commercial in confidence - uclh internet · this outline business case invites the board to support...
TRANSCRIPT

University College London Hospitals
Proton Beam Therapy
Outline Business Case
Volume 1 of 4
COMMERCIAL IN CONFIDENCE
Please note that this paper has been approved by the Department of Health and HM Treasury. Given the Trusts have commenced the procurement of the equipment and construction partners a redacted version is being prepared for publication. Those sections that include commercially sensitive assumptions will be redacted. This version is provided on the understanding that it will not be shared with any outside parties.
Version 5 31/05/2013

UCLH PBT Outline Business Case
Version 5 Page 1
ForewordThe UCLH vision is to provide top quality patient care, excellent education and world classresearch. This vision is supported by the Trust’s objectives to improve clinical outcomes,patient safety and the patient experience whilst maintaining financial sustainability andmaking more efficient use of our assets.
As agreed by the Board in late 2011, our strategic service priorities are to continue to build aworld class position in neurosciences and cancer whilst developing our position in women’shealth. We recognise that in order to achieve our objectives for our specialist services weneed to continue to develop a platform of excellence in surgery and medicine.
The proposal to develop one of the first Proton Beam Therapy centres in the UK at UCLH willdeliver ground breaking radiotherapy treatment alongside UCLH’s already leadingRadiotherapy practice. It will also strengthen the Trusts position as an internationally leadingcancer centre, as one of only around thirty centres in the world.
The Proton Beam Therapy development will provide quality patient care and improve thepatient experience through an enhanced 21st Century environment providing appropriateclinical adjacencies, streamlined patient pathways, and support development of new modelsof care and innovative technologies. Proton Beam Therapy will build upon the service modelchange that was core to the design of the Cancer Centre and will support the delivery ofsuccessful patient outcomes and the development of partnership working across UCLPartners and the wider health economy.
This Outline Business Case invites the Board to support the further development of the PBTvision at UCLH to Full Business Case stage.
UCLH PBT Outline Business Case
CONTENTS:
CHAPTER 1: INTRODUCTION ...............................................................................17
1.1 ........................................................................................17DOCUMENT PURPOSE1.2 .....................................................................17BACKGROUND & PROJECT SCOPE1.3 ............................................................................................18BOARD APPROVAL1.4 ...................................................................................18SYNOPSIS OF CHAPTERS
CHAPTER 2: THE STRATEGIC CASE ...................................................................19
2.1 ...................................................................................19PROTON BEAM THERAPY2.2
.....................................................................................................20THE ORGANISATION: UNIVERSITY COLLEGE LONDON HOSPITAL NHS
FOUNDATION TRUST2.3 ...........................................................20UCLH VISION, VALUES AND OBJECTIVES2.4 .....................................21UCLH STRATEGIC SERVICE DEVELOPMENT PRIORITIES2.5 ..........................................................................................23ESTATES STRATEGY2.6 .......................................................25THE CHRISTIE LOCAL STRATEGIC CONTEXT2.7 .......................................................................................25GOVERNMENT POLICY2.8 ...................................................26COMMISSIONER AND STAKEHOLDER SUPPORT2.9 ..................................................................................27INVESTMENT OBJECTIVES2.10 ...............................................30CURRENT PROVISION: INTERNATIONAL CONTEXT2.11 ........................................................31CURRENT PROVISION: NATIONAL CONTEXT2.12 ....................................32DEVELOPING THE U.K.’S FIRST NATIONAL PBT SERVICE2.13 ..............................................................................................34BUSINESS NEEDS2.14 ..................................................................................................37CLINICAL NEED2.15 .............................38POTENTIAL BUSINESS SCOPE & KEY SERVICE REQUIREMENTS2.16 ..................................................................................43MAIN BENEFITS CRITERIA2.17 .......................................................................................................47MAIN RISKS2.18 ....................................................................................................49CONSTRAINTS2.19 ..................................................................................................49DEPENDENCIES2.20 ..........................................................................................................49SUMMARY
CHAPTER 3: CHAPTER 3: ECONOMIC CASE......................................................50
3.1 ..................................................................................50ASSESSING THE OPTIONS3.2 ................................................................50CRITICAL SUCCESS FACTORS (CSFS)3.3 .....................................52THE LONG LIST OF OPTIONS CONSIDERED FOR PHASE 43.4 ....................................................................................54SHORT-LISTED OPTIONS3.5 ......................................................................................59SHORTLIST APPRAISAL3.6 ......................................................................................60ECONOMIC APPRAISAL3.7 ...................................................................69QUALITATIVE BENEFITS APPRAISAL3.8 ...............................................................................................75RISK APPRAISAL3.9 ....................................................................81OPTION APPRAISAL CONCLUSIONS3.10 .......................................................................................83SENSITIVITY ANALYSIS3.11 ...........................................................................................85SWITCHING VALUES3.12 ..........................................................................................87PREFERRED OPTION
CHAPTER 4: COMMERCIAL CASE .......................................................................89
4.1 ..................................................................................................89INTRODUCTION
Version 4 Page 2
UCLH PBT Outline Business Case
4.2 .........................................................................................89REQUIRED SERVICES4.3 ........................................................................89POTENTIAL FOR RISK TRANSFER4.4 .................................................................90PROPOSED CHARGING MECHANISMS4.5 ............................................................................91KEY CONTRACTUAL CLAUSES4.6 ................................................................................92PERSONNEL IMPLICATIONS4.7 .....................................................................92PROCUREMENT OPTION ANALYSIS4.8 ......................93PROPOSED PROCUREMENT STRATEGY FOR THE PBT EQUIPMENT4.9 ............103PROPOSED PROCUREMENT STRATEGY FOR THE BUILD PROCUREMENT
CHAPTER 5: FINANCIAL CASE...........................................................................105
5.1 ................................................................................................105INTRODUCTION5.2 ............................................................................................106IMPACT ON UCLH5.3 ......108IMPACT ON THE INCOME AND EXPENDITURE ACCOUNT AND BALANCE SHEET5.4 ................................................................................111OVERALL AFFORDABILITY5.5 .......................................................................113IMPACT ON CLINICAL SERVICES5.6 ...............................................................................................114CAPITAL COSTS5.7 ...................................................................................................117CASH SPEND5.8 ............................................................................................118REVENUE IMPACT5.9 ..........................................................................................119SOURCE OF FUNDS5.10 .........................................121NET PRESENT COST & EQUIVALENT ANNUAL COST5.11 ................................................................................122IMPACT ON I&E ACCOUNT5.12 ............................................................................125IMPACT ON BALANCE SHEET5.13 ..................................................................................126IMPACT ON RISK RATIOS5.14 ...............................................................................127ACCOUNTING TREATMENT5.15 ................................................................................128OVERALL AFFORDABILITY
CHAPTER 6: MANAGEMENT CASE....................................................................129
6.1 ............................................................129NATIONAL PROGRAMME MANAGEMENT6.2 ......................................................130UCLH AND THE CHRISTIE JOINT WORKING6.3 .................................................................131UCLH PROGRAMME MANAGEMENT6.4 .............................................................133PROGRAMME REPORTING STRUCTURE6.5 ............................................................................143PBT PROJECT RESOURCING6.6 ................................................................................................146PROJECT PLAN6.7 ..........................................................................147STAKEHOLDER ENGAGEMENT6.8 .............................................................................148USE OF SPECIAL ADVISORS6.9 ...........149OUTLINE ARRANGEMENTS FOR CHANGE AND CONTRACT MANAGEMENT6.10 ...................................150OUTLINE ARRANGEMENTS FOR BENEFITS REALISATION6.11 ...............................150OVERALL APPROACH TO RISK ANALYSIS & MANAGEMENT6.12 ............................154OUTLINE ARRANGEMENTS FOR POST PROJECT EVALUATION6.13 .....................................................154APPROVALS PROCESS AND DH GATEWAYS6.14 .......................................................................156CONTINGENCY ARRANGEMENTS6.15 ........................................................................................................156SUMMARY
CHAPTER 7: CONCLUSION & RECOMMENDATIONS.......................................157
7.1 ........................................................................................157RECOMMENDATIONS
Version 4 Page 3

UCLH PBT Outline Business Case
List of Figures:Figure 1 UCLH Values, Behaviours and Standards................................................................... 21Figure 2 UCLH Trust Vision, Values and Objectives................................................................. 22Figure 3 Odeon & Rosenheim Site........................................................................................... 25Figure 4 Different Types of Procurement Routes.................................................................. 101Figure 5 National PBT Programme Management Arrangements.......................................... 130Figure 6 Phase 4 Programme Organogram ........................................................................... 132Figure 7 Phase 4 Clinical Projects and Functional Workstreams........................................... 133Figure 8 PBT Project Structure .............................................................................................. 139
List of Tables:Table 1 Contribution of PBT to the Delivery of UCLH Service Priorities.................................. 23Table 2 PBT UK Government Policy......................................................................................... 26Table 3 PBT Project Investment Objectives and Associated Benefits Criteria ........................ 27Table 4 High energy PBT Facilities in Operation (July 2012) ................................................... 30Table 5 Key Service Requirements and Business Scope.......................................................... 40Table 6 Facilities to Deliver Scope and Key Service Requirements ......................................... 42Table 7 Investment Objectives and Benefits Criteria .............................................................. 44Table 8 Main Risks and Counter Measures ............................................................................. 47Table 9 PBT Critical Success Factors ........................................................................................ 50Table 10 PBT Long List Options ............................................................................................... 53Table 11 Short Listed Options for PBT Facility ........................................................................ 54Table 12 Implementation Opening Dates ............................................................................. 58Table 13 Main Benefits............................................................................................................ 61Table 14 Indicative NPV for PBT Options ................................................................................ 65Table 15A PBT Options Appraisal ............................................................................................ 66Table 16 Summary of Results .................................................................................................. 68Table 17 Summary of Results .................................................................................................. 69Table 18 Qualitative Benefits Criteria ..................................................................................... 70Table 19 Benefits Appraisal Results......................................................................................... 74Table 20 Risk Scoring Methodology ........................................................................................ 75Table 21 Summary of Risk Assessment by Option .................................................................. 76Table 22 Risk Transfer Matrix.................................................................................................. 86Table 23 Risk Transfer Matrix.................................................................................................. 89Table 24 Analysis of Build Procurement................................................................................ 102Table 25 UCLH Income and Expenditure Analysis ................................................................. 106Table 26 UCLH Balance Sheet Extracts .................................................................................. 107Table 27 Income and Expenditure Impact of PBT ................................................................. 109Table 28 Trust Reimbursements............................................................................................ 112Table 29 PBT Initial Capital Costs .......................................................................................... 114Table 30 Summary of Contingency and Optimism Bias ........................................................ 115Table 31 Phasing of Capital Spend ........................................................................................ 116Table 32 PBT Cashflow .......................................................................................................... 117Table 33 Estimate of Non Recurring Funding During Construction ...................................... 118
Version 4 Page 4

UCLH PBT Outline Business Case
Table 34 Estimated PBT Financing Requirements ................................................................. 119Table 35 Net Present Value of PBT........................................................................................ 122Table 36 Income and Expenditure for PBT ............................................................................ 123Table 37 PBT Balance Sheet .................................................................................................. 125Table 38 Accounting Treatment ............................................................................................ 127Table 39 Terms of Reference for the Phase 4 Programme Board......................................... 134Table 40 Clinical Workstream Responsibilities...................................................................... 140Table 41 Operations Workstream Responsibilities ............................................................... 141Table 42 Technical Workstream Responsibilities .................................................................. 141Table 43 Strategic Workstream Responsibilities ................................................................... 142Table 44 Capital Investment Workstream Responsibilities................................................... 142Table 45 Finance Workstream Responsibilities..................................................................... 143Table 46 Research Workstream Responsibilities .................................................................. 143Table 47 Stakeholder Engagement Responsibilities Matrix .................................................. 147Table 48 Specialist Advisors .................................................................................................. 148Table 49 Change Management Process ................................................................................ 149Table 50 Risk Impact Assessment Summary ......................................................................... 152Table 51 Key Strategic and Operational PBT Delivery Risks .................................................. 153Table 52 Scope and Timing of Approval Stages..................................................................... 155Table 53 Board Approvals and Associated Timeline for PBT................................................. 157Table 54 Abbreviations.......................................................................................................... 158
Volume 2 AppendicesAPPENDIX 1A CIB AND MONITOR CHECKLIST
APPENDIX 2A: OVERVIEW OF PROTON BEAM THERAPY
APPENDIX 2B: UCLH SERVICE STRATEGY
APPENDIX 2C: EQUALITY IMPACT ASSESSMENT
APPENDIX 2D PROJECT RISK REGISTER
APPENDIX 3A: UCLH AND THE CHRISTIE PBT THROUGHPUT MODELLING
APPENDIX 3B: PBT QUALITATIVE BENEFITS ANALYSIS
APPENDIX 3C: ECONOMIC ASSESSMENT WITH QALY ANALYSIS
APPENDIX 3D: BENEFITS REGISTER
APPENDIX 3E: FINANCIAL APPRAISAL
APPENDIX 4A PROPOSED TARIFF ARRANGEMENTS
APPENDIX 4B: EQUIPMENT PROCUREMENT STRATEGY
APPENDIX 4C: CONSTRUCTION PROCUREMENT STRATEGY
APPENDIX 4D: CABINET OFFICE ICT SPEND CONTROL FORM (V2.18)
Version 4 Page 5

UCLH PBT Outline Business Case
APPENDIX 6A: PROJECT RESOURCING SCHEDULE
APPENDIX 6B: STAKEHOLDER MANAGEMENT PLAN
APPENDIX 6C: LETTERS OF COMMISSIONER AND STAKEHOLDER SUPPORT
APPENDIX 6D: CONTINGENCY IN THE EVENT OF ACCELERATOR / PBT CENTRE FAILURE
APPENDIX 6E: RISK POTENTIAL ASSESSMENT
Volume 3 Design Details
Volume 4 Strategic Investment Framework
Version 4 Page 6
UCLH PBT Outline Business Case
Executive Summary
1. IntroductionThe purpose of this Outline Business Case (OBC) is to explain the need for and to justify thecapital investment of £135 million by the Department of Health (DH) for University CollegeLondon Hospital (UCLH) NHS Foundation Trust to develop the Proton Beam Therapy (PBT)Centre, as part of the DH national programme, to service the population of England and theDevolved Nations.
High energy PBT is a precise form of radiotherapy which is currently unavailable in theUnited Kingdom (UK). Compared to conventional radiotherapy, PBT can treat the patient bydelivering a dose which is targeted more precisely at the tumour with less irradiation ofnormal tissue, thus reducing the side effects of therapy. It has particular advantages forpaediatrics and for tumours located near a patient’s brain, eyes, inner ears or spinal cord
This PBT OBC forms part of the UCLH overall Phase 4 Programme and this Phase 4 OBC waspresented to the UCLH Board of Directors and approved on the 13th September 2012.
This PBT OBC was submitted to the UCLH Board of Directors on the 13th February 2013. Aspart of the DH’s national programme, this business case, in conjunction with The Christie,will be submitted to the DH and subsequently Her Majesty’s Treasury (HM Treasury) forapproval.
2. Strategic caseThis section sets out the strategic context and the case for change, together with thesupporting investment objectives, the scope of service for the new facility and the keyconstraints and critical success factors.
The case for change
As of July 2012, there are 27 high energy PBT facilities operational around the world. Manyare also stand alone treatment delivery facilities and not integrated with other clinicalfacilities
The National Health Service (NHS), National Specialised Commissions Team (NSCT) supportsthe PBT Overseas Programme for UK patients and overall 394 patients have been referred tothe programme since it started in 2008.
Costs for overseas treatment vary greatly from £42,000 per patient in Switzerland to over£100,000 at the commercially run centres in the USA. In addition, the NSCT have alsorecognised that European centres are under increasing pressure to prioritise treatment oftheir own nationalities. Patients are often without their full family support network for anextended period. Funding is not provided for the whole family so typically families are splitplacing greater pressure on individuals at a time of significant personal stress.
In August 2009, the NSCT was asked to hold a competition to identify possible providers ofhigh energy PBT services in England. Proposals were received from eight interested Trusts inMarch 2010. In September 2010, the DH announced that The Christie and UCLH wereselected as potential sites.
Version 4 Page 8

UCLH PBT Outline Business Case
The Business NeedThe DH have specified a world class service in the UK, delivering treatment to a significantlymore complex casemix than typically experienced in PBT centres across the world. The DHhas identified the need for at least two centres to treat the anticipated patient demand.
UCLH and The Christie have recognised the commercial advantages of developing a singleservice rather than two competing centres. The project teams have identified that providingone service which refers patients appropriately and equally between the centres limits therisk associated by any one Trust.
3. Economic case
The long list
The long list of options explored within the economic case are listed below;
Option 1 A 3 PBT Gantry’s plus 1 Accelerator
Option 1 B 3 PBT Gantries plus 1 Accelerator
Option 1 C 3 PBT Gantries plus 1 Accelerator
Option 2 A 4 PBT Gantries plus 1 Accelerator
Option 2 B 4 PBT Gantries plus 1 Accelerator
Option 2 C 4 PBT Gantries plus 1 Accelerator
Option 3A 3 PBT Gantries plus 1 Accelerator plus an adjacent concrete boxwhich could be converted into additional rooms and/or Accelerator capacity at alater date
Option 3 B 3 PBT Gantries plus 1 Accelerator plus an adjacent concrete boxwhich could be converted into additional rooms and/or Accelerator capacity at alater date
Option 3 C 3 PBT Gantries plus 1 Accelerator plus an adjacent concrete boxwhich could be converted into additional rooms and/or Accelerator capacity at alater date
The short list
The following short list of options emerged:
Option 1 – status quo, do nothing or do minimum
Option 2 – Construct a PBT facility on the UCLH campus comprising of 3Compact Gantries and one Accelerator.
Option 3 – Construct a PBT facility on the UCLH campus comprising of 4Compact Gantries and one Accelerator.
Option 4 – Construct a PBT facility on the UCLH campus comprising 3 CompactGantries and one Accelerator plus an additional unequipped room to allow forfuture flexibility.
Version 4 Page 9


UCLH PBT Outline Business Case
4. Commercial case
Proposed Charging MechanismsThe Trust has agreed the following contractual structure for the delivery of PBT services;
The contract for services will be between the Commissioning Board and eachFoundation Trust. The contract will broadly be based on the standard nationalcontract and will define the service specification, activity, payment mechanism,and consequences of termination. To the extent possible, other schedules willbe standard schedules.
The duration of the contract is likely to be 10 years including the developmentphase from FBC and an initial “open book” reimbursement period with anadditional period of 10 years where an episode based tariff is used.
The same contract will commence from the opening of the facility and will onlycover the period of service delivery.
A separate Development Contract will cover the period from Full Business Caseapproval to the opening of the facility.
Procurement strategyThere are a number of procurement routes available to UCLH. The principal considerationsassociated with each of these alternatives procurement routes are;
Value for Money to the organisation
In line with the organisational strategic objectives and the investment objectives
The project timeline is to deliver an operational building, with projectedtreatment date for the first patient by Q4 – 2018.
Level of risk which can be accepted or transferred adequately
Outturn cost certainty
Flexibility in terms of control of design interface by client & contractor designapprovals necessary
Change which can be accommodated within the project or resulting contract
Level of technical competence within the market to deliver the project
Meeting OJEU thresholds and regulatory requirements
The intended procurement strategy has taken into consideration a review of the followingscenarios;
Joint equipment and build contracts or as separate procurement work streams
Build procurement in isolation
Equipment procurement in isolation
The recommendation is to separate the equipment and construction elements of the build.It is believed that additional risk of the equipment firm managing the design andconstruction will add significant cost, reduce time predictability and also affect technicaldelivery and quality of product.
Version 4 Page 11


UCLH PBT Outline Business Case
gap of some of total capital expenditure. There is an expectation that this smallfunding gap will be closed once the procurement moves to a more competitive process.
AffordabilityThe Trust has a robust financial platform from which to undertake this PBT development.Notwithstanding this, the Trust’s existing I&E is not strong enough to mitigate substantialPBT risk. The DH has recognised that in this regard the Trust has less potential to pool riskand so the majority of risk will be borne at Department level.
The Trust and DH have clearly defined the funding streams for both capital and revenuealong with the broad allocation of risk within the SIF. In doing so the Trust can demonstratethat the scheme is affordable and deliverable.
6. Management case
Project management arrangementsThe National Programme Management arrangements are detailed in the DH SIF andsummarised in the Figure below, with representatives from UCLH sitting on the JointProgramme Board as required.
Version 4 Page 13

UCLH PBT Outline Business Case
UCLH and the Christie will continue their close working relationships at both the workstreamand executive levels to ensure the development of the service is coordinated nationally.Operational and strategic items in need of wider discussion will be brought to the existingJoint Working Group currently held on a bi monthly basis.
In order to support clinical ownership and engagement in the whole life of the programme,the reporting structure is divided into three clinical projects and four functional workstreamsas shown in the below diagram.
Version 4 Page 14

UCLH PBT Outline Business Case
Risk ManagementRisk management is an essential part of the development of any project. Risk should bemanaged proactively through a process of identification, assessment and mitigation. TheRisk Management Strategy will incorporate the following activities:
Risk identification and reporting
Evaluation of proximity, probability and impact of the risk occurring
Allocation of risk owner
Development of risk responses including prevention, reduction, transference,acceptance of reduction
Identification of escalation procedures
Planning and resourcing of responses to risks
Monitoring and reporting of risk status
The identification and assessment of risks at the OBC stage was conducted at a riskworkshop. The mitigation of the identified risks at the OBC stage was conducted at a riskworkshop on the 17th August 2012.
Post project evaluation arrangementsProject evaluation reports are learning tools that ensure UCLH and other stakeholders applythe knowledge gained from the Phase 4 Programme to future projects. UCLH are committedto ensuring PERs are undertaken in order to assess how the Programme has met itsobjectives and realised the project benefits. At the following key evaluation stages:
Stage 1 Project Procurement: OBC to Financial Close
Stage 2 Implementation: Financial Close to Practical Completion
Stage 3 Initial: Operational Commissioning to first 6 months of operation
Stage 4 Follow Up: 6 months to first 2 years of operational phase
Evaluation reports will be completed within six months of the data collection for each stageoutlined above and will be disseminated to stakeholders following approval by the Phase 4Programme Board.
Version 4 Page 15

UCLH PBT Outline Business Case
The Phase 4 Project Working Group will manage the PER process on behalf of the Phase 4Programme Board, supported by an independent review body.
7. RecommendationThis Business Case seeks approval for the following:
The selection of the Preferred Option.
Commitment of resources for the next stage of the project.
Approval to proceed to the next stage of the project.
Version 4 Page 16

UCLH PBT Outline Business Case
Chapter 1: Introduction
Why the chapter matters
This chapter sets the scene for the reader by providing an overview of University CollegeLondon Hospitals and the Proton Beam Therapy Project.
What the chapter says
This Chapter establishes the structure of the business case identifying what each Chapterwill include. It provides a brief background to University College London Hospitals NHSFoundation Trust and to the scope of the Proton Beam Therapy Project.
1.1 Document Purpose
1.1.1 The purpose of this Outline Business Case (OBC) is to explain the need for and tojustify the capital investment of £135 million for University College London Hospital(UCLH) NHS Foundation Trust to develop the Proton Beam Therapy (PBT) Centre, aspart of the Department of Health’s (DH) national programme, to service thepopulation of England and the Devolved Nations.
1.2 Background & Project Scope
1.2.1 This PBT OBC describes the viability of the proposed London PBT Centre to belocated at the UCLH site. It would be one of two centres that will provide acoordinated national PBT service, the other to be located at The Christie NHSFoundation Trust (The Christie) site in Manchester.
1.2.2 High energy PBT is a precise form of radiotherapy which is currently unavailable inthe United Kingdom (UK). Compared to conventional radiotherapy, PBT can treat thepatient by delivering a dose which is targeted more precisely at the tumour with lessirradiation of normal tissue, thus reducing the side effects of therapy. It hasparticular advantages for paediatrics and for tumours located near a patient’s brain,eyes, inner ears or spinal cord.
1.2.3 PBT equipment is highly unusual relative to other equipment used in the NHS in thatit has a life span of over 20 years and each machine is highly expensive. Investmentin PBT facilities is too costly and risky even for the largest and best run NHSproviders to undertake alone, from approximately for the equipment and
for the building. As a result, the DH has announced plans for theavailability of public finance to fund the development of PBT in the UK.
1.2.4 This OBC provides the basis for the development, delivery and operation of the PBTCentre at UCLH. This project reflects the culture of UCLH with significant clinical andmanagerial input into clinical pathways, staffing models, the financial case anddesigns.
Version 4 Page 17

UCLH PBT Outline Business Case
1.3 Board Approval
1.3.1 This PBT OBC forms part of the UCLH overall Phase 4 Programme and this Phase 4OBC was presented to the UCLH Board of Directors and approved on the 13th
September 2012.
1.3.2 The Trust Board requested that the PBT component of the Phase 4 OBC be discussedfurther following completion of the Service and Investment DevelopmentFramework (SIF) discussion with the DH.
1.3.3 The PBT OBC is presented as the first stage in the approval process for the UCLH PBTcentre and was submitted to the UCLH Board of Directors on the 13th February 2013.
1.3.4 As part of the DH’s national programme, this business case, in conjunction with TheChristie, will be submitted to the DH and subsequently Her Majesty’s Treasury (HMTreasury) for approval.
1.4 Synopsis of Chapters
1.4.1 This OBC is structured on the Five Case Business Case Model with additionalelements to meet the governance requirements of the UCLH Board of Directors, theDH, HM Treasury and Monitor.
1.4.2 The completed CIB and Monitor Business Case Checklist is available at Appendix 1A
1.4.3 This OBC has been produced by UCLH in accordance with all relevant DH, HMTreasury and Buying Solutions Guidelines, including the Capital Investment Manual.It consists of the following;
the strategic case this sets out the strategic context and the case forchange, together with the supporting investment objectives, the scope ofservice for the new facility and the key constraints and critical successfactors.
the economic case this demonstrates that the organisation has selectedthe choice for investment which best meets the existing and future needs ofthe service, taking account of benefits, costs and risks. In addition, thisChapter identifies the proposed preferred options for the delivery of PBT atUCLH.
the commercial case this outlines the proposed commercial terms of theproject, highlights the procurement strategy for the scheme and identifiesany workforce/employment issues.
the financial case this confirms funding arrangements and affordability andexplains any impact on the balance sheet of the Trust.
the management case this demonstrates that the scheme is achievableand explains the Trust’s approach to project management, riskmanagement, benefits realisation and communication.
1.4.4 Further information on this project is available fromUCLH NHS Foundation Trust.
Version 4 Page 18

UCLH PBT Outline Business Case
Chapter 2: The Strategic Case
Why the chapter matters
This Chapter describes UCLH and the relationship between the PBT project and theorganisational key strategic business drivers.
What the chapter says
This Chapter establishes the case for change and the need for investment in the projectincluding:
Demonstrating business fit and synergy with other parts of the Organisation.
The proposed investment objectives identify what we are seeking to achieve.
The proposed scope of the project and service requirements.
Main project benefits criteria
Part A: The Strategic Context
2.1 Proton Beam Therapy
2.1.1 High energy PBT is a precise form of radiotherapy which is currently unavailable inthe UK. Like all forms of radiotherapy, PBT works by irradiating target tumours,damaging the Deoxyribonucleic Acid (DNA) of the cancerous cells and interferingwith their ability to reproduce.
2.1.2 The chief advantage of PBT over other types of external beam radiotherapy is theability to more precisely target the tumour. The targeted area can be varied bychanging the energy and position of the proton beam. As the proton beam deliversno dose beyond this sharp peak, the radiation is focussed more precisely allowing aneffective dose to be delivered to the tumour. This spares the surrounding healthytissue and reducing the likelihood of longer term side effects.
2.1.3 PBT is advantageous for treating tumours in locations where conventional X rayradiotherapy (photons) would damage surrounding healthy tissue to anunacceptable level. This is particularly beneficial for patients whose cancers areclose to the spinal cord and critical structures within the brain, eye or inner ear. Thegreatest potential benefit of PBT is for children, teenagers and young adults, as thelong term side effects of radiotherapy to younger people are of great concern. Lessdamage to surrounding tissue leads to a reduction in late effects such as theinduction of secondary cancers, reduced effects on growth of bones and soft tissues,reduction in hormone deficiencies and reduced neuropsychological sequelae.
2.1.4 PBT techniques have been used for the treatment of some cancers since the 1950s.The technology is still advancing, with a number of research groups developing newways of delivering protons more effectively and economically.
2.1.5 PBT costs remains around four times more expensive than traditional radiotherapywhich is mainly due to the capital costs. It is difficult to obtain accurate and up todate equipment costs as most procurement processes are typically undertaken
Version 4 Page 19

UCLH PBT Outline Business Case
Version 4 Page 20
under non disclosure agreements. The DH Strategic Outline Case (SOC)1 along withthe Value for Money Addendum2 provides a wide anticipated cost range with theequipment investment to be in the region of . The building is expected tocost between .
2.1.6 An overview of Proton Beam Therapy Technology is available within Appendix 2A
2.2 The Organisation: University College London Hospital NHSFoundation Trust
2.2.1 UCLH, located in the heart of London, is one of the largest teaching hospitals in theUK and provides first class acute and specialist services in eight hospitals acrosscentral London. UCLH was one of the first wave Foundation Trusts and in 2011 wasawarded the top hospital in London for the second time in three years by Dr Foster.
2.2.2 UCLH together with University College London (UCL), Moorfields Eye Hospital, TheRoyal Free Hospital, Barts Health NHS Trust, Queen Mary University of London,Oxford Research Facility and Great Ormond Street Hospital is part of Europe’slargest and strongest Academic Health Science Network – UCL Partners. It includesthe UK’s Number 1 NHS Trust, the world’s fourth best university, and the largest UKcentres for paediatric cancers, brain cancers and sarcomas. UCL Partners are able tobring their collective expertise to this bespoke clinical venture.
2.3 UCLH Vision, Values and Objectives
2.3.1 The UCLH Vision states: we are committed to delivering top quality patient care,excellent education and world call research. Underpinning this corporate vision isour commitment to continue to provide both a service to our local populationalongside specialist services for the population of London and beyond. UCLH deliversour vision through the Trust Values and Annual Objectives.
UCLH Values
2.3.2 The UCLH Values set out how UCLH serve our patients and their families and howUCLH work with colleagues in the Trust and beyond.
1 Available at https://www.wp.dh.gov.uk/publications/files/2012/10/national-proton-beam-therapy-service-development-programme-strategic-outline-case-16102012.pdf
2 Available at https://www.wp.dh.gov.uk/publications/files/2012/10/national-proton-beam-therapy-service-development-programme-value-for-money-addendum.pdf

UCLH PBT Outline Business Case
Figure 1 UCLH Values, Behaviours and Standards
UCLH Top Ten Objectives for 2012/13
2.3.3 UCLH have identified the Top Ten Objectives for 2012/13. They focus on three areasincluding:
Delivering quality for our patients – ensuring that our patients received thebest clinical outcomes, are safe and have the highest quality patientexperience.
Differentiating our patient services – Delivering integration in line withresearch & development, education and innovation.
Fundamentals – Ensuring business sustainability through our financialmanagement, delivering against statutory and mandatory requirements andthe development of staff.
2.4 UCLH Strategic Service Development Priorities
2.4.1 Sitting underneath our vision, our Trust Objectives and our strategic servicedevelopment priorities, the Board agreed a service strategy for UCLH in 2007/8based upon four key research specialities: neurosciences, cancer, cardiac andwomen’s health and three service areas; dental, paediatrics and acute services, asshown in Appendix 2B. In November 2011, the Board reviewed the service strategyand agreed to focus on development of three service areas in 2012/13 where theTrust was or could become world class:
Neurosciences: priorities include securing further neuro oncology andneurosurgery activity (starting with the Royal Free Hospital), ensuringacademic and clinical priorities are aligned where possible, building on thesuccessful Wolfson bid to develop experimental neurology and increaserecruitment to clinical trials, and developing plans for new capacityincluding working up a Queens Square “at” delivery model.
Cancer: priorities include successful commissioning of the new CancerCentre, delivering a step change in patient experience, supporting thedevelopment of specialist services at UCLH as part of the London Cancer
Version 4 Page 21

UCLH PBT Outline Business Case
partnership (initial priorities include: radiotherapy, diagnostics and surgery)and supporting the expansion of academic cancer to compete nationally
Women’s Health: priorities include developing plans for expansion ofmaternity in line with women’s choice, to further develop UCLH’s role as anetwork, local and national provider of complex care for women andneonates, and in addition supporting the cancer agenda in gynaecologicalcancers and breast cancer surgery.
2.4.2 The Service Strategy recognises that the successful development of specialistservices requires a platform of excellence in surgery, emergency medicine and acutepaediatrics. This means investing in development of surgery particularly in areaswhich support our objectives and ensuring that new commissioner standards foracute service quality and safety are met.
2.4.3 Figure 2 demonstrates the UCLH Vision, underpinned by the UCLH Values, TrustObjectives and Service Development Priorities supported by a platform of Surgery,A&E and Medicine.
Figure 2 UCLH Trust Vision, Values and Objectives
Version 4 Page 22


UCLH PBT Outline Business Case
2.5.3 The maximum area suitable for development on the site is more than sqm.UCLH aims to maximise the development potential of the whole site by developingadditional clinical facilities on the top of the PBT Centre in order to take advantageof the economies of scale of construction, but also due to the scarcity of availabledevelopment space in central London. UCLH plan to maximise this opportunity bybuilding an ambulatory care facility above the PBT Centre. The adjoining facilities willimprove the coordination of services, enhance patient experience and releaseeconomies of scale through integrated and streamlined clinical and operationalpathways.
2.5.4 When preparing the PBT OBC the Trust was mindful that above ground and PBTcapital costs should not be cross subsidised. A full detailed elemental cost plan wasprepared for the OBC which identified the full project costs which were brokendown between above ground and PBT cost centres. Where costs could not beallocated between cost centres then they were apportioned across the two projectsby either GIFA or other known quantities. In order to maximise the build capacity,the Trust took the opportunity to realise an additional floor by “pushing” PBT downto level 4. The incremental cost of moving PBT down a level was allocated in full tothe above ground proposal
2.5.5 The centrality of PBT to our core work is reflected in the site we have dedicated todeveloping it on. Sitting at the centre of the UCH campus, we have designed a PBTfacility which has a unique set of clinical adjacencies that no other UK provider couldoffer. Every single necessary clinical adjacency exists, but more than this, theseclinical adjacencies are proven – already performing successfully for patients on adaily basis. These links include one of the newest and most advanced radiotherapydepartments in the country, a world class paediatric service, and the UCH MacmillanCancer Centre which will offer a model of patient focused care unparalleled in theUK. New clinical and basic science research facilities (including the UCL CancerInstitute), together costing almost £100m, are also directly adjacent – ensuring theresearch opportunities inherent within PBT are fully realised.
2.5.6 As well as a proven set of clinical links, the site is also located at the centre ofnational and international transport links. Proximity to five underground lines andmajor rail stations (Euston, St Pancras International and King’s Cross) allow readyaccess by public transport for the entire country, including those patients who wishto fly (Gatwick is accessed via Victoria and Heathrow via Paddington – both stationsbeing just a short underground journey from UCLH). The development of a UK highspeed rail network centred on Euston will further enhance this accessibility, as willthe completion of a Crossrail station at Tottenham Court Road.
Version 4 Page 24







UCLH PBT Outline Business Case
Version 4 Page 31
Spending Review period. Estimated spend on overseas PBT treatment by 2014/15 is£30m per annum.
2.11 Current Provision: National Context
Current Practice
2.11.1 The only PBT facility in the UK is a low energy facility at The Clatterbridge CancerCentre NHS Foundation Trust (CCCFT), Centre for Oncology; suitable for eye tumoursonly. It treats around 100 patients a year with excellent outcomes and over 90%permanent control (effective local cure and saves enucleating the eye)
2.11.2 There are no current providers of high energy PBT in the UK. As previouslymentioned, the NSCT has commissioned PBT interventions for a limited number ofUK patients in Switzerland, France and the USA, focusing on paediatric patients andtwo types of adult cancer in particular: chondrosarcomas and chordomas affectingthe base of the skull and the upper part of the spine respectively. In other countries,most notably the USA, many patients with prostate cancer have been treated withPBT. After a review of the existing outcomes evidence base for these less complexindications, they were not included on the DH’s list of indications consideredappropriate for overseas treatment. It is currently expected that these indicationswould not be treated within a UK NHS PBT service.
2.11.3 Costs for overseas treatment vary greatly from £42,000 per patient in Switzerland toover £100,000 at the commercially run centres in the USA. In 2011/12 the averagecost is nearer £90,000 per patient as the majority of patients are treated inJacksonville, Florida. Less expensive European centres have not been used asfrequently due to difficulties integrating supporting treatments and the quality ofthe patient experience (including language issues). In addition, the NSCT have alsorecognised that European centres are under increasing pressure to prioritisetreatment of their own nationalities.
2.11.4 Planning and delivery of treatment takes between eight and twelve weeks sopatients are often without their full family support network for an extended period.Funding is not provided for the whole family so typically families are split, placinggreater pressure on individuals at a time of significant personal stress. An extendedvisit abroad disrupts family life and often affects household income. Many patientsthat would benefit from PBT are unable to take advantage of the service eitherbecause of practical reasons such as a lack of family support to travel.
2.11.5 Patients that would benefit from PBT, but are unable access the overseas treatmentreceive alternative local treatments, all characterised with inferior clinical outcomes:
In the majority (90%) of cases, these patients will be treated with advancedconventional radiotherapy solutions such as Intensity Modulated RadiationTherapy (IMRT).
For approximately 7% of cases, current conventional treatment is withsurgery alone.

UCLH PBT Outline Business Case
Version 4 Page 32
For approximately 3% of cases, no alternative to PBT can be offered eitherdue to the young age of the patient, or the risk of serious toxicity withconventional radiotherapy.
Existing UK Capacity
2.11.6 Although there are currently no providers of high energy PBT services in the UK, aspreviously mentioned cancers of the eyes have been treated with low energy protontherapy at CCCFT since 1992.
It is technically challenging, but feasible totreat eye patients in a high energy PBT centre with some modifications, but the DH’sService and Investment Framework (SIF), as shown in Volume 3, explicitly notes thatthe high energy PBT centres will not be expected to deliver or be commissioned forlow energy eye treatments.
2.11.7 A planning application has been lodged with the relevant authorities in London todevelop a commercially run high energy PBT centre in Moorgate, London. At thisstage the level of maturity and sophistication of this plan is unknown.
2.11.8 Discussions with the private healthcare market in the UK ( ) haveestablished that there is little appetite for capital investment in a PBT facility orwillingness on the part of private healthcare insurers to pay for treatment. Privatepatients in the UK would therefore be self funders.
Tender Process
2.11.9 In August 2009, the NSCT was asked to hold a competition to identify possibleproviders of high energy PBT services in England. Proposals were received from eightinterested Trusts in March 2010.
2.11.10 In September 2010, the DH announced that The Christie and UCLH were selected aspotential sites, subject to the HM Treasury approving a Proton Strategic OutlineBusiness Case (SOC). University Hospitals Birmingham NHS Foundation Trust (UHB)was informed that the case for three centres would be explored within the businesscase and if proved, UHB would host a third centre.
2.11.11 The DH SOC concludes that on the basis of affordability, two centres will provide adegree of resilience and provide sufficient capacity to treat the patients fromEngland and the devolved administrations.
2.12 Developing the U.K.’s first National PBT service
UCLH PBT Centre
2.12.1 The DH proposed National PBT Service will focus on a case mix of Head & Neck andBrain cancers and Sarcomas as well as Paediatric patients. Although not part of thePBT service, the DH have set out in the PBT Strategic Investment Framework theparallel developments in the configuration of specialist surgery services and referralpathways for these rare cancers to ensure optimum outcomes. These includepaediatric surgery, paediatric neurosurgery, adult ENT surgery, Maxillofacial andskull base surgery and neurosurgery and spinal surgery

UCLH PBT Outline Business Case
Version 4 Page 33
PBT will build on UCLH’s current Radiotherapy practice and enhance UCLH’scancer services. With the focus of the DH PBT casemix, and the paralleldevelopments in surgery, there will also be an important clinical fit withUCLH’s Head & Neck and Neuroscience services
2.12.2 UCL Partners (UCLP) is one of five accredited academic health science systems in theUK. Its purpose is to translate cutting edge research and innovation into measurablehealth gain for patients and populations – in London, across the UK, and globally.UCLP is organised around 11 clinical programmes with one of the focus areasCancer. The aim of the UCLP Cancer Programme is to improve quality of care,patient experience and outcomes – by focusing on the delivery of integrated carepathways across organisational boundaries, and by embedding access to researchand innovation at every step of the patient journey. This system wide approach isurgently needed to address the historically poorer survival rates and patientexperience documented for cancer patients treated in London compared to the restof the UK. This vision is being delivered through three main projects:
Development of the first integrated cancer system in the UK – LondonCancer
Expanding the early phase clinical trials portfolio across all age groups,including paediatrics
Provision of the UK’s first proton beam therapy service
The National PBT Service
2.12.3 The DH have specified a world class service in the UK, delivering treatment to asignificantly more complex casemix than typically experienced in PBT centres acrossthe world. The DH has identified the need for at least two centres to treat theanticipated patient demand.
2.12.4 UCLH and The Christie have recognised the commercial advantages of developing asingle service rather than two competing centres. The project teams have identifiedthat providing one service which refers patients appropriately and equally betweenthe centres limits the risk associated by any one Trust.
2.12.5 There are additional benefits of sharing platforms and developing a commonapproach to delivery that will save costs, ensure best practice and ultimatelyimprove clinical outcomes and increase the patient experience. Some of the benefitsthat a coordinated service could deliver include:
Provision of a backup if one centre suffers from a catastrophic failure
Development of National Standards, operating a standardised service
Coordinated approach to commissioning of indications to increase thenumber of patients that could be treated during ramp up
Unified clinical evaluation of PBT
Coordinate academic health science and research activities
UCLH PBT Outline Business Case
Version 4 Page 34
Joint procurement of the PBT system and treatment planning system
Appointment of joint international experts
A single staff training programme
Raising referring centre awareness
Staff exchanges
2.12.6 Specifically, the benefits of UCLH and The Christie link include:
Geographically located services with sound transport links that allow a largepercentage of patients to stay at home during treatment.
UCLH and The Christie see more PBT eligible patients in their respectiveregional locales than any other centre. The combined practices of UCLH andManchester create one of the largest child cancer practices in the world,together with Europe’s largest practices in sarcoma and brain cancers.
Both UCLH and The Christie have internationally recognised radiotherapyachievements. Both Trusts are able to offer a range of modalities includingIMRT and a variety of stereotactic techniques – which will ensure PBT is usedas effectively and objectively as possible.
Both organisations have a range of overlapping strengths – which if broughttogether will raise respective levels of excellence still further. Both Trustshave strong clinical academic alignment within the patient groups benefitingfrom PBT. UCLH and The Christie are by far the two foremost organisationsfor child, teenage and young adult oncology nationally (and jointly, one ofthe largest globally). Both Trusts also have major clinical academic resourcesfor neurosurgery (the largest research active units in UK, and combinedlargest in Europe), with major academic work on late effects andsurvivorship.
2.12.7 The DH is fully aware of the potential benefits of developing a national service asopposed to two competing services. Although both organisations will operate twofinancially independent centres, both Trusts continue to promote cooperation as theappropriate market environment where the benefits to patients are maximised, andvalue for money for the DH is ensured.
2.12.8 The DH SIF identifies that should future business cases support additional centres,they should be fully incorporated into national service. As such the initial serviceshould be set up with the ability to incorporate additional centres.
2.13 Business Needs
2.13.1 The DH SOC identifies a clear need to develop PBT services in the UK in order toexpand access to all patients for whom this treatment has been identified as themost clinically appropriate as summarised below:
Clinical limitations to overseas treatment because of the complex nature oftheir cancer treatment.
UCLH PBT Outline Business Case
Version 4 Page 35
Limited opportunities for truly collaborative treatments possibly limiting theeffectiveness of treatment.
Impact on patient experience from treatment overseas due to disruption tofamily life, lack of fully integrated care packages and difficulties withcommunications between different countries.
Limited overseas capacity
Pressure on the current overseas programme in determining those patientswho should receive treatment overseas
Cost of treatments overseas
Current lack of research capabilities in the advances of particle therapy.There is considerable expertise in the UK in advanced particle acceleratordevelopment, but a lack of matching clinical expertise which may limitpotential scientific and commercial developments.
Appropriateness of Overseas Treatment
2.13.2 Overseas treatment limits the ability to offer a truly collaborative service betweenthe referring oncology centre and the PBT centre, possibly limiting the effectivenessof the treatment presenting a risk of the clinical care being compromised. In manycases, it is inappropriate to send patients for overseas treatment due to the complexnature of their cancer treatment, which may require associated surgery,chemotherapy and other supportive treatments.
2.13.3 The DH does not fund all the overseas concurrent treatment for PBT patients. TheSOC states that for some of these patients, there are proven clinical advantages tostaying in this country for conventional radiotherapy treatment and the associatedconcurrent treatments. There are also limitations on when a patient may fly aftercranial surgery.
2.13.4 Another major reason for not receiving protons is the time to treatment, i.e. forsome brain tumours the time from surgery to radiation should not exceed 28 days;Currently this is impossible with PBT overseas treatment.
2.13.5 In addition, some patients will require urgent treatment. Given the time associatedwith planning an international treatment, conventional radiotherapy in the UK issometimes a more preferable option. Typically, the time taken from referral tocommencement of overseas treatment is four to six weeks. It is anticipated that thiswill reduce to three to four weeks for most cases and sooner for urgent cases, in aUK based service.
Impact on Patient Experience
2.13.6 Treatment of UK patients at overseas centres as a long term strategy is not idealgiven the significant disruption to family life due to travel and long periods of stayingoverseas. For example, patients treated in the USA will be required to stay there foran average of eight to twelve weeks for treatment. Removing patients from theirfamily and friend support networks for such a long period of time can be distressing,

UCLH PBT Outline Business Case
Version 4 Page 36
and also has potential implications for the ability for the patients or carers tocontinue their paid employment.
2.13.7 The problem of communication between different countries should also not beunderestimated, either due to linguistic or cultural differences.
Limited Capacity Overseas
2.13.8 The ability of the NHS to commission PBT services from overseas is dependent ontheir available capacity. The increasing demand for PBT treatment poses a risk thatthere is limited capacity for patients from the UK as the local population areprioritised.
2.13.9 Many of the USA centres have a business model based around treating a relativelysimpler casemix of treatments, predominately prostate cancer. The capabilities oftechnology required to deliver the UK case mix is different to what is available in theUSA therefore further reducing available capacity. Where technology allows, acommercially run USA service may prefer to not undertake the lengthier complex UKcases in favour of more profitable simpler cases.
Cost of Overseas Treatment
2.13.10 The NSCT PBT panel is currently carefully managing the costs of the programme asthere is an anticipated over spend compared to plan. For 2011/12 an average cost of£75,000 per patient was anticipated for the expected 120 patients. After 7 monthsthe existing cost per patient was £110,000 per patient. To some degree, this is dueto the over reliance on sending patients to USA PBT services at a higher cost.
Ability to Leverage the UK’s expertise of Radiotherapy Research
2.13.11 The UK has contributed much to conventional radiotherapy through innovativeresearch and could contribute significantly to advances in proton and particletherapy. UCLH’s radiotherapy service is one of the leading UK centres for complexand highly technical radiotherapy. The service sees approximately 2,000 patients peryear and is the largest radiotherapy department in the North Central London and theWest Essex Cancer Commissioning Network. UCLH recently became only the secondUK centre to provide Rapid Arc, it provides a full range of modalities including IMRT,brachytherapy, Gamma Knife and a new state of the art TrueBeam LinearAccelerator has been installed at UCLH and is now in operation.
UCLH is a supra regional centre for bone tumours;
UCLH is part of North Central London and West Essex CancerCommissioning Network centre for gynaecological cancers and head andneck cancers;
UCLH is the largest paediatric and young adult centre for radiotherapy inthe UK working in a close partnership with Great Ormond Street HospitalNHS Foundation Trust.

UCLH PBT Outline Business Case
Version 4 Page 37
2.13.12 This clinical strength in radiotherapy extends across UCL Partners with the UK’slargest paediatric cancer service, largest integrated sarcoma service, and largestbrain cancer service. The UCLP services lead not just nationally in their expertise andreputation, but in many instances internationally. In addition to this clinicalexpertise, UCLH’s partnership includes UCL and this brings together capability notjust in biomedicine, but also research applied to healthcare within Engineering,Maths and the Physical Sciences.
2.13.13 Provision of particle therapy in England, given the complexity of the identifiedindication list, would enable unique world leading clinical and technical research tobe undertaken as well as specialist clinical trials to be delivered including novelregimes of combined treatments.
2.14 Clinical Need
2.14.1 PBT has a good clinical fit with UCLH’s current service offering. With its significantPaediatric practice, UCLH is currently one of the biggest referrers into DH’s overseasProton Beam Therapy programme. Initial modelling suggests that UCLH’sradiotherapy practice could provide over 200 patients into the PBT service – and thiscould be significantly larger if we include all of UCLP. As a result, if PBT wereprovided at another facility, it would threaten UCLH’s current radiotherapy practice,particularly its Paediatric caseload. UCLH’s strengths in Radiotherapy and Paediatricservices were the basis for bidding for PBT in 2010 and the basis for the DHannouncing UCLH as the site of one of the two PBT centres in the UK.
2.14.2 PBT will be a part of a UCLH integrated radiotherapy service. Only a handful ofcurrent PBT centres offer both standard photon Radiotherapy alongside PBT, andthose that do are not necessarily integrated – for example, PBT facility isnot on the same site as its standard Radiotherapy facility. As a result, UCLH has theopportunity to develop one of the leading PBT centres and Radiotherapy practices inthe world, as well as benefit from efficiencies of onsite integration. Integration canwork across a number of dimensions: location, staffing, systems. For example,UCLH’s integrated radiotherapy service will utilise one imaging facility as well ashave one staffing model across the two services. UCLH will need to support itsfoundation in Radiotherapy with PBT experience through appropriate appointmentsacross UCLP.
2.14.3 UCLH has the opportunity to become one of the relatively few PBT facilities aroundthe world. As would be expected in a relatively immature, high technology market,we also have the opportunity to install technology at a higher specification than inany other centre in the world. But due to the long lead in time from procurement toan operational facility, the technical solution will be a balance between what istested and can be delivered, and what will limit technological obsolescence risk.There are three scenarios that have been considered in developing the technology:
Due to micro level developments in PBT systems, the system we procurebecomes outdated and does not represent the highest clinical quality systemfor UK patients. This would result in patients, or commissioners, choosingother centres over UCLH
PBT is superseded by technological developments – either within the field ofradiotherapy (i.e. heavy ion therapy), or by a “silver bullet” cure for cancer.

UCLH PBT Outline Business Case
Version 4 Page 38
This would result in a loss of patients, income, and the viability of the wholeservice
2.15 Potential business scope & key service requirements
2.15.1 This section describes the potential business scope and key service requirements forthe project in relation to the business needs previously identified against acontinuum of need ranging from;
A minimum scope – essential or core requirements / outcomes
An intermediate scope – essential and desirable requirements / outcomes
A maximum scope – essential, desirable and optional requirement /outcomes.
2.15.2 As defined in the DH SIF, the following identifies the “Minimum Scope” or essentialrequirements for the national PBT service:
A capacity requirement of up to 1,500 patients per annum between the twocentres (UCLH and The Christie) treating the complexity of indications shownin the framework for the development of PBT service. UCLH recognises thatthe indication list may change over time depending on technologicaladvancements and reviews of clinical outcomes; the complexity of theidentified indications will inevitably affect the treatment capacity of eachcentre.
A single integrated clinical network for all potential PBT cases, using acommon referral process, assessment and care pathway. This will ensurecommon access and treatment protocols and selection of the optimum subspecialism of treatment.
A national service to ensure equitable and appropriate service across thenation and to ensure any consequences upon existing services are carefullymanaged.
A full range of dedicated professional support infrastructure will be availableto deliver care at the highest quality, efficiency and safety on site including:
o Anaesthetists
o Social Work and care support
o Specialist nursing
o Play therapy
o Physiotherapy
o Educational support for children

UCLH PBT Outline Business Case
Version 4 Page 39
o Specialist outcomes assessment support
Innovative models of care delivered the necessary patient support including:
o Good patient information
o Use of video links early in referral process
o Access to adequate low cost accommodation
o Dedicated social worker and support staff
o Encourage of community feeling and mutual support
o Educational support and facilities
o Activities to prevent boredom
o Flexible transport models
Outcomes research to contribute to the international knowledge on the useof PBT modality and improving patients’ outcomes.
Research to explore technological advancements to maximise the benefitsto patients and to ensure that the technology remains competitive withother developments in radiotherapy technology over the lifespan of theequipment.
2.15.3 An Equality Impact Assessment has been undertaken and is included at Appendix 2C.
2.15.4 Table 5 identifies the potential business scope against each key service requirement.Table 6 identified the potential facilities required to deliver these services. Theoptions within these ranges are considered within the economic case.




UCL
HPB
TO
utlin
eBu
sine
ssCa
se
2.16
Mai
nBe
nefit
sCr
iteri
a
2.16
.1Th
isse
ctio
nde
scri
bes
the
mai
nou
tcom
esan
dbe
nefit
sas
soci
ated
with
the
impl
emen
tatio
nof
the
pote
ntia
lsco
pein
rela
tion
tobu
sine
ssne
eds.
2.16
.2Sa
tisfy
ing
the
pote
ntia
lsco
pefo
rth
isin
vest
men
tw
illde
liver
the
follo
win
ghi
ghle
vels
trat
egic
and
oper
atio
nalb
enef
itsw
hich
are
clas
sifie
das
follo
ws: Qua
ntifi
able
(QB)
Cash
Rele
asin
g(C
RB)
Fina
ncia
lbut
non
cash
rele
asin
g(n
onCR
B)
Non
Qua
ntifi
able
(non
QB)
2.16
.3Ta
ble
7be
low
high
light
sth
ePr
ojec
tsIn
vest
men
tObj
ectiv
esan
das
soci
ated
Bene
fits
Crite
ria
cate
gori
sed
byth
eab
ove
clas
sific
atio
ns.
Vers
ion
4Pa
ge43






UCLH PBT Outline Business Case
2.18 Constraints
2.18.1 The project is subject to the following constraints:
DH guidance on PBT service developments
Site and Building constraints – central London location
Availability of Capital Funding
Planning Consent
Building Control
Staffing recruitment and associated training
Availability of PBT equipment capable of delivering the complex casemix andthroughput required.
2.19 Dependencies
2.19.1 The project is subject to the following dependencies that will be carefully monitoredand managed throughout the lifespan of the scheme. These are external influencesthat are predominately outside the control of UCLH and must be actively managedto ensure the overall success of the investment. Any issues that arise must bemanaged and resolved in a timely manner.
National PBT Programme – parameters and guidance determined by the DH.
Ability of the DH to underwrite project costs to deliver the Full Business Caseand procurement phases of the project.
Availability of the technology to deliver treatments to the required numberof patients
Procurement phase of the PBT equipment
Procurement phase of the Contractor for Construction of the building.
Changes to indication list of PBT patients
2.20 Summary
2.20.1 This Chapter has presented the concept of PBT services and the strategic context fordelivery in the UK. It has discussed how the PBT service aligns with the NationalProgramme as well as the UCLH vision, values and objectives. The projectinvestment objectives recognise the qualitative and quantitative benefit that wouldbe realised through the successful completion of the project. The identified risks,constraints and dependencies for the project have also been considered.
Version 4 Page 49



UCLH PBT Outline Business Case
3.3 The Long List of options considered for Phase 4
3.3.1 The DH have committed to the development of two PBT Centres (UCLH and TheChristie), and agreed to fund one accelerator and three gantry treatment rooms oneach site. From this infrastructure investment the DH would like 750 patients to betreated at each site per annum.
3.3.2 The PBT indications list identified by DH represents one of the most clinically richtreatment profiles worldwide. Accordingly, it has been very difficult to definitivelyestimate the likely patient throughput for a 3 room facility despite extensivethroughput modelling at UCLH and the Christie in conjunction with expertise fromUSA facilities and DH PBT experts. Currently the best estimate of likely throughput isa range of through a 3 room facility.
3.3.3 On this basis, and in order to be able to deliver the target activity of 750 patients perUK PBT facility, UCLH have considered the introduction of a second accelerator,thereby increasing beam availability and improving patient throughput. However, ithas been estimated that the additional cost of a second accelerator would be in theregion of Given this increases the total capital investment far in excess ofavailable funding this option was discarded.
3.3.4 An alternative solution to increase patient throughput is the use of single roomsolutions whereby each gantry is service by its own accelerator. Rather than sharingthe beam in a 3 room 1 accelerator proposal, a single room solution eliminates beamswitching time and accordingly should increase patient throughput. Single roomsolutions are currently being developed combine an accelerator and delivery systemin a gantry. However, this technology is unproven and no patient to date has everbeen treated clinically using it. Additionally, the indicative cost at aroundmeans that this solution is likely to be cost prohibitive. Our PBT long list of optionshas therefore focussed on 3 or 4 rooms supported by a cost effective and technologyproven solution that is currently in clinical use.
3.3.5 The following table identifies the PBT long list, of which 9 core proposals have beenconsidered.
Version 4 Page 52



UCLH PBT Outline Business Case
Option 1 – Do Nothing
3.4.3 This do nothing option does not meet the CSFs for the project but is retained in theshort list of options to provide a benchmark for value for money and is predicatedupon the following parameters.
Scope
3.4.4 There is an existing commitment to send up to 400 patients of the highest prioritypatients abroad for PBT treatment. From a DH perspective the do nothing optionassumes that this commitment will continue over the full appraisal horizon. The costof this commitment as identified in the DH Strategic Outline Case is expected to bein the region of £90,000 per patient.
3.4.5 Although PBT facilities continue to be developed across Europe and the USA, thelead time for generating additional PBT is extensive. Whilst patient numbers remainin the region of 70 to 100 per annum, sending this number of patients overseaswould appear to remain a viable solution. However, as the number of patientsrequiring overseas PBT treatment increase the administrative burden of coordinating an overseas PBT programme becomes increasing onerous and costly.
3.4.6 From a Trust perspective the do nothing option consists of the Trust discontinuing itswork on developing a PBT proposal. Should the proposal not proceed past the OBCstage, the Trust would be required to write off PDC funded costs of around £0.8m.
Solution
3.4.7 Although in theoretical terms, it would appear that up to 400 PBT patients could betreated overseas, it is currently uncertain that there is in fact sufficient capacity totreat this number of patients, as set out in the DH SOC; capacity pressures also haveled to upward pressure on PBT prices.
3.4.8 In addition, at round £90,000 per patient, do nothing effectively reaches financialcapacity at around 400 patients p.a. Continuing with an overseas programmeeffectively caps activity at around 400 patients and provides no further capacity,both financially and from an infrastructure perspective, to satisfy patient levels of1,500 as identified in the SOC.
Service Delivery
3.4.9 Patients without access to PBT overseas treatment would receive alternativetreatment. In the majority of cases, these patients would be treated with advancedradiotherapy solutions such as IMRT.
3.4.10 For a minority of cases, no alternative to PBT can be offered either due to young ageor risk of serious toxicity with conventional radiotherapy.
3.4.11 Capacity in Europe and elsewhere cannot be guaranteed as being available for NHSpatients as activity levels increase. Holding the line to the current prioritisedindications list is unlikely to be sustainable, most particularly around the treatmentof paediatric cancers. The adult cases would have been treated with surgery aloneor conventional radiotherapy with inferior outcomes.
Version 4 Page 55

UCLH PBT Outline Business Case
Option 2 3 PBT Compact Gantries plus 1 Accelerator
3.4.12 The Trust has worked closely with a number of overseas PBT facilities to betterunderstand the throughput modelling of a PBT facility. At this stage it should berecognised that there is no other facility in the world that is undertaking such aclinically rich indications list. In addition to seeking overseas PBT support, the Trusthas reflected on its Radiotherapy knowledge to supplement the overseas PBTexperience.
3.4.13 Throughput is directly affected by availability of the proton beam such that as thebeam is shared between several rooms any additional rooms only receive anincremental increase in availability i.e. a 2 room facility with 1 accelerator will treatless than two 1 room facilities. From a throughput perspective a 1 room facility is thebest solution although each room is disproportionately more expensive than for amulti room facility.
3.4.14 The Trust has analysed the clinical throughput and compared this to the projectedcapital infrastructure cost. Based on a capital funding constraint of around £135m athree room facility appears to represent the optimum service/affordability solution.
3.4.15 This option will be based on a proposal of developing a PBT facility of somehousing 1 accelerator and 3 compact gantries. Joint analysis between, UCLH, Christieand DH has identified a throughput range of based on the current DHindications list. Modelling for this option has been based on a throughput figure of
(details of how this figure was reached is attached at Appendix 3A).Analysis identifies that the capital cost of this solution should be broadly comparablewith the available capital funding resources.
Option 3 4 PBT Compact Gantries plus 1 Accelerator
3.4.16 Based on throughput indications indicating that 3 gantries may be unable to deliverthe proposed activity target of 750 patients p.a., the PBT Programme team retainedthe option of a 4 gantry solution in order to be able to treat additional patients overand above the proposed 3 room solution of circa . This proposal is basedon a fourth gantry costing approximately (net) and enabling the treatment ofan additional per year.
3.4.17 Although a four room solution will allow for the treatment of around 60 NHSpatients per annum, the additional capital cost of this solution creates a financialchallenge of being able to deliver this solution with the available capital and revenuefunding envelopes.
3.4.18 This proposal will require the raising of an additional funding of around toconstruct and equip the 4th room. This proposal will result in the following changesover and above the 3 room solution:
additional funding requirement – modelled as FTFF at 2.25%.
additional non recurring funding during construction period Y 3 to Y0(interest on additional FTFF).
additional revenue cost during ramp up Phase year 1 and year 2(interest plus additional running costs).
Version 4 Page 56

UCLH PBT Outline Business Case
Effective marginal tariff of for additional patients compared to 3room solution tariff of around
Increase in total annual revenue for a 4 room proposal torepresenting an increase in costs over 3 room solution of . foradditional
Option 4 3 PBT Compact Gantries plus 1 accelerator plus anadjacent concrete box for conversion into additional roomand/or Accelerator capacity at a later date
3.4.19 The proposed PBT facility will be constructed underground whereby UCLH will thenbuild a Trust funded non PBT clinical facility above ground. On this basis, theconstruction phase of the PBT facility represents a “one time” opportunity todevelop the site below ground. Given the size of each room, it will be exceedinglydifficult and most likely cost prohibitive to develop an additional room once the totalabove and below ground facility has been constructed. As the structure will remainthe same in any scenario due to underground construction, space will be foundwithin the existing construction.
3.4.20 The additional capital construction cost to build a fourth room is around .The intention is that this room would remain unequipped in the first instance, butcould be used to accommodate a fourth compact gantry or an additional Acceleratoronce additional funding sources are identified. This proposal will allow the Trust tofurther develop the PBT facility at a future date by providing a “spare” bunker duringthe initial construction phase.
3.4.21 The financial challenge will be to demonstrate value for money of increasing thetotal capital costs of the PBT proposal by to develop potential futurecapacity but with no additional patient activity.
3.4.22 The following aspects are consistent across short listed options 2 through 4.
Service Solution – working day
3.4.23 Given the substantial capital investment in PBT, and clinical practice from aroundthe world, it is envisage that the UK PBT Centre will operate extended working hoursof 14 hours per day to gain full benefit of the large capital investment. This will besupported by two shifts for staff. Extending the day further would require anadditional shift. As a result, this has been discounted.
Implementation Solution
3.4.24 In order to ensure that sufficiently qualified and trained staff are available once thePBT facility opens it will be necessary to undertake a detailed training programme inadvance of the centre opening. For the technical physics staff this training is likely toinvolve overseas placements at operational PBT facilities. On this basis, it isenvisaged the staff training programme will commence around the last year ofconstruction i.e. year 1. In order to establish the PBT team, recruitment of leadclinical positions will most likely commence in year 2.
Version 4 Page 57


UCLH PBT Outline Business Case
Repatriation of paediatric patients currently being treated abroad should befirst, with adult patients later.
Repatriation of those treatments where surgery and chemotherapy areoften given in close proximity to the radiation therapy.
As planning experience will be at its early stages upon opening of the PBTcentre, from a planning point of view it would be better if the ‘simpler’ cases(fewer beams etc.) were the first to be treated, with progressive ramping upthrough the anatomical sites.
Funding Solution
3.4.29 The funding solution has been determined in agreement with the DH; thecommitment being outlined in the Strategic Investment Framework. The PBTfunding proposal is described in the Commercial case of this OBC, but broadlyconsists of:
Technology Choice
3.4.30 The choice of technology will be determined by the ability to treat the defined set ofpatients and be selected within the procurement process. In this regard the Trust iscognisant of the number of procurement challenges raised by Proton Beam Therapyequipment manufacturers. The minimum requirement defined by the DH is assumedto include three gantry treatment rooms.
3.5 Shortlist Appraisal
3.5.1 The Economic Case requires each option to be appraised by three factors and thentest the sensitivity of the conclusions drawn from the appraisals. These stages of theshortlist appraisal are as follows:
Economic (Financial) Appraisal:
The comparison of the costs of the options against the associated cashreleasing benefits in order to rank the shortlisted options to identify theirrelative Value for Money (VfM).
Qualitative Benefits Appraisal:
The appraisal of each option against the project investment objectives,benefits criteria and critical success factors in order to rank each option toidentify which has the capability of delivering the qualitative benefits mostsuccessfully.
Version 4 Page 59

UCLH PBT Outline Business Case
Risk Appraisal:
The risks associated with the PBT project are assessed against each option toidentify which has the highest level of inherent risk.
Sensitivity Analysis:
Review of the outcomes of the above appraisal in the context of changes toany assumptions made.
3.6 Economic Appraisal
Introduction
3.6.1 This section provides a detailed overview of the main costs and benefits associatedwith each of the selected options. Importantly, it indicates how they were identifiedand the main sources and assumptions.
3.6.2 More detailed information is shown for each cost and benefit line within theeconomic benefits appraisals at Appendix 3B.
3.6.3 In accordance with Green Book guidance, the following core assumptions have beenapplied within the financial analysis in the Economic Case.
3.6.4 The Trust has included an assessment of QALY (Quality Adjusted Life Year) analysis,which is derived from the analysis presented in the DH Strategic Outline Case, this isincluded in Appendix 3C. The QALY assessment presents the UCLH options analysiswithin the QALY analysis framework development for the DH Strategic Outline Case.
Basis of the Economic Assessment
3.6.5 The focus for the Economic case is based on an assessment of Value for Money,reflecting on net present value/and net present cost calculations.
3.6.6 The following broad assumptions have been applied in the Economic analysis:
constant (real) prices
includes opportunity cost
includes indirect and attributable costs – ‘costs of others’
includes all quantifiable costs, benefits and risks
includes environmental costs
excludes all Exchequer ‘transfer’ payments – for example, VAT
excludes general inflation
excludes sunk costs
excludes depreciation, impairments and capital charges
Version 4 Page 60


UCLH PBT Outline Business Case
purposes of the appraisal capital costs associated with the above ground facilityhave been allocated to those services.
3.6.10 The construction costs have been estimated by the Trust’ external professionaladvisors including 10% added for contingencies and 14.3% optimism bias. The PBTequipment costs have been assessed based on non contractual quotes frompotential vendors.
3.6.11 The following section provides further explanation of the methodology used by theexternal advisors to reach the capital and construction costs including the level ofcontingency at 10% and optimism bias of 14.3%.
PBT Equipment
3.6.12 The cost estimate for PBT equipment has been derived based on indicative costsprovided by PBT suppliers including projected payment profile. These costs haveincluded non recoverable VAT at 20%.
Other Equipment
3.6.13 Cost of other equipment, such as CT scanners is based on local knowledge and actualcosts from historical procurement, again inclusive of non recoverable VAT at 20%.
Construction costs
3.6.14 A full detailed elemental cost plan was prepared from approximate quantities on thebasis of cost per sqm rates for building of a similar design and specification. Theserates have been derived from the quantity surveyors cost information relating tohospital projects and from cost analysis published by the BCIS online.
3.6.15 Additional advice has been sought from specialist design team consultants such aswho have extensive knowledge of the construction and delivery of PBT
schemes both in the USA and Europe.
3.6.16 Further cost certainty has been sought through a benchmarking exercise by softtendering the project on Stage C information and an un priced elemental cost planthrough major contractors, who have been involved in per construction on anumber of PBT sites internationally.
3.6.17 The elemental cost plan included an element of quantified risk allowance amountingto 10% together with an industry standard contingency appropriate to a project ofthis size and complexity of 10% (Note: this quantified risk allowance is included inthe Works Total Cost on OB1 (line5)
3.6.18 The optimism bias has been calculated taking into account the separate 10%contingency and quantified risks of 10% as noted above.
3.6.19 In summary, the overall risk allowance on construction costs can be categorised asfollows:
Contingency risk 10%
Optimism bias 14.3%
Version 4 Page 62

UCLH PBT Outline Business Case
Further risk allowance for price design risk, quantified allowances and abnormalpreliminaries of 10%
3.6.20 This is consistent with the Green Book Guidance which sets out the percentageadjustments for cost overruns on historical generic projects where projects with acapital value over £25m increase on average by 30% from OBC to FBC.
3.6.21 OB forms are included on Page 54 of Volume 2 and the optimism bias calculation isincluded on Page 61 of Volume 2.The estimated infrastructure operating costs forthe new facility have been derived wherever possible based on comparison tocurrent Trust operational facilities, i.e. the University College Hospital and the UCHMacmillan Cancer Centre to ensure that estimates are linked to actual running costs.
Opportunity costs
3.6.22 The Green Book states that when developing a build option appraisal, considerationshould be given to the opportunity costs of building on a piece of land. Opportunitycost can be considered as the value of the most valuable of alternative uses i.e. useof land in a different way than in its current use.
3.6.23 The site on which PBT will be located is currently fallow. However, the Trust Boardapproved in principle the proposal to construct a clinical facility on the site abovePBT in September 2012. As such the site is not planned for sale by the Trust andaccordingly it would be inappropriate to represent the opportunity cost of the site asthe potential sale proceeds.
3.6.24 Should the Trust develop the site without PBT then it is likely that the clinical facilitywill go down to level 2. If the Trust develops PBT and the above ground facility, thenthe Trust is likely to go down to either level 3 or level 4, dependent on the PBTequipment. The Trust considers that the potential disposal or rental proceeds fromlevel 3 of the site would be fairly immaterial in the scheme of the overalldevelopment. On this basis it is felt that the opportunity cost of the remaining site isimmaterial.
3.6.25 In addition, given the financial analysis of the PBT facility has been prepared on anincremental basis the opportunity value would have no impact on the directcomparability of the core options.
Description, sources and assumptions
3.6.26 PBT income and expenditure represents a new service and as such has been derivedon a full cost basis. Patient numbers and income have been derived based onextensive work with The Christie, functional USA PBT facilities and also inconjunction with DH PBT experts. Similarly operating expenses have been derived bycomparing and contrasting the cost of the Trust’s UK radiotherapy service with thecost of PBT facilities in the USA. The methodologies used to derive PBT income andcost estimates will be included with the DH SIF that will be jointly signed by DH andthe Trust.
3.6.27 The operating cost estimates identified to operate the PBT facility fell into thefollowing main categories
Staff costs
Version 4 Page 63

UCLH PBT Outline Business Case
Infrastructure costs including utilities, rates and facilities management
Equipment and property maintenance costs
3.6.28 The Trust recognises the additional risk in deriving a cost base for a new service andso has wherever appropriate included prudent cost estimates. A more detailedexplanation for each PBT cost line is included within the Financial AppraisalAppendix 3D.
3.6.29 In accordance with Green Book guidance, the analysis excludes VAT, inflation,depreciation and capital charges as these effectively represent transfer payments.
Net Present Value Findings
3.6.30 The economic benefits appraisal has been carried out on the basis of the full impacton discounted cash flows of the options for PBT. The Net Present Value (NPV) ofeach of the shortlisted options has been calculated by setting out all the cash basedproject costs over the appraisal period. The NPV has been derived by applying adiscount factor to the following broad cash item.
EBITDA
Adjustment for non cash items
Cash releasing benefits
Capital Expenditure (excluding VAT)
Non recurring cash items
3.6.31 Where options have different lifespans, an Equivalent Annual Cost (EAC) is typicallyused for comparison purposes to taking account of the different time periods.However, it terms of the economic case, all options have been appraised over thesame time period in order that the NPV is directly comparable.
3.6.32 The economic useful life of the PBT equipment has been estimated to be 20 years.The economic useful life of the PBT building has been estimated as 40 years. Thelong timescale associated with the development of the FBC and construction of thesite has required consideration on how to take account of cashflows in the outeryears of the life of the building.
3.6.33 On this basis, the NPV calculation has been performed on a 45 year basis being 5years FBC development and construction and 40 years operation. The nominal cashflows of the project have been discounted applying the following Green Bookdiscount rates 3.5% for years 0 to 30 and 3.0% for years 31 to 45.
3.6.34 The OBC Net Present Value analysis was predicated on a 40 year appraisal period.The Trust has responded to the challenge of considering the proposal over a 20 yearperiod. This is presented in Appendix 3E.
3.6.35 Discounted cashflow estimates has been completed making allowance for therefresh of both the PBT equipment (around year 20) and other supportingequipment based on the estimated useful life of these assets.
3.6.36 The following table summarises the NPV of the shortlisted PBT options:
Version 4 Page 64


UCLH PBT Outline Business Case
capacity represents good value for money. As such, the Trust Board approvedOption 4 as the preferred route for PBT.
Risk adjustment
3.6.48 The financial analysis for the 4th room has been prepared on the basis that the Trustis able to treat an additional at a rate of , thereby generating anadditional income stream for the facility of around .
3.6.49 Reflecting on the throughput work, it has been recognised that the marginal benefitof any additional room substantially reduces based on the availability of beam for allrooms. Throughput model and Monte Carlo simulation has indicated that theplanning for the sharing of beam across 4 rooms is substantially more complex than3 rooms. As well as the lost beam switching time the complexity of the casemixmeans that there is likely to be an increase in inefficiency as the solution moves to 4rooms. On this basis, it is felt that there is an inherent risk of treating the complexcasemix through a 4 room solution and whether the Trust would be able to deliver inexcess on patients from a 4 room solution.
3.6.50 On this basis the financial analysis for option 3 (the 4 gantry NHS facility) has beensubject to a risk adjustment to take account of the nature of uncertainty around thedelivery of projected activity from a 4 room solution.
3.6.51 This risk adjustment has been derived as 10.0% of the additional NHS incomediscounted from year 1 of operation through to year 40. As can be identified fromthe risk adjustment in the NPV table above, additional NHS patient throughput fromthe 4th room is an area of high sensitivity. Additionally there is a risk regardingpayment where the marginal cost is in excess of the common tariff.
3.6.52 The Trust has undertaken detailed throughput analysis with the Christie and DHexperts modelling a number of variables including:
Number of fractions and fields per fraction
Time taken to set up and verify the patient
Beam switching and Beam tuning
3.6.53 Throughput monte carlo simulation indicated that the incremental benefit of a 4th
room was around per annum with a lower end estimate of .The Trust then modelled the patient throughput at a prudent perannum. It was agreed to apply a risk adjustment to reduce activity to around the 25percentile of the activity range. This represented a 10% risk adjustment.
Do Nothing
3.6.54 As identified above the impact on the Trust of do nothing will be the writing off ofOBC expenditure of around £0.8m. On this basis the net cost to the Trust of DoNothing is £0.8m from both a cash and NPV perspective.
Three compact gantries from one Accelerator
3.6.55 The DH Strategic Outline Case identified that two centres each with 3 gantries from1 accelerator was the most appropriate solution from an affordability basis as wellas providing a degree of resilience and providing appropriate patient capacity.
Version 4 Page 67



UCLH PBT Outline Business Case
Version 4 Page 70
above ground. Both of these groups have met to evaluate the qualitative benefitsassociated with each of the above PBT options.
Methodology
3.7.2 The appraisal of the qualitative benefits associated with each option was undertakenby:
Identifying the benefits criteria relating to each of the investment objectives
Weighting the relative importance (in %s) of each benefit criterion inrelation to each investment objective
Scoring each of the short listed options against the benefit criteria on ascale of 0 to 10 (where 10 is the maximum score)
Deriving a weighted benefits score for each option
Qualitative Benefits Criteria
3.7.3 The benefits criteria were weighted as follows for each investment objective:
Table 18 Qualitative Benefits Criteria










UCLH PBT Outline Business Case
Version 4 Page 81
3.9 Option Appraisal Conclusions
3.9.1 The selection of the preferred option is dependent upon the relative emphasisplaced on the qualitative factors over the financial constraints. From a qualitativeperspective, the preferred option would be additional capacity for PBT (Options 3and 4). From a financial perspective, the preferred option would be 3 rooms (Option2).
3.9.2 The Trust has had a PBT project team established for the last 3 years, themembership of which includes direct clinical and non clinical staff. In addition, thePBT project team reports to the Phase 4 Programme Board (Phase 4 representingPBT and the above ground clinical facility). Both of these groups provide the fullcomplement of relevant staff and skills to be able to provide input and scrutiny tothe assessment.
3.9.3 As identified above, the assessment was primarily based around the incrementaldifferences between the options and assessing the advantages of developing the 4th
room noting:
It would be a huge logistical challenge and most probably financially prohibitiveto try and build a 4th room after the facility has been constructed.
The implications of the overall construction timeline would be very modest.
The Trust has agreed to fund the modest cost for the 4th room of
This spare room would allow for the development of a future separate case torespond to future developments in PBT or to deliver additional activity.
3.9.4 On this basis, the PBT team, as agreed by the Phase 4 Programme Board and theBoard of Directors felt that the qualitative benefits of constructing the 4th room faroutweighed the additional cost of .
3.9.5 This Chapter has presented the various options available for the clinical PBT services.These options have been appraised against the investment objectives, benefitscriteria and critical success factors as well as economically appraised against capitaland revenue costs to identify which option is the most advantageous
3.9.6 The qualitative benefits appraisal indicates that the preferred option would be tobuild 4 PBT rooms (Options 3 and 4).
3.9.7 The financial appraisal indicates that the most cost effective solution would be tobuild and fit out 3 PBT rooms with gantries
Option 1 – Do nothing
3.9.8 This option ranks 4th.
3.9.9 Although the solution has the lowest capital cost, from a service perspective thisfails to deliver the appropriate capacity to meet the demands of future projectedpatient numbers. Additionally, it leaves the future treatment exposed to theavailability of future “spare” capacity in overseas facilities and provides no tangibleresilience.

UCLH PBT Outline Business Case
Version 4 Page 82
Option 2 – 3 Gantries and 1 Accelerator
3.9.10 This option ranks as 2nd.
3.9.11 Throughput modelling has indicated that, in conjunction with affordability, a 3 roomsolution is currently an optimal solution with regard to the cost effective treatmentof PBT patients. It should be noted that in recognising the very complex indicationslist, the Trust have been prudent in undertaking throughput analysis and that PBTEquipment continues to develop i.e. improvements in beam switching time.
3.9.12 Notwithstanding these points, this option is wholly consistent with the StrategicOutline Case in that a 3 gantry 1 accelerator facility (on each of two sites) providesresilience, provides sufficient patient capacity and is affordable.
3.9.13 The only downside when compared with Option 4 is that it provides no additionalinfrastructure expansion capacity and as such this option means that any futureextension or services at a later date may be highly cost prohibitive.
Option 3 – 4 Gantries and 1 Accelerator
3.9.14 This option ranks as 3rd.
3.9.15 It provides additional patient throughput over and above the 3 room solution ofaround p.a. (based on a same complex indications list). From a costperspective the capital cost of the equipped 4th room is some greater than a 3room solution. This additional cost exceeds the capital budget and accordingly willrequire an additional funding source of around ).
3.9.16 Where this additional activity is used to treat NHS patients the marginal cost of this4th room will push up the average tariff price from around per patient aswell as exceed the current DH proposed budgets.
3.9.17 This option is therefore unaffordable from both a capital and revenue perspective.
3.9.18 In addition to the fact that this option produces a lower NPV than both options 2and 4, option 3 is also not without additional risk. The development of a 4 roomsolution will increase the configuration phase and will most likely extend the rampup period to full operation.
3.9.19 Whilst this option allows for the delivery of additional NHS activity, the proposaldoes not come without additional risk. The DCF analysis has therefore been adjustedto reflect an estimate of this additional risk.
3.9.20 After taking account of the additional operational and financial risk, it would appearto be an inappropriate proposal to equip a 4th room at this stage until more provensolution is identified to reduce cost, enhance beam sharing or to deliver a singleroom solution for the 4th room so as to mitigate operational risk.
Option 4 – 3 Gantries and 1 Accelerator and a spare bunker
3.9.21 This option ranks as 1st.

UCLH PBT Outline Business Case
Version 4 Page 83
3.9.22 This option proposes building an additional non equipped bunker as part of the PBTdevelopment at a capital cost of circa £1m over and above Option 2. In practicalterms, the only real potential to develop an additional bunker is during the coreconstruction period as reverse engineering an additional bunker at a later stage willprove to be a very difficult construction challenge and most likely cost prohibitive.
3.9.23 Given that the Trust has proposed to separately fund the 4th room, at a cost of ,this option provides future expansion potential at no additional cost to DH.
3.9.24 By building an additional bunker during the initial construction phase this will allowfor the room to be equipped at a later stage by either extending the current beam orby introducing a super compact 1 room solution. However, from a value for moneyperspective, the Trust has prudently assumed any future benefit from the 4th roomand so the total capital costs of the additional bunker merely worsens the DCF.
Overall conclusion
3.9.25 In summary, this OBC recommends a preferred option (Option 4) based upon:
3 PBT Compact Gantries, 1 accelerator and an additional spare (unequipped)room.
3.9.26 Full details of the design of this Option is attached at Volume 3.
3.10 Sensitivity Analysis
3.10.1 In general the methods used for sensitivity analysis would be:
‘switching values’
scenario planning / analysis (‘what if‘) by altering the values of the‘uncertain’ costs and benefits to observe the effect on the overall ranking ofoptions.
3.10.2 However, with regards to the proposed PBT facility there is a core level of capitalcost and operating cost that is consistent across all three options 2, 3 and 4. In thissituation there is little benefit to be made by arbitrarily switching or changing valuesand so sensitivity analysis will instead be focussed by considering those items that inpractice are likely to vary.
3.10.3 The Trust identified that it was more appropriate to undertake sensitivity analysis ina focussed manner rather than simply changing numbers. By way of example theprovision of a three room facility with 3 gantries is a consistent scenario across the 3options. As such it was noted that sensitising items in this “base” PBT option wouldnot alter the order of the ranking of the core proposals.
3.10.4 Regarding the 4th room the Trust has recognised the robust process undertaken toderive the construction cost of the facility. On this basis, the Trust does not perceiveit is a realistic or appropriate sensitivity that it had incorrectly estimated this cost ofthe additional room by 500%. Such a sensitivity would clearly undermine thecomplete basis upon which the capital costs were derived. Additionally, any costincrease in the 4th room would be matched by additional funding by the Trust. From
UCLH PBT Outline Business Case
Version 4 Page 84
an NPV perspective, it would take an increase in cost of over before the 3 plus1 gantry option had a worse NPV than a 4 gantry option.
3.10.5 The NPV of do nothing is at least £30m worse than any PBT scenario. Therefore itwould take a sizeable movement in a number of sensitivities before do nothingbecame the preferred option.
Capital sensitivity
3.10.6 The capital cost bases of options 2, 3 and 4 are all derived from a core capitalinfrastructure being the core PBT facility and single accelerator. The only differencesbetween the options are therefore any additional room, at a cost of around ,and the cost of an additional gantry at .
3.10.7 The core capital cost for a 3 gantry facility is estimated at some . This cost willbe the same for options 2, 3 and 4. Should this capital cost flex, then it will flexsimilarly for all three of these options.
3.10.8 Relative to the cost of the core facility the additional costs of an additional room oran additional gantry are fairly marginal and will not materially switch the ranking ofthe options.
Conclusion on capital sensitivity
3.10.9 On this basis, there is little gain to arbitrarily flexing the capital cost base as this willnot change the order of the three PBT options.
Income sensitivity
3.10.10 The income bases of options 2, 3 and 4 are all derived from a core assumption beingNHS income, once fully operational, of around arising from the treatment ofaround patients p.a., at a tariff rate of
3.10.11 Options 2 and 4 are both based on this same income assumption and so theirranking will not switch through a flexing in income assumptions.
3.10.12 Option 3 is predicated on deriving additional NHS income over and above options 2and 4 by using the equipment 4th room to treat additional NHS patients. Once fullyoperational, this option is projected to generate additional income of aroundp.a. arising from the treatment of an additional patients p.a., at a marginaltariff rate of around .
3.10.13 Were the Trust able to treat in the region of NHS patients in the additional 4th
room, then the additional income will have a direct improvement on the NPV ofOption 3. However, in order to reach this level of income, the facility would need tobe treating around patients p.a. a target that both the Trust and DH feel wouldbe very difficult to achieve.

UCLH PBT Outline Business Case
Version 4 Page 85
Conclusion on income sensitivity.
3.10.14 The Trust feels that it would be inappropriate to further flex the NHS activity. Assuch, it is not felt that the ranking of options 2 and 4 will switch as a result of achange in income assumptions.
3.10.15 However, as identified in the economic analysis above it is recognised that thisassumption of additional income is highly sensitive. Were the Trust to over achieveon this target it is likely that the ranking of option 3 will switch to 1st whereasunderachievement will retain the ranking 3rd place ranking.
Expenses sensitivity
3.10.16 Similar to Capital, there will be a high degree of commonality between the operatingcost bases of options 2, 3 and 4.
3.10.17 Given the 4th room for option 4 is non equipped and will be mothballed untildeveloped, the running costs of options 2 and 4 will be substantially identical.Although option 3 will consume additional pay and non pay resources over andabove options 2 and 4 it is felt that a change in this additional NHS cost base will bemarginal and would not switch the rankings of the options.
3.10.18 The equipping of the 4th room in option 3 will incur additional staff and non paycosts. However, this additional cost is fairly marginal in relation to the overall PBToperating budget. Additionally, the 4th room is by definition a separate area and so itis felt there would be sufficient ability to realise sufficient cost savings so as to alterthe ranking of the options.
Conclusion on expenses sensitivity.
3.10.19 Sensitivity in expenses will not switch the options.
3.11 Switching Values
3.11.1 In order to consider the impact of switching values, the Economic analysis considersthe change in incremental values whereby the order of the raking of the optionsswitches..
3.11.2 The switching analysis has been undertaken on the net present value analysisincluded in Table 14. This switching analysis is summarised in the following tablewith an accompanying commentary below:


UCLH PBT Outline Business Case
Version 4 Page 87
Income
3.11.6 The 3 gantry and 3 gantries and a spare room option have the same income and sothe switching of values has no impact on the raking of these two options.
3.11.7 Regarding income switching, in order for the 4 gantry option to become raking of 1,it would require an increase in EBITDA of £370k p.a. with an EBITDA of 34% for the 4gantry option, this would equate to an increase in income of p.a.
3.11.8 In order to switch ranking to 1, the 4 gantry option would require an increase in theincremental income from p.a. an increase of 39%.
3.11.9 Over 20 years, do nothing would have to generate additional income of £3.15m withno associated cost in order to be ranked 1.
Expenses
3.11.10 The 3 gantry and 3 gantries and a spare room option have the same expense baseand so the switching of values has no impact on the raking of these two options.
3.11.11 Regarding expenditure switching, in order for the 4 gantry option to become rakingof 1, it would require an increase in EBITDA of £370k p.a. with an EBITDA of 34% forthe 4 gantry option, this would equate to an increase in income of p.a.
3.11.12 In order to switch rankings to 1, the 4 gantry option would require a decrease in theincremental expenses from p.a. a decrease of 48%.
3.11.13 The do nothing option has no capital involved therefore switching is not relevant.
Conclusion
3.11.14 The above switching analysis shows given that the only difference between a 3gantry option and a 3 gantry with a spare room option is the additional capital costof the 4th room at an estimated cost of around . The switching analysis showsthat it is highly unlikely that these options would switch ranks based on a switch incapital value.
3.11.15 Regarding the 4 gantry option, in order to switch value to a 1, from a capitalperspective this would require a reduction in the estimated capital costs of the 4th
room by around 76%. Considering income, in order to switch the ranking of thisoption to a 1, would require an increase to incremental income from the 4th room ofaround £1.1m a year or 39%. Similar consideration of expenses would require areduction in incremental expenses for the 4th room of p.a. or 48%
3.11.16 As identified in the sensitivity section of the Economic Case, each option ispredicated on a core 3 room option. As such, in order to switch values for the 4gantry option would require a substantial change in incremental values.
3.11.17 The analysis shows that it seems highly unlikely that switching would make the donothing the preferred option.
3.12 Preferred Option

UCLH PBT Outline Business Case
Version 4 Page 88
3.12.1 Having considered the likely impact of sensitivity the preferred option remainsunchanged being:
3 PBT Compact Gantries, 1 Accelerator and an additional spare (unequipped)room
3.12.2 Further details of the Preferred Option can be found in the Design Volume 3





UCLH PBT Outline Business Case
Version 4 Page 93
The project timeline to deliver an operational building and treat the firstpatient by Q4 – 2018
Level of risk which can be accepted or transferred adequately
Outturn cost certainty
Flexibility in terms of control of design interface by client & contractordesign approvals necessary
Change which can be accommodated within the project or resulting contract
Level of technical competence within the market to deliver the project
Meeting OJEU thresholds and regulatory requirements
4.7.7 In particular the considerations of the intended procurement strategy has taken intoconsideration review of :
Joint equipment and build contracts or as separate procurement workstreams
Build procurement in isolation
Equipment procurement in isolation
4.8 Proposed Procurement Strategy for the PBT Equipment
4.8.1 UCLH and The Christie will jointly run a procurement process for PBT equipment andthe associated services. On assessment of the different options, the Trusts’preferred route is a single procurement with one Lot. On balance, this was seen asoffering a number of advantage to the national programme:
Trust would move through the procurement at the same rate with common legaland procurement advisors and associated savings to the project budgets.
Suppliers would make offers for the supply of both sites allowing savings to beleveraged and the value of working with a single supplier to be tested andevaluated in the procurement.
It would mitigate the risk of Trusts not being able to conclude a joint evaluationconsistently to meet the needs of their own sites, thus risking delay to thenational programme.
4.8.2 These advantages balanced possible issues such as reduced influence for each Trust,requirement for both Trusts to sing off on a final solution to complete the processand no fall back if Trusts cannot agree on a preferred option.

UCLH PBT Outline Business Case
Version 4 Page 94
4.8.3 Following EU procurement rules for public bodies, the procurement will beadvertised in the supplement to the Official Journal of the European Union. Due tothe complexity of the equipment procurement, it has been determined thatCompetitive Dialogue (CD) is the most appropriate procurement route to ascertainthe technical means of meeting the Trusts’ requirements. The Trusts’ equipmentprocurement strategy is available in Appendix 4B.
4.8.4 Due to the complexity of the equipment and the assessment of the equipmentsupplier market, it would be preferable to separate out the equipment and buildprocurement to enable the selection of optional equipment and also optimal buildsolutions. It was further considered preferable for each Trust to run separate buildprocurements to enable links to the local Trust and integration with other (nonproton) constructions within each Trust’s programme. Further information on theUCLH Construction procurement strategy is available in Appendix 4C.
4.8.5 An overview of the proposed ICT expenditure for the PBT project at UCLH has beenprovided in Appendix 4D.
4.8.6 It has been assumed that due to the complexity and uniqueness of the equipment inthe UK that the procurement of the PBT equipment will be carried out using the EUCompetitive Dialogue procedure. This will allow the Trust to explore the mosteconomical way of buying the technology whilst being able to explore the mostadvanced equipment.
4.8.7 A detailed Equipment Procurement Strategy is set out in Appendix 4B.
4.8.8 The following identifies the key dates for the PBT equipment procurement(Appendix 4E for milestone tracker):
Issue OJEU July 2013
Evaluate expressions of interest and select short list (4 months) November2013
1st stage dialogue complete – April 2014
Evaluate and select preferred vendor October 2014
4.8.9 The DH proposal is for PBT to be provided by two centres at UCLH and The Christie.UCLH have worked closely with The Christie with the submission of a joint bid inMarch 2010 and subsequent development of the project. On the procurement of thePBT equipment, the Trusts have worked together to consider the optimal approachfor both Trusts and opportunities to benefit from partnership.
4.8.10 Since approval of the DH SOC, the Trusts have developed the procurement approachwith the DH. The default position for all three organisations is to hold oneprocurement as the technical specification is the same across both Trusts and therewill be project efficiencies from running a single procurement. Consideration hasbeen given to running a procurement with three Lots (one for the equipment

UCLH PBT Outline Business Case
Version 4 Page 95
requirement at each Foundation Trust and one for a joint solution). The concernwith this approach was the added complexity of the bidding process and evaluation.As outlined in the DH SIF, the approach agreed is for a one Lot procurement (SeeVolume 4 for DH SIF). This is based on the benefits of one vendor across the twosites and the potential procurement savings. This may be revisited if the preferredsolution does not satisfy the conditions above.
4.8.11 The expectation is that the procurement will be for the Equipment plus maintenanceservice (currently expected to be for a minimum of five years).
4.8.12 A managed service has been discounted as the service needs to be integrated intoeach Foundation Trust service delivery strategy.
4.8.13 A technology refresh option, whilst being attractive, was considered unlikely torepresent value for money and would be difficult both to document in aspecification and evaluate in a bid. Whilst it will be a bid requirement for state ofthe art equipment to be provided, technology improvements are likely to be limitedto upgrade packs.
4.8.14 Vendors will be prequalified to ensure that they are able to meet the corerequirements of the Trust’s needs and then taken througha
. This will maintain competition whilst reducing costs for both the publicand private sectors.
4.8.15 The DH and Commissioning Board have confirmed that they wish to sign off thespecification prior to procurement and be involved in setting the evaluation criteriaand the evaluation of the technical solutions. However, the final selection will be theresponsibility of the Trust.
4.8.16 An Appointment Business Case will be developed for approval prior to selecting apreferred bidder and Confirmation Business Case will be submitted for approvalprior to contract signature.
4.8.17 From initial issue of the OJEU advert for a PBT equipment supplier is 25 months. Thecompetitive dialogue route has been selected on the basis that this will be a first inthe UK and therefore the contract and specification can be refined as the processdevelops. It is anticipated that the contract negotiations will take 9.5 months andwill therefore be the critical path activity that will delay selection of a preferredvendor until the end of April 2014.
Confirming Business Case needs tobe produced for Trust approval and then DH, Treasury and Monitor approval beforean order can be placed. The allowance in the programme for these activities is 7months with approval to place an order being granted at the end of February 2015.

UCLH PBT Outline Business Case
Version 4 Page 96
Separate Build Procurement Option Analysis
4.8.18 Having established that it is beneficial to separate the equipment procurement fromthe construction procurement; there are a number of approaches to theprocurement of the design and construction work and these offer competingadvantages and disadvantages in seeking to deliver the project’s priorities.
4.8.19 There are a variety of options and add ons within each group (e.g. cost plus or targetcost) each with their own pros and cons. The main procurement routes are asfollows:
Traditional contract route
Two Stage “Traditional” form of contract
Design & Build form of contract
Managed form of contract
Procure 21+
IESE Framework
Competitive Dialogue
Traditional contract route
4.8.20 This procurement route is projected to deliver the project by Q1 – 2018. Anyalterations to the contract would need therefore to be assessed and instructed ontheir merits. This route does however offer the following points:
Positive Issues:
More time for the Design Team to refine the detail / Coordinate andcomplete the design.
More time for the Design Team to obtain End user input to the resultingdesign which will be contracted and detailed in the contract thereby refiningthe brief.
Control of design remains with the employer
Negative Issues:

UCLH PBT Outline Business Case
Version 4 Page 97
Two Stage Traditional Form of contract
4.8.21 This procurement route is projected to deliver the project by Q1 – 2018 – Thisprocurement approach is dependent upon agreeing approximately 80% of theprojects value prior to contract execution and the client & stakeholders accept thatthe contractor then works with the client to finalise the remainder (20%). This issimilar to the Traditional route in that the client bears the risk of change to the initialcontract and is dependent upon accurate information being made available to thecontractor at all times.
Positive Issues:
More time for the Design Team to refine the detail / Coordinate andcomplete the design.
More time for the Design Team to obtain End user input (i.e.: post PrincipalAward & with respect to FF&E) when brief is emerging or unclear.
Control of design remains with the employer
Negative Issues:
Design & Build form of contract
4.8.22 This procurement route is projected to deliver the project by Q1 – 2018 – This routeoffers Design & Cost certainty and allows the Design Process to proceed in tandemwith both the Procurement and Construction Process. It necessitates an agreementup front of a fixed price & a programme and may also involve the novation or nonnovation of some or all of the present design consultants to the Main Contractor (forthe construction delivery).
4.8.23 To enable the facility to be open on time the team are proposing a Design & Buildform of contract where a contractor is selected from a list of 3 or 4 to proceed toprice & develop the design from that point to a point where a fixed price is agreedwhilst also separate Equipment vendor is being sought. The final order placement ismade when an equipment providers details are finalised and coordinated with thecontractor’s proposals.
Positive Issues:

UCLH PBT Outline Business Case
Version 4 Page 98
Single Point responsibility for the above and below ground (Constructionworks)
Programme Certainty to deliver the building for required opening.
Cost certainty to deliver the building once contract has been awarded
Retains a degree of control with client team through remaining designevaluation reviews with contractor (with or without novation of designteam)
Negative Issues:
Managed Form of contract
4.8.24 This procurement route is projected to deliver the project by Q1 – 2018 – Themanaged form of contract involves a contractor who will manage and procure eachof the individual elements of work (work packages), then place contracts with thesesuppliers and the employer to execute the works, he also then coordinates theirdelivery on site.
Positive Issues:
More time for the Design Team to refine the detail / Coordinate andcomplete the design.
More time for the Design Team to obtain End user input, if the brief isemerging or unclear
Negative Issues:
Procure 21+
4.8.25 ProCure 21 is a framework which has been organised by the DH for constructioncontracts throughout the NHS. The framework, now in its second generation, isbased on collaborative working through the use of the ECC Contract, Option C. Theframework was let in October 2010 and is due to run for 6 years.

UCLH PBT Outline Business Case
Version 4 Page 99
4.8.26 As the framework has already passed through the EU procurement process, acontractor can be appointed without notification in the OJEU. Because theframework is based on a pre agreed pricing mechanism, no actual tender process isrequired. Selection is made from the framework contractors, referred to as PrincipalSupply Chain Partners (PSCPs), solely on the basis of quality.
4.8.27 To do this, a scheme information pack is emailed to the PSCPs, in response to whichPSCPs who wish to be considered submit an expression of interest. The NHS clientselects a shortlist of PSCPs and invites them to an open day, following which theyattend an interview and a selection is made. This process takes three to four weeksalthough, in some circumstances, a PSCP can be appointed quicker than this. Theearly appointment of the contractor has both programme benefits and enablesconstruction input to the design process, thus influencing “build ability”.
4.8.28 Under ProCure21+, the Trust and PSCP agree a Target Price. Should the project costless than this figure, the first 5% of the difference is split 50/50 between the Trustand PSCP. Any saving below this level goes 100% to the Trust. Should the projectcost more, the client Trust only pays the Target Price. For this reason the TargetPrice under ProcCure21+ is normally referred to as the Guaranteed Maximum Price(GMP). The GMP is established based on framework rates and a process of openbook market testing of works packages.
Positive Issues:
Easy and quick timescale to appoint contractor
More time for the Design Team to refine the detail / Coordinate andcomplete the design.
More time for the Design Team to obtain End user input, if the brief isemerging or unclear
Negative Issues:
IESE Framework
4.8.29 The Improvement and Efficiency South East (IESE) framework supports councils andpublic sector organisations in the south east including London Authorities. As suchUCLH are eligible to utilise the framework. The framework was originally placed inJuly 2007.

UCLH PBT Outline Business Case
Version 4 Page 100
4.8.30 The IESE framework is based on the principal of a two stage tender process. Otherthan a reduction in timescales, a major advantage of this approach is the earlyinvolvement of the contractor who can contribute his construction expertise to thedesign process, thus influencing ‘build ability’ cost and timescales. An additionalbenefit of IESE is that it is not based on a specific form of contract enabling the Trustto select as appropriate.
4.8.31 To appoint a contractor, a project outline would be developed by the design teamand issued to the ten contractors by the framework managers. The contractorsrespond, demonstrating their intent via an expression of interest. From thesubmissions, the framework managers draw up a shortlist of contractors. The nextstage of the process involves a mini tender whereby the shortlisted contractors areinvited to submit their bids on the basis of information developed by the designteam. Rates for prelims, overhead and profit were confirmed when the contractorswere appointed to the framework which the contractors utilise when building thepreliminaries costs for evaluation in mini competition.
4.8.32 Within the mini tender submissions, contractors are required to demonstrate theirproject specific approach, competencies and key initial commercial information.Predominantly evaluation and selection of a contractor is on the basis of quality andvalue rather than lowest price, on 70% quality 30% commercial basis. Following themini tender the chosen contractor would be appointed on a pre constructionagreement to develop the design, depended on the procurement route and form ofcontract and then enter into a process of open book market testing of workspackages to arrive at a Target Price. This is then firmed up after the open booktenders to a fixed contract offer. On arrival at the target price, the Trust wouldappoint the contractor to deliver the project. If the project were aborted at thisstage the Trust would be liable for any contractor costs incurred.
Positive Issues:
Easy and quick timescale to appoint contractor
More time for the Design Team to refine the detail / Coordinate andcomplete the design.
More time for the Design Team to obtain End user input, if the brief isemerging or unclear
No set or defined contract and therefore potentially flexible to contractterms
Negative Issues:

UCLH PBT Outline Business Case
Version 4 Page 101
4.8.33 The diagram illustrated below highlights the majority of differing types ofprocurement routes and resulting contract opportunities which exist each withcompeting characteristics with regard to:
Design Flexibility
Programme Certainty
Cost
Change
Figure 4 Different Types of Procurement Routes
4.8.34 The analysis below summarises the various advantages and disadvantages of theseoptions considered. The main issues relate to cost certainty flexibility and timelinessof the development.
4.8.35 Based on this analysis, UCLH’s PBT project will proceed with two procurementroutes, firstly the Design & Build contract for the Construction elements of theproject and secondly a Competitive Dialogue route for the PBT equipment.



UCLH PBT Outline Business Case
Version 4 Page 104
and construction risk whilst maintaining the integrity of the Trust’s design andfunctional requirements.
4.9.2 The EU Restricted procedure will be used for this contract which will incorporateboth the PBT element below ground and the Phase 4 element above ground.
4.9.3 In accordance with the Trust’s Standing Financial Instructions 6 tenderers will beprequalified to provide a tender submission. The tenders will be evaluated againstagreed criteria prior to submitting a FBC for approval.
4.9.4 It is currently assumed that the incumbent design team will be novated to thesuccessful contractor at contract signature with necessary warranties in place to theTrust.

UCLH PBT Outline Business Case
Version 4 Page 105
Chapter 5: Financial Case
Why the chapter matters
The investment required for the Phase 4 Project must show value for money in achieving theinvestment objectives and benefits criteria. The proposed financing and financial implicationof the project provides confirmation of on going affordability.
What the chapter says
This Chapter outlines the forecasted financial implications of the proposed option (as set outin the economic case) and the proposed deal.
5.1 Introduction
5.1.1 The financial appraisal in the Economic Case considered the comparable value formoney of the shortlisted options. From this analysis, a three room PBT solution wasidentified as the preferred option.
5.1.2 This Financial Case identifies the overall forecast financial implications of thispreferred option and demonstrates how the proposed investment can be paid for.
Development of the financial model
5.1.3 During 2009/10 the Trust constructed an operating PBT model in order to support itsbid to DH in October 2010. Once it was identified that the Trust’s Phase 4 proposalwould incorporate PBT services below ground and a non PBT clinical facility aboveground, the Trust engaged to produce a joint financial model for both UCLHand The Christie. The brief was to produce a financial model that could provideoutputs for PBT to support the DH bid and for the total Phase 4 facility to supportthe Trust’s overall development.
5.1.4 The financial model has been produced, fully tested and utilised to producethe financial projections for the preferred option. The process of producing the OBChas revealed some limitations in the functionality of the model i.e the change to thefunding proposal and the requirement for FTFF functionality. Workarounds wereincorporated into the model and these limitations will be addressed after the OBChas been agreed so that more detailed financial analysis can be developed.
Basis of the Financial Assessment
5.1.5 The focus for the Financial Case is based on an assessment of the financialimplications of the proposal including analysis of the impact on Income andExpenditure, Balance Sheet, Cashflow and an assessment of how the proposal willbe funded.
5.1.6 The following broad assumptions have been applied in the Financial analysis:
Inflated (Nominal) prices
Excludes opportunity cost



UCLH PBT Outline Business Case
Version 4 Page 108
With PBT income at around .this represents about of Trust income andwas noted as being a smaller transaction in income terms than the recentlyacquired RNTNEH hospital with income of around £30m p.a.
5.2.11 Finally it is noted that the Strategic Investment Framework includes provision thePBT tariff will set at a level so as to reimburse the Trusts and that sufficient marginwill be included within the tariff to avoid dilution of the Foundation Trust totalreturn. On this basis the Trust recognises that the financial implications of the PBTproposal should not alter the Trusts overall risk rating
5.3 Impact on the income and expenditure account and balance sheet
5.3.1 As identified in the Strategic Case, this represents a significant transaction for boththe Trust and the Department of Health. Given the intention to procure the PBTequipment through competitive dialogue, the broad timeline in which to completethe business case, construct the facility and then configure the site is approximately7 years, the first patient being treated during the 7th year
5.3.2 The following table summarises both the capital and revenue outgoings for theperiod up to opening at or around year 7 (2018/19). Additionally, this tablesummarises the new capital and revenue streams from which the proposal will befunded.


UCLH PBT Outline Business Case
Version 4 Page 110
5.3.3 The above table projects some minor timing difference between sources andoutgoings. In reality the Trust will take the opportunity to fine tune the timing forthe receipt of sources of funds such that drawdown of funds is much more closelymatched to outgoings i.e. phased drawdown of FTFF facility.
Capital expenditure
5.3.4 The overall capital cost of the proposal, subject to competitive procurement, hasbeen estimated to be . Of this some represents the capital cost ofcompleting the Full Business Case (FBC) and design work, which will be incurredduring years 1 to 3.
5.3.5 The Trust has considered the accounting treatment of capital expenditure asidentified in 5.14 below. Generally Property, Plant and Equipment is capitalisedwhere:
It is held for use in delivering services or for administrative purposes
It is probable that future economic benefits associated with the asset will flow tothe trust
It is expected to be used for more than one financial year
the cost of the asset can be measured reliably
5.3.6 Costs of site preparation, delivery and handling, installation, related professionalfees for architects and engineers. Where OBC to FBC costs are felt to be directlyattributable the proposal is that they will be capitalised. DH has indicated generalagreement with this proposal by proposing that OBC to FBC costs are funded by PDCrather than non recurring income.
5.3.7 The capital construction works will commence in year 4 and take approximately 3years. As a result of retentions, final capital payments of around will be paidduring the set up stage, year 7.
Revenue outgoings
5.3.8 It is expected that the cost of around to produce the FBC, will be funded byPublic Dividend Capital (PDC) and will be capitalised rather than recorded as arevenue expense.
5.3.9 During the FBC phase it is estimated that there will only be a small revenue impactof represented by the interest charge on the PDC drawdown.
5.3.10 During the construction phase, the Trust will start to incur items of expenditure forwhich it will not be possible to capitalise, and so will be recognised as a revenueexpense (e.g. training costs and interest). The treatment of these costs is consideredbelow.
5.3.11 Such revenue costs during the construction phase will be funded by a separate nonrecurring expense.

UCLH PBT Outline Business Case
Version 4 Page 111
Capital Funding sources:
5.3.12 The capital funding solution has been determined in agreement with the DH; thecommitment being outlined in the Strategic Investment Framework. The PBTfunding proposal is described in the Commercial case of this OBC, after takingaccount of the financial implications of the programme slippage, broadly consists of:
5.3.13 Currently it is recognised that the projected capital cost of the proposal exceeds thebase source of funds of by some . Of this (gross cost) represents thecost of the 4th spare room which will be funded entirely by the Trust. This leaves aprojected funding gap of some or 3.3% of total capital expenditure.
5.3.14 It should be noted that in deriving the capital cost estimate of the Trust haswherever possible included prudent capital cost estimates and that for PBTequipment in particular cost has effectively been included at “list price”. Accordinglythere is a clear expectation that this small funding gap will be closed once theprocurement moves to a more competitive process.
5.3.15 Currently the Trust has bridged this funding gap in the financial model by assumingthat additional donation income will be achieved, given that the financial impact ontariff will be broadly comparable to a reduction in capital cost.
Revenue funding sources
5.3.16 Both the Trust and the Department of Health have recognised that there will be anelement of pre operating revenue expenditure prior to the facility being configured,opened and available to treat patients
5.3.17 The Department of Health will require the Trust to retain tight controls over suchrevenue costs and minimise these where possible. With regards to the funding ofthese revenue costs, the Strategic Investment Framework recognises that these willbe funded by the Department of Health by way of non recurring revenue.
Further information
5.3.18 A more comprehensive analysis of the impact of the proposal on the Trust’s incomeand expenditure account and balance sheet are included in sections below.
5.4 Overall affordability
5.4.1 The availability of sufficient funds to finance the PBT proposal is an absolute prerequisite for the final approval of the project. Initial consideration was given todeveloping a PBT solution by developing a Special Purpose Vehicle (SPV) sourcedwith commercial funding. After considering this proposal it was felt that it would bechallenging to deliver a value for money solution through a commercially fundedSPV.


UCLH PBT Outline Business Case
Version 4 Page 113
Conclusion on Affordability
5.4.7 In conclusion, the Trust has a robust financial platform from which to undertake thisPBT development. Notwithstanding this the Trust’s existing I&E is not strong enoughto mitigate substantial PBT risk. The DH has recognised that in this regard the Trusthas less potential to pool risk and so the majority of risk will be borne at Departmentlevel.
5.4.8 The proposal for the Trust to take on an additional FTFF debt will result in theTrust being comparatively highly leveraged for an NHS provider and anyconsideration of the availability and affordability of finance will need to reflectregulatory limits and the potential limits on the Trust’s ability to finance otherdevelopments.
5.4.9 The Trust fully recognises the nationally challenging financial environment regardingthe real term reductions in NHS wide budgets and the requirement to deliver yearon year savings. However, the Trust can demonstrate a strong financial position withan associated Monitor risk rating of 3, although in doing so it recognises that thisposition is based on controlling operational risks in a challenging environment.Additionally, the Trust can demonstrate a proven track record of delivering real andsubstantial savings programmes along with experience to deliver major projects ontime and on budget.
5.4.10 The Trust and DH have clearly defined the funding streams for both capital andrevenue along with the broad allocation of risk within the SIF. In doing so the Trustcan demonstrate that the scheme is affordable and deliverable.
5.5 Impact on Clinical Services
Cost of Services
5.5.1 The high energy PBT proposal represents a new clinical service not only for the Trustbut for the UK. The Trust recognised at an early stage that it was fundamental toseek external support from functioning PBT facilities. In this endeavour, the Trusthas committed substantial resource to better understand the delivery of PBT in a UKfacility. The Trust PBT team has been in place for some 4 years and to date everymember of the team has visited at least one PBT facility.
5.5.2 With regard the treatment pathway the Trust has been able to contrast overseasPBT advice with its local radiotherapy knowledge in order that it can betterunderstand and appropriately cost the treatment.
5.5.3 The clinical pathway is, in part, outside the control of the Trust in that the clinicalteam are generally only able to provide treatment once the patient presents at thefacility. Notwithstanding this, the Trust, during preparation of its initial PBT bid, tookthe opportunity to visit a number of UK Trusts that it felt would be highly influentialin supporting the national PBT programme. As well as assisting in identifying therequired clinical resource to deliver PBT, it identified certain costs that would beexcluded from the cost base i.e. patient transport and accommodation.







UCLH PBT Outline Business Case
Version 4 Page 120
5.9.2 The Department of Health has previously announced that of public finance willbe available to fund PBT. In our discussions with the DH PBT programme team wehave agreed in principle that an appropriate total public funding mix would beof PDC and FTFF. As identified in 5.4.3 above a potential 6 month programmeslippage has been quantified and the capital cost has been estimated to increase byaround . Accordingly the Trust has modelled the public funding mix as ofPDC and FTFF. The basis for this funding mix was that the high risk nature ofthe PBT programme was more suited to a substantial proportion of equity financeand because the two Trusts, might struggle to finance a significant portion of thePBT capital costs from other sources.
5.9.3 The OBC has been prepared on the basis that the PDC is in practice nonrepayable and carries a 3.5% cost of capital. Monitor currently treats PDC as equityfor accounting and regulatory purposes so the addition of the PDC represents arelatively low cost source of finance.
5.9.4 The proposed FTFF facility has not yet been formally established and so it isrecognised that there is a risk associated with movement in interest rates betweennow and formal approval of the FTFF facility. Should this arise, the SIF recognisesthat any change in interest rate will be addressed through the reimbursementfunding mechanism such that the DH bears the risk of any movement in interestrates.
5.9.5 The Trust has modelled the FTFF facility based on a 20 year repayable loan at a rateof Capital repayments will not commence until the first year of operation(18/19). The timing of the full repayment of the FTFF coincides with the potentialreplacement of the PBT equipment at or around the 20th year of operation. Currentlyit is expected that any capital refresh of the PBT equipment would be funded by afurther loan facility.
5.9.6 Donation funding is noted above including the that the Trust has informallycommitted to DH that it will raise. In order to raise this source the Trust will target acombination of both national and local charities although the fundraising potentialof PBT is thought to have been limited by the move to a 100% publicly fundedsolution. UCLH Charity has indicated in principle that it will commit £10m if sufficientfunds cannot be raised.
5.9.7 Finally, the cost of constructing the unequipped 4th room has been estimated at. The UCLH Trust Board recognises the “one off” opportunity to develop this 4th
room and has to date indicated that it is willing to fully fund this .
5.9.8 The Trust has agreed the principle that PDC will be drawn down first followed byFTFF and donations. The Trust has prepared an indicative capital spend profile withinthe SIF based on previously constructed Trust assets. This has been supplementedwith PBT specific knowledge i.e. indicative payment profile from PBT supplier. TheTrust is proposing to draw down PDC and FTFF a quarterly basis. The Trust can ofcourse further influence plusses and minuses by agreeing flexing supplier paymentterms.

UCLH PBT Outline Business Case
Version 4 Page 121
Conclusion on availability of funds
5.9.9 The analysis of funding options above has generated a preferred mix of sources offunds for the base case that should be available subject to changes of policy at DHand Monitor.
5.9.10 The SIF was approved by the DH on the basis of of PDC and of FTFF,although it is recognised that the FTFF has not been approved at this stage. Asidentified in section 5.13, the Trust recognises that Monitor has issued draftguidance “Risk Assessment Framework” (RAF) consultation document on 10 January2013. Although the Trust feels that the PBT proposal is suitably de risked from aTrust perspective, it is recognised that the Trust will be required to demonstrate tothe Regulator that the PBT proposal does not adversely affected its financialstanding, prior to it accessing any FTFF funding. In doing so, the Trust will berequired to demonstrate that the proposal does not have any adverse impact on itsrisk rating and that it can satisfy incumbent metric requirements such as being ableto service the Capital Funding requirements of the proposal.
5.9.11 The Trust has agreed to fully fund the for the additional room and endeavourto raise donation funding currently estimated at (subject to cost reductionsresulting from competitive procurement), of which it has received initial support of£10m.
5.9.12 Where there is any overrun in the cost base and a shortfall of source of funds arises,the SIF has identified a course of action to resolve the issue including, valueengineering, disproportionate sharing of donations with the Christie or additionalfunding support by DH.
5.9.13 In summary the Trust feels that there is a robust plan in place in order to raisesufficient source of funds to deliver the propose development.
5.10 Net Present Cost & Equivalent Annual Cost
5.10.1 As identified in the Economic Case, it has been recognised that currently there is apreferred option based on 3 gantry PBT option plus an additional Trust funded 4th
room. The PBT projections are based on a number of key financial assumptions(capital funding, tariff and non recurring funding) for which broad agreement hasbeen reached with DH.
5.10.2 On this basis, it should be recognised that the following NPV assessment for PBT hasbeen derived based on a number of assumptions, as included in Financial Appendix3E.
5.10.3 The Green Book provides guidance on the appropriate discount rate for thecalculation of NPV as:
Flows Y0 to Y30 – 3.5%
Flows Y31 to Y45 – 3.0%
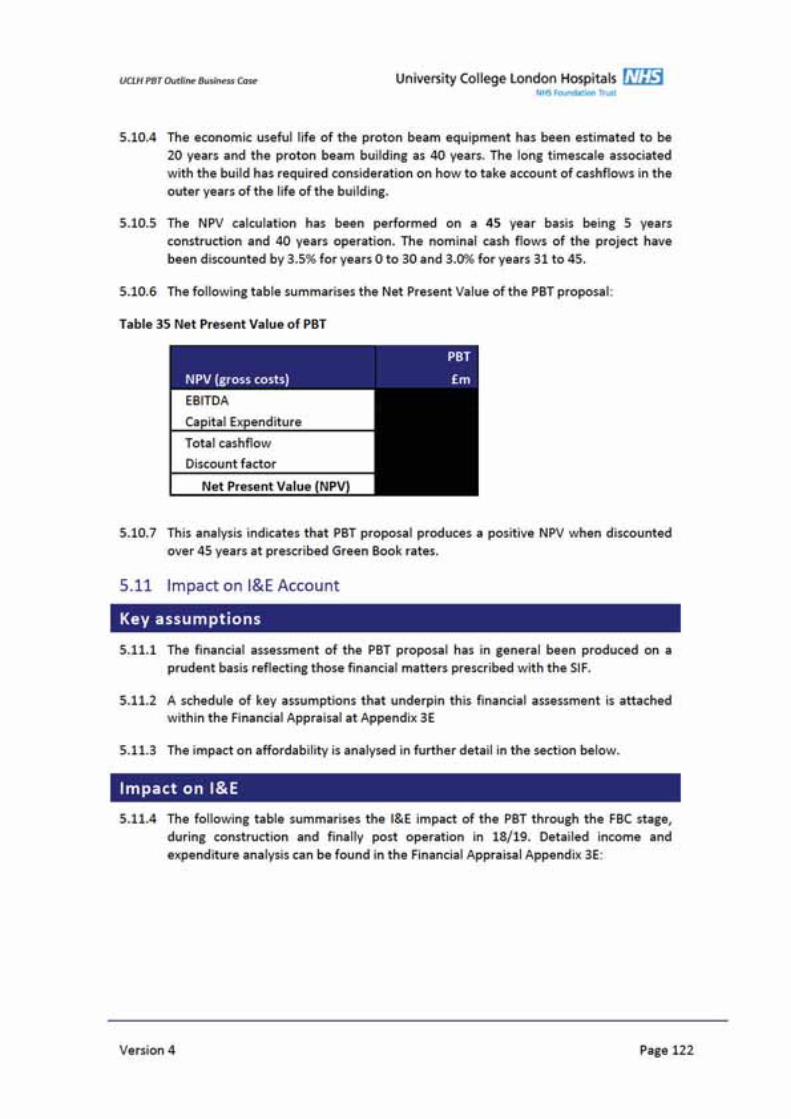


UCL
HPB
TO
utlin
eBu
sine
ssCa
se
5.11
.8Th
esu
bsta
ntia
llos
sin
18/1
9ar
ises
asa
resu
ltof
anes
timat
edim
pair
men
tof
the
faci
lity.
Prev
ious
expe
rien
ceha
ssh
own
that
upon
open
ing
ofa
new
faci
lity,
the
Trus
tw
illin
cur
anin
itial
impa
irm
ent
ofar
ound
20%
ofth
eco
stof
the
faci
lity
bein
gar
ound
.Thi
ssu
mis
part
ially
miti
gate
dby
the
2ndtr
anch
eof
dona
tion
inco
me
ofre
cogn
ised
inth
eI&
Ein
18/1
9
5.11
.9O
nce
the
PBT
faci
lity
isfu
llyop
erat
iona
laro
und
2020
/21,
the
Trus
tha
sde
rive
da
draf
tta
riff
that
crea
tes
am
odes
tsu
rplu
sof
abou
taf
ter
abso
rptio
nof
dire
ctco
sts,
indi
rect
cost
san
dap
prop
riat
eco
rpor
ate
over
head
s.
5.11
.10
Giv
enth
atPB
Tis
aca
pita
lint
ensi
vetr
eatm
ent
this
mea
nsth
atth
epr
opos
alge
nera
tes
anEB
ITD
Am
argi
nof
mor
eth
an40
%,t
his
bein
gre
quir
edto
cove
rde
prec
iatio
n,fin
ance
PDC
and
FTFF
inte
rest
char
gean
dto
gene
rate
am
odes
tsu
rplu
sm
argi
n.Th
isEB
ITD
Am
argi
nis
very
diff
eren
tin
prof
ileto
the
Trus
t’s
curr
entE
BITD
Am
argi
nth
isbe
ing
9.7%
in20
11/1
2.
5.11
.11
Furt
her
deta
ilsof
the
assu
mpt
ions
used
tode
velo
pth
efo
reca
sts
for
the
impa
ctof
PBT
are
seto
utin
the
Fina
ncia
lApp
rais
alA
ppen
dix
3E.
Vers
ion
4Pa
ge12
4


UCLH PBT Outline Business Case
Version 4 Page 126
5.12.2 The impact of PBT is that it increases the Trust’s net assets by around (postimpairment) when compared to the 11/12 final net assets position of . Thisincrease is mainly in fixed assets being funded by PDC and FTFF. This effect on theTrust’s balance sheet is relatively disproportionate to the size of the new PBT servicebecause PBT is capital intensive compared to other Trust services and because thatcapital is funded in part by additional equity of whereas almost half (44%) ofthe Trust’s current financing is from debt and PFI obligations.
5.13 Impact on Risk Ratios
5.13.1 The Trust is currently regulated against five key financial ratios by Monitor:achievement of plan (i.e. accuracy of EBITDA forecasts); EBITDA margin, surplusmargin, net return after financing (a measure of underlying surplus divided by totalfinancing) and liquidity (liquid assets expressed as days of operating expenditure).Monitor is consulting on a risk assessment framework to replace these ratios from 1April 2013, but details are limited at present.
5.13.2 The Trust recognises that Monitor issued draft guidance “Risk AssessmentFramework” (RAF) consultation document on 10 January 2013, the deadline forresponses being 4 April 2013. Broadly this draft RAF builds extensively on theexisting Compliance Framework. Subject to consultation, Monitor intended to runelements of the new framework in “shadow” for the first 6 months of 13/14. Insummary, this draft guidance proposes to use a new risk rating based on only 2metrics, namely:
Liquidity Ratio
Capital Servicing capacity
5.13.3 Given that RAF is only in draft format at this stage there is clearly an inherent risk inattempting to provide a definitive estimate regarding the impact that the PBTproposal may have on the Trust’s overall ratios. However, the Trust has in generalconsidered the potential impact of the PBT proposal on these new metrics. Giventhe funding for the proposal will be a mix of both PDC and FTFF, the developmentwould appear to leave the Trust’s overall risk rating broadly unchanged.Notwithstanding this, the SIF includes provision that the PBT proposal should notdilute the Trusts margin.
5.13.4 The financial risk ratios were designed by Monitor to indicate financial risk in NHSbusinesses within a normal range of financial profiles. That is to say Trusts withEBITDA margin between 5% and 10% and making surplus margins of between 1%and 3%. PBT is unusual in an NHS context in being very capital intensive generatinghigh EBITDA margin in order to meet high depreciation and financing charges. Thishigh EBITDA margin means that any service will receive favourable ratings in anysystem based on EBITDA margin and measures of liquidity in relation to operatingexpenses. This effect is inherent in PBT and is unlikely to be significantly altered bythe results of on going negotiations with the Department of Health.
5.13.5 It is likely that any metric based on accuracy of planning could be adversely affectedby PBT given that it may be difficult to plan accurately in the early years. There maybe a similar effect for the Above Ground operations given the experience of movinginto Phase 3
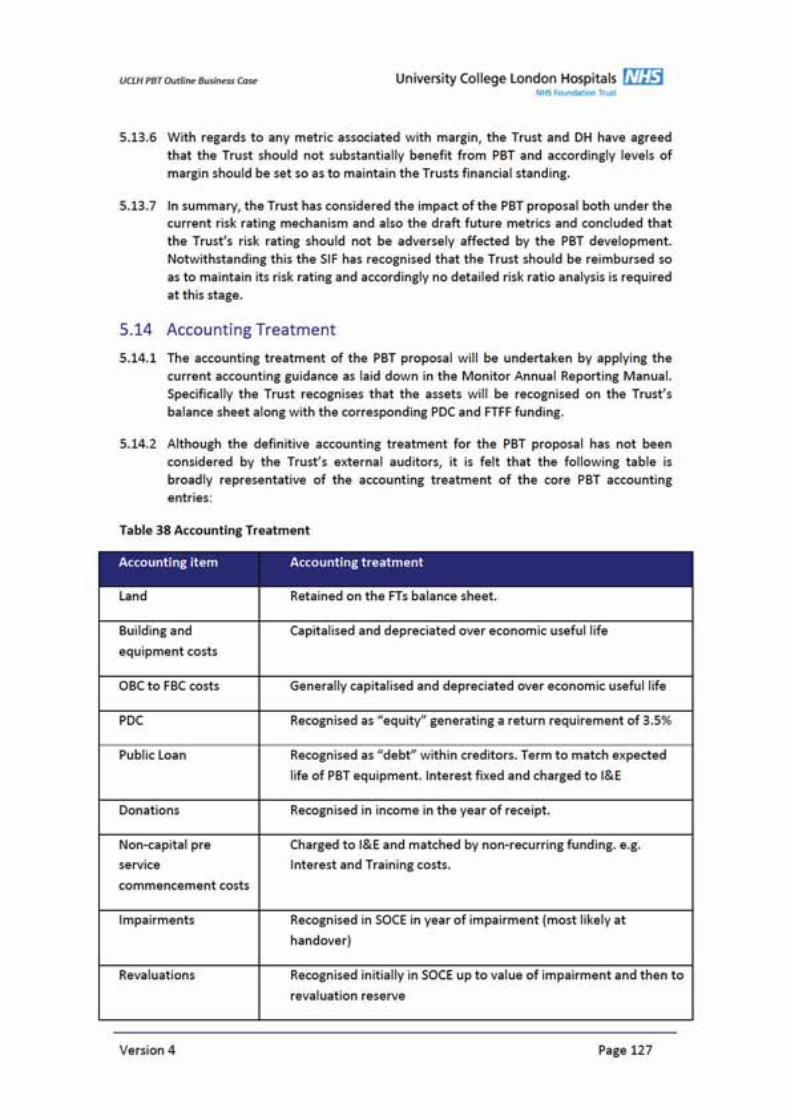


UCLH PBT Outline Business Case
Version 4 Page 129
Chapter 6: Management Case
Why the chapter matters
As a subset of the National PBT Programme, UCLH have instigated robust ProjectManagement arrangements to ensure the successful delivery of PBT at the Trust. PBT formspart of the overall Phase 4 Development at UCLH.
What the chapter says
This chapter of the OBC addresses the “achievability” of the scheme setting out the actionsrequired to ensure its successful delivery in accordance with best practice. It outlines theUCLH internal programme management arrangements as well as the externalinterdependencies with the PBT National Programme.
Section 1: External Programme Management Arrangements
6.1 National Programme Management
6.1.1 The UCLH PBT facility is one of two projects that forms part of the DH’s programmeto develop a National PBT service in the UK. The DH has developed wider strategicprogramme interdependencies at a national level including programmemanagement structures, governance and stakeholder management arrangements.The National Programme Management arrangements are detailed in the DH SIF andsummarised in the Figure below, with representatives from UCLH sitting on the JointProgramme Board as required.

UCLH PBT Outline Business Case
Version 4 Page 130
Figure 5 National PBT Programme Management Arrangements
6.2 UCLH and The Christie Joint Working
6.2.1 UCLH and the Christie will continue their close working relationships at both theworkstream and executive levels to ensure the development of the service iscoordinated nationally. Operational and strategic items in need of wider discussionwill be brought to the existing Joint Working Group currently held on a bi monthlybasis.
6.2.2 The Joint Working Group is currently chaired by.

UCLH PBT Outline Business Case
Version 4 Page 131
Section 2: Internal Programme Management Arrangements
6.3 UCLH Programme Management
6.3.1 The PBT project will be managed as part of the wider UCLH Phase 4 Programmestructure. The purpose of Phase 4 Development is to deliver the next stage of theUCLH vision and associated service strategy as highlighted in the StrategicCase.
,all of which seek to improve patient outcomes and experience and provide seamlessand efficient pathways of care.
6.3.2 The Phase 4 Programme comprises of a portfolio of projects including:
Decant and demolition of the Rosenheim building, currently occupying theOdeon and Rosenheim site.
Design and construction of the PBT facility
Design and construction of an “above ground” clinical facility.
Development of Commercial space and the management of site disposalsthat contribute towards the overall financing strategy of the development
The development of plans to potentially backfill services in Phases 1,2 and 3.
6.3.3 UCLH have implemented Programme Management arrangements to facilitate theachievability of Phase 4 which will be managed in accordance with PRINCE2methodology. The key programme management team comprises of the Phase 4Programme Board, the Phase 4 Working Group, Workstream leads, Project leads andspecialist Project Advisors as shown in the below Phase 4 Project Organogram:

UCL
HPB
TO
utlin
eBu
sine
ssCa
se
Vers
ion
4Pa
ge13
2
Figu
re6
Phas
e4
Prog
ram
me
Org
anog
ram

UCLH PBT Outline Business Case
Version 4 Page 133
6.4 Programme Reporting Structure
6.4.1 In order to support clinical ownership and engagement in the whole life of theprogramme, the reporting structure is divided into three clinical projects and fourfunctional workstreams as shown in the below diagram.
Figure 7 Phase 4 Clinical Projects and Functional Workstreams
6.4.2 The Clinical Projects have overall responsibility for the successful achievement of theproject deliverables and utilise the resources and expertise of the functionalworkstreams. The following programme management arrangements have beenimplemented to ensure clinical and operational engagement and responsibility,supported by functional expertise:
The Clinical Projects each have a clinical and operational lead who representtheir project at the Phase 4 Programme Board and a project manager whoregularly reports to the Phase 4 Working Group regarding the on goingstatus of deliverables.
Each Clinical Project has a Project Initiation Document (PID) that highlightsthe project aims and objectives, structure, roles and responsibilities,deliverables and timescales.
Functional Workstream leads are members of the Phase 4 Programme Boardand Working Group and report to the Programme Board on a monthly basisvia the Programme Management Office (PMO).
Each Functional Workstream has a workstream plan that highlights theproject aims and objectives, structure, roles and responsibilities,deliverables and timescales.


UCLH PBT Outline Business Case
Version 4 Page 138
Follow up to ensure actions from both these meetings are completedagainst the required delivery dates
Overview of the project work streams to ensure seamless communication
Business case development and management
Maintenance of the project and workstream governance structures andoverall PID.
Risk register management
UCLH Board, SPB and Committee updates
Change Control Process management
Knowledge Management System
6.4.10 The Programme Management for this project at OBC stage has been outsourced to.
Proton Beam Therapy: Project Management
6.4.11 As previously identified, PBT forms one of the Phase 4 Developments ClinicalProjects.
6.4.12 The PBT Project is structured as shown in figure 8. Operational, clinical and strategicPBT leads represent the project on both the Phase 4 Working Group and Phase 4Programme Board. The PBT Project Team Sponsor and Chair is
.

UCL
HPB
TO
utlin
eBu
sine
ssCa
se
Figu
re8
PBT
Proj
ectS
truc
ture
Vers
ion
4Pa
ge13
9




UCLH PBT Outline Business Case
Version 4 Page 144
6.5.3 The team, either in part or whole, has visited more than ten working PBT centrestogether with a newly commissioned site in Europe. Amongst these visits are;
2008 – Paris, France: Understanding the pathways of UK patients sent fortreatment
2009 – ProCure Proton Therapy Center in Oklahoma City, U.S.A: Patientpathways, imaging and throughput
2009 – University Hospital of Heidelberg Ion Therapy Centre, Germany: ProtonConference and clinical visit.
2009 – Rinecker Proton Therapy Centre in Munich, Germany: Patient pathways,clinical protocols and patient throughput.
2010 – International Proton conference in Japan and visit to Japanese PBTcentres together with a visit to Accelerator manufacturers
2010 – West German Proton Therapy Centre at Essen University Hospital, ,Germany: Understanding contractual situation together with imaging andpatient pathway development
2010 – Site Visits to the Roberts Proton Therapy Centre at the University ofPennsylvania, Philadelphia and the University of Florida Proton TherapyInstitute, Jacksonville: Networking with the clinical sites taking UK patients underthe Department of Health PBT Programme for patients to be treated abroad.
2012 – The University of Florida Proton Therapy Institute visit to UCLH and UCL
2012 – visit to the Roberts Proton Therapy Centre at theUniversity of Pennsylvania, Philadelphia and Massachusetts General HospitalFrancis H. Burr Proton Therapy Centre, Boston
6.5.4 The visits have enabled the project team to clearly understand the needs of patientsundergoing PBT treatment abroad as well as the design of facilities and financialmodels. The last visit allowed UCLH to develop an in depth understanding of thechallenges facing UCLH in the development of a PBT centres in the UK. Theseincluded service ramp up and patient pathways, patient imaging, complex PBTdelivery and the depth of the physics service required to deliver.
6.5.5 In the interim, visits by the physics team have been made to the
During this time the knowledge base for all aspects of the PBT process has extendedand deepened. Our links with all disciplines has strengthened and we are regularlyworking now with several PBT centres over PBT physics dosimetry, operationalissues and Clinical complexity and patient throughput.

UCLH PBT Outline Business Case
Version 4 Page 145
6.5.6 UCLH have hosted visiting experts from some of these sites. The clinical oncologydepartment have received excellent feedback from these experts with regard to theway we are delivering our existing Radiotherapy Practice, and in the way we aredeveloping models to deliver the National service with The Christie.
6.5.7 To date several members of clinical oncology have attended accredited PBT trainingschools.
6.5.8 There are outline plans to begin staffing the PBT centre following the business caseapproval for the activities required pre opening, planning and preparation purposes.The most active recruitment will be required in Medical Physics within CancerServices:
A Head of Proton Radiotherapy Physics and an Operational Lead will beappointed in the third year before opening. The former will be anexperienced Senior Physicist from a long standing Proton Centre. They willbe overseeing all of the technical and logistic details during the design,tender, procurement and installation periods. They would visit existingProton Centres, and work in close collaboration with the vendors, externalconsultants and the Physics counterparts in the Christie PBT Centre
In the second year before opening, two dosimetrists and an additionalPhysicist will be recruited. They will be seconded (under an SLA) for a sixmonth period each to existing Proton Centres abroad to become proficientin planning and QA techniques for protons. They will spend the rest of thetime becoming familiar with UCLH photon practice (IMRT, RapidArc).
In the year before clinical operations, the PBT centre will have a staffingcomplement equivalent to around half the level at the opening of thecentre, as three major activities will need to be pursued:
Acceptance and commissioning of the first three treatment rooms
Double planning of all proton eligible patients that are treated atUCLH that year. This exercise will ensure that staff are up to speedwith the TPS and proton specific techniques by the time the firstpatients are treated with PBT. Cascade training will be given by thepreviously trained staff. Cross site double planning can happen withthe Christie PBT Centre.
Patient Specific Quality Assurance on a wide selection of doubleplans. These dosimetry measurements will happen as part of thecommissioning of the first room, before the first patient is treated.Cascade training will be given by the previously trained staff. Crosssite QA can happen with the Christie PBT Centre if beam is available
6.5.9 The Programme currently includes plans for an extensive PBT training programmefor UCLH clinicians, medical physicists and Radiotherapy staff after the FBC isapproved and in advance of the PBT centre going operational. This includes plans topartner with a current PBT centre for training and education purposes. Full detailson the training programme will be worked up for the FBC with the appropriate

UCLH PBT Outline Business Case
Version 4 Page 146
partnering centre dependent on the choice over PBT equipment vendor. It isanticipated that most training for radiotherapy staff could happen in the UK. A coregroup together with some specialist posts will need to visit and understand thedelivery requirements in a functioning centre, but the process should be less timeand cost intensive than those for clinical and physics staff. A training programme willbe focused on:
Vendor training: At present vendors routinely train radiography staff on newequipment. This requirement will be made in our tender
Visits to foreign PBT centres: These will be short placements (between one andfour weeks), based at centres which use the same vendor we are intending to. Acore group of radiographers (around five) alongside lead clinicians will thenreturn and deliver continual training to the rest of the staff
Early access: All radiographers will be given the opportunity to visit thedepartment prior to opening and familiarise themselves with the environment,treatment equipment, rooms, software and hardware
External support after opening: For a period of 3 6 months after opening, wewould plan to have a radiographer experienced in PBT stationed in theDepartment – to assist with the continuous on going development of all staff.We anticipate it being much easier to hire such an expert radiographer thansimilarly qualified clinicians and physicists
6.6 Project Plan
6.6.1 An indicative project plan has been developed and will be included followingapproval of the OBC.
6.6.2 The DH programme for the delivery of the PBT facility include the followingassumptions:
Specifications for the PBT Equipment will be drawn up and agreed between theDH and The Christie ready to commence the Competitive Dialogue process.
The Competitive Dialogue process will seek expressions of interest and thenshortlist 2 3 potential equipment vendors for the dialogue process. Thedialogue process is set to be two stages followed by a final tender to select apreferred vendor.
The selection of a preferred equipment vendor will allow the design to concludeand a tender to be issued for a building contractor
Business cases for both the procurement of the equipment and the buildingcontractor for the PBT will require approval by DH and HM Treasury are subjectto Cabinet Office Gateway Reviews.
The installation, commissioning and calibration are programmed for 18 monthsmeaning that first patients will be treated in mid 2018.




UCLH PBT Outline Business Case
Version 4 Page 150
6.10 Outline Arrangements for Benefits Realisation
6.10.1 The Phase 4 Benefits Realisation Plan identifies the benefits planned for the project.
6.10.2 The projects outline arrangements for Benefit Realisation Planning include:
Agreeing the desired benefits for Phase 4 with project stakeholders.
Identifying the outcomes and enablers affected by each benefit.
Determining measurements to identify when a benefit has been realised andallocating responsibility for the delivery of these benefits.
6.10.3 The Phase 4 Programme Board will manage and monitor the projects BenefitsRegister.
6.11 Overall Approach to Risk Analysis & Management
6.11.1 Risk management is an essential part of the development of any project. Risk shouldbe managed proactively through a process of identification, assessment andmitigation. The Risk Management Strategy will incorporate the following activities:
Risk identification and reporting
Evaluation of proximity, probability and impact of the risk occurring
Allocation of risk owner
Development of risk responses including prevention, reduction, transference,acceptance of reduction
Identification of escalation procedures
Planning and resourcing of responses to risks
Monitoring and reporting of risk status
6.11.2 There is significant interdependency between the UCLH and the Christie PBTschemes, Appendix 6D outlines the PBT contingency paper submitted to theNational PBT Programme Steering Committee and sets out the interdependenciesbetween the two centres and how to manage the risks.
Stage 1: Risk identification and Assessment
6.11.3 The identification and assessment of risks at the OBC stage was conducted at a riskworkshop where the following attended:
UCLH PBT Outline Business Case
Version 4 Page 151
6.11.4 Attendees identified the key strategic, commercial, financial, design / technical andclinical risks associated with the project.
6.11.5 Operational risks for the clinical services were collated via 1:1’s with the projectsidentified operational leads and the inclusion of the existing PBT risk register thatwas initially developed at the preliminary stages of the PBT project and supported bya further risk workshop with the DH.
Stage 2: Risk mitigations
6.11.6 The mitigation of the identified risks at the OBC stage was conducted at a riskworkshop on the 17th August 2012 where the following attended:
6.11.7 From the previously identified risks, attendees at this workshop sought to identifyrealistic mitigations for each risk and then re score based on the successfulcompletion of these mitigation actions. Additional risks were also added whereappropriate.
Future Stages for Risk Management
6.11.8 The following identifies the future stages of the projects where a risk determinationand analysis will be conducted by the Phase 4 Programme Board and associatedclinical and operational project leads. This process will be managed by the Phase 4Programme Manager.
Post OBC UCLH Board (and HM Treasury approval for PBT OBC)
Design specific workshops for the development of the designs and associatedrisk areas (e.g. sustainability)
FBC completion and submission to UCLH Board (and HM Treasury for PBT FBC)
Contract signature and financial close
Design completion
Facility opening
Project handover
Commissioning Commencement


UCLH PBT Outline Business Case
Version 4 Page 154
6.12 Outline Arrangements for Post Project Evaluation
6.12.1 The outline arrangements for post implementation review (PIR) and projectevaluation reviews (PER) have been established in accordance with best practice andare as follows.
Post Implementation Review (PIR)
6.12.2 This review will ascertain how well the project has been managed which will includean End Project Report and a Lessons Learnt Report. This will be carried out by aproject manager, independent to the programme, to obtain an objective evaluationof the delivery of the project.
Project Evaluation Reviews (PERs)
6.12.3 PERs are learning tools that ensure UCLH and other stakeholders apply theknowledge gained from the Phase 4 Programme to future projects. UCLH arecommitted to ensuring PERs are undertaken in order to assess how the Programmehas met its objectives and realised the project benefits.
6.12.4 The DH published guidance identifies the following key evaluation stages:
Stage 1 Project Procurement: OBC to Financial Close
Stage 2 Implementation: Financial Close to Practical Completion
Stage 3 Initial: Operational Commissioning to first 6 months of operation
Stage 4 Follow Up: 6 months to first 2 years of operational phase
6.12.5 Evaluation reports will be completed within six months of the data collection foreach stage outlined above and will be disseminated to stakeholders followingapproval by the Phase 4 Programme Board.
6.12.6 The Phase 4 Project Working Group will manage the PER process on behalf of thePhase 4 Programme Board, supported by an independent review body.
6.13 Approvals Process and DH Gateways
6.13.1 A Major Project is defined as central government funded project or programme thatrequires HM Treasury approval during its life, as set out in Delegated Authorityletters, or is otherwise of special interest to the Government, delivering ProtonBeam Therapy in the UK falls under this definition. The HM Treasury has revised itsproject approval processes as part of a wider programme of strengthened spendingcontrol. These revisions aim to provide a more coherent approvals and assuranceframework, and make the tools HM Treasury uses to approve major projects moreconsistent across Government.
6.13.2 HM Treasury approval is required for major projects at 3 key business case stages:
Strategic Outline Case





UCLH PBT Outline Business Case
Version 4 Page 159
NHS National Health Service
NPC Net Present Cost
NPV Net Present Value
NSCG National Specialised Commissioning Group
NWL North West London
OBC Outline Business Case
OPD Outpatients Department
PACS Picture Archiving and Communication System
PBL Prudential Borrowing Limits
PBR Payment By Results
PBT Proton Beam Therapy
PDC Public Dividend Capital
PDT Photo dynamic therapy
PFI Private Finance
PID Project Initiation Document
QALY Quality Adjusted Life Years
QEP Quality, Efficiency and Productivity Programme
RFH Royal Free London NHS Foundation Trust
RFID Radio Frequency Identification
RIBA Royal Institute of British Architects
RNTNEH Royal National Throat, Nose and Ear Hospital
RRO Radiology Reporting Online
SIF Strategic Investment Framework
SoA Schedule of accommodation
SOC Strategic Outline Case
The Christie The Christie NHS Foundation Trust
UCH Campus University College Hospital Main Campus (Phase 1)
UCL University College London
UCLH University College London Hospitals NHS Foundation Trust (Trust)
UCLP University College London Partners
VfM Value for Money
WACC Weighted Average Cost of Capital