complete remission is a reachable goal in mrcc - kca … · 2014-05-14 · complete remission is a...
TRANSCRIPT
Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Complete Remission is a Reachable Goal in mRCC
L. Albiges
Institut Gustave Roussy

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Is complete remission an achievable goal in mRCC?
• Lessons from observation
• Lessons from immunotherapy
• Current status in VEGFR/mTOR targeting therapy
• Coming steps

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Is complete remission an achievable goal in mRCC?
• Lessons from observation
• Lessons from immunotherapy
• Current status in VEGFR/mTOR targeting therapy
• Coming steps

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
73 year old lady
11/2000: Kidney tumor with pleural effusion and lung nodules
Pleural biopsy showed pleural mets
Nephrectomy performed: clear cell RCC, grade 2
Lessons from clinical case

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
11/2000
2/2001
Control CT scan performed before systemic
treatment

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
11/2000
2/2001
2/2009

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Is complete remission an achievable goal in mRCC?
• Lessons from observation
• Lessons from immunotherapy
• Current status in VEGFR/mTOR targeting therapy
• Coming steps

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Immunotherapy ERA
Yes CR is achievable and immune response is involved
Study Treatment n Complete Remission
(%)
Median CR
duration
(months)
MRC
Lancet 1999
IFN vs MPA 335 2%
Pyrhonen
JCO 1999
IFN-vbl vs Vbl 160 8%
(7/80)
6
(3-65)
Motzer
JCO 2000
IFN-cRA vs IFN 284 5% (5/139)
1% (1/145)
4%
Fisher
Can J Sci Am 2000
IL2HD 255 7%
(17/255)
80
(7-131)
Atzpodien
Cancer 2002
IL2- & IFN (+5FU or 13cRA) 443 8%
(37/443)
13 years
Coppin
CochraneDatabase 2005
Meta analysis of randomized
study with IFN
6117 4%
51 study/53
Négrier
Cancer J Sci Am. 2000
4 studies <8% Up to 5 years
Figlin
Cancer J Sci Am. 1997
6%
(12/203)
36

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Immunotherapy ERA
Yes CR is achievable and immune response is involved
• Identification of predictive factors for CR? – Factors of prolonged CR (predictive of CR duration)
• Number of metastatic site
• Cytoreductive Nephrectomy
• IL2 HD vs non HD
– Biological factors
• SELECT trial McDermott, ASCO JCO210
Elias, Oncology 2001

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
Is complete remission an achievable goal in mRCC?
• Lessons from observation
• Lessons from immunotherapy
• Current status in VEGFR targeting therapy
• Coming soon

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
• Achievable with medical treatment only?
– incidence among phase III? • <1% across all
– Mecanism of action? • VEGFR target, tumor cell effect
• Immuno-modulation
– Neo adjuvant data? No pCR!
VEGFR TKI era
Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
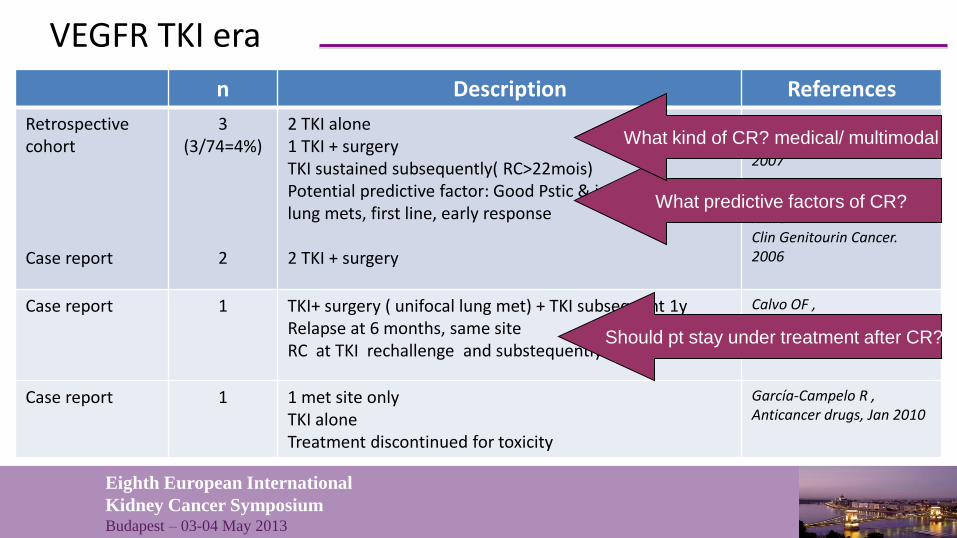
VEGFR TKI era
n Description References
Retrospective cohort Case report
3 (3/74=4%)
2
2 TKI alone 1 TKI + surgery TKI sustained subsequently( RC>22mois) Potential predictive factor: Good Pstic & intermediate, lung mets, first line, early response 2 TKI + surgery
Heng DY, Clin Genitourin Cancer. 2007 Rini B Clin Genitourin Cancer. 2006
Case report 1 TKI+ surgery ( unifocal lung met) + TKI subsequent 1y Relapse at 6 months, same site RC at TKI rechallenge and substequently sustained
Calvo OF , Anticancer drugs, Jan 2010
Case report 1 1 met site only TKI alone Treatment discontinued for toxicity
García-Campelo R , Anticancer drugs, Jan 2010
What predictive factors of CR?
Should pt stay under treatment after CR?
What kind of CR? medical/ multimodal

