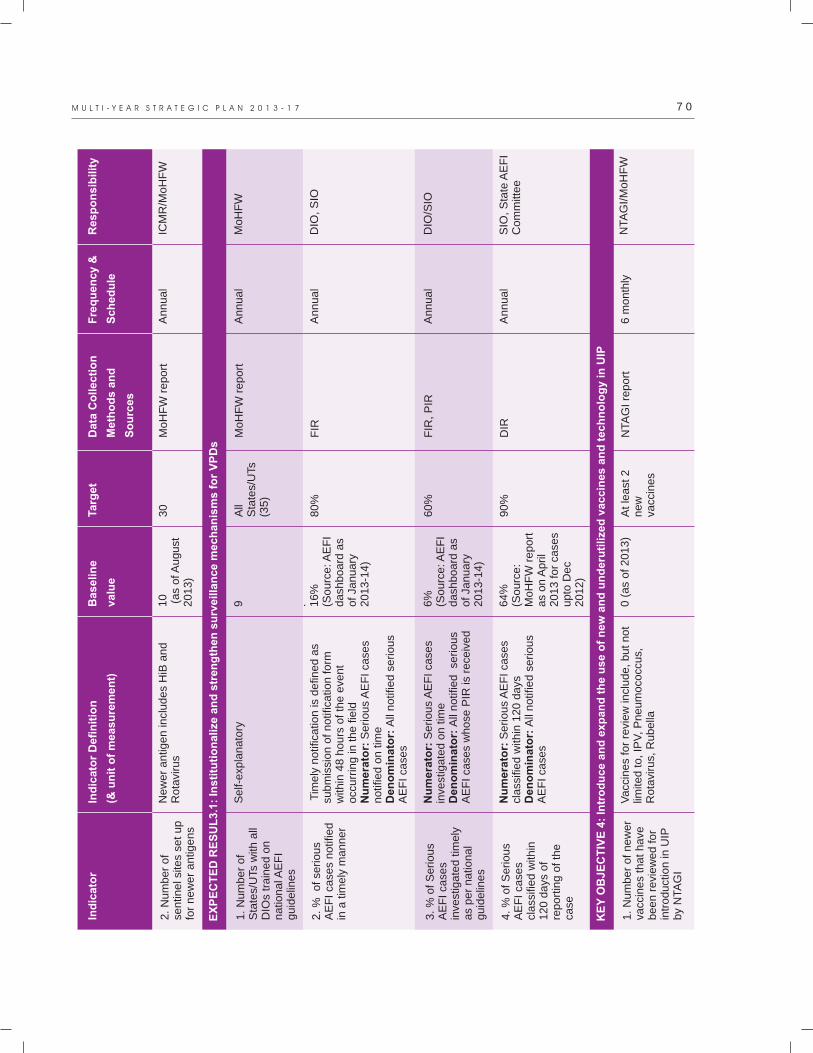
7 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
New
er
antig
en in
clu
de
s H
iB a
nd
R
ota
viru
s
Self-
exp
lanato
ry
Tim
ely
notif
icatio
n is
de
fine
d a
s su
bm
issi
on o
f notif
ica
tion
fo
rm
with
in 4
8 h
ours
of th
e e
ven
t occ
urr
ing in
the f
ield
Nu
mera
tor:
Serious
AE
FI
case
s notif
ied o
n t
ime
Den
om
inato
r: A
ll n
otif
ied
se
rio
us
AE
FI
case
s
Nu
mera
tor:
Seriou
s A
EF
I ca
ses
inve
stig
ate
d o
n t
ime
Den
om
inato
r: A
ll n
otif
ied
se
rio
us
AE
FI
case
s w
hose
PIR
is r
ece
ive
d
Nu
mera
tor:
Serious
AE
FI
case
s cl
ass
ified w
ithin
12
0 d
ays
Den
om
inato
r: A
ll n
otif
ied
se
rio
us
AE
FI
case
s
Vacc
ines
for
revi
ew
incl
ud
e,
bu
t n
ot
limite
d t
o,
IPV
, P
ne
um
oco
ccu
s,
Rota
viru
s, R
ubella
10
(a
s o
f A
ug
ust
2
01
3)
9 . 16
%
(So
urc
e: A
EF
I d
ash
bo
ard
as
of
Jan
ua
ry
20
13
-14
)
6%
(So
urc
e: A
EF
I d
ash
bo
ard
as
of
Jan
ua
ry
20
13
-14
)
64
%(S
ou
rce
: M
oH
FW
re
po
rt
as
on
Ap
ril
20
13
fo
r ca
ses
up
to D
ec
20
12
)
0 (
as
of
20
13
)
30
All
Sta
tes/
UTs
(3
5)
80
%
60
%
90
%
At
lea
st 2
n
ew
va
ccin
es
Mo
HF
W r
ep
ort
Mo
HF
W r
ep
ort
FIR
FIR
, P
IR
DIR
NTA
GI
rep
ort
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
6 m
on
thly
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
2. N
um
ber
of
sentin
el s
ites
set
up
for
new
er
antig
ens
1. N
um
ber
of
Sta
tes/
UTs
with
all
DIO
s tr
ain
ed o
n
natio
nal A
EF
I guid
elin
es
2. %
of
serious
AE
FI ca
ses
notif
ied
in a
tim
ely
manner
3. %
of S
erious
AE
FI ca
ses
inve
stig
ate
d t
imely
as
per
natio
nal
guid
elin
es
4. %
of
Serious
AE
FI ca
ses
class
ifie
d w
ithin
120 d
ays
of
report
ing o
f th
e
case
1. N
um
ber
of
new
er
vacc
ine
s th
at
have
been r
evi
ew
ed f
or
intr
oductio
n in
UIP
by
NTA
GI
EX
PE
CT
ED
RE
SU
L3.1
: In
sti
tuti
on
alize a
nd
str
en
gth
en
su
rveilla
nce m
ech
an
ism
s f
or
VP
Ds
KE
Y O
BJE
CT
IVE
4:
Intr
od
uce a
nd
exp
an
d t
he u
se o
f n
ew
an
d u
nd
eru
tilized
vaccin
es a
nd
tech
no
log
y in
UIP
ICM
R/M
oH
FW
Mo
HF
W
DIO
, S
IO
DIO
/SIO
SIO
, S
tate
AE
FI
Co
mm
itte
e
NTA
GI/M
oH
FW
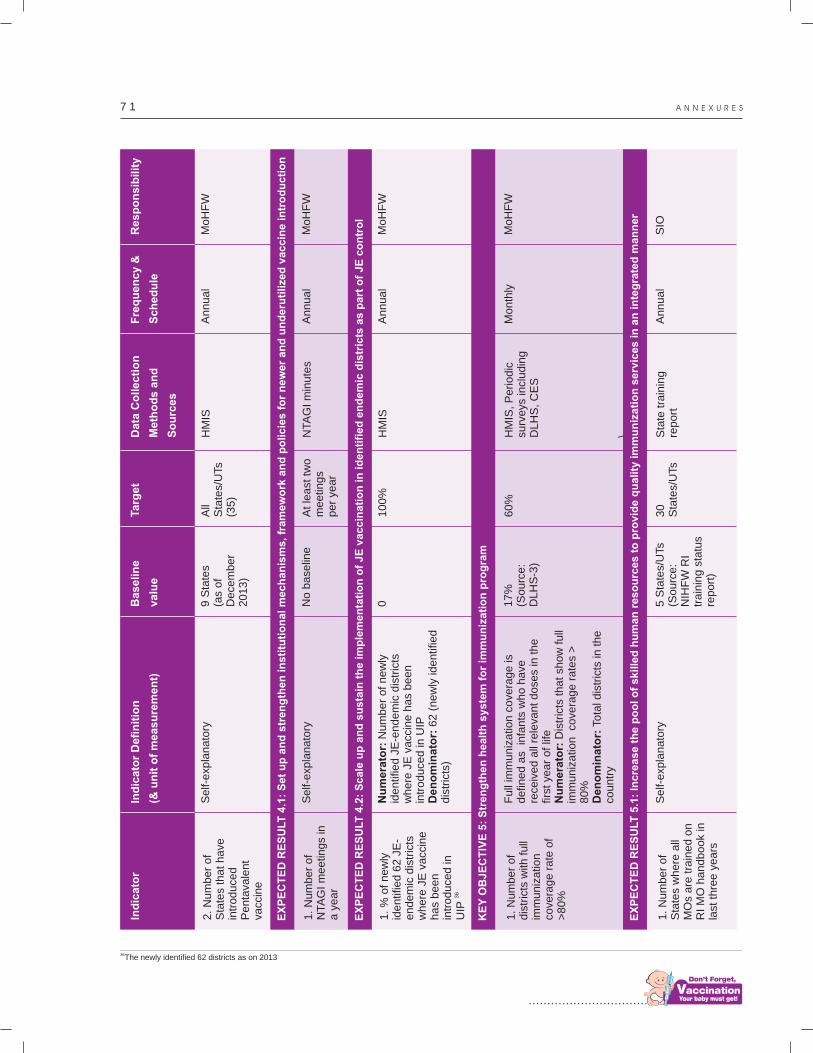
................................
7 1 A N N E X U R E S
Self-
exp
lanato
ry
Self-
exp
lanato
ry
Nu
mera
tor:
Num
be
r o
f n
ew
ly
identif
ied J
E-e
ndem
ic d
istr
icts
w
here
JE
vacc
ine h
as
be
en
in
troduce
d in
UIP
Den
om
inato
r: 6
2 (
ne
wly
ide
ntif
ied
dis
tric
ts)
Full
imm
uniz
atio
n c
ove
rag
e is
defin
ed a
s in
fants
wh
o h
ave
re
ceiv
ed a
ll re
leva
nt
do
ses
in t
he
fir
st y
ear
of
life
Nu
mera
tor:
Dis
tric
ts t
ha
t sh
ow
fu
ll im
muniz
atio
n
cove
rag
e r
ate
s >
80%
Den
om
inato
r: T
ota
l dis
tric
ts in
th
e
countr
y
Self-
exp
lanato
ry
9 S
tate
s (a
s o
f D
ece
mb
er
20
13
)
No
ba
selin
e
0 17
%(S
ou
rce
: D
LH
S-3
)
5 S
tate
s/U
Ts
(So
urc
e:
NIH
FW
RI
tra
inin
g s
tatu
s re
po
rt)
All
Sta
tes/
UTs
(3
5)
At
lea
st t
wo
m
ee
ting
s p
er
yea
r
10
0%
60
%
30
S
tate
s/U
Ts
HM
IS
NTA
GI
min
ute
s
HM
IS
HM
IS,
Pe
rio
dic
su
rve
ys in
clu
din
g
DL
HS
, C
ES
\ Sta
te t
rain
ing
rep
ort
An
nu
al
An
nu
al
An
nu
al
Mo
nth
ly
An
nu
al
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
2. N
um
ber
of
Sta
tes
that
have
in
troduced
Penta
vale
nt
vacc
ine
1. N
um
ber
of
NTA
GI m
eetin
gs
in
a y
ear
1. %
of
new
ly
identif
ied 6
2 J
E-
endem
ic d
istr
icts
w
here
JE
vacc
ine
has
bee
n
intr
oduce
d in
36
UIP
1. N
um
ber
of
dis
tric
ts w
ith f
ull
imm
uniz
atio
n
cove
rag
e r
ate
of
>80%
1. N
um
ber
of
Sta
tes
where
all
MO
s are
tra
ined o
n
RI M
O h
andbook
in
last
thre
e y
ears
Mo
HF
W
Mo
HF
W
Mo
HF
W
Mo
HF
W
SIO
EX
PE
CT
ED
RE
SU
LT
4.1
: S
et
up
an
d s
tre
ng
the
n i
ns
titu
tio
na
l m
ec
ha
nis
ms
, fr
am
ew
ork
an
d p
oli
cie
s f
or
ne
we
r a
nd
un
de
ruti
lize
d v
ac
cin
e i
ntr
od
uc
tio
n
EX
PE
CT
ED
RE
SU
LT
4.2
: S
ca
le u
p a
nd
su
sta
in t
he
im
ple
me
nta
tio
n o
f J
E v
ac
cin
ati
on
in
id
en
tifi
ed
en
de
mic
dis
tric
ts a
s p
art
of
JE
co
ntr
ol
KE
Y O
BJ
EC
TIV
E 5
: S
tre
ng
the
n h
ea
lth
sy
ste
m f
or
imm
un
iza
tio
n p
rog
ram
EX
PE
CT
ED
RE
SU
LT
5.1
: In
cre
as
e t
he
po
ol
of
sk
ille
d h
um
an
re
so
urc
es
to
pro
vid
e q
ua
lity
im
mu
niz
ati
on
se
rvic
es
in
an
in
teg
rate
d m
an
ne
r
36The newly identified 62 districts as on 2013
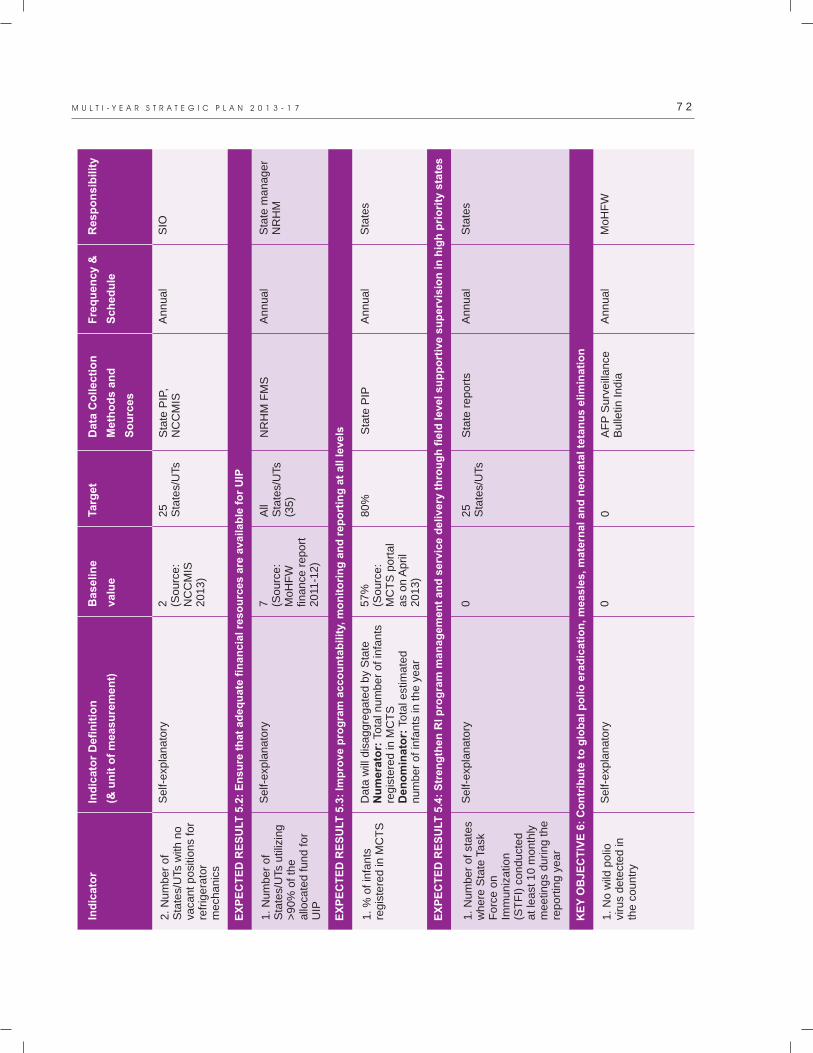
7 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Self-
exp
lanato
ry
Self-
exp
lanato
ry
Data
will
dis
aggre
ga
ted
by
Sta
teN
um
era
tor:
Tota
l nu
mb
er
of
infa
nts
re
gis
tere
d in
MC
TS
Den
om
inato
r: T
ota
l est
ima
ted
num
ber
of
infa
nts
in t
he
ye
ar
Self-
exp
lanato
ry
Self-
exp
lanato
ry
2 (So
urc
e:
NC
CM
IS
20
13
)
7 (So
urc
e:
Mo
HF
W
fina
nce
re
po
rt
20
11-1
2)
57
%(S
ou
rce
: M
CT
S p
ort
al
as
on
Ap
ril
20
13
)
0
0 0
25
S
tate
s/U
Ts
All
Sta
tes/
UTs
(3
5)
80
%
25
S
tate
s/U
Ts
0
Sta
te P
IP,
NC
CM
IS
NR
HM
FM
S
Sta
te P
IP
Sta
te r
ep
ort
s
AF
P S
urv
eill
an
ce
Bu
lletin
In
dia
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
2. N
um
ber
of
Sta
tes/
UTs
with
no
vaca
nt p
osi
tions
for
refr
igera
tor
mech
anic
s
1. N
um
ber
of
Sta
tes/
UTs
util
izin
g
>90%
of
the
allo
cate
d f
und f
or
UIP
1. %
of
infa
nts
re
gis
tere
d in
MC
TS
1. N
um
ber
of
state
s w
here
Sta
te T
ask
F
orc
e o
n
Imm
uniz
atio
n
(ST
FI)
conduct
ed
at le
ast
10 m
onth
ly
meetin
gs
during t
he
report
ing y
ear
1. N
o w
ild p
olio
vi
rus
de
tect
ed in
th
e c
ountr
y
SIO
Sta
te m
an
ag
er
NR
HM
Sta
tes
Sta
tes
Mo
HF
W
EX
PE
CT
ED
RE
SU
LT
5.2
: E
ns
ure
th
at
ad
eq
ua
te f
ina
nc
ial
res
ou
rce
s a
re a
va
ila
ble
fo
r U
IP
EX
PE
CT
ED
RE
SU
LT
5.3
: Im
pro
ve
pro
gra
m a
cc
ou
nta
bil
ity,
mo
nit
ori
ng
an
d r
ep
ort
ing
at
all
le
ve
ls
EX
PE
CT
ED
RE
SU
LT
5.4
: S
tre
ng
the
n R
I p
rog
ram
ma
na
ge
me
nt
an
d s
erv
ice
de
liv
ery
th
rou
gh
fie
ld l
ev
el
su
pp
ort
ive
su
pe
rvis
ion
in
hig
h p
rio
rity
sta
tes
KE
Y O
BJ
EC
TIV
E 6
: C
on
trib
ute
to
glo
ba
l p
oli
o e
rad
ica
tio
n,
me
as
les
, m
ate
rna
l a
nd
ne
on
ata
l te
tan
us
eli
min
ati
on
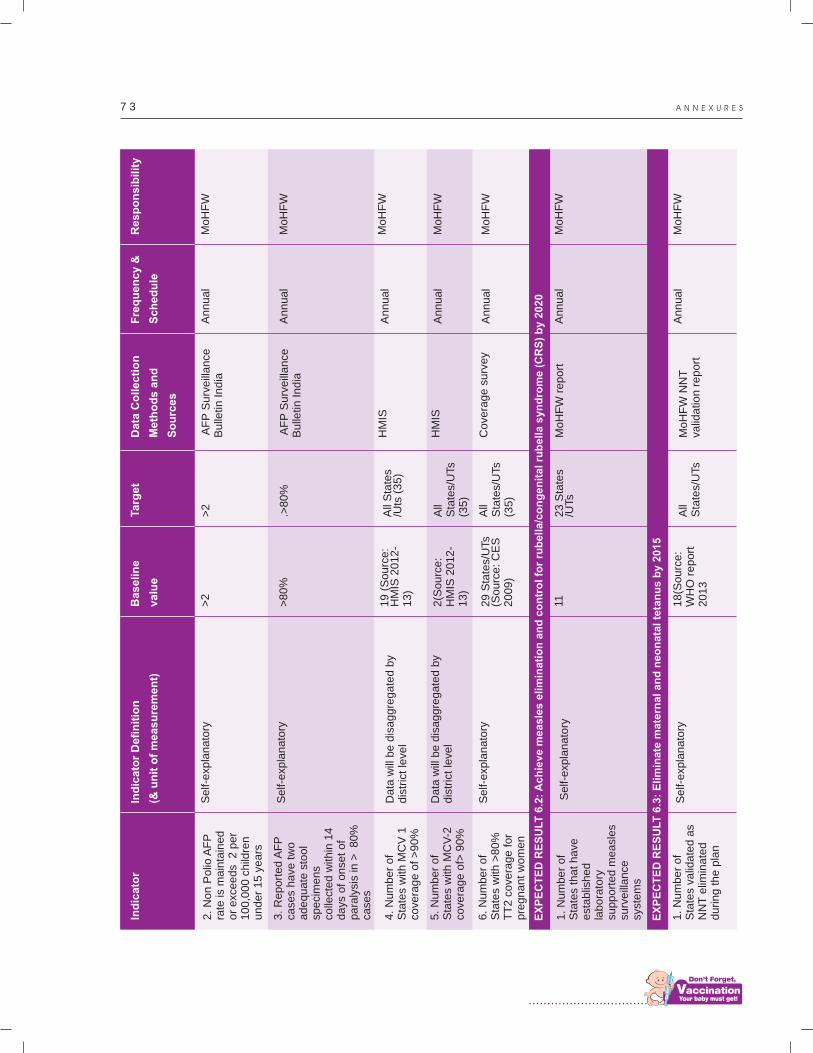
................................
7 3 A N N E X U R E S
Self-
exp
lanato
ry
Self-
exp
lanato
ry
Data
will
be d
isagg
reg
ate
d b
y dis
tric
t le
vel
Data
will
be d
isaggre
ga
ted
by
dis
tric
t le
vel
Self-
exp
lanato
ry
Self-
exp
lanato
ry
Self-
exp
lanato
ry
>2
>8
0%
19
(S
ou
rce
: H
MIS
20
12
-1
3)
2(S
ou
rce
: H
MIS
20
12
-1
3)
29
Sta
tes/
UTs
(So
urc
e:
CE
S
20
09
)
11 18
(So
urc
e:
WH
O r
ep
ort
2
01
3
>2
.>8
0%
All
Sta
tes
/Uts
(3
5)
All
Sta
tes/
UTs
(3
5)
All
Sta
tes/
UTs
(3
5)
23
Sta
tes
/UTs
All
Sta
tes/
UTs
AF
P S
urv
eill
an
ce
Bu
lletin
In
dia
AF
P S
urv
eill
an
ce
Bu
lletin
In
dia
HM
IS
HM
IS
Co
vera
ge
su
rve
y
Mo
HF
W r
ep
ort
Mo
HF
W N
NT
va
lida
tion
re
po
rt
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
An
nu
al
Ind
icato
r In
dic
ato
r D
efi
nit
ion
(& u
nit
of
measu
rem
en
t)
Ba
se
lin
e
va
lue
Ta
rge
tD
ata
Co
lle
cti
on
Me
tho
ds
an
d
So
urc
es
Fre
qu
en
cy
&
Sc
he
du
le
Re
sp
on
sib
ilit
y
2. N
on P
olio
AF
P
rate
is m
ain
tain
ed
or
exc
ee
ds
2 p
er
100,0
00 c
hild
ren
under
15 y
ears
3. R
eport
ed A
FP
ca
ses
have
tw
o
adequate
sto
ol
speci
mens
co
llect
ed w
ithin
14
days
of onse
t of
para
lysi
s in
>
80%
ca
ses
4. N
um
ber
of
Sta
tes
with
MC
V 1
co
vera
ge o
f >
90%
5. N
um
ber
of
Sta
tes
with
MC
V-2
co
vera
ge o
f> 9
0%
6. N
um
ber
of
Sta
tes
with
>80%
T
T2 c
ove
rage f
or
pre
gnan
t w
om
en
1. N
um
ber
of
Sta
tes
that
have
est
ablis
hed
labora
tory
su
pport
ed m
easl
es
surv
eill
ance
sy
stem
s
1. N
um
ber
of
Sta
tes
valid
ate
d a
s N
NT
elim
inate
d
during t
he p
lan
Mo
HF
W
Mo
HF
W
Mo
HF
W
Mo
HF
W
Mo
HF
W
Mo
HF
W
Mo
HF
W
EX
PE
CT
ED
RE
SU
LT
6.2
: A
ch
iev
e m
ea
sle
s e
lim
ina
tio
n a
nd
co
ntr
ol
for
rub
ell
a/c
on
ge
nit
al
rub
ell
a s
yn
dro
me
(C
RS
) b
y 2
02
0
EX
PE
CT
ED
RE
SU
LT
6.3
: E
lim
ina
te m
ate
rna
l a
nd
ne
on
ata
l te
tan
us
by
20
15
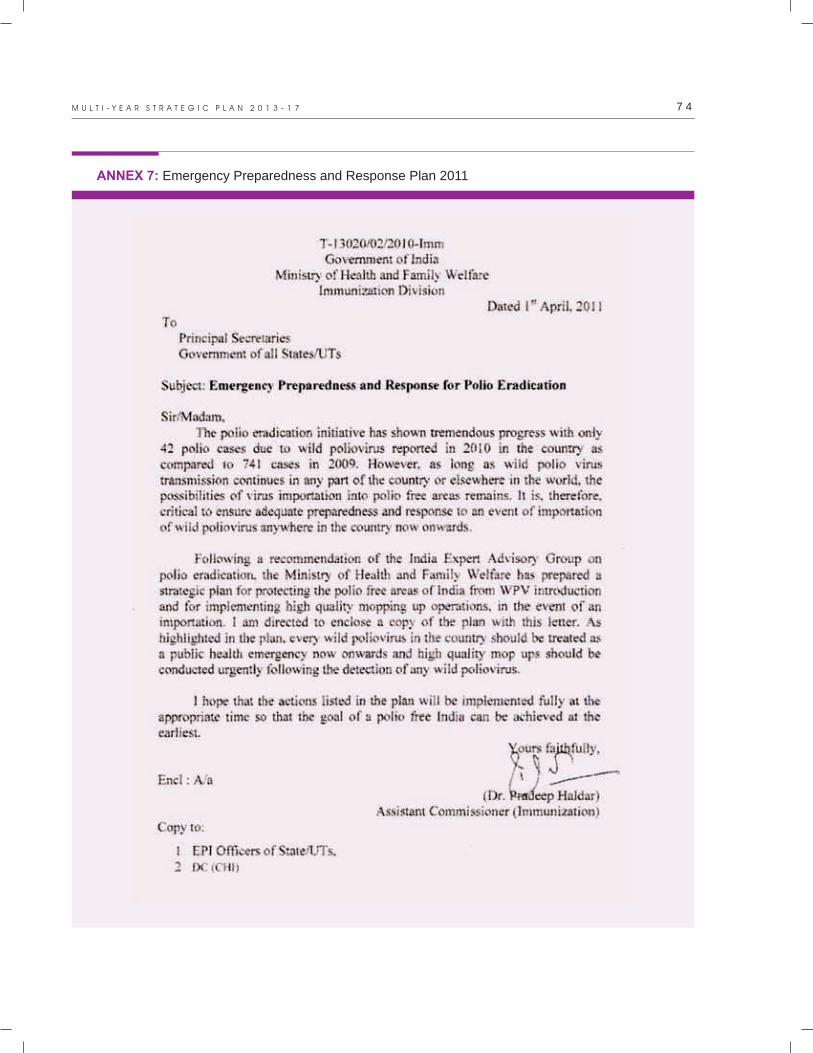
7 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
ANNEX 7: Emergency Preparedness and Response Plan 2011

................................
7 5 A N N E X U R E S
Emergency Preparedness and Response Plan 2011
1. Background
The Emergency Preparedness and Response Plan has been developed at the request of the Minister of Health & Family Welfare to ensure adequate preparedness and response to an event of importation of poliovirus anywhere in India during 2011.
India has made remarkable progress towards polio eradication in 2010. Only 42 wild poliovirus (WPV) cases have been detected in the country, compared to 724 cases detected during the same period in 2009. The progress in polio eradication was reviewed during the India Expert Advisory Group (IEAG) meeting held in November 2010. At this meeting the IEAG concluded that “the epidemiologic, genetic, serologic, operational & technical evidence show that India is on the right path to achieve eradication”. However, the IEAG identified certain risks to the polio eradication Program in India. One of the major risks identified includes continued transmission of poliovirus within the mobile / migrant populations, resulting in re-introduction and
spread of the virus in Uttar Pradesh (UP) and Bihar or in areas outside these historically core endemic states that are at high risk of importation and further spread of polio. The IEAG highlighted the fact that as long as virus transmission continues in any part of India or elsewhere in the World, the possibility of virus importation to polio-free areas in India remains.
In view of these risks, the IEAG recommended that while intensive efforts should continue to stop transmission in areas with recent WPV transmission and the traditionally endemic areas of UP and Bihar, the program in India should:
a. make efforts to protect polio-free areas from importation of virus from within or outside India
b. rapidly respond to any WPV detected anywhere in India during 2011 with an aggressive mop-up vaccination campaign to stop any further circulation of the virus.
The IEAG recommended that “From now, any WPV from any source should be considered a public health emergency and responded to with urgent mop-ups; government & partners must
deploy additional, highly experienced human resources to ensure that mop-up rounds are of
the highest quality. Mop-ups should target both
the area of detection of the virus in a case or in the environment and, if there is a clear genetic link, the area of origin of the virus”. Thus any isolation of WPV requires a rapid high quality mopping-up response as an utmost priority to stop circulation and spread.
This document is a strategic plan for protecting the polio-free areas of India from WPV and for implementing high quality mopping-up operations with the aim of stopping the final chains of WPV transmission.
The Government of India will have a “Central Emergency Preparedness and Response Group” to ensure adequate preparedness for a rapid response and manage the actual response to the detection of a wild poliovirus anywhere in India during 2011. The group will be chaired by the Joint Secretary, Health & Family Welfare, Government of India, and comprise of senior officials from the Ministry of Health and Family Welfare (GoI), and representatives of National Polio Surveillance Project (NPSP) – WHO, UNICEF and Rotary. The key responsibilities of the group will include:
lIdentify and train Rapid Response Team (RRT) members at the national level. The RRT members will include experienced, government and partner agency staff from the fields of epidemiology, public health, management and communica t ion (including a media specialist).
lFollow up with state governments to ensure that a Rapid Response Team, headed by an officer of the rank of a Principal Secretary, is constituted in each state. The state RRT should include at least 2 to 4 well performing Medical Officers from within the state who have at least
2. Immediate actions - Preparedness for virus importation and response
2.1 National-level Actions

7 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
5 years' experience in dealing with senior district level officials and a familiarity with the basic principles of mass vaccination campaign implementation. The RRT members will be trained by MoHFW, GoI with assistance from WHO NPSP and UNICEF. In the event of WPV detection, it will be necessary to assign the RRT members full time duty by the state governments to provide support to mop up vaccination campaigns.
lDevelop a media response plan to be used in the event of detection of WPV.
lReview the availability of buffer stocks of oral polio vaccines to manage mop-up vaccination campaigns.
Summary of the national actions with the proposed time frame:
lConstitute the “Central Emergency Preparedness and Response Group” by mid-April 2011.
lWrite to state governments and partners, in the second week of April 2011, for identification of RRT members in each state by the end of April 2011.
lOrganize a training of the RRT members jointly with NPSP and UNICEF by the second week of May 2011.
lMonitor the identification and training status of the RRT members.
lProcure sufficient buffer stocks of bOPV, tOPV and mOPVs to manage the mop-ups.
lDevelop a media response plan by end of April 2011 that includes mechanisms of harmonizing messages from union and state governments to the detection of any polio cases.
The following states have been identified at a high or medium risk of importation based on past epidemiology of polio: Haryana, Delhi, Ut tarakhand, Maharashtra , Punjab, Rajasthan, West Bengal, Gujarat, Jharkhand, Madhya Pradesh, Assam, Orissa, Andhra Pradesh, Himachal Pradesh, Jammu & Kashmir and
2.2 State level
2.2.1 States at risk of importation
Karnataka.
Endemic states
States at high & medium risk of importation
States at low risk of importation
lHigh Risk of Importation: 8 or more importations and 5 years or more with importations
lMedium Risk of Importation: 5 or more importations and 3 to 4 years with importations
Risk Categorization of States based on history of polio importations during last fiveyears

................................
7 7 A N N E X U R E S
2.2.2 State Level Actions
Each state at high or medium risk should undertake the following actions to prepare for the emergency response:
lConstitute a State Emergency Preparedness and Response Group chaired by the Secretary (Health & Family Welfare) and comprised of senior officials from the State Government such as the Director Health Services, State EPI Officer and other nominated senior government officials. State representatives of WHO- NPSP,
UNICEF and Rotary International should also be a part of the group. This group should monitor the preparedness and implementation of the mop-up.
lUndertake a risk analysis, in coordination with WHO- NPSP officials, to identify
districts, blocks or urban areas at high risk of importation and spread of poliovirus.
This analysis should identify areas that have had repeated importations of polio viruses during previous years or a recent clustering of polio compatible cases in time and space, or are hard-to-reach areas or have
demographic/ environmental factors that would facilitate the spread of wild polio virus following an introduction (such as high population density, poor sanitation). Special focus should be on the identification of areas with low routine immunization coverage and areas with migratory or mobile populations in each state as per guidelines issued by GOI in 2010. This risk analysis should be completed at the earliest by each state and the lists of all high-risk areas and
populations shared with GOI.
lUndertake a communication risk analysis in coordination with UNICEF/ WHO- NPSP
and based on the analysis develop a communication plan for issues related to n o n - c o m p l i a n c e / r e s i s t a n c e t o administration of polio vaccines.
lDevelop a media response plan to be used in case a virus is detected.
lDevelop and implement a plan to increase polio SIA coverage and RI coverage in these high-risk areas/ populations to achieve high
immunity against polioviruses in these areas, which in turn will prevent spread and establishment of circulation of any imported wild polioviruses. These areas should be targeted for better planning, training, social mobilization and monitoring efforts during the SIAs in 2011–12. The states should also begin the process of harmonizing the polio microplans with Routine Immunization plans in the high-risk
areas.
lIdentify and nominate two to four experienced medical officers to be a part of the Rapid Response Teams (RRTs).
lReview the surveillance quality in these areas with the district and block officials in coordination with NPSP officials to identify actions to strengthen surveillance sensitivity in these areas, which in turn will assist with early detection and response following any importation.
lAssign senior state government officials to visit high risk districts and blocks to review progress in updating and implementing microplans for improving immunization coverage and surveillance sensitivity.
Summary of the state actions with the proposed time frame:
lConstitute a State Emergency Preparedness and Response group by end of April 2011.
lIdentify RRT members by end of April 2011.
lIdentify high-risk districts and high-risk are
as within districts by mid-May 2011.
lIdentify and assign senior officials to high-risk districts by third week of May
2011.
lThe above items should be reported back to the Central Emergency Preparedness and Response Group by the end of May 2011.
7 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
3. Response and actions following the detection of wild poliovirus
3.1 Key steps in the planning phase of the mopping up vaccination campaign
3.1.1 National-Level Actions:
lThe Ministry of Health and Family Welfare will be informed about the detection of the virus without delay.
lThe Ministry of Health and Family Welfare will inform the Chief Secretary of the affected state of the detection of the polio case in the state.
lThe Central Emergency Preparedness and Response Group will meet within 24 hours of receiving the information. The Group will review and analyze, in detail, the field epidemiological investigation findings pertaining to the polio case. Based on the above findings, the areas and populations at risk of poliovirus circulation will be identified and a SIA response within the broad strategic framework recommended by the IEAG will be decided. The group will make specific recommendations on:
§Timing of the response
§Areas to be covered during the response
§Type of vaccine to be used during the response
§Number of proposed rounds
§Additional investigations and analyses to be conducted
lMembers from the Central Emergency Preparedness and Response Group will visit the concerned state to meet the state health secretary and other state officials. The members of the National and State Emergency Preparedness and Response groups will subsequently visit the concerned districts accompanied by the state RRT members to review planning for an emergency response.
lThe Central Emergency Preparedness and Response Group will meet on a weekly basis to review the planning and implementation
o f t h e r e s p o n s e a n d p r o v i d e recommendations to the immunization division and state authorities to make improvements.
lVaccine will be mobilized to reach the state or districts undertaking the mop-up at least three days before the start of the campaign.
lMoHFW shall seek support from other government departments such as Social Welfare, Railways, Panchayati Raj, Urban Development, Education, for the emergency mop-up operation.
lThe State Emergency Preparedness and Response Group should be activated within 24 hours of receipt of information to initiative the following actions:
§Inform the Divisional Commissioners and the District Magistrates of the areas undertaking the mop-up within 24 hours of
receipt of information.
§Allocate geographical areas and operational responsibilities to all RRT members ensuring an appropriate distribution of human resource within 72 hours of receipt of information.
§Assign senior state officials to the districts and members of the State Emergency Preparedness and Response Group to visit and mobilize the districts within 72 hours of confirmation of case.
lThe current ly exist ing State- level Steering/Coordination Committee for polio eradication should be requested to organize a meeting within five days of case confirmation to seek support and coordinate ac t iv i t i e s wi th o ther gover nment departments and NGOs.
lDistrict-level officials from health and administration should begin mobilizing block officials to start preparations within 48 hours of identify the importation.
3.1.2 State level Actions:
3.1.3 District-level Actions:
................................
7 9 A N N E X U R E S
lDistrict Task Force (DTF) meetings should be organized in the district with RRT members, NPSP, UNICEF staff and key government officials to allocate specific responsibilities within the district and ensure participation of all sectors for a successful implementation of the mop-up. The first DTF to be conducted within five days of confirmation of the case. Subsequently there should be a weekly DTF to take stock of the situation and address requirements of the response activities.
lDivisional Commissioners should review the preparedness through participation in DTFs and field visits.
lTehsil or Block Task force meetings should be organized at sub-district level in all urban
and rural areas within sevendays of the confirmation of the case.
lAll existing micro plans should be reviewed as per operational guide for mop-up with special emphasis to ensure no areas are missed and there is high coverage of high risk areas and migratory populations. All micro plans should be reviewed and modified within 10 days of confirmation of the case.
lAll vaccinators should be retrained on operational and IPC skills in the week before the start of the mop-up.
lThe district and block in consultation with UNICEF and other social mobilization partners should plan and initiate IEC and social mobilization measures based on solid data collected through standardized data tools.
lDevelop a media response plan to be used in case a virus is detected.
lIn consultation with the government, NPSP should develop a monitoring plan for intensive monitoring and mid course corrections during the activity. Additional independent monitors should be deployed by NPSP in addition to the existing NPSP and UNICEF staff present in the district.
3.2 Key actions during the mopping up vaccination campaign
3.2.1 National-level Actions
3.2.2 State-level Actions
3.2.3 District/ Sub District-level Actions:
lMembers from the Central Emergency Preparedness and Response Group will monitor the activity in the highest risk blocks.
lThe Central Emergency Preparedness and Response Group will meet to review the feedback from its members, states, RRTs and provide directions for corrective actions.
lMembers of the State Emergency Preparedness and Response Group and the State monitors should visit high risk blocks to monitor the activity and provide feedback to the State Principal Secretary (H & FW)
lThe State Emergency Preparedness and Response Group should meet daily to review feedback from the districts and plan corrections.
lThe district should implement the SIA activity under the direction of the District Magistrate (DM) and supervision of the Chief Medical Officer/Civil Surgeon. The DMs should report on the quality of the activity to the State Principal Secretary (H & FW).
lDaily monitoring and review of activity to plan for corrective actions over subsequent days
§Senior district-level officials from health and administration (Divisional Commissioner/ D M / A D M / C M O / D P O / D y CMO/BDOs) should monitor the implementation of the activity and attend evening meetings at the high risk blocks.
§A daily evening review meeting should be organized at the district under the chairmanship of the District Magistrate.
8 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
4. Key actions at the end of the activity
5. Role of partners
6. States at low risk of importation of poliovirus
lThe District Magistrate should send a report of the completed activity to the State Emergency Preparedness and Response Group for review and corrective actions.
lThe State Emergency Preparedness and Response Group should meet to review this and forward the report to the Central Emergency Preparedness and Response Group.
lThe Central Emergency Preparedness and Response Group will review the activity and inform the Union Minister who, at his discretion, will inform the Chief Minister of the concerned state about the quality of response activities and ongoing risk assessment.
Partners should participate in the Central and State Emergency Preparedness and Response Groups. The key role of the partners will be as follows:
lNPSP: Provide sur vei l lance data, epidemiologic analysis and strategic planning and other technical support to the group as well as support monitoring of the preparedness and response at the district, state and national levels.
lUNICEF: Provide suppor t to the communication/ social mobilization and media strategies and their implementation and monitor their impact
lRotary International:Provide support to the advocacy at the state and district levels and to the communication strategy and social mobilization activities
lUndertake a risk analysis, in coordination with WHO-NPSP officials, to identify
districts, blocks, and urban areas at higher risk of importation and spread of poliovirus.
This analysis should include identification of areas that have had importations of polio viruses during previous years or a recent clustering of compatibles in time and space, or are hard-to-reach areas or have
demographic or environmental factors that would facilitate the spread of wild poliovirus following an introduction (such as low routine immunization coverage, high population density, migrant sites, poor sanitation). Special focus should be on the identification of areas with migratory or mobile populations in each state as per guidelines issued by GOI in 2010. This risk analysis should be completed at the earliest and the lists of all high risk areas and populations shared by each state with GOI.
lThe state should assign Senior State Government officials to visit high risk districts and blocks to review progress in updating and implementing micro plans prior to the 2011 NIDs for improving immunization coverage and surveillance sensitivity.
The basic aim of the mop-up would be to vaccinate all under-5 children in the mop-up area. Each household in the mop-up area will be visited by vaccination teams to vaccinate all under-5 children. The duration of the house-to-house (h-t-h) search and vaccination
would be decided by the number of available vaccination teams in the area. In principle, there would be a minimum of 2 to 5-day h-t-h
activity in all areas to ensure a rational workload for each vaccination team. Additional 1 to 2 days of h-t-h activity will be
undertaken in special areas with lesser number of available teams e.g. in large urban areas. B team activity will continue in UP and Bihar. Transit teams and mobile teams will be deployed to cover migrant and mobile populations.
In areas that have used booths during the SNID/NID, booths will also be setup on day 1 of the mop-up campaign because of their IEC/SM value.
7. Strategy for mop-ups

................................
8 1 A N N E X U R E S
The mop-ups shall be implemented as per the Operational Guide for SIAs published by Government of India in 2006.
The following guidelines as recommended by the WHA andIEAG should be followed:
lSpeed of response: As early as possible but no later than two weeks from confirmation of the case.
lExtent of mop-ups: The response should consist of at least three large scale, house-to-house rounds of immunization.
The World Health Assembly Resolution (59.1) calls for coverage of 2 to 5 million children in each round. Mop-ups should
cover at a minimum the infected district and all districts contiguous with it, across state boundaries if necessary. Where there is a clear genetic link of the virus to the strains in another area, the area of origin should also be included. In the demographic context of India and considering that this is the final
7.1 General principles for mopping-up operations
stage of polio eradication, the 18th IEAG has recommended the appropriate target population for mop-ups around 5 million
children per round.
o In high risk areas: SNID rounds may constitute one or more of the three rounds, but in principle at least one additional round should be carried out in an appropriate area using a short interval approach – all rounds must be of the highest possible quality!
o In non-high risk areas: Mop-ups should
consist of a minimum of three high quality rounds, using a short interval approach (minimum interval of two weeks but within four weeks) – all rounds must be of the highest possiblequality!
lVaccine of choice for mop-ups is mOPV
appropriate to the local epidemiology or bOPV; a rolling stockpile of 30 million doses of bOPV and 10 million doses of mOPV1 should be maintained to allow for rapid implementation of mopping up vaccination with the appropriate vaccine.

................................ 8 3
Costing and Financial Sustainability of the
Universal Immunization Program
7


................................
8 5
1. Introduction
India is at an important time in the development of its Universal Immunization Program (UIP). It is planning several improvements such as the addition of many new and underutilized vaccines as well as adding new staff at different administrative levels. India will need to secure other sources of financing as it will probably be graduating from GAVI support since its high Gross National
1Income (GNI) per capita will make it ineligible for support. As a result, information on the costs and sources of financing for the UIP will be particularly important for policy-makers to make informed decisions on phasing-in strategies and timing of these Program improvements.
The report on costing and financial sustainability of the India Immunization Program was developed during the period June to December 2013, under the auspices of the Immunization Technical Support Unit (ITSU) in India and assisted by the immunization partners, WHO and UNICEF. The team that collected and analyzed the data was led by a research scientist from the Public Health Foundation of India and consisted of
Government of India officials, and experts from the Immunization Technical Support Unit (ITSU-MoHFW) and the immunization partners. Data was collected from June to September 2013. Then meetings were held with ministry officials to go over the preliminary findings and assumptions to be made in the analysis. Finally, from September to December 2013 the data was analyzed and put into a report.
The main findings of the cost analysis are the following:
lTotal baseline expenditure was INR 3,446 2crore ($718 million), including shared
3personnel costs, and INR 2,131 crore ($444 million) without shared costs.
o Expenditure on the routine Program was INR 1,253 crore ($261 million) and, on the supplemental immunization activities (SIAs), was INR 878 crore ($182 million).
l
2. Summary of Findings on Baseline Expenditures
Table 1 shows total baseline expenditures with shared costs and selected indicators on cost per output and Program financing.
1 Countries' GAVI eligibility for the year 2014 is GNI per capita lower or equal to $1,570. 2 1 crore= ten million (10,000,000)3 Shared costs include the value of inputs that are not specific to immunization and which are used by different Programs or activities in the health sector — i.e. their utilization for immunization is less than 100%.
Table 1. Baseline Expenditures and Selected Indicators, 2012.
Total Expenditures (USD)
261,089,884
182,995,523
444,085,407
273,942,919
718,028,326
0.2
14
90
1
2
0.03
Total Expenditures (INR)
12,532,314,431
8,783,785,120
21,316,099,550
13,149,260,100
34,465,359,650
9.6
672
90
1
2
0.03
Baseline Indicators
Routine Immunization only
Campaigns
Total immunization specific expenditure (A)
Total shared cost (B)
Grand Total (A + B)
Per capita
Per DTP3 child
Percentage national funding
Percentage total health expenditures
Percentage govt. health expenditures
Percentage GDP
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m

8 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
3. Details of Baseline Program Cost and Financing
The year 2012 is the baseline for the cost and financing projections since it has the most recent complete information. The actual expenses of the government and the immunization partners were taken into account for the baseline cost calculation.
Table 2 shows the baseline cost profile. In 2012, the total estimated cost of the UIP was INR 3,446 crore ($718 million), including shared cost. Shared personnel cost (those who spent less than 100 percent of their time for immunization) contributed the maximum in total expenditure (38 percent) while all routine recurrent cost contributed 36 percent. The contribution of SIAs was 25 percent in total cost. The detailed expenditure on shared personnel cost is provided in Table 3. Vaccines
and injection supplies under routine recurrent cost are those used for Routine Immunization only. The amount spent on vaccines and injection supplies for supplementary immunization has been provided under SIAs. Personnel cost includes salaries and benefits for all who spent 100 percent of their time for immunization starting from the national level. Transport cost included the operational cost of Teeka Express, vaccine handling cost at GMSD and the petrol, oil, lubricant for vaccine transport. It was assumed that there were a total of 700 vaccine vans (250 4WD and 450 2WD) and 120 Teeka Express in 2012. Training cost included the actual expenditure of the government on training as well as the training expenses by immunization partners. The components and detailed expenditures under social mobilization, Program management and other routine recurrent cost are shown in Tables 4, 5 and 6 respectively.
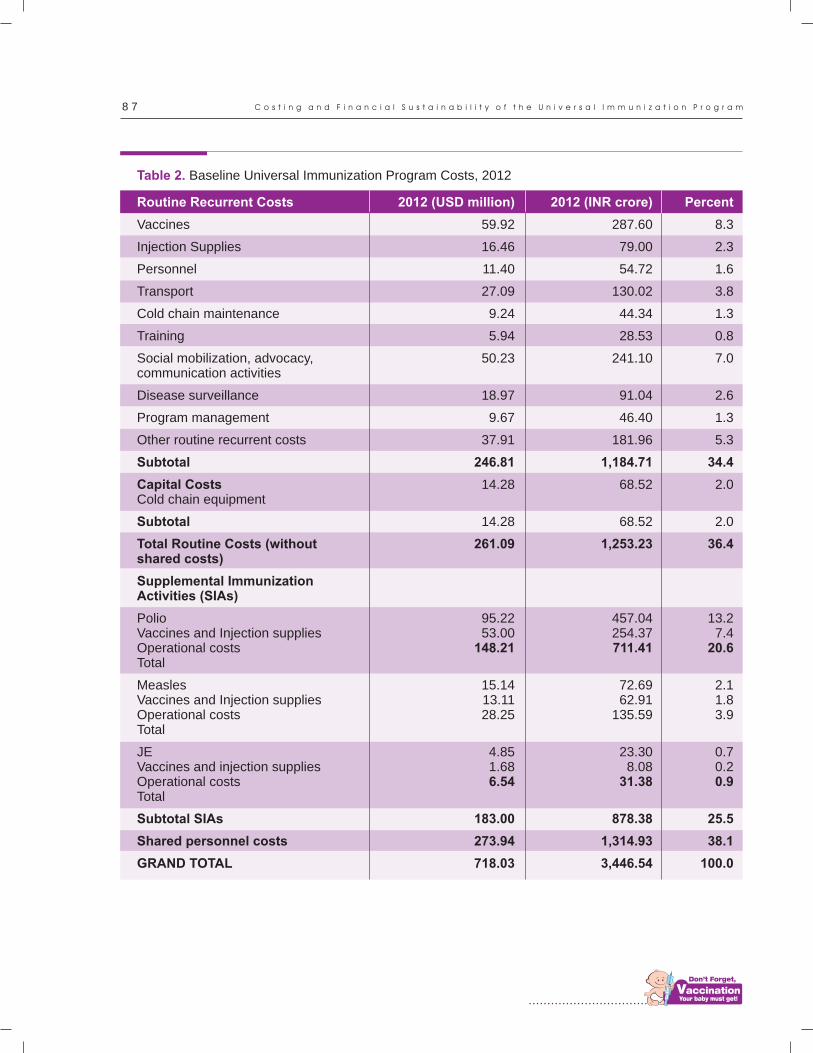
................................
8 7
Table 2. Baseline Universal Immunization Program Costs, 2012
Routine Recurrent Costs
Vaccines
Injection Supplies
Personnel
Transport
Cold chain maintenance
Training
Social mobilization, advocacy,communication activities
Disease surveillance
Program management
Other routine recurrent costs
Subtotal
Capital CostsCold chain equipment
Subtotal
Total Routine Costs (without shared costs)
Supplemental Immunization Activities (SIAs)
Polio Vaccines and Injection suppliesOperational costsTotal
MeaslesVaccines and Injection suppliesOperational costsTotal
JEVaccines and injection suppliesOperational costsTotal
Subtotal SIAs
Shared personnel costs
GRAND TOTAL
2012 (USD million)
59.92
16.46
11.40
27.09
9.24
5.94
50.23
18.97
9.67
37.91
246.81
14.28
14.28
261.09
95.2253.00
148.21
15.1413.1128.25
4.851.686.54
183.00
273.94
718.03
2012 (INR crore)
287.60
79.00
54.72
130.02
44.34
28.53
241.10
91.04
46.40
181.96
1,184.71
68.52
68.52
1,253.23
457.04254.37711.41
72.6962.91
135.59
23.308.08
31.38
878.38
1,314.93
3,446.54
Percent
8.3
2.3
1.6
3.8
1.3
0.8
7.0
2.6
1.3
5.3
34.4
2.0
2.0
36.4
13.27.4
20.6
2.11.83.9
0.70.20.9
25.5
38.1
100.0
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m

8 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Numbers in 2012*
4,833
4,833
24,049
207,578
14,648
16,109
24,049
296,099
Percentage of time spent on
immunization
10
5
10
33
33
33
5
Shared personnel
MO (in charge) at block level
Data entry operators at block level
MO (in charge) at PHC level
ANM
MPW
LHV
Data entry operators at PHC level
Total
Table 3: Details of shared personnel cost in 2012
Salary per month (INR)
35,000
8,000
35,000
12,500
12,500
12,500
8,000
INR (crore)
20.30
2.32
101.01
1027.51
72.51
79.74
11.54
1,314.93
USD (million)
4.23
0.48
21.04
214.06
15.11
16.61
2.40
273.94
Table 4: Details of expenditure on social mobilization, advocacy and communication activities in 2012
Cost components
ASHA incentives for social mobilizations
Printed materials (banners, posters, IEC materials) BCC tool
Advocacy and communication (UNICEF)
SMNet (UNICEF)
Total
INR Crore
194.62
24.98
5.73
15.77
241.10
USD million
40.55
5.20
1.19
3.29
50.23
Table 5: Details of Program management expenditure in 2012
Cost components
Evaluations, program reviews and assessment meetings
Office supplies and consumables
Micro planning
Immunization Technical Support Unit (ITSU)
Operational cost of polio and other VPDs (UNICEF)
Operational cost of polio and other VPDs (WHO)
Total
INR Crore
10.97
0.31
2.17
4.77
9.36
18.83
46.40
USD million
2.29
0.06
0.45
0.99
1.95
3.92
9.67
* Source: Rural Health Statistics in India, 2012.
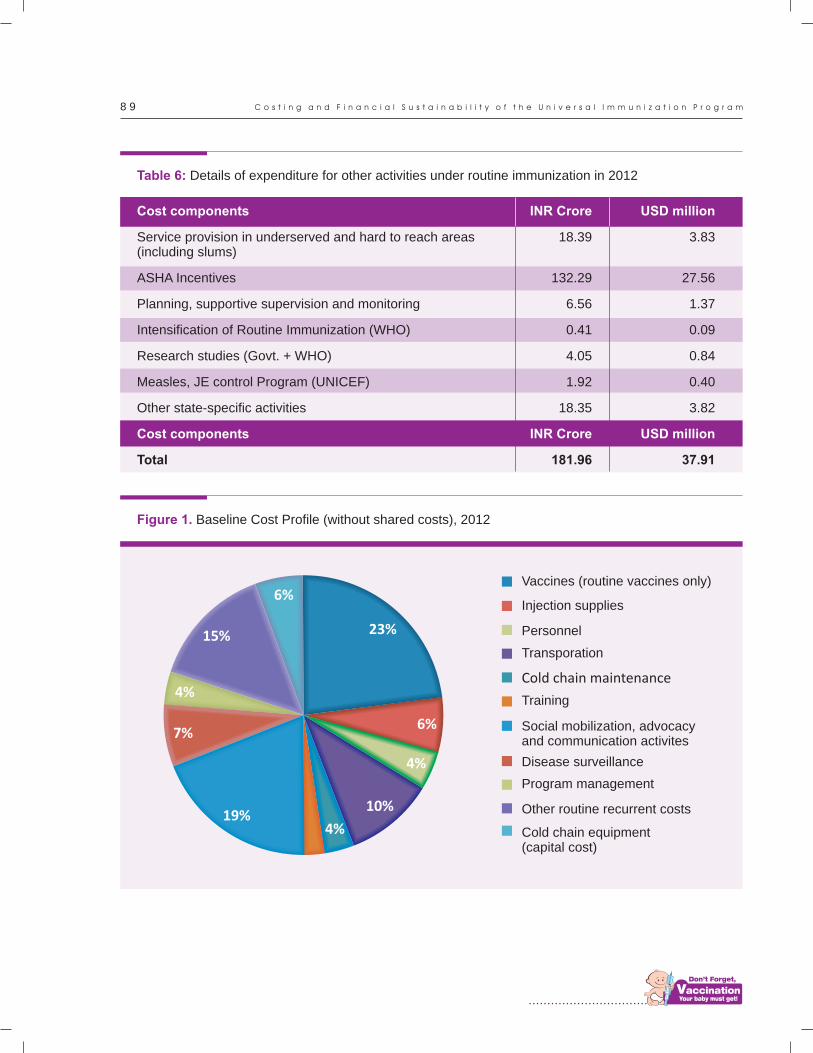
................................
8 9
Table 6: Details of expenditure for other activities under routine immunization in 2012
Cost components
Cost components
Service provision in underserved and hard to reach areas (including slums)
ASHA Incentives
Planning, supportive supervision and monitoring
Intensification of Routine Immunization (WHO)
Research studies (Govt. + WHO)
Measles, JE control Program (UNICEF)
Other state-specific activities
Total
INR Crore
INR Crore
18.39
132.29
6.56
0.41
4.05
1.92
18.35
181.96
USD million
USD million
3.83
27.56
1.37
0.09
0.84
0.40
3.82
37.91
Figure 1. Baseline Cost Profile (without shared costs), 2012
6%
15% 23%
4%
6%
4%
4%
7%
10%19%
Vaccines (routine vaccines only)
Injection supplies
Personnel
Transporation
Cold chain maintenance
Training
Social mobilization, advocacy and communication activites
Disease surveillance
Program management
Other routine recurrent costs
Cold chain equipment (capital cost)
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
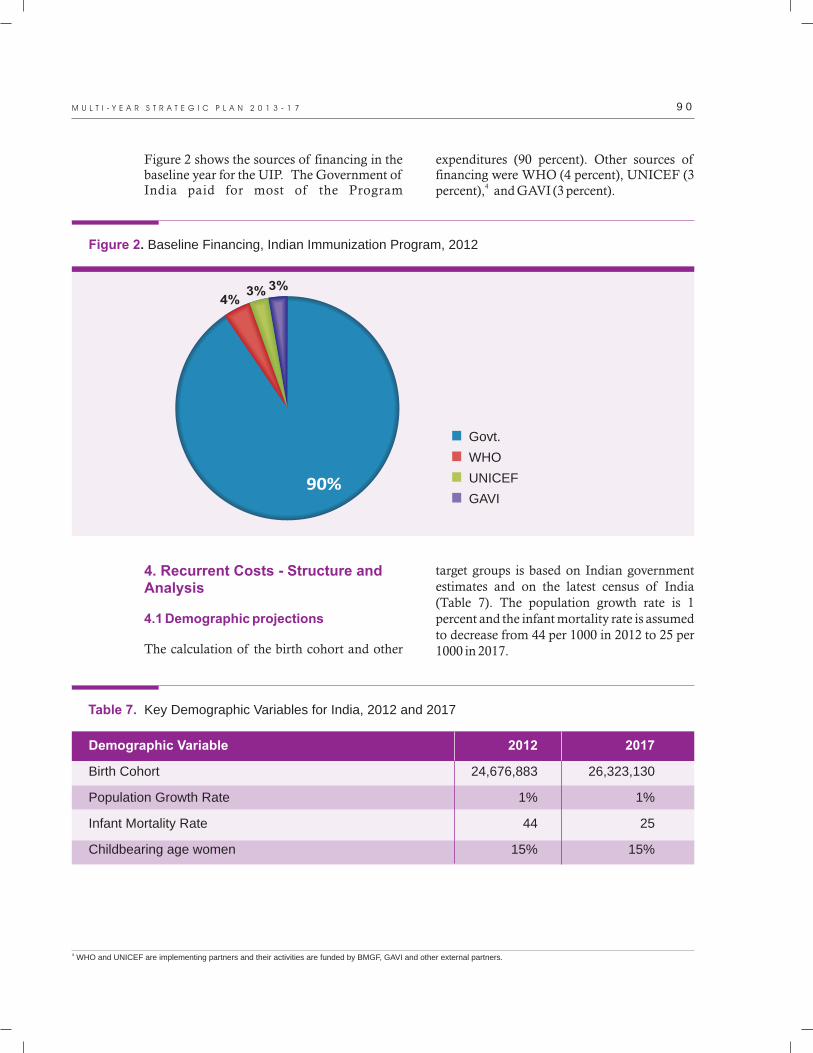
90%
4%3% 3%
Govt.
WHO
UNICEF
GAVI
9 0M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Figure 2. Baseline Financing, Indian Immunization Program, 2012
Figure 2 shows the sources of financing in the baseline year for the UIP. The Government of India paid for most of the Program
expenditures (90 percent). Other sources of financing were WHO (4 percent), UNICEF (3
4percent), and GAVI (3 percent).
4. Recurrent Costs - Structure and Analysis
4.1 Demographic projections
The calculation of the birth cohort and other
target groups is based on Indian government estimates and on the latest census of India (Table 7). The population growth rate is 1 percent and the infant mortality rate is assumed to decrease from 44 per 1000 in 2012 to 25 per 1000 in 2017.
Demographic Variable
Birth Cohort
Population Growth Rate
Infant Mortality Rate
Childbearing age women
2012
24,676,883
1%
44
15%
2017
26,323,130
1%
25
15%
Table 7. Key Demographic Variables for India, 2012 and 2017
4 WHO and UNICEF are implementing partners and their activities are funded by BMGF, GAVI and other external partners.

................................
9 1
4.2 Vaccine and injectionsupplies
The vaccine prices used for the baseline and projections are shown in Table 8. The costs are
a mixture of GAVI prices as well as prices obtainable by the government of India. India is unique since it has many local manufacturers from which it can purchase vaccines for the national Program.
Vaccines
BCG
Hep B (birth dose)
OPV
Measles
DTP
TT
JE
DTP-Hib-HepB (penta)
IPV
MR
Rotavirus
Pneumococcal
Implementation strategy
Routine
Routine
Routine
Routine
Routine
Routine
Campaign
Roll out to all states2014 - 11 states2015 - 16 states
Pan India
Pending NTAGI endorsement. Start with campaign (1-15 yr olds) in 2014. 2015 onwards under routine at 9 months or 1.5 years old.
Pending NTAGI
Pending NTAGI
Sources of financing
Govt.
Govt.
Govt.
Govt.
Govt.
Govt.
Govt.
GAVI up to 2015
Govt.
Govt.
Govt.
Govt.
Table 8. Prices per Dose and Expected start year, and Implementation Strategy for Vaccines
Expected start year
NA
NA
NA
NA
NA
NA
NA
2014-15
2015-16
2014-15
2016-17
2017
Price per dose
USD 0.05
USD 0.05
USD 0.06
USD 0.16
USD 0.04
USD 0.02
USD 0.18
USD 2.11
USD 1.00
USD 0.50*
USD 1.00(Bharat)
USD 3.30**
Sources: *MR: http://www.gavialliance.org/library/news/press-releases/2013/over-700-million-children-in-49-countries-to-be-protected-against-measles-and-rubella/**Pneumococcal: http://www.pfizer.com/news/press-release/press-release-detail/pfizer signs new agreement with unicef to supply a total of up to 740 million doses of prevenar 13 for the world's poorest countries through 2025
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
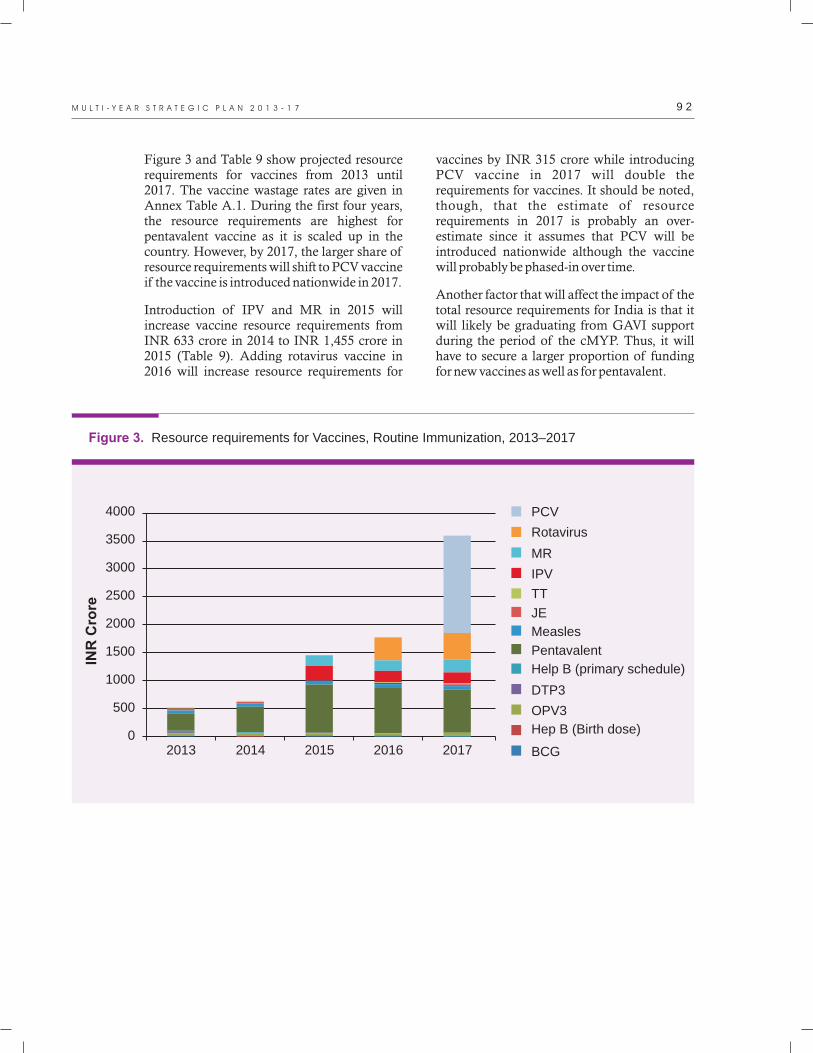
9 2M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Figure 3 and Table 9 show projected resource requirements for vaccines from 2013 until 2017. The vaccine wastage rates are given in Annex Table A.1. During the first four years, the resource requirements are highest for pentavalent vaccine as it is scaled up in the country. However, by 2017, the larger share of resource requirements will shift to PCV vaccine if the vaccine is introduced nationwide in 2017.
Introduction of IPV and MR in 2015 will increase vaccine resource requirements from INR 633 crore in 2014 to INR 1,455 crore in 2015 (Table 9). Adding rotavirus vaccine in 2016 will increase resource requirements for
vaccines by INR 315 crore while introducing PCV vaccine in 2017 will double the requirements for vaccines. It should be noted, though, that the estimate of resource requirements in 2017 is probably an over-estimate since it assumes that PCV will be introduced nationwide although the vaccine will probably be phased-in over time.
Another factor that will affect the impact of the total resource requirements for India is that it will likely be graduating from GAVI support during the period of the cMYP. Thus, it will have to secure a larger proportion of funding for new vaccines as well as for pentavalent.
Figure 3. Resource requirements for Vaccines, Routine Immunization, 2013–2017
INR
Cro
re
4000
3500
3000
2500
2000
1500
1000
500
02013 2014 2015 2016 2017
PCV
Rotavirus
MR
IPV
TT
JE
Measles
Pentavalent
Help B (primary schedule)
DTP3
OPV3
Hep B (Birth dose)
BCG
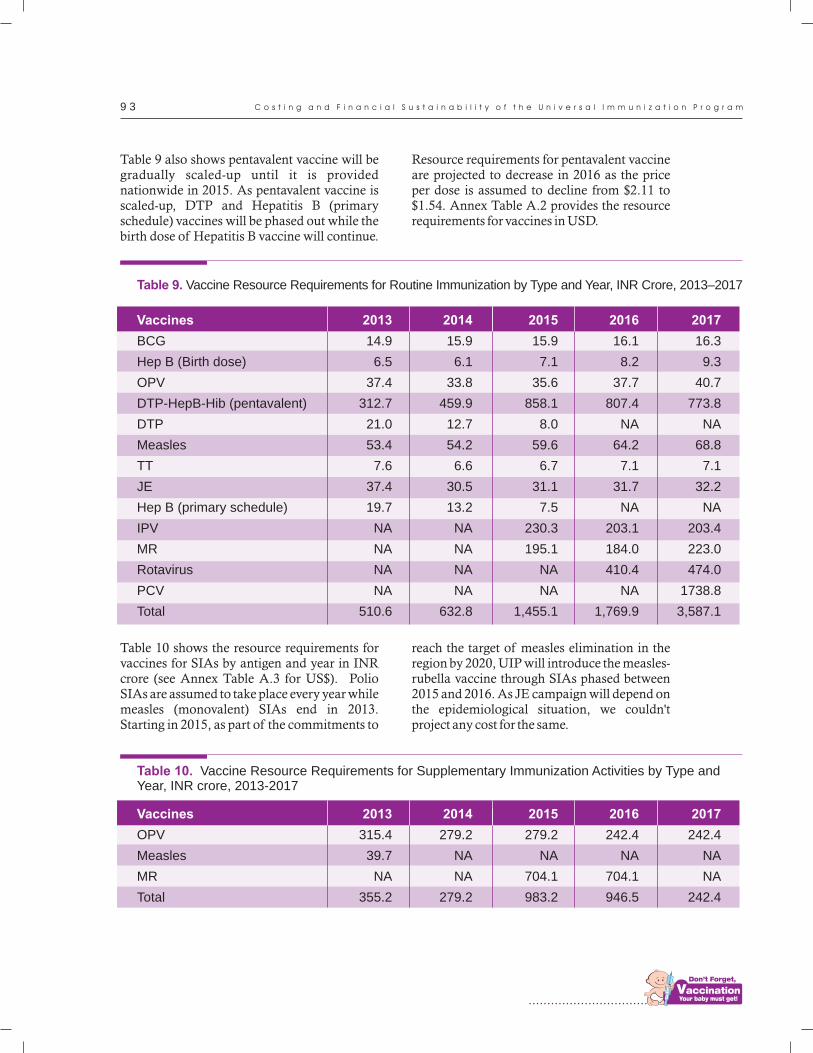
................................
9 3
Table 9 also shows pentavalent vaccine will be gradually scaled-up until it is provided nationwide in 2015. As pentavalent vaccine is scaled-up, DTP and Hepatitis B (primary schedule) vaccines will be phased out while the birth dose of Hepatitis B vaccine will continue.
Resource requirements for pentavalent vaccine are projected to decrease in 2016 as the price per dose is assumed to decline from $2.11 to $1.54. Annex Table A.2 provides the resource requirements for vaccines in USD.
Table 10 shows the resource requirements for vaccines for SIAs by antigen and year in INR crore (see Annex Table A.3 for US$). Polio SIAs are assumed to take place every year while measles (monovalent) SIAs end in 2013. Starting in 2015, as part of the commitments to
reach the target of measles elimination in the region by 2020, UIP will introduce the measles-rubella vaccine through SIAs phased between 2015 and 2016. As JE campaign will depend on the epidemiological situation, we couldn't project any cost for the same.
2015
15.9
7.1
35.6
858.1
8.0
59.6
6.7
31.1
7.5
230.3
195.1
NA
NA
1,455.1
2016
16.1
8.2
37.7
807.4
NA
64.2
7.1
31.7
NA
203.1
184.0
410.4
NA
1,769.9
2014
15.9
6.1
33.8
459.9
12.7
54.2
6.6
30.5
13.2
NA
NA
NA
NA
632.8
2013
14.9
6.5
37.4
312.7
21.0
53.4
7.6
37.4
19.7
NA
NA
NA
NA
510.6
Table 9. Vaccine Resource Requirements for Routine Immunization by Type and Year, INR Crore, 2013–2017
2017
16.3
9.3
40.7
773.8
NA
68.8
7.1
32.2
NA
203.4
223.0
474.0
1738.8
3,587.1
Vaccines
BCG
Hep B (Birth dose)
OPV
DTP-HepB-Hib (pentavalent)
DTP
Measles
TT
JE
Hep B (primary schedule)
IPV
MR
Rotavirus
PCV
Total
2015
279.2
NA
704.1
983.2
2016
242.4
NA
704.1
946.5
2014
279.2
NA
NA
279.2
2013
315.4
39.7
NA
355.2
2017
242.4
NA
NA
242.4
Vaccines
OPV
Measles
MR
Total
Table 10. Vaccine Resource Requirements for Supplementary Immunization Activities by Type and Year, INR crore, 2013-2017
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m

9 4M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
4.3 Personnel Costs
Resource requirements for health care staff are projected based on assumptions about salary ranges, the percentage of time spent on immunization, increase in number of staff per year and annual increases in salary levels. The assumptions on staffing are shown in annex Tables A.4 to A.6. The assumptions about the need for new staffing are based on the findings and recommendations of the 2011 HR Needs Assessment Study (GoI 2011). The study found inadequacies in staffing for the UIP at the national and state levels. Thus, the estimates include recommended additional staff at MOH level (three deputy commissioners and 12 assistant commissioners) and at state level (two Program officers; one MIS officer; one administrative and finance officers; one data
analyst; two cold chain / vaccine handler and vaccine store technicians in each state). At the state level, the estimates also include some new immunization staff such as cold chain/vaccine handler and vaccine store technicians.
Apart from full-time staff, there are shared personnel who work for immunization. Figure 4 shows that resource requirements on shared personnel are much higher than those of full-time staff and are increasing due to annual salary increments and additions to the number of total staff. The amount spent on full-time personnel will increase from INR 55 crore in 2012 to INR 101 crore in 2017 if all new staff are hired as per assumptions given in annex tables. On the other hand, the shared personnel cost will increase from INR 1,315 crore in 2012 to INR 2,509 crore in 2017 (Tables 2 and 11).
Figure 4. Personnel Costs, 2012-2017, INR Crore
INR
Cro
re
2012 2013 2014 2015 2016 2017
3000
2000
1000
0
Baseline Full time personnel
Shared personnel
4.4 Training, Program Management, Disease Surveillance, Social Mobilization, Advocacy and Communication
Training: The government is the main source of funding for trainings (Figure 5). However, the immunization partners such as WHO and
UNICEF also implement some training programs on immunization. The amount spent by the government on training will increase from INR 21 crore in 2012 to INR 42 crore in 2017. The resource requirements are projected to double by 2017 because of the increased need for trainings due to recruitment of health workers, new vaccine introduction and planned SIAs.
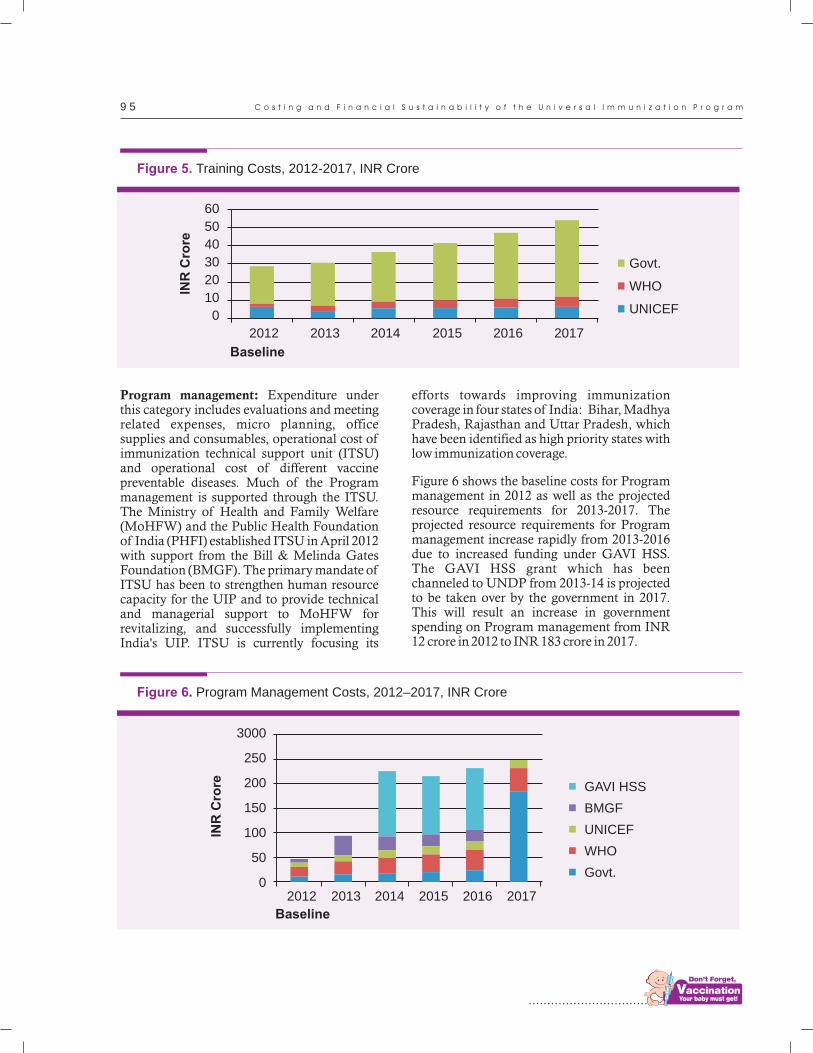
................................
9 5
Program management: Expenditure under this category includes evaluations and meeting related expenses, micro planning, office supplies and consumables, operational cost of immunization technical support unit (ITSU) and operational cost of different vaccine preventable diseases. Much of the Program management is supported through the ITSU. The Ministry of Health and Family Welfare (MoHFW) and the Public Health Foundation of India (PHFI) established ITSU in April 2012 with support from the Bill & Melinda Gates Foundation (BMGF). The primary mandate of ITSU has been to strengthen human resource capacity for the UIP and to provide technical and managerial support to MoHFW for revitalizing, and successfully implementing India's UIP. ITSU is currently focusing its
efforts towards improving immunization coverage in four states of India: Bihar, Madhya Pradesh, Rajasthan and Uttar Pradesh, which have been identified as high priority states with low immunization coverage.
Figure 6 shows the baseline costs for Program management in 2012 as well as the projected resource requirements for 2013-2017. The projected resource requirements for Program management increase rapidly from 2013-2016 due to increased funding under GAVI HSS. The GAVI HSS grant which has been channeled to UNDP from 2013-14 is projected to be taken over by the government in 2017. This will result an increase in government spending on Program management from INR 12 crore in 2012 to INR 183 crore in 2017.
Figure 5. Training Costs, 2012-2017, INR Crore
60
50
40
30
20
10
0
Baseline
2012 2013 2014 2015 2016 2017
Govt.
WHO
UNICEF
INR
Cro
re
Figure 6. Program Management Costs, 2012–2017, INR Crore
Baseline
INR
Cro
re
3000
250
200
150
100
50
02012 2013 2014 2015 2016 2017
GAVI HSS
BMGF
UNICEF
WHO
Govt.
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
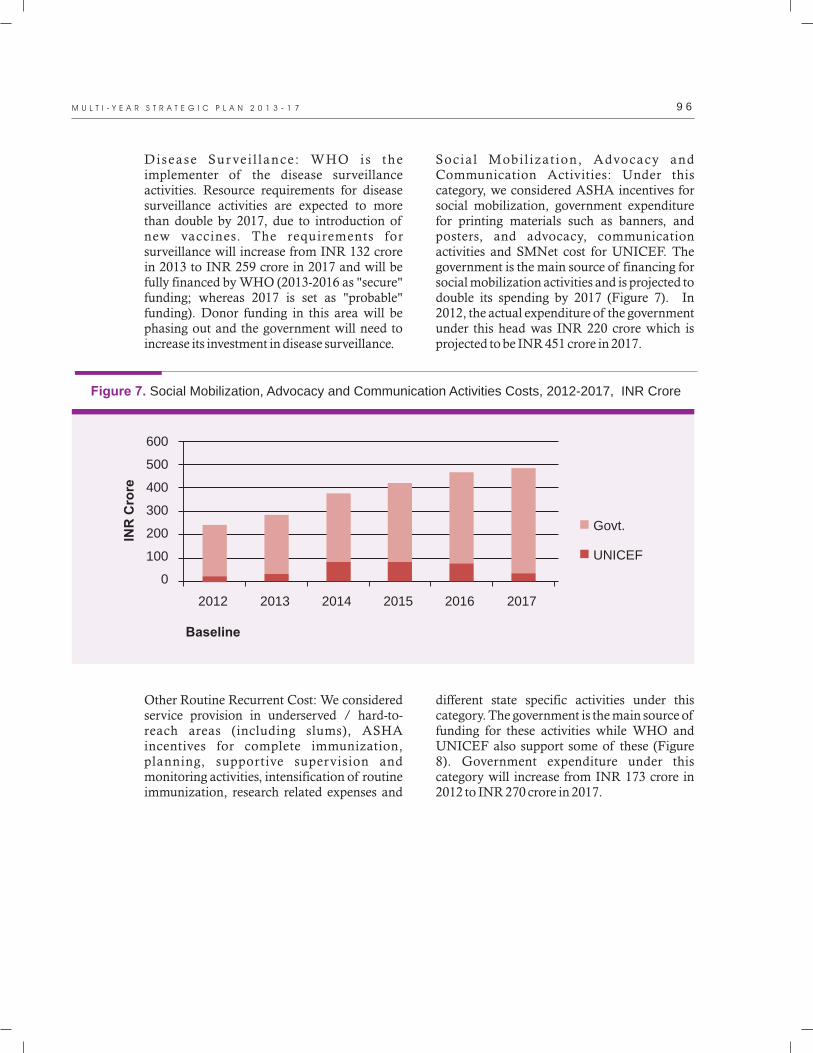
9 6M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Disease Sur ve i l lance : WHO is the implementer of the disease surveillance activities. Resource requirements for disease surveillance activities are expected to more than double by 2017, due to introduction of new vaccines. The requirements for surveillance will increase from INR 132 crore in 2013 to INR 259 crore in 2017 and will be fully financed by WHO (2013-2016 as "secure" funding; whereas 2017 is set as "probable" funding). Donor funding in this area will be phasing out and the government will need to increase its investment in disease surveillance.
Social Mobi l izat ion, Advocacy and Communication Activities: Under this category, we considered ASHA incentives for social mobilization, government expenditure for printing materials such as banners, and posters, and advocacy, communication activities and SMNet cost for UNICEF. The government is the main source of financing for social mobilization activities and is projected to double its spending by 2017 (Figure 7). In 2012, the actual expenditure of the government under this head was INR 220 crore which is projected to be INR 451 crore in 2017.
Figure 7. Social Mobilization, Advocacy and Communication Activities Costs, 2012-2017, INR Crore
Baseline
INR
Cro
re
600
500
400
300
200
100
0
2012 2013 2014 2015 2016 2017
Govt.
UNICEF
Other Routine Recurrent Cost: We considered service provision in underserved / hard-to-reach areas (including slums), ASHA incentives for complete immunization, planning, supportive supervision and monitoring activities, intensification of routine immunization, research related expenses and
different state specific activities under this category. The government is the main source of funding for these activities while WHO and UNICEF also support some of these (Figure 8). Government expenditure under this category will increase from INR 173 crore in 2012 to INR 270 crore in 2017.
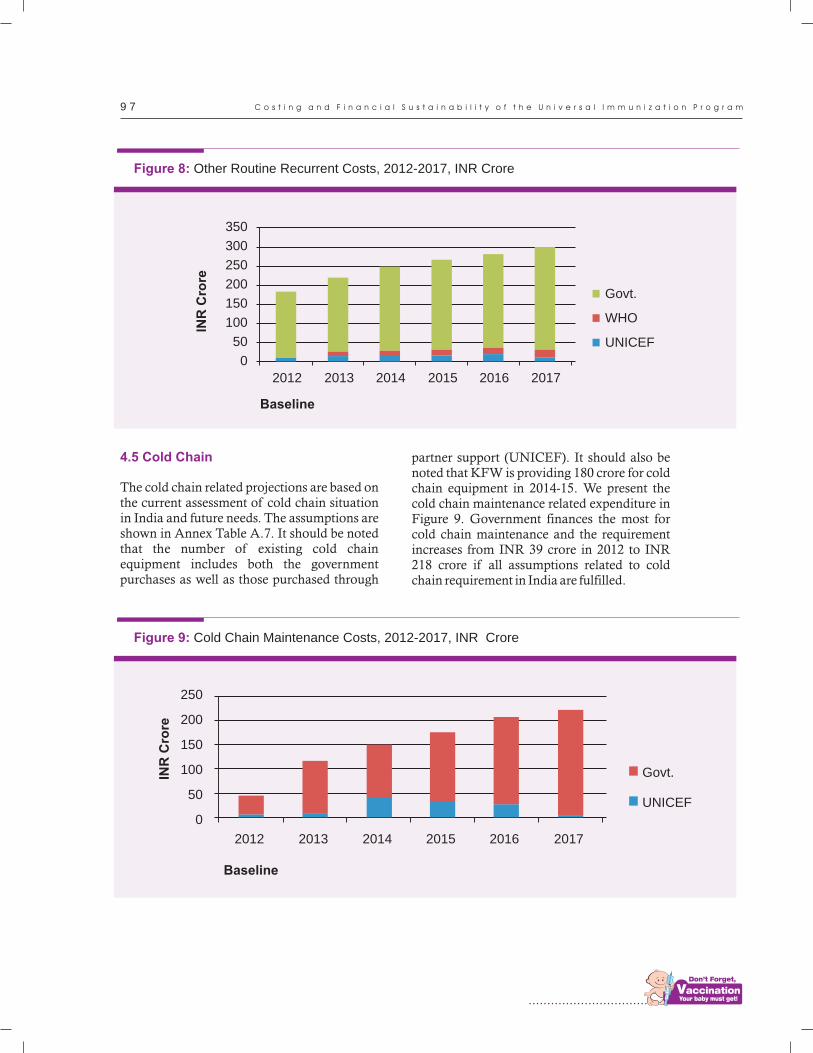
................................
9 7
4.5 Cold Chain
The cold chain related projections are based on the current assessment of cold chain situation in India and future needs. The assumptions are shown in Annex Table A.7. It should be noted that the number of existing cold chain equipment includes both the government purchases as well as those purchased through
partner support (UNICEF). It should also be noted that KFW is providing 180 crore for cold chain equipment in 2014-15. We present the cold chain maintenance related expenditure in Figure 9. Government finances the most for cold chain maintenance and the requirement increases from INR 39 crore in 2012 to INR 218 crore if all assumptions related to cold chain requirement in India are fulfilled.
Figure 8: Other Routine Recurrent Costs, 2012-2017, INR Crore
Baseline
INR
Cro
re
350
300
250
200
150
100
50
0
2012 2013 2014 2015 2016 2017
Govt.
WHO
UNICEF
Figure 9: Cold Chain Maintenance Costs, 2012-2017, INR Crore
Baseline
INR
Cro
re
250
200
150
100
50
0
2012 2013 2014 2015 2016 2017
Govt.
UNICEF
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m

9 8M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
5.0. Future Resource Requirements
Table 11 and Figure 10 show the future resource requirements for the routine immunization Program by Program components. Total requirement for the five-year period is INR
34,336 crore ($5,282 million). Resource requirements for vaccines increase rapidly from INR 510 crore in 2013 to INR 3,587 crore in 2017 as new vaccines are assumed to be introduced in the Program. The amount in USD is presented in Annex Table A.8.
Cost Category
Vaccines (routine vaccines only)
Injection supplies
Personnel
Transportation
Cold chain and other capital equipment maintenance
Training
Social mobilization / advocacy / communication activities
Disease surveillance
Program management
Other routine recurrent costs
Cold chain equipment
Supplemental Immunization Activities
Shared personnel costs
Total
2013
510.6
71.8
78.7
203.4
116.3
30.8
284.1
132.9
94.1
219.3
131.4
789.6
1,907.1
4,570.0
Table 11. Resource Requirements for India National Immunization Program, INR crore, 2013-2017
2014
632.8
72.3
84.7
234.9
149.4
36.5
373.8
161.4
225.5
248.4
198.2
740.6
2,042.5
5,201.0
2015
1,455.1
89.7
89.9
271.3
175.9
41.5
421.3
186.4
215.4
266.3
269.2
1,520.7
2,187.5
7,190.2
2016
1,769.9
84.7
95.5
313.3
207.0
47.4
467.9
215.3
231.7
282.0
343.6
1,522.6
2,342.8
7,923.9
2017
3,587.1
102.9
101.4
361.9
220.9
54.1
483.1
248.7
248.5
300.2
419.7
813.5
2,509.1
9,451.0
Total
7,955.5
421.4
450.2
1,384.8
869.4
210.3
2,030.3
944.7
1,015.2
1,316.3
1,362.1
5,386.9
10,989.0
34,336.1

................................
9 9
6.0. Future Financing and funding gap analysis
Figure 11 shows the future secure financing
and gaps in financing for 2013-2017. This
figure does not include other financing that is 5probable. The largest source of financing for
UIP is the government. The financing gap
increases from INR 56 crore in 2013 to 815
crore in 2015 and further to INR 3,537 crore in
2017 and reflects the fact that funding has not
yet been secured for the new vaccines to be
introduced during those years.
Figure 10. Total Resource Requirements for UIP, 2013-2017, INR CroreIN
R C
rore
10000
9000
8000
7000
6000
5000
4000
3000
2000
1000
02013 2014 2015 2016 2017
Shared personnel costs
Supplemental Immunization Activities
Cold chain equipment
Other routine recurrent costs
Program managememt
Disease surveillance
Social mobilization / advocacy /communication activities
Training
Cold chain and other capitalequipment maintenance
Personnel
Injection supplies
Vaccines (routine vaccines only)
Transportation
5cMYP costing & financing tool has two categories of funding: 1.Secure funding refers to projected future financing available in the short term, that is considered assured;2.Probable funding refers to all other funding that is not assured but is likely to be made available in the short and medium term.
C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
Figure 11. Future Secure Financing and Funding Gaps, 2013-2017, INR Crore
INR
Cro
re
10000
8000
6000
4000
2000
02013 2014 2015 2016 2017
Funding Gap
GAVI HSS
BMGF (ITSU)
GAVI
UNICEF
WHO
Govt.
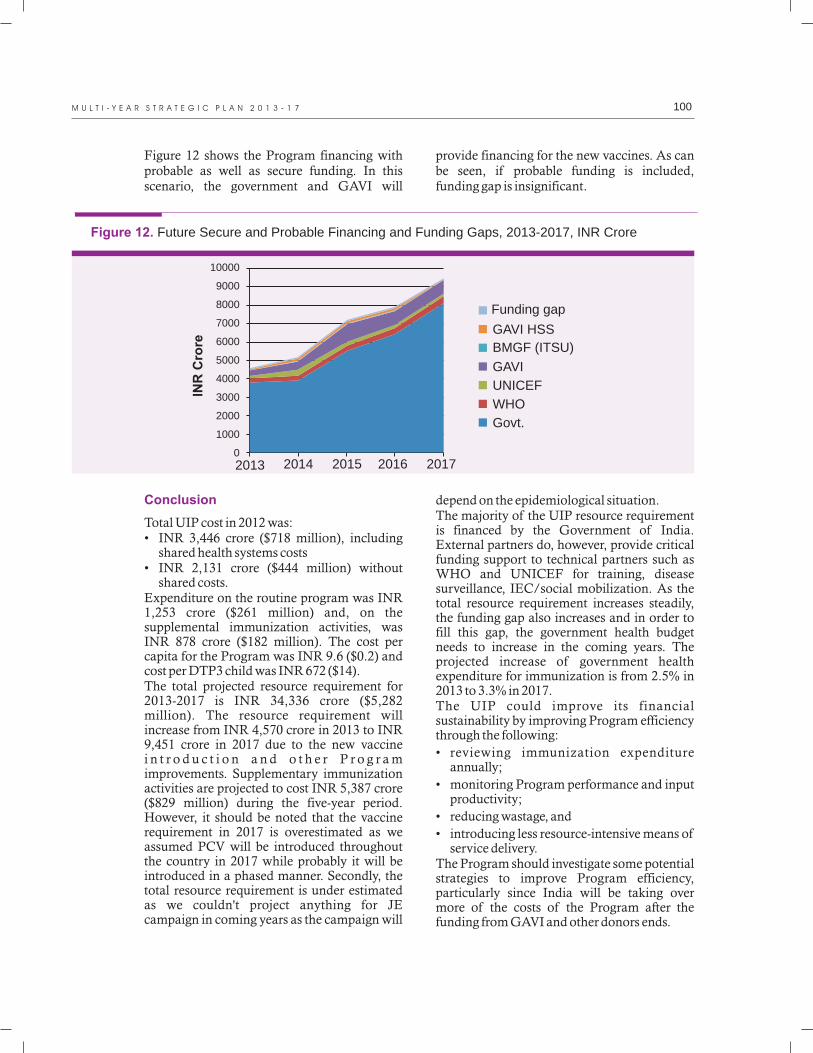
100M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Figure 12 shows the Program financing with probable as well as secure funding. In this scenario, the government and GAVI will
provide financing for the new vaccines. As can be seen, if probable funding is included, funding gap is insignificant.
Figure 12. Future Secure and Probable Financing and Funding Gaps, 2013-2017, INR Crore
INR
Cro
re
10000
9000
8000
7000
6000
5000
4000
3000
2000
1000
02013 2014 2015 2016 2017
Funding gap
GAVI HSS
BMGF (ITSU)
GAVI
UNICEF
WHO
Govt.
Conclusion
Total UIP cost in 2012 was:• INR 3,446 crore ($718 million), including
shared health systems costs• INR 2,131 crore ($444 million) without
shared costs. Expenditure on the routine program was INR 1,253 crore ($261 million) and, on the supplemental immunization activities, was INR 878 crore ($182 million). The cost per capita for the Program was INR 9.6 ($0.2) and cost per DTP3 child was INR 672 ($14). The total projected resource requirement for 2013-2017 is INR 34,336 crore ($5,282 million). The resource requirement will increase from INR 4,570 crore in 2013 to INR 9,451 crore in 2017 due to the new vaccine i n t r o d u c t i o n a n d o t h e r P r o g r a m improvements. Supplementary immunization activities are projected to cost INR 5,387 crore ($829 million) during the five-year period. However, it should be noted that the vaccine requirement in 2017 is overestimated as we assumed PCV will be introduced throughout the country in 2017 while probably it will be introduced in a phased manner. Secondly, the total resource requirement is under estimated as we couldn't project anything for JE campaign in coming years as the campaign will
depend on the epidemiological situation.The majority of the UIP resource requirement is financed by the Government of India. External partners do, however, provide critical funding support to technical partners such as WHO and UNICEF for training, disease surveillance, IEC/social mobilization. As the total resource requirement increases steadily, the funding gap also increases and in order to fill this gap, the government health budget needs to increase in the coming years. The projected increase of government health expenditure for immunization is from 2.5% in 2013 to 3.3% in 2017.The UIP could improve its financial sustainability by improving Program efficiency through the following:
• reviewing immunization expenditure annually;
• monitoring Program performance and input productivity;
• reducing wastage, and
• introducing less resource-intensive means of service delivery.
The Program should investigate some potential strategies to improve Program efficiency, particularly since India will be taking over more of the costs of the Program after the funding from GAVI and other donors ends.

................................
101 C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
Annexures
A.1 Wastage rates
Proposed wastage rates for single and ten dose vials are in line with WHO/UNICEF recommendations and others are as per government wastage rate calculations.
Vaccine
BCG
Hep B (birth dose)
OPV
DTP-Hep B- Hib (Penta)
DTP3
Measles
MR
Hepatitis B
IPV
JE
TT
Table A.1. Assumptions on Wastage Rates by Antigen
2013 (percentage)
50
15
25
25
25
25
25
25
30
25
25
2017 (percentage)
10
10
25
10
30
10
Table A.2. Vaccine Resource Requirements for Routine Immunization by Type and Year, US$ millions, 2013-2017
Vaccines
BCG
Hep B (Birth dose)
OPV3
DTP-Hep B-Hib (Pentavalent)
DTP
Measles
TT
JE
Hep B (primary schedule)
IPV
MR
Rotavirus
PCV
Total
2013
2.3
1.0
5.8
48.1
3.2
8.2
1.2
5.8
3.0
NA
NA
NA
NA
78.5
2014
2.4
0.9
5.2
70.8
1.9
8.3
1.0
4.7
2.0
NA
NA
NA
NA
97.4
2015
2.4
1.1
5.5
132.0
1.2
9.2
1.0
4.8
1.2
35.4
30.0
N
N
223.9
2016
2.5
1.3
5.8
124.2
0.0
9.9
1.1
4.9
NA
31.3
28.3
63.1
NA
272.3
2017
2.5
1.4
6.3
119.0
0.0
10.6
1.1
4.9
NA
31.3
34.3
72.9
267.5
551.9

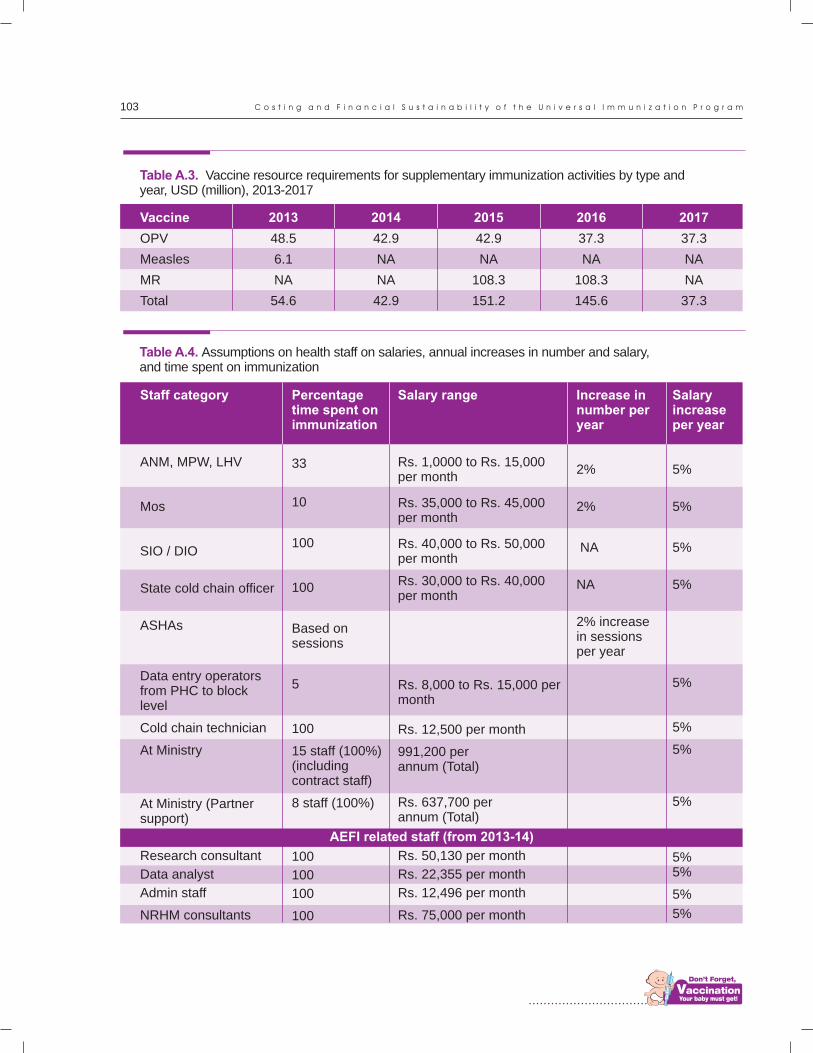
................................
103 C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
Vaccine
OPV
Measles
MR
Total
Table A.3. Vaccine resource requirements for supplementary immunization activities by type and year, USD (million), 2013-2017
2013
48.5
6.1
NA
54.6
2014
42.9
NA
NA
42.9
2015
42.9
NA
108.3
151.2
2016
37.3
NA
108.3
145.6
2017
37.3
NA
NA
37.3
Table A.4. Assumptions on health staff on salaries, annual increases in number and salary, and time spent on immunization
Salary range
Rs. 1,0000 to Rs. 15,000 per month
Rs. 35,000 to Rs. 45,000 per month
Rs. 40,000 to Rs. 50,000 per month
Rs. 30,000 to Rs. 40,000 per month
Rs. 8,000 to Rs. 15,000 per month
Rs. 12,500 per month
991,200 per annum (Total)
Rs. 637,700 per annum (Total)
Rs. 50,130 per month
Rs. 22,355 per month
Rs. 12,496 per month
Rs. 75,000 per month
Percentage time spent on immunization
33
10
100
100
Based on sessions
5
100
15 staff (100%) (including contract staff)
8 staff (100%)
100
100
100
100
Increase in number per year
2%
2%
NA
NA
2% increase in sessions per year
Salary increase per year
5%
5%
5%
5%
5%
5%
5%
5%
5%5%
5%
5%
Staff category
ANM, MPW, LHV
Mos
SIO / DIO
State cold chain officer
ASHAs
Data entry operators from PHC to block level
Cold chain technician
At Ministry
At Ministry (Partner support)
Research consultant
Data analyst
Admin staff
NRHM consultants
AEFI related staff (from 2013-14)

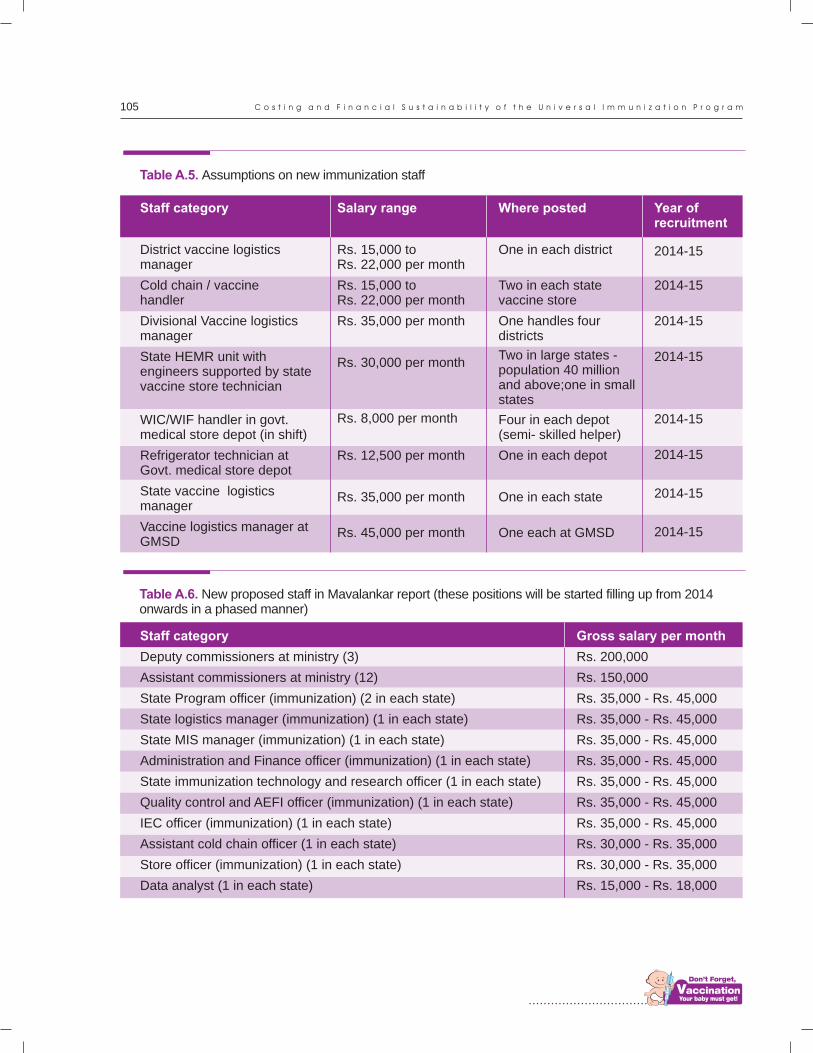
................................
105 C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
Staff category
District vaccine logistics manager
Cold chain / vaccine handler
Divisional Vaccine logistics manager
State HEMR unit with engineers supported by state vaccine store technician
WIC/WIF handler in govt. medical store depot (in shift)
Refrigerator technician at Govt. medical store depot
State vaccine logistics manager
Vaccine logistics manager at GMSD
Salary range
Rs. 15,000 to Rs. 22,000 per month
Rs. 15,000 to Rs. 22,000 per month
Rs. 35,000 per month
Rs. 30,000 per month
Rs. 8,000 per month
Rs. 12,500 per month
Rs. 35,000 per month
Rs. 45,000 per month
Table A.5. Assumptions on new immunization staff
Where posted
One in each district
Two in each state vaccine store
One handles four districts
Two in large states - population 40 million and above;one in small states
Four in each depot (semi- skilled helper)
One in each depot
One in each state
One each at GMSD
Year of recruitment
2014-15
2014-15
2014-15
2014-15
2014-15
2014-15
2014-15
2014-15
Staff category
Deputy commissioners at ministry (3)
Assistant commissioners at ministry (12)
State Program officer (immunization) (2 in each state)
State logistics manager (immunization) (1 in each state)
State MIS manager (immunization) (1 in each state)
Administration and Finance officer (immunization) (1 in each state)
State immunization technology and research officer (1 in each state)
Quality control and AEFI officer (immunization) (1 in each state)
IEC officer (immunization) (1 in each state)
Assistant cold chain officer (1 in each state)
Store officer (immunization) (1 in each state)
Data analyst (1 in each state)
Gross salary per month
Rs. 200,000
Rs. 150,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 35,000 - Rs. 45,000
Rs. 30,000 - Rs. 35,000
Rs. 30,000 - Rs. 35,000
Rs. 15,000 - Rs. 18,000
Table A.6. New proposed staff in Mavalankar report (these positions will be started filling up from 2014 onwards in a phased manner)

106M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Number of cold chain points (existing)
Cold chain points required
Total cold chain points required
New cold chain points required
Present number of ILR in cold chain points
Present number of DF in cold chain points
Existing ILR/DF needs replacement
New ILR / DF required at cold chain points
Cold chain points need solar or hybrid
.
Existing solar or hybrid
Solar or hybrid
At GMSD level
Present number of WIC at GMSD
Present number of WIF at GMSD
Required WICs/WIFs
27,000
One cold chain point per 30,000 population (2011 census)
40,340
28,238
27,000 (assuming one in each cold chain point)
27,000 (assuming one in each cold chain point)
50% (27,000) needs immediate replacement - should be replaced within 2-3 years
The required number (56,476) will be procured within 3 years
30% of all PHCs will have less than 8 hours electricity; hence need solar or hybrid
50% of these will be hybrid where there is supply for 4-6 hours
Solar - 270; Hybrid - 300.
The required number (Solar - 5,781; hybrid - 5,751) will be procured in 2-3 years
At each GMSD, 8 WIC of 40 cub. Mt; 4 WIF to accommodate rotavirus / IPV vaccine
8
6
Required number at GMSD level (22 WICs / 10 WIFs) will be available in 2 years
State report NCCMIS
CCO meeting minutes
CCO meeting minutes
CCO meeting minutes
CCO meeting minutes + standard assumptions
CCO meeting minutes + standard assumptions
Based on NCCMIS of ageing and useful life of 10 years
Based on NCCMIS of ageing and useful life of 10 years
NCCMIS
.
State CCO Report
NCCMIS
National EVM, 2013
National EVM, 2013
National EVM, 2013
National EVM, 2013
Table A.7 Cold chain related assumptions
Assumptions Sources
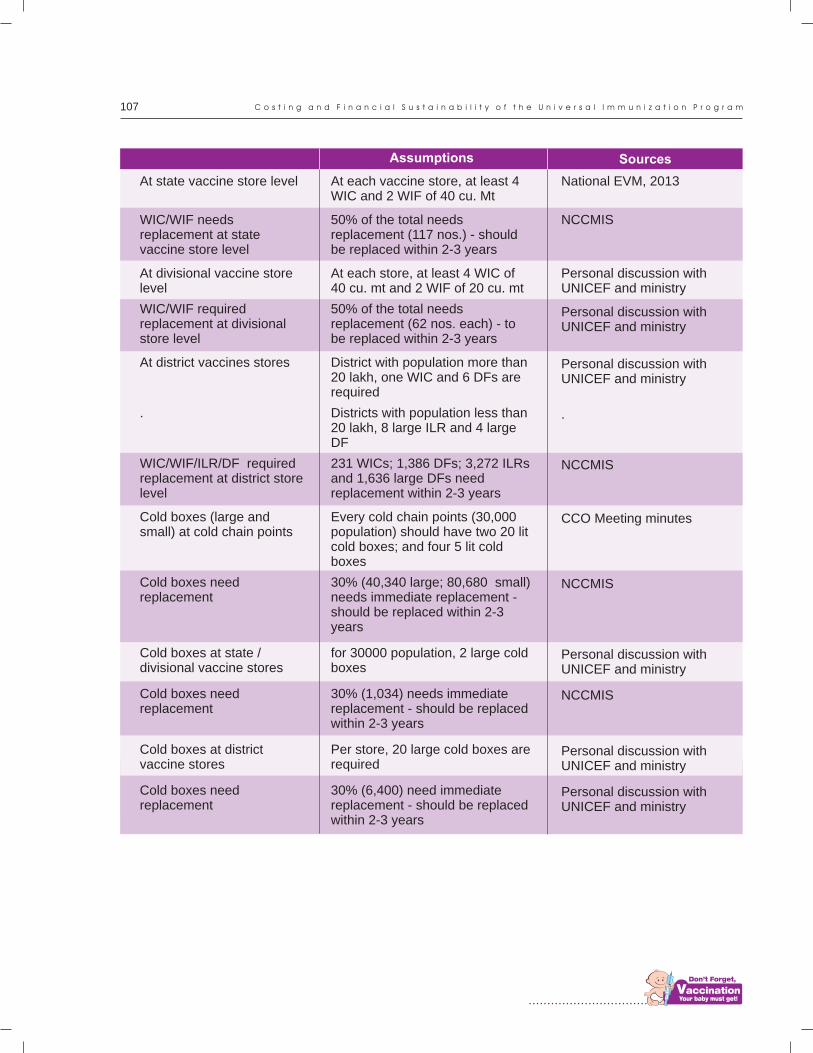
................................
107 C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
At state vaccine store level
WIC/WIF needs replacement at state vaccine store level
At divisional vaccine store level
WIC/WIF required replacement at divisional store level
At district vaccines stores
.
WIC/WIF/ILR/DF required replacement at district store level
Cold boxes (large and small) at cold chain points
Cold boxes need replacement
Cold boxes at state / divisional vaccine stores
Cold boxes need replacement
Cold boxes at district vaccine stores
Cold boxes need replacement
At each vaccine store, at least 4 WIC and 2 WIF of 40 cu. Mt
50% of the total needs replacement (117 nos.) - should be replaced within 2-3 years
At each store, at least 4 WIC of 40 cu. mt and 2 WIF of 20 cu. mt
50% of the total needs replacement (62 nos. each) - to be replaced within 2-3 years
District with population more than 20 lakh, one WIC and 6 DFs are required
Districts with population less than 20 lakh, 8 large ILR and 4 large DF
231 WICs; 1,386 DFs; 3,272 ILRs and 1,636 large DFs need replacement within 2-3 years
Every cold chain points (30,000 population) should have two 20 lit cold boxes; and four 5 lit cold boxes
30% (40,340 large; 80,680 small) needs immediate replacement - should be replaced within 2-3 years
for 30000 population, 2 large cold boxes
30% (1,034) needs immediate replacement - should be replaced within 2-3 years
Per store, 20 large cold boxes are required
30% (6,400) need immediate replacement - should be replaced within 2-3 years
National EVM, 2013
NCCMIS
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
.
NCCMIS
CCO Meeting minutes
NCCMIS
Personal discussion with UNICEF and ministry
NCCMIS
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Assumptions Sources
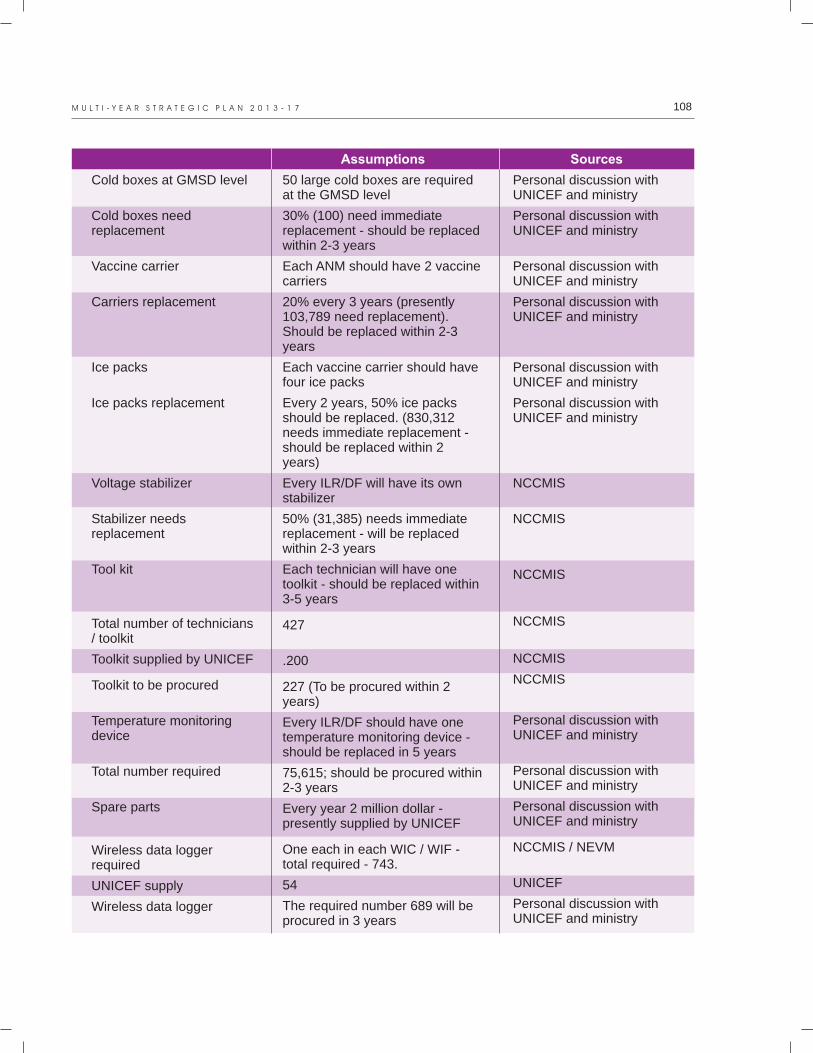
108M U L T I - Y E A R S T R A T E G I C P L A N 2 0 1 3 - 1 7
Cold boxes at GMSD level
Cold boxes need replacement
Vaccine carrier
Carriers replacement
Ice packs
Ice packs replacement
Voltage stabilizer
Stabilizer needs replacement
Tool kit
Total number of technicians / toolkit
Toolkit supplied by UNICEF
Toolkit to be procured
Temperature monitoring device
Total number required
Spare parts
Wireless data logger required
UNICEF supply
Wireless data logger
Assumptions
50 large cold boxes are required at the GMSD level
30% (100) need immediate replacement - should be replaced within 2-3 years
Each ANM should have 2 vaccine carriers
20% every 3 years (presently 103,789 need replacement). Should be replaced within 2-3 years
Each vaccine carrier should have four ice packs
Every 2 years, 50% ice packs should be replaced. (830,312 needs immediate replacement - should be replaced within 2 years)
Every ILR/DF will have its own stabilizer
50% (31,385) needs immediate replacement - will be replaced within 2-3 years
Each technician will have one toolkit - should be replaced within 3-5 years
427
.200
227 (To be procured within 2 years)
Every ILR/DF should have one temperature monitoring device - should be replaced in 5 years
75,615; should be procured within 2-3 years
Every year 2 million dollar - presently supplied by UNICEF
One each in each WIC / WIF - total required - 743.
54
The required number 689 will be procured in 3 years
Sources
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
NCCMIS
NCCMIS
NCCMIS
NCCMIS
NCCMIS
NCCMIS
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
Personal discussion with UNICEF and ministry
NCCMIS / NEVM
UNICEF
Personal discussion with UNICEF and ministry
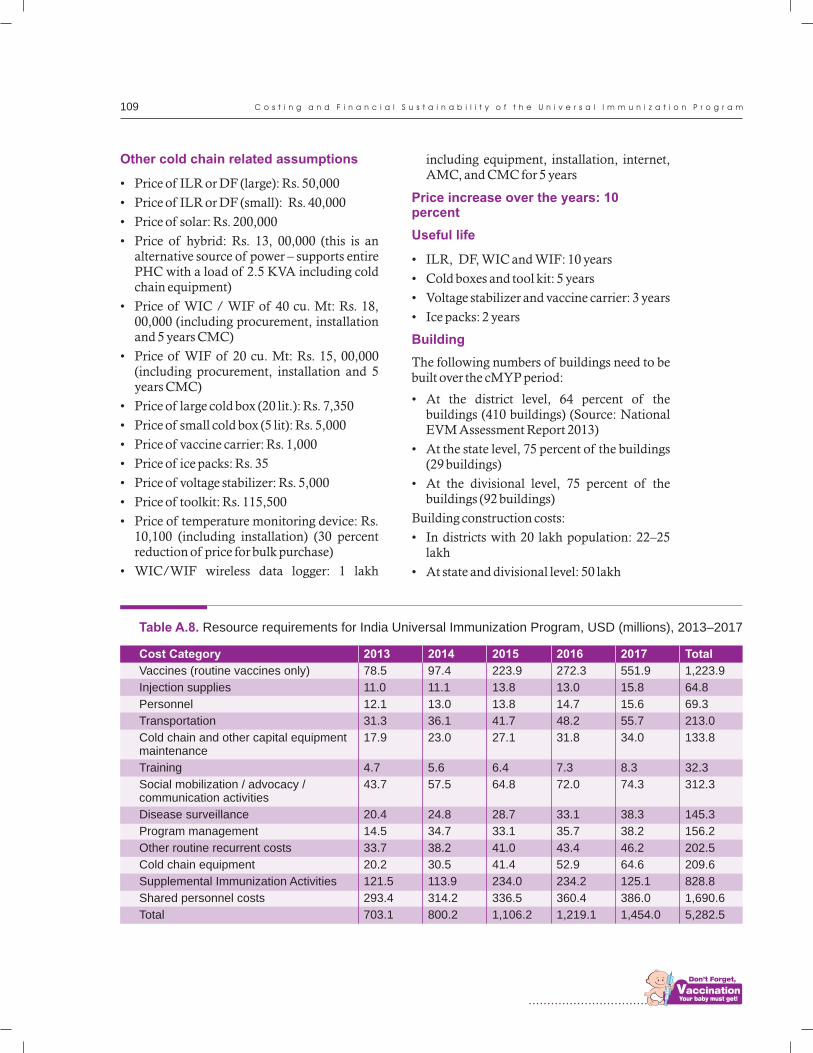
................................
109 C o s t i n g a n d F i n a n c i a l S u s t a i n a b i l i t y o f t h e U n i v e r s a l I m m u n i z a t i o n P r o g r a m
Table A.8. Resource requirements for India Universal Immunization Program, USD (millions), 2013–2017
Cost Category
Vaccines (routine vaccines only)
Injection supplies
Personnel
Transportation
Cold chain and other capital equipment maintenance
Training
Social mobilization / advocacy / communication activities
Disease surveillance
Program management
Other routine recurrent costs
Cold chain equipment
Supplemental Immunization Activities
Shared personnel costs
Total
2013
78.5
11.0
12.1
31.3
17.9
4.7
43.7
20.4
14.5
33.7
20.2
121.5
293.4
703.1
2014
97.4
11.1
13.0
36.1
23.0
5.6
57.5
24.8
34.7
38.2
30.5
113.9
314.2
800.2
2015
223.9
13.8
13.8
41.7
27.1
6.4
64.8
28.7
33.1
41.0
41.4
234.0
336.5
1,106.2
2016
272.3
13.0
14.7
48.2
31.8
7.3
72.0
33.1
35.7
43.4
52.9
234.2
360.4
1,219.1
2017
551.9
15.8
15.6
55.7
34.0
8.3
74.3
38.3
38.2
46.2
64.6
125.1
386.0
1,454.0
Total
1,223.9
64.8
69.3
213.0
133.8
32.3
312.3
145.3
156.2
202.5
209.6
828.8
1,690.6
5,282.5
Other cold chain related assumptions
• Price of ILR or DF (large): Rs. 50,000
• Price of ILR or DF (small): Rs. 40,000
• Price of solar: Rs. 200,000
• Price of hybrid: Rs. 13, 00,000 (this is an alternative source of power – supports entire PHC with a load of 2.5 KVA including cold chain equipment)
• Price of WIC / WIF of 40 cu. Mt: Rs. 18, 00,000 (including procurement, installation and 5 years CMC)
• Price of WIF of 20 cu. Mt: Rs. 15, 00,000 (including procurement, installation and 5 years CMC)
• Price of large cold box (20 lit.): Rs. 7,350
• Price of small cold box (5 lit): Rs. 5,000
• Price of vaccine carrier: Rs. 1,000
• Price of ice packs: Rs. 35
• Price of voltage stabilizer: Rs. 5,000
• Price of toolkit: Rs. 115,500
• Price of temperature monitoring device: Rs. 10,100 (including installation) (30 percent reduction of price for bulk purchase)
• WIC/WIF wireless data logger: 1 lakh
including equipment, installation, internet, AMC, and CMC for 5 years
• ILR, DF, WIC and WIF: 10 years
• Cold boxes and tool kit: 5 years
• Voltage stabilizer and vaccine carrier: 3 years
• Ice packs: 2 years
The following numbers of buildings need to be built over the cMYP period:
• At the district level, 64 percent of the buildings (410 buildings) (Source: National EVM Assessment Report 2013)
• At the state level, 75 percent of the buildings (29 buildings)
• At the divisional level, 75 percent of the buildings (92 buildings)
Building construction costs:
• In districts with 20 lakh population: 22–25 lakh
• At state and divisional level: 50 lakh
Price increase over the years: 10 percent
Useful life
Building