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
n Caractéristiques Références
Retrospective study 12 (12/266= 4%)
6 TKI alone 6 TKI + surgery Median FU 8.5 m; TTP: 6 mo 5/12 relapse (41%) 100% PR or SD at TKI re-introduction
Johanssen M, Eu Urol , Jun 2009
Retrospective study 5 (5/194=2.5%)
5 ccRCC 2 TKI alone 3 TKI + surgery 4/5 case : TKI discontinuation, 1/5 TKI continuation Median FU 24 mo, no relapse
Staehler M , Urol Oncol , Mar 2010
Retrospective study 36 (*12 + 24)
16 TKI alone 20 TKI+ local treatment 34/36 ccRCC Favorable pstic 39%, intermediate pstic: 61% 22 sunitinib; 11 sorafenib; 2 bevacizumab; 1 temsirolimus Median time to CR: 12mo Relapse: 24/36 ( 66,7%) TKI efficacy at re-introduction: PR or SD: 87% 12 Pt without relapse with 12mo median FU Median of drug – off period: 7m
Johannsen M, Ann Oncol 2011

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
n Caractéristiques Références
Retrospective study 12 (12/266= 4%)
6 TKI alone 6 TKI + surgery Median FU 8.5 m; TTP: 6 mo 5/12 relapse (41%) 100% PR or SD at TKI re-introduction
Johanssen M, Eu Urol , Jun 2009
Retrospective study 5 (5/194=2.5%)
5 ccRCC 2 TKI alone 3 TKI + surgery 4/5 case : TKI discontinuation, 1/5 TKI continuation Median FU 24 mo, no relapse
Staehler M , Urol Oncol , Mar 2010
Retrospective study 36 (*12 + 24)
16 TKI alone 20 TKI+ local treatment 34/36 ccRCC Favorable pstic 39%, intermediate pstic: 61% 22 sunitinib; 11 sorafenib; 2 bevacizumab; 1 temsirolimus Median time to CR: 12mo Relapse: 24/36 ( 66,7%) TKI efficacy at re-introduction: PR or SD: 87% 12 Pt without relapse with 12mo median FU Median of drug – off period: 7m
Johannsen M, Ann Oncol 2011
Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
• Multicenter • Retrospective analysis • Patient developping CR
– With VEGFR-TKI alone – With VEGFR-TKI plus local treatment
• Double radiological review
Aim at:
- Description CR incidence, profil
- Description of management
- Identify predictive marquers

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
J Clin Onco 2012
CR with systemic therapy
TKI discontinuation (n=16 ; 44%)
CR with VEGFR TKI alone (n=36)
TKI continuation (n=8 ; 22%)
TKI discontinuation
after additional cycles (n=12; 33%)
Median duration of TKI after CR obtention= 3.9 months (range 1.06–32.5)
Relapse (n=7/16 ; 44%)
Relapse (n=4/12 ; 33%)
Relapse (n=1/8 ; 13%)

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
TKI discontinuation (n=16 ; 44%)
CR with VEGFR TKI alone (n=36)
TKI continuation (n=8 ; 22%)
TKI discontinuation after
additional cycles (n=12; 33%)
Media duration of TKI after CR obtention = 3.9 months (range 1.06–32.5)
Relapse (n=7/16 ; 44%)
Relapse (n=4/12 ; 33%)
Relapse (n=1/8 ; 13%)
J Clin Onco 2012
CR with systemic therapy Median time to CR: 12.6 mo
range [2-28]
12/36 relapsed (33%)
Median time from CR to relapse:
7.9 months [3-32]
17/28 pts (61%) with treatment
discontinuation had prolonged
with median FUp 8.5mo

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
BL
08/01/08

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
BL
08/01/08
06/06/08

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
BL
08/01/08
06/06/08
05/01/09
BL
08/01/08

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR with VEGFR TKI + local ttt
(n=28)
TKI discontinuation (n=19)
TKI continuation (n=3)
TKI discontinuation after additional cycles
(n=6) Median duration of TKI administration
after CR obtention = 3.5 months
(range 1.0–15.4)
Relapse (n=10/19 ; 52%)
Relapse (n=3/6 ; 50%)
Relapse (n=1/3 ; 33%)
J Clin Onco 2012
CR with multimodal approach

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR with VEGFR TKI + local ttt
(n=28)
TKI discontinuation (n=19)
TKI continuation (n=3)
TKI discontinuation after additional cycles
(n=6) Median duration of TKI
administration after CR obtention = 3.5 months
(range 1.0–15.4)
Relapse (n=10/19 ; 52%)
Relapse (n=3/6 ; 50%)
Relapse (n=1/3 ; 33%)
J Clin Onco 2012
CR with multimodal approach
Site of local treatment n=28 %
Lung LN Adrenal Pancreas Gastric/Colon Other (liver…)
13 4 5 2 2 3
46 14 18 7 7
11
Among the 22 surgical samples:
NO pathological CR was observed

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR with VEGFR TKI + local ttt
(n=28)
TKI discontinuation (n=19)
TKI continuation (n=3)
TKI discontinuation after additional cycles
(n=6) Median duration of TKI
administration after CR obtention = 3.5 months
(range 1.0–15.4)
Relapse (n=10/19 ; 52%)
Relapse (n=3/6 ; 50%)
Relapse (n=1/3 ; 33%)
J Clin Onco 2012
CR with multimodal approach Median time to CR: 18.5 mo
range [5-45]
14/28 relapsed (50%)
Median time from CR to relapse:
8.2 months [3-25]
12/25 pts (48%) with treatment
discontinuation had prolonged
with median FUp 10.7mo

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
• CR: Population
– Can be obtained in all prognosis group
– Can be obtained in various and multiple metastatic profil
– No predictive identified factors
• CR: feasibility of drug interruption
– Cons: – Any proof of delaying recurrence?
– Potential rebound?
– Pros: – Quality of life,
– prevention of drug resistance
– cost
– Efficacy of drug re-introduction at relapse
CR with TKI : Conclusion (1/2)
18 patient received subsequent VEGFR i
(14 same TKI, 4 alternative TKI):
• 10 PR
• 4 SD
• 1 PD
• 3UKN
J Clin Onco 2012

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR: Proposed management
• TKI alone CR: sustained 3 months of TKIs after CR then drug arrest
• Multimodal CR: no « adjuvant » TKI after local treatment
• Follow up:
– CT- scan every 3 months during first year
– and then every 6 months
CR with TKI : Conclusion (2/2)
J Clin Onco 2012

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR with TKI : Next step
ANALYSE PROSPECTIVE DES REMISSIONS COMPLETES OBSERVEES
SOUS SUNITINIB CHEZ DES PATIENTS ATTEINTS D’UN CANCER DU
REIN METASTATIQUE (mRCC)
• Prospective national study – Case - control design study
– multicentric
– Central Radiological review
– Tissue collection
– Blood sampling at time of CR and relapse
N = 120: 40 case, 80 control pts

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
CR : Coming soon… • Not obtained with combination of current VEFR/mTOR agents
• What about new agents alone or new combinations?
PD
1 inh
ibitio
n
Bra
hm
er
et
al., JC
O 2
01
0
No treatm Anti PD1 Sunitinib Sunitinib + Anti PD1
AS
CO
GU
20
13,D
r M
c D
erm
ott
,
Ed
uca
tion
al se
ssio
n

Eighth European International
Kidney Cancer Symposium Budapest – 03-04 May 2013
« It is ethical to believe in it!»
Dr Besse